Embed Size (px)
DESCRIPTION
Citation preview

The D2B Quality Alliance
Matthew E. Fitzgerald, DrPH
Sr. Director, Science & Quality
American College of Cardiology

Evidence-base Review Subgroup
Betsy Bradley, PhD – Chair• Yale School of Public Health
– Connecticut
Jeptha Curtis, MD• Yale University
– Connecticut
Chris Granger, MD• Duke Clinical Research
Institute– North Carolina
Mauro Moscucci, MD• University of Michigan
– Michigan
Brahmajee Nallamothu, MD• University of Michigan
– Michigan
Harlan Krumholz, MD• Yale University
– Connecticut

Evaluation and Research Subgroup
Brahmajee Nallamothu, MD – Chair• University of Michigan - Michigan
Wayne Batchelor, MD• Southern Medical Group - Florida
Betsy Bradley, PhD• Yale School of Public Health -
Connecticut Jeptha Curtis, MD
• Yale University - Connecticut Chris Granger, MD
• Duke Clinical Research Institute– North Carolina
Harlan Krumholz, MD• Yale University - Connecticut
Mauro Moscucci, MD• University of Michigan - Michigan
April Simon, RN, MSN• Cardiac Data Solutions - Indiana
Kalon Ho, MD• Beth Israel Deaconess Medical Center
- Massachusetts David Janicke, MD
• SUNY at Buffalo - New York Fred Masoudi, MD, MPH
• Denver Health Medical Center - Colorado

Toolkit Subgroup
Wayne Batchelor, MD - Chair• Southern Medical Group
– Florida Ralph Brindis, MD, MPH
• Oakland Kaiser Medical Center– California
Jeptha Curtis, MD• Yale University
– Connecticut Eva Kline-Rogers, RN, MS
• University of Michigan– Michigan
Harlan Krumholz, MD• Yale University
– Connecticut Peter O’Brien, MD
• Lynchburg General Hospital– Virginia
Art Riba, MD• Oakwood Hospital and Medical Ctr
- Michigan April Simon, RN, MSN
• Cardiac Data Solutions– Indiana
Charles Chambers, MD• Penn State Milton Hershey Med Ctr
– Pennsylvania David Magid, MD, MPH
• Kaiser Permanente– Colorado

Change Package Subgroup
Eva Kline-Rogers, RN, MS - Chair• University of Michigan –
– Michigan
Wayne Batchelor, MD• Southern Medical Group
– Florida
Chris Granger, MD• Duke Clinical Research Institute
– North Carolina
Harlan Krumholz, MD• Yale University
– Connecticut
Mauro Moscucci, MD• University of Michigan
– Michigan
Ivan Rokos, MD• UCLA – Olive View
– California
Aaron Kugelmass, MD• Henry Ford Health System
– Michigan
Barry Uretsky, MD• University of Texas – Galveston
– Texas

Partnership and Communications Subgroup
John Brush, MD – Chair• Sentara Hospital
– Virginia Ralph Brindis, MD, MPH
• Oakland Kaiser Medical Center– California
Harlan Krumholz, MD• Yale University
– Connecticut Peter O’Brien, MD
• Lynchburg General Hospital– Virginia
Art Riba, MD• Oakwood Hospital and Medical Ctr
– Michigan
April Simon, RN, MSN• Cardiac Data Solutions
– Indiana Ivan Rokos, MD
• UCLA – Olive View– California
Barry Uretsky, MD• University of Texas – Galveston
– Texas Henry Ting, MD
• Mayo Clinic– Minnesota

PIM Subgroup
Eric S Holmboe, MD• American Board of Internal
Medicine– Pennsylvania
Henry Ting, MD• Mayo Clinic
– Minnesota Ivan Rokos, MD
• UCLA – Olive View– California
Janet Parkesovich• Yale New Haven Hospital
– Connecticut
Patrick O’Gara, MD• Brigham & Women’s Hospital
– Massachusetts John Spertus, MD, MPH
• Mid America Heart Institute– Missouri
Martha Radford, MD• New York University Hospitals Ctr
– New York

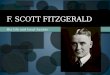
Relationship Between Delay in PTCA and 30-day Mortality
Primary PTCA in the Era of Balloon Angioplasty
GUSTO IIb Substudy
Berger et al. Circulation 1999;100:14.
1.0%
3.7%4.0%
6.4%
0%
1%
2%
3%
4%
5%
6%
7%
< 60 min 61-75 76-90 > 90

020
40
60
80
100
120
Door-
to-b
alloon tim
e (
min
ute
s)
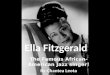
Jan 99 Jul 00 Jan 02 Jul 03Month
National Trend in Door-to-Balloon Time
1999-2003

Percent of Hospitals Meeting Median Door-to-Balloon Times Guidelines
McNamara et al., JACC 2006

010
20
30
40
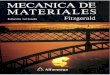
Hospitals
50 100 150 200Door-to-balloon time (minutes)
Hospital-Level Variation in Median Door-to-Balloon Times

D2B Quality Alliance Goal
Goal: • To improve door-to-balloon (D2B) times at participating
hospitals in non-transfer patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI).
Outcome Measure:• The proportion of hospitals with at least 75 percent of all
their non-transfer patients undergoing primary PCI with D2B times of 90 minutes or less.

Evidence Base
Synthesis of existing literature (13 studies)
- Pre/post interventional studies
- Qualitative studies of top performers
- National cross-sectional studies
Together, these data provide insights about specific interventions that work

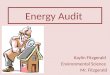
Time Intervals in Fastest and Slowest Quintiles of Hospitals
0
20
40
60
80
Door-to-ECG ECG-to-Lab Lab-to-Balloon
Fastest
Slowest
Bradley et al., AHJ 2006

Strategies that Work (10-15 minutes saving in some cases)
1. ED activation of cath lab 2. Single-call system 3. Cath team target 20-30 minute assembly time4. Prompt data feedback to ED and cath lab staff5. Senior management commitment6. Team-based approach7. Pre-hospital ECGs activate cath lab team

Room for ImprovementEmergency medicine activation
22% of hospitals on days27% of hospital on nights and weekends
Single-call system14% of hospitals
Expectation for cath lab team arrival after page11% of hospitals within 20 minutes77% of hospitals within 21-30 minutes

Interaction Among EMS, ED, and Cath Lab
EMS routinely calls in or transmits ECGs
40% of hospitals
Hospital activates while patient is still en route
9% of hospitals

Reported False Alarm Rates
Hospitals where cardiology activates cath lab 1 (range: 0-3) in 6 months
Hospitals where emergency medicine activates 2 (range: 1-4) in 6 months
Hospitals that activate while patient en route
2 (range: 1-4) in 6 months

Organizational Context Explicit goal of improving door-to-balloon time
Senior management support
Uncompromising clinical champions (and teams)
Organizational culture that fostered resilience to challenges and setbacks (non-blame)
Data feedback to trend, motivate, and reward

Summary
The literature supports a set of specific strategies associated with faster door-to-balloon time
These are underutilized currently
Changes require organizational commitment and cooperation among disciplines and departments
National GAP-D2B campaign can help foster needed organizational visibility and commitment

D2B Tool Kit SubgroupD2B Tool Kit Subgroup
Developed by experts in the field and in Developed by experts in the field and in D2B researchD2B research
Included representatives of D2B Team Included representatives of D2B Team across disciplines and specialties:across disciplines and specialties:
• Nurses Nurses
• Emergency physiciansEmergency physicians
• Interventional cardiologistsInterventional cardiologists
• Quality improvement professionalsQuality improvement professionals

Tool Kit Development
Tools from other facilities are compiled, assessed, and modified for D2B Tool Kit
development.
Hospital Site Review
Development ProcessDevelopment Process
D2B Work Group Review
Peer Review
Three-part review process to ensure a high-Three-part review process to ensure a high-quality tool kitquality tool kit

Development ProcessDevelopment Process
Step 1 - Call for D2B ToolsStep 1 - Call for D2B Tools Requested all hospitals performing primary PCI to submit tools and QI storiesRequested all hospitals performing primary PCI to submit tools and QI stories
Step 2 – Assess Tools ReceivedStep 2 – Assess Tools Received Identified tools from the existing collection that support Tier 1 strategiesIdentified tools from the existing collection that support Tier 1 strategies
Step 3 – Modify/Develop ToolsStep 3 – Modify/Develop Tools Modified existing tools and/or developed new tools to support Tier 1 strategiesModified existing tools and/or developed new tools to support Tier 1 strategies

Development ProcessDevelopment Process
Step 4 – Finalize Draft #1Step 4 – Finalize Draft #1 Finalize D2B Tool Kit (Draft #1) by incorporating D2B Finalize D2B Tool Kit (Draft #1) by incorporating D2B
Tool Kit Subgroup commentsTool Kit Subgroup comments
Step 5 – Initiate Review ProcessStep 5 – Initiate Review Process Initiate Review Process by releasing Draft #2 to hospital Initiate Review Process by releasing Draft #2 to hospital
reviewers and peer reviewersreviewers and peer reviewers

D2B Tool KitD2B Tool Kit
How to use D2B toolkitHow to use D2B toolkit Strategies ChecklistStrategies Checklist Process Flow ChartProcess Flow Chart ““STEMI Alert” ChecklistSTEMI Alert” Checklist Cath Lab Activation Protocol Cath Lab Activation Protocol Team Roles and ResponsibilitiesTeam Roles and Responsibilities Time Entry Form with Target TimesTime Entry Form with Target Times Data Collection FormData Collection Form Standard Order SetStandard Order Set Pre-hospital ECG ChecklistPre-hospital ECG Checklist

Take Home MessagesTake Home Messages
The D2B Tool Kit…The D2B Tool Kit… is based on practical tools from the fieldis based on practical tools from the field is intended to be easily implementedis intended to be easily implemented applies evidence-based strategies for D2B improvementapplies evidence-based strategies for D2B improvement is constantly improving based on user feedbackis constantly improving based on user feedback

D2B: An Alliance for Quality
International quality improvement campaign to reduce door-to-balloon times in STEMI patients
200+ hospitals, 27 strategic partners (and growing!) Participating hospitals asked to commit to following:
• Implement as many of 6 evidence-based strategies as possible• Allow ACC to publicize their good efforts
• Complete three surveys to let ACC know what the hospital is doing to improve D2B times
• Participate in the D2B online community to share experiences and learn from others

D2B: An Alliance for Quality
Reasons for joining D2B:• Improve on CMS/JCAHO core measure results
• ABIM and CME credit for participation
• Publicity for your efforts
• No cost to hospitals to join
• It’s the right thing to do!
March 1, 2007 – deadline for hospitals to join D2B and be included in initial public release of participating hospitals at ACC ’07 (hospitals are permitted to join after March 1)
More information: www.d2balliance.org

How can hospitals join D2B?
By visiting www.d2balliance.org

D2B Manual and Tool Kit

D2B Tool Kit
The D2B Tool Kit is located about midway down the “D2B Implementation Manual” web page. Hospitals can access each tool to determine whether it is appropriate for their facility and are encouraged to modify tools to fit their needs.

How to Participate and What is Expected of Hospitals
Complete a Participation Agreement and Join the D2B Alliance!
Commit to implementing the evidence-based strategies.
Allow D2B Alliance to use hospital name in D2B promotional materials.
Help contribute to the learning community by sharing stories, successes and obstacles.
And it’s FREE - No cost to join.

Where can I get more information?
www.d2balliance.com
* website for information on D2B, download tools and resources, sign up your hospital
and participate in the online D2B community D2B Staff Email – [email protected]