Embed Size (px)
Citation preview

The Journal of Arthroplasty Vol. 23 No. 8 2008
Management of Extensor Mechanism Deficit as aConsequence of Patellar Tendon Loss in
Total Knee Arthroplasty
A New Surgical Technique
Rajesh Malhotra, MS (Orthopedics), Bhavuk Garg, MS (Orthopedics),Vivek Logani, MS (Orthopedics), and Surya Bhan, MS (Orthopedics), FRCS
Abstract: Extensor mechanism disruption is an uncommon but devastatingcomplication of total knee arthroplasty. A new technique of extensor mechanismreconstruction for patellar tendon loss, after total knee arthroplasty, with the help ofextensor mechanism composite allograft is described. Four patients with chronicextensor mechanism–deficient total knee arthroplasty were undertaken for revisionsurgery along with reconstruction of extensor mechanism with an innovativetechnique using an extensor mechanism composite allograft consisting of a patella–patellar tendon–tibial tubercle. On final follow-up, none of the patients had extensorlag but for 10° of extensor lag in 1 patient only. Providing an environment for bone-to-bone healing both proximally as well as distally and supervised postoperativerehabilitation led to encouraging results in the management of a failed extensormechanism after total knee arthroplasty. Key words: extensor mechanism, totalknee arthroplasty, allograft, extensor mechanism composite allograft.© 2008 Elsevier Inc. All rights reserved.
Extensor mechanism disruption is an uncommonyet devastating complication of total knee arthro-plasty. Its prevalence is 0.17% to 2.5% [1,2]. Theproblem seems multifactorial [3], and a spectrum ofsurgical procedures ranging from direct repair of theacute rupture [4,5] to the reconstruction of achronically deficient extensor mechanism has beenrecounted [6,7].
From the Department of Orthopaedics, All India Institute of MedicalSciences, New Delhi, India.
Submitted March 9, 2007; accepted August 8, 2007.No benefits or funds were received in support of the study.Reprint requests: Rajesh Malhotra, MS (Orthopedics), Depart-
ment of Orthopaedics, All India Institute of Medical Sciences,New Delhi, India.
© 2008 Elsevier Inc. All rights reserved.0883-5403/08/2308-0009$34.00/0doi:10.1016/j.arth.2007.08.011
1146
A unique solution to this problem of chronicextensor mechanism rupture/deficiency is recon-struction with the help of an extensor mechanismallograft. A fresh-frozen or freeze-dried allograftconsisting of quadriceps tendon, patella, patellartendon, and tibial tubercle is used as promoted byEmerson, Jr, et al [6,7]. Although the early clinicalresults were promising, further follow-up revealedthat an extensor lag of 20° to 40° had developed in 3of the 9 knees. The preceding technique wasmodified by Nazarian and Booth, Jr [8], so that theallograft be tightly tensioned in full extension.
All the aforementioned techniques bank on softtissue–to–soft tissue healing and have reportedattenuation of host donor junction, particularly atthe proximal host donor quadriceps junction, as themost common complication, resulting in poor out-come of these procedures. We describe an innovativetechnique of extensor mechanism reconstruction

Table 1. Clinical and Demographic Data
Patient 1 2 3 4Age (y) 68 71 63 69Sex Male Female Female FemaleExtensor lag (degrees) 40 45 40 30Other clinical findings Genu recurvatum Genu recurvatum Valgus laxity of 15°, genu recurvatum Genu recurvatumAssociated medical comorbidities Obese, hypertensive Rheumatoid arthritis Obese, hypothyroid, hypertensive DiabeticPrior surgical treatment Primary repair Primary repair Primary repair followed by
augmentation with semitendinosusPrimary repair
Postulated cause of patellartendon rupture
Extensive release Extensive release Distal realignment with lateral release Difficult exposure
Management of Extensor Mechanism Deficit as a Consequence of Patellar Tendon Loss � Malhotra et al 1147
with patella–patellar tendon–tibial tubercle allograftcounting exclusively on extrapolative bone-to-bonehealing, which is more predictable.
Materials and Methods
Consecutive reconstructions with extensormechanism allograft in 4 patients (3 women and 1man) were under taken by the surgeon (RM) in theinstitute. The clinical and demographic data of all 4patients are shown in Table 1.All knees had a failed extensor mechanism
associated with a total knee arthroplasty. Onepatient had a prior failed direct repair and again afailed extensor mechanism repair augmented bysemitendinosus autograft. The other 3 patients hadfailed primary repair. Nonoperative treatment,including bracing as well as other operative options,including additional attempt at direct repair and
Fig. 1. A and B, Intraoperative and schematic diagram showinundersurface of patella.
augmentation with tendon grafts, was discussedwith all of the patients. None of the patients hadclinical or laboratory evidence of infection.
On physical examination, the following variableswere recorded: active and passive range of motion,presence or absence of extensor lag, extensormechanism tracking, as well as neurovascularstatus. The tracking of the extensor mechanismduring range-of-motion testing was examined clo-sely and was found to be normal. There was no distalneurovascular deficit in any of the patients.
All but 1 patient had revision total knee arthro-plasty at the time of extensor mechanism recon-struction because of associated aseptic loosening orcomponent malrotation. Implants were retained,and the polyethylene was changed in the fourthpatient during extensor mechanism reconstruction.
The patients were observed for a mean of21 months, ranging from 14 to 30 months. Clinical
g preparation of donor allograft and creation of ridge on

Fig. 2. Intraoperative (A) and schematic diagram (B) showing creation of trough in host patella.
1148 The Journal of Arthroplasty Vol. 23 No. 8 December 2008
and radiographic examination was performed at 6and 12 weeks, 6 months, 1 year, and every yearthereafter. Active and passive range of motion,along with extensor lag, were recorded at an eachfollow-up. The knee was graded in accordance withthe 100-point system of the Hospital for SpecialSurgery (New York, NY), preoperatively and post-operatively, beginning at 3 months. A score of morethan 84 points is considered an excellent result; 70to 84 points, a good result; 60 to 69 points, a fairresult; and less than 60 points, a poor result.
Surgical TechniqueAllograft Preparation. Simultaneous with the
revision or placement of the total knee arthroplastycomponents, the patella–patellar tendon–tibialtubercle allograft was prepared on the back table.We first marked with a marking pen over the tibialtubercle and proximal part of the allograft tibia andplanned harvest of the allograft tibial bone block, ina rectangular fashion. With the use of a small thinmicrosagittal saw, the allograft block was harvestedfrom the allograft tibia, with careful attention so asnot to damage the allograft patellar tendon.Next, we cut the articular portion of patella in
such a way that a longitudinal ridge of bone
Fig. 3. Intraoperative (A) and schematic diagram
remained in the central portion, on either sideof which the cancellous surface was exposed(Fig. 1A and B).
Preparation of Host Patellar Trough
We divided the host patella in midline long-itudinally and removed some bone on either sidewith the help of an oscillating saw to create a troughof a width of 1 cm (Fig. 2A and B). The allograftpatella with a ridge created on its articular surfacewas then fitted/fixed into this trough (Fig. 3A and B)and secured with the help of screws insertedhorizontally, going from host bone to allograft tohost bone.
Preparation of the Host Proximal Tibial Trough
We created a trough in the proximal portion ofthe tibia as recommended [9,10]. The allografttibial tubercle was then inserted into the host tibialtrough and was gently press-fit with a bone tampor punch, in an “up and in” fashion, to lock thegraft in place. This graft was then secured with thehelp of wires. Once the allograft was secured,extensor mechanism tracking and strength waschecked and was found satisfactory.
(B) showing securing of allograft proximally.
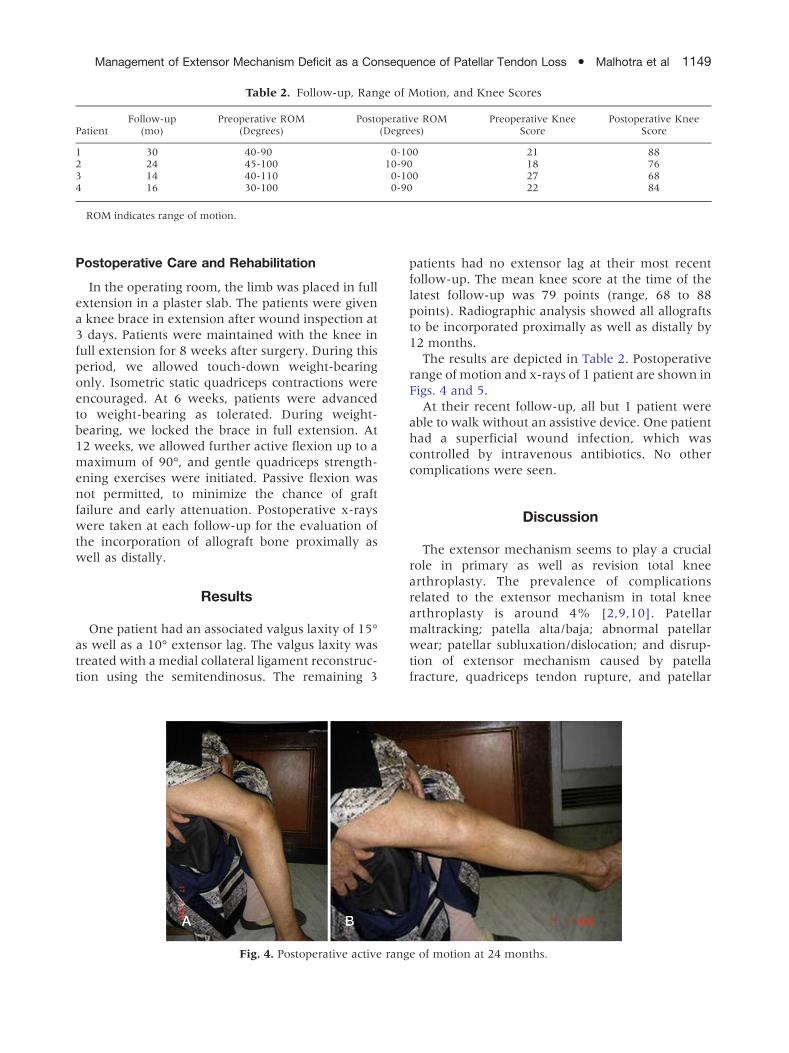
Table 2. Follow-up, Range of Motion, and Knee Scores
PatientFollow-up
(mo)Preoperative ROM
(Degrees)Postoperative ROM
(Degrees)Preoperative Knee
ScorePostoperative Knee
Score
1 30 40-90 0-100 21 882 24 45-100 10-90 18 763 14 40-110 0-100 27 684 16 30-100 0-90 22 84
ROM indicates range of motion.
Management of Extensor Mechanism Deficit as a Consequence of Patellar Tendon Loss � Malhotra et al 1149
Postoperative Care and Rehabilitation
In the operating room, the limb was placed in fullextension in a plaster slab. The patients were givena knee brace in extension after wound inspection at3 days. Patients were maintained with the knee infull extension for 8 weeks after surgery. During thisperiod, we allowed touch-down weight-bearingonly. Isometric static quadriceps contractions wereencouraged. At 6 weeks, patients were advancedto weight-bearing as tolerated. During weight-bearing, we locked the brace in full extension. At12 weeks, we allowed further active flexion up to amaximum of 90°, and gentle quadriceps strength-ening exercises were initiated. Passive flexion wasnot permitted, to minimize the chance of graftfailure and early attenuation. Postoperative x-rayswere taken at each follow-up for the evaluation ofthe incorporation of allograft bone proximally aswell as distally.
Results
One patient had an associated valgus laxity of 15°as well as a 10° extensor lag. The valgus laxity wastreated with a medial collateral ligament reconstruc-tion using the semitendinosus. The remaining 3
Fig. 4. Postoperative active rang
patients had no extensor lag at their most recentfollow-up. The mean knee score at the time of thelatest follow-up was 79 points (range, 68 to 88points). Radiographic analysis showed all allograftsto be incorporated proximally as well as distally by12 months.
The results are depicted in Table 2. Postoperativerange of motion and x-rays of 1 patient are shown inFigs. 4 and 5.
At their recent follow-up, all but 1 patient wereable to walk without an assistive device. One patienthad a superficial wound infection, which wascontrolled by intravenous antibiotics. No othercomplications were seen.
Discussion
The extensor mechanism seems to play a crucialrole in primary as well as revision total kneearthroplasty. The prevalence of complicationsrelated to the extensor mechanism in total kneearthroplasty is around 4% [2,9,10]. Patellarmaltracking; patella alta/baja; abnormal patellarwear; patellar subluxation/dislocation; and disrup-tion of extensor mechanism caused by patellafracture, quadriceps tendon rupture, and patellar
e of motion at 24 months.
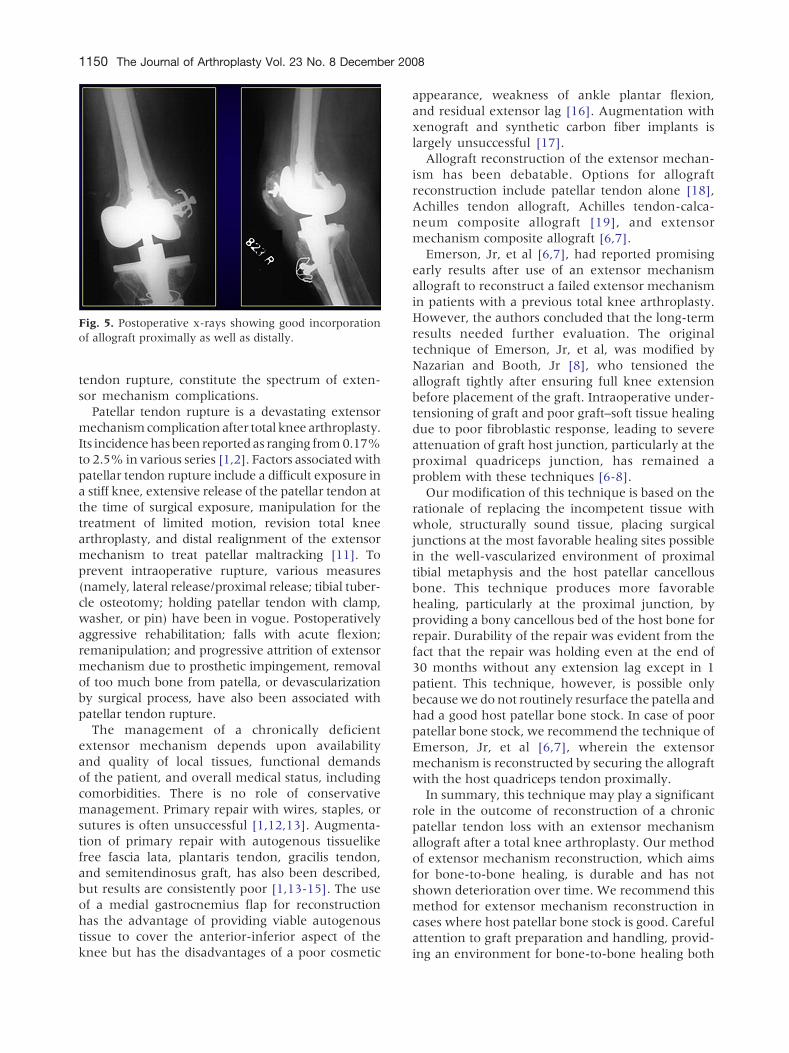
Fig. 5. Postoperative x-rays showing good incorporationof allograft proximally as well as distally.
1150 The Journal of Arthroplasty Vol. 23 No. 8 December 2008
tendon rupture, constitute the spectrum of exten-sor mechanism complications.Patellar tendon rupture is a devastating extensor
mechanismcomplication after total knee arthroplasty.Its incidencehas been reportedas ranging from0.17%to 2.5% in various series [1,2]. Factors associatedwithpatellar tendon rupture include a difficult exposure ina stiff knee, extensive release of the patellar tendon atthe time of surgical exposure, manipulation for thetreatment of limited motion, revision total kneearthroplasty, and distal realignment of the extensormechanism to treat patellar maltracking [11]. Toprevent intraoperative rupture, various measures(namely, lateral release/proximal release; tibial tuber-cle osteotomy; holding patellar tendon with clamp,washer, or pin) have been in vogue. Postoperativelyaggressive rehabilitation; falls with acute flexion;remanipulation; and progressive attrition of extensormechanism due to prosthetic impingement, removalof too much bone from patella, or devascularizationby surgical process, have also been associated withpatellar tendon rupture.The management of a chronically deficient
extensor mechanism depends upon availabilityand quality of local tissues, functional demandsof the patient, and overall medical status, includingcomorbidities. There is no role of conservativemanagement. Primary repair with wires, staples, orsutures is often unsuccessful [1,12,13]. Augmenta-tion of primary repair with autogenous tissuelikefree fascia lata, plantaris tendon, gracilis tendon,and semitendinosus graft, has also been described,but results are consistently poor [1,13-15]. The useof a medial gastrocnemius flap for reconstructionhas the advantage of providing viable autogenoustissue to cover the anterior-inferior aspect of theknee but has the disadvantages of a poor cosmetic
appearance, weakness of ankle plantar flexion,and residual extensor lag [16]. Augmentation withxenograft and synthetic carbon fiber implants islargely unsuccessful [17].
Allograft reconstruction of the extensor mechan-ism has been debatable. Options for allograftreconstruction include patellar tendon alone [18],Achilles tendon allograft, Achilles tendon-calca-neum composite allograft [19], and extensormechanism composite allograft [6,7].
Emerson, Jr, et al [6,7], had reported promisingearly results after use of an extensor mechanismallograft to reconstruct a failed extensor mechanismin patients with a previous total knee arthroplasty.However, the authors concluded that the long-termresults needed further evaluation. The originaltechnique of Emerson, Jr, et al, was modified byNazarian and Booth, Jr [8], who tensioned theallograft tightly after ensuring full knee extensionbefore placement of the graft. Intraoperative under-tensioning of graft and poor graft–soft tissue healingdue to poor fibroblastic response, leading to severeattenuation of graft host junction, particularly at theproximal quadriceps junction, has remained aproblem with these techniques [6-8].
Our modification of this technique is based on therationale of replacing the incompetent tissue withwhole, structurally sound tissue, placing surgicaljunctions at the most favorable healing sites possiblein the well-vascularized environment of proximaltibial metaphysis and the host patellar cancellousbone. This technique produces more favorablehealing, particularly at the proximal junction, byproviding a bony cancellous bed of the host bone forrepair. Durability of the repair was evident from thefact that the repair was holding even at the end of30 months without any extension lag except in 1patient. This technique, however, is possible onlybecausewe do not routinely resurface the patella andhad a good host patellar bone stock. In case of poorpatellar bone stock, we recommend the technique ofEmerson, Jr, et al [6,7], wherein the extensormechanism is reconstructed by securing the allograftwith the host quadriceps tendon proximally.
In summary, this technique may play a significantrole in the outcome of reconstruction of a chronicpatellar tendon loss with an extensor mechanismallograft after a total knee arthroplasty. Our methodof extensor mechanism reconstruction, which aimsfor bone-to-bone healing, is durable and has notshown deterioration over time. We recommend thismethod for extensor mechanism reconstruction incases where host patellar bone stock is good. Carefulattention to graft preparation and handling, provid-ing an environment for bone-to-bone healing both

Management of Extensor Mechanism Deficit as a Consequence of Patellar Tendon Loss � Malhotra et al 1151
proximally as well as distally and supervised post-operative rehabilitation, led to encouraging resultsin the management of a failed extensor mechanismafter total knee arthroplasty. However, a moreextensive and long-term study involving morepatients is needed to authenticate the success inaddressing this complex problem.
References
1. Rand JA, Morrey BF, Bryan RS. Patellar tendonrupture after total knee arthroplasty. Clin Orthop1989;244:233.
2. Lynch AF, Rorabeck CH, Bourne RB. Extensormechanism complications following total knee arthro-plasty. J Arthroplasty 1987;2:135.
3. Parker DA, Dunbar MJ, Rorabeck CH. Extensormechanism failure associated with total knee arthro-plasty: prevention and management. J Am AcadOrthop Surg 2003;11:238.
4. Ecker ML, Lotke PA, Glazer RM. Late reconstructionof the patellar tendon. J Bone Joint Surg Am 1979;61:884.
5. Larsen E, Lund PM. Ruptures of the extensor mechan-ism of the knee joint. Clinical results and patellofemoralarticulation. Clin Orthop 1986;213:150.
6. Emerson Jr RH, Head WC, Malinin TI. Reconstructionof patellar tendon rupture after total knee arthro-plasty with an extensor mechanism allograft. ClinOrthop 1990;260:154.
7. Emerson Jr RH, Head WC, Malinin TI. Extensormechanism reconstruction with an allograft after totalknee arthroplasty. Clin Orthop 1994;303:79.
8. Nazarian DG, Booth Jr RE. Extensor mechanismallografts in total knee arthroplasty. Clin Orthop 1999;367:123.
9. MacCollum MS, Karpman RR. Complications of thePCA anatomic patella. Orthopedics 1989;12:1423.
10. Doolittle KH, Turner RH. Patellofemoral problemsfollowing total knee arthroplasty. Orthop Rev 1988;17:696.
11. Rand JA. Extensor mechanism complications follow-ing total knee arthroplasty. J Bone Joint Surg Am2004;86:2062.
12. Grace JN, Rand JA. Patellar instability after total kneearthroplasty. Clin Orthop 1988;237:184.
13. Abril JC, Alvarez L, Vallejo JC. Patellar tendonavulsion after total knee arthroplasty. A new techni-que. J Arthroplasty 1995;10:275.
14. Cadambi A, Engh GA. Use of a semitendinosus tendonautogenous graft for rupture of the patellar ligamentafter total knee arthroplasty. A report of seven cases.J Bone Joint Surg Am 1992;74:974.
15. Wilson FC, Venters GC. Results of knee replacementwith the Walldius prosthesis: an interim report. ClinOrthop 1976;120:39.
16. Jaureguito JW, Dubois CM, Smith SR, et al. Medialgastrocnemius transposition flap for the treatment ofdisruption of the extensor mechanism after totalknee arthroplasty. J Bone Joint Surg Am 1997;79:866.
17. Jenkins DH, McKibbin B. The role of flexible carbon-fibre implants as tendon and ligament substitutes inclinical practice. A preliminary report. J Bone JointSurg Br 1980;62-B:497.
18. Zanotti RM, Freiberg AA, Matthews LS. Use of patellarallograft to reconstruct a patellar tendon-deficientknee after total joint arthroplasty. J Arthroplasty1995;10:271.
19. Crossett LS, Sinha RK, Sechriest VF, et al. Reconstruc-tion of a ruptured patellar tendon with Achillestendon allograft following total knee arthroplasty.J Bone Joint Surg Am 2002;84:1354.


![Imaging Patellar Complications After Knee Arthroplasty · ing axial radiograph to better assess patellofemoral kinematics. [2-3] Although radiographs are the mainstay in evaluating](https://img.dokumen.tips/doc/110x75/5faeb6201161442eea6324ec/imaging-patellar-complications-after-knee-arthroplasty-ing-axial-radiograph-to-better.jpg)


























