Embed Size (px)
Citation preview

Matthew Doyle, MS, LAT, ATC

Definitions Pathogenesis Pathophysiology Treatment options What we do at the
University of Iowa and why

UNTREATED OR MISMANAGED AURICULAR HEMATOMA
FIBRO-NEOCARTILAGE FORMATION STARTS @ 7-10 DAYS


Caused by blunt trauma Tangent/shearing
forces, commonly occurs: during a takedown or
from the neutral position
when athlete isn’t wearing headgear or wears a poor fitting protector and fails to adjust it properly
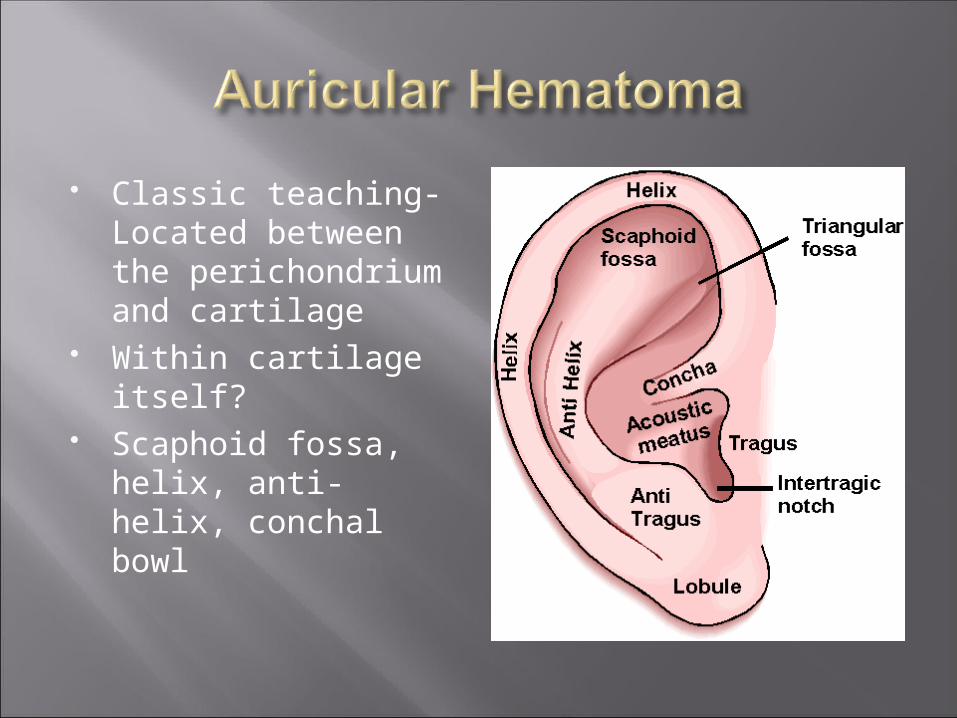
Classic teaching- Located between the perichondrium and cartilage
Within cartilage itself? Scaphoid fossa, helix,
anti-helix, conchal bowl

Proper management of auricular hematoma Protection
Headgear use became mandatory for NCAA wrestling competition in the late 1960s
Mandatory for wrestling practice in 2004 Not used in international competition or post collegiate
wrestling; Rugby rules? Compliance?


No randomized controlled trials, clinical trials, or cohort studies
48 Articles: Reviews, expert opinions, case series, case reports
Jones SE, Mahendran S. Interventions for acute auricular hematoma (Review). Cochrane Database of Systematic Reviews 2004 (2).

Treatment: Remove hematoma and prevent recurrence No clear consensus exists for best treatment Various interventions are effective
Literature generally agrees that treatment is better than no treatment
Small risk other than failure, leading to re-accumulation or deformity
Infection (acquired or induced by tx) may result in serious consequences of perichondritis and severe tissue loss

Perichondritis and chondritis; erythema, tenderness, recurrent swelling
Cartilage necrosis, contracture, and neocartilage

Cosmesis Reconstructive plastic surgery for cauliflower deformity
Functional Hearing loss Wax transport from the ear canal Increased risk of otitis externa Difficulty wearing earphones

Time consuming Missed training and competition Viewed as cosmetic problem not worthy of time
loss “A mark of pride and distinction” Cauliflower Ear Deformity remains a common
stigmata to wrestlers, boxers, and rugby players Noncompliance due to refusal to stop training

Adequate removal of hematoma Simple and effective method of maintaining
pressure to prevent recurrence Satisfactory aesthetics Appropriate follow up Minimal impact on patient activity

Removal of hematoma Needle Aspiration Incision and drainage Incision and drainage with resection of cartilage
Prevention of reaccumulation Non-invasive Invasive

Invasive Bolsters (Cotton, buttons, thermoplastic splint)
Through and through suturing Tie over dressings
Placement of drains (passive or suction) Antibiotic prophylaxis
Noninvasive Application of plaster mold, silicone splints, cotton/wool
impregnated with collodion, swimmer’s nose clip










First line of treatment approved by Otolaryngology
Needle aspiration Collodion Casting (Jaffee) Simple, effective,
cosmetically satisfactory, allow quick return
Many just want reduction of pain

Koopman (1979) and Schuller et al (1989) technique preferred
Cotton dental roll bolster sutured through and through, treatment with antibiotics
Allowed to continue as tolerated

Collodion Casting Modified Headgear





























