Embed Size (px)
Citation preview

Management of Skin Cancer in OrganTransplant RecipientsbyDr Catherine A Harwood1
and Dr Charlotte M Proby2
1Clinical Reader and ConsultantDermatologistCentre for Cutaneous ResearchBlizard Institute of Cell andMolecular ScienceBarts and the London School ofMedicine and DentistryQueen Mary University of London4 Newark Street, London E1 2AT
Email: [email protected]
2Clinical Reader and ConsultantDermatologistCancer Research UK Skin TumourLaboratoryWellcome Trust Centre forMolecular MedicineClinical Research Centre, Level 7University of DundeeMail Box 11Ninewells Hospital & MedicalSchoolDundee DD1 9SY
Email: [email protected]
SKIN CANCERS are overwhelminglythe most common post-transplantmalignancies and represent an
important and escalating challenge interms of their frequency, diversity,atypical, and often aggressive nature1,2.Although mortality may be relatively low,their associated morbidity is oftenconsiderable, representing a significantburden of disease for a subgroup of high-risk patients3. A robust evidence base toguide management is lacking in manykey areas, and decision-making is oftenbased upon expert consensus opinion.This review aims to summarise currentclinical practice relating to diagnosis,treatment, prevention and surveillancestrategies for post-transplant skin cancer.It will particularly focus on keratinocyteskin cancers (squamous and basal cellcarcinoma), which account for more than95% of skin cancers seen in European andNorth American transplant populations4.
DIAGNOSISFor most skin cancers, diagnosis is madeclinically prior to primary excision. In someinstances, particularly for larger lesions requir-ing more extensive surgery, in cases of diag-
nostic uncertainty, or for tumours in whichnon-surgical treatment is being considered, aninitial incisional biopsy may be required toconfirm the diagnosis before definitive therapy.
Squamous cell carcinoma (SCC)SCC in organ transplant recipients (OTRs) mayhave an atypical clinical appearance, and a highindex of suspicion is required. Pain andtenderness are useful guides to possible malig-nancy, but diagnostic accuracy may be as low as50%5. Important differential diagnoses includeviral warts (which may be clinically andhistologically atypical), squamous cellcarcinoma-in-situ (Bowen’s disease), actinickeratoses (AK, partial thickness keratinocyteintraepithelial dysplasia), other rare skintumours such as appendageal malignanciesand atypical infections (Figure 1).
Basal cell carcinoma (BCC):Diagnosis of OTR BCC is usually straight-forward, although superficial BCCs on thetrunk are more common, usually asymptom-atic and are often unnoticed by patients6. Onecommon, benign post-transplant skin lesionoften misdiagnosed as nodular BCC issebaceous gland hyperplasia (Figure 2).
Figure 1: Infective lesionssimulating squamous cellcarcinoma:1a: Ulcerated nodule on thedorsum of the left middle fingerdue to atypical mycobacterialinfection.1b: Chronic herpes simplexinfection on the chin. Bothlesions 1a and 1b werediagnosed clinically as possibleSCC.
Figure 2: Sebaceous gland hyperplasia may simulate BCCSebaceous gland hyperplasia is common in OTRs and isprobably related to ciclosporin exposure. Individual lesionsmay be misdiagnosed as BCC or as molluscumcontagiosum.
Actinic keratoses, Bowen’s disease and fieldcarcinogenesisUsually presenting as red, hyperkeratoticpapules and plaques, AK and Bowen’s diseasemay arise as discrete lesions or may be multipleand confluent on locations such as the dorsa ofthe hands and scalp. These areas of ‘fieldcarcinogenesis’ are sites at which SCC
December 2010 7
1b
References1. Berg D, Otley CC 2002 Skin cancer in
organ transplant recipients:Epidemiology, pathogenesis, andmanagement. J Am Acad Dermatol47(1) 1-17. Review
2. Euvrard S, Kanitakis J, Claudy A 2003Skin cancers after organ transplantation.N Engl J Med 348 1681-1691
3. Ulrich C, Kanitakis J, Stockfleth E,Euvrard S 2008 Skin cancer in organtransplant recipients – where do westand today? Am J Transplant 8(11)2192-2198. Review
4. Proby CM, Wisgerhof HC, CasabonneD et al 2009 The epidemiology of
MANAGEMENT OF SKIN CANCER IN ORGAN TRANSPLANT RECIPIENTS
the skin (Figure 5). Diagnosis is confirmed byskin biopsy; upper gastrointestinal endoscopyand lung imaging/bronchoscopy may berequired to exclude visceral disease.
Rare skin malignanciesSkin tumours of eccrine, apocrine, follicular andsebaceous appendages, particularly sebaceouscarcinoma and eccrine porocarcinoma, aremore common in OTRs, but are rarely diag-nosed prior to surgery, as most present asrather non-specific, ulcerated, red nodules11.Merkel cell carcinoma, a highly aggressivecutaneous neuroendocrine tumour, is alsomore common in OTRs, is associated withsignificant mortality and presents as a rapidlygrowing, purple nodule on sun-exposed sites12.
TREATMENT OF PRIMARY TUMOURSThe available evidence informing appropriatetreatment for OTR skin malignancies is farfrom complete. There are few prospective,randomised control trials and only limitednumbers of retrospective and/or observationalstudies to guide decision-making. In theabsence of systematic evidence, efforts havebeen made to obtain consensus expertopinion in particularly important managementareas13,14,7. A multidisciplinary approach is
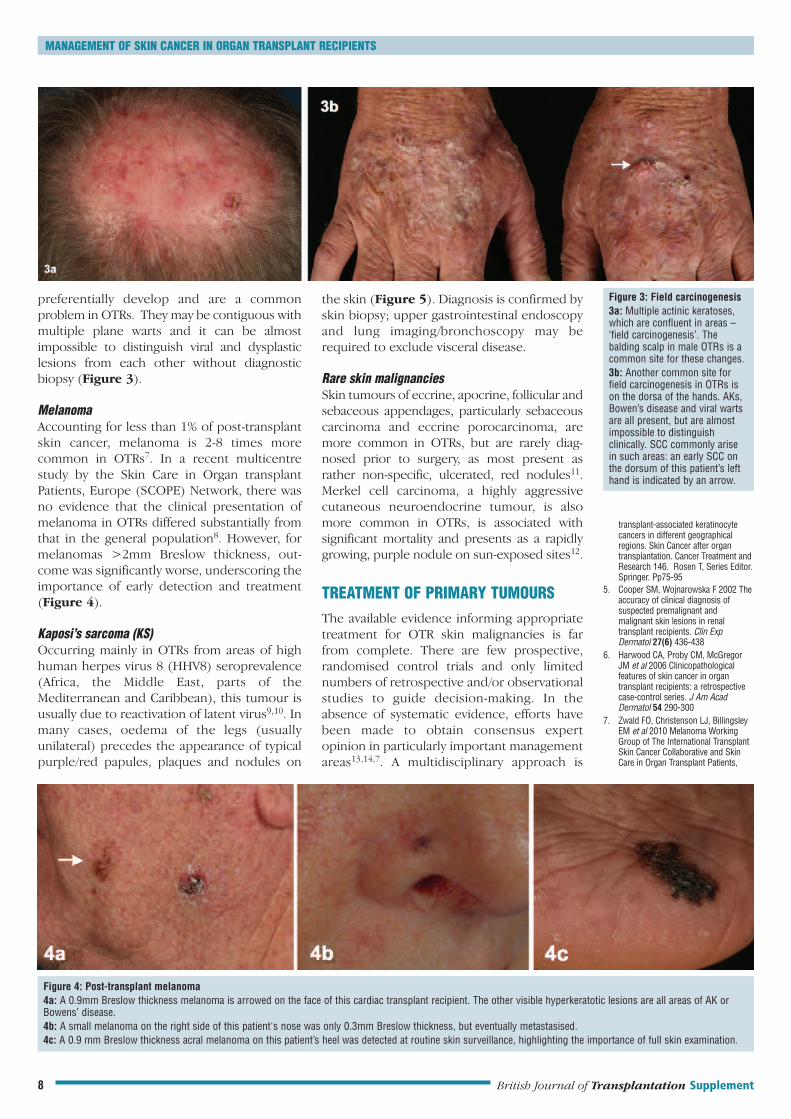
preferentially develop and are a commonproblem in OTRs. They may be contiguous withmultiple plane warts and it can be almostimpossible to distinguish viral and dysplasticlesions from each other without diagnosticbiopsy (Figure 3).
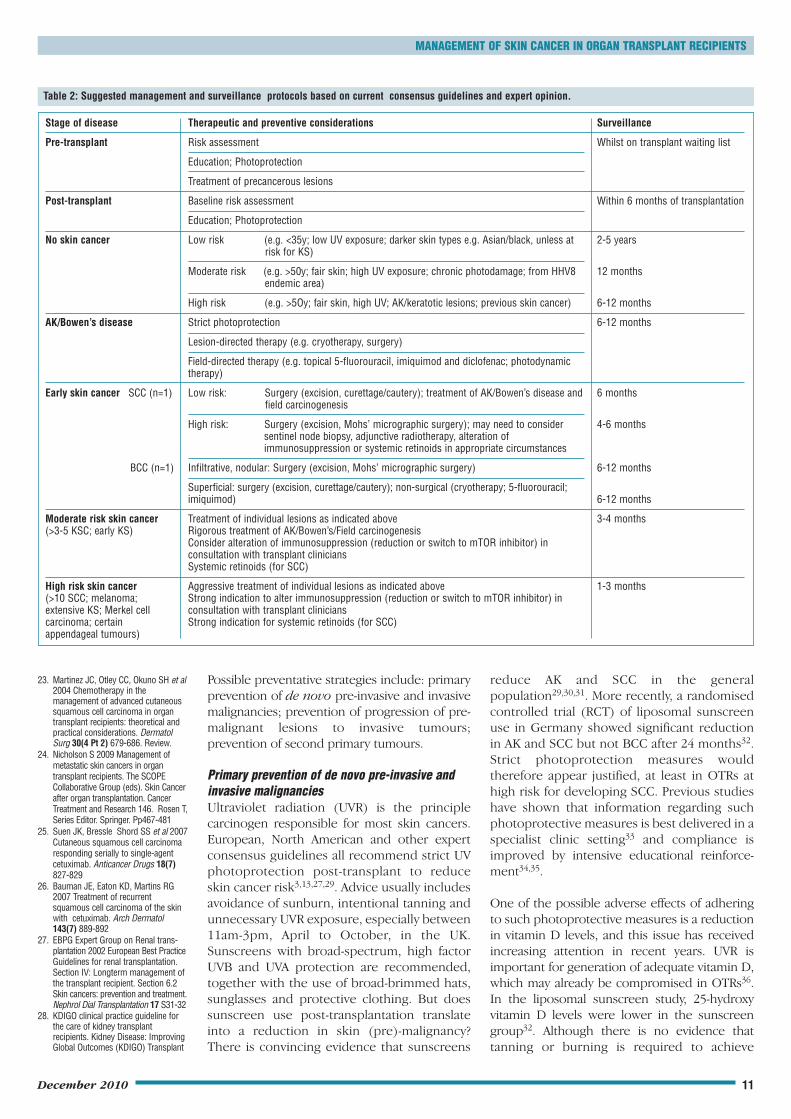
MelanomaAccounting for less than 1% of post-transplantskin cancer, melanoma is 2-8 times morecommon in OTRs7. In a recent multicentrestudy by the Skin Care in Organ transplantPatients, Europe (SCOPE) Network, there wasno evidence that the clinical presentation ofmelanoma in OTRs differed substantially fromthat in the general population8. However, formelanomas >2mm Breslow thickness, out-come was significantly worse, underscoring theimportance of early detection and treatment(Figure 4).
Kaposi’s sarcoma (KS)Occurring mainly in OTRs from areas of highhuman herpes virus 8 (HHV8) seroprevalence(Africa, the Middle East, parts of theMediterranean and Caribbean), this tumour isusually due to reactivation of latent virus9,10. Inmany cases, oedema of the legs (usuallyunilateral) precedes the appearance of typicalpurple/red papules, plaques and nodules on
Figure 3: Field carcinogenesis3a: Multiple actinic keratoses,which are confluent in areas –‘field carcinogenesis’. Thebalding scalp in male OTRs is acommon site for these changes.3b: Another common site forfield carcinogenesis in OTRs ison the dorsa of the hands. AKs,Bowen’s disease and viral wartsare all present, but are almostimpossible to distinguishclinically. SCC commonly arisein such areas: an early SCC onthe dorsum of this patient’s lefthand is indicated by an arrow.
Figure 4: Post-transplant melanoma4a: A 0.9mm Breslow thickness melanoma is arrowed on the face of this cardiac transplant recipient. The other visible hyperkeratotic lesions are all areas of AK orBowens’ disease.4b: A small melanoma on the right side of this patient's nose was only 0.3mm Breslow thickness, but eventually metastasised.4c: A 0.9 mm Breslow thickness acral melanoma on this patient’s heel was detected at routine skin surveillance, highlighting the importance of full skin examination.
transplant-associated keratinocytecancers in different geographicalregions. Skin Cancer after organtransplantation. Cancer Treatment andResearch 146. Rosen T, Series Editor.Springer. Pp75-95
5. Cooper SM, Wojnarowska F 2002 Theaccuracy of clinical diagnosis ofsuspected premalignant andmalignant skin lesions in renaltransplant recipients. Clin ExpDermatol 27(6) 436-438
6. Harwood CA, Proby CM, McGregorJM et al 2006 Clinicopathologicalfeatures of skin cancer in organtransplant recipients: a retrospectivecase-control series. J Am AcadDermatol 54 290-300
7. Zwald FO, Christenson LJ, BillingsleyEM et al 2010 Melanoma WorkingGroup of The International TransplantSkin Cancer Collaborative and SkinCare in Organ Transplant Patients,
British Journal of Transplantation Supplement8

MANAGEMENT OF SKIN CANCER IN ORGAN TRANSPLANT RECIPIENTS
Table 1: Factors associated with risk of local SCC recurrence and metastasis13,76,77.
Low risk SCC: High risk SCC:
Size <2cm diameter Size >2cm diameter
Well differentiated Poorly differentiated
Depth of invasion <2mm Depth of invasion >4mm
No perineural/vascular invasion Perineural/vascular invasion and satellite lesions
High-risk location (forehead, temple, ear, lip)
important1,2,15 and close dialogue betweendermatologists and transplant clinicians iscrucial1,2,16.
Low-risk primary tumoursLow-risk invasive skin tumours and premalig-nancies, e.g. superficial and nodular BCC,Bowen’s disease, low-risk SCC (Table 1), aremanaged in a similar manner to the generalpopulation, using ‘standard treatments withincreased diligence’1.
1. Surgery: Surgical excision is often the mostappropriate option for the majority of tumours.There are few data to indicate whether excisionmargins should differ in OTRs and, in theabsence of such data, it is reasonable to exciselesions with narrow margins13. Curettage andelectrocautery also offers satisfactory clearancerates for most selected low-risk tumours,including well-differentiated SCC, and may bethe preferred option in certain clinicalsituations for reasons of cosmesis andconvenience17.
2. Non-surgical modalities: In carefully selectedcases, non-surgical approaches, includingcryotherapy, photodynamic therapy, topicalimiquimod and 5-fluorouracil (see below),may also have a therapeutic role. This is aparticular consideration in OTRs with multiplemalignancies and field carcinogenesis, inwhom repeated surgery is otherwiserequired.1,13
High-risk primary tumoursThe characteristics of high-risk SCC, i.e. thoseat potentially increased risk of local recurrenceand metastasis1,13,18 are detailed in Table 1.Other skin tumours regarded as high-risk incl-ude infiltratve/morphoeic and baso-squamousBCC, melanoma, Merkel cell carcinoma, andcertain appendageal tumours1,2,3,7,14.
1. Surgery: It is usually recommended thatsurgery for high-risk OTR tumours should be‘more aggressive’13, but in most cases thenature of the surgical approach required hasnot been clearly defined. For example, in high-risk SCC, optimal excision margins are not
established and, although Mohs’ micrographicsurgery with intra-operative margin control isoften advised13, the circumstances in which itis preferable to standard surgical approaches inOTRs have not been rigorously evaluated18. Inthe case of melanoma, there is reasonablygood evidence for recommended surgicalexcision margins in the general population, butthere has been no specific validation of this inOTRs7. Sentinel node biopsy may be used as astaging procedure in selected melanomas7 andit has also been proposed that it may provideprognostic information in other high-risk OTRskin cancers13, although there are currentlyfew data to guide its use18.
2. Radiotherapy: Surgery with clear marginsusually gives the best outcome in terms ofrecurrence18. In the general population,radiotherapy is indicated for selected primaryBCCs, inoperable SCCs and cases of SCC inwhich there are positive excision margins notamenable to further surgery or as adjunctivetherapy if extensive perineural invasion ispresent, although the evidence for this islimited19. Radiotherapy may have a similar rolein OTRs13, but case selection is particularlyimportant: given the increased long-term riskof second skin malignancies following radio-therapy and in view of the accelerated carcino-genesis seen in OTRs, there is at least atheoretical concern that they may be moresusceptible to subsequent ionising radiation-induced skin tumours.
3. Alteration of immunosuppression: This import-ant adjunctive management strategy is discus-sed further in the accompanying article in thisSupplement by Mackintosh and Jardine.Reduction of immunosuppression or switch tomTOR inhibitors should be considered forhigh-risk and/or multiple tumours and is usuallya first-line intervention for patients withKaposi’s sarcoma10,20.
4. Systemic retinoids: In patients with high-riskand/or multiple primary SCC in whomimmunosuppression cannot be altered,adjunctive use of systemic retinoids may bebeneficial (see below).
Treatment of locally advanced andmetastatic diseaseSquamous cell carcinomaThere is an estimated 7% metastatic risk for SCCin OTRs, with an overall 5-year survival of 14-39%and median 3-year survival of 56%21. In transitmetastases are more common in OTRs and oftenpresent as discrete dermal papules distinct fromthe primary SCC22. It has been suggested that
December 2010 9
Europe. Melanoma in solid organtransplant recipients. Am J Transplant10(5) 1297-304
8. Matin RN, Mesher D, Proby CM et al2008 Melanoma in organ transplantrecipients: clinicopathological featuresand outcome in 100 cases. Am JTransplantation 8 1191-1900
9. Frances C, Lebbé C 2009 Kaposi’sSarcoma. The SCOPE CollaborativeGroup (eds). Skin Cancer after organtransplantation. Cancer Treatment andResearch 146. Rosen T, Series Editor.Springer. Pp467-481
10. Lebbé C, Legendre C, Francès C.Kaposi 2008 sarcoma intransplantation. Transplant Rev(Orlando) 22(4) 252-261. Review
11. Harwood CA, McGregor JM, Swale VJet al 2003 High frequency anddiversity of cutaneous appendagealtumours in organ transplantrecipients. J Am Acad Dermatol48 401-408
12. Kanitakis J 2009 Merkel cellcarcinoma. The SCOPE CollaborativeGroup (eds). Skin Cancer after organtransplantation. Cancer Treatment andResearch 146. Rosen T, Series Editor.Springer.Pp329-341
13. Stasko T, Brown MD, Carucci JA et al2004 International Transplant-SkinCancer Collaborative; European SkinCare in Organ Transplant PatientsNetwork. Guidelines for themanagement of squamous cellcarcinoma in organ transplantrecipients. Dermatol Surg 30(4 Pt 2)642-650
14. Otley CC, Berg D, Ulrich C et al 2006Reduction of immunosuppressiontask force of the InternationalTransplant Skin Cancer Collaborativeand the Skin Care in Organ TransplantPatients Europe. Reduction ofimmunosuppression for transplant-associated skin cancer: expertconsensus survey. Br J Dermatol154(3) 395-400
15. Geusau A, Pohanka E 2009 Aftercare– a multidisciplinary approach. TheSCOPE Collaborative Group (eds).Skin Cancer after organtransplantation. Cancer Treatment andResearch 146. Rosen T, Series Editor.Springer. Pp405-415
16. Morelon E, Mahe E, Touraine J-L 2009The role of the transplant physician inthe management of skin cancers afterorgan transplantation. The SCOPECollaborative Group (eds). SkinCancer after organ transplantation.Cancer Treatment and Research 146.Rosen T, Series Editor. Springer.Pp377-390
17. de Graaf YG, Basdew VR, van Zwan-Kralt N et al 2006 The occurrence ofresidual or recurrent squamous cellcarcinomas in organ transplantrecipients after curettage andelectrodesiccation. Br J Dermatol154(3) 493-497
18. Jennings L, Schmults CD 2010Management of high-risk cutaneous

MANAGEMENT OF SKIN CANCER IN ORGAN TRANSPLANT RECIPIENTS
advanced cutaneous OTR SCC resembles headand neck SCC in the general population23.Although this is likely to become anincreasingly common scenario in the future,there are currently no standards of care formanagement of regionally advanced andmetastatic SCC in OTRs. In the absence ofspecific clinical trials, the use of surgery andradiotherapy is currently broadly similar tothat in the general population23,24. Chemo-therapeutic approaches reported include useof systemic 5-fluorouracil (capecitabine),cisplatin, paclitaxel, interferon and retinoids,with transplant-directed dosage adjustmentand close monitoring of graft function24.Epidermal growth factor receptor (EGFR)inhibitors are showing promise in metastatichead and neck SCC and there are case reportsof benefit from cetuximab in cutaneousSCC25,26. Such targeted therapies for SCC havenot specifically been evaluated in OTRs, butsome ongoing clinical trials allow OTRrecruitment, e.g. OTRs with aggressive and/ormetastatic SCC are eligible for inclusion inphase II trial of erlotinib prior to surgery orradiation and a phase II study of dasatinib(www.clinicaltrials.gov). Systemic retinoids may
also play a role in the management of advancedSCC, as may reduction of immunosuppressionand/or switch to mTOR inhibitors. However,there are few data to guide of when and howsuch approaches should be introduced1,14,18,21,24.
Other skin cancersThe prognosis for melanoma in OTRs is worsefor tumours with a Breslow thickness greaterthan 2mm8. Current management for advancedmelanoma and other skin tumours (e.g.metastatic Merkel cell or sebaceous carcinoma)is similar to that for the general population, inthe absence of specific clinical studies, althoughwith the additional strategy of possibleimmunosuppression reduction7,14,24.
PREVENTION OF SKIN CANCERIn the face of the growing clinical problem ofpost-transplant skin cancer, what should bedone to reduce or prevent this risk? Despitelimited availabile evidence addressing thisissue, OTRs present an accelerated model ofskin carcinogenesis and may therefore beregarded as an ideal population in which to testinterventions aimed at preventing skin cancer.
Figure 5: Post-transplantKaposi’s sarcoma (KS)5a: KS may initially present withunilateral leg oedema, especiallyin OTRs of African origin.5b: Early macular skin lesions.5c: An ulcerated nodule of KS.5d: More extensive plaque KS.5e: Chronic lymphoedema dueto KS may lead to secondaryskin changes, as illustrated here.
squamous cell carcinoma. J ClinAesthet Dermatol 3(4) 39-48
19. Jambusaria-Pahlajani A, Miller CJ,Quon H et al 2009 Surgicalmonotherapy versus surgery plusadjuvant radiotherapy in high-riskcutaneous squamous cell carcinoma:a systematic review of outcomes.Dermatol Surg 35(4) 574-585
20. Stallone G, Schena A, Infante B et al2005 Sirolimus for Kaposi's sarcomain renal-transplant recipients. N Engl JMed 352(13) 1317-1323
21. Martinez JC, Otley CC, Stasko T et al2003 Transplant-Skin Cancer Collab-orative. Defining the clinical course ofmetastatic skin cancer in organtransplant recipients: a multicentercollaborative study. Arch Dermatol139(3) 301-306
22. Carucci JA, Martinez JC, Zeitouni NCet al 2004 In-transit metastasis fromprimary cutaneous squamous cellcarcinoma in organ transplant recipientsand nonimmunosuppressed patients:clinical characteristics, management,and outcome in a series of 21 patients.Dermatol Surg 30(4 Pt 2) 651-655
British Journal of Transplantation Supplement10
Possible preventative strategies include: primaryprevention of de novo pre-invasive and invasivemalignancies; prevention of progression of pre-malignant lesions to invasive tumours;prevention of second primary tumours.
Primary prevention of de novo pre-invasive andinvasive malignanciesUltraviolet radiation (UVR) is the principlecarcinogen responsible for most skin cancers.European, North American and other expertconsensus guidelines all recommend strict UVphotoprotection post-transplant to reduceskin cancer risk3,13,27,29. Advice usually includesavoidance of sunburn, intentional tanning andunnecessary UVR exposure, especially between11am-3pm, April to October, in the UK.Sunscreens with broad-spectrum, high factorUVB and UVA protection are recommended,together with the use of broad-brimmed hats,sunglasses and protective clothing. But doessunscreen use post-transplantation translateinto a reduction in skin (pre)-malignancy?There is convincing evidence that sunscreens
reduce AK and SCC in the generalpopulation29,30,31. More recently, a randomisedcontrolled trial (RCT) of liposomal sunscreenuse in Germany showed significant reductionin AK and SCC but not BCC after 24 months32.Strict photoprotection measures wouldtherefore appear justified, at least in OTRs athigh risk for developing SCC. Previous studieshave shown that information regarding suchphotoprotective measures is best delivered in aspecialist clinic setting33 and compliance isimproved by intensive educational reinforce-ment34,35.
One of the possible adverse effects of adheringto such photoprotective measures is a reductionin vitamin D levels, and this issue has receivedincreasing attention in recent years. UVR isimportant for generation of adequate vitamin D,which may already be compromised in OTRs36.In the liposomal sunscreen study, 25-hydroxyvitamin D levels were lower in the sunscreengroup32. Although there is no evidence thattanning or burning is required to achieve
Table 2: Suggested management and surveillance protocols based on current consensus guidelines and expert opinion.
Stage of disease Therapeutic and preventive considerations Surveillance
Pre-transplant Risk assessment Whilst on transplant waiting list
Education; Photoprotection
Treatment of precancerous lesions
Post-transplant Baseline risk assessment Within 6 months of transplantation
Education; Photoprotection
No skin cancer Low risk (e.g. <35y; low UV exposure; darker skin types e.g. Asian/black, unless at 2-5 yearsrisk for KS)
Moderate risk (e.g. >50y; fair skin; high UV exposure; chronic photodamage; from HHV8 12 monthsendemic area)
High risk (e.g. >5Oy; fair skin, high UV; AK/keratotic lesions; previous skin cancer) 6-12 months
AK/Bowen’s disease Strict photoprotection 6-12 months
Lesion-directed therapy (e.g. cryotherapy, surgery)
Field-directed therapy (e.g. topical 5-fluorouracil, imiquimod and diclofenac; photodynamictherapy)
Early skin cancer SCC (n=1) Low risk: Surgery (excision, curettage/cautery); treatment of AK/Bowen’s disease and 6 monthsfield carcinogenesis
High risk: Surgery (excision, Mohs’ micrographic surgery); may need to consider 4-6 monthssentinel node biopsy, adjunctive radiotherapy, alteration ofimmunosuppression or systemic retinoids in appropriate circumstances
BCC (n=1) Infiltrative, nodular: Surgery (excision, Mohs’ micrographic surgery) 6-12 months
Superficial: surgery (excision, curettage/cautery); non-surgical (cryotherapy; 5-fluorouracil;imiquimod) 6-12 months
Moderate risk skin cancer Treatment of individual lesions as indicated above 3-4 months(>3-5 KSC; early KS) Rigorous treatment of AK/Bowen’s/Field carcinogenesis
Consider alteration of immunosuppression (reduction or switch to mTOR inhibitor) inconsultation with transplant cliniciansSystemic retinoids (for SCC)
High risk skin cancer Aggressive treatment of individual lesions as indicated above 1-3 months(>10 SCC; melanoma; Strong indication to alter immunosuppression (reduction or switch to mTOR inhibitor) inextensive KS; Merkel cell consultation with transplant clinicianscarcinoma; certain Strong indication for systemic retinoids (for SCC)appendageal tumours)
MANAGEMENT OF SKIN CANCER IN ORGAN TRANSPLANT RECIPIENTS
December 2010 11
23. Martinez JC, Otley CC, Okuno SH et al2004 Chemotherapy in themanagement of advanced cutaneoussquamous cell carcinoma in organtransplant recipients: theoretical andpractical considerations. DermatolSurg 30(4 Pt 2) 679-686. Review.
24. Nicholson S 2009 Management ofmetastatic skin cancers in organtransplant recipients. The SCOPECollaborative Group (eds). Skin Cancerafter organ transplantation. CancerTreatment and Research 146. Rosen T,Series Editor. Springer. Pp467-481
25. Suen JK, Bressle Shord SS et al 2007Cutaneous squamous cell carcinomaresponding serially to single-agentcetuximab. Anticancer Drugs 18(7)827-829
26. Bauman JE, Eaton KD, Martins RG2007 Treatment of recurrentsquamous cell carcinoma of the skinwith cetuximab. Arch Dermatol143(7) 889-892
27. EBPG Expert Group on Renal trans-plantation 2002 European Best PracticeGuidelines for renal transplantation.Section IV: Longterm management ofthe transplant recipient. Section 6.2Skin cancers: prevention and treatment.Nephrol Dial Transplantation 17 S31-32
28. KDIGO clinical practice guideline forthe care of kidney transplantrecipients. Kidney Disease: ImprovingGlobal Outcomes (KDIGO) Transplant
adequate vitamin D levels, this is clearly an arearequiring further research. At present, monitor-ing of vitamin D levels in OTRs and oralsupplementation, if necessary, is advisable whenrigorous photoprotection is being advocated36.
2. Preventing progression of pre-malignantlesions to invasive tumoursIt is assumed, although not proven, that AK andBowen’s disease are precursors of SCC. Thepresence of 7.7 AKs predicts a 10% risk oftransformation to SCC within 10 years in thegeneral population37; no equivalent data existfor OTRs. The rate of progression from anindividual AK to SCC is controversial, rangingfrom 0.025% to 20% per year/per lesion in thegeneral population, with up to 25% of AKregressing over one year and numbers ofprevalent AK strongly influenced by ongoing UVexposure38. A recent prospective study showedthat the risk of progression for a specific AK was2.57% at 4 years, but that 65% of all primary SCCarose directly in AK39. The remainder of SCC arepresumed to arise from sub-clinical AK,providing a rationale for treating the whole‘field’ and not just individual lesions. However,there are no clinical trials in either the generalpopulation or in OTRs confirming that treatingAK/Bowen's disease will prevent SCCs. In theabsence of such proof, it would nonethelessseem prudent to treat AK/Bowen’s disease,which may cause morbidity in their own right.
Lesion-directed versus field-directed treatments:Cryotherapy and surgery are used as ‘lesion-directed’ treatments for individual AKs/Bowen’slesions. Although surgery to prophylacticallyresurface areas of severe field carcinogenesison the dorsa of the hands may be beneficial inreducing SCC40, such approaches generallytend to be less suitable for larger areas ofmultiple and confluent pre-malignancy(Figure 3). These are usually more amenableto ‘field-directed’ therapies. Those currentlylicensed in the UK include three topical agents
(5-fluorouracil cream, imiquimod 5% creamand diclofenac 3% gel), and photodynamictherapy. Sub-clinical lesions within the areas offield change are also likely to be treated withthis approach, possibly increasing the benefitin terms of potential reduction in SCC. Field-directed treatments are often combined withlesion-directed therapies for more resistantlesions, and a low threshold for biopsy of anypersistent lesions is indicated to excludeinvasive malignancy.
(i) 5-Fluorouracil cream, an inhibitor ofthymidylate synthetase, is cytostatic to prolifer-ating cells. As a 5% cream, it has been usedwidely for over 35 years as a treatment for AK,although few controlled studies of its efficacyin either the general population or OTRs havebeen published40,41. It is usually applied onceor twice daily for 3-4 weeks. In two studies inthe general population, it achieved 70%clearance of AK at 6 months42 and 78%clearance sustained for 12 months43. Lowerclearance rates have been reported in OTRs 44.Both 5-fluorouracil (5-FU) and 5% imiquimodhave similar local side-effects with erythema(often severe) with crusting, erosions or evenulceration (Figure 7). The clinical response islargely in proportion to these side-effects.
(ii) 5% Imiquimod cream is an immuneresponse modifier and agonist for toll-likereceptors 7 and 8, activating the innate immunesystem and generating a Th1 cytotoxic response.It has been more rigorously studied in clinicaltrials compared to 5-FU41. Several randomisedcontrolled trials in the general population, using5% imiquimod 3 times per week for 4-16 weeksdemonstrated 64-84% clearance of AK, withlimited long-term data45,46. In an RCT in 20 OTRs,50% clinical and 37% histological improvementwere obtained and there were fewer SCC intreated skin over 12 months, although this didnot reach statistical significance47. In a larger,multicentre RCT including 43 OTRs in 6
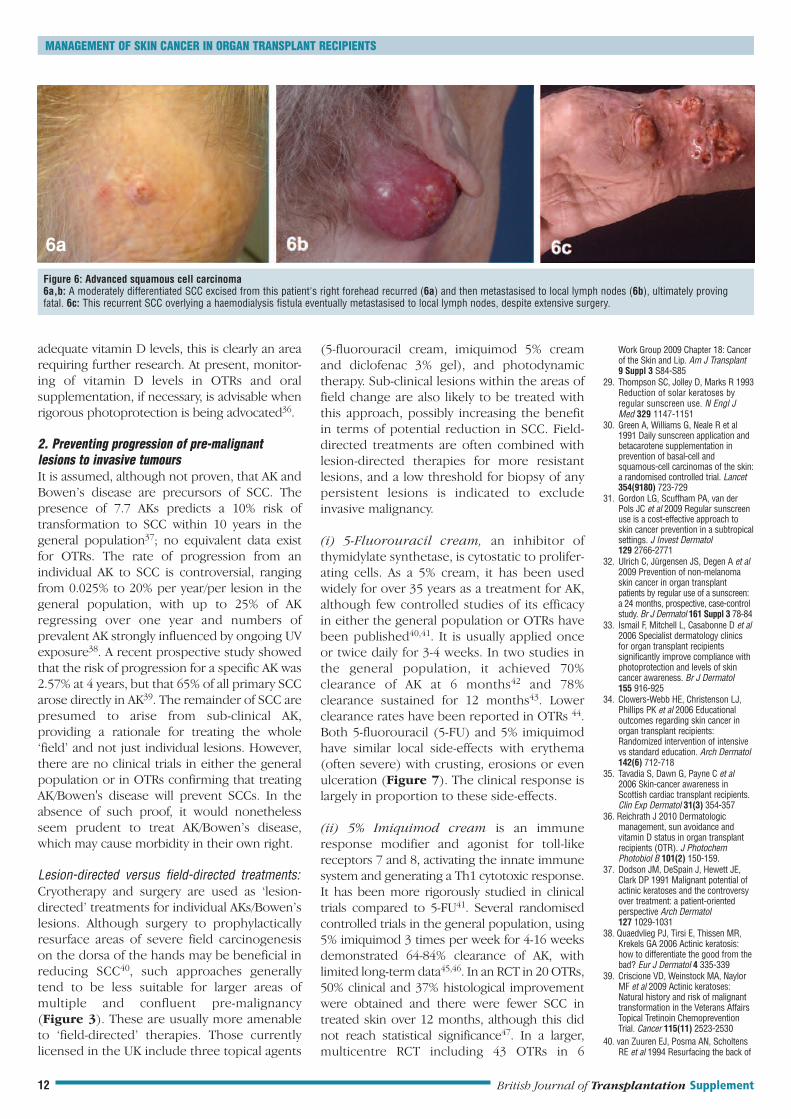
Figure 6: Advanced squamous cell carcinoma6a,b: A moderately differentiated SCC excised from this patient's right forehead recurred (6a) and then metastasised to local lymph nodes (6b), ultimately provingfatal. 6c: This recurrent SCC overlying a haemodialysis fistula eventually metastasised to local lymph nodes, despite extensive surgery.
MANAGEMENT OF SKIN CANCER IN ORGAN TRANSPLANT RECIPIENTS
Work Group 2009 Chapter 18: Cancerof the Skin and Lip. Am J Transplant9 Suppl 3 S84-S85
29. Thompson SC, Jolley D, Marks R 1993Reduction of solar keratoses byregular sunscreen use. N Engl JMed 329 1147-1151
30. Green A, Williams G, Neale R et al1991 Daily sunscreen application andbetacarotene supplementation inprevention of basal-cell andsquamous-cell carcinomas of the skin:a randomised controlled trial. Lancet354(9180) 723-729
31. Gordon LG, Scuffham PA, van derPols JC et al 2009 Regular sunscreenuse is a cost-effective approach toskin cancer prevention in a subtropicalsettings. J Invest Dermatol129 2766-2771
32. Ulrich C, Jürgensen JS, Degen A et al2009 Prevention of non-melanomaskin cancer in organ transplantpatients by regular use of a sunscreen:a 24 months, prospective, case-controlstudy. Br J Dermatol 161 Suppl 3 78-84
33. Ismail F, Mitchell L, Casabonne D et al2006 Specialist dermatology clinicsfor organ transplant recipientssignificantly improve compliance withphotoprotection and levels of skincancer awareness. Br J Dermatol155 916-925
34. Clowers-Webb HE, Christenson LJ,Phillips PK et al 2006 Educationaloutcomes regarding skin cancer inorgan transplant recipients:Randomized intervention of intensivevs standard education. Arch Dermatol142(6) 712-718
35. Tavadia S, Dawn G, Payne C et al2006 Skin-cancer awareness inScottish cardiac transplant recipients.Clin Exp Dermatol 31(3) 354-357
36. Reichrath J 2010 Dermatologicmanagement, sun avoidance andvitamin D status in organ transplantrecipients (OTR). J PhotochemPhotobiol B 101(2) 150-159.
37. Dodson JM, DeSpain J, Hewett JE,Clark DP 1991 Malignant potential ofactinic keratoses and the controversyover treatment: a patient-orientedperspective Arch Dermatol127 1029-1031
38. Quaedvlieg PJ, Tirsi E, Thissen MR,Krekels GA 2006 Actinic keratosis:how to differentiate the good from thebad? Eur J Dermatol 4 335-339
39. Criscione VD, Weinstock MA, NaylorMF et al 2009 Actinic keratoses:Natural history and risk of malignanttransformation in the Veterans AffairsTopical Tretinoin ChemopreventionTrial. Cancer 115(11) 2523-2530
40. van Zuuren EJ, Posma AN, ScholtensRE et al 1994 Resurfacing the back of
British Journal of Transplantation Supplement12
6a

countries, complete response was observed in62.1% and partial response in 80%48.
(iii) Diclofenac 3% gel inhibits cyclo-oxygenase-2pathways and tends to be used for less severedisease, as it generally causes less inflammatoryresponse compared with 5-fU and 5%imiquimod. In an RCT of 32 OTR with multipleAK treated twice daily for 16 weeks with 3%dicofenac gel, complete clearance wasobtained in 41% but recurrent disease wasnoted at 24 months in 55%49.
A problem with many previous clinical trials hasbeen that rates of recurrence and/or develop-ment of new lesions within the field after acourse of treatment with these topical agentshave not been well characterised, as follow-upis often insufficiently prolonged. It is thereforenot clear how frequently such field treatmentsshould be used to maintain clearance andthereby, it is assumed, to reduce SCC develop-ment. This is particularly important in OTRs inwhom the rate of recurrence and/or develop-ment of new lesions within a field is likely to beaccelerated compared with the generalpopulation.
Photodynamic Therapy (PDT) PDT is an altern-ative non-surgical option for treating individualAKs or larger fields of thin, non-hyperkeratoticAK. Topical aminolaevulinic acid (ALA) ormethylaminolaevulinic acid (MAL) is applied tothe target lesions (after removal of hyper-keratosis if necessary). The drug preferentiallyaccumulates in dysplastic keratinocytes and isconverted into protoporphyrin IX. This is apotent photosensitiser and, upon exposure to alight source, generates reactive oxygen species,which leads to destruction of dysplastic cells.The use of PDT for treatment of AK in the
general population is well established41, andthere have been a number of studies in OTRs.In an RCT of ALA-PDT with red light, 88% ofOTRs responded at 4 weeks, reducing to 48% at48 weeks, compared with 94% responsereducing to 72% in immunocompetent patients(p<0.05). This difference possibly reflects eithermore persistent lesions in OTRs or increasedrecurrence rates. Response was lowest onhands/arms, a feature also noted in use oftopical agents50. In a separate RCT in 17 OTRusing MAL-PDT, 76% complete clearance wasobserved at 16 weeks51. In a small, within-patient RCT comparing MAL-PDT with topical 5-fluorouracil, PDT was found to be significantlymore effective, with superior cosmesis andpatient satisfaction, but was also associated withmore pain44. Several RCTs have directly invest-igated PDT in SCC prevention52,53,54,55. Althoughall have shown significant reductions in AK, thisis not always sustained and only one has showna possible prophylactic effect55.
3. Prevention of second primary tumoursOver 60% of OTRs will develop more than oneskin malignancy and, after a first KSC, 75% willhave a second within 5 years56,57. The timeinterval between subsequent KSC shortensprogressively. What additional preventativestrategies are available for such high-riskindividuals?
1. Alteration of immunosuppressive drug regimensAlteration of immunosuppression as an approachto reducing SCC risk has been discussed in detailin the accompanying review by Mackintosh andJardine. Reduction of immunosuppression isprobably the most frequently consideredapproach in current practice, but there is limitedevidence on which to base the decision of whento consider it and to what extent immuno-suppression should be reduced14. Increasingevidence also supports conversion fromcalcineurin inhibitors to mTOR inhibitors as anadditional strategy; Salgo et al58 have recentlyshown that conversion from CNIs to sirolimussignificantly reduces incidence of SCC at 12months and there are a number of other ongoingRCTs (TUMORAPA, RESCUE, PROSKIN,CERTICOEUR; www.clinicaltrials.gov), whichshould inform development of clear guidelines inthe near future.
2. Systemic retinoids Retinoids (acitretin,isotretinoin and previously etretinate) alter genetranscription through action on cellular retinoidreceptors. They are antiproliferative, antiapop-totic, immunomodulatory, modulate keratinocytedifferentiation and arrest growth and replicationof HPV59, all of which may be relevant to skincancer prophylaxis. Three RCTs have examined
Figure 7: Topical treatments for AK/field carcinogenesisBoth 5-fluorouracil and 5% imiquimod creams usually cause erythema with crusting, erosions andeven ulceration. Areas of subclinical disease are often highlighted by the application of theseagents, as illustrated here. The reaction to topical diclofenac gel tends to be milder.
MANAGEMENT OF SKIN CANCER IN ORGAN TRANSPLANT RECIPIENTS
December 2010 13
the hand as treatment and preventionof multiple skin cancers in kidneytransplant recipients. J Am AcadDermatol 31(5 Pt 1) 760-764
41. Amini S, Viera MH, Valins W et al2010 Nonsurgical innovations in thetreatment of non-melanoma skincancer. J Clin Aesthet Dermatol3(6) 20-34
42. Kurwa HA, Yong-Gee SA, Seed PT etal 1999 A randomized pairedcomparison of photodynamictherapy and topical 5-fluorouracil inthe treatment of actinic keratoses.J Am Acad Dermatol41(3 Pt 1) 414-418
43. Witheiler DD, Lawrence N, Cox SE etal 1997 Long-term efficacy and safetyof Jessner’s solution and 35%trichloroacetic acid vs 5-fluorouracil inthe treatment of facial actinickeratoses. Dermatol Surg 23 191-196
44. Perrett CM, McGregor JM, Warwick Jet al 2007 Treatment of post-transplant pre-malignant skin disease:a randomised intra-patientcomparative study of 5-fluorouracilcream and topical photodynamictherapy Br J Dermatol 156 320-328
45. Lebwohl M et al 2004 Imiquimod 5%cream for the treatment of actinickeratosis: results from two phase III,randomised, double-blind, parallelgroup, vehicle-controlled trials JAAD50 714-721
46. Stockfleth E et al 2007 Multicentre,open-label study using imiquimod 5%cream in one or two 4-week treatmentcourses for multiple actinic keratoseson the head. Br J Dermatol157(suppl2) 41-46
47. Brown VL, Atkins CL, Ghali L et al2005 Safety and Efficacy of 5%Imiquimod Cream for the Treatment ofSkin Dysplasia in High Risk RenalTransplant Recipients: Randomised,Double-Blind, Placebo-Controlled Trial.Arch Dermatol 141 985-993
48. Ulrich C, Bichel J, Euvrard S et al 2007Topical immunomodulation undersystemic immunosuppression: resultsof a multicentre, randomized, placebo-controlled safety and efficacy study ofimiquimod 5% cream for the treatmentof actinic keratoses in kidney, heart,and liver transplant patients.Br J Dermatol 157 Suppl 2 25-31
49. Ulrich C, Johannsen A, Röwert-HuberJ et al 2004 Results of a randomized,

the chemopreventive effects of systemic retinoidsin reducing in AK and/or SCC in OTRs60,61,62. Allstudies except one were for 2 years or less, but allconfirmed a reduction in AK and, to a variableextent, SCC. In a retrospective analysis of low-dose systemic retinoids over 16 years at ourinstitution, retinoids resulted in a significantreduction in SCC, particularly in the first 3-4 yearsof treatment, but probably sustained for muchlonger. They were generally well tolerated, themain adverse effects being cheilitis, xerosis andhyperlipidaemia. Although adverse effects limiteddosing in some patients, in only a small minoritywas the drug discontinued because of theseadverse effects. If withdrawn, either intentionallyor inadvertently, a rebound phenomenon with asharp increase in SCC development was commonapproximately 3-4 months after stopping systemicretinoids63. Consensus opinion recommends thatretinoids should be started at low dose andincreased as tolerated to minimally effectivedose64. However, further research is needed toclarify the indications for their initiation, as well asthe tolerability and efficacy of optimal dosingregimens.
Future prospects for preventionA number of topical and systemic approachesare currently in clinical trials in OTRs or haveshown promise in the immunocompetentpopulation and may have potential prophylacticproperties. For most, clinical evidence remainsrelatively limited.
T4 endonuclease V (T4N5) is an enzymeinvolved in repair of DNA damage after expos-ure to UVR, specifically cyclobutane pyrimidinedimers. Clinical efficacy of a topical liposomalformulation in reducing AKs has been demon-strated in patients with the xerodermapigmentosum, a disorder of nucleotideexcision repair65. A Phase II study of T4N5lotion looking at safety and efficacy inpreventing keratinocyte skin cancer inOTRs is currently underway in OTRs(www.clinicaltrials.gov; identifier, NCT00089180).
New topical agents for treatment of AK are indevelopment and include, for example, alpha-difluoromethylornithine (an irreversible inhibitorof ornithine decarboxylase), resiquimod (a morepotent toll-like receptor 7/8 agonist thanimiquimod), ingenol mebutate (an extract fromthe plant Euphorbia peplus) and betulinic acid (apentacyclic triterpene from the outer bark ofbirch). These agents have various antitumouraleffects and are currently in phase II and III clinicaltrials in the general population41.
Laser induction of coagulative necrosis andtissue destruction has been used in the general
population to treat skin cancer; CO2 lasers havebeen used to treat superficial BCCs and Bowen’sdisease66 and neodymium (Nd) and Nd:YAGlasers have also been used to treat BCC andSCC67. Their use in field carcinogenesis in OTRshas not yet been specifically reported, but lasersand other resurfacing techniques such asdermabrasion and chemical peels may bepredicted to be a potentially useful adjunct totreatment of field change1.
Capecitabine is an oral prodrug of 5-fluorouracil. Its use in prevention of SCC wasreported recently in a retrospective series of 15OTRs with recurrent KSC in whom it was usedat low dose over 12 months. It significantlyreduced the incidence rates of SCC, BCC and AKand associated toxicity was deemed to bemanageable, although one-third of patients haddiscontinued use by 12 months68.
Afamelanotide (CUV1647) is a chemical ana-logue of alpha-melanocyte stimulating hormone(a-MSH). Alpha-MSH is produced by keratino-cytes and melanocytes in response UVB andinduces synthesis of melanin in melanocytes aspart of the tanning response. Afamelanotide ismore potent and longer acting than naturalalpha-MSH. It may be administered by sub-cutaneous pellet. It is currently in phase II trialsto investigate its efficacy in reducing AKs andSCC in OTRs (www.clinicaltrials.gov; identifierNCT00829192).
SCREENING, SURVEILLANCE ANDFOLLOW-UPGiven the greatly increased incidence of skincancer in the OTR population, it would seemappropriate to offer routine screening andsurveillance for this high-risk group. However,the effectiveness and cost-benefit of screeningfor skin cancer has not been established ineither the general population or in OTRs69. Inthe absence of such data, and based uponexpert consensus opinion1,3,13,27,28,69,70,71, thefollowing OTR surveillance strategies havebeen proposed:
Baseline post-transplant assessmentFollowing transplantation, OTRs should beoffered baseline assessment in whicheducation regarding individual skin cancer risk,photoprotection, regular self-skin examinationand early detection of suspicious lesions isprovided. There is evidence that such healtheducation advice is better recalled andimplemented and skin cancer awareness isimproved if information is provided in thesetting of a specialist skin clinic33.
MANAGEMENT OF SKIN CANCER IN ORGAN TRANSPLANT RECIPIENTS
placebo-controlled safety and efficacystudy of topical diclofenac 3% gel inorgan transplant patients with multipleactinic keratoses. Eur J Dermatol 20(4)482-488
50. Dragieva G, Hafner J, Dummer R et al2004 Topical photodynamic therapy inthe treatment of actinic keratoses andBowen's disease in transplantrecipients. Transplantation77(1) 115-121
51. Dragieva G, Prinz BM, Hafner J et al2004 A randomized controlled clinicaltrial of topical photodynamic therapywith methyl aminolaevulinate in thetreatment of actinic keratoses intransplant recipients. Br J Dermatol151(1) 196-200
52. de Graaf YG, Kennedy C, WolterbeekR et al 2006 Photodynamic therapydoes not prevent cutaneoussquamous-cell carcinoma in organ-transplant recipients: results of arandomized-controlled trial. J InvestDermatol 126(3) 569-574
53. Wulf HC, Pavel S, Stender I, Bakker-Wensveen CA 2006 Topicalphotodynamic therapy for preventionof new skin lesions in renal transplantrecipients. Acta Derm Venereol86(1) 25-28
54. Wennberg AM, Stenquist B, StockflethE et al 2008 Photodynamic therapywith methyl aminolevulinate forprevention of new skin lesions intransplant recipients: a randomizedstudy. Transplantation 86(3) 423-429
55. Willey A, Mehta S, Lee PK 2010Reduction in the incidence ofsquamous cell carcinoma in solidorgan transplant recipients treatedwith cyclic photodynamic therapy.Dermatol Surg 36(5) 652-658
56. Euvrard S, Kanitakis J, Decullier E et al2006 Subsequent skin cancers inkidney and heart transplant recipientsafter the first squamous cell carcinoma.Transplantation 81(8) 1093-1100.
57. Wisgerhof HC, Edelbroek JR, de FijterJW et al 2010 Subsequent squamous-and basal-cell carcinomas in kidney-transplant recipients after the first skincancer: cumulative incidence and riskfactors. Transplantation 89 1231-1238
58. Salgo R, Gossmann J, Schöfer H et al2010 Switch to a sirolimus-basedimmunosuppression in long-termrenal transplant recipients: reducedrate of (pre-)malignancies andnonmelanoma skin cancer in aprospective, randomized, assessor-blinded, controlled clinical trial. Am JTransplant 10(6) 1385-1393
59. Shumack S 2009. Systemicchemoprevention. The SCOPECollaborative Group (eds). SkinCancer after organ transplantation.Cancer Treatment and Research 146.Rosen T, Series Editor. Springer.Pp461-466.
60. Bouwes Bavinck JN, Tieben LM, VanDer Woude FJ et al 1995 Preventionof skin cancer and reduction ofkeratotic skin lesions during acitretintherapy in renal transplant recipients:a double-blind, placebo-controlledstudy. J Clin Oncol 13 1933-1938
61. George R, Weightman W, Russ GR etal 2002 Acitretin for chemopreventionof non-melanoma skin cancers inrenal transplant recipients. Austral JDermatol 43 269-273
62. De Sévaux RGL, Smit JV, de JongEMGJ et al 2003 Acitretin treatment ofpremalignant and malignant skindisorders in renal transplantrecipients: clinical effects of arandomized trial comparing two doses
British Journal of Transplantation Supplement14

Subsequent post-transplant skin cancersurveillanceIndividual risk stratification at baseline shoulddetermine the appropriateness and frequencyof long-term surveillance. It is widely recom-mended that all OTRs should performmonthly self-skin examination and shouldhave a full skin examination by a specialistevery 6-12 months3,13,27,28,70,71, but the data tosupport these recommendations are limited.It might be argued, for example, that youngerOTRs with darker skin types do not requiresuch frequent surveillance, at least in the first5-10 years post-transplant.
Once skin cancers and pre-cancerous lesionsdevelop, routine surveillance is justifiablebased upon the known epidemiology of skincancer in this group; tumours are multiple intwo-thirds of OTRs, the time interval betweenconsecutive KSCs steadily decreases and over75-80% of OTRs develop further tumourswithin 5 years of the first56,57,72. The increasingclinical need was highlighted in England andWales in the 2006 National Institute for Healthand Clinical Excellence (NICE) document‘Guidance on Improving Outcomes in Peoplewith Melanoma and Other Skin Cancers’73. Thishas recommended that OTRs (and otherimmunosuppressed individuals) who have pre-cancerous skin lesions or who have developeda skin cancer should be seen in dedicatedclinics. Based upon OTR skin cancer epidem-iology, those with low risk lesions, e.g. AK,Bowen’s disease, BCC, are likely to benefitfrom at least annual review. Once SCC develop,surveillance should be more frequent – at least6 monthly, reducing to 3-4 monthly for patientswith multiple tumours and even morefrequently in those with very high risktumours1,2,7,13,18,27,28,70,71,72,73.
Pre-transplantation screeningIn order to make the greatest impact upon post-transplant skin cancer incidence, it is plausiblethat potential risk reduction strategies such asphotoprotection and treatment of AK are bestinitiated in the pre-transplant period, althoughthis has yet to be confirmed1,3,13,69,71,74. Riskstratification including, for example, deter-mination of HHV 8 status, may informappropriate tailoring of transplant immuno-suppressive drug regimens. It is also becoming
increasingly common for patients with a historyof skin cancer to present for organ trans-plantation74,75. For most, the benefits will out-weigh the risks associated with further skin cancerdevelopment or possible recurrence andmetastasis. In cases of metastatic KSC and in moreadvanced primary melanoma, transplantation isalmost always contraindicated. In all other cases, itis advisable that decisions should be made inconsultation with a transplant dermatologist74,75.
ORGANISATIONS FOR PATIENTS ANDHEALTH CARE PROFESSIONALSSeveral special interest groups focusing oneducation for patients and health care providers,prevention, treatment and research have beenlaunched in recent years, the most active beingSCOPE and ITSCC. In Europe, SCOPE (Skin Carein organ transplant patients – Europe;www.scopenetwork.org) has coordinated anumber of research initiatives and, in collab-oration with ITSCC (International TransplantSkin Cancer Collaborative; www.itscc.org), hasproduced several expert consensus guidelinedocuments for management of post-transplantskin cancer7,13,14. The AT-RISC Alliance (AfterTransplant-Reduce the incidence of Skin Cancer;www.at-risc.org) is linked to ITSCC and hasdeveloped very helpful educational resources forboth patients and healthcare providers.
CONCLUSIONSThe growing clinical problem of skin cancer inOTRs represents a significant burden for patientsand a poses a challenge for health care providersand resources. Recognition and assessment ofthe potential risk, together with appropriatecounselling, surveillance, preventative strategiesand, when suspicious skin lesions arise, rapidtreatment, should help reduce the incidence andimpact of these skin cancers in the future.However, the evidence base for their treatmentand prevention is lacking in many areas andfurther research is urgently required. These high-risk patients present a model of accelerated skincarcinogenesis and are an ideal population forsuch clinical studies examining established andnovel therapeutic and preventative approaches.Indeed, it is likely that many future advances inmanagement of skin cancer, particularly KSC, willcome from research in the transplant population.
MANAGEMENT OF SKIN CANCER IN ORGAN TRANSPLANT RECIPIENTS
Funding sources:CAH is currently supported by Cancer Research UK, Barts and the London Charity, the Medical Research Council and the British Skin Foundation.
CMP is currently supported by Cancer Research UK, Tenovus, Association for International Cancer Research, Leng Charitable Trust andAnomymous Trust.
December 2010 15
of acitretin. J Am Acad Dermatol49 407-412
63. Harwood CA, Leedham-Green M,Leigh IM, Proby CM 2005 Low-doseretinoids in the prevention ofcutaneous squamous cell carcinomasin organ transplant recipients: a 16-year retrospective study. ArchDermatol 141(4) 456-464
64. Martinez JC, Otley CC, Euvrard S et al2004 International Transplant-SkinCancer Collaborative. Complications ofsystemic retinoid therapy in organtransplant recipients with squamouscell carcinoma. Dermatol Surg30(4 Pt 2) 662-666
65. Yarosh D, Klein J, O'Connor A et al2001 Effect of topically applied T4endonuclease V in liposomes on skincancer in xeroderma pigmentosum: arandomised study. XerodermaPigmentosum Study Group. Lancet357(9260) 926-929
66. Covadonga Martínez-González M, delPozo J, Paradela S et al 2008 Bowen’sdisease treated by carbon dioxidelaser. A series of 44 patients.J Dermatolog Treat 19(5) 293-299
67. Moskalik K, Kozlov A, Demin E et al2009 The efficacy of facial skin cancertreatment with high energy pulsedneodymium and Nd:YAG lasers.Photomed Laser Surg 27(2) 345-349
68. Jirakulaporn T, Endrizzi B, Lindgren Bet al 2010 Capecitabine for skincancer prevention in solid organtransplant recipients. Clin Transplantdoi:10.1111/j.13990012.2010.01348.x
69. Webster AC, Wong G, Craig JC,Chapman JR 2008 Managing cancerrisk and decision making after kidneytransplantation. Am J Transplant 8(11)2185-2191
70. Carucci JA 2004 Cutaneous oncologyin organ transplant recipients; meetingthe challenge of squamous cell carcinoma.J Invest Dermatol 123 809-816
71. Christenson LJ, Geusau A, Ferrandiz Cet al 2004 Specialty clinics for thedermatologic care of solid-organtransplant recipients. Dermatol Surg30(4 Pt 2) 598-603. Review
71. Brewer JD, Colegio OR, Phillips PK etal 2009 Incidence of and risk factorsfor skin cancer after heart transplant.Arch Dermatol 145 1391-1396
73. National Institute for Health andClinical Excellence 2006 Improvingoutcomes for people with skintumours including melanoma: themanual (guidance)
74. Otley CC 2009 Pre-transplantationdermatologic screening andprophylaxis. The SCOPE CollaborativeGroup (eds). Skin Cancer after organtransplantation. Cancer Treatment andResearch 146. Rosen T, Series Editor.Springer. Pp391-404
75. Otley CC, Hirose R, Salasche SJ. 2005.Skin cancer as a contraindication toorgan transplantation. Am JTransplant 5(9) 2079-2084. Review
76. Rowe DE, Carroll RJ, Day CL Jr.Prognostic factors for localrecurrence, metastasis, and survivalrates in squamous cell carcinoma ofthe skin, ear, and lip. Implications fortreatment modality selection. J AmAcad Dermatol 26(6) 976-990.Review.
77. Brantsch KD, Meisner C, Schönfisch Bet al 2008 Analysis of risk factorsdetermining prognosis of cutaneoussquamous-cell carcinoma: aprospective study. Lancet Oncol9(8) 713-20.





























