Embed Size (px)
DESCRIPTION
Â
Citation preview

Management of chronic HBV infection in 2013
Dr Madunil A Niriella
26.09.13

Goals of therapy in HBV patients
• Prevent the development of cirrhosis, hepatic failure, liver cancer and liver-related deaths
• Intermediate endpoints predicting clinical benefits:
– Sustained suppression of HBV DNA
– HBeAg seroconversions
– HBsAg anti-HBs (best marker of immune control)
HBV probably is never cured, but rather controlled

Natural history of HBV infection
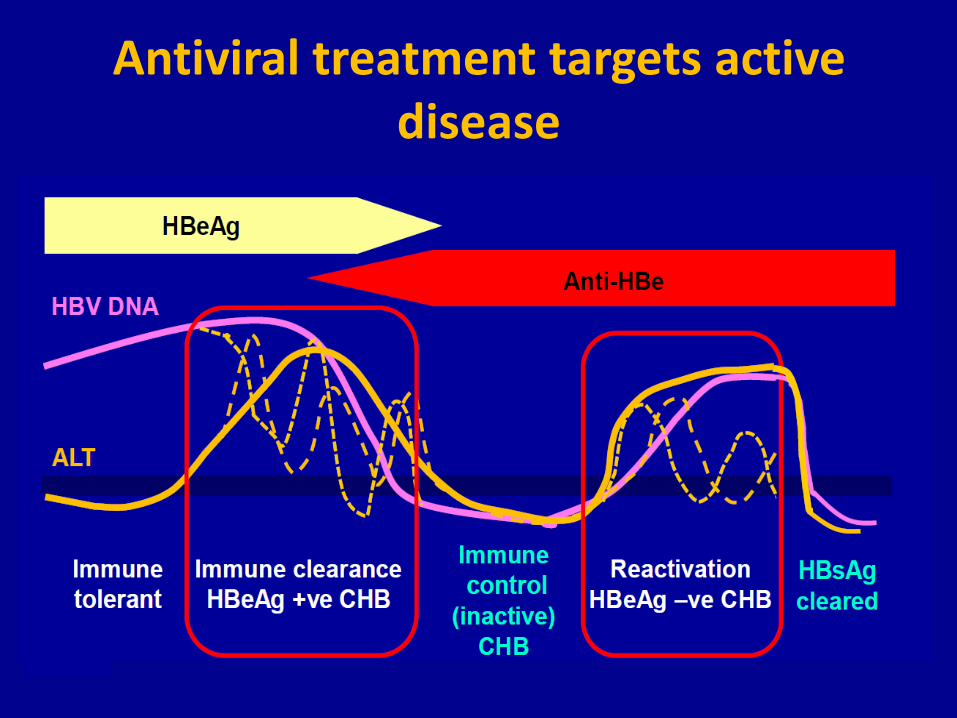
Antiviral treatment targets active disease

Antiviral Therapy Reduces Risk of Liver Related Complications

Algorithm to Determine Need for Treatment

Approved Treatments for HBV

Preferred First Line Therapy
• Peginterferon*
• Entecavir
• Tenofovir
• Tenofovir (or peginterferon) for lamivudine resistant infection
• Non-preferred HBV drugs may have role in special populations
*contraindicated in decompensated cirrhosis
AASLD Guidelines 2009 EASL Guidelines 2009 APASL Guidelines 2008

Treatment of HBeAg-Positive CHB Key Aspects of Treatment
• Preferred drugs have very low risk of resistance in treatment-naïve patients
– Tenofovir: 0% at 4 yrs (0% in LMVr)
– Entecavir: 1-2% at 3-4 yrs
– Peg-IFN: non-issue
• HBeAg seroconversion is “sentinel event”
– Duration of therapy linked with this outcome
• HBsAg is highly desired
– HBeAg loss is prerequisite but other factors emerging

Efficacy of Preferred HBV Therapies in HBeAg CHB
*Off treatment response

Controversies/Evolving Areas
• Peg-IFN: when to consider using
• Durability of HBeAg seroconversion
• Mono vs combination therapy in treatment-naïve patients

Predictors of Response HBeAg+ CHB
Traditional
• Elevated ALT
• Lower baseline HBV
DNA
• HBV genotype – A and B > C and D
Emerging
• Presence of PC/BCP mutations
• IL28 B genotype
• HBsAg level at baseline and during treatment

HBeAg Seroconversion Rates by HBV Genotype and IL28B Type
A B C D
Sonneveld M, Gastroenterology, 2012;142:513-20

Distribution of PC/BCP Varies Across HBV Genotype
Sonneveld M, EASL 2012

HBV and Precore Variant

HBV and BCP Variants

Presence of PC/BCP Mutants and HBeAg Loss at Week 78 (n=50)
Sonneveld M, EASL 2012

Durability of HBeAg Seroconversion with NA Therapy
• Conflicting results in literature
– Durability rates of 30-90%
• Potential causes for variability
– HBV DNA level at time of discontinuation
– Duration of consolidation
– Antiviral used • N=42 NA-treated patients with seroconversion • F/U mean 56 mos post seroconversion • 44% HBeAg recurrence and 50% HBV DNA >10K copies/mL
Dienstag JL, Hepatology 2003;37:748-55 Song BC Hepatology 2000;32:803-6 Reijnders J, Gastroenterology. 2010 Aug;139(2):491-8

Monotherapy Vs. Combination Therapy for Treatment-Naïve CHB
Lok AS, Gastroenterology, 2012;143(3):619-28.
Implications of New Findings
• IL28B, HBV genotype and presence of PC/BCP mutations affect HBeAg and HBsAg clearance – Favorable IL28B genotype -> consider peg-IFN as first
line therapy
• Durability of HBeAg seroconversion likely enhanced by: – Use preferred antiviral drugs
– Longer duration of consolidation therapy
• No role for combination therapy in treatment-naive patients treated with drug with higher genetic barrier to resistance

Treatment of HBeAg-Negative CHB Key Aspects of Treatment
• Preferred drugs associated with very low risk of resistance in treatment-naïve patients – Tenofovir: 0% at 4 yrs – Entecavir: 1-2% at 3-4 yrs – Peg-IFN = non-issue
• Sustained suppression of HBV DNA is immediate treatment goal
• HBsAg loss is highly desired – More frequently achieved with peg-IFN than NAs – Long-term NA therapy necessary for many – Treatment withdrawal of NA may be key

Efficacy of Preferred HBV Therapies in HBeAg-Negative CHB
*Off treatment response
Controversies/Evolving Areas
• Duration of therapy if NA used
– Discontinuation to identify sustained responders
– Adherence issues
• Enhancing HBsAg loss
– Role of peg-IFN

5-Year Follow-Up After Discontinuing
Long-Term Adefovir Therapy
Hadziyannis S, et al. J Hepatol. 2009;50(suppl 1):S9. Abstract 18

Adherence to Long-Term Oral Therapy
Ha N, Dig Dis Sci 2011;56:2423-31

Peg-IFN Add-On Therapy
• N=12 patients, peg-IFN added to NA therapy, HBeAg+ – 2/12 seroconverted after peg-IFN X 24 weeks
• Patient A - HBeAg-positive, genotype A, HBVDNA negative on entecavir plus tenofovir for 10 months
• Patient B - HBeAg negative, genotype D, cirrhosis – on entecavir with HBV-DNA non detectable for 27 mos
Kittner JM, J Clin Virol 2012;54:93-5

Summary
• Treatment initiation: ALT and HBV DNA levels all you need to make decision – Severity of histologic disease additional guide in those with
“borderline values” – HBeAg may influence choice of drugs
• Tenofovir, entecavir, and peginterferon are preferred firstline drugs – Peg-IFN offers finite therapy but more side effects – NA well tolerated and effective in achieving viral suppression
• HBsAg loss is desired goal of therapy – Peg-IFN more likely to achieve this, especially in HBeAg negative
CHB – HBV genotype, IL28B genotype, PC/BCP influence conversion

Update on HBV Management in Special Populations
• Cirrhosis
• HBV-HIV

Algorithm for Management of Patients With Cirrhosis
Keeffe EB, et al. Clin Gastroenterol Hepatol. 2008;6:1315-1341.

Issues Regarding HBV Treatment of Decompensated Cirrhosis
• Combination therapy vs monotherapy
– Multiple negative clinical consequences including death and need for LT if drug resistance develops
– If using drugs with low genetic barrier to resistance, combination therapy best long-term, otherwise monotherapy is acceptable
• Safety
– Entecavir: monitor for lactic acidosis
– Tenofovir: monitor for renal toxicity (Cr/CrCl, PO4)

Antiviral Therapy in Decompensated Cirrhotics
Summary
• Antiviral therapy indicated for all with concurrent evaluation for LT – Combination therapy recommended to avoid
virological breakthrough with prolonged therapy but this recommendation may be outdated
• Expected time to LT should influence drug choice – Need potent antiviral activity
– No clear advantage of combo if potent antiviral used
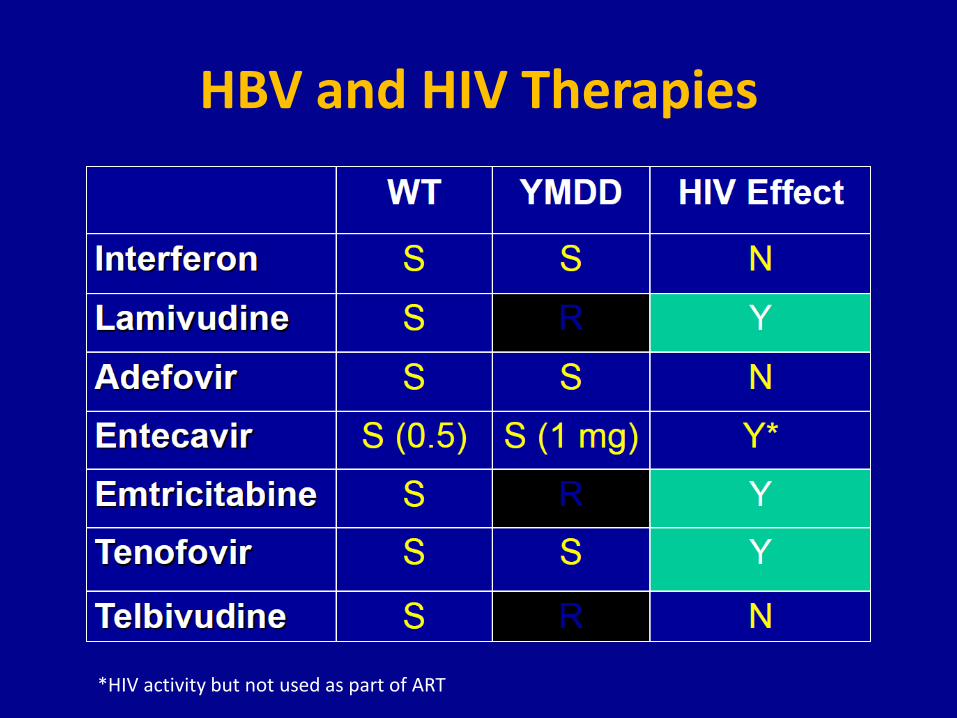
HBV and HIV Therapies
*HIV activity but not used as part of ART

Treatment Decisions in HBV-HIV Co-infected Patients
If meets criteria for HIV treatment:
• HBV DNA and ALT levels, HBeAg status have little to no role in decision-making
• Choose regimen that is effective against both HIV and HBV
If HIV does not need treatment:
• Decision to treat based on ALT and HBV DNA levels
• Options:
– Use drugs that have no activity against HIV
– Treat HIV and HBV simultaneously

Anti-HBV Therapy in HBV/HIV Co-infected Patients
* Not recommended if cirrhosis

HBV-HIV Summary
• HBV is dynamic disease - close monitoring needed
• Treat all cirrhotics, even if decompensated
• Always treat HBV if “active”
• Always treat HBV if treating HIV
• Monitor for response and make changes if
suboptimal virologic responses apparent
• ART interruptions: alternatives limited

Hepatitis B Treatment Summary
• HBV is controlled not cured
• Treatment targets individuals with active disease or advanced fibrosis
• Tenofovir, entecavir and peg-IFN are preferred drugs
• Risks-benefits of treatment need to be individualized
• Endpoints of treatment evolving - HBsAg is highly
desirable but infrequently obtained






























