Embed Size (px)
Citation preview

Patricia Leung 5.26.2013
Department of Surgery SUNY Downstate Medical Center
Management of Tracheo-Innominate Fistulas

Case presentation
• SM - 52 year old male • PMH: HTN, DM, Afib, no PSH • 11/2012 – transferred to KCHC from Woodhull
for evaluation of right temporal mass • 11/20/12 – biopsy c/w high grade glioma • 12/5/12 – right temporal craniotomy with
debulking, pathology c/w glioblastoma multiforme

Case presentation • 12/24/12 – acute decline in mental status requiring
intubation, imaging c/w tumor recurrence, mass effect with midline shift
• Per discussion with family – no radiation or chemotherapy; steroid therapy initiated
• Persistent poor neurological status, malnutrition, pneumonia with respiratory failure requiring vent dependence
• 1/4/13 – Percutaneous tracheostomy and PEG placement
• 3/31/13 - transferred back to SICU for presumed sepsis, started on IV antibiotics for total of 7 day course

Case presentation
• 4/11/13 7:10 PM – Code called after patient found pulseless with massive bleeding from oropharynx and tracheostomy
• Cuff was hyperinflated • ACLS protocol initiated • Anesthesia unable to orally intubate patient
secondary to poor visualization; % O2 saturation remained in 70s
• Despite several rounds of ACLS, the patient expired

History
• 1897 - Korte reported a fatal TIF in 5-year old child with diphtheria after tracheostomy
• 1924 - Schlaepter reviewed 115 cases of fatal hemorrhage after tracheostomy and documented that the innominate artery was involved in most cases
• 1964 - Silen reported the first short-term survivor • 1968 - Reich reported the first long-term survivor of TIF

Introduction
• Pressure necrosis of anterior tracheal wall from cuff or tip causing erosion of trachea and innominate artery
• Rare complication of tracheostomy • Incidence 0.7% • Survival rate 14.3% • Mortality rate 100% without operative
intervention • ~75% of TIF develop within first 3 weeks after
tracheostomy

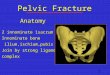
Anatomy
• Trachea is 11.8 cm long with 18-22 cartilaginous rings
• Innominate artery traverses trachea at level 9th tracheal ring
• Ranges between 6-13th tracheal rings
• Anatomical variants
A & A April 1999 vol. 88 no. 4 777

Contributing factors • Low tracheostomy tube placement • Overinflation of tracheostomy cuff >20 mmHg • Malpositioned tracheostomy tube tip • Anatomical variations • Local infection of tracheostomy wound • Excessive manipulation of tracheostomy tube • Long-term ventilation • Radiation therapy • Steroids • Malnutrition • Diabetes
Pearson’s Thoracic and Esophageal Surgery Fig 20-7

Diagnosis
• Early diagnosis is key • Warning signs: - Sentinel bleed - Pulsating tracheostomy tube • Bronchoscopy • CT Angiogram • Angiogram • Low sensitivities, delay
in treatment
J Korean Neurosurg Soc. 2011 February; 49(2): 107–111
Journal of Vascular Surgery volume 33 Pages 1280-1282, June 2001

Principles of Management
• Secure airway • Control bleeding • Resuscitation
OR

Initial management
• Cuff overinflation • Oral endotracheal tube
placement distal to site • Digital compression of
artery via pretracheal space OR in trachea against sternum
• Compression via rigid bronchoscope
• Take to OR
e Department of Surgical Education, Orlando Regional Medical Center

Surgical management
• Median sternotomy • Extension into right third or fourth intercostal space • Innominate artery exposure by division of thymus
and superior retraction of innominate vein • Proximal and distal control • Preservation of anomalous left common carotid
artery
Figure 4 Ann Surg. 1976 August; 184(2): 194–204

Surgical management
• Interruption of flow - Simple ligation and resection • Maintenance of flow - Direct repair of defect - Interposition grafting

• Resection of involved innominate artery segment
Greenfield Chapter 80 Figure 80.33C
Figure 13-1, Chapter 13 Tracheal fistula to brachiocephalic artery

• Segment of damaged trachea excised with primary end-to-end anastomosis
• Strap muscle interposition
• Primary repair with buttress
• Relocation of tracheostomy Access Surgery Figure 37-1 A

• Aorto-to-axillary artery bypass graft
Ann Thorac Surg 2004;77:1424-1426

• Interposition graft between ascending aorta and division of innominate artery
Interact CardioVasc Thorac Surg(2008) 7 (4): 654-655.

Studies 1994 Gelman et al • 71 survivors of TIF from 1962 to 1994 • 40 survived long-term (>2 months) • Maintenance of flow 15.8% LT survival • Interruption of flow 71.2% LT survival • Recurrent bleeding and death: Maintenance of flow 60% and 86% vs. Interruption of flow 7% and 29% • Minimal neurologic sequelae 1988 Yang et al • 24 survivors from 1875 to 1984 • Similar results

Prevention • Reserve tracheostomy for patients requiring prolonged
ventilation • � Avoid: - Tight wound closure - Excessive neck hyperextension -� Tube manipulation (use long flexible tube
connection) • � Monitor cuff pressures to < 20 mmHg frequently • � Expose anterior trachea by isthmus division to count
rings from cricoid • Selection of site at 2nd or 3rd tracheal rings • �Bronchoscopy if questionable positioning

Summary
• Tracheoinnominate artery fistula is a rare but devastating complication of tracheostomy
• Outcomes highly dependent on rapid diagnosis and immediate management
• Resuscitation, airway protection, control of bleeding
• Simple ligation and resection recommended

References • The anatomical basis for post-tracheostomy innominate artery rupture. Laringoscope 98:1061, 1988 J Korean Neurosurg Soc. 2012 December; 52(6):
547–550. • Successful Treatment of Tracheoinnominate Artery Fistula Following Tracheostomy in a Patient with Cerebrovascular Disease • Tracheo-Innominate Artery Fistula After Tracheostomy Leonardo Kapural, MD*, Juraj Sprung, MD, PhD†, Ivo Gluncic, MD‡, Miranda Kapural,
MD*, Simon Andelinovic, MD§, Dragan Primorac, MD§, and Peter K. Schoenwald, MD† *Division of Anesthesiology and Critical Care Medicine and †Department of General Anesthesiology, The ClevelandClinic Foundation, Cleveland Anesth Analg 1999;88:777–80
• Tracheo-innominate artery fistula after percutaneous tracheostomy: three case reports and a clinical reviewC. A. Grant1,*, G. Dempsey1, J. Harrison1 and T. Jones2 Br. J. Anaesth. (January 2006) 96(1): 127-131.
• Journal of Vascular Surgery Volume 33, Issue 6 , Pages 1280-1282, June 2001 • Successful management of tracheo-innominate artery fistula with endovascular stent graft repair Jun-o Deguchi, MD Takatoshi Furuya,
MD, Nobutaka Tanaka, MD Masakazu Nobori, MD Yasuo Seki, MD Yukihiro Nomura, MDIsao Umehara, MD Haruhisa Saito, MD, Tetsuro Miyata, MD J Korean Neurosurg Soc. 2011 February; 49(2): 107–111. • Is Computerized Tomography Angiographic Surveillance Valuable for Prevention of Tracheoinnominate Artery Fistula, a Life-Threatening
Complication after Tracheostomy? Jae Hoon Sung, M.D., Il Sup Kim, M.D., Seung Ho Yang, M.D., Jae Taek Hong, M.D., Byung Chul Son, M.D., andSang Won Lee, M.D.
• Preventive ligation of the innominate artery in patients with neuromuscular disorders Francesca Iodicea,*, Gianluca Brancacciob, Aldo Lauria and Roberto Di Donatob Eur J Cardiothorac Surg (2007) 31(4): 747-749.
• Access Surgery Chapter 37 Tracheal Injuries • Gelman J.J., Aro M., Weiss S.M. Tracheo-innominate artery fistula. J Am Coll Surg 1994;179:626-634 • Pearson’s Thoracic and Esophgeal Surgery 3rd Edition Chapter 20 • A novel approach to the management of tracheoinnominate artery fistula Mario G. Gasparri, MDa*, Alfred C. Nicolosi, MDa, G. Hossein Almassi,
Mda Ann Thorac Surg 2004;77:1424-1426 • Graft repair of tracheo-innominate artery fistula following percutaneous tracheostomy Hassan Jamal-Eddinea, Adel K. Ayeda,b, Ahmed Al-
Moosaa and Nael Al-Sarrafa,Interact CardioVasc Thorac Surg(2008) 7 (4): 654-655.

Farewell!




![Tracheo-Innominate Fistula diagnosis and treatment: A …Tracheo-Innominate Fistula [TIF] is a rare lethal complication following tracheostomy occurring approximately 1% of cases](https://img.dokumen.tips/doc/110x75/60ad42be92879e62c24d0267/tracheo-innominate-fistula-diagnosis-and-treatment-a-tracheo-innominate-fistula.jpg)


















![BancaMovil2.0vf[1]- Rodolfo Gasparri](https://img.dokumen.tips/doc/110x75/577d24181a28ab4e1e9b9ea1/bancamovil20vf1-rodolfo-gasparri.jpg)




