Embed Size (px)
Citation preview

176 Case reports
chronic bilateral renal papillary necrosis. Atten-tion is drawn to the dangers of prolonged anal-gesic abuse.
AcknowledgmentsWe would like to thank Dr E. Bulmer for per-
mission to record this case. We are also grateful toDr D. B. Brewer for his advice and criticism, MrS. A. Gaunt for the photography and Mrs J. Seabournefor secretarial assistance.
ReferencesANNOTATION (1959) Phenacetin nephropathy. Lancet,
i, 84.BOYD, D.H.A. (1964) The use and abuse of phenacetin.
Scot. med. J. 9, 423.DAWBORN, J.K., FAIRLEY, K.E., KINCAID-SMITH, P. &
KING, W.K. (1966) The association of peptic ulcera-tion, chronic renal disease and analgesic abuse.Quart. J. Med. 137, 69.
EDITORIAL (1964) Analgesic abuse and the kidney-a commentary. J. Amer. med. Ass. 190, 238.
JACOBS, L.A. & MORRIS, J.G. (1962) Renal papillarynecrosis and the abuse of phenacetin. Med. J. Aust.11, 531.
LEADING ARTICLE (1960) Renal risks of phenacetin.Brit. med. J. i, 714.
LEADING ARTICLE (1965) Phenacetin and the kidney.Brit. med. J. i, 673.
LINDENEG, O., FISCHER, S., PEDERSEN, J. & NISSEN,N.I. (1959) Necrosis of the renal papillae and pro-longed abuse of phenacetin. Acta med. scand. 165,321.
Monthly Index of Medical Specialities (1965) Vol. 7,No. 11.
NELP, W.B., WAGNER, H.N. & REBA, R.C. (1964) Renalexcretion of vitamin B12 and its use in measurementof glomerular filtration rate in man. J. Lab. clin.Med. 63, 480.
OLAFSSON, O., GUDMUNDSSON, W.R. & BREKKAN, A.(1966) Migraine, gastritis and renal papillarynecrosis. Acta med. scand. 179, 121.
REYNOLDS, T.B. & EDMONDSON, H.A. (1963) Chronicrenal disease and heavy use of analgesics. J. Amer.med. Ass. 184, 435.
SANERKIN, N.G. & WEAVER, C.M. (1964) Chronicphenacetin nephropathy ('chronic interstitial nephri-tis') with papillary necrosis. Brit. med J. i, 288.
SPUHLER, 0. & ZOLLINGER, H. (1953) Die chronishinterstitielle Nephritis. Z. klin. Med. 151, 1.
Mast cell diseaseT. I. McBRIDEM.B., M.R.C.P.
Registrar in Medicine
G. A. McDONALDM.D., M.C.Path.
Consultant HaematologistW. P. DUGUIDM.B., M.C.Path.
Consultant Pathologist
The Royal Infirmary, Glasgow
IntroductionIn recent years much interest has been focused
on the physiology and pathology of the mast cell.It is accepted that the mast cell features in a widevariety of disorders and mastocytosis has beenproposed as a generic name for syndromes inwhich extensive mast cell involvement is present.Selye (1965) has collected and analysed the rele-vant literature on mast cells and this has beenused as the main reference text in the preparationof this report. The patient described is of par-ticular interest in that he had a syndrome whichwas first considered to be a non-specific masto-cytosis, but in which several unusual features werediscovered.
Case reportA 63-year-old male clerk was first seen at the
Medical Out-Patient Department of GlasgowRoyal Infirmary where he was discovered to beanaemic and to have hepatosplenomegaly. He was
consequently admitted for further investigation.The presenting complaints were dyspnoea, somechest tightness and nausea of only 6 weeks' dura-tion. Detailed questioning revealed no otherfeatures of note in the past history-in particularthere was no history of drug ingestion, episodicflushing or of any haemorrhagic tendency.
Physical examination revealed a well-developedman with no evidence of recent weight loss. Themucous membranes were pale and the liver andspleen were each palpable 2 finger breadths belowthe respective costal margins. Examination of theother systems revealed no abnormality. In par-ticular no skin lesions were present.
InvestigationsHb, 6-6 g/100 ml; PCV, 22% ; WBC, 2100/mm3
-with a normal distribution in the differentialcount. Platelet count, 98,000/mm3; ESR, 35 mmin the 1st hour (Westergren). The blood filmshowed anisocytosis and poikilocytosis. The liver
copyright. on A
ugust 30, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.497.176 on 1 M
arch 1967. Dow
nloaded from

Case reports 177
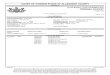
FIG. 1. Marrow film. Low power view showing numerous mast cells. May-Grulnwald-Giemsa stain, x400.
4a,,_.
FIG. 2. Marrow film showing binucleate erythroblasts and mast cells. May-Grinwald-Giemsa stain,x 1280.
copyright. on A
ugust 30, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.497.176 on 1 M
arch 1967. Dow
nloaded from

178 Case reports
......~... ~
Di ~ ~ ~ ~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ .
vou~~~ ~ ~
..........~~~~
FIG. 3. Marrow film. Toluidine Blue Stain confirming the presence of mast cells, x400.
function tests revealed no abnormality; electrolytesnormal; blood urea, 54 mg/l00 ml; blood group'O' Rh +ve; Coomb's test negative. An M.S.U.submitted for bacteriological examination revealedno abnormality. An augmented histamine testrevealed free acid in stomach. A radioactivevitamin B12 absorption test (Schilling Test) showednormal absorption of vitamin B12. The serum acidphosphatases were normal; s e r u m iron,125 ug/ 100 ml; saturation, 35%; serum vitaminB12, 170 pg/ml; serum folate, 17 pg; serumcholesterol, 145 mg/100 ml. Chest X-ray showedno abnormality, as did barium swallow and meal,bone survey and I.V.P. Gastric mucosal antigentest negative.
Sternal marrow examination revealed a cellularmarrow in which the striking finding was the largenumber of mast cells spread diffusely through themarrow smears (Fig. 1). Many bizarre erythro-blasts were also present-binucleate, trinucleateand quadrinucleate forms being noted (Fig. 2).The identity of the mast cells was confirmed withmetachromatic staining (toluidine blue) (Fig. 3).The PAS stain was negative. Iliac crest aspirationshowed a similar marrow picture.A jejunal biopsy revealed an increased number
of lymphocytes and plasma cells. The appearanceswere regarded as abnormal but not specific. In
view of the finding of the mast cells in the bonemarrow the patient was tested for dermagraphismbut this was not present. A skin biopsy showed anincrease of mast cells around the dermo-capillaries but was not considered to be diagnosticof urticaria pigmentosa.At this stage a diagnosis of possible primary
mast cell disorder was postulated. Blood trans-fusion, 3 pints of packed red cells, was given andhe was allowed home. The patient felt much betterand he was kept under close surveillance as anout-patient over the next 2 months. By the end ofthis period the haemoglobin level had again fallenand he was readmitted. The blood picture againshowed a pancytopenia and the pertinent clinicalfindings were as before. At this time detailed in-vestigations to exclude any abnormality of thehaemostatic mechanism were undertaken. Thesetests revealed no abnormality. He was again trans-fused with good effect and this was repeated on asubsequent admission. His condition deterioratedand on his final admission 8 months after theinitial one he had become increasingly tired andlethargic. There was evidence of a right basaleffusion. The liver and spleen were again easilypalpable. The blood picture revealed: Hb,5-6 g/100 ml; PCV, 20%; WBC, 1000/mm3;ESR, 120 mm in the 1st hour; platelets,
copyright. on A
ugust 30, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.497.176 on 1 M
arch 1967. Dow
nloaded from

Case reports 179
At
FIG. 4. Post-mortem marrow. Toluidine Blue Stain confirming the presence of numerous mast cells, x 1280.
29,000/mm3. Electrophoresis of the serum proteinsrevealed a decrease in albumin but no abnormalityof the globulin fractions.
In spite of further blood transfusion there wasno improvement. The pleural effusion was aspir-ated and the fluid was found to be straw coloured.In this material no malignant cells, organisms ormast cells were found. Steroid therapy was startedmainly because of the fall in the platelet count,but he slowly deteriorated and died 3 weeks later.
NecropsyThe principal findings were the presence of large
haemorrhagic pleural effusions and ascites. Thepleural surfaces of liver and diaphragm and theperitoneal surfaces of stomach and intestine werecovered with numerous small white nodules.Histology showed granulomatous lesions withcentral necrosis, epithelioid cells and multinucleategiant cells. These lesions were morphologicallyconsistent with tuberculosis. No obvious focus orprimary lesion could be found in the lungs butenlarged mediastinal lymph nodes were found andthese contained acid and alcohol fast bacilli. Inaddition there were two ulcers in the larynx andhistology showed necrosis with thrombi in thevessels which contained numerous Gram-positivecocci. Similar lesions were found at the lung base.A pyaemic abscess was present in the adrenal and
septic infarcts in the kidney. The bone marrowshowed a leuco-erythroblastic reaction and his-tology showed the presence of numerous mast cellsand abnormal erythroid precursors (Fig. 4).The pathological diagnosis was: (1) tubercu-
losis of serous cavities; (2) pyaemia; (3) pancyto-penia; and (4) mastocytosis.
DiscussionThe initial presentation of this case was of a
man who had pancytopenia and hepatospleno-megaly. Bone marrow examination showedextensive infiltration with tissue mast cells.Although the post-mortem examination revealedthe presence of tuberculosis, on review of the caseit was considered that this was most probably aterminal feature associated with the administra-tion of steroids.
In attempting to assess the relevance and partplayed by the mast cells, it is first of all acceptedthat mast cells may be present in the marrow inlarge numbers in the presence of severe anaemia.This could have been the cause in this case but aninteresting feature here was the presence ofunusual abnormal erythroblasts. Fadem (1951), inreporting seven cases in which there had beentissue mast cells in the marrow, remarked thatthree of them exhibited evidence of severe marrowdepression and he further noted that abnormal
copyright. on A
ugust 30, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.497.176 on 1 M
arch 1967. Dow
nloaded from

180 Case reports
binucleated erythroblasts were present. The possi-bility therefore exists that there may be a specifichaematological disorder characterized by marrowmastocytosis with abnormal erythroblasts whichmay lead to aplastic anaemia without havingnecessarily systemic mast cell involvement.
SummaryA case is presented in which pancytopenia was
associated with marrow mastocytosis and abnor-mal erythroid precursors. At post-mortem tuber-culosis of the serous cavities was found. Thepossible significance of these findings is discussed.
AcknowledgmentsWe wish to express our thanks and appreciation to
Dr J. H. Wright under whose care the patient wasinvestigated. The help and co-operation of ProfessorA. S. Douglas is also acknowledged, and we are verymuch indebted to Professor J. V. Dacie and ProfessorH. W. Fullerton for kindly reviewing the blood andmarrow films.
ReferencesSELYE, H. (1965) The Mast Cells. Butterworths, Wash-
ington.FADEM, R.S. (1951) Tissue mast cells in human bonemarrow. Blood, 6, 614.
Phaeochromocytoma as a cause of gastro-intestinal distension
A. BERNSTEIN*B.A., M.B. (Dubl.)
Senior House Officer
ANN C. WRIGHTM.B., Ch.B.
Medical RegistrarD. SPENCER tM.B., Ch.B.
Registrar in Pathology
Hope Hospital, Salford 6
Too often the diagnosis of phaeochromocytoma ismissed, because the possibility has not even beenconsidered. This is largely due to its diverse clinicalpresentations. While paroxysmal hypertension withvasomotor instability, or sustained hypertension,may suggest the diagnosis, less familiar featuresmay distort the picture. Those recorded includeparoxysmal hypotension (Gjol, Dybkaer & Funder,1957; Richmond, Frazer & Millar, 1961; Hamrin,1962; Leather et al., 1962), a typical hyperthyroid-ism (Davies, 1952), glycosuria, or even diabetesmellitus (Freedman et al., 1958) and urinary reten-tion (Barnet et al., 1950; Baird & Cohen, 1954).There is a well-documented association withthyroid carcinoma (Williams, 1965) and withneurofibromatosis (Glushien, Mansuy & Littman,1953). Phaeochromocytoma may cause suddendeath from pulmonary oedema (Harrison &
*At present: Medical Registrar, St Mary Abbott'sHospital, London, S.W.7.tAt present: Senior Registrar in Morbid Anatomy,
Westminster Hospital (Vincent Square Laboratories,124 Vauxhall Bridge Road, London, S.W.1).
Seward, 1954) and from cardiac arrhythmia(Durant & Soloff, 1962).We report here a patient with bilateral phaeo-
chromocytomata, presenting with gross abdominaldistension and simulating acute intestinal obstruc-tion. Although distension of the abdomen hasbeen recorded in case reports of phaeochromo-cytoma, a direct connection between the two hasnot previously been stressed.
Case reportIn August 1965, a 26-year-old housewife was
admitted to Hope Hospital with a diagnosis ofacute intestinal obstruction. She gave an 8-dayhistory of progressive abdominal distension andcolicky pains. There had been absolute constipa-tion for 6 days, and persistent vomiting for 3 days.She gave a lifelong history of constipation, butthere had been no previous episode of abdominaldistension. Other complaints were exertionaldyspnoea for 2 weeks, spontaneous bruising ofher legs for a week, and thirst with polyuria for 3days.
copyright. on A
ugust 30, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.43.497.176 on 1 M
arch 1967. Dow
nloaded from