Embed Size (px)
Citation preview

Management of the axilla post Z0011
Hiram S. Cody III MD
Attending Surgeon
The Breast Service, Department of Surgery
Memorial Sloan-Kettering Cancer Center
Professor of Clinical Surgery
Weill Cornell Medical College
Global Breast Cancer Conference 2015
4th International Breast Cancer Symposium
Plenary Lecture 2

Local control and survival are related

EBCTCG. Lancet 2005; 366: 2087-2106
2005 overview
>10% reduction in 5-year LR*
25276 women, 51% node positive Local recurrence Breast cancer mortality
* among 24 types of treatment comparisons

EBCTCG. Lancet 2005; 366: 2087-2106
2005 overview
<10% reduction in 5-year LR*
16804 women, 43% node postive Local recurrence Breast cancer mortality
* among 24 types of treatment comparisons
SLN biopsy works

Kim T et.al. Cancer 2006;106:4-16
SLN 2014
69 observational studies in 8059 patients
# pts
SLN found
SLN false-neg
(SLN-/AX+)
Accuracy
(SLN correct/total)
8059
96%
7%
97%

SLN 2014
5 randomized trials Trial # pts SLN found SLN false-
negative
Accuracy
EIO 532 99% 9% 97%
B-32 5611 97% 10% 97%
ALMANAC 836 96% 7% 98%
GIVOM 749 95% 17% 95%
SNAC 1088 94% 5% 98%
61-73% had SLN-only disease

Van der Ploeg IMC et.al. EJSO 2008:34:1277-84
SLN 2014
False-negative = axillary LR # pts # axillary LR
(%)
median f/u
SLN-/no ALND
48 series*
14,959 0.3% 3 yr
SLN-/no ALND
IEO (RCT)
167 1.2% 8 yr
SLN-/no ALND
B-32 (RCT)
2011 0.7% 8 yr
*all with >3 yrs followup

SLN 2014
Time course of axillary LR
• 48 studies
• 14,959 SLN-negative pts
• axillary LR in 67 (0.3%)
• 34 mo median f/u
van der Ploeg IMC, et.al. EJSO 2008;34:1277-84

* 300 deaths triggered the definitive analysis
* 309 reported as of 12/31/2009
Years After Entry
% S
urv
ivin
g
0 2 4 6 8
0
20
40
60
80
100
Trt N Deaths
SNR+AD 1975 140
SNR 2011 169 HR=1.20 p=0.117
Data as of December 31, 2009
84.6% received systemic therapy
NSABP B-32
OS: SLN negative (8 yr results)
Krag, DN et.al. Lancet Oncology 2010;11:927-33

Years After Entry
% D
isea
se-F
ree
0 2 4 6 8
0
20
40
60
80
100
Trt N Deaths
SNR+AD 1975 315
SNR 2011 336 HR=1.05 p=0.542
Data as of December 31, 2009
84.6% received systemic therapy
NASBP B-32
DFS: SLN negative (8 yr results)
Krag, DN et.al. Lancet Oncology 2010;11:927-33z

Do we still need IHC
to examine SLN?

Z0010 trial
Survival by staining method
Method
H&E
negative
(3945/5184)
H&E
positive
(1239/5184)
IHC
negative
(3595)
IHC
positive
(350)
5 year
survival (95% CI)
95.6%
(95.0-96.3)
92.8%
(91.3-94.3)
p=0.0002
95.8%
(95.0-96.5)
95.1%
(92.7-97.5)
p=0.53
Cote R et.al. ASCO 2010

NSABP B-32
IHC study
• 5611 accrued
• 3989 (71%) pN0 by H&E
– 2 mm slices
– routine IHC prohibited
• 3887 (97%) path
• 3884 (99.9%) follow up
• 95 mo median f/u
• IHC sections at UVM
– 0.5 and 1.0 mm deeper
• 15.9% IHC+
– 11.1% ITC (N0i+)
– 4.4% micromets (N1mi)
– 0.4% macromets (N1)
Weaver DL et.al. NEJM 2011; epub 1/19/11

NSABP B-32
Survival by IHC status
5 year
survival
IHC negative
n=3268
IHC positive
n=616
p
OS
95.8%
94.6% (-1.2%)
0.03
DFS
89.2%
86.4% (-2.8%)
0.02
DDFS
92.5
89.7% (-2.8%)
0.04
Weaver DL et.al. NEJM 2011; epub 1/19/11
90% of patients received systemic therapy
(40% chemo, 68% hormonal)

Should ALND be routine for SLN+?

SLN 2014
Use of ALND (NCDB 1998-2005)
Bilimoria KY et.al. JCO 2009;27:2946-53
23% no ALND 36% no ALND

SLN 2014
Trends in ALND (NCDB 1998-2005)
Bilimoria KY et.al. JCO 2009;27:2946-53
SLN+ and
no ALND
%

SLN 2014
Outcome +/- ALND (NCDB) Axillary local
recurrence
5 yr relative
survival
SLN micrometastases (<2 mm)
SLN only
(n=802)
0.4% 99%
SLN/ALND
(n=2357)
0.2% 98%
SLN macrometastases (>2 mm)
SLN only
(n=5596)
1.0% 90%
SLN/ALND
(n=22591)
1.1% 89%
Bilimoria KY et.al. JCO 2009;27:2946-53

SLN 2014
SLN micromet/no ALND
(26 publications)
2001-2010
# pts
BCT
follow-up
axillary
LR
TOTAL
3395
44-100%
42 mo
0.3% (10)
Francissen CMTP et.al. Ann Surg Oncol 2012;19:4140-49

IBCSG 23-01

IBCSG trial 23-01
SLN micromet/no ALND
• cN0, T1-2, SLN micromets (<2 mm)
• randomize to ALND (n=464) vs no ALND (n=467)
– 95% had 1 SLN+
– 91% had BCT (98% with RT)
– additional positive nodes in 13% of ALND
•
• median f/u 5 yrs
Galimberti V et.al. Lancet Oncol 2013;14:297-305

IBCSG trial 23-01
SLN micromet/no ALND Event ALND
n=464
No ALND
n=467
Local 2% 2%
Regional 0.2% 1%
Distant 7% 5%
Death 4% 4%
Galimberti V et.al. Lancet Oncol 2013;14:297-305

SLN 2014
SLN macromet/no ALND
(16 publications)
2003-2010
16 studies
# pts
BCT
follow-up
axillary
LR
TOTAL
3268
29-100%
43 mo
0.7% (24)
Francissen CMTP et.al. Ann Surg Oncol 2012;19:4140-49

ACOSOG Z0011

www.acosog.org
Z0010-Z0011 trials (ACOSOG)
suspended 12/04 at n=889 due to
slow accrual and too few events
SLNB
Z0011
SLN+
ALND Observation
Z0010
SLN-
Observation

SLN 2014
Z0011 eligibility
Eligible
• clinical T1-2N0 breast cancer
• H&E-detected SLN metastases
• lumpectomy + whole breast RT
• adjuvant systemic therapy by
choice
Ineligible
• Nodal RT
• IHC-detected SLN metastases
• Matted nodes
• 3 or more involved SN
Giuliano AE et.al. Ann Surg 2010;252:439

SLN 2014
Z0011 systemic therapy
Systemic therapy SLN+/ALND SLN+/no ALND
chemo 58% 58%
hormonal 46% 47%
chemo and/or
hormonal
96% 97%
Giuliano AE et.al. Ann Surg 2010;252:439

SLN 2014
Z0011 locoregional recurrence
Recurrence
@ 6.3 yrs
median follow-up
SLN+
ALND
(n=388)
SLN+
no ALND
(n=425)
local
3.6%
1.9%
regional node
0.5%
0.9%
local+regional
4.1%
2.8% p=0.47
Giuliano AE et.al. Ann Surg 2010;252:439 Additional positive nodes in 27% of ALND’s

SLN 2014
Z0011 overall survival
Giuliano AE et.al. JAMA 2011;305:569-75
SLN 2014
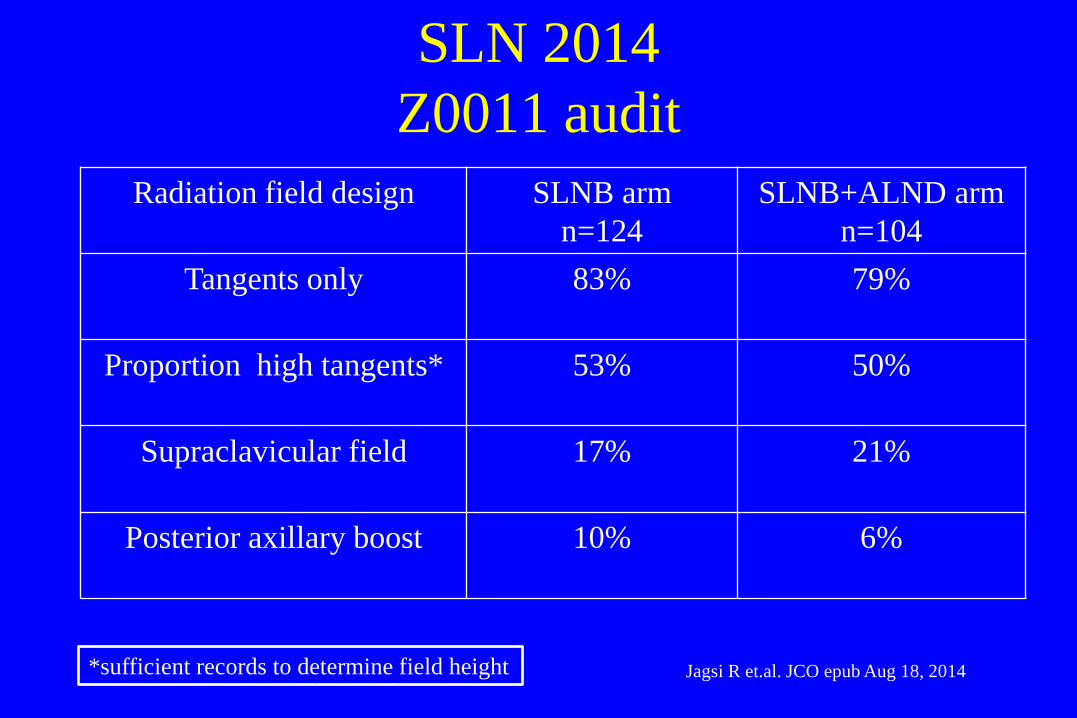
Z0011 audit
Radiation field design SLNB arm
n=124
SLNB+ALND arm
n=104
Tangents only 83% 79%
Proportion high tangents* 53% 50%
Supraclavicular field 17% 21%
Posterior axillary boost 10% 6%
*sufficient records to determine field height Jagsi R et.al. JCO epub Aug 18, 2014

SLN 2014
Z0011 use of axillary RT
# nodes positive (#pts)
SLNB arm
SLNB+ALND arm
1 (n=140)
11% 7%
2 (n=44)
24% 16%
3 (n=9)
100% 33%
>4 (n=16)
100% 79%
Jagsi R et.al. JCO epub Aug 18, 2014

SLN 2014
Current MSKCC algorithm
• preop axillary US only for high risk patients
– cT3-4
– cN1-2
• no IHC staining for SLN
• For patients who meet Z0011 entry criteria
– no intraoperative frozen section
– no ALND for <2 SLN+

SLN 2014
MSKCC
post-Z0011
algorithm
Dengel LT et.al. Ann Surg Oncol 2014;21:22-27
ALND avoided for 84%
of Z0011-eligible patients

SLN 2014
Z0011 for non-Z0011 patients?
• can the policy of “SLN+/no ALND” be extended
to patients outside the Z0011 criteria?
– Mastectomy without RT?
– Partial breast RT?
– Neoadjuvant chemotherapy?

Z0011 for mastectomy?

SLN 2014
SLN+/no ALND (NCDB 1998-2000)
Axillary LR
at 5 yrs
SLN macromet
no ALND
(5596)
SLN micromet
no ALND
(802)
All SLN+
no ALND
(6398)
LR %
1%
0.4%
0.9%
LR #
56
3
59
Bilimoria KY et.al. JCO 2009;27:2946-53

MSKCC
SLN+/no axillary rx
• MSKCC 1997-2009
– 210 mastectomy
– 325 BCT
• SLN+
• no axillary-specific rx
• median f/u 58 months
Milgrom S et.al. Ann Surg Oncol 2012;19:3762
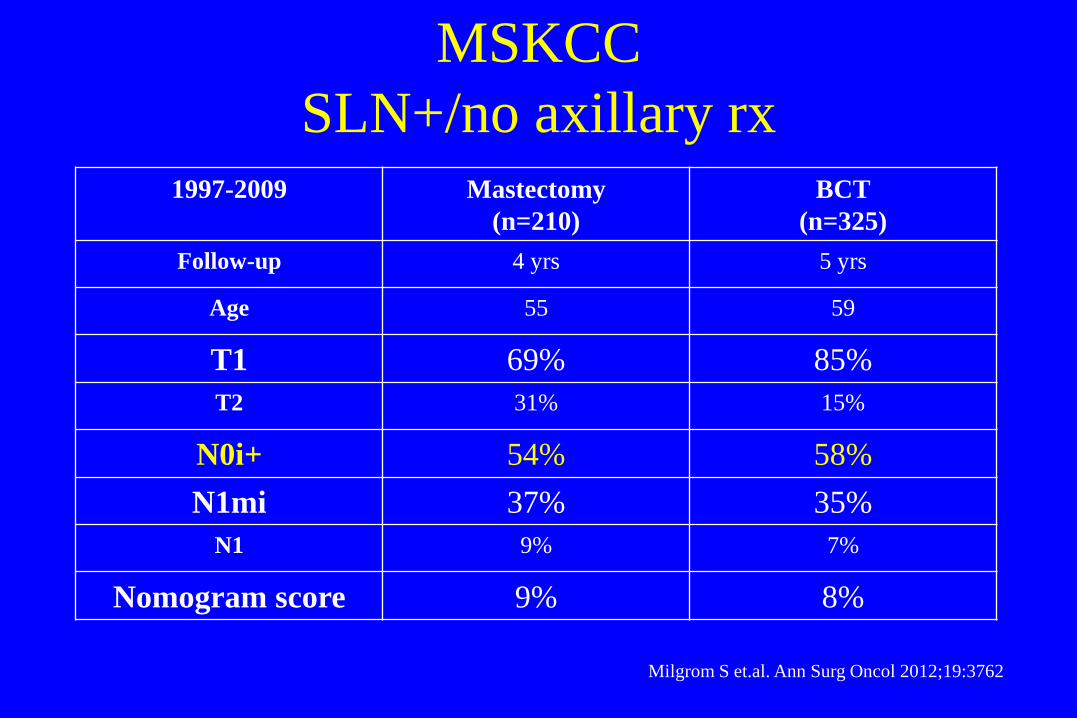
MSKCC
SLN+/no axillary rx 1997-2009 Mastectomy
(n=210)
BCT
(n=325)
Follow-up 4 yrs 5 yrs
Age 55 59
T1 69% 85%
T2 31% 15%
N0i+ 54% 58%
N1mi 37% 35%
N1 9% 7%
Nomogram score 9% 8%
Milgrom S et.al. Ann Surg Oncol 2012;19:3762

MSKCC
SLN+/no axillary rx
Milgrom S et.al. Ann Surg Oncol 2012;19:3762
All patients
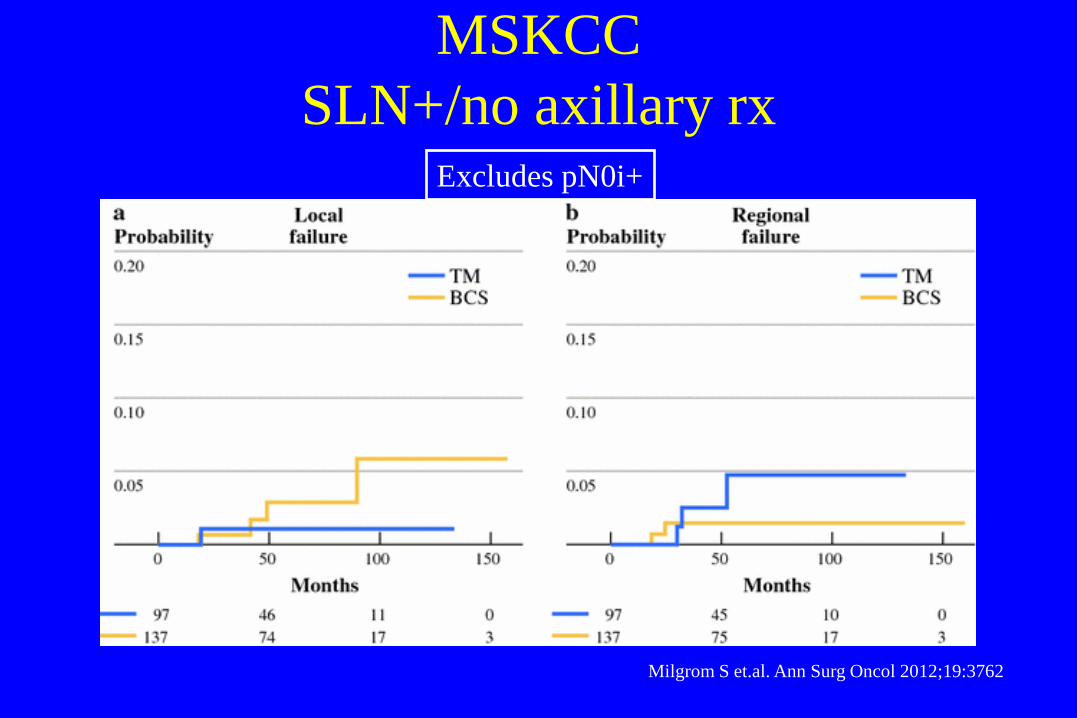
MSKCC
SLN+/no axillary rx
Milgrom S et.al. Ann Surg Oncol 2012;19:3762
Excludes pN0i+

Z0011 for partial breast RT?
PBI
The issues
• SLN negative/no ALND: axillary LR <<1%
• SLN positive/no ALND: axillary LR <1%
• Were the good results in Z0011 due to WBRT?
• If so, is PBI really safe?

PBI
some caveats
• PBI is usually limited to node-negative cancers
• axillae staged by SLNB and/or ALND
• “first event “ reporting underestimates event rates

SLN 2014
PBI trials
follow up
node neg.
Ax LR #
Ax LR %
Mammosite
registry
n=1449
59 mo
97%
10
0.79%
TARGIT
RCT
n=1113
60 mo
83%
4
0.35%
Ann Surg Oncol 2011; 18: 3415
Lancet 2013; 383: 603-613

Z0011 for neoadjuvant?

SLN biopsy
after neoadjuvant chemo
Systematic review of
27 studies
2148 patients*
2000-2009
SLN found SLN false negative
(SLN-/axilla+)
90.5%
(88-92)
10.5%
(8-14)
*23 single center, 4 multicenter:
1) Neoadjuvant chemo
2) SLN biopsy
3) Backup ALND
van Deurzen CHN et.al. Eur J Cancer 2009;45:3124-30

SLN biopsy
after neoadjuvant chemo Success rate False-negative rate
2000
2009
van Deurzen CHN et.al. Eur J Cancer 2009;45:3124-30

SLN biopsy
NSABP B-27 vs B-32
# pts
SLN found
SLN false-neg
B-27*
SLN biopsy
after chemo
428
89%
10.7%
B-32**
SLN biopsy
upfront
720
97%
9.7%
*JCO 2005;23:2694-2702 ** Lancet Oncol 2007;8:881-8

ACOSOG Z1071

SLN 2014
ACOSOG Z1071
• 708 pts (2009-2011) with cT0-4, N1-2, M0 disease
• all had neoadjuvant chemo, then SLNB/ALND
• SLN identified 92.5%
• pathologic CR 40%
Boughey JC et.al. JAMA 2013; online 10/7/13

SLN 2014
ACOSOG 1071
• False negative rate by # of SLN removed
– 1 SLN 31.5%
– 2 SLN 21%
– >2 SLN 12.6%
– >3 SLN 9.1%
• False negative rate by mapping technique
– Dye or isotope alone 20.3%
– Dye plus isotope 10.8%
Boughey JC et.al. JAMA 2013; online 10/7/13

SENTINA trial

SENTINA trial
prospective cohort study (n=1737)
• cN0: SLNB before chemo
– Arm A: SLN-, no further axillary surgery
– Arm B: SLN+, chemo, then re-SLNB/ALND
• if cN1-2: SLNB after chemo
– Arm C: if converted to cN0, SLNB/ALND
– Arm D: if still cN1-2, ALND
Bauerfeind KT et.al. SABCS 2012: Abstract S2-2

SENTINA trial
Outcome
1737 pts
103 institutions
Arms A+B
cN0
SLNB upfront
n=1022
Arm B
cN0/SLN+
SLNB upfront
chemo
re-SLNB/ALND
n=360
Arm C
cN1-2
Chemo upfront
SLNB/ALND
n=592
Success
(SLN found)
99%
61%
80%
False negative
(SLN-/axilla+)
-
52%
14%
Bauerfeind KT et.al. SABCS 2012: Abstract S2-2
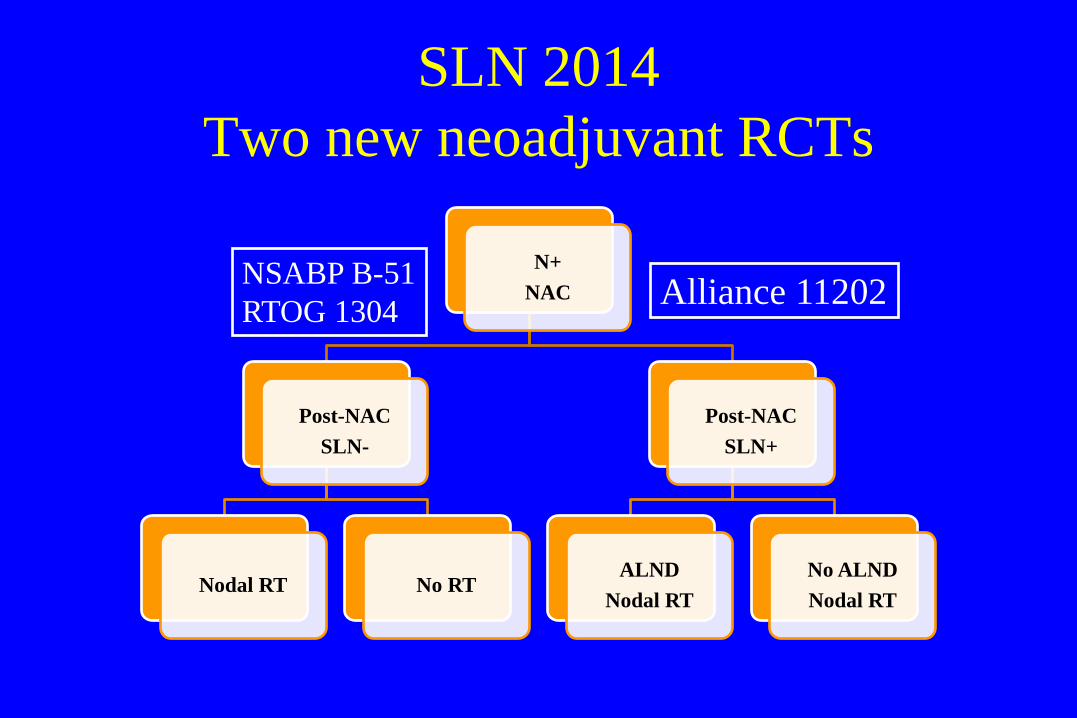
SLN 2014
Two new neoadjuvant RCTs
N+
NAC
Post-NAC
SLN-
Nodal RT No RT
Post-NAC
SLN+
ALND
Nodal RT
No ALND
Nodal RT
NSABP B-51
RTOG 1304 Alliance 11202

Z0011 for non-Z0011?
Conclusions
• SLN+/no ALND is feasible for selected low-risk patients
outside the Z0011 selection criteria
• present evidence for mastectomy and PBI is insufficient
– low event rates but little data
– RCTs of “Z0011 for mastectomy, PBI” will be difficult
– prospective well-characterized cohort studies may be
informative

Z0011 for non-Z0011?
Conclusions
• present evidence for SLNB post-NAC is sufficient
– Success rate somewhat lower than SLNB in general
– False negative rate comparable to SLNB in general
– Technique matters
• Remove >2 SLN
• Map with dye + isotope

AMAROS trial

Name of presenter
Function of presenter
Radiotherapy or surgery of the axilla after
a positive sentinel node in breast cancer
patients: final analysis of the EORTC
AMAROS trial
By the EORTC Breast Cancer Group and
Radiation Oncology Group
In collaboration with the Dutch BOOG Group
and ALMANAC Trialists’ Group
Emiel J.T. Rutgers
The Netherlands Cancer Institute, Amsterdam
Clinical trial information: NCT00014612

Trial design
cT1-2
N0
R
SNB
Stratification: institution
Adjuvant systemic therapy by choice
ALND
AxRT
AxSN+
AxSN-

5-years axillary recurrence rate:
ALND 0.43% (4 / 744 events (0.54%))
AxRT 1.19% (7 / 681 events (1.03%))
<< hypothesis (2%)
Consequence: planned comparison is underpowered
Axillary recurrence rate

Axillary recurrence rate SN-
5-years axillary recurrence rate:
0.72% (25/3131 events (0.80%))

Lymphedema: clinical observation
P < 0.0001 P = 0.0027
27.8%
22.5% 23.2%
15.1% 13.8%
10.8%
%
P < 0.0001
Years after randomization
0
5
10
15
20
25
30
1 3 5
ALND
AxRT

Shoulder function
Results:
No significant differences in all 4 excursions
Trend towards impaired movement after AxRT in first year only
Years after randomization
Multivariate ANOVA: p =
0.29
Relative movement:
Excursion treated arm
Excursion untreated arm

Results:
Trend towards more difficulties to move
the arm after ART
Trend towards more swelling after
ALND
Quality of Life
AxRT ALND
AxRT ALND

Local control and biologic subtype

Local recurrence post BCT
Non-TN vs TN
RR, 0.49
95% CI, 0.33-0.73
p = .0005
Lowery AJ, Br Ca Res Treat 2012;133:831
n = 7174

Local recurrence post mastectomy
Non-TN vs TN
Lowery AJ, Br Ca Res Treat 2012;133:831
n = 5418
RR, 0.66
95% CI, 0.53-0.83
p = .0003

Locoregional recurrence by subtype
T1mic, T1a, T1b
Cancello G, Br Can Res Treat 2011;127:713

Gene signatures and LR
21 Gene Recurrence Score 70 Gene Signature
MP High Risk n = 492
MP Low Risk n = 561
p < 0.0001
Unpublished, courtesy of E Rutgers Mamounas EP, J Clin Oncol 2010; 28:1677

Local control and systemic therapy

Systemic rx and LRR
declining proportion LRR over time
• 53 RCT’s
• 86,598 patients
• 1990-2011
• No interaction with
– Mastectomy vs BCT
– Adjuvant RT
– Menopausal status
Bouganim N et.al. Breast Cancer Res Treat 2013;139:603-606

Systemic rx and LRR
declining proportion LRR by rx
Bouganim N et.al. Breast Cancer Res Treat 2013;139:603-606

Systemic therapy reduces LR
EBCTCG Overview
EBCTCG, Lancet 2005;366:2087
Systemic Therapy RR of LR
Tam x5 yrs vs placebo 0.47
Chemotherapy vs none
(CMF or anthracyclines)
age < 50 0.63
age 50-69 0.70
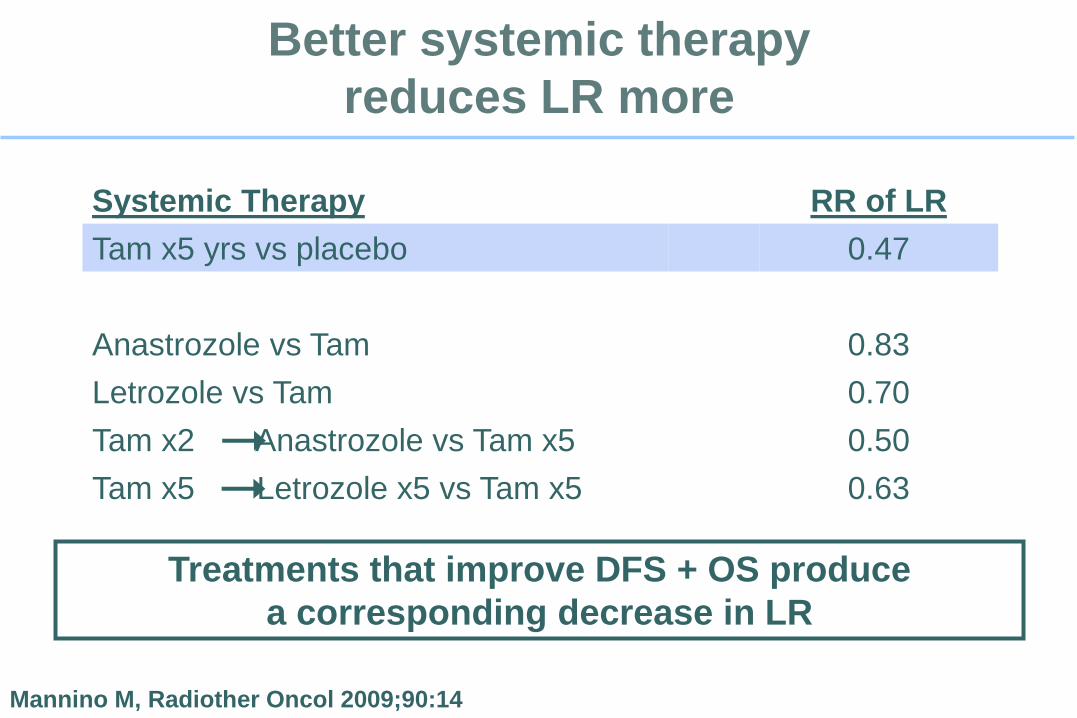
Better systemic therapy
reduces LR more
Mannino M, Radiother Oncol 2009;90:14
Systemic Therapy RR of LR
Tam x5 yrs vs placebo 0.47
Anastrozole vs Tam 0.83
Letrozole vs Tam 0.70
Tam x2 Anastrozole vs Tam x5 0.50
Tam x5 Letrozole x5 vs Tam x5 0.63
Treatments that improve DFS + OS produce
a corresponding decrease in LR

Effect of systemic therapy on LR
independent of surgery type
Kiess AP, Cancer 2012;118:1982 Lanning R, ASCO Breast 2013
Memorial Sloan-Kettering Cancer Center
No trastuzumab
n = 70
3yr LRR: 7%
Dx 2002-4
Dx 2002-4
p = 0.01
Trastuzumab
n = 102
3yr LRR: 1%
T1-T2 N0, HER2+
BCS + RT
Dx 2002-2008
Dx 2005-8
p = 0.04
Dx prior 2005 Dx 2005-2007
T1-T3, N0, N+
MRM ± RT
Dx 1999-2007
No trastuzumab
n = 256
5yr LRR: 6.6%
Trastuzumab
n = 139
5yr LRR: 1.5%

Systemic therapy and LR
NSABP Trials
Anderson SJ, J Clin Oncol 2009;27:2466
Study ER Status n 10 yr IBTR (%)
B 13 - 116 3.5
B 14 + 530 3.6
B 19 - 389 6.5
B 20 + 1027 4.7
B 23 - 1084 4.3

Axillary management in breast cancer
Conclusions I
• SLN biopsy is well established BUT
– next-generation trials in cN0 breast cancer will
compare SLNB vs no axillary staging
– next-generation trials in cN+ breast cancer will
compare combinations of ALND and RT

Axillary management in breast cancer
Conclusions II
• The role of ALND for the prevention of axillary LR is in
decline
• ALND remains an option
– for treatment of gross axillary disease
– for salvage of axillary recurrence (an infrequent event)
Axillary management in breast cancer
Conclusions III
• For SLN+ patients, axillary RT appears equivalent to
ALND in locoregional control, with fewer side effects
and better QOL
Axillary management in breast cancer
Conclusions IV
• Locoregional control is a function of
– Disease burden
– Tumor biology
– Treatment (surgery, RT, and systemic)
• Our hope is that continued improvements in systemic
therapy will allow increasing conservatism in the use of
surgery and RT