Embed Size (px)
Citation preview

Rick Pope MPAS, PA-C, DFAAPA, CPAAPA
Maine NP2017
Annual Conference
Joint injections
1:45-3:45 PM
Friday April 28th

Disclosures
Rick Pope PA-C, MPAS, DFAAPA, CPAAPA
No conflicts of Interest
Do any of you know what the CPAAPA
designation stands for?

What is the most common diagnosis for which joint injections are performed?
1. Trigger finger
2. Shoulder impingement syndrome
3. Trochanter bursitis
4. Low back pain (facet arthritis/disc disease)
5. Osteoarthritis knee

What is the most common diagnosis for which joint injections are performed?
1. Trigger finger
2. Shoulder impingement syndrome
3. Trochanter bursitis
4. Low back pain (facet arthritis/disc disease)
5. Osteoarthritis knee

What is the most important Dx not to miss when you see an effusion?
1. Acute Gout
2. Acute Pseudogout
3. Osteoarthritis
4. Septic arthritis
5. Lyme arthritis

What is the most important Dx not to miss when you see an effusion?
1. Acute Gout
2. Acute Pseudogout
3. Osteoarthritis
4. Septic arthritis
5. Lyme arthritis

Practice Type?
1. Are any of you in Primary Care/Family Practice?
2. Orthopedics?
3. Occupational Med?
4. Emergency/Urgent Care?
5. OPD subspecialty clinic?
6. Hospital based?
7. Others?

GOALS for participants
1. Review the disease states and conditions for which injections are appropriate.
2. Provide rationale for use of specific types of corticosteroid injectables with anesthetic mixture.
3. Review the indications and side effects of corticosteroids.
4. Demonstrate injection techniques both orthopedic and rheumatologic.
5. Be able to perform mock procedures on shoulder, elbow, hip, knee and trigger points on each other.
MY GOAL AS AN INSTRUCTOR
provide a safe participant oriented environment

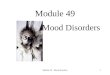
U.S. Prevalence* of Rheumatic Disorders1
2007, 2008, *2010 (ACR)
Reference: 1. Lawrence RC, et al. Arthritis Rheum. 1998;41:778-799. 2. Lawrence RC et all. Arthritis Rheum 2008;58:26-35
27
51.3 1.1
0
5
10
15
20
25
Cases(millions)
*Calculated by the National Arthritis Data Workgroup based on available surveys, such as the National Health and Nutrition
Examination Survey.
Inflammatory
Mildly inflammatory
*8.0
Arthritis and Rheumatism Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II 28
December 2007

Treatment of Knee OA
• Pt education
• Reach ideal body weight in those who are overweight
– Weight loss can result in significant decrease in symptoms
• Alter lifestyle behaviors, eg, overuse syndromes
• Mostly palliative to decrease pain, leading ideally to improved health-related quality of life
.

Treatment of Knee OA
• Analgesics/anti-inflammatory therapies
• Assistive devices to “unload” joints
• Cognitive behavior therapy
• Physical therapy and exercise therapy
• No proven structure-modifying therapies
• Recent data regarding metalloproteinase inhibitors suggests some benefit in patients with progressive disease

Principles for Knee Osteoarthritis management
• National guidelines from AAOS, ACR, and AGS1,3,4
–Exercise, weight loss relieve symptoms and
maintain function
–NSAIDs and tramadol preferred for most
patients
–Acetaminophen may be preferred for older
patients because of better safety profile
1. Hochberg MC, et al. Arthritis Care Res (Hoboken). 2012;64:465-474; 2. Centers for Disease Control and Prevention.
http://www.cdc.gov/arthritis/basics/osteoarthritis.htm. Updated May 16, 2014. Accessed July 11, 2014;
3. AAOS. Treatment of Osteoarthritis of the Knee: Evidence-Based Guideline. Rosemont, IL: AAOS; 2013;.
2. 4. AGS. J Am Geriatr Soc. 2009;57:1331-1346.
AAOS: American Academy of Orthopedic Surgeons
AGS: American Geriatric society

Treatment of OsteoarthritisPharmacolgic
Topical agentsLidocaine
Methylsalicylate (Ben Gay etc)
Bio-freeze™
Diclofenac gel/patch/lotion
Local InjectionsCorticosteroid Injections
Hyaluronic Injections (knee)

Injectables

Benefits of local corticosteroid injections
• Reduce inflammation
• Rapid reduction in pain
• Improve range of motion
• Prevent contracture
*In inflammatory conditions chondroprotective and may prevent or inhibit erosion of cartilage and bone

Benefits of aspirations and intra-articular steroid injection include:

Steroid Duration/Potency Dose/site
Hydrocortisone acetate Low/Short 10-25 mg for soft tissue and small
joints/ 50 mg for large joints
Methylprednisolone acetate
(Depo Medrol) Intermediate/Intermediate
2-10 mg for soft tissue and small
joints / 10-80 mg for large joints
Triamcinolone acetonide
(Aristocort, Kenalog)
Triamcinilone
Hexacetonide (Aristospan)
Intermediate/Intermediate
Long/High
2-10 mg for soft tissue and small
joints / 10-80 mg for large joints
Dexamethasone sodium
phosphate (Decadron) High/Long
0.5-3.0 mg for soft tissue and
small joints / 2-4 mg for large
joints
Betamethasone (Celestone
Soluspan) High/Long
1-3 mg for soft tissue and small
joints, 2-6 mg for large joints
Overview of steroid types
Duration , doses and site
Am Fam Physician 2002; 66: 283-8

Mechanism of action:Corticosteroid Injections
Purported to be a local anti-inflammatory?
Steroids locally in the joint have effects on:
edema
lymphocytes
macrophages
mast cells

Side Effects:Corticosteroid Injections
Infection (1 in 50,000 injections)¹
Post injection flare (2% crystal induced synovitis)¹
Skin hypopigmentation, subcutaneous atrophy¹
Vasovagal syncope (procedure related)¹
Tendon rupture (rare)¹
Osteonecrosis (rare)¹1. West, S Rheumatology Secrets 2rd edition 2002

Relative contraindications to injections
• superficial infection or broken skin
• unstable coagulopathy
• prosthetic joint (hemiarthroplasty can be injected)
Aspiration should be performed if
sepsis is suspected

Hyaluronic Acid Injections

Synovial Fluid
Acts as lubricant
Serves as shock absorber
Relieves pain
Retards inflammation
May support the synthesis of normal hyaluronic acid

Hyaluronic Acid Injectables(Knee Only)
EUFLEXXA™ 3
SYNVISC™ 3 or 1
HYALGAN ™ 5
SUPARTZ ™ 3
ORTHOVISC ™ 3
GEL ONE ™ 3
Once weekly forBranded names™

Why is HA usedto treat pain in O/A?
Cannot take NSAIDs
Will not take corticosteroid injections
Too young for total knee replacement
Not ready for total knee replacement
“nothing else has worked”
Early chondral problems in young patients

Common
injection sites
for corticosteroid injections
•Shoulder
•Trochanteric bursa
•Knee
•Trigger points

Uncommon
sites•HIP (guided)
•SIJ (guided)
•Achilles Tendon
•Infra-patellar Bursa
•TMJ
•Flexor Tendons
•Small joints of hands or feet

Tips for good procedures I•Beginners’ main problem;
Finding the right spot.
•Anatomy picture
for joints and think of referred patterns
Trigger points:
In general stick the needle where it hurts.
•Difficult to cause real
Damage except side of neck
or chest wall.

length vs. gauge
•The longer and thinner the needle,
The more flexible
•The shorter and larger the bore,
The more rigid
Larger needles for larger joints
Smaller needles for smaller joints
Needle choices

Tips for good procedures II
•Relaxed Patient
•Relaxed Operator

Tips for good procedures III
•Right hand injects
•Left hand supports
•Patient is foundation
•Left hand must be
anchored to patient

Tips for good procedures IV
•Pain caused by
rapid tissue invasion
•Introduce needle slowly
•Use smallest needle
possible
•Use smallest injectate
volume possible
•Pain should be no worse
than venipuncture

X-RAY view of the shoulder

Shoulder Anatomy


Posterior Shoulder Approach

Anterior Shoulder Approach

Lateral Epicondyle

Greater trochanterspinal needle
large volume

Hip jointGreater Trochanter

Posterior view right hip
Posterior trochanter
large area

Kneesuperior lateral approach
note knee extension

Kneemedial approach
aspiration or injection

Osteoarthritic fluid

Knee outline patella, patellar tendon, medial and
lateral tibial plateau
Courtesy of Michael Rudzinski

Lateral flexed knee approach Pt supine
Courtesy of Michael Rudzinski

Medial approach 90° flexed
Courtesy of Michael Rudzinski

Trigger Point Injections
Both lidocaine and saline injections result in clinical reductions in pain for headaches
Does dry needling
Help for soft tissue
and why?
White et al. Presented at: ACR; 2004. PECK; FMS

Fibromyalgia
PECK;FMS

Thank youQuestions?
Richard S. Pope MPAS, PA-C, DFAAPA, CPAAPA
If you would like the ppt
E-mail me at:


Questions for the audience
1. Do you participate in the process of quality review of your care with patient's?
2. Do you perform procedures in your practice?
3. What are the 3 most commonly perform procedures you do?
4. What are 3 procedures you would like to learn how to perform ?
5. Is your compensation from your employer
salary; productivity; or combination of both ?