Embed Size (px)
Citation preview

Current Concepts Review
Management of Articular CartilageDefects of the Knee
By Asheesh Bedi, MD, Brian T. Feeley, MD, and Riley J. Williams III, MD
� Articular cartilage has a poor intrinsic capacity for healing. The goal of surgical techniques to repair articularcartilage injuries is to achieve the regeneration of organized hyaline cartilage.
� Microfracture and other bone marrow stimulation techniques involve penetration of the subchondral plate in orderto recruit mesenchymal stem cells into the chondral defect. The formation of a stable clot that fills the lesion is ofparamount importance to achieve a successful outcome.
� Mosaicplasty is a viable option with which to address osteochondral lesions of the knee and offers the advantageof transplanting hyaline cartilage. However, limited graft availability and donor site morbidity are concerns.
� Transplantation of an osteochondral allograft consisting of intact, viable articular cartilage and its underlyingsubchondral bone offers the ability to address large osteochondral defects of the knee, including those involvingan entire compartment.
� The primary theoretical advantage of autologous chondrocyte implantation is the development of hyaline-likecartilage rather than fibrocartilage in the defect, which presumably leads to better long-term outcomes and lon-gevity of the healing tissue.
� Use of synthetic scaffolds is a potentially attractive alternative to traditional cartilage procedures as they arereadily available and, unlike allogeneic tissue transplants, are associated with no risk of disease transmission.Their efficacy, however, has not been proven clinically.
The management of articular cartilage defects continues to beone of the most challenging clinical problems for orthopaedicsurgeons. Articular cartilage is a highly organized tissue withcomplex biomechanical properties and substantial durability1.However, it has a poor intrinsic capacity for healing, anddamage from trauma or degeneration can result in morbidityand functional impairment2. Untreated lesions can lead todebilitating joint pain, dysfunction, and degenerative arthritis.
Cartilage repair strategies include debridement; bonemarrow stimulation; and cell-based, cell plus scaffold-based,and whole-tissue transplantation techniques3. In this review,we discuss the basic science, indications, advantages, short-comings, and outcomes of each of these interventions in orderto provide an evidence-based assessment for the treatment ofthese conditions.
Bone Marrow Stimulation: MicrofractureBone marrow stimulation is the most frequently used techniquefor treating small symptomatic lesions of the articular cartilagein the knee. These procedures are technically straightforward,and the costs are low compared with those of other treatmentmodalities. Bone marrow stimulation techniques involve per-foration of the subchondral plate in order to recruit mesen-chymal stem cells from the bone marrow space into the lesion4,5.The mesenchymal stem cells are able to differentiate into fi-brochondrocytes, which contribute to fibrocartilage repair ofthe lesion. However, the overall concentration of the mesen-chymal stem cells is quite low and declines with age6. Theformation of a stable blood clot that maximally fills thechondral defect is important, and it has been correlated withthe success of bone marrow stimulation procedures7. Unstable
Disclosure: The authors did not receive any outside funding or grants in support of their research for or preparation of this work. Neither they nor a memberof their immediate families received payments or other benefits or a commitment or agreement to provide such benefits from a commercial entity.
994
COPYRIGHT � 2010 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
J Bone Joint Surg Am. 2010;92:994-1009 d doi:10.2106/JBJS.I.00895

clots that are only partially adherent to or fill only a portion ofthe defect will result in suboptimal repair7.
Reparative fibrocartilage consists of type-I, type-II, andtype-III collagen in varying amounts8,9. The fibrocartilage doesnot resemble the surrounding hyaline cartilage and has lesstype-II collagen. Unlike other cartilage restoration techniques,bone marrow stimulation does not involve transfer of chon-drocytes into the lesion.
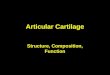
Creating a contained lesion is critical to achieving astable base for filling the defect with a clot and adhesion of theclot. If the lesion is not shouldered by a stable rim of healthycartilage, achieving a stable clot may be more difficult10-12. Thecalcified cartilage layer at the base of the lesion must be re-moved as well (Figs. 1-A through 1-D). Removal of this layer isimportant for clot adhesion and the ultimate success of themicrofracture technique13. The prepared channels must be ofsufficient depth to ensure penetration of the subchondral plateand communication with the marrow. Fatty droplets should beseen to emanate from the channel apertures to confirm thatadequate depth has been achieved.
The postoperative regimen after bone marrow stimula-tion procedures is demanding and has been reported to be acritical aspect of the ultimate efficacy14. Patients with a femoralcondylar lesion are initially treated with continuous passivemotion with a 0� to 60� range of motion for six weeks post-operatively15. Studies have shown that continuous passivemotion improves cartilage nutrition and stimulates mesen-chymal stem-cell differentiation16-19. The patient typically re-mains non-weight-bearing with the use of crutches for sixweeks. Patients who have undergone microfracture of a pa-tellar or trochlear defect are allowed to bear weight as toleratedpostoperatively, but knee motion is restricted from 0� to 40� ina brace20,21. Continuous passive motion is initiated immediatelyand used, within this arc of motion, for approximately six toeight hours daily. At two months, unrestricted motion is typ-ically allowed and closed-chain exercises are initiated. Short-arcclosed-chain concentric and eccentric muscle strengthening iseffective and protects the patellofemoral articulation. Typically,a return to full activities is permitted at three months after afull, painless range of motion is achieved20,21.
Outcomes (See Appendix)Steadman et al. reported what we believe to be the first long-term follow-up study of microfracture, in which seventy-oneknees were followed for an average of eleven years20. The pa-tients all had a traumatic full-thickness chondral defect, had nomeniscal or ligament injury, and were less than forty-five yearsof age. At the time of final follow-up, the patients had signif-icant improvement in multiple clinical outcome measures (p <0.02). The authors found that age was an independent pre-dictor of functional improvement. Mithoefer et al. performed aprospective study of forty-eight patients (mean age, forty-twoyears) a mean of 3.6 years following the operation22. Most ofthe lesions (52%) were between 1 and 4 cm2. Overall, kneefunction was good to excellent in thirty-two (67%) of theforty-eight patients, fair in twelve (25%), and poor in four
(8%). The authors found that a lower body mass index cor-related with better outcomes. Magnetic resonance imagingshowed that 54% of the patients had good fill with repairtissue, 29% had moderate fill, and 17% had poor fill. The gradeof fill on magnetic resonance imaging correlated with betterclinical outcomes12.
Microfracture has been compared with other cartilagerestoration procedures in multiple well-designed, randomizedstudies. Knutsen et al. compared autologous chondrocyteimplantation with microfracture in eighty patients with anaverage age of 32.2 years23. The average lesion size was 4.8 cm2.After two years of follow-up, both groups had significantclinical improvement (p < 0.05). The Short Form-36 (SF-36)score, however, was significantly better in the microfracturegroup (p = 0.004). Histological assessment demonstratedhyaline-like or mixed hyaline/fibrocartilage-like tissue in 29%of the patients in the microfracture group and 50% of those inthe group treated with autologous chondrocyte implantation.There was, however, a 23% failure rate with both procedures.
Gudas et al. compared the outcomes of osteochondralautologous transplantation with those of microfracture inyoung athletes in a randomized, controlled study 24. Fifty-sevenpatients (twenty-eight treated with osteochondral autologoustransplantation and twenty-nine treated with microfracture)were available at the time of final follow-up. The average agewas 24.3 years, and the average lesion size was 2.8 cm2 (range,1 to 4 cm2). At a mean of thirty-seven months postoperatively,both groups had substantial clinical improvement. However,on the basis of Hospital for Special Surgery (HSS) and Inter-national Cartilage Repair Society (ICRS) scores, 96% had agood-to-excellent result after the osteochondral autologoustransplantation compared with 52% after the microfractureprocedure. Biopsy specimens were obtained from 58% of thepatients and histological evaluation of repair showed betterICRS scores for the group treated with osteochondral autolo-gous transplantation. In addition, subjective evaluation of le-sion fill, osseous incorporation, and surface congruency withmagnetic resonance imaging showed good-to-excellent repairin 94% of the patients treated with osteochondral autologoustransplantation compared with only 49% of those treated withmicrofracture. Twenty-six (93%) of the patients treated withosteochondral autologous transplantation and fifteen (52%) ofthose treated with microfracture returned to sports activities attheir preinjury level at an average of 6.5 months. The authorsconcluded that osteochondral autologous transplantation wasclinically superior to microfracture for the treatment of car-tilage lesions in patients under the age of forty years.
Several recent studies have focused on the outcomes ofmicrofracture in high-level athletes. Steadman et al. reviewedthe outcomes in twenty-five active National Football League(NFL) players at an average 4.5 years after they underwentmicrofracture to treat a full-thickness chondral lesion15.Nineteen players (76%) returned to football the season fol-lowing the microfracture. The athletes who returned to foot-ball played an average 4.6 seasons (range, one to thirteenseasons) and fifty-six games (range, two to 183 games) after the
995
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

procedure. Gobbi et al.25 reviewed the results in fifty-threeathletes (twenty-six professional and twenty-seven recrea-tional) with a mean age of thirty-eight years and a mean lesionsize of 4 cm2. At six years following the microfracture surgery,the International Knee Documentation Committee (IKDC)score26 was normal or nearly normal in 70% of the patients andthe Tegner score27,28 had increased from 3.2 to 5.0 points. Theauthors found that an age of less than forty years, lesions of<2 cm2, preoperative symptoms of less than twelve months’duration, and no prior operative intervention were associatedwith a better return to high-impact sports. Cerynik et al.29
reported on changes in efficiency ratings for twenty-four
professional basketball players who had undergone micro-fracture surgery. The mean time until they returned to play wasthirty weeks. Twenty-one percent were unable to return tocompetition. Similarly, Namdari et al. reported the outcomesfor twenty-four professional basketball players who had un-dergone microfracture for the treatment of a chondral lesion ofthe knee30. Eight of these athletes were unable to return to play,and those who did return to competition had a significantreduction in the number of points scored (p = 0.008) andminutes played (p = 0.045) postoperatively, although the au-thors found no difference in performance variables that hadbeen averaged over forty minutes of play.
Fig. 1-A Fig. 1-B
Fig. 1-C Fig. 1-D
Figs. 1-A through 1-D Reproduced, with modification, from: Mithoefer K, Williams RJ 3rd, Warren RF, Potter HG, Spock CR, Jones EC, Wickiewicz TL, Marx
RG. Chondral resurfacing of articular cartilage defects in the knee with the microfracture technique. Surgical technique. J Bone Joint Surg Am. 2006;88
Suppl 1(Pt 2):294-304. Figs. 1-A and 1-B Creation of a well-shouldered lesion is critical to achieve a stable base for filling of the defect with a clot and
adhesion of the clot after microfracture. The calcified cartilage layer at the base of the lesion must be removed to allow clot adhesion13. Figs. 1-C and 1-D
The prepared channels must be of sufficient depth to ensure penetration of the subchondral plate and communication with the marrow.
996
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

Proper patient selection and meticulous attention totechnical detail are critical to achieving a successful outcomefollowing microfracture. Several studies have documentedbetter outcomes in younger patients12,31. Kreuz et al. comparedthe results of microfracture in eighty-five consecutive patientsand found that patients less than forty years of age had sig-nificantly better results than those over forty (p < 0.01)31.Older patients had evidence of deterioration of the healingcartilage on magnetic resonance imaging as early as eighteenmonths after the operation. Osseous overgrowth has beenfound to occur after errant removal of the subchondral boneduring the microfracture procedure. Osseous overgrowth iscommon, occurring in 25% to 49% of patients22,32, and canlead to adverse biological and biomechanical outcomes.
Even with meticulous operative technique and properpatient selection, the results of microfracture appear to dete-riorate over time. Mithoefer et al. found that, despite the initialimprovement in clinical outcomes, the results deterioratedover time in 47% of elite athletes12,33. Similar results have beenfound in other studies as well25. Thus, although microfractureis a straightforward technique that is commonly employed as afirst-line treatment for small cartilage lesions, the results arenot as good in older patients and tend to deteriorate over time.
Adjuncts to Bone Marrow StimulationAdjuncts to improve the stability of the clot and the lesion fillwith marrow stimulation procedures have been described.Hoemann et al. demonstrated that stabilization of the bloodclot through the addition of chitosan, a thrombogenic andadhesive polymer, resulted in improved lesion fill, cellularorganization, and biochemical composition of healing tissuecompared with those variables after microfracture alone in anovine model34. Growth factors used as biological augments toin vivo cartilage repair have been studied as well. Insulin-likegrowth factor placed into fibrin clots in an equine chondraldefect model improved both the quantity and the quality ofcartilage repair tissue and reduced the severity of postoperativeinflammation35,36. Platelet-derived growth factor is another po-tent mitogen for mesenchymal cells, and preliminary studieshave demonstrated promising results with respect to its abil-ity to stimulate hyaline cartilage formation and chondrocyteproliferation37,38.
Hyaluronic acid viscosupplementation has also recentlybeen evaluated as an adjunct to microfracture for chondrallesions of the knee. Strauss et al. evaluated the results of mi-crofracture of focal medial femoral condylar defects with andwithout viscosupplementation in a New Zealand White rabbitmodel39. At three months postoperatively, gross and histolog-ical examination of the repair tissue revealed better fill andmore hyaline-like tissue compared with controls. In addition,at the final, six-month follow-up evaluation, the knees that hadreceived viscosupplementation were observed to have less de-generative change than controls. However, adjuncts to bonemarrow stimulation have not been tested in clinical trials ofpatients, and therefore their clinical efficacy remains unprovenat this time.
Platelet-Rich PlasmaThere has been a remarkable increase in the use of platelet-richplasma to facilitate healing in a variety of pathological muscu-loskeletal conditions. The theoretical advantage of this autolo-gous blood product rests in the concentrated platelets andassociated quantity of platelet-derived growth factor and othermitogenic factors that may promote the healing of chondralinjuries. Sun et al. compared the efficacy of platelet-rich plasmadelivered in a poly-lactic-co-glycolic acid (PLGA) scaffold withthat of the scaffold alone in a rabbit osteochondral defect modeland noted improved bone formation and histological charac-teristics of the cartilage repair tissue in the platelet-rich plasma-treated specimens40. Furthermore, Mishra et al. demonstrated,in in vitro studies, that platelet-rich plasma increases mesen-chymal stem cell proliferation and chondrogenic differen-tiation41. Akeda et al. similarly demonstrated increased cellproliferation and proteoglycan and collagen production byadult porcine chondrocytes cultured in platelet-rich plasma-augmented media42. Despite these encouraging preliminaryresults, however, no clinical studies have proven the efficacy ofplatelet-rich-plasma injection for focal chondral injuries of theknee, to our knowledge.
Whole-Tissue TransplantationAutologous Osteochondral TransplantationAutologous osteochondral mosaicplasty, sometimes referred toas OATS (osteoarticular transfer system), is an effective methodfor resurfacing osteochondral defects of the knee. The techniqueinvolves transplantation of multiple small cylindrical autoge-nous osteochondral plugs harvested from the less weight-bearing periphery of the articular surface of the femoralcondyle and transferred to create a congruent and durableresurfaced area in the defect (Figs. 2-A, 2-B, and 2-C). Theprocedure offers several advantages over other repair tech-niques, including transplantation of viable hyaline cartilage, arelatively brief rehabilitation period, and the ability to performthe procedure in a single operation.
The limitations of autologous osteochondral mosaic-plasty include donor site morbidity and a limited availabilityof graft that can be harvested from the patellofemoral jointor the zone adjacent to the intercondylar notch. Other po-tential limitations include differences in orientation, thick-ness, and mechanical properties between donor and recipientcartilage as well as graft subsidence at the surface with post-operative weight-bearing. In addition, absence of fill and thepotential dead space between cylindrical grafts may limit thequality and integrity of the repair. Lane et al. transplantedautologous osteochondral grafts into the knee joints of goatsand found a lack of integration of the cartilage, resulting inthe persistence of full-thickness gaps in all specimens43. Amagnetic resonance imaging analysis in a clinical settingsimilarly demonstrated a failure of chondral integration, al-though there was good osseous integration of the subchondralbone44.
Donor site healing by natural processes results in filling ofthe defects with cancellous bone and an overlying fibrocartilage-
997
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

like cap. However, larger grafts are associated with greaterdonor site morbidity. It has been suggested that, when graftswith a diameter of >8 mm are harvested, filling of the defectwith biocompatible material may help to prevent morbidity atthe donor site45. Feczko et al. evaluated healing of donor sitedefects treated with hydroxyapatite, carbon fiber, polyglyconateB, compressed collagen, and two versions of polycaprolactonesin a canine model45. While all of these substitutes demonstratedgood integration with the surrounding cancellous bone, onlylimited repair-tissue formation was evident even at thirty weekspostoperatively. Compressed collagen, however, yielded themost favorable fibrocartilage covering as seen on second-lookarthroscopy and histological evaluation.
The effect of surface plug incongruity on articularsurface contact pressures has been evaluated. Koh et al. as-sessed contact pressures with controlled axial loads on swineknees with variable plug positions46. The study demonstratedthat flush or slightly sunk grafts could restore contact pressuresto nearly normal levels, but that elevated angled grafts ad-versely increased contact pressures. The authors also demon-strated that grafts seated 0.5 to 1 mm proud relative to theadjacent surface resulted in a 50% increase in mean contactpressures47.
The biomechanical stability of the plug after autologousosteochondral transplantation is important and is affected byseveral technical factors. In experimental models, osseous in-
Fig. 2-A Fig. 2-B
Fig. 2-C
Figs. 2-A, 2-B, and 2-C Reprinted from: Hangody L,
Rathonyi GK, Duska Z, Vasarhelyi G, Fules P, Modis L.
Autologous osteochondral mosaicplasty. Surgical
technique. J Bone Joint Surg Am. 2004;86 Suppl 1:65-
72. Fig. 2-A Schematic drawing demonstrating the
autologous osteochondral transplantation technique. A
chisel can be used to harvest osteochondral plugs from
the blue-shaded regions along the margins of the
trochlea or adjacent to the notch. Fig. 2-B The donor
region along the trochlear margin can be accessed
through a small arthrotomy and visualized with the knee
in extension. Fig. 2-C Flexion of the knee can expose
the recipient chondral defect through the same expo-
sure and allow placement of grafts in the desired
configuration to fill the lesion.
998
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

tegration of the graft and recipient has been observed at fourweeks48. Prior to this healing, the press-fit mechanism is criticalfor maintaining a stable graft position. Plugs of a matcheddepth (i.e., with the donor plug length and recipient defectlength matched) are more stable than short plugs (i.e., with acavity left at the bottom of the defect), which rely exclusivelyon circumferential frictional forces for stability49. This stabilityof short plugs is further compromised in multiple plug con-figurations in which gaps between the round plugs and sur-rounding bone reduce frictional forces50.
The effect of impact loading of the hyaline cartilageduring delivery of the osteochondral plug has been evaluated.Chondrocyte viability is critical, as each cell maintains adiscrete maximum volume of robust matrix around it51,52.Whiteside et al. demonstrated that the percentage of chon-drocyte death was predicted more strongly by the mean forceof impact than by the number of impacts required duringplacement of the graft48. Huntley et al. identified a markedmarginal zone of cell death with a thickness of ;400 mm atthe plug periphery within two hours after harvesting53. Usinga planar model for mosaicplasty, they demonstrated thatapproximately one-third of the mosaicplasty surface wasnonviable (secondary to the 24% rate of marginal zone celldeath and 9% rate of interposed dead space between grafts).Gulotta et al. recently corroborated these findings of chon-drocyte necrosis, apoptosis, and matrix degradation afterpress-fit osteochondral autograft implantation in a rabbitmodel54.
Outcomes (See Appendix)The outcomes of autologous mosaicplasty for symptomaticchondral defects have been encouraging, and the procedurehas been used with success2,55-57. Hangody and Fules evaluatedthe largest series of mosaicplasties (831) performed for local-ized Outerbridge grade-III or IV chondral lesions58 and re-ported good-to-excellent results for 92% of femoral lesions,87% of tibial lesions, and 79% of patellofemoral lesions58. Therate of donor site morbidity, as assessed with the Bandi score58,was 3%. Eighty percent of the second-look arthroscopic pro-cedures performed in eighty-five patients demonstrated con-gruent gliding surfaces and histological evidence of transplantedhyaline cartilage. Ozturk et al. reported on the clinical andradiographic outcomes of nineteen patients with a grade-IVchondral lesion treated with mosaicplasty 59. The mean Lys-holm score27,28 improved from 46 points preoperatively to 88points postoperatively, with an 85% rate of good-to-excellentresults after a mean duration of follow-up of thirty-two months.Magnetic resonance imaging revealed excellent fill and con-gruency of <1 mm without fissuring or delamination in 84%of the cases.
Authors of recent studies have also reported on thesuccessful use of autologous osteochondral grafts for the sta-bilization and healing of unstable osteochondritis dissecanslesions60,61. Twenty patients were assessed arthroscopically, andthe lesions were fixed in situ with use of multiple 4.5-mmosteochondral dowel grafts61. All knees were scored as clinically
normal by eighteen months, and serial magnetic resonanceimages demonstrated healing of the osseous lesion in all casesby six months and with a continuous articular cartilage surfaceby nine months.
The use of autologous osteochondral transplantation forthe treatment of symptomatic, isolated patellar chondral le-sions has recently been evaluated. Nho et al. retrospectivelyevaluated twenty-two patients (mean age, thirty years) fol-lowed for a mean of twenty-five months after plug trans-plantation62. Nine patients underwent a concomitant distalpatellar realignment procedure for the treatment of associatedinstability. The mean defect size was 1.66 cm2, and the meandonor plug size was 9.7 mm in diameter. An average of 1.8plugs were placed in each defect. The mean IKDC score26
improved from 47.2 points preoperatively to 74.4 pointspostoperatively. Magnetic resonance imaging performed at thetime of final follow-up revealed nearly complete or completefill in all plugs, with 71% being completely incorporated andflush with the adjacent hyaline cartilage.
The efficacy of mosaicplasty has been compared withthat of autologous chondrocyte implantation in some series.Two randomized, prospective studies comparing mosaicplastywith autologous chondrocyte implantation demonstrated a90% rate of good-to-excellent results in the autologous os-teochondral transplantation group and more rapid improve-ment with osteochondral autologous transplantation than withautologous chondrocyte implantation63. A small randomizedcontrolled trial of forty-seven patients assigned to receive au-tologous chondrocyte implantation or mosaicplasty after aninitial arthroscopic assessment and debridement of a focalchondral lesion was performed by Dozin et al.63. The study,which had limited power, demonstrated clinically equivalentoutcomes in the two groups. Interestingly, one-third of thepatients had spontaneous improvement after debridementalone, raising some concern regarding the efficacy of eitherintervention.
Osteochondral Allograft TransplantationOsteochondral allograft transplantation is a cartilage resur-facing procedure that involves transplantation of a cadavergraft consisting of intact, viable articular cartilage and its un-derlying subchondral bone into the defect. The size, depth, andlocation of the defect are all critical factors in the tailoring ofthe donor graft. Advantages to the use of osteochondral allo-grafts include the ability to achieve precise surface architecture,immediate transplantation of viable hyaline cartilage as asingle-stage procedure, the potential to replace large defects oreven hemicondyles, and no donor site morbidity. Use of a largedowel osteochondral transplant in this capacity (Figs. 3-A and3-B) eliminates the dead space that is encountered between thesmaller cylindrical grafts that are used with autologous mo-saicplasty. Limitations of osteochondral allografting includelimited graft availability, high cost, risk of immunological re-jection, possible incomplete graft incorporation, potential fordisease transmission, and the technically demanding aspects ofmachining and sizing of the allograft64.
999
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

Fresh AllograftsFresh osteochondral allografts are typically utilized, as freezingand cryopreservation have both been shown to decreasechondrocyte viability. Although the critical threshold of viablechondrocytes necessary to achieve clinical success remainsunknown, chondrocyte function is critical to maintain thedynamic homeostasis of the extracellular matrix and is animportant factor in ensuring long-term allograft survivalin vivo65,66. Traditionally, grafts have been harvested, stored in
lactated Ringer solution at 4�C, and transplanted within oneweek. Recently, there has been a shift toward allograft storagein culture medium67. At fourteen days, specimens stored inlactated Ringer solution demonstrated an 80% rate of chon-drocyte viability compared with a 91% rate for those stored inculture medium68. This is particularly important in the settingof modern tissue-banking procedures for microbiologicalscreening and recipient matching, which have necessitatedprolonged periods of storage prior to implantation.
Fig. 3-A Fig. 3-B
Fig. 3-C
Figs. 3-A, 3-B, and 3-C Reprinted from: Williams RJ 3rd, Ranawat
AS, Potter HG, Carter T, Warren RF. Fresh stored allografts for the
treatment of osteochondral defects of the knee. J Bone Joint
Surg Am. 2007;89:718-26. Fig. 3-A Harvesting of an os-
teochondral allograft dowel from a hemicondylar specimen with
the size and radius of curvature matched to the recipient. Fig. 3-B
Implantation with circumferential flush congruity at the recipient
site for the treatment of an osteochondritis dissecans lesion of
the femoral condyle. Corresponding pen marks are made at the
12 o’clock, 4 o’clock, and 8 o’clock positions in an effort to
optimally match the orientation and surface congruity between
the donor graft and the recipient defect. Fig. 3-C Sagittal fast
spin-echo magnetic resonance image made at twenty-four
months after implantation of the osteochondral allograft. There
is excellent lesion fill and congruency with the adjacent native
cartilage interface. The graft demonstrates articular cartilage
signal (arrow) that is isointense compared with the native hyaline
cartilage.
1000
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

The matrix properties and chondrocyte viability ofstored fresh osteochondral allografts have been evaluated.Allen et al.69 demonstrated preserved biomechanical andmatrix characteristics but decreased chondrocyte density andmetabolic activity in specimens stored for twenty-one daysbefore implantation. The superficial zone of cartilage wasmost severely affected. Pearsall et al. studied sixteen refrig-erated allografts and reported progressively less matrixstaining with prolonged refrigeration and a mean chondro-cyte viability rate of 67% at an average of thirty days70. Al-though the biomechanical properties and matrix integrity ofhyaline cartilage are preserved for up to twenty-eight days,the number of viable chondrocytes has been shown to de-crease progressively over that time71. Nonetheless, the rate ofchondrocyte viability was approximately 50% at sixty days,which may represent a potentially longer window for suc-cessful implantation.
A number of studies have confirmed the long-term sur-vival of donor chondrocytes after transplantation68,72-74. Hyalinecartilage is a relatively immunoprivileged tissue with an avas-cular matrix that shields donor chondrocytes from the hostimmune reaction. Williams et al. reported on twenty-six re-trieved osteochondral allograft specimens after an average sur-vival time of forty-two months75. The rate of chondrocyteviability was 82%, and there was evidence of allograft boneincorporation in most specimens. The allograft bone is necroticand is replaced by creeping substitution, but it provides astructural scaffold to support the articular surface during thisgradual incorporation.
Cryopreserved AllograftsCryopreservation involves rate-controlled freezing of speci-mens in a nutrient-rich, cryoprotectant medium (glycerol ordimethyl sulfoxide) to minimize cellular freezing and maintaincell viability. Recently, Gole et al. found a 77% rate of chon-drocyte viability at one year in cryopreserved osteochondralallografts implanted into load-bearing sites in an animalmodel76. However, another study demonstrated degenerativechanges at the articular surface of cryopreserved allograftscompared with fresh allografts at five years65. A study of anovine model by Schachar et al. demonstrated that the mem-brane integrity of the allograft chondrocytes immediately fol-lowing cryopreservation is the most reliable predictor of thelong-term outcome of the graft77. Use of cryopreserved allo-grafts achieved an overall intermediate result compared withthe results associated with the use of fresh autografts (thepositive controls in the study).
Fresh-Frozen AllograftsFresh-frozen preservation of allografts offers the advan-tages of reduced immunogenicity and decreased diseasetransmission at the expense of reduced chondrocyte via-bility. The process of deep freezing to 280�C destroys theviability of all articular cartilage cells within the graft78, andretrieval studies have demonstrated deterioration of cells andmatrix over time79.
Outcomes (See Appendix)A number of retrospective studies have been performed toassess the outcomes of osteochondral allograft transplantationfor the treatment of focal osteochondral defects of the knee,and they have demonstrated good-to-excellent results. Chuet al. reported on fifty-five knees at a mean of six years aftertransplantation of fresh osteochondral allografts80. Eighty-fourpercent of the knees treated for an isolated focal defect wererated as having a good-to-excellent outcome with use of theMerle d’Aubigne and Postel scale81, while similar success wasachieved in only 50% of the knees that had undergone trans-plantation for the treatment of bipolar lesions (i.e., articulatingchondral defects on both the tibial and the femoral side).Ghazavi et al. reported the results at a mean of 7.5 years fol-lowing 126 procedures for the transplantation of fresh os-teochondral allografts for the treatment of posttraumaticcondylar defects82. While a good-to-excellent result was achievedin 85% of the knees, an increased rate of failure was seenin the setting of bipolar lesions and limb malalignment andin patients insured by Workers’ Compensation. Bugbee andConvery reported the outcomes at a mean of fifty monthsafter the use of fresh osteochondral allografts in ninety-sevenknees83. An 86% success rate was achieved in the treatment oflarge unipolar defects (mean size, 8 cm2), whereas only a 54%success rate was seen after the management of bipolar lesions.Other factors contributing to failure in this series includeddiffuse arthritis, inflammatory conditions, and lower-extremitymalalignment. Davidson et al. reported on sixty-seven patientswho had received an osteochondral allograft for the treatmentof a symptomatic femoral chondral lesion84. At a mean of fortymonths postoperatively, significant improvements in both theIKDC26 and the SF-36 scores, as compared with the preoper-ative scores, were noted (p = 0.002). So-called second-lookarthroscopy was performed in ten knees and revealed repairtissue that was grossly similar to native cartilage with a per-sistence of a small seam surrounding the cylindrical grafts.Chondrocyte viability and density in the repair tissue did notdiffer from those of native (control) cartilage retrieved withbiopsy. Overall, these studies indicate that, while allografttransplantation is largely successful when done for appropriateindications, outcomes are less reliable and predictable in thesettings of primary osteoarthritis, inflammatory arthropathy,limb malalignment, and bipolar lesions of the knee.
Favorable results have been reported after allograft trans-plantation for the treatment of osteochondritis dissecans lesionsof the knee. In a study of sixty-three knees followed for a meanof 4.3 years, Bugbee et al. reported an 89% rate of good-to-excellent functional outcomes as rated with the modifiedMerle d’Aubigne and Postel scale85. Emmerson et al. reportedthe outcomes at a mean of 7.7 years after osteochondral allo-graft transplantation for osteochondritis dissecans lesions86.The mean allograft size was 7.5 cm2, and either a dowel or shelltechnique was utilized on the basis of the lesion location andthe surgeon’s preference. The authors reported a 72% rate ofgood-to-excellent outcomes as rated with the Merle d’Aubigneand Postel scale. The preliminary results of osteochondral al-
1001
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

lograft transplantation for treatment of condylar osteonecrosishave also been encouraging. Gortz and Bugbee found that 88%of forty-three patients treated with allograft transplantation forosteonecrosis were satisfied with the result, and 82% thoughtthat the condition of the knee was improved87. At a mean of 4.5years, none of the patients had required conversion to a totalknee arthroplasty.
The use of osteochondral allografts for the managementof patellofemoral chondral lesions has yielded variable results.Chu et al. reported a good-to-excellent outcome in five patientsat a mean of six years after they had undergone transplantationof a fresh osteochondral allograft into an isolated patellar de-fect80. Jamali et al., however, reported only a 60% rate of good-to-excellent results at a mean of 7.8 years after transplantationof a fresh osteochondral allograft into the patellofemoral jointof twenty knees88. Five knees in that series subsequently re-quired salvage with revision allograft transplantation, patel-lectomy, arthrodesis, or total knee replacement.
Extended storage time for allografts enhances the effec-tive use of these tissues by allowing improved identification ofsuitable recipients and more feasible scheduling of operativetreatments. Williams et al. demonstrated no correlation be-tween functional outcome scores and graft storage times ofup to forty-two days89. Eighteen of nineteen patients demon-strated a normal appearance of the articular cartilage onmagnetic resonance imaging at a mean of twenty-five months(Fig. 3-C). A similar study corroborated these results as itdemonstrated no correlation between the duration of storageof fresh grafts before implantation and the cellular viability ordensity at a mean of forty months postoperatively84. McCullochet al. reported that 84% of twenty-five patients were satisfiedtwo years following allograft transplantation with use of a‘‘prolonged fresh’’ graft that had been stored for a mean oftwenty-four days (range, fifteen to forty-three days)90. LaPradeet al. reported on twenty-three consecutive patients who hadundergone treatment of a focal chondral defect of the femoralcondyle with a refrigerated osteochondral allograft stored for amean of 20.3 days (range, fifteen to twenty-eight days)91. Themean IKDC score improved from 52 points at baseline to 68.5points at the time of final follow-up (at three years), with goodincorporation and a stable position in the host bone in twenty-two of the twenty-three cases.
Osteochondral allograft transplantation has also beeninvestigated in survivorship studies. Gross et al. reported sur-vival rates of 95% at five years, 85% at ten years, and 73% atfifteen years after osteochondral allograft transplantation forposttraumatic femoral condylar lesions92. Sixty-eight percent ofthe patients in their series had concomitant limb-realignmentprocedures, and they were not found to have any differences inoutcomes or complications as compared with the patients whodid not have such procedures. Histological characteristics fa-voring long-term survival included viable chondrocytes,functional preservation of the matrix, and complete replace-ment of the graft with host bone. The authors concluded that ahigh density of viable chondrocytes and mechanical stability ofthe allograft are crucial for long-term survival. In a series of
ninety-two knees that underwent fresh allograft transplanta-tion, Beaver et al. found survival rates of 75% at five years, 64%at ten years, and 63% at fourteen years66. Failure rates werehigher in patients older than sixty years of age or in those withbipolar lesions.
Autologous Chondrocyte ImplantationAutologous chondrocyte implantation, originally described in199493, is an innovative, novel technique to restore cartilagecells into full-thickness chondral defects. The primary theo-retical advantage of autologous chondrocyte implantation isthe development of hyaline-like cartilage rather than fibro-cartilage in the defect, presumably leading to better long-termoutcomes and longevity of the healing tissue. However, theprocedure is not without limitations. It involves a minimum oftwo operations, one for tissue harvest and the other for cellimplantation. Furthermore, autologous chondrocyte implan-tation is technically demanding, and complications related tothe periosteal graft have been reported94,95.
Outcomes (See Appendix)The initial outcomes of autologous chondrocyte implantationwere reported by Brittberg et al.93, in a study of twenty-threepatients ranging in age from fourteen to forty-eight years andwith lesions ranging in size from 1.6 to 6.5 cm2. The averageduration of follow-up was forty-four months. Biopsies showedthat eleven of fifteen femoral transplants and one of sevenpatellar transplants had the appearance of hyaline cartilage.Fourteen of the sixteen patients with a femoral condylar lesionhad a good-to-excellent result. Zaslav et al. recently performeda prospective clinical study to determine the effectiveness ofautologous chondrocyte implantation in patients with failedprior treatments for articular cartilage defects of the knee96.One hundred and twenty-six patients were followed for a meanof four years in this multicenter study. At the time of follow-up, 76% of the patients were deemed to have a good clinicalresult based on knee pain, quality of life, and overall health.The results did not differ if the patient had had a prior marrowstimulation procedure or debridement. The authors concludedthat autologous chondrocyte implantation was effective inproviding pain relief as well as an improved quality of life forpatients who had undergone a previous operative procedurefor the defect.
Many studies have compared autologous chondrocyteimplantation with other cartilage restoration techniques.Anderson et al. compared autologous chondrocyte implantationwith microfracture in a prospective study97. There were twenty-three patients in each group, and all lesions were >2 cm2.There was a mean improvement in the overall condition scorein both groups (1.3 points in the microfracture group and 3.1points in the autologous chondrocyte implantation group, p <0.05). It should be noted, however, that the outcomes of mi-crofracture reported in that series were considerably inferior tothose reported by other authors98. Bentley et al. performed aprospective, randomized study comparing autologous chon-drocyte implantation with mosaicplasty, with fifty patients in
1002
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

each treatment group99. The patients were young (average age,thirty-one years), and the lesions were an average of 4.7 cm2.At an average of nineteen months postoperatively, 88% of thepatients treated with autologous chondrocyte implantationand 69% of those treated with mosaicplasty had a good-to-excellent clinical result. Arthroscopy at one year demonstrateda good-to-excellent repair in 82% of the patients after autol-ogous chondrocyte implantation and in 34% after mosaic-plasty. The authors concluded that autologous chondrocyteimplantation was better than mosaicplasty in terms of bothclinical and biological outcomes.
Autologous chondrocyte implantation is not withoutlimitations. Many patients are unwilling to undergo two pro-cedures and the long recovery time that is necessary in order toallow the chondrocytes to mature. There is also a risk of donorsite morbidity at the periosteal harvest site. Wood et al. re-viewed the adverse outcomes of autologous chondrocyte im-plantation reported to the U.S. Food and Drug Administrationfrom 1996 to 2003100. During this time, there were 7500 lots ofCarticel (Genzyme Tissue Repair, Cambridge, Massachusetts)distributed to physicians and 294 adverse-event reports. Morethan one adverse event was reported for 135 (46%) of the 294patients. The most common adverse event was graft failure,accounting for 24.8% of all adverse events. Delamination ac-counted for 22.1% of the adverse events, and tissue hyper-trophy accounted for 17.7%. Of the 294 patients who had anadverse event, 273 (93%) required a total of 389 surgical re-visions subsequent to implantation. Almost 25% of the re-operations were periarticular procedures such as lysis ofadhesions, lateral release, or synovectomy. Eight patients un-derwent a total knee replacement. Furthermore, Peterson et al.reported fifty-two adverse events, including twenty-six in-stances of periosteal hypertrophy and seven graft failures, in101 patients101. Thus, although the overall complication rateappears to be relatively low, the adverse events that do occurfollowing autologous chondrocyte implantation can be sub-stantial and often result in subsequent operative intervention.
Cell-Based and Scaffold TreatmentAlthough cell-based therapies for inducing cartilage regener-ation, such as autologous chondrocyte implantation, havedemonstrated progress, the results have not been highly pre-dictable or reproducible. In addition, limitations have includeda requirement for a two-stage procedure and a technicallydemanding operation that fails to provide structural supportfor cells during the postoperative healing and incorporationphase.
So-called second-generation techniques in which har-vested autologous chondrocytes are delivered on absorbablescaffolds that support the cells during the preimplantationculturing and postoperative healing phases have evolved. Es-sential properties of these scaffolds include biocompatibilityand biodegradability through safe biomechanical pathways atsuitable time intervals. In the matrix-associated chondrocyteimplantation procedure, chondrocytes are incorporated into aporcine type-I/III collagen membrane. One surface has a rel-
atively higher density of collagen fibers that creates a smoothlow-friction surface, while the other has a rough appearancebecause of larger interstices between the collagen fibers to al-low for seeding of chondrocytes. Hyaluronan-based scaffoldsdeliver the autologous chondrocytes in a scaffold of hyaluronanderivatives. Advantages of these procedures over autologouschondrocyte implantation include a more even cell distribu-tion, avoidance of periosteal harvest and implantation, andincreased technical ease without the need for suturing to ad-jacent articular cartilage.
Matrix-Associated Chondrocyte ImplantationAlthough chondrocytes are harvested in a fashion identical tothat used for the autologous chondrocyte implantation pro-cedure, matrix-associated chondrocyte implantation mini-mizes donor site morbidity by avoiding the harvest andimplantation of a periosteal flap and prevents dedifferentiationof chondrocytes during the culturing process. In addition,matrix-associated chondrocyte implantation makes an ar-throscopic implantation technique feasible for accessiblelesions. In a multicenter study101 of the clinical outcomes afterautologous chondrocyte implantation, 26% of the procedure-related complications were associated with the open arthro-tomy. Furthermore, periosteal hypertrophy occurs betweenthree and seven months after surgery in 10% to 25% of casesand often requires revision surgery102,103. Some authors havereported a substantial risk of arthrofibrosis as well104. Marlovitset al. demonstrated the efficacy of suture-free fixation of thecell-scaffold matrix-associated chondrocyte implantationconstruct with the use of fibrin glue only105. In a pilot study ofsixteen patients who had undergone matrix-associated chon-drocyte implantation to treat a weight-bearing chondral defectof the femoral condyle, high-resolution magnetic resonanceimaging was used to grade the quality of the attachment of theimplant at a mean of thirty-five days postoperatively. A com-pletely attached graft was observed in 88% of the patients.
Jones et al. utilized an ovine model of articular cartilageinjury repair to assess the efficacy of the matrix-associatedchondrocyte implantation procedure106. Six-millimeter defectswere created on the trochlea and medial femoral condyle oftwenty-one sheep that were randomized to treatment withmatrix-associated chondrocyte implantation or unseeded,porcine-derived type-I/III collagen membrane alone. Arthro-scopic assessment with ICRS scores107 at ten weeks postoper-atively revealed superior fill, integration, and appearance of thematrix-associated chondrocyte implantation-treated trochlearand condylar lesions compared with the controls. Magneticresonance imaging demonstrated that the results of matrix-associated chondrocyte implantation were superior to those inboth the untreated control and the scaffold-only group at alltime points. Overall, unseeded scaffolds were characterizedby immature cartilage with poor architectural restoration anddemonstrated no treatment effect compared with unfilledcontrol lesions. Matrix-associated chondrocyte implantationdemonstrated an improved treatment effect across time pointsin comparison with the use of a collagen scaffold only and
1003
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

unfilled controls for all parameters of assessment except his-tological findings106,108,109.
OutcomesZheng et al. examined the phenotype of chondrocytes seededon a type-I/III collagen scaffold and performed progressivehistological analyses of matrix-associated chondrocyte im-plants in a cohort of fifty-six patients over a period of sixmonths postoperatively110. Chondrocytes in the delivery scaf-fold appeared spherical and appropriately integrated into thematrix, expressing aggrecan, type-II collagen, and S-100.Histological analysis of biopsy specimens revealed 75% hyaline-like cartilage regeneration after six months. Behrens et al. re-ported on thirty-four patients with a localized cartilage defectwho were treated with matrix-associated chondrocyte im-plantation111. The mean follow-up period was 34.5 months,and the mean lesion size was 4.1 cm2. The Meyer, Lysholm-Gillquist, and ICRS scores27,28,107 were all substantially improvedin eleven patients at five years postoperatively.
In a similar study, Trattnig et al. serially monitored repairafter matrix-associated autologous chondrocyte implantationin twenty patients using noninvasive cartilage-specific mag-netic resonance imaging112. In ten of these patients, incomplete
defect filling progressed to complete defect filling (six patients)or less incomplete defect filling (four patients). The signalintensity of the matrix-associated chondrocyte implants wasthe same as that of native cartilage in thirteen patients, andcomplete integration was achieved in ten cases.
Bartlett et al. presented the outcomes of a matrix-associatedchondrocyte implantation ‘‘sandwich’’ technique for treatmentof symptomatic chondral defects with a depth of >8 mm in fivepatients113. With this technique, two membranes are templatedand cut to the size of the defect. The first membrane is securedwith fibrin glue to the base of the prepared defect with itsrough cell-loaded surface facing up. The second membrane isimplanted on top of the first one with the cell surface downand is sealed with fibrin glue to the adjacent cartilage. Withinsix months after the surgery, all five patients had improvedCincinnati knee, Stanmore functional rating, and visual ana-logue pain scores27,28. Four patients had arthroscopy at one yearpostoperatively, and stable reparative tissue (ICRS grade II intwo knees and grade III in two) was seen.
Hyaluronan-Based ScaffoldsHyaluronan-based scaffolds are another approach to cartilagerepair that employs a biodegradable, three-dimensional scaf-
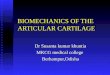
Fig. 4
A: To create tissue-engineered collagen scaffolds, harvested autologous chondrocytes are cultured in
an acellular honeycomb collagen matrix for six weeks with mechanical loads applied to stimulate
matrix production and mature organization. B: An arthroscopic photograph made three months after
implantation of a tissue-engineered collagen scaffold (outlined by red dots) seeded with autologous
chondrocytes for treatment of a focal femoral condyle chondral defect. Note the excellent incorpo-
ration, fill, and congruous margin with the adjacent native cartilage. C: Sagittal fast spin-echo
magnetic resonance image of a focal medial femoral chondral defect (left) and T2-mapping sagittal
images, made at one year (middle) and two years (right) postoperatively, demonstrating progressive
maturation and stratification of repair tissue to approach the appearance of native articular cartilage
(Images courtesy of Dr. Dennis Crawford, MD, Portland, Oregon).
1004
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

fold for cell proliferation. A benzylic ester of hyaluronic acidis used to generate a scaffold with variably sized intersticesbetween 20-mm-thick fibers. In addition to providing thestructural support for cell contact and matrix deposition, thethree-dimensional nonwoven scaffold prevents dedifferentia-tion of harvested autologous chondrocytes even after longperiods of ex vivo culture expansion and promotes the ex-pression of chondrocyte-specific markers. Gradual degrada-tion occurs as the cells start secreting their own extracellularmatrix to allow for an optimal transition between newlyformed and existing tissue114-116.
OutcomesThe results of implantation of hyaluronan-based scaffoldsseeded with autologous chondrocytes to treat chondral defectshave been encouraging. Histological analysis has shownhyaline-like cartilage in the lesion as soon as twelve monthsafter implantation. Marcacci et al. reported the clinical out-comes at a minimum of twenty-four months followingarthroscopic implantation of a seeded hyaluronan-basedscaffold in a prospective series of seventy patients with asymptomatic chondral defect117. All lesions were Outer-bridge grade III or IV118, and their mean size was 2.4 cm2.Fifteen patients underwent a second-look arthroscopy attwelve to thirty-six months. There was improvement inthe IKDC subjective and objective scores from the preopera-tive examination to the twenty-four, thirty-six, and forty-eight-month follow-up examinations, although the objectivescores improved more for patients with a traumatic or os-teochondritis dissecans lesion than they did for those with adegenerative lesion. Arthroscopic evaluation revealed com-plete coverage of the defect with a hyaline-like reparativetissue. The outcomes were not compromised by larger de-fects or a concomitant meniscal or lower-extremity realignmentprocedure.
Gobbi et al. evaluated the efficacy of hyaluronan-basedscaffolds seeded with autologous chondrocytes as a treatmentfor symptomatic patellofemoral chondral lesions119. Thirty-twochondral lesions with a mean size of 4.7 cm2 were treated withdebridement and scaffold implantation through an arthro-scopic or mini-arthrotomy approach. Outcomes were assessedwith the ICRS-IKDC score as well as magnetic resonanceimaging at twelve and twenty-four months postoperatively.The ICRS-IKDC scores improved, with only 18% of the pa-tients having a score of A or B preoperatively and 91% havingsuch a score at twenty-four months postoperatively. Magneticresonance imaging at twenty-four months revealed that 71% ofthe cases had complete filling, nearly normal signal, and ab-sence of subchondral edema, with a positive correlation withclinical outcomes. Second-look arthroscopy in six cases re-vealed complete filling of the defects with reparative tissue thatwas characterized as hyaline-like histologically.
Marcacci et al. presented the results of an ongoingmulticenter study of the subjective and functional outcomes ata mean of thirty-eight months following treatment with ahyaluronan-based scaffold seeded with autologous chondro-
cytes in a cohort of 141 patients117. Ninety-two percent of thepatients had improvement in the IKDC score, and 96% hadthe involved knee rated as normal or nearly normal by thetreating surgeon. Kon et al. compared the clinical outcomes,after five years of follow-up, of treatment with a cell-seededhyaluronan-based scaffold and treatment with a microfracturerepair technique in patients with a grade-III or IV chondraldefect120. Both groups showed significant improvement inIKDC scores, but better improvement in the IKDC objectiveand subjective scores was observed in the hyaluronan-based-scaffold group. The return to sports at two years was similar inthe two groups; however, it remained stable after five years inthe hyaluronan-based-scaffold group but not in the micro-fracture group.
Tissue-Engineered Collagen Matrices Seeded withAutologous ChondrocytesTissue-engineered collagen matrices seeded with autologouschondrocytes provide a promising new technology with whichto address chondral lesions of the knee. This procedure involvesharvesting of the autologous chondrocytes from non-weight-bearing aspects of the knee in a manner analogous to conven-tional autologous chondrocyte implantation. The cells are thenloaded onto a type-I bovine collagen honeycomb matrix and arecultured ex vivo (Fig. 4). In distinction to second-generationtechniques, however, the cell-scaffold construct is subsequentlysubjected to mechanical stimulation with use of a proprietarybioreactor that applies hydrostatic pressure to the chondro-cytes for a minimum of seven days. A lack of mechanicalstimulation may be responsible for chondrocyte dedifferenti-ation and inferior mechanical properties, and the applicationof mechanical load stimulates chondrocytes to produce in-creased amounts of type-II collagen, aggrecan, and other criticalcomponents of a hyaline extracellular matrix121-123.
Use of tissue-engineered scaffolds with autologous chon-drocytes requires a staged procedure that begins with an ar-throscopic biopsy for chondrocyte harvest, which is followedby an arthrotomy for implantation. The harvested chondro-cytes are cultured in the acellular honeycomb collagen matrixfor six weeks. A mini-arthrotomy is then performed to providedirect access to the chondral lesion. The lesion is debrided tocreate stable vertical edges, and meticulous hemostasis is ob-tained. A template of the dimensions of the chondral defect isthen obtained, typically with use of a malleable device thatdelineates its vertical margins. The collagen membrane ismeticulously cut to match the shape of the lesion, but withapproximately 10% greater dimensions in anticipation of slightshrinkage after implantation and fixation. The implant is fixedwith use of a proprietary collagen bioadhesive, which is appliedto the base of the defect and evenly coated over the implant andits seam to the adjacent native cartilage.
OutcomesGiven the relatively recent development of this technology,reports on the clinical outcomes associated with tissue-engineered collagen matrices seeded with autologous chon-
1005
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

drocytes are very limited. However, Crawford et al. recentlyreported the results of a phase-I clinical trial of eight patientswith twenty-four months of follow-up124. Outcomes were as-sessed with use of a visual analogue pain scale and the IKDCsubjective score. Serial evaluations were performed at six,twelve, and twenty-four months. As a secondary outcome,cartilage repair quality was evaluated with magnetic resonanceimaging at three, twelve, and twenty-four months (Fig. 4, C).No serious adverse events were identified. By twelve months,all patients had decreased pain scores (mean, 0.9 ± 1.5 points)compared with the baseline scores (mean, 3.3 ± 2.8 points). Attwenty-four months, the pain scores remained significantlylower than the baseline scores, and the IKDC score had in-creased in seven of the eight patients, to a mean of 76 ± 17points from a mean of 57 ± 25 points at baseline. Magneticresonance imaging showed that seven of the eight patients hadnearly complete or complete filling of the defect at one year,and six of the eight retained good filling at two years. Magneticresonance imaging was performed to assess the collagen matrixcontent and organization. At twenty-four months, four of theeight patients had stratification of T2 values similar to that ofthe adjacent hyaline cartilage124 (Fig. 4, C). These promisingresults prompted a prospective, randomized phase-II trial ofthirty patients to compare this technique with microfracture;this trial is currently in progress.
OverviewIn conclusion, the management of articular cartilage lesions ofthe knee is a challenging problem for orthopaedic surgeons.While a number of surgical approaches have been described, itremains difficult to compare the efficacy of these techniquesbecause of a paucity of well-designed randomized controlledtrials in the literature (Table I). The current evidence, basedprimarily on large case series, suggests that bone marrowstimulation procedures and whole-tissue transplantation of al-lografts or autografts can achieve favorable outcomes when usedfor the management of focal chondral defects of the knee. Cell-based techniques performed with or without a scaffold havedemonstrated early promise in animal and basic-science models,but additional human trials must be completed in order tovalidate their efficacy in achieving successful clinical outcomes.
AppendixTables summarizing studies in the literature about thevarious techniques described in this review are available
with the electronic version of this article on our web site atjbjs.org (go to the article citation and click on ‘‘SupportingData’’). n
Asheesh Bedi, MDRiley J. Williams III, MDHospital for Special Surgery,535 East 70th Street,New York, NY 10021.E-mail address for A. Bedi: [email protected] address for R.J. Williams III: [email protected]
Brian T. Feeley, MDDepartment of Orthopaedic Surgery,University of California at San Francisco,1701 Divisadero Street,Suite 240,San Francisco, CA 94115.E-mail address: [email protected]
References
1. Simon TM, Jackson DW. Articular cartilage: injury pathways and treatment op-tions. Sports Med Arthrosc. 2006;14:146-54.
2. Widuchowski W, Lukasik P, Kwiatkowski G, Faltus R, Szyluk K, Widuchowski J,Koczy B. Isolated full thickness chondral injuries. Prevalance and outcome oftreatment. A retrospective study of 5233 knee arthroscopies. Acta Chir OrthopTraumatol Cech. 2008;75:382-6.
3. Williams RJ 3rd. Cartilage repair strategies. Totowa, NJ: Humana Press; 2007.
4. Williams RJ 3rd, Harnly HW. Microfracture: indications, technique, and results.Instr Course Lect. 2007;56:419-28.
5. Breinan HA, Martin SD, Hsu HP, Spector M. Healing of canine articular cartilagedefects treated with microfracture, a type-II collagen matrix, or cultured autologouschondrocytes. J Orthop Res. 2000;18:781-9.
6. Tran-Khanh N, Hoemann CD, McKee MD, Henderson JE, Buschmann MD. Agedbovine chondrocytes display a diminished capacity to produce a collagen-rich,mechanically functional cartilage extracellular matrix. J Orthop Res. 2005;23:1354-62.
7. Frisbie DD, Oxford JT, Southwood L, Trotter GW, Rodkey WG, Steadman JR,Goodnight JL, McIlwraith CW. Early events in cartilage repair after subchondral bonemicrofracture. Clin Orthop Relat Res. 2003;407:215-27.
TABLE I Grades of Recommendation for Cartilage Repair
Procedures
Grade*
Marrow stimulation procedures B
Adjuncts to marrow stimulation I
Platelet-rich plasma I
Autologous osteochondral transplantation B
Osteochondral allograft transplantation B
Autologous chondrocyte implantation C
Hyaluronan-based scaffolds seeded withautologous chondrocytes
I
Tissue-engineered collagen matrices seededwith autologous chondrocytes
I
*A = good evidence (Level-I studies with consistent findings) for oragainst recommending intervention, B = fair evidence (Level-II or IIIstudies with consistent findings) for or against recommendingintervention, C = poor-quality evidence (Level-IV or V studies withconsistent findings) for or against recommending intervention, andI = there is insufficient or conflicting evidence not allowing arecommendation for or against intervention.
1006
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

8. Frisbie DD, Trotter GW, Powers BE, Rodkey WG, Steadman JR, Howard RD, ParkRD, McIlwraith CW. Arthroscopic subchondral bone plate microfracture techniqueaugments healing of large chondral defects in the radial carpal bone and medialfemoral condyle of horses. Vet Surg. 1999;28:242-55.
9. Bae DK, Yoon KH, Song SJ. Cartilage healing after microfracture in osteoarthriticknees. Arthroscopy. 2006;22:367-74.
10. Asik M, Ciftci F, Sen C, Erdil M, Atalar A. The microfracture technique for thetreatment of full-thickness articular cartilage lesions of the knee: midterm results.Arthroscopy. 2008;24:1214-20.
11. Mithoefer K, Williams RJ 3rd, Warren RF, Potter HG, Spock CR, Jones EC,Wickiewicz TL, Marx RG. Chondral resurfacing of articular cartilage defects in theknee with the microfracture technique. Surgical technique. J Bone Joint Surg Am.2006;88 Suppl 1(Pt 2):294-304.
12. Mithoefer K, Williams RJ 3rd, Warren RF, Wickiewicz TL, Marx RG. High-impactathletics after knee articular cartilage repair: a prospective evaluation of the mi-crofracture technique. Am J Sports Med. 2006;34:1413-8.
13. Frisbie DD, Morisset S, Ho CP, Rodkey WG, Steadman JR, McIlwraith CW.Effects of calcified cartilage on healing of chondral defects treated with micro-fracture in horses. Am J Sports Med. 2006;34:1824-31.
14. Steadman JR, Ramappa AJ, Maxwell RB, Briggs KK. An arthroscopic treatmentregimen for osteoarthritis of the knee. Arthroscopy. 2007;23:948-55.
15. Steadman JR, Miller BS, Karas SG, Schlegel TF, Briggs KK, Hawkins RJ. Themicrofracture technique in the treatment of full-thickness chondral lesions of theknee in National Football League players. J Knee Surg. 2003;16:83-6.
16. Mussa R, Hans MG, Enlow D, Goldberg J. Condylar cartilage response to con-tinuous passive motion in adult guinea pigs: a pilot study. Am J Orthod DentofacialOrthop. 1999;115:360-7.
17. Williams JM, Moran M, Thonar EJ, Salter RB. Continuous passive motionstimulates repair of rabbit knee articular cartilage after matrix proteoglycan loss.Clin Orthop Relat Res. 1994;304:252-62.
18. Salter RB. The physiologic basis of continuous passive motion for articularcartilage healing and regeneration. Hand Clin. 1994;10:211-9.
19. Salter RB. The biologic concept of continuous passive motion of synovial joints.The first 18 years of basic research and its clinical application. Clin Orthop RelatRes. 1989;242:12-25.
20. Steadman JR, Briggs KK, Rodrigo JJ, Kocher MS, Gill TJ, Rodkey WG. Outcomesof microfracture for traumatic chondral defects of the knee: average 11-year follow-up. Arthroscopy. 2003;19:477-84.
21. Gill TJ, Asnis PD, Berkson EM. The treatment of articular cartilage defectsusing the microfracture technique. J Orthop Sports Phys Ther. 2006;36:728-38.
22. Mithoefer K, Williams RJ 3rd, Warren RF, Potter HG, Spock CR, Jones EC,Wickiewicz TL, Marx RG. The microfracture technique for the treatment of articularcartilage lesions in the knee. A prospective cohort study. J Bone Joint Surg Am.2005;87:1911-20.
23. Knutsen G, Engebretsen L, Ludvigsen TC, Drogset JO, Grøntvedt T, Solheim E,Strand T, Roberts S, Isaksen V, Johansen O. Autologous chondrocyte implantationcompared with microfracture in the knee. A randomized trial. J Bone Joint Surg Am.2004;86:455-64.
24. Gudas R, Kalesinskas RJ, Kimtys V, Stankevicius E, Toliusis V, BernotaviciusG, Smailys A. A prospective randomized clinical study of mosaic osteochondralautologous transplantation versus microfracture for the treatment of osteo-chondral defects in the knee joint in young athletes. Arthroscopy. 2005;21:1066-75.
25. Gobbi A, Nunag P, Malinowski K. Treatment of full thickness chondral lesions ofthe knee with microfracture in a group of athletes. Knee Surg Sports TraumatolArthrosc. 2005;13:213-21.
26. Higgins LD, Taylor MK, Park D, Ghodadra N, Marchant M, Pietrobon R, Cook C;International Knee Documentation Committee. Reliability and validity of the Inter-national Knee Documentation Committee (IKDC) Subjective Knee Form. Joint BoneSpine. 2007;74:594-9.
27. Wright RW. Knee injury outcomes measures. J Am Acad Orthop Surg. 2009;17:31-9.
28. Marx RG, Jones EC, Allen AA, Altchek DW, O’Brien SJ, Rodeo SA, Williams RJ,Warren RF, Wickiewicz TL. Reliability, validity, and responsiveness of four kneeoutcome scales for athletic patients. J Bone Joint Surg Am. 2001;83:1459-69.
29. Cerynik DL, Lewullis GE, Joves BC, Palmer MP, Tom JA. Outcomes of micro-fracture in professional basketball players. Knee Surg Sports Traumatol Arthrosc.2009;17:1135-9.
30. Namdari S, Baldwin K, Anakwenze O, Park MJ, Huffman GR, Sennett BJ. Re-sults and performance after microfracture in National Basketball Association ath-letes. Am J Sports Med. 2009;37:943-8.
31. Kreuz PC, Erggelet C, Steinwachs MR, Krause SJ, Lahm A, Niemeyer P, GhanemN, Uhl M, Sudkamp N. Is microfracture of chondral defects in the knee associatedwith different results in patients aged 40 years or younger? Arthroscopy. 2006;22:1180-6.
32. Brown WE, Potter HG, Marx RG, Wickiewicz TL, Warren RF. Magnetic resonanceimaging appearance of cartilage repair in the knee. Clin Orthop Relat Res. 2004;422:214-23.
33. Mithoefer K, Scopp JM, Mandelbaum BR. Articular cartilage repair in athletes.Instr Course Lect. 2007;56:457-68.
34. Hoemann CD, Hurtig M, Rossomacha E, Sun J, Chevrier A, Shive MS,Buschmann MD. Chitosan-glycerol phosphate/blood implants improve hyalinecartilage repair in ovine microfracture defects. J Bone Joint Surg Am. 2005;87:2671-86.
35. Fortier LA, Nixon AJ, Lust G. Phenotypic expression of equine articular chon-drocytes grown in three-dimensional cultures supplemented with supraphysiologicconcentrations of insulin-like growth factor-1. Am J Vet Res. 2002;63:301-5.
36. Nixon AJ, Haupt JL, Frisbie DD, Morisset SS, McIlwraith CW, Robbins PD, EvansCH, Ghivizzani S. Gene-mediated restoration of cartilage matrix by combinationinsulin-like growth factor-I/interleukin-1 receptor antagonist therapy. Gene Ther.2005;12:177-86.
37. Kieswetter K, Schwartz Z, Alderete M, Dean DD, Boyan BD. Platelet derivedgrowth factor stimulates chondrocyte proliferation but prevents endochondral mat-uration. Endocrine. 1997;6:257-64.
38. Lohmann CH, Schwartz Z, Niederauer GG, Carnes DL Jr, Dean DD, Boyan BD.Pretreatment with platelet derived growth factor-BB modulates the ability of costo-chondral resting zone chondrocytes incorporated into PLA/PGA scaffolds to formnew cartilage in vivo. Biomaterials. 2000;21:49-61.
39. Strauss E, Schachter A, Frenkel S, Rosen J. The efficacy of intra-articularhyaluronan injection after the microfracture technique for the treatment of artic-ular cartilage lesions. Am J Sports Med. 2009;37:720-6.
40. Sun Y, Feng Y, Zhang CQ, Chen SB, Cheng XG. The regenerative effect ofplatelet-rich plasma on healing in large osteochondral defects. Int Orthop. 2009May 12 [Epub ahead of print].
41. Mishra A, Tummala P, King A, Lee B, Kraus M, Tse V, Jacobs CR. Bufferedplatelet-rich plasma enhances mesenchymal stem cell proliferation and chondro-genic differentiation. Tissue Eng Part C Methods. 2009;15:431-5.
42. Akeda K, An HS, Okuma M, Attawia M, Miyamoto K, Thonar EJ, Lenz ME, SahRL, Masuda K. Platelet-rich plasma stimulates porcine articular chondrocyte prolif-eration and matrix biosynthesis. Osteoarthritis Cartilage. 2006;14:1272-80.
43. Lane JG, Massie JB, Ball ST, Amiel ME, Chen AC, Bae WC, Sah RL, Amiel D.Follow-up of osteochondral plug transfers in a goat model: a 6-month study. Am JSports Med. 2004;32:1440-50.
44. Rose T, Craatz S, Hepp P, Raczynski C, Weiss J, Josten C, Lill H. The autologousosteochondral transplantation of the knee: clinical results, radiographic findingsand histological aspects. Arch Orthop Trauma Surg. 2005;125:628-37.
45. Feczko P, Hangody L, Varga J, Bartha L, Dioszegi Z, Bodo G, Kendik Z, Modis L.Experimental results of donor site filling for autologous osteochondral mosaicplasty.Arthroscopy. 2003;19:755-61.
46. Koh JL, Wirsing K, Lautenschlager E, Zhang LO. The effect of graft heightmismatch on contact pressure following osteochondral grafting: a biomechanicalstudy. Am J Sports Med. 2004;32:317-20.
47. Koh JL, Kowalski A, Lautenschlager E. The effect of angled osteochondralgrafting on contact pressure: a biomechanical study. Am J Sports Med. 2006;34:116-9.
48. Whiteside RA, Jakob RP, Wyss UP, Mainil-Varlet P. Impact loading of articularcartilage during transplantation of osteochondral autograft. J Bone Joint Surg Br.2005;87:1285-91.
49. Kock NB, Van Susante JL, Buma P, Van Kampen A, Verdonschot N. Press-fitstability of an osteochondral autograft: influence of different plug length and perfectdepth alignment. Acta Orthop. 2006;77:422-8.
50. Kordas G, Szabo JS, Hangody L. Primary stability of osteochondral grafts usedin mosaicplasty. Arthroscopy. 2006;22:414-21.
51. Gilmore RS, Palfrey AJ. A histological study of human femoral condylar articularcartilage. J Anat. 1987;155:77-85.
52. Gilmore RS, Palfrey AJ. Chondrocyte distribution in the articular cartilage ofhuman femoral condyles. J Anat. 1988;157:23-31.
1007
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

53. Huntley JS, Brenkel IJ, McBirnie JM, Simpson AH, Hall AC. Chondrocyte viabilityat the osteochondral graft edge [abstract]. J Bone Joint Surg Br. 2006;88 SuppII:392.
54. Gulotta LV, Rudzki JR, Kovacevic D, Chen CC, Milentijevic D, Williams RJ 3rd.Chondrocyte death and cartilage degradation following autologous osteochondraltransplantation surgery in a rabbit model. Am J Sports Med. 2009;37:1324-33.
55. Hangody L, Vasarhelyi G, Hangody LR, Suksd Z, Tibay G, Bartha L, Bodo G.Autologous osteochondral grafting—technique and long-term results. Injury. 2008;39 Suppl 1:S32-9.
56. Solheim E. [Mosaicplasty in articular cartilage injuries of the knee]. Tidsskr NorLaegeforen. 1999;119:4022-5. Norwegian.
57. Horas U, Pelinkovic D, Herr G, Aigner T, Schnettler R. Autologous chondrocyteimplantation and osteochondral cylinder transplantation in cartilage repair ofthe knee joint. A prospective, comparative trial. J Bone Joint Surg Am. 2003;85:185-92.
58. Hangody L, Fules P. Autologous osteochondral mosaicplasty for the treatmentof full-thickness defects of weight-bearing joints: ten years of experimental andclinical experience. J Bone Joint Surg Am. 2003;85 Suppl 2:25-32.
59. Ozturk A, Ozdemir MR, Ozkan Y. Osteochondral autografting (mosaicplasty) ingrade IV cartilage defects in the knee joint: 2- to 7-year results. Int Orthop. 2006;30:200-4.
60. Berlet GC, Mascia A, Miniaci A. Treatment of unstable osteochondritis dis-secans lesions of the knee using autogenous osteochondral grafts (mosaicplasty).Arthroscopy. 1999;15:312-6.
61. Miniaci A, Tytherleigh-Strong G. Fixation of unstable osteochondritis dissecanslesions of the knee using arthroscopic autogenous osteochondral grafting (mo-saicplasty). Arthroscopy. 2007;23:845-51.
62. Nho SJ, Foo LF, Green DM, Shindle MK, Warren RF, Wickiewicz TL, Potter HG,Williams RJ 3rd. Magnetic resonance imaging and clinical evaluation of patellarresurfacing with press-fit osteochondral autograft plugs. Am J Sports Med. 2008;36:1101-9.
63. Dozin B, Malpeli M, Cancedda R, Bruzzi P, Calcagno S, Molfetta L, Priano F, KonE, Marcacci M. Comparative evaluation of autologous chondrocyte implantation andmosaicplasty: a multicentered randomized clinical trial. Clin J Sport Med. 2005;15:220-6.
64. Bugbee WD. Fresh osteochondral allografts. J Knee Surg. 2002;15:191-5.
65. Bakay A, Csonge L, Papp G, Fekete L. Osteochondral resurfacing of the kneejoint with allograft. Clinical analysis of 33 cases. Int Orthop. 1998;22:277-81.
66. Beaver RJ, Mahomed M, Backstein D, Davis A, Zukor DJ, Gross AE. Freshosteochondral allografts for post-traumatic defects in the knee. A survivorshipanalysis. J Bone Joint Surg Br. 1992;74:105-10.
67. Ball ST, Amiel D, Williams SK, Tontz W, Chen AC, Sah RL, Bugbee WD. Theeffects of storage on fresh human osteochondral allografts. Clin Orthop Relat Res.2004;418:246-52.
68. Langer F, Gross AE. Immunogenicity of allograft articular cartilage. J Bone JointSurg Am. 1974;56:297-304.
69. Allen RT, Robertson CM, Pennock AT, Bugbee WD, Harwood FL, Wong VW, ChenAC, Sah RL, Amiel D. Analysis of stored osteochondral allografts at the time ofsurgical implantation. Am J Sports Med. 2005;33:1479-84.
70. Pearsall AW 4th, Tucker JA, Hester RB, Heitman RJ. Chondrocyte viability inrefrigerated osteochondral allografts used for transplantation within the knee. Am JSports Med. 2004;32:125-31.
71. Williams RJ 3rd, Dreese JC, Chen CT. Chondrocyte survival and materialproperties of hypothermically stored cartilage: an evaluation of tissue used for os-teochondral allograft transplantation. Am J Sports Med. 2004;32:132-9.
72. Convery FR, Akeson WH, Amiel D, Meyers MH, Monosov A. Long-term survival ofchondrocytes in an osteochondral articular cartilage allograft. A case report. J BoneJoint Surg Am. 1996;78:1082-8.
73. Czitrom AA, Keating S, Gross AE. The viability of articular cartilage in freshosteochondral allografts after clinical transplantation. J Bone Joint Surg Am. 1990;72:574-81.
74. McGoveran BM, Pritzker KP, Shasha N, Price J, Gross AE. Long-term chondro-cyte viability in a fresh osteochondral allograft. J Knee Surg. 2002;15:97-100.
75. Williams SK, Amiel D, Ball ST, Allen RT, Tontz WL Jr, Emmerson BC, Badlani NM,Emery SC, Haghighi P, Bugbee WD. Analysis of cartilage tissue on a cellular level infresh osteochondral allograft retrievals. Am J Sports Med. 2007;35:2022-32.
76. Gole MD, Poulsen D, Marzo JM, Ko SH, Ziv I. Chondrocyte viability in press-fitcryopreserved osteochondral allografts. J Orthop Res. 2004;22:781-7.
77. Schachar NS, Novak K, Hurtig M, Muldrew K, McPherson R, Wohl G, ZernickeRF, McGann LE. Transplantation of cryopreserved osteochondral dowel allograftsfor repair of focal articular defects in an ovine model. J Orthop Res. 1999;17:909-19.
78. Enneking WF, Campanacci DA. Retrieved human allografts: a clinicopathologi-cal study. J Bone Joint Surg Am. 2001;83:971-86.
79. Enneking WF, Mindell ER. Observations on massive retrieved human allografts.J Bone Joint Surg Am. 1991;73:1123-42.
80. Chu CR, Convery FR, Akeson WH, Meyers M, Amiel D. Articular cartilagetransplantation. Clinical results in the knee. Clin Orthop Relat Res. 1999;360:159-68.
81. Merle d’Aubigne R, Postel M. Functional results of hip arthroplasty with acrylicprosthesis. J Bone Joint Surg Am. 1954;36:451-75.
82. Ghazavi MT, Pritzker KP, Davis AM, Gross AE. Fresh osteochondral allografts forpost-traumatic osteochondral defects of the knee. J Bone Joint Surg Br. 1997;79:1008-13.
83. Bugbee WD, Convery FR. Osteochondral allograft transplantation. Clin SportsMed. 1999;18:67-75.
84. Davidson PA, Rivenburgh DW, Dawson PE, Rozin R. Clinical, histologic, andradiographic outcomes of distal femoral resurfacing with hypothermically storedosteoarticular allografts. Am J Sports Med. 2007;35:1082-90.
85. Bugbee W, Emmerson BC, Jamali AA. Fresh osteochondral allografting in thetreatment of osteochondritis dissecans of the femoral condyle. Read at the 70thAnnual Meeting of the American Academy of Orthopaedic Surgeons; 2003 Feb 5-9;New Orleans, LA.
86. Emmerson BC, Gortz S, Jamali AA, Chung C, Amiel D, Bugbee WD. Fresh os-teochondral allografting in the treatment of osteochondritis dissecans of the fem-oral condyle. Am J Sports Med. 2007;35:907-14.
87. Gortz S, Bugbee WD. Allografts in articular cartilage repair. Instr Course Lect.2007;56:469-80.
88. Jamali AA, Emmerson BC, Chung C, Convery FR, Bugbee WD. Fresh os-teochondral allografts: results in the patellofemoral joint. Clin Orthop Relat Res.2005;437:176-85.
89. Williams SK, Amiel D, Ball ST, Allen RT, Wong VW, Chen AC, Sah RL, BugbeeWD. Prolonged storage effects on the articular cartilage of fresh human osteo-chondral allografts. J Bone Joint Surg Am. 2003;85:2111-20.
90. McCulloch PC, Kang RW, Sobhy MH, Hayden JK, Cole BJ. Prospective evalua-tion of prolonged fresh osteochondral allograft transplantation of the femoral con-dyle: minimum 2-year follow-up. Am J Sports Med. 2007;35:411-20.
91. LaPrade RF, Botker J, Herzog M, Agel J. Refrigerated osteoarticular allografts totreat articular cartilage defects of the femoral condyles. A prospective outcomesstudy. J Bone Joint Surg Am. 2009;91:805-11.
92. Gross AE, Kim W, Las Heras F, Backstein D, Safir O, Pritzker KP. Fresh os-teochondral allografts for posttraumatic knee defects: long-term followup. Clin Or-thop Relat Res. 2008;466:1863-70.
93. Brittberg M, Lindahl A, Nillson A, Ohlsson C, Isaksson O, Peterson L. Treatmentof deep cartilage defects in the knee with autologous chondrocyte transplantation.N Engl J Med. 1994;331:889-95.
94. Kish G, Hangody L. A prospective, randomised comparison of autologouschondrocyte implantation versus mosaicplasty for osteochondral defects in theknee. J Bone Joint Surg Br. 2004;86:619.
95. Gikas PD, Aston WJ, Briggs TW. Autologous chondrocyte implantation: where dowe stand now? J Orthop Sci. 2008;13:283-92.
96. Zaslav K, Cole B, Brewster R, DeBerardino T, Farr J, Fowler P, Nissen C; STARStudy Principal Investigators. A prospective study of autologous chondrocyte im-plantation in patients with failed prior treatment for articular cartilage defect of theknee: results of the Study of the Treatment of Articular Repair (STAR) clinical trial.Am J Sports Med. 2009;37:42-55.
97. Anderson AF, Fu F, Mandelbaum B. A controlled study of autologous chondro-cyte implantation vs microfracture for articular cartilage lesions of the femur. Readat the 69th Annual Meeting of the American Academy of Orthopaedic Surgeons;2002 Feb 13-17; Dallas, TX.
98. Mithoefer K, McAdams T, Williams RJ, Kreuz PC, Mandelbaum BR. Clinicalefficacy of the microfracture technique for articular cartilage repair in the knee: anevidence-based systematic analysis. Am J Sports Med. 2009;37:2053-63.
99. Bentley G, Biant LC, Carrington RW, Akmal M, Goldberg A, Williams AM, SkinnerJA, Pringle J. A prospective, randomised comparison of autologous chondrocyteimplantation versus mosaicplasty for osteochondral defects in the knee. J BoneJoint Surg Br. 2003;85:223-30.
1008
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E

100. Wood JJ, Malek MA, Frassica FJ, Polder JA, Mohan AK, Bloom ET, Braun MM,Cote TR. Autologous cultured chondrocytes: adverse events reported to the UnitedStates Food and Drug Administration. J Bone Joint Surg Am. 2006;88:503-7.
101. Peterson L, Minas T, Brittberg M, Nilsson A, Sjogren-Jansson E, Lindahl A.Two- to 9-year outcome after autologous chondrocyte transplantation of the knee.Clin Orthop Relat Res. 2000;374:212-34.
102. Minas T. Autologous chondrocyte implantation for focal chondral defects ofthe knee. Clin Orthop Relat Res. 2001;391 Suppl:S349-61.
103. Kreuz PC, Steinwachs, Erggelet C, Krause SJ, Ossendorf C, Maier D, GhanemN, Uhl M, Haag M. Classification of graft hypertrophy after autologous chondrocyteimplantation of full-thickness chondral defects in the knee. Osteoarthritis Cartilage.2007;15:1339-47.
104. Micheli LJ, Browne JE, Erggelet C, Fu F, Mandelbaum B, Moseley JB,Zurakowski D. Autologous chondrocyte implantation of the knee: multicenterexperience and minimum 3-year follow-up. Clin J Sport Med. 2001;11:223-8.
105. Marlovits S, Striessnig G, Kutscha-Lissberg F, Resinger C, Aldrian SM, VecseiV, Trattnig S. Early postoperative adherence of matrix-induced autologous chon-drocyte implantation for the treatment of full-thickness cartilage defects of thefemoral condyle. Knee Surg Sports Traumatol Arthrosc. 2005;13:451-7.
106. Jones CW, Willers C, Keogh A, Smolinski D, Fick D, Yates PJ, Kirk TB, ZhengMH. Matrix-induced autologous chondrocyte implantation in sheep: objective as-sessments including confocal arthroscopy. J Orthop Res. 2008;26:292-303.
107. Smith GD, Taylor J, Almqvist KF, Erggelet C, Knutsen G, Garcia Portabella M,Smith T, Richardson JB. Arthroscopic assessment of cartilage repair: a validationstudy of 2 scoring systems. Arthroscopy. 2005;21:1462-7.
108. Dorotka R, Windberger U, Macfelda K, Bindreiter U, Toma C, Nehrer S. Repairof articular cartilage defects treated by microfracture and a three-dimensional col-lagen matrix. Biomaterials. 2005;26:3617-29.
109. Frenkel SR, Kubiak EN, Truncale KG. The repair response to osteochondralimplant types in a rabbit model. Cell Tissue Bank. 2006;7:29-37.
110. Zheng MH, Willers C, Kirilak L, Yates P, Xu J, Wood D, Shimmin A. Matrix-induced autologous chondrocyte implantation (MACI): biological and histologicalassessment. Tissue Eng. 2007;13:737-46.
111. Behrens P, Bitter T, Kurz B, Russlies M. Matrix-associated autologous chon-drocyte transplantation/implantation (MACT/MACI)—5-year follow-up. Knee.2006;13:194-202.
112. Trattnig S, Ba-Ssalamah A, Pinker K, Plank C, Vecsei V, Marlovits S. Matrix-based autologous chondrocyte implantation for cartilage repair: noninvasive moni-toring by high-resolution magnetic resonance imaging. Magn Reson Imaging.2005;23:779-87.
113. Bartlett W, Gooding CR, Carrington RW, Skinner JA, Briggs TW, Bentley G.Autologous chondrocyte implantation at the knee using a bilayer collagen mem-brane with bone graft. A preliminary report. J Bone Joint Surg Br. 2005;87:330-2.
114. Kang JY, Chung CW, Sung JH, Park BS, Choi JY, Lee SJ, Choi BC, Shim CK,Chung SJ, Kim DD. Novel porous matrix of hyaluronic acid for the three-dimensionalculture of chondrocytes. Int J Pharm. 2009;369:114-20.
115. Filova E, Jelınek F, Handl M, Lytvynets A, Rampichova M, Varga F, Cinatl J,Soukup T, Trc T, Amler E. Novel composite hyaluronan/type I collagen/fibrin scaffoldenhances repair of osteochondral defect in rabbit knee. J Biomed Mater Res B ApplBiomater. 2008;87:415-24.
116. Schlegel W, Nurnberger S, Hombauer M, Albrecht C, Vecsei V, Marlovits S.Scaffold-dependent differentiation of human articular chondrocytes. Int J Mol Med.2008;22:691-9.
117. Marcacci M, Berruto M, Brocchetta D, Delcogliano A, Ghinelli D, Gobbi A, Kon E,Pederzini L, Rosa D, Sacchetti GL, Stefani G, Zanasi S. Articular cartilage engineeringwith Hyalograft C: 3-year clinical results. Clin Orthop Relat Res. 2005;435:96-105.
118. Cameron ML, Briggs KK, Steadman JR. Reproducibility and reliability of theOuterbridge classification for grading chondral lesions of the knee arthroscopically.Am J Sports Med. 2003;31:83-6.
119. Gobbi A, Kon E, Berruto M, Francisco R, Filardo G, Marcacci M. Patellofemoralfull-thickness chondral defects treated with Hyalograft-C: a clinical, arthroscopic,and histologic review. Am J Sports Med. 2006;34:1763-73.
120. Kon E, Gobbi A, Filardo G, Delcogliano M, Zaffagnini S, Marcacci M. Arthro-scopic second-generation autologous chondrocyte implantation compared with mi-crofracture for chondral lesions of the knee: prospective nonrandomized study at 5years. Am J Sports Med. 2009;37:33-41.
121. Torzilli PA, Bhargava M, Park S, Chen CT. Mechanical load inhibits IL-1 in-duced matrix degradation in articular cartilage. Osteoarthritis Cartilage. 2009 Sep1 [Epub ahead of print].
122. Tanimoto K, Kitamura R, Tanne Y, Kamiya T, Kunimatsu R, Yoshioka M,Tanaka N, Tanaka E, Tanne K. Modulation of hyaluronan catabolism in chondrocytesby mechanical stimuli. J Biomed Mater Res A. 2009 Jun 30 [Epub ahead of print].
123. Ryan JA, Eisner EA, DuRaine G, You Z, Reddi AH. Mechanical compression ofarticular cartilage induces chondrocyte proliferation and inhibits proteoglycan syn-thesis by activation of the ERK pathway: implications for tissue engineering andregenerative medicine. J Tissue Eng Regen Med. 2009;3:107-16.
124. Crawford DC, Heveran CM, Cannon WD Jr, Foo LF, Potter HG. An autologouscartilage tissue implant NeoCart for treatment of grade III chondral injury to thedistal femur: prospective clinical safety trial at 2 years. Am J Sports Med. 2009;39:1334-43.
125. Marcacci M, Kon E, Delcogliano M, Filardo G, Busacca M, Zaffagnini S. Ar-throscopic autologous osteochondral grafting for cartilage defects of the knee:prospective study results at a minimum 7-year follow-up. Am J Sports Med. 2007;35:2014-21.
126. Chow JC, Hantes ME, Houle JB, Zalavras CG. Arthroscopic autogenous os-teochondral transplantation for treating knee cartilage defects: a 2- to 5-year follow-up study. Arthroscopy. 2004;20:681-90.
127. Garrett JC. Fresh osteochondral allografts for treatment of articular defects inosteochondritis dissecans of the lateral femoral condyle in adults. Clin Orthop RelatRes. 1994;303:33-7.
128. Peterson L, Brittberg M, Kiviranta I, Akerlund EL, Lindahl A. Autologouschondrocyte transplantation. Biomechanics and long-term durability. Am J SportsMed. 2002;30:2-12.
1009
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 4 d A P R I L 2010MA N AG E M E N T O F AR T I C U L A R CA RT I L AG E DE F E C T S O F T H E KN E E