Embed Size (px)
DESCRIPTION
Malnutrition, Starvation and Refeeding Syndrome. Khursheed Jeejeebhoy. Starvation and Semi-starvation. State of Negative Protein-Energy Balance Absence of nutrient intake Intake below requirements. Metabolic Adaptation to Starvation. Post Absorptive state --- Overnight fast after a meal. - PowerPoint PPT Presentation
Citation preview

Malnutrition, Starvation and Malnutrition, Starvation and Refeeding Syndrome Refeeding Syndrome
Khursheed JeejeebhoyKhursheed Jeejeebhoy

Starvation and Semi-starvationStarvation and Semi-starvation
State of Negative Protein-Energy BalanceState of Negative Protein-Energy Balance– Absence of nutrient intakeAbsence of nutrient intake– Intake below requirementsIntake below requirements

Metabolic Adaptation to StarvationMetabolic Adaptation to Starvation
Post Absorptive state --- Overnight fast after a meal
Fast lasting 12-24 Hours
Fast lasting > 3days
Prolonged Starvation

Post-Absorptive StatePost-Absorptive State
The Brain Must receive GlucoseThe Brain Must receive Glucose Insulin levels fall:Insulin levels fall: Glucose delivery to Tissues 8-10 g/hrGlucose delivery to Tissues 8-10 g/hr
– Increased Glycogenolysis 50%Increased Glycogenolysis 50%– Continued Gluconeogensis 50%Continued Gluconeogensis 50%
Lactate and Pyruvate 50%Lactate and Pyruvate 50% Amino acids 50%Amino acids 50%
Muscle uses mainly fatty acidsMuscle uses mainly fatty acids– 2/3 fuel oxidation is derived from fatty acids2/3 fuel oxidation is derived from fatty acids

Fasting ~ 2-4 daysFasting ~ 2-4 days Liver glycogen depletedLiver glycogen depleted Insulin levels fallInsulin levels fall Glucose production by Gluconeogenesis:Glucose production by Gluconeogenesis:
– Lactate and PyruvateLactate and Pyruvate– Amino acidsAmino acids
Nitrogen loss from amino acid is 10-12 g/dayNitrogen loss from amino acid is 10-12 g/day Branched chain aminoacids released by muscle Branched chain aminoacids released by muscle
and oxidizedand oxidized Ketone production increasesKetone production increases Brain reduces glucose utilization and increases Brain reduces glucose utilization and increases
Ketone body oxidationKetone body oxidation

Prolonged StarvationProlonged Starvation
Metabolic rate fallsMetabolic rate falls Nitrogen losses decrease to 4-5 g/dayNitrogen losses decrease to 4-5 g/day Brain now uses ketones as the sole source Brain now uses ketones as the sole source
of energyof energy Muscle uses fatty acid and spares Muscle uses fatty acid and spares
branched-chain amino acid oxidationbranched-chain amino acid oxidation

Clinical Effects of StarvationClinical Effects of Starvation
Resting Energy Expenditure fall by about Resting Energy Expenditure fall by about 25-35% by 3 weeks25-35% by 3 weeks
Serum Albumin Concentrations remain Serum Albumin Concentrations remain normalnormal
Serum Prealbumin fallsSerum Prealbumin falls Death occurs when body fat is depletedDeath occurs when body fat is depleted Obese persons can withstand prolonged Obese persons can withstand prolonged
starvationstarvation

Clinical effects of Fasting: Clinical effects of Fasting: Weight lossWeight loss
0100020003000400050006000700080009000
Normal Obese
Gra
ms Day 0-5
Day 6-11>3 Weeks

Clinical effetcs of Fasting: Na excretion
0
20
40
60
80
100
120
140
160
Urine Na
Mm
/day
Day 1Day 4Day 7>3 Weeks

Weight and Sodium lossWeight and Sodium loss
Fall in insulin level reduces sodium Fall in insulin level reduces sodium reabsorption by the kidneyreabsorption by the kidney– Increased sodium excretionIncreased sodium excretion– DiuresisDiuresis
Reduced sodium intake increases negative Reduced sodium intake increases negative sodium balancesodium balance
Water loss main cause of rapid weight loss Water loss main cause of rapid weight loss seen early in starvationseen early in starvation

MalnutritionMalnutrition Malnutrition is a condition in which there is unbalanced deficiency of nutrients.Malnutrition is a condition in which there is unbalanced deficiency of nutrients. Causes are:Causes are:
– Macronutrient deficiencyMacronutrient deficiency Protein-energy malnutritionProtein-energy malnutrition Protein deficiencyProtein deficiency Energy deficiencyEnergy deficiency
– Micronutrient deficiencyMicronutrient deficiency Electrolyte Electrolyte
– PotassiumPotassium– MagnesiumMagnesium– PhosphorusPhosphorus
Trace elementTrace element– ZincZinc– CopperCopper– ChromiumChromium– SeleniumSelenium
Vitamin DeficiencyVitamin Deficiency– Fat soluble - Vitamin DFat soluble - Vitamin D– Water soluble - ThiamineWater soluble - Thiamine

Protein-Energy MalnutritionProtein-Energy MalnutritionReduced intake of both Protein and energyReduced intake of both Protein and energy
1944-46 32 volunteers reduced their intake 1944-46 32 volunteers reduced their intake from 2400 kcals/d to 1600 kcals/day (Keys from 2400 kcals/d to 1600 kcals/day (Keys Minnesota study)Minnesota study)
Lost 70% body fat and 24% FFMLost 70% body fat and 24% FFM New equilibrium at 24 weeks into the diet.New equilibrium at 24 weeks into the diet.

PEM: Nitrogen adaptation PEM: Nitrogen adaptation Martin and Robison 1922Martin and Robison 1922
0
5
10
15
20
25
Day 0Day 1
Day 2Day 3
Day 4Day 5
Day 6Day 7
Day 8Day 9
Day 10
gN/d
ay Nitrogen IntakeNitrogen loss
Neg N balance
Pos. N balance

Nitrogen AdaptationNitrogen Adaptation
Loss of labile nitrogen pool reduces nitrogen Loss of labile nitrogen pool reduces nitrogen outputoutput
Equilibrium restored unless protein intake fall Equilibrium restored unless protein intake fall below < 37 mg/Kg/day on a diet meeting below < 37 mg/Kg/day on a diet meeting energy requirementsenergy requirements

Energy AdaptationEnergy Adaptation
Body reduces energy requirements by:Body reduces energy requirements by:– Reduced metabolic rate of the body cell mass.Reduced metabolic rate of the body cell mass.– Reduced body cell mass.Reduced body cell mass.
Body weight equilibrates approximately at:Body weight equilibrates approximately at:– 28-30 kcal/kg/day28-30 kcal/kg/day

Hormonal response Hormonal response
Insulin levels fall promoting release of Insulin levels fall promoting release of glucose and free fatty acids for energyglucose and free fatty acids for energy
T3 levels reduced resulting in a lower T3 levels reduced resulting in a lower metabolic ratemetabolic rate
IGF -1 levels fall with starvation reducing IGF -1 levels fall with starvation reducing protein synthesisprotein synthesis

HypoproteinemiaHypoproteinemia Low prealbumin levels can be due to:Low prealbumin levels can be due to:
– Protein deficiencyProtein deficiency– Protein lossProtein loss– Acute Phase reactionAcute Phase reaction
Low Albumin levels are:Low Albumin levels are:– ?Low protein with high energy intake?Low protein with high energy intake– Protein lossProtein loss– Acute Phase reactionAcute Phase reaction
Hypoalbuminemia is a sign of disease not Hypoalbuminemia is a sign of disease not malnutritionmalnutrition

Micronutrient deficiencyMicronutrient deficiency Iron deficiency:Iron deficiency:
– Blood loss due to diseaseBlood loss due to disease– Dietary deficiency Dietary deficiency
intake of cereal iron (India)intake of cereal iron (India) Magnesium DeficiencyMagnesium Deficiency
– Dietary – AlcoholismDietary – Alcoholism– Renal Renal – Endocrine metabolic Endocrine metabolic – MalabsorptionMalabsorption– Short BowelShort Bowel– IatrogenicIatrogenic
Phosphorus deficiency – Iatrogenic– Alcoholism– Recovery from diabetic ketoacidosis
Zinc DeficiencyZinc Deficiency– IatrogenicIatrogenic– Gastrointestinal lossesGastrointestinal losses
Copper DeficiencyCopper Deficiency– Infants recovering from malnutritionInfants recovering from malnutrition– IatrogenicIatrogenic
Vitamin D deficiencyVitamin D deficiency– DietaryDietary– MalabsorptionMalabsorption– Lack of sun exposureLack of sun exposure

Micronutrient deficiencyMicronutrient deficiency Vitamin A deficiencyVitamin A deficiency
– Dietary deficiency in developing countriesDietary deficiency in developing countries– IatrogenicIatrogenic
Thiamine deficiencyThiamine deficiency– AlcoholismAlcoholism– IatrogenicIatrogenic– DiureticsDiuretics
Folate deficiencyFolate deficiency– AlcoholismAlcoholism– MalabsorptionMalabsorption
Vitamin B12 DeficiencyVitamin B12 Deficiency– VegansVegans– MalabsorptionMalabsorption– Poor intake in an ageing populationPoor intake in an ageing population

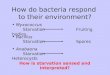
Refeeding SyndromeRefeeding Syndrome
Refeeding a malnourished patient results in:Refeeding a malnourished patient results in:– Rise of insulin levelsRise of insulin levels
Sodium and water retentionSodium and water retention Potassium retentionPotassium retention Phosphorus retentionPhosphorus retention Magnesium retentionMagnesium retention
Refeeding may cause serious:Refeeding may cause serious:– HypokalemiaHypokalemia– HypophosphatemiaHypophosphatemia

Refeeding SyndromeRefeeding Syndrome
Refeeding a malnourished patient can result Refeeding a malnourished patient can result in Heart failure due to:in Heart failure due to:– Atrophic myocardium in malnutritionAtrophic myocardium in malnutrition– Muscle depletion of Mg, K, PMuscle depletion of Mg, K, P– Sodium and water overloadSodium and water overload– Increased metabolic rateIncreased metabolic rate

6
7
8
9
10
11ST
RO
KE
VOLU
ME
(ML)
18 20 22 24 26 28 30FAT FREE MASS (KG)
PCM
LEAN
OBESE
16 7
Heymsfiled In Heart Diseases 1988

6
7
8
9
10
11LV
Wal
l Thi
ckne
ss (m
m)
18 20 22 24 26 28 30Chamber Radius (mm)
PCM
LEAN
OBESE
16 7
Heymsfield In Heart Disease 1988

Heymsfield In Heart Disease 1988
020406080
100120140160180
% INCREASE
DAY 20
EDVVO2CO2
REFEEDING EDEMA: CARDIAC FAILURE 36 year old Anorexia fed by NG 3200 kcal/d

Micronutrient DeficienciesMicronutrient DeficienciesIn Malnutrition and the HeartIn Malnutrition and the Heart
MICRONUTRIENT SYNDROMEThiamine deficiency Heart Failure Magnesium Deficiency ArrhythmiasPhosphorus Deficiency CardiomyopathySelenium Deficiency CardiomyopathyPotassium Deficiency Arrhythmias
Myocardial injury

Refeeding SyndromeRefeeding Syndrome
High CHO intake exacerbates the refeeding High CHO intake exacerbates the refeeding syndromesyndrome
Low protein High energy diet causes fat gain Low protein High energy diet causes fat gain but not lean tissuebut not lean tissue
High protein diet can reduce nitrogen loss High protein diet can reduce nitrogen loss even if energy deficienteven if energy deficient
Exercise important to regain muscle massExercise important to regain muscle mass



Relationship of Protein and Energy to Relationship of Protein and Energy to Nitrogen retentionNitrogen retention
-6
-4
-2
0
2
4
6
8
0 0.5 1 1.5 2 2.5
Protein intake (g/kg/d)
Nitr
ogen
Bal
ance
(g/d
)
0104060Linear (0)Linear (40)Linear (60)
Energy intake kcal/d

Refeeding SyndromeRefeeding SyndromeJournal of Internal Medicine 2005; 257: 461–468
Case controlled study in Geriatric wardCase controlled study in Geriatric ward 325 had hypophosphatemia325 had hypophosphatemia 326 normal plasma phosphorus levels326 normal plasma phosphorus levels

Refeeding SyndromeRefeeding SyndromeJournal of Internal Medicine 2005; 257: 461–468

Refeeding SyndromeRefeeding SyndromeJournal of Internal Medicine 2005; 257: 461–468

Refeeding SyndromeRefeeding SyndromeAm J Clin Nutr 1979;32:981-91Am J Clin Nutr 1979;32:981-91
Severely starved men fed: 27 g/day protein Severely starved men fed: 27 g/day protein + 2250 Kcal/d+ 2250 Kcal/d
Weight gainWeight gain– Increased CholesterolIncreased Cholesterol– Albumin levels fellAlbumin levels fell– Nitrogen balance 0Nitrogen balance 0
Protein intake increased to 100 g/dayProtein intake increased to 100 g/day– Positive nitrogen balancePositive nitrogen balance– Rise in serum albuminRise in serum albumin

Refeeding SyndromeRefeeding SyndromeAm J Clin Nutr 1979;32:981-91Am J Clin Nutr 1979;32:981-91
Refeeding of malnourished patients:Refeeding of malnourished patients:– 20 kcal/kg/day and 1.5-2.0 g/protein/day20 kcal/kg/day and 1.5-2.0 g/protein/day– Low CHO and higher fatLow CHO and higher fat– Monitor K, P, Mg and weight gainMonitor K, P, Mg and weight gain– Diuretics if rquiredDiuretics if rquired– Gradually increase energy intake depending on Gradually increase energy intake depending on
response.response.