Embed Size (px)
Citation preview

1
Mali PRRO 10610.0: “Fighting/controlling malnutrition in food-insecure areas in Mali”
Project duration 1 January 2009 – 31 December 2010
Number of beneficiaries 896,324
WFP food tonnage 24,696 mt
Cost (US Dollars)
WFP food cost 15,929,405
Total cost to WFP 32,748,374
Executive Summary The conclusion of the previous PRRO 10452.0 on 31 December 2008 coincides with increases in the prices of essential foods: the cost of rice, for example, has been over 20 percent higher than the average price over the past five years. Severe food insecurity already affects 8 percent of households; 18 percent are vulnerable to food insecurity.
The proposed PRRO, which aims to consolidate the achievements of its predecessor, has the following objectives:
� improve the nutritional status of children under 5 and pregnant and lactating women;
� improve the nutritional status of people living with HIV;
� increase treatment of people affected by tuberculosis; and
� improve nutrition-related practices and knowledge.
Geographical targeting is based on the areas assisted under the previous PRRO in partnership with UNICEF in the regions of Kayes, Koulikoro, Ségou, Mopti, Gao, Timbuktu and Kidal. Anticipating the effects of price increases, the district of Sikasso will also be covered. A survey of household food security is being considered for the urban areas of Bamako District to possibly integrate vulnerable populations into the HIV and tuberculosis component.
The components of the operation include nutrition interventions among children aged 6–59 months, food assistance for vulnerable groups and communication activities.
Capacity-building will be developed to facilitate the transfer of knowledge and skills to the Government and civil-society organizations. A gradual transfer of activities to health departments in Kayes, Gao and Timbuktu will be tested, and the National Tuberculosis Control Programme will progressively take on programme implementation tasks. These measures, which will be assessed in a mid-term review in 2010, are expected to provide the foundation for an eventual hand-over to the Government.
The proposed activities contribute to: i) WFP’s Strategic Objective 4; ii) Objective 3.5 of the UNDAF; and iii) Goals 1, 4, 5 and 6 of the MDGs. It also addresses Objective 2 in Mali’s Strategy Document on Growth and Poverty Reduction.

2
SITUATIONAL ANALYSIS AND SCENARIOS Context
1. Mali is a landlocked Sahelian country with an area of 1.2 million km2, two thirds of which is desert. It is a predominantly agropastoralist country with erratic rainfall that makes the economy vulnerable to external shocks. In 2004, Mali ranked 173rd of 177 countries in the UNDP Human Development Index.1 The poverty rate, which is measured by calorie consumption, was 64 percent in 2006, compared with 68 percent in 2001: this decline was reported mainly in urban areas – the situation in rural areas has not improved.2
2. The prices of essential foods in international markets increased significantly in 2008. In Mali, the price of rice in April 2008 was 23 percent higher than the average of the previous five years; prices have remained below those in neighbouring countries, however. Increases in the prices of meat, oil and flour were reported by the Observatoire du Marché Agricole (Agricultural Market Observatory, OMA) in 2008. The low price of cereals compared with neighbouring countries and the porous nature of the borders could lead to large-scale exports of cereals and consequential price increases.3
3. This situation is a threat to food and nutritional security in structurally vulnerable areas. The food and nutrition situation could deteriorate in the semi-urban areas, which are occupied by migrants and poor people who depend largely on rice.
4. The Government has decided to provide several healthcare services free of charge, but factors such as long distances, poor roads and social and cultural barriers limit access. Women and children are most affected by these limiting factors because of their weak economic situation and the impact of culture on their behaviour.
5. According to the 2006 Enquête Démographique et de Santé au Mali (Mali Demographic and Health Survey, EDSM IV), AIDS prevalence is 1.3 percent, but the rate among sex workers is 35.3 percent; among women street vendors it is 5.9 percent.4 The socio-economic vulnerability of women and young people relative to men exacerbates the problem.
6. The Government programme for the prevention of mother-to-child transmission (PMTCT) operates at 103 sites across the country, promoting PMTCT among pregnant women.
7. The number of TB cases increased by 14 percent from 2004 to 2005.5 Controlling TB continues to be an acute problem; the treatment drop-out rate remains high in spite of the gradual expansion of the internationally recommended control strategy (DOTS6).
1 UNDP Human Development Report, 2007/2008. 2 International Monetary Fund. 2008. Mali: Joint Staff Advisory Note of the Poverty Reduction Strategy Paper.Country Report 08/122, Washington, D.C. 20431. 3 Mali Periodic Update on the domestic food security situation, USAID/Mali Summary – Situation as at June 6, 2008. Bamako.4USAID. 2006. Integrated STI/HIV Prevalence and Behaviour Surveys (ISBS). Final Report. Bamako.5 National Tuberculosis Control Programme. 2006. Technical Guide for Health Personnel, Bamako. 6 The DOTS strategy is the internationally recommended control strategy for tuberculosis, which comprises five elements: political commitment, case detection, standardized short-course chemotherapy, regular supply of medicines, and recording and reporting. See document WHO/CDS/TB/2002.297.

3
The Food Security and Nutrition Situation 8. Despite three consecutive years of good harvests, food insecurity affects 26 percent of
households, of which 8 percent are severely food-insecure.7 The regions most affected, in order of severity, are Gao, Sikasso, Koulikoro, Mopti and Ségou. Kidal is affected by moderate food insecurity. Acute food insecurity affects the following livelihood systems: i) “agro/onion” livelihoods in Mopti in the Bandiagara highlands – 20 percent; ii) agropastoralist livelihoods north of the 15th parallel – 18.8 percent; and iii) “agro/cotton, fruit” livelihoods in Sikasso, south of Koulikoro and Kayes –18 percent. In “agro-migration” livelihoods in Kayes and “agro/onion” livelihoods in Mopti, the number of meals per day is reduced.8
9. Global acute malnutrition (GAM) is a public health issue: the rate in 2007 was estimated at 9.7 percent, which approaches the WHO threshold of 15 percent which signifies an emergency situation. Young children are the group most affected by GAM: 16.9 percent of those aged 9–11 months, 22.5 percent of those aged 12–17 months and 15.4 percent of those aged 18–23 months. The regions most affected are Gao (16.1 percent) and Kayes (14.3 percent). The situation is serious even under favourable conditions: it could deteriorate rapidly into a crisis comparable with the situation in 2005, when the national GAM average reached the 15 percent threshold. According to EDSM IV, the level of GAM in 2005 was high in all regions, and very high in Kidal (27.2 percent), Gao (17.4 percent), Timbuktu (16.5 percent), Koulikoro (16.2 percent), Sikasso (15.8 percent) and Kayes (15.2 percent).
10. Anaemia affects 81 percent of children aged 6–59 months, 68 percent of women of reproductive age and 76 percent of pregnant women.9
Scenario 11. The consolidation of achievements under the previous PRRO (10452.0) requires
continued activities in the areas that it covered. The current trend of rising prices for rice, oil, meat and wheat – and presence of rebel movements in the northern regions – are likely to lead to a deterioration of the food and nutrition situation. Civil society organizations continue to pressure for a response to the increases in food prices.
POLICIES, CAPACITIES AND ACTIONS OF THE GOVERNMENT AND OTHER STAKEHOLDERS Government
12. The Programme de Développement Sanitaire et Social 2005–2009 (Health and Social Development Programme, PRODESS II) aims at a 30 percent reduction in malnutrition-related mortality and morbidity rates among children under 5 and a 70 percent reduction in vitamin A and iron deficiencies among pregnant women.
13. The Government of Mali’s policy documents for nutrition, AIDS and TB include: the Plan Stratégique Nationale pour l’Alimentation et la Nutrition (National Food and Nutrition Strategic Plan, PSNAN), the Country Protocol for the Management of Acute
7 Consumption in households is used as a proxy food-security indicator: the frequency and variety of meals help to classify household food security as poor (severely food-insecure), limited (moderately food-secure) or acceptable (food-secure). 8 The Commission for Food Security/Early Warning System, UNICEF, WFP and Helen Keller International (HKI). Baseline Survey on Food Security and Nutrition, Round 2, March 2008. 9 EDSM IV, 2006.

4
Malnutrition, nutritional management guides for people living with HIV (PLHIV), the National Strategy Paper for HIV and AIDS Control, and technical guides on TB for technical staff.
14. The Government has provided free access to TB treatment and ART drugs.
Other Stakeholders 15. Mali has a national child survival strategy and a roadmap for maternal mortality
reduction. A Semaine d’Intensification des Activités de Nutrition (National Nutrition Week, SIAN) is organized twice a year by the Ministry of Health in partnership with donors and communities. Several NGOs are involved in nutrition work, but their capacities need to be reinforced. The criteria for selecting NGOs will be developed in the operational plan.
Coordination 16. The Government’s Nutrition Division, UNICEF and WFP operate a working group to
coordinate stakeholders’ nutrition work. A Memorandum of Understanding (MOU) between UNICEF and WFP stipulates that WFP provides support for cases of moderate malnutrition and UNICEF for cases of severe malnutrition.
OBJECTIVES OF WFP ASSISTANCE 17. PRRO 10610.0 will support Objective 3 of the UNDAF – “Reinforce access of the
most vulnerable groups to quality basic social services” – and result 3.5 – “...the nutritional condition of pregnant and lactating women and children under 5 is improved”.
18. The operation also addresses WFP’s Strategic Objective 4 with the following objectives related to the MDGs:
� stabilize and improve the nutritional status of children under 5 and pregnant and lactating women (MDGs 1, 4 and 5);
� improve the nutritional situation of PLHIV (MDG 6); and
� increase access to TB treatment (MDG 6).
WFP RESPONSE STRATEGY Nature and Effectiveness of Food Security Assistance to Date
19. Since 1964, WFP’s operations in Mali have provided 490,000 mt of food under various programmes that have contributed mainly to promoting girls’ education, establishing emergency food stocks, increasing agricultural productivity and rehabilitating malnourished children.
20. The current PRRO covers: i) the management of moderately malnourished children under 5; ii) food assistance for pregnant and lactating women; iii) food assistance for PLHIV and people with TB; and iv) support for nutritional education. The management of cases of moderate malnutrition is ongoing at 300 community health centres.

5
Strategy Outline 21. The proposed PRRO 10610.0 is in line with the recommendations of the mid-term
evaluation and the objectives of the Government’s Cadre Stratégique pour la Croissance et la Réduction de la Pauvreté (Strategic Framework for Growth and Poverty Reduction, CSCRP). It will support the National Protocol for the Management of Severe Malnutrition, focusing on emergency situations. Geographical coverage will complement that of UNICEF.
22. The supplementary feeding components of PRRO 10610.0 are as follows:
� Children aged 6–59 months will be covered by targeted supplementary feeding. As a further and separate intervention during lean seasons, food supplements will be distributed to all children aged 6–24 months (blanket coverage) in at-risk areas, irrespective of their nutritional status.
� Food assistance for women will target malnourished pregnant and lactating women.
� Food assistance for PLHIV will targets patients on anti-retroviral therapy (ART) and people registered in a PMTCT programme who show poor nutritional status.
23. Nutritional education will be given to mothers of moderately malnourished children, pregnant and lactating women, PLHIV and people with TB who are supported under the PRRO. Beneficiaries will also include adolescent girls, women of reproductive age and caregivers to ensure good nutrition and hygiene in households.
24. Communication tools and the selection of cases of malnourishment at the community level will be developed by WFP and partners. A cross-cutting communications strategy will be developed that will include support for community radios and the production, design and dissemination of communications tools at health centres and among community health volunteers.
25. The country office has reviewed all data-collection tools and has developed a database to evaluate routine indicators. External evaluations under the early warning system (EWS) sentinel sites will also be used to assess performance.
Hand-Over Strategy
26. The implementation of nutrition activities at health centres will help to build the Government’s capacity to prevent and manage malnutrition. Nutrition education for women will reinforce their knowledge of health, nutrition and hygiene.
27. As activities are handed over, an approach involving direct collaboration with health departments without the assistance of cooperating partners will be tested in the regions of Kayes, Gao and Timbuktu.
28. Under an agreement with WFP, the National Tuberculosis Control Programme is involved in the monitoring and transmission of data to WFP. This experiment will continue and will if possible be extended to other components.
29. Building the capacities of partners and holding quarterly meetings with stakeholders in the health and nutrition sector will increase ownership of the nutrition activities and facilitate the hand-over. The capacity-building includes standard training and supervision and exchange meetings.
6
30. To improve livelihoods and minimize the risk of relapse, PLHIV will be referred to organizations that support social and economic integration through income-generating activities.
BENEFICIARIES AND TARGETING 31. The PRRO targets four groups of beneficiaries: i) children aged 6–59 months;
ii) pregnant and lactating women; iii) PLHIV; and iv) TB patients. These beneficiaries will be assisted according to criteria developed during implementation of the strategy.
32. Children aged 6–59 months with a weight/height index of ≥70 percent and <80 percent of the average will be regarded as moderately malnourished. Testing will be conducted at health centres under the advanced strategy.10 Community health volunteers will refer cases to health centres on the basis of mid-upper arm circumference (MUAC) of ≥110 mm and <120 mm. A moderately malnourished child will be regarded as treated on attaining a weight/height index of 85 percent at two consecutive weigh-ins. To reduce the risk of relapse, such children will receive food assistance for a further three months. As a further and separate intervention during lean seasons, food supplements will be distributed to all children aged 6–24 months in at-risk areas, irrespective of their nutritional status.
33. Food assistance for women will target pregnant and lactating women with a MUAC of <210 mm. Malnourished women will be identified at pre-natal and post-natal visits and at medical checks of children at health centres and through the advanced strategy by community health volunteers. Women will receive food assistance for six months. The criterion for lactating women will be a body mass index (BMI) of ≥ 18.5; the criterion for pregnant women will be defined as underweight of children at birth.
34. Food assistance for PLHIV will targets patients on anti-retroviral therapy (ART) and people registered in a PMTCT programme whose MUAC is <210 mm. Cases will be tested and managed in hospitals and district health centres for six months, after which cases with a MUAC of ≥ 230 mm will be regarded as having recovered.
35. In the three components above, cases that do not meet discharge criteria at the end of the planned period will be regarded as not responding to treatment and will be investigated to identify the causes.
36. Food assistance for people affected by TB targets those with a MUAC of <210 mm. Cases will be tested and managed at hospitals and district health centres. Patients will be regarded as having recovered if their MUAC is ≥230 mm at two consecutive visits. TB patients will receive an individual ration for the six months of DOTS with a view to increasing access.
37. The communications activities related to nutritional education will target the beneficiaries of the four components and 5 percent of women of reproductive age in the target areas.
38. Geographical mapping will be based on areas covered by PRRO 10452.0 and will be in line with the UNICEF nutrition programme. This targeting aims primarily to consolidate the achievements of PRRO 10452.0, covering the regions of Kayes,
10 The advanced strategy is a tool for detecting nutritional problems. Once a month, heads of health centres visit the villages covered to carry out vaccinations, at which time they weigh and inspect children to detect new cases of malnutrition.
7
Koulikoro, Ségou, Mopti, Gao, Timbuktu and Kidal; to ensure synergy with UNICEF, the region of Sikasso will also be considered.
39. Extension of HIV and TB coverage will follow the expansion of care units. A survey of household food security is being considered for Bamako with a view to integrating it into the HIV and TB component.
40. In 2009, assistance from WFP will ensure coverage of 60 percent of the anticipated cases of malnutrition among children 6–59 months, pregnant and lactating women and TB patients and 30 percent of PLHIV in ART or PMTCT programmes. The food assistance associated with nutritional education provided to adolescent girls and mothers should help to reduce the number of beneficiaries in 2010. The coverage rate for HIV and TB will remain the same throughout the PRRO. Rations will be distributed to target groups in line with the national protocols.
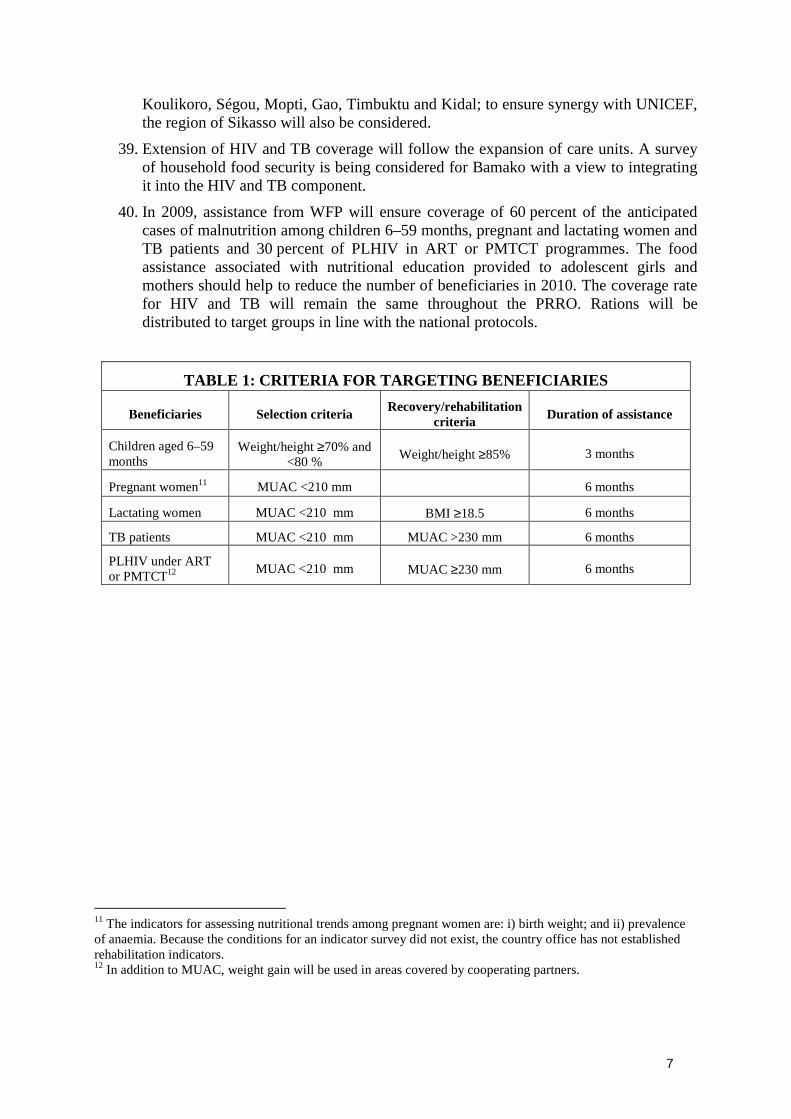
TABLE 1: CRITERIA FOR TARGETING BENEFICIARIES
Beneficiaries Selection criteria Recovery/rehabilitation criteria Duration of assistance
Children aged 6–59 months
Weight/height ≥70% and <80 % Weight/height ≥85% 3 months
Pregnant women11 MUAC <210 mm 6 months
Lactating women MUAC <210 mm BMI ≥18.5 6 months
TB patients MUAC <210 mm MUAC >230 mm 6 months
PLHIV under ART or PMTCT12 MUAC <210 mm MUAC ≥230 mm 6 months
11 The indicators for assessing nutritional trends among pregnant women are: i) birth weight; and ii) prevalence of anaemia. Because the conditions for an indicator survey did not exist, the country office has not established rehabilitation indicators. 12 In addition to MUAC, weight gain will be used in areas covered by cooperating partners.

8
TABLE 2: BENEFICIARIES IN 2009, BY CATEGORY AND REGION13
Region PopulationChildren
6–59 months
Pregnant/ lactating women
HIV TB Adol. girls14 Mothers14
Children 6–24
months*Total
Kayes 1 791 438 34 310 9 280 1 248 1 542 7 524 4 803 7 434 66 141
Koulikoro 2 047 172 41 787 10 318 2 444 1 763 8 598 5 850 8 496 79 256
Sikasso 2 323 063 46 248 13 009 1 387 2 000 8 757 6 475 9 641 87 516
Ségou 2 183 848 40 174 10 777 2 825 1 880 8 314 5 624 9 063 78 658
Mopti 1 927 249 30 840 7 218 2 685 1 659 8 094 4 318 7 998 62 812
Gao 514 365 11 277 2 736 563 443 2 160 1 579 25 615 44 374
Timbuktu 621 524 12 921 3 198 309 535 2 610 1 809 30 952 52 335
Kidal 55 244 1 893 271 33 48 255 265 2 751 5 516
Bamako 1 324 747 -- -- 2 504 1 141 -- -- -- 3 645
Total, 2009 12 788 652 219 450 56 806 13 998 11 011 46 314 30 723 101 950 480 252
* Targeted general food distribution during lean seasons to children under 3 years
TABLE 3: BENEFICIARIES IN 2010, BY CATEGORY AND REGION
Region PopulationChildren
6–59 months
Pregnant/lactating women
HIV TB Adol. girls14 Mothers14
Children 6–24
months*Total
Kayes 1 830 850 30 055 8 129 1 275 1 351 5 932 3 107 6 838 56 687
Koulikoro 2 092 210 36 605 9 038 2 498 1 544 6 779 3 393 7 814 67 672
Sikasso 2 374 170 40 513 11 396 1 417 1 752 7 692 3 862 8 868 75 500
Ségou 2 231 893 35 192 9 441 2 887 1 647 7 231 2 223 8 336 66 958
Mopti 1 969 649 27 016 6 323 2 744 1 454 6 382 2 442 7 357 53 716
Gao 525 681 9 879 2 397 575 388 1 703 992 23 997 39 932
Timbuktu 635 198 11 319 2 801 316 469 2 058 1 158 28 997 47 118
Kidal 56 460 1 659 237 34 42 183 199 2 577 4 930
Bamako 1 353 892 -- -- 2 560 999 -- -- -- 3559
Total 2010 13 070 002 192 238 49 762 14 306 9 646 37 960 17 376 94 784 416 072GRAND TOTAL
2009–2010 411 688 106 569 28 304 20 657 84 274 48 099 196 735 896 324
* Targeted general food distribution during lean seasons to children under 2 years. Source: National Division for Population Affairs, National Directorate of Statistics and Data Processing, 2006, Bamako, Mali. Populations updated with an annual growth rate of 2.2 percent.
13 The estimated number of beneficiaries is a function of the prevalence rate in each region for target components. 14 Participation in nutritional education.
9
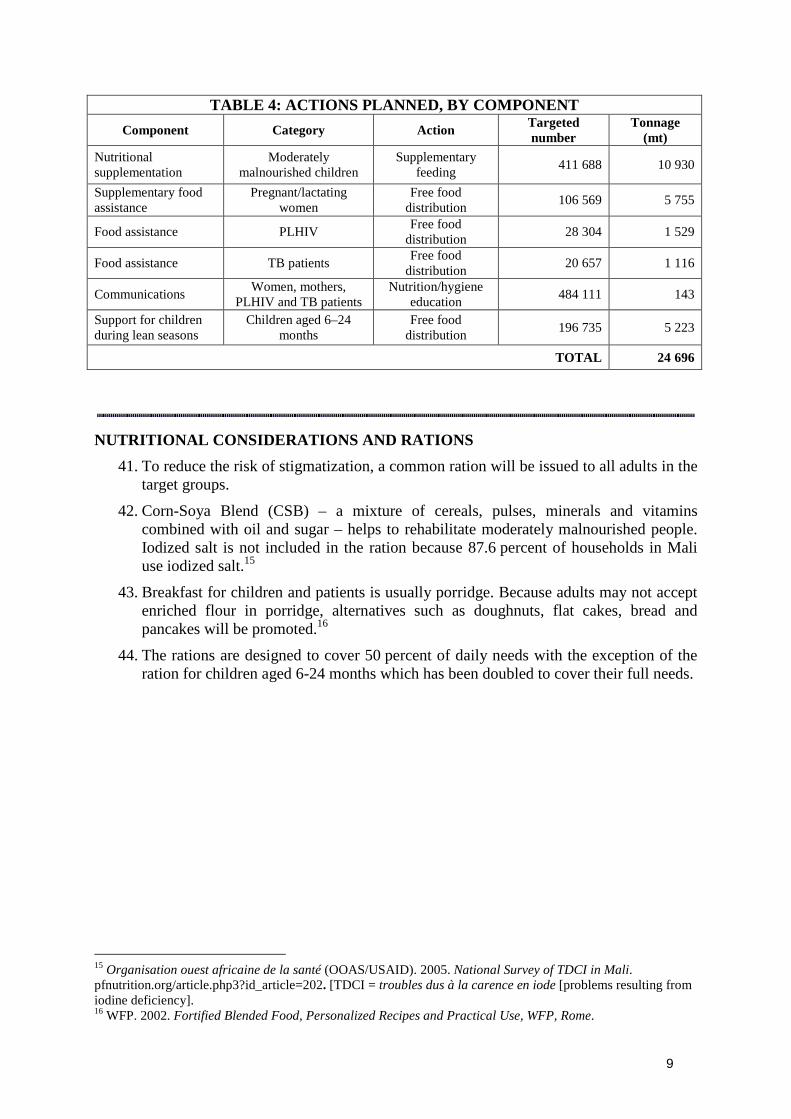
TABLE 4: ACTIONS PLANNED, BY COMPONENT Component Category Action Targeted
number Tonnage
(mt) Nutritional supplementation
Moderately malnourished children
Supplementary feeding 411 688 10 930
Supplementary food assistance
Pregnant/lactating women
Free food distribution 106 569 5 755
Food assistance PLHIV Free food distribution 28 304 1 529
Food assistance TB patients Free food distribution 20 657 1 116
Communications Women, mothers, PLHIV and TB patients
Nutrition/hygiene education 484 111 143
Support for children during lean seasons
Children aged 6–24 months
Free food distribution 196 735 5 223
TOTAL 24 696
NUTRITIONAL CONSIDERATIONS AND RATIONS 41. To reduce the risk of stigmatization, a common ration will be issued to all adults in the
target groups.
42. Corn-Soya Blend (CSB) – a mixture of cereals, pulses, minerals and vitamins combined with oil and sugar – helps to rehabilitate moderately malnourished people. Iodized salt is not included in the ration because 87.6 percent of households in Mali use iodized salt.15
43. Breakfast for children and patients is usually porridge. Because adults may not accept enriched flour in porridge, alternatives such as doughnuts, flat cakes, bread and pancakes will be promoted.16
44. The rations are designed to cover 50 percent of daily needs with the exception of the ration for children aged 6-24 months which has been doubled to cover their full needs.
15 Organisation ouest africaine de la santé (OOAS/USAID). 2005. National Survey of TDCI in Mali.pfnutrition.org/article.php3?id_article=202. [TDCI = troubles dus à la carence en iode [problems resulting from iodine deficiency]. 16 WFP. 2002. Fortified Blended Food, Personalized Recipes and Practical Use, WFP, Rome.

10
TABLE 5: FOOD RATIONS, PER PERSON/DAY, BY COMPONENT Ration Nutritional composition
Component Food Duration (days) (g) Energy
(kcal) Protein
(g) Lipids
(g)
CSB 250 950 45 15
Oil 25 221 -- 25
Sugar 20 80 -- --
Supplementary nutritional for
children Total
90
295 1 251 45 40
14% 29%
CSB 150 570 27 9
Oil 20 177 -- 20
Sugar -- -- -- --
Cereals 100 335 -- 3
Pulses 30 100.5 6.6 0.42
Food assistance for pregnant and
lactating women
Total
180
280 1 182.5 33.6 32.42
11.4% 24.7%
CSB 150 570 27 9
Oil 20 177 -- 20
Sugar -- -- -- --
Cereals 100 335 -- 3
Pulses 30 100.5 6.6 0.42
Food assistance for
PLHIV
Total
180
280 1 182.5 33.6 32.42
11.4% 24.7%
CSB 150 570 27 9
Oil 20 177 -- 20
Sugar -- -- -- --
Cereals 100 335 -- 3
Pulses 30 100.5 6.6 0.42
Food assistance for TB patients
Total
180
280 1 182.5 33.6 32.42
11.4% 24.7%
CSB 250 950 45 15
Oil 25 221 -- 25
Sugar 20 80 -- --
Assistance for nutritional education
Total
1*
295 1 251 45 40
14% 28% * Daily ration per participant in culinary demonstration sessions.

11
IMPLEMENTATION ARRANGEMENTS Participation
45. Implementation of PRRO 10610.0 is aligned with current decentralization processes in Mali and with the work of the food security and nutrition committees. At the national level, coordination will be handled by a steering committee of WFP, ministries, the Commission for Food Security, bilateral and multilateral donors, and national and international cooperating partners. The Ministry of Foreign Affairs will chair the committee.
46. Women will have an important role in distributing food for all the components. Awareness-raising through the communications component will promote the involvement of women and will reinforce their presence in decision-making positions on the food distribution committees.
Partners 47. PRRO 10610.0 will be implemented in partnership with government departments,
cooperating partners and United Nations agencies under the leadership of the steering committee.
48. The Nutrition Division of the Ministry of Health coordinates nutrition management at the national level and leads the working sessions of the nutrition group. A national coordinator in the Division liaises with WFP and other divisions within the Ministry of Health, and is involved in the design of the project document.
49. At the regional level, nutrition actors meet periodically under the leadership of the Regional Health Directorate.
50. WFP’s implementing partners – international or national organizations with competence and/or comparative advantage in nutrition – will be responsible for implementing PRRO 10610.0. An MOU will be signed with each to outline roles, responsibilities and resource contributions; an implementation guideline prepared by WFP will provide operational details.
51. In the regions where cooperating partners have an agreement with UNICEF for health and nutrition activities targeting the same beneficiaries as WFP, the possibility of a tripartite agreement between WFP, UNICEF and the cooperating partner(s) will be explored.
52. An MOU between UNICEF and WFP integrates all aspects of malnutrition, ensures synergy and coordinates assistance to the Government. UNICEF will provide assistance in managing cases of severe and acute malnutrition, systematic treatment including the administration of micronutrients, training and the provision of anthropometric equipment and support for data collection. To promote harmonization and effectiveness, the same tools will be utilized by the Ministry of Health, UNICEF and WFP.
53. WFP and UNICEF activities will cover the same regions and districts. In the few cases where the two agencies do not implement a joint programme, they will work to promote the development of a comprehensive package. Joint monitoring and evaluation will be carried out, and advocacy will continue with a view to controlling acute malnutrition among children.
12
54. Community health associations will help to raise awareness and involve communities in tracking cases of malnutrition by appointing and supporting volunteers; and transporting food closer to beneficiaries’ villages.
Non-Food Items (NFIs) 55. WFP, donors, partners and communities will provide funding for NFIs required for
PRRO 10610.0, which include:
� equipment such as Shakir strips17 and measuring devices for identifying and monitoring malnourished people;
� teaching materials such as textbooks and pictures for health and nutrition education;
� scales and measuring equipment for ration distribution and culinary demonstrations;
� registers, cards and report forms for management and monitoring; and
� pallets for the storage of food.
Negative Environmental Impact 56. Actions planned under PRRO 10610.0 do not have a negative environmental impact.
The cooking of enriched porridge requires very little energy.
Logistics 57. WFP food purchased on international markets or received as in-kind donations will
continue to be shipped to Lomé in Togo, Dakar in Senegal and ports in other countries for transport by a WFP-approved forwarding agent to regional warehouses in Mopti, Gao, Timbuktu, Kidal, Bamako and Kayes and onwards with local transporters to final delivery points. Most of the food warehouses have been made available to WFP by the Government. The Office des Produits Agricoles du Mali (OPAM; Mali Agricultural Products Board), which is an entity of the Comissariat à la Sécurité Alimentaire (CSA; Commission for Food Security) and in charge of managing the Stock Nationale de Sécurité Alimentaire (SNS; National Food Security Stock), has a storage capacity of 135,000 mt. WFP will temporarily rent some of the warehouses should the need arise.
58. Offloading charges in ports, storage and delivery will be the responsibility of WFP, and are included in the budget. Landside Transport, Storage and Handling (LTSH) is estimated at US$326.80/mt.
59. WFP has its country office and five sub-offices in the target areas, which ensure smooth logistics operations particularly with regard to internal transport, storage and handling (ITSH). Staff in the sub-offices and warehouses receive food, store it and deliver it to institutions for distribution to beneficiaries, in collaboration with cooperating partners and health services.
17 A simple technology for obtaining MUAC measurements.

13
Local Purchases and WFP’s Operational Responsibilities 60. Under the P4P initiative, some of the cereals will be purchased locally from
smallholders, depending on the availability of cereals from October to December each year.
PERFORMANCE MONITORING 61. Under the leadership of the Ministry of Foreign Affairs, the PRRO steering committee
will organize committee meetings every six months to assess progress in implementation and make recommendations for improvement.
62. Internal and external approaches will be used to monitor performance. The internal monitoring system will conform with results-based management standards and will include a mid-term review in March 2010. External monitoring will be conducted by the CSA and partners. Food and nutritional data will be collected and processed under a regular monitoring process.
63. WFP sub-offices and operational partners will monitor activities and food distribution in line with the performance indicators; information will be loaded into a database to facilitate assessment. Data from sub-offices will be centralized and analysed by the country office.
64. The number of PLHIV beneficiaries will be tracked using medical files. To protect privacy, names will not be captured in the system.
RISK ASSESSMENT AND CONTINGENCY PLANNING Risk Assessment
65. The main risks are: i) difficulties related to timely mobilization and availability of resources; and ii) difficulties in mobilizing target communities and ensuring their full buy-in and ownership.
66. Food insecurity and moderately acute malnutrition are likely to worsen if action is not taken quickly. Populations already affected by structural food insecurity and weakened by the economic crisis are likely to sink into the vicious cycle of severe poverty, including severe malnutrition and asset depletion.
Contingency Planning 67. A contingency plan is being developed at the country office level to integrate the
increase in food prices in all programme areas and cover disaster preparedness and response.
SECURITY CONSIDERATIONS 68. Mali is in United Nations security phase zero, except for the regions of Kidal
(phase 3), Gao (phase 2) and Timbuktu (phase 1).
69. Some of the northern regions targeted by PRRO 10610.0 are affected by criminal acts outside towns such as car-jackings and theft by armed bandits who are sometimes violent. For this reason, WFP vehicles in these regions are equipped with radios and
14
global positioning systems. WFP staff has received United Nations advanced security training; support staff will also receive United Nations security training.
70. Security companies will be contracted to oversee the safety of stocks and equipment in warehouses. The budget for PRRO 10610.0 takes these security-related costs into account.
APPROVAL
...................................................……. Date: .....................................
Josette Sheeran Executive Director

15
ANNEX I-A
BREAKDOWN OF PROJECT COSTS
Quantity (mt)
Average cost/mt (US$)
Value (US$)
WFP COSTS
Direct operational costs
Food
CSB1 18 010 588 10 589 880
Oil 1 941 1 525 2 960 025
Sugar 1 105 500 552 500
Cereals 1 400 480 672 000
Maize flour 1 400 450 630 000
Pulses 840 625 525 000
Total food 24 696 15 929 405
External transport 3 059 305
- Landside Transport 5 056 012
- ITSH 3 014 641
Total LTSH 8 070 633
Other Direct Operational Costs 940 880
A. Total Direct Operational Costs 28 000 223
B. Direct Support Costs2 (see Annex 1-B) 2 605 734
C. Indirect Support Costs (7.0 percent)3 2 142 417
TOTAL WFP COSTS 32 748 374
1 This is a notional food basket for budgeting and approval purposes. The contents may vary. 2 Indicative figure for information purposes. The direct support costs allotment is reviewed annually. 3 The indirect support cost rate may be amended by the Board during the project.
16
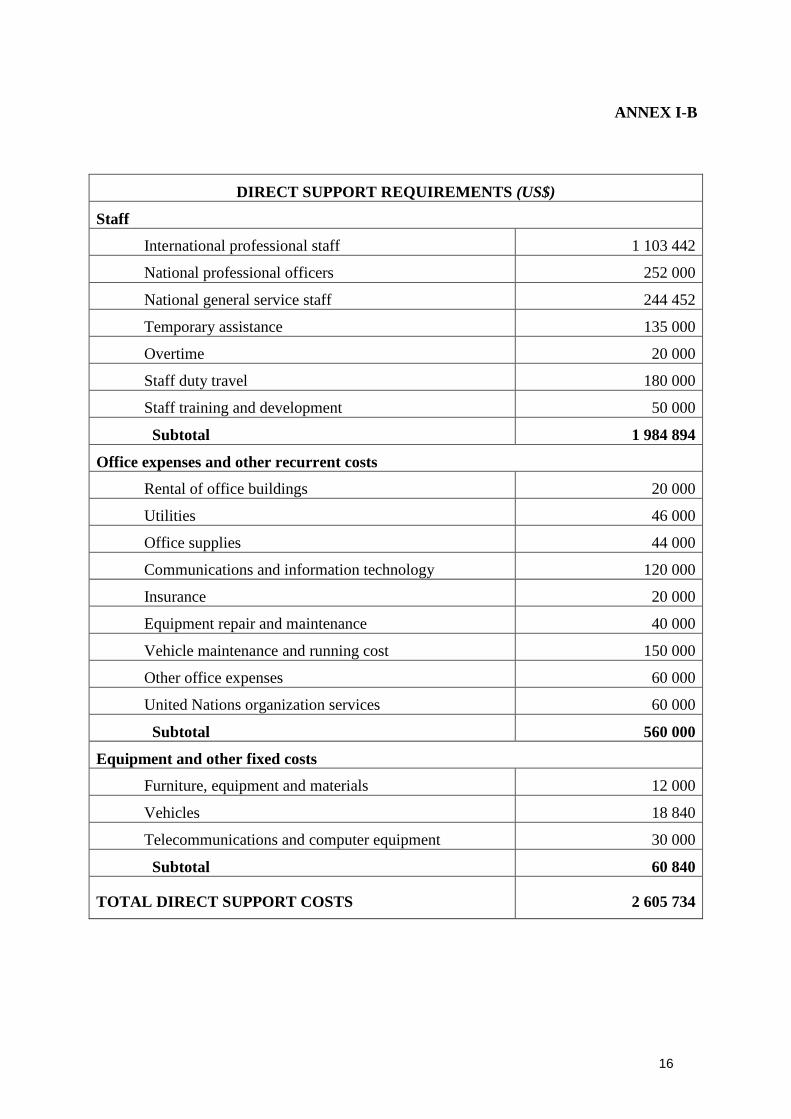
ANNEX I-B
DIRECT SUPPORT REQUIREMENTS (US$)
Staff
International professional staff 1 103 442
National professional officers 252 000
National general service staff 244 452
Temporary assistance 135 000
Overtime 20 000
Staff duty travel 180 000
Staff training and development 50 000
Subtotal 1 984 894
Office expenses and other recurrent costs
Rental of office buildings 20 000
Utilities 46 000
Office supplies 44 000
Communications and information technology 120 000
Insurance 20 000
Equipment repair and maintenance 40 000
Vehicle maintenance and running cost 150 000
Other office expenses 60 000
United Nations organization services 60 000
Subtotal 560 000
Equipment and other fixed costs
Furniture, equipment and materials 12 000
Vehicles 18 840
Telecommunications and computer equipment 30 000
Subtotal 60 840
TOTAL DIRECT SUPPORT COSTS 2 605 734
17
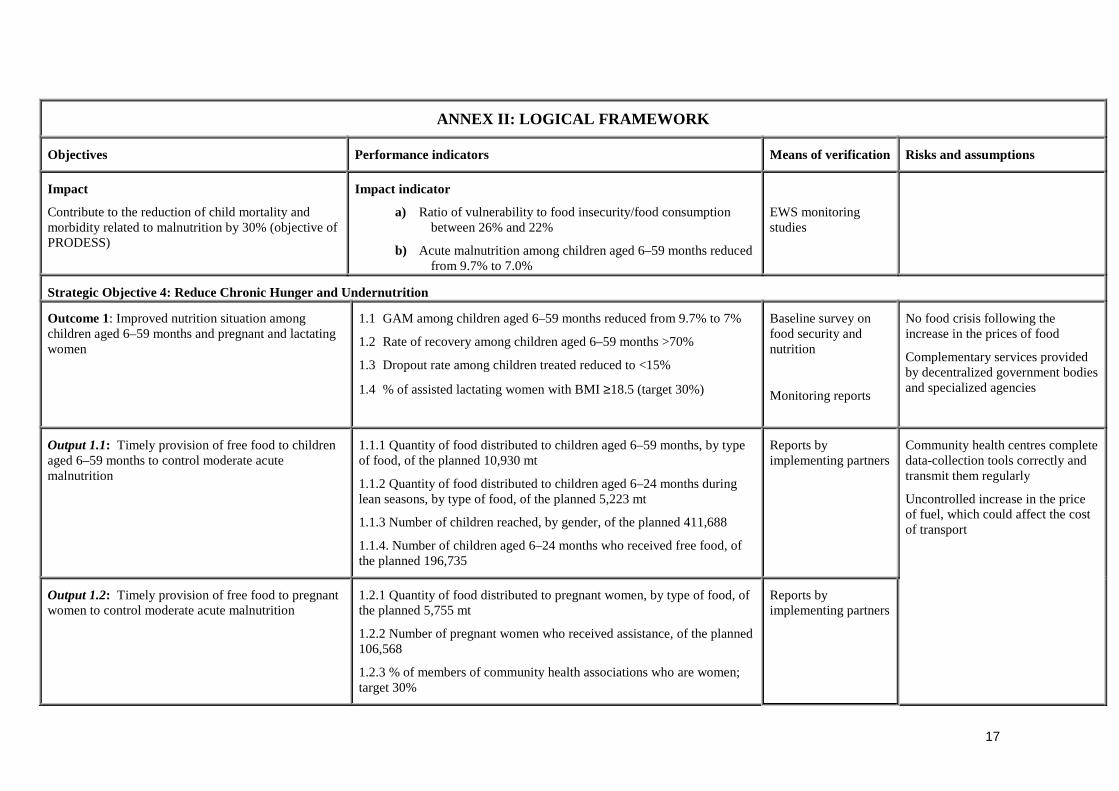
ANNEX II: LOGICAL FRAMEWORK
Objectives Performance indicators Means of verification Risks and assumptions
Impact
Contribute to the reduction of child mortality andmorbidity related to malnutrition by 30% (objective ofPRODESS)
Impact indicator
a) Ratio of vulnerability to food insecurity/food consumptionbetween 26% and 22%
b) Acute malnutrition among children aged 6–59 months reducedfrom 9.7% to 7.0%
EWS monitoringstudies
Strategic Objective 4: Reduce Chronic Hunger and Undernutrition
Outcome 1: Improved nutrition situation amongchildren aged 6–59 months and pregnant and lactatingwomen
1.1 GAM among children aged 6–59 months reduced from 9.7% to 7%
1.2 Rate of recovery among children aged 6–59 months >70%
1.3 Dropout rate among children treated reduced to <15%
1.4 % of assisted lactating women with BMI ≥18.5 (target 30%)
Baseline survey onfood security andnutrition
Monitoring reports
No food crisis following theincrease in the prices of food
Complementary services providedby decentralized government bodiesand specialized agencies
Output 1.1: Timely provision of free food to childrenaged 6–59 months to control moderate acutemalnutrition
1.1.1 Quantity of food distributed to children aged 6–59 months, by typeof food, of the planned 10,930 mt
1.1.2 Quantity of food distributed to children aged 6–24 months duringlean seasons, by type of food, of the planned 5,223 mt
1.1.3 Number of children reached, by gender, of the planned 411,688
1.1.4. Number of children aged 6–24 months who received free food, ofthe planned 196,735
Reports byimplementing partners
Output 1.2: Timely provision of free food to pregnantwomen to control moderate acute malnutrition
1.2.1 Quantity of food distributed to pregnant women, by type of food, ofthe planned 5,755 mt
1.2.2 Number of pregnant women who received assistance, of the planned106,568
1.2.3 % of members of community health associations who are women;target 30%
Reports byimplementing partners
Community health centres completedata-collection tools correctly andtransmit them regularly
Uncontrolled increase in the priceof fuel, which could affect the costof transport
18
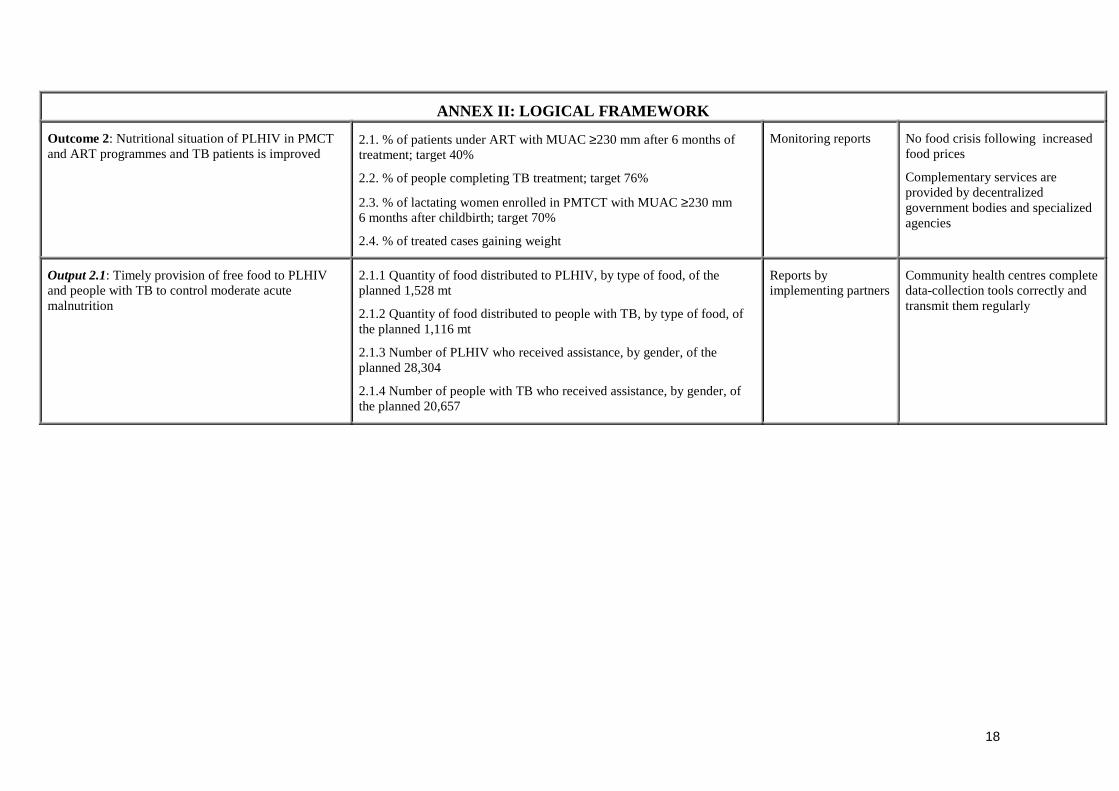
ANNEX II: LOGICAL FRAMEWORK
Outcome 2: Nutritional situation of PLHIV in PMCTand ART programmes and TB patients is improved
2.1. % of patients under ART with MUAC ≥230 mm after 6 months oftreatment; target 40%
2.2. % of people completing TB treatment; target 76%
2.3. % of lactating women enrolled in PMTCT with MUAC ≥230 mm6 months after childbirth; target 70%
2.4. % of treated cases gaining weight
Monitoring reports No food crisis following increasedfood prices
Complementary services areprovided by decentralizedgovernment bodies and specializedagencies
Output 2.1: Timely provision of free food to PLHIVand people with TB to control moderate acutemalnutrition
2.1.1 Quantity of food distributed to PLHIV, by type of food, of theplanned 1,528 mt
2.1.2 Quantity of food distributed to people with TB, by type of food, ofthe planned 1,116 mt
2.1.3 Number of PLHIV who received assistance, by gender, of theplanned 28,304
2.1.4 Number of people with TB who received assistance, by gender, ofthe planned 20,657
Reports byimplementing partners
Community health centres completedata-collection tools correctly andtransmit them regularly

19
Outcome 3: Improved nutrition knowledge amongtarget groups and relatives.
3.1 Increased knowledge among target groups about the utility of varioustypes of food
Information,Education andCommunications book
Tools to support IEC activities arenot available
No difficulty in the mobilization oftarget communities, their buyinginto the principles of theprogramme and their ownership
Output 3.1: Timely provision of free food to targetgroups for nutrition education
3.1.1 Quantity of food distributed to target groups, by food type, of theplanned 143 mt
3.1.2 Number of mothers or tutors who attended education sessions, of theplanned 48,099
3.1.3 Number of pregnant and lactating women who attended the sessions,of the planned 106,569
3.1.4 Number of PLHIV, disaggregated by gender, who attended thesessions, of the planned 28,304
3.1.5 Number of people with TB, by gender, who attended the sessions, ofthe planned 20,657
3.1.6 Number of women of reproductive age who attended the sessions, ofthe planned 84,274
3.1.7 Number of nutritional education sessions and cookingdemonstrations of 30,240 planned
Reports byimplementing partners
Community health centre stafforganize regular nutritionaleducation sessions
Baseline assumption: Donorssupport PRRO 10610.0.

20
ANNEX III - Map

Acronyms used in the document ART Anti-retroviral therapy
BMI Body mass index
CSA Comissariat à la Sécurité Alimentaire (Commission for Food Security)
CSB Corn-Soya Blend
CSCRP Cadre Stratégique pour la Croissance et la Réduction de la Pauvreté (Strategic Framework for Growth and Poverty Reduction)
DOTS Directly Observed Treatment Short-Course
EDSM IV Enquête démographique et de santé au Mali (Mali Demographic and Health Survey)
EWS Early Warning System
GAM Global acute malnutrition
HKI Helen Keller International
IEC Information, Education and Communications
ISBS Integrated Survey of STD/HIV and Behaviours
ITSH Internal Transport, Storage and Handling
LTSH Landside Transport, Storage and Handling
MDG Millennium Development Goal
MOU Memorandum of Understanding
MUAC Mid-Upper Arm Circumference
OMA Observatoire du Marché Agricole (Agricultural Market Observatory)
OOAS Organisation Ouest Africaine de la Santé (West African Health Organization)
OPAM Office des Produits Agricoles du Mali (Mali Agricultural Products Board)
PLHIV People living with HIV
PRODESS Programme de développement sanitaire et social (Health and Social Development Programme)
PSNAN Plan Stratégique Nationale pour l’Alimentation et la Nutrition (National Food and Nutrition Strategic Plan)
PMTCT Prevention of Mother-to-Child Transmission
SIAN Semaine d’Intensification des Activités de Nutrition (National Nutrition Week)
SNS Stock Nationale de Sécurité Alimentaire (National Food Security Stock)
TDCI Troubles dus à la carence en iode (problems resulting from iodine deficiency)





























