Embed Size (px)
Citation preview

January 19, 2017
Mary Stankos, RN, MJ, CPHQ, CPPS, Patient Safety Consultant, MAPS
Alexis M. LaPietra, DO
Medical Director EM Pain Management St. Joseph’s Healthcare System

MAPS Patient Safety Organization Promoting a Culture of Safety in a Protected Environment
An Illinois Health and Hospital Association company.
Member Benefits: Supports health care providers across the continuum of care Certified by AHRQ since 2010 Provides Legal privileges, confidentialities & PSES support Promotes peer learning & networking Delivers data analysis to members & RCA feedback Meets the required ACA Healthcare Insurance Marketplace
mandate 42 CFR 3.20 Member of the Coalition to Improve Diagnosis, and Alliance for
Quality Improvement & Patient Safety

Housekeeping:
- Please place your phones on mute
- Feel free to ask questions via the webinar
chat feature located in the lower left-hand portion
of your screen
- Today’s presentation will be recorded
- The presentation slides will be made available to
all attendees
- A CE survey will be sent to all registrants by
Tammy DeLeonardis following the event.
Welcome!
A Federally-Listed Patient Safety Organization
CE Info for Today’s Webinar By the end of today’s webinar, participants will be able to
Learning Objectives:
Discuss the current prescription opioid epidemic and the role providers play
Review evidence-based alternatives to opioids for acute and chronic pain in the ED
Evaluate the role of novel modalities
As the sponsor of this webinar, the Illinois Health and Hospital Association is authorized by
the State of Illinois Department of Financial and Professional Regulation (license number
236.000109) to award up to 1.0 hours of nurse continuing education credit for this
program.
This program has been approved by the National Association for Healthcare Quality for
1.00 CPHQ continuing education hours.
This activity meets the criteria of the Certification Board for Professionals in Patient Safety
for 1.0 CPPS CE hours.
4

ALTERNATIVES TO OPIOIDS ALTOSM
Alexis M. LaPietra, DO Medical Director EM Pain Management
St. Joseph’s Healthcare System
I have no financial disclosures

Objectives
Discuss the current prescription
opioid epidemic and the role
providers play
Review evidence-based alternatives
to opioids for acute and chronic pain
in the ED
Evaluate the role of novel modalities

1.9 million
75%
51
18,893

Substance Abuse and Mental Health Administration (SAMHA) estimated
2.8 million seniors ABUSED opioids
in the past year
In 2014, 467,000 adolescents were current nonmedical users of pain reliever,
with 168,000 having an addiction to prescription pain relievers
http://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1-2014/NSDUH-FRR1-2014.pdf.
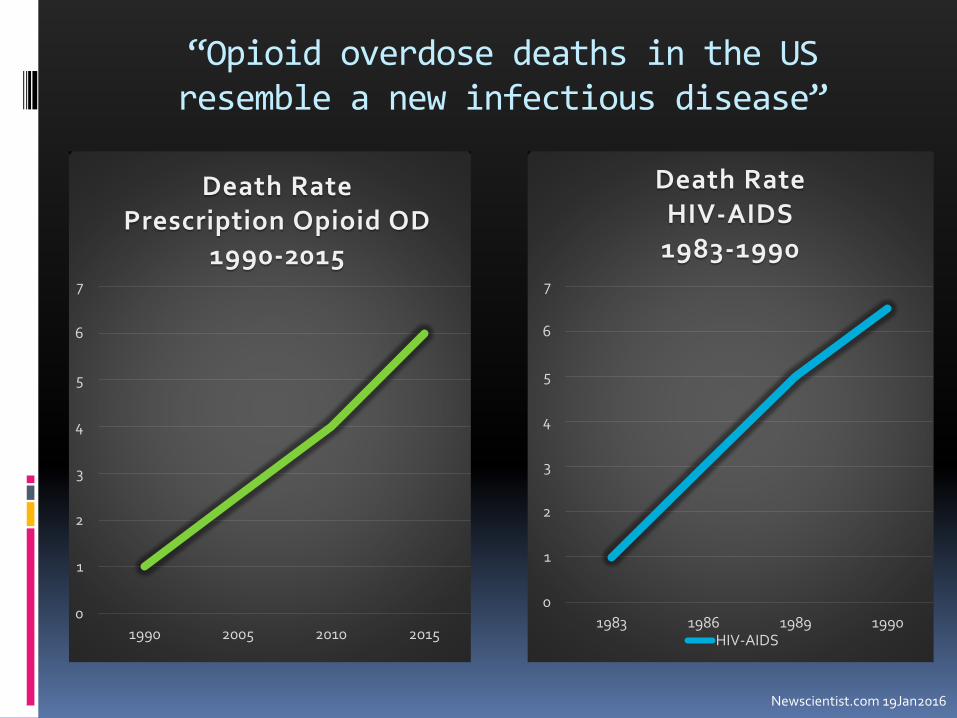
“Opioid overdose deaths in the US resemble a new infectious disease”
Newscientist.com 19Jan2016
0
1
2
3
4
5
6
7
1990 2005 2010 2015
Death Rate Prescription Opioid OD
1990-2015
0
1
2
3
4
5
6
7
1983 1986 1989 1990
Death Rate HIV-AIDS
1983-1990
HIV-AIDS

1990 1995 2000 2005 2010 2015
Opioid Prescribing Habits vs. Prescription Opioid OD Deaths
Rx opioid DEATHS Rx Opioids

Europe
11.4%
Canada
0.6%
100% of the world’s hydrocodone
81% of world’s oxycodone
USA 5.1%
Dalal 2013
80 %

What can we do in the ER?
Addiction
Acute Pain
Feel Better
Opiates Alternatives
ALTOSM Alternatives to Opioids
Acute Pain Protocols
Renal Colic
Musculoskeletal Pain
Lumbar Radiculopathy
Migraine Headache
Extremity Fracture/Dislocation

Opioids are necessary……
……but they are not the solution for all pain
THINK before you prescribe
USE alternatives whenever possible
CARE about the patient

Talk about painful
Feodor Vassilyev G27P69 c 1707-1782

Case 1
MM is a 57 year old female who presents to the ED with severe LEFT flank pain and vomiting. She has h/o kidney stones in the past. PMHx: none, PSHx: none, NKDA, No med prior to
arrival
Toradol® 30 mg IV
1 L NS
Zofran® 4 mg IV

Case 1, continued
MM reports minimal pain relief and is still in distress. Next line therapy?
Morphine?
Patient received morphine 5 mg IV.
VERY minimal pain relief
She receives another morphine 5 mg IV + Zofran®
Pain is unchanged and she is vomiting
Case 2
JA 28 year old male presents with severe kidney stone pain. He has a history of kidney stone pain in the past and is in recovery for heroin addiction, 7 months clean.
Last time he has a kidney stone, he received morphine, he states it took him weeks to overcome the craving for heroin

Alternatives?
He asks if there is an alternative to morphine, he states at another facility they said “no” and he was torn between pain relief and a potential relapse.
Is there evidence to support the use of alternatives for kidney stone pain?
Intravenous Lidocaine
Intractable oncological pain Improved pain with fewer side effects, compared
to opiates alone
Little to no toxicity
Improved quality of life
Post-operative pain relief, meta-analysis Reduced pain at rest, with movement, and with
cough
No statistical difference in adverse events
Ferrini 2004 Vigneault 2011
Lidocaine for Post- Op Pain Cochrane Review
Immediately reduced pain
lasting up to 24 hours
Less opiates
Decreased LOS
Quicker bowel function return
Less nausea
No difference in rate of death, arrhythmia, toxicity, or other heart disorder
Moderate evidence that intravenous lidocaine has an impact on pain scores compared to placebo
Kranke 2015

Lidocaine vs. Morphine RCT Renal Colic
Lidocaine had lower pain scores compared to morphine at 5, 10, 15, and 30 minutes post-administration
No difference in adverse events
Solemanipour 2012
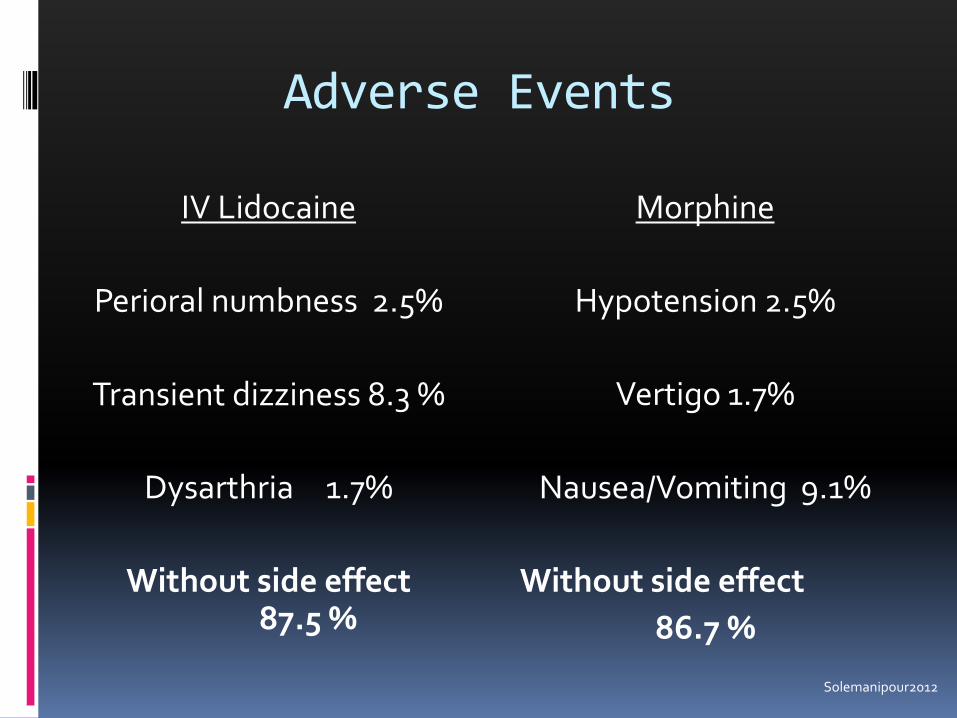
Adverse Events
IV Lidocaine
Perioral numbness 2.5%
Transient dizziness 8.3 %
Dysarthria 1.7%
Without side effect 87.5 %
Morphine
Hypotension 2.5%
Vertigo 1.7%
Nausea/Vomiting 9.1%
Without side effect
86.7 %
Solemanipour2012

Mechanism of action
Inhibits afferent sensory conduction
Analgesia
Paralyzes the ureter
Quicker stone passage?
Intravenous Lidocaine
Cardiac Monitor
1.5 mg/kg (200 mg/100 mL NS) over 10 minutes on a pump MAX 200 mg
EXCLUSIONS- Seizure or malignant arrhythmia

Take Home Point #1
Intravenous lidocaine is a safe and effective analgesic for renal colic.

Fastest Toilet 55 mph

Case 3
57 M presents with 2 days of acute low back pain after moving a sofa. Has tried ibuprofen once per day without much relief. He states oxycodone has helped him in the past.
PMHx- high cholesterol
NKDA
What’s the best treatment for him?

Acute Low Back Pain
Opioids are not first line, especially in the ED
Early opioids prescribing
Increase rate of MRI
Significantly higher medical costs
29% more likely to end up on chronic opioids
Friedman 2015 Lee 2016

Alternatives
NSAIDS
Tylenol®
Topicals
Lidoderm®, Voltaren®, Flector®
Trigger Point Injection
Muscle Relaxants
NSAIDs and Tylenol®
NSAIDs are effective No better with Oxycodone/APAP No better with Cyclobenzaprine
Analgesic ceiling ~400 mg/dose or ~1200 mg/day
NSAIDs work better with Tylenol® Tylenol® 1000 mg
Friedman 2015 Derry 2013 McQuay 2007 Seymour 1996

Topicals
Lidoderm® patches
Diclofenac gel improves pain associated with OA of the knee and musculoskeletal injuries
NNT 1.8
Galer 2004 Wadsworth 2016 Baraf 2011 Barthel 2010 Cochrane 2015
Trigger Point Injection Definition

Myofascial Trigger Points
Tension Headache
Tinnitus
Temporomandibular joint pain
Torticollis
Dommerholt 2006

Myofascial Trigger Points
According to the CDC in a 2009 report, myofascial pain of the back is the second most common cause of disability in working-age adults.
Myofascial pain effects an estimated 10% of the US population and is typically underdiagnosed in the ED as a cause of pain
MMWR Morb Mortal Wkly 2009 Wheeler 2004
Most Common Trigger Point Location
Roldan 2015

Trigger Point Injection
Indications
Palpable taunt band or nodule in skeletal muscle with referred pain
Palpation reproduces pain
Acute or chronic MSK pain
Contraindications
Cellulitis over target area
Anticoagulation
Allergy to local
anesthetic

Trigger Point Injection Equipment
0.5% bupivacaine without epi- 1-2 mL
+/- steroids
25 gauge needle
Alcohol swap
Band-Aid®
Consent
Infection, bleeding

Trigger Point Injection Technique

Take Home Point # 2
Most acute low back pain does not require opioids
NSAIDs + Tylenol® + Topicals Muscle relaxant may be necessary
Trigger Point Injections It’s a billable procedure

2,583 unique rubber ducks!
Case 4
57 M with chronic pain due to lumbar radiculopathy presents with an acute flare. He takes MS Contin® 100 mg PO BID and oxycodone 30 prn.
No focal neuro deficits but in severe distress.
Management?

Your Brain on Opioids
The neurochemistry of the brain changes when exposed to chronic opioids
More opioids does not equal better relief
Allodynia
Hyperalgesia
Chronic Pain

Opioid Tolerant Patients
NSAID + Tylenol®
Gabapentin 300 mg
Diazepam or cyclobenzaprine
Ketamine infusion + drip

Ketamine for Analgesia
Antagonizes NMDA receptor Sole agent for analgesia
Sub-dissociative dosing 0.3 mg/kg infusion
0.1 mg/kg/hour drip
Opioid sparing effect
No vital sign changes, no additional monitoring Galinski 2006 Motov 2015 Miller 2015

Ketamine
Intranasal
Safe in children
0.5 mg/kg MAX 50 mg/dose
MAX volume 1 mL/naris
No change in vital signs
Significant reduction in pain score
Easy to administer
Can re-dose
Works within 15 minutes
Andalfatto 2013 Yeaman 2013 Yeaman 2014 Shrestha 2016

Take Home Message #3
Ketamine can be used in conjunction with opioids or as a sole agent for analgesia in the emergency department for acute and chronic pain.
Intranasal administration is effective and easy.
Supported by ACEP and SAEM

Case 5 (last case)
23 M comes to ED for gluteal abscess. You are in the urgent care/fast track section. The abscess is LARGE. He has had them before and is pleading with you to “put me to sleep”!
What do you do?
Nitrous Oxide
Nitrous Oxide
Tasteless colorless gas administered in combination with oxygen via mask or nasal hood Maximum concentration 70% N2O
Absorbed via pulmonary vasculature and does not combine with hemoglobin or other body tissues
Rapid onset and elimination <60 seconds
Becker 2008
Benefits of Nitrous Oxide
Analgesic and anxiolytic agent Use along with local anesthetic or other pain
medications
Releases enkephalins, effects reversed with naloxone
Only monitoring is pulse oximetry
No NPO requirements, patient can drive after administration, no IV line needed
Babl 2015 Zhang 1999
Becker 2008 Champman 1979
Nitrous Oxide Evidence
It indicated for any and every painful condition
All ages
Laceration
Lumbar puncture
Peripheral and central venous access
I&D
FB removal
Burn/Wound Care
Fecal Disimpaction Herres 2015 Ducasse 2013 Klomp 2012 Aboumarzouk 2011 Furuya 2009 Atassi 205

The Downside to Nitrous Oxide
Abuse potential
Mobile unit
Patient or nurse must hold mask
Patients may feel claustrophobic when using the facemask

Contraindications
COPD or severe active asthma
Severe vitamin B12 deficiency
Otitis Media, Sinusitis
Bowel Obstruction
Altered level of consciousness
Psychiatric disease, EtOH, Head Injury
1st and 2nd trimester pregnancy

Take Home Point #4
Nitrous Oxide is a fast acting easily administered analgesic, ideal for the management of acute pain

Summary
Renal colic IV LIDOCAINE
Low Back Pain Tylenol®, NSAIDs, topicals
and Trigger Point Injection
Opiate Tolerance KETAMINE
Procedures NITROUS

ALTOSM results
N= 1600 patients
47.6% reduction in opioids for acute low back pain, renal colic, and headache p= 0.0001
Pain scores pre-ALTO 8 1.9
Pain score post-ALTO 7.9 2.0
Keep exposure to a minimum
The use of alternatives for pain management
decreases unnecessary exposure of potential harmful medications to our patients.
Opioids are important but should not be reflexively prescribed
Dr. Shroff says “I’ve gone 3 shifts without prescribing any Percocet®, people are happy and have had great pain relief”

ALTOSM Partnerships
Departments
Physical Therapy
Family Medicine
Psychiatry
Pain Management

ALTOSM Partnerships
St. Joseph’s Opioid Overdose Prevention and Naloxone Distribution Program
Opioid Overdose Recovery Program
49% of patients approached enrolled in recovery
Straight and Narrow Program
Coming soon…
Suboxone® induction in the ED
Acupuncture for pain management in the ED

EDUCATE
Multidisciplinary approach
Prevention is KEY! Keep opioid naïve patients opioid free Utilize alternatives when possible
Collaborate with outpatient physicians
Reserve opioids as rescue medication NOT first line
Support patients who suffer from the DISEASE of addiction
If you’d like to know more
Join the ACEP Pain Management Section
THANKS

THANK YOU!
We look forward to seeing you at
future MAPS PSO events.
For questions, contact
630-276-5657
65




















![CPPS Chapter 2[CompatibilityMode]](https://img.dokumen.tips/doc/110x75/577cc03c1a28aba7118f578b/cpps-chapter-2compatibilitymode.jpg)








