Embed Size (px)
Citation preview

MALARIAA MAJOR CAUSE OF CHILD DEATHAND POVERTY IN AFRICA

CONTROLLING THE MALARIA BURDEN IN AFRICA–KEY ACTIONS FOR UNICEF
n Strengthen UNICEF input to evidence-based antenatalservices
n Forge partnership with the Expanded Programme onImmunization for joint programming of insecticide-treatednets and intermittent preventive treatment (i.e., treatment ofinfants with an antimalarial drug linked to immunizationdelivery, currently under study)
n Provide Roll Back Malaria leadership to expand availabilityand coverage of insecticide-treated mosquito nets, includingforecasting and procurement
n Work with Roll Back Malaria partners to increase theavailability of artemisinin-based combination treatment (ACT)
n Offer continued UNICEF leadership in the monitoring andevaluation of Roll Back Malaria progress towards theMillennium Development Goals
n Work with Roll Back Malaria partners to coordinate effectivecountry programming support.
Cover photo: Spreading a cloth around her, her baby strapped to her side, awoman in the town of Xai-Xai, Gaza Province, Mozambique, prepares for homeafter a day’s work at the market.©UNICEF/HQ94-1280/PIROZZI

THE BURDEN OF MALARIAEvery year malaria, a parasitic disease spread by thebite of a mosquito, results in 300 million to 500 millionclinical cases and causes more than 1 million deaths.Mostly it is young children under the age of five in sub-Saharan Africa who are affected, dying at the rate ofnearly 3,000 every day. In Africa, malaria causesapproximately 20 per cent of all child deaths. Somechildren suffer an acute attack of cerebral malaria thatquickly leads to coma and death; others succumb to thesevere anaemia that follows repeated infections, or tothe consequences of low birthweight caused by malariainfection in the mother’s womb.
Those children who escape death are not untouched bythe disease. Malaria also hinders the development ofthose who survive. In sub-Saharan Africa, the disease isresponsible for 30 per cent to 50 per cent of alloutpatient visits to clinics and up to 50 per cent ofhospital admissions.
Malaria contributes to increased maternal morbidity andmortality. Malaria during pregnancy is the major cause of
1
©U
NIC
EF/H
Q00
-002
1/PI
ROZZ
IIn Africa, malariasickens and killsmany children like 16-month-oldSaid in the UnitedRepublic of Tanzania.
low birthweight in sub-Saharan Africa. The disease alsohas a crippling effect on the continent’s economic growthand perpetuates vicious cycles of poverty. It costs AfricaUS $10 billion to $12 billion every year in lost grossdomestic product – even though it could be controlled fora fraction of that sum.
RENEWED URGENCY TO ROLL BACK MALARIA
Africa is now at a critical stage in the struggle against adisease that saps its development. Without intervention,the crisis will deepen. But if national and global commitmentand support for the Roll Back Malaria initiative can beput into action on the ground, then the devastationbeing wrought by malaria can be reversed.
2
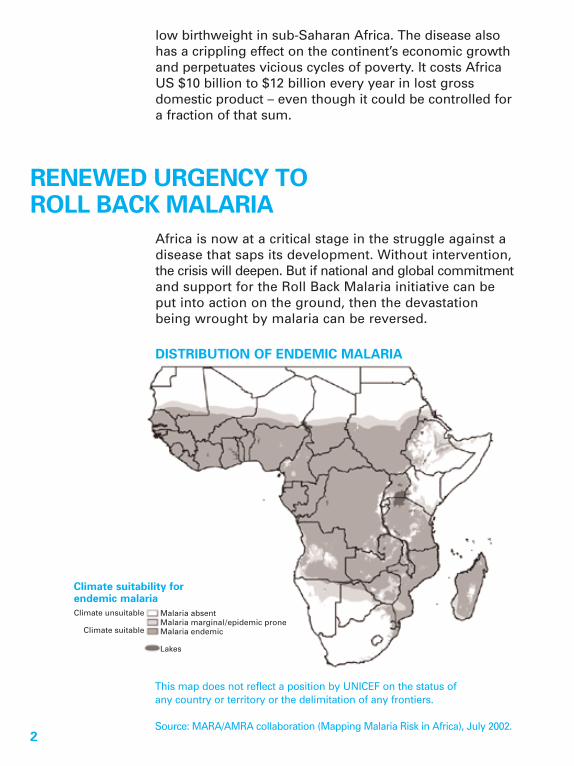
DISTRIBUTION OF ENDEMIC MALARIA
Climate suitability for endemic malariaClimate unsuitable
Climate suitable
Malaria absentMalaria marginal/epidemic proneMalaria endemic
Lakes
This map does not reflect a position by UNICEF on the status ofany country or territory or the delimitation of any frontiers.
Source: MARA/AMRA collaboration (Mapping Malaria Risk in Africa), July 2002.

The Roll Back Malaria Partnership was launched in 1998by the World Health Organization, the United NationsChildren’s Fund, the United Nations DevelopmentProgramme and the World Bank to galvanize globalsupport, mobilize resources and build partnerships toreduce the malaria burden. The partnership is nowfocusing its efforts at country and community levels tomake cost-effective interventions more readily availableto those at risk.
Governments and other Roll Back Malaria partners allknow what must be done. Goals and targets have beenagreed upon by the international community. UNICEF isfirmly committed to achieving the Millennium DevelopmentGoals of a two-thirds reduction in under-five childhoodmortality, and to halt and reverse the incidence of malariaby 2015. This will be done in accordance with the Abujamalaria summit targets for 2005:
n At least 60 per cent of those at risk from malaria,especially young children and pregnant women, tobenefit from the best use of insecticide-treated nets.
n At least 60 per cent of those suffering from malariato have access to effective and affordable treatmentwithin 24 hours.
n At least 60 per cent of pregnant women at risk frommalaria to have access to effective preventivetreatments.
WE HAVE THE TOOLS AT HANDWe have effective tools that can make a difference.Widespread use of insecticide-treated mosquito nets canreduce child mortality by 20 per cent. This mortalityreduction can be further improved by ensuring promptaccess to effective antimalarial treatment (preferablyACT). One new intervention that can bring quick resultsis the intermittent preventive treatment (IPT) of malariaduring pregnancy, which involves giving two or three
3
doses of an antimalarial drug, sulfadoxine-pyrimethamine (SP), during the second and thirdtrimesters of pregnancy. This will significantly reducethe proportion of low-birthweight infants and will alsoreduce maternal morbidity. The provision of intermittentpreventive treatment for infants, linked to the routineimmunization schedule, is now on the horizon.
However, serious challenges still exist. Many childdeaths occur at home, where families are withoutaccess to life-saving treatments or prevention. Andmalaria drug resistance is intensifying in many parts ofAfrica. Household use of insecticide-treated nets iscurrently low and there are many constraints to regularand timely re-treatment of these nets.
WIDESPREAD USE OF INSECTICIDE-TREATED NETS IS CRITICAL
One of the major breakthroughs of recent years is therealization that mosquito nets treated with insecticideprovide a much higher degree of protection againstmalaria than other nets. As well as stopping their
4
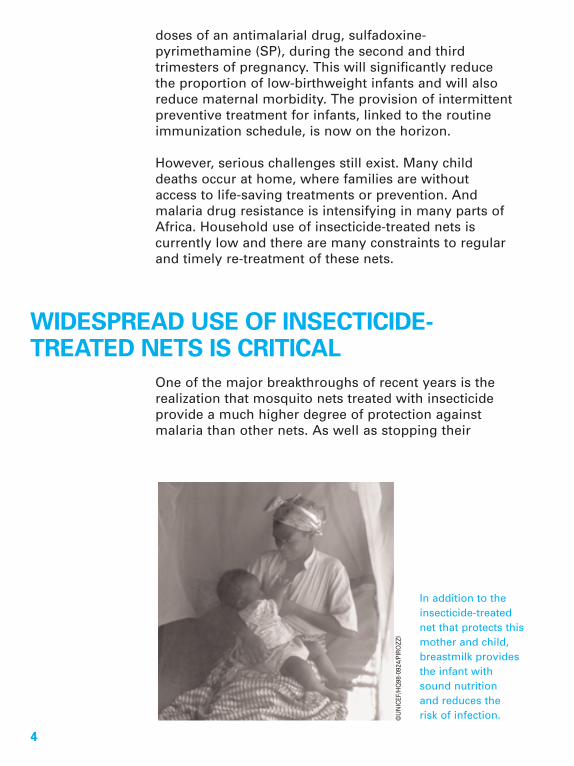
In addition to theinsecticide-treatednet that protects thismother and child,breastmilk providesthe infant withsound nutritionand reduces therisk of infection.©
UN
ICEF
/HQ
98-0
924/
PIRO
ZZI
bite, the treated nets kill mosquitos. Properly used,insecticide-treated nets can cut malaria transmission byat least 50 per cent and child deaths by 20 per cent.
The use of insecticide-treated nets during pregnancyprovides significant protection against maternalanaemia and low birthweight, major contributors toneonatal mortality. In addition, use of these netsbenefits the infants who sleep under them with theirmothers, by decreasing exposure to malaria infectionand subsequent severe disease.
However, by 2002 fewer than 5 per cent of sub-SaharanAfrican children were sleeping under insecticide-treatednets. And fewer than 15 per cent were sleeping underany net at all. At the present rate of progress, Africa willfail to reach the Abuja malaria targets.
The principal problem is the gap between what netscost and what families can and will pay for them.Research in Africa indicates that treated mosquito netsare too expensive for or are unavailable to the mostvulnerable: pregnant women, children under five yearsof age and the poorest families and communities.
UNICEF’S APPROACH TO INCREASING THE USE OF INSECTICIDE-TREATED NETS
UNICEF supports the distribution of insecticide-treatednets to vulnerable groups through targeted subsidies inorder to accelerate net usage in Africa and maximizepublic health benefits. In doing so:
n The aim is to ensure that all pregnant women, infantsand young children have use of insecticide-treatednets.
n Insecticide-treated nets must be made affordable,particularly for the most vulnerable groups.
5

n National health systems should initially strive toachieve high net usage by the most vulnerablegroups, while stimulating the private sector toproduce enough nets for future needs.
UNICEF lauds the new technology of long-lastinginsecticidal nets (LLINs), in which the insecticide isincorporated into the netting at the factory. The netcontinuously releases insecticide, repelling and killingmosquitoes for four to five years. UNICEF is workingwith partners to ensure that this technology is deployedas rapidly as possible, and that supplies of LLINs canbe increased to meet demand.
6
©U
NIC
EF/H
Q98
-092
2/PI
ROZZ
I
In Zambia, acommunity malariacommittee discussesthe value of inex-pensive, locallyavailable mosquitonets treated withinsecticide.

Strengthening antenatal care
As a part of effective antenatal care, the provisionof insecticide-treated nets can be combined withintermittent preventive treatment in partnership withnational reproductive health and Safe Motherhoodprogrammes. This would ensure the provision of anaffordable treated mosquito net to each pregnantwoman at her first antenatal visit, for use particularlythroughout pregnancy and during the lactating period.Newborn infants sleeping with their mothers willalso benefit during the vulnerable period of infancy.Since some 70 per cent of women in sub-SaharanAfrica receive antenatal care at least once during apregnancy, a high proportion of women can be reachedin this way.
Strengthening infant health
Overall strengthening of health services for youngchildren and collaboration with other key programmesfor child survival, such as the Expanded Programmeon Immunization, nutrition and the IntegratedManagement of Childhood Illness, are essential for aneffective malaria programme. Infant and child healthprevention programmes in malaria-endemic countriesemphasize that all infants should sleep under insecticide-treated nets, initially under the mother’s mosquito net.Mosquito net distribution can therefore also be linkedto routine childhood immunization programmes.UNICEF proposes that the prime caregiver be providedwith a treated mosquito net when routine childhoodimmunization takes place. This would ensure netcoverage for every child throughout infancy. In selectedinstances, distribution of insecticide-treated nets shouldbe linked to immunization campaigns. This has proveneffective in Ghana, Zambia and other countries.
To further reduce mortality from malaria, it is essentialto provide access to effective treatment within 24hours of illness and as close to home as possible,especially for young children. To ensure prompt andeffective malaria case management, the distribution of
7

8
ROLL BACK MALARIA PARTNERSHIPSFOR MOTHER AND CHILD HEALTH
Antenatal Child
Roll Back Malaria Intermittent preventivetreatment (IPT) withan antimalarial drug
Insecticide-treatedmosquito nets (ITNs)
Insecticide-treatedmosquito nets
Expanded Programmeon Immunization
Tetanus toxoid Child immunization
Nutrition Iron and folate Iron
Vitamin A
Breastfeeding
Prevention of mother-to-child transmissionof HIV
Screening
Antiretroviral drugs
Antiretroviral drugs
C-IMCI (Communitycomponent, IntegratedManagement ofChildhood Illness)
Community capacitydevelopment
Community capacitydevelopment
Home/Communitymanagement ofmalaria andpneumonia

pre-packaged antimalarial drugs (e.g., ACTs) at the time ofroutine immunization, for later home use, should also beconsidered.
Community capacity development
In developing countries, the majority of child deathsoccur in the home, so services must not focus only onclinics and hospitals. UNICEF’s approach includeshelping communities recognize and take effectiveaction against malaria. To reduce childhood death anddisease, partnerships need to be strengthened betweenhealth facilities and communities.
Re-treatment of nets
Until long-lasting insecticidal nets are more widelyavailable, strategies and plans must be in place toensure that existing nets are re-treated with an effective
9
©U
NIC
EF/H
Q99
-045
2/PI
ROZZ
I
At a hospital inRwanda, a nursedemonstrates howto treat a mosquitonet with insecticideto prevent malaria.

insecticide on a regular basis. Community-level healthworkers, trained volunteers, community groups orvillage health committees can distribute insecticidekits and ensure proper and timely re-treatment. Re-treatment should be free, if possible, as this hasbeen shown to result in higher re-treatment rates andoverall mosquito net usage.
CONCLUSIONUNICEF is committed to supporting countries inscaling up malaria prevention and control programmes.In addition to technical support, this includes theidentification of resource gaps, both human andfinancial, and helping to ensure that these gaps areaddressed. UNICEF has already assisted several Africancountries in making substantial progress to combatmalaria. The case studies on the following pagesillustrate the importance of strong commitment bygovernments and communities. These examples chartthe way forward for a broader regional effort againstthe disease.
10

11
CASE STUDIESBENINImproving malaria case management
In Benin, as in many other countries in sub-SaharanAfrica, some 70 per cent of child deaths are caused byfive preventable conditions: malaria, diarrhoea, measles,pneumonia and malnutrition. Malaria is the main causeof hospital visits and deaths of children under five. In1999, Benin introduced the Integrated Managementof Childhood Illness (IMCI) programme and choseOuémé District as the initial implementation site. IMCIprogrammes have three components: strengtheningthe national health system, improving the skills of healthworkers, and improving family and community practices.
StrategyThe Ministry of Health put in place a ManagementCommittee of IMCI partners, led by the Ministry’sSecretary-General. The United States Agency forInternational Development (USAID) funded many ofthe technical activities, UNICEF provided most of thelogistical support and WHO supported training andcapacity-building.
Results The main achievement was better case management ofmalaria by health workers, especially in the diagnosisof danger signs and referral of very sick patients tothe nearest health facilities. Steps are being taken toimprove family and community health practices,including use of insecticide-treated nets. Almost half thepopulation of Benin now benefits from the programme.
Lessons learnedThe most important lesson learned is that partnershipsbetween health ministries and WHO, USAID and UNICEFcan reduce the cost of IMCI programme implementation.This model can be used to improve community healthpractices and to strengthen links between communitiesand their national health systems.

MALAWIPromoting malaria prevention during pregnancy
Malaria is the leading cause of illness and death inMalawi and the most frequent cause of outpatientconsultations and hospital admissions. The majority of thepopulation lives in poverty, with almost 20 per cent ofchildren dying before the age of five. About 30 per cent of these deaths are caused by malaria. Approximatelytwo thirds of women are anaemic during pregnancy andup to 40 per cent of women pregnant for the first orsecond time have placental malaria at the time of delivery,resulting in an increased incidence of low birthweight andhigher neonatal and infant mortality rates.
StrategyMalawi was the first country in Africa to adopt sulfadoxine-pyrimethamine as the primary therapy for malaria. Thischange was necessitated by the high level of resistanceto chloroquine by the malaria parasites, leading tofrequent failure in treatment response. With UNICEFsupport, Malawi is scaling up the implementation ofintermittent preventive treatment to avoid infection with malaria by providing two doses of sulfadoxine-pyrimethamine to all pregnant women during thesecond and third trimesters. UNICEF is also supportingMalawi’s rapid expansion of the use of insecticide-treatednets by pregnant women and young children through distribution of subsidized nets at antenatal andmaternal/child health clinics.
ResultsA recent household survey in the town of Blantyreshowed increased use of intermittent preventivetreatment during pregnancy, a one-third reduction inplacental malaria infection, a reduction by half in thenumber of low-birthweight babies and a 35 per centreduction in the incidence of anaemia among mothers.
12

The Demographic and Health Survey in 2000 found that94 per cent of pregnant women made at least one visitto the antenatal clinic, and that 76 per cent of pregnantwomen received the first dose of intermittent preventivetreatment. However, only 37 per cent of women receiveda full two-dose course, indicating that further work isnecessary.
Lessons learnedSeveral factors have contributed to the widespread useof intermittent preventive treatment in Malawi. Theyinclude: development of a national policy on intermittentpreventive treatment by the Ministry of Health andPopulation; working closely with UNICEF, WHO, USAID,Population Services International and other Roll BackMalaria partners on programme implementation; highuse of antenatal care by pregnant women; increasedaccess to health information and services by communities;and a ten-week training course for Health SurveillanceAssistants, to enable them to serve as health agents intheir communities.
13

MOZAMBIQUECommunity capacity development and malaria control
Malaria is the number one cause of illness inMozambique, accounting for more than 40 per centof outpatient consultations, 60 per cent of paediatricinpatients and a third of hospital deaths. Poor, ruralcommunities tend to suffer the effects of malaria morethan urban communities because of greater numbersof infective mosquitoes, poor access to health care,inadequate knowledge of how to avoid malaria and itsrisks, and limited funds for prevention measures suchas insecticide-treated nets.
StrategyIn Zambézia and Gaza Provinces, UNICEF supports theimplementation of a community capacity developmentstrategy based on local participation. Communities areencouraged to analyse their health situation and maketheir own choices about appropriate tools to combatmalaria. A participatory tool kit has been developed toimprove knowledge about malaria, sanitation, hygieneand nutrition. UNICEF works with the Ministry of Healthand other partners to ensure that they have access toinsecticide-treated nets and appropriate drugs.
ResultsImplementation began in two districts of ZambéziaProvince and has since expanded to 12 districts. By theend of 2003, it will be in action throughout the province,which has a population of 3.5 million. There are now500 community councils, reaching some 400,000 people.Most councils have chosen insecticide-treated nets astheir preferred method of malaria prevention, andmore than 200,000 nets have been sold, resulting in anaverage net coverage rate of 37 per cent for pregnantwomen and 27 per cent for children. One hundred andtwenty five councils have achieved greater than 60 percent coverage of vulnerable groups.
14

After major floods in southern Mozambique in 2000,the Ministry of Health, UNICEF and several non-governmental partners distributed 200,000 nets freeof charge to affected families. Participatory approacheswere used to increase the community’s capacity torecognize the symptoms of malaria, identify risk groupsand correctly use and re-treat the nets. Over 250,000people in seven districts participated in activities toenhance community capacity development. A surveyconducted 10 months later revealed high levels ofknowledge about malaria and excellent net retention,with more than 97 per cent of the nets still in use.
Lessons learnedThe programmes in Zambézia and Gaza Provincesdemonstrate the benefits of a participatory approach tocommunity capacity development. Among populationswhere participatory processes were used, 93 per centcited insecticide-treated nets as a malaria preventionmethod as compared to only 15 per cent among thosewho attended theatre presentations where the netswere demonstrated. The use of insecticide-treated netscan be an important component of post-emergencyrehabilitation activities when distributed in conjunctionwith comprehensive participatory education.
15

UNITED REPUBLIC OF TANZANIAPreventing child deaths through malaria control
Malaria accounts for more than a quarter of all deathsof children under five in the United Republic ofTanzania. More than 31 million people are at risk ofmalaria infection, including 5.5 million children underfive years of age. Recent research has shown that theuse of insecticide-treated nets would effectively preventmalaria and reduce illness and death. In a rural pop-ulation of 60,000, the use of these nets was linked toa 27 per cent reduction in deaths of children aged fromone month to 4 years. Children sleeping regularly underinsecticide-treated nets were generally healthier andgrew better than those not using nets.
StrategyDuring the 1980s, mosquito nets were expensive ($10 to$15 each) and net usage was low. The United Republicof Tanzania was the first African country to remove taxesand tariffs on mosquito-netting materials, a major factorin the expansion of the net-production industry. Socialmarketing of insecticide-treated nets started on a smallscale in 1997 and now covers the whole country.Currently three manufacturing companies producemore than 4 million nets per year, enough to supply thelocal market and create a thriving export trade.
UNICEF supports malaria projects in two rural districts,Kibaha and Kilosa, with financial support from the UnitedKingdom National Committee for UNICEF. UNICEF worksclosely with the Ministry of Health to seek ways to reachthe most vulnerable members of the population. This hasincluded designing community-participation activities topromote the use of insecticide-treated nets by pregnantwomen and young children. These activities are ongoingand the results are promising.
Malaria prevention is one of many integrated initiativesin Kibaha and Kilosa and another five ‘Early ChildhoodDevelopment districts’. Village Child Health Days areheld monthly, children are immunized and weighed,
16

their weights are charted and discussed and caretakersare given advice on nutrition. During antenatal carevisits, pregnant women receive intermittent preventivetreatment to protect them against malaria and protecttheir unborn children against premature birth and lowbirthweight. The aim is to provide the most critical andaffordable interventions that maximize health benefitsfor women and young children.
ResultsBy 2002, the cost of a net in the United Republic ofTanzania had dropped to $3.50 and net coverage roseto 37 per cent of households: 71 per cent in urban areasand 10 per cent to 57 per cent in rural areas. Through theGlobal Fund to Fight AIDS, Tuberculosis and Malaria, the country has secured financial support for a nationalvoucher plan to distribute insecticide-treated nets to themost vulnerable groups: young children and pregnantwomen. The voucher plan will reduce, by about twothirds, the cost of mosquito nets for pregnant womenattending antenatal care services. The plan will alsoprovide free insecticide re-treatment kits to caregiverswho bring infants for routine immunization services.
Lessons learnedThe United Republic of Tanzania has shown that it ispossible to scale up the use of insecticide-treated netswithin a short period of time through the reduction oftaxes and tariffs on netting materials and insecticides;social marketing of nets, especially in rural areas; andthe use of vouchers for the most vulnerable groups –children and pregnant women. The use of antenatalclinics and Village Child Health Days has been veryeffective in promoting maternal and child health.
17
For more information on malariacontact the Health SectionProgramme Division(212) 326 7554
Published by theUnited Nations Children’s Fund (UNICEF)Division of Communication3 UN Plaza, H-9FNew York, NY 10017, [email protected]
©The United Nations Children’s Fund (UNICEF), New York
Reprinted October 2004





















![Malaria Journal BioMed Central - COnnecting REpositories · 2017. 4. 11. · malaria, up to half a billion clinical cases are reported each year [1] with an annual death rate of 2.7](https://img.dokumen.tips/doc/110x75/6091e69b8aa2fe179b03fc39/malaria-journal-biomed-central-connecting-repositories-2017-4-11-malaria.jpg)






![Kenneth E. Hagin - Redeemed From Poverty, Sickness, And Spiritual Death [1 eBook - PDF]](https://img.dokumen.tips/doc/110x75/5525d6e1550346446f8b4a40/kenneth-e-hagin-redeemed-from-poverty-sickness-and-spiritual-death-1-ebook-pdf.jpg)
