Embed Size (px)
Citation preview

METABOLIC IMAGING - AMEDEO CHIRIBIRI
Introduction
Cardiac magnetic resonance (CMR) perfusion imaging is increasingly used to diagnose noninvasively the presence of coronary artery disease (CAD) and to plan revascularization pro-cedures [1].
The main advantages of CMR perfusion are the lack of radiation exposure, the excellent safetyprofile of the contrast agents and the capability of CMR perfusion to provide dynamic images ofmyocardial perfusion with a far better spatial resolution compared with other imaging modalities[2]. CMR perfusion has been shown to be superior to nuclear perfusion imaging [3], has been val-idated against microspheres [4–6] and invasive reference standards such as fractional flow reserve(FFR) [7–9], and therefore has the potential to become the non invasive test of choice to guide pa-tients’ clinical decision making.
Among the other advantages of CMR perfusion, the superior spatial resolution in particularplays an important role, and is thought to be the key factor explaining the superiority of CMRperfusion over nuclear perfusion imaging. Due to the complex interactions between coronary vas-culature and myocardium, myocardial ischemia arises from and affects more severely thesubendocardial layers of the left ventricular myocardium in comparison with the outer epicar-dial layers (Figure 1) [10, 11]. CMR perfusion is capable of an independent visualization of mul-tiple left ventricular layers [7, 12, 13], and therefore allows the identification of ischemia at its on-
Amedeo Chiribiri, Eike NagelKing’s College London BHF Centre of Excellence, NIHR Biomedical Research Centre and
Wellcome Trust and EPSRC Medical Engineering Centre at Guy’s and St Thomas’ NHS Foundation Trust, Division of Imaging Sciences and Biomedical Engineering, The Rayne Institute, London, UK
Correspondence: Dr Amedeo Chiribiri, Division of Imaging Sciences and Biomedical Engineering, The Rayne Institute – 4th Floor Lambeth Wing, St Thomas’ Hospital, London SE1 7EH, UK
email: [email protected]
AbstractCardiovascular magnetic resonance (CMR) is increasingly used to assess non-invasively the presence andthe extent of myocardial ischemia. CMR perfusion has been shown to be superior to nuclear perfusion im-aging, allows high-resolution quantitative assessment of myocardial perfusion reserve, has been validatedagainst invasive reference standards and microspheres and therefore has the potential to become the non-invasive and radiation-free test of choice to guide patients’ clinical decision making. The higher spatial res-olution of CMR is thought to be one the key factors explaining the superior diagnostic capabilities of CMRvisual assessment when compared with other ischemia imaging techniques.
Keywords: Adenosine; coronary disease; fractional flow reserve; high-resolution quantification; magneticresonance imaging; perfusion.
� Heart Metab; 2013;59:14–19
Magnetic resonance imaging perfusion toassess transmural flow distribution
14 Heart Metab. (2013) 59:14-19
Metab
olic I
magin
g
14_VA_1008_BA_INTERIEUR_Heart&Metabolism 21/05/13 23:52 Page14

set from the endocardium. This might conversely bemissed by lower spatial resolution techniques due topartial volume effects (Figure 2).
Regardless of the specific technical parametersused for the acquisition of the images, CMR perfusionallows a spatial resolution comparable or superior tonuclear medicine techniques. In recent years, oldersequences based on echo planar imaging, turbo gra-dient echo or steady state free precession have beenprogressively replaced by more advanced sequences
that exploit jointly the spatial and temporal k-space datacorrelations. One of these methods in particular, k-tsensitivity encoding, allows a net increase in the effi-ciency of acquisition and enables a considerable im-provement in spatial resolution [14], particularly at 3Tesla (Figure 3).
In comparison with standard perfusion sequences,high-resolution k-t CMR perfusion results in signifi-cantly improved image quality, signal-to-noise and con-trast-to-noise, and a significant reduction in the extent
Heart Metab. (2013) 59:14-19 15
METABOLIC IMAGING - AMEDEO CHIRIBIRI
Epicardial resistance (R1) Epicardial stenosis
Autoregulation(R2)
Epicardium
Endocardium
R2
R2
R2
R2
Myo
card
ial
cont
ract
ion
LV p
ress
ure
(R3
)
Fig. 1 Schematic representation of the left ventricular wall and of the coronary vessels. Coronary resistances can be categorized in epicar-dial (R1), arteriolar (R2) and phasic intramyocardial resistances (R3). Systolic contraction and left ventricular pressure are responsible for aprogressive increase of the resistance to myocardial perfusion from the epicardial to the endocardial layers due to the compression of smallerintramyocardial vessels. This imbalance is compensated in physiological conditions (left) by a proportional decrease of the autoregulatory re-sistances, located in the arteriolar R2 compartment. In areas of myocardium supplied by hemodynamically significant epicardial lesions (inred), a further increase in the total coronary resistances is due to the fixed increase in R1 epicardial stenosis, resulting in a full vasodilatationof the autoregulatory R2 compartment and in an insufficient compensation for systolic R3 increase, culminating in the onset of subendocar-dial ischemia. LV = left ventricular.
Dis
tanc
e fr
om L
V en
doca
rdiu
m (
mm
) Epicardium
Endocardium
SPECT4 x 4mm
TFE-CMR2.9 x 2.9
mm
PET3.3 x 3.3
mm
k-t 3Tesla-CMR1.2 x 1.2
mm
0
10
5
Fig. 2 Comparison between spatial resolution of positron emission tomography, single photon emission computed tomography, turbo gra-dient echo CMR and k-t 3 Tesla CMR. The capability of an imaging diagnostic technique to identify the presence of subendocardial ischemiais strictly dependent on its spatial resolution. CMR = cardiac magnetic resonance; LV = left ventricular; PET = positron emission tomogra-phy; SPECT = single photon emission computed tomography; TFE = turbo field echo.
14_VA_1008_BA_INTERIEUR_Heart&Metabolism 21/05/13 23:52 Page15

and transmurality of subendocardial dark-rim artifacts,supporting the use of advanced perfusion sequencesfor clinical perfusion imaging [15].
Analysis of high-resolution CMR perfusion
Visual assessment
Visual assessment of CMR perfusion is currently re-garded as the reference standard for the evaluation ofthe scans, and is mainly based on the spatial and tem-poral information of the CMR perfusion images. Severalfeatures in the images improve the confidence of theoperators in visual diagnosis and in particular the iden-tification of ischemic areas, which are predominantlysubendocardial and the characteristic epi to endocar-
dial wash-in of the contrast agent during first pass in ar-eas of abnormal perfusion (Table I).
An appreciable series of studies have validated vi-sual CMR assessment versus invasive coronary an-giography and other non invasive diagnostic tech-niques and invasive hemodynamic measurements [16].A recent meta-analysis of the literature [17] demon-strated an elevated diagnostic accuracy of CMR per-fusion with a sensitivity of 0.91 and specificity of 0.81at a patient level. More recently, the CE-MARC study[3], the largest clinical study on CMR published so far(752 patients) comparing a combined CMR protocol(stress and rest perfusion, functional analysis, lategadolinium enhancement and CMR coronary angiog-raphy) for the assessment of patients with suspectedCAD versus single photon emission computed to-mography and coronary angiography, demonstrated asensitivity and specificity of the CMR approach of 87%and 83%, respectively.
Quantification
A potential limitation of CMR visual assessment, how-ever, is the presence of balanced ischemia in patientswith three-vessel disease, in which the absence ofnormal reference segments can cause false negativeresults [18]. To overcome this limitation, quantitativeanalysis has been developed and validated [2, 19, 20].Myocardial perfusion reserve (MPR) can be assessedin an objective [18] and reproducible way [21] usingspecific contrast agent injection schemes [22] in com-bination with signal deconvolution [19]. Quantitative
16 Heart Metab. (2013) 59:14-19
METABOLIC IMAGING - AMEDEO CHIRIBIRI
Table 1 Visual assessment diagnostic criteria for CMR perfusion series, in view of the spatial and temporal resolution of CMR perfusion.
Diagnostic criterion Notes1. Delayed wash-in of the contrast agent in one or Strictly dependent on the elevated temporal resolution
more left ventricular segments of CMR perfusion and the possibility to visualize a dynamic series of the first-pass
2. TPG during wash-in of the contrast agent, with Strictly dependent on the spatial resolution of CMRmore delayed and reduced perfusion affecting the perfusion enabling the visualization of multiple inner left ventricular layers independent left ventricular transmural layers
3a. Exclusion of subendocardial dark-rim artifacts The presence and severity of these artifacts is inverselyproportional to the spatial resolution of the sequence
3b. Exclusion of subendocardial dark-rim artifacts Dark-rim artifacts usually appear when contrast agent arrives in the left ventricular cavity and before any signal increase in the left ventricular myocardium. This feature allows the identification of the artifacts from true perfusion defects and is based on the temporal resolution of CMR perfusion
CMR = cardiac magnetic resonance; TPG = transmural perfusion gradient.
Fig. 3 Comparison between 3 Tesla and 1.5 Tesla perfusion seriesfrom the literature (modified with permission from Plein et al [13]). k-t Sensitivity encoding accelerated cardiac magnetic resonance per-fusion images at 3 Tesla and 1.5 Tesla in a patient with three-vesseldisease and occluded right coronary artery. Both datasets containthe same diagnostic information, with an area of subendocardial is-chemia in the inferior left ventricular region and a transmural gradi-ent of perfusion. The image quality is superior at 3 Tesla. k-t SENSE= k-t sensitivity encoding.
14_VA_1008_BA_INTERIEUR_Heart&Metabolism 21/05/13 23:52 Page16

analysis has been validated against microspheres [5]and FFR [7], and has recently been shown to allow anaccurate assessment of patients with suspected CAD,providing comparable quantitative results to positronemission computed tomography [15].
However, until very recently, quantitative analysishas been used to analyze full-thickness myocardialsegments or to quantify MPR in the subendocardial halfof the myocardial wall, potentially neglecting importantinformation about the localization and the extent ofmyocardial ischemia. This restriction is responsible foran important limitation to the overall accuracy of quan-titative analysis when compared with visual assessment[23].
In order to overcome these limitations, methods forhigh-resolution voxel-wise quantification have recentlybeen developed and validated by our group [23], usinga novel hardware CMR perfusion phantom [24] and pa-tients’ data (on advanced high-resolution k-t scans)and by others [6] (on standard resolution turbo gradientecho scans) in comparison to microsphere experimentsin dogs and clinical data. Voxel-wise quantitative analy-sis allows the quantification of MPR while preserving theinformation about the extent, localization, and trans-murality of ischemia (ischemic burden; Figure 4). Com-bining the advantages of visual (high spatial resolution)and quantitative (more objective and reproducible) as-sessment, voxel-wise quantification has the potential toallow an improvement in the accuracy of detection ofCAD, as well as to provide novel and valuable informa-tion on the severity and extent of ischemia.
Transmural perfusion gradient analysis
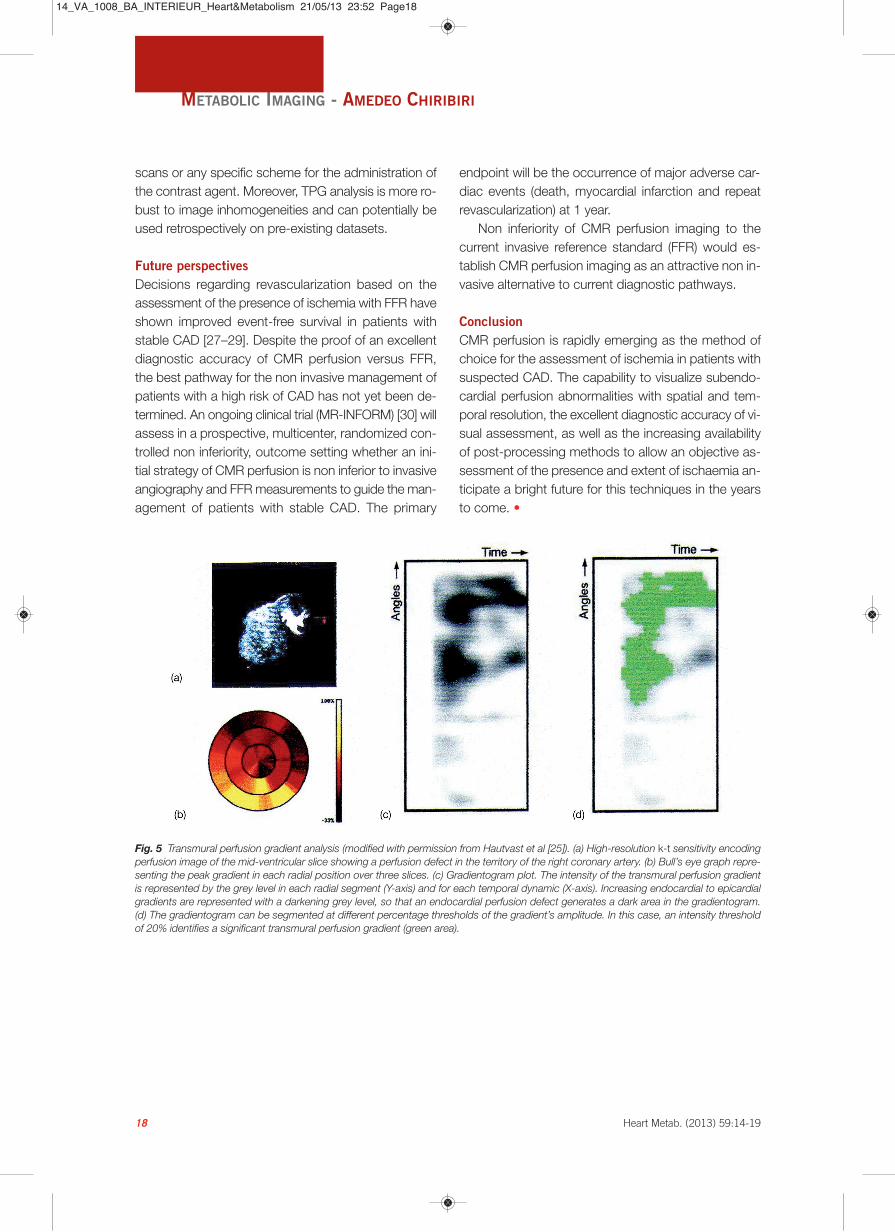
In an attempt to exploit the full diagnostic informationprovided by high-resolution k-t perfusion scans to visu-alize the presence and extent of subendocardial is-chemia, we have recently developed and validated anovel diagnostic technique for the identification of he-modynamically significant CAD, based on the spatialand temporal distribution of ischemia in the left ventric-ular myocardium and on the identification of differencesin perfusion between the left ventricular layers. Trans-mural perfusion gradient (TPG) analysis is based on atwo dimensional, “gradientogram” representation, whichdisplays the evolution of the transmural gradient in leftventricular myocardial perfusion (contrast uptake) overtime (Figure 5). Several new measurements of suben-docardial ischemia are defined on the gradientogram(maximum and mean intensity of the TPG, temporal per-
sistence and radial extent of the TPG), revealing a cleardistinction between normal perfusion and areas of in-ducible ischaemia and a good correlation with invasivecoronary angiography [25]. As FFR is considered the in-vasive reference standard for the assessment of thefunctional significance of CAD, the optimal TPG diag-nostic criterion has recently been defined and inde-pendently validated in two distinct populations of pa-tients with suspected CAD versus FFR [26].
A transmural redistribution of myocardial perfusionof 20% (TPG 20%) was the best diagnostic criterion forthe identification of FFR hemodynamically significantCAD, with a sensitivity of 0.78 and a specificity of 0.94for a per-vessel analysis and a sensitivity of 0.89 and aspecificity of 0.83 on a per-patient analysis. Moreover,TPG correlated well with the degree of severity of thecoronary lesions as assessed with FFR.
While TPG analysis had a similar diagnostic accu-racy to expert visual assessment, it is a fully automatedanalysis method, which analyzes the perfusion CMRdata based on the expected spatial distribution andtemporal evolution of myocardial ischemia. TPG analy-sis has several advantages over quantitative perfusionassessment, as it does not require the acquisition of rest
Heart Metab. (2013) 59:14-19 17
METABOLIC IMAGING - AMEDEO CHIRIBIRI
Fig. 4 Example of voxel-wise quantitative analysis on cardiac mag-netic resonance perfusion data. (a) Arrival of the contrast agent in theleft ventricle. Mid-ventricular slice, images acquired at 3 Tesla usinga k-t sensitivity encoding sequence with high in-plane spatial reso-lution (voxel size 1.2 × 1.2 × 10 mm). (b) Wash-in of the contrastagent in the left ventricular myocardium, showing an area of suben-docardial perfusion deficit extending from the infer-septal to the in-ferolateral wall. (c) Maximum myocardial enhancement. (d) High res-olution (voxel-wise) quantitative perfusion map showing thedistribution of subendocardial ischemia and the variable degree ofseverity in the transmural direction.
14_VA_1008_BA_INTERIEUR_Heart&Metabolism 21/05/13 23:52 Page17
scans or any specific scheme for the administration ofthe contrast agent. Moreover, TPG analysis is more ro-bust to image inhomogeneities and can potentially beused retrospectively on pre-existing datasets.
Future perspectives
Decisions regarding revascularization based on the assessment of the presence of ischemia with FFR haveshown improved event-free survival in patients withstable CAD [27–29]. Despite the proof of an excellentdiagnostic accuracy of CMR perfusion versus FFR,the best pathway for the non invasive management ofpatients with a high risk of CAD has not yet been de-termined. An ongoing clinical trial (MR-INFORM) [30] willassess in a prospective, multicenter, randomized con-trolled non inferiority, outcome setting whether an ini-tial strategy of CMR perfusion is non inferior to invasiveangiography and FFR measurements to guide the man-agement of patients with stable CAD. The primary
endpoint will be the occurrence of major adverse car-diac events (death, myocardial infarction and repeatrevascularization) at 1 year.
Non inferiority of CMR perfusion imaging to thecurrent invasive reference standard (FFR) would es-tablish CMR perfusion imaging as an attractive non in-vasive alternative to current diagnostic pathways.
Conclusion
CMR perfusion is rapidly emerging as the method ofchoice for the assessment of ischemia in patients withsuspected CAD. The capability to visualize subendo-cardial perfusion abnormalities with spatial and tem-poral resolution, the excellent diagnostic accuracy of vi-sual assessment, as well as the increasing availabilityof post-processing methods to allow an objective as-sessment of the presence and extent of ischaemia an-ticipate a bright future for this techniques in the yearsto come. •
18 Heart Metab. (2013) 59:14-19
METABOLIC IMAGING - AMEDEO CHIRIBIRI
Fig. 5 Transmural perfusion gradient analysis (modified with permission from Hautvast et al [25]). (a) High-resolution k-t sensitivity encodingperfusion image of the mid-ventricular slice showing a perfusion defect in the territory of the right coronary artery. (b) Bull’s eye graph repre-senting the peak gradient in each radial position over three slices. (c) Gradientogram plot. The intensity of the transmural perfusion gradientis represented by the grey level in each radial segment (Y-axis) and for each temporal dynamic (X-axis). Increasing endocardial to epicardialgradients are represented with a darkening grey level, so that an endocardial perfusion defect generates a dark area in the gradientogram.(d) The gradientogram can be segmented at different percentage thresholds of the gradient’s amplitude. In this case, an intensity thresholdof 20% identifies a significant transmural perfusion gradient (green area).
14_VA_1008_BA_INTERIEUR_Heart&Metabolism 21/05/13 23:52 Page18

REFERENCES
1. Bruder O, Schneider S, Nothnagel D, et al (2009) EuroCMR (Eu-ropean Cardiovascular Magnetic Resonance) registry: results ofthe German pilot phase. J Am Coll Cardiol 54:1457-1466
2. Ishida M, Morton G, Schuster A, Nagel E, Chiribiri A. (2010)Quantitative assessment of myocardial perfusion MRI. CurrentCardiovascular Imaging Reports 3:65-73
3. Greenwood JP, Maredia N, Younger JF, et al (2012) Cardiovas-cular magnetic resonance and single-photon emission com-puted tomography for diagnosis of coronary heart disease (CE-MARC): a prospective trial. Lancet 379:453-460
4. Wilke N, Simm C, Zhang J, Ellermann J, et al (1993) Contrast-enhanced first pass myocardial perfusion imaging: correlation be-tween myocardial blood flow in dogs at rest and during hyper-emia. Magnetic Resonance in Medicine: official journal of theSociety of Magnetic Resonance in Medicine/Society of MagneticResonance in Medicine 29:485-497
5. Christian TF, Aletras AH, Arai AE (2008) Estimation of absolutemyocardial blood flow during first-pass MR perfusion imaging us-ing a dual-bolus injection technique: comparison to single-bolusinjection method. J Magn Reson Imaging 27:1271-1277
6. Hsu LY, Groves DW, Aletras AH, Kellman P, Arai AE (2012) Aquantitative pixel-wise measurement of myocardial blood flow bycontrast-enhanced first-pass CMR perfusion imaging. JACCCardiovasc Imaging 5:154-166
7. Lockie T, Ishida M, Perera D, et al (2011) High-resolution mag-netic resonance myocardial perfusion imaging at 3.0-Tesla to de-tect hemodynamically significant coronary stenoses as deter-mined by fractional flow reserve. J Am Coll Cardiol 57:70-75
8. Watkins S, McGeoch R, Lyne J, et al (2009) Validation of mag-netic resonance myocardial perfusion imaging with fractionalflow reserve for the detection of significant coronary heart dis-ease. Circulation 120:2207-2213
9. Costa MA, Shoemaker S, Futamatsu H, et al (2007) QuantitativeMagnetic resonance perfusion imaging detects anatomic andphysiologic coronary artery disease as measured by coronary an-giography and fractional flow reserve. J Am Coll Cardiol 50:514-522
10. Algranati D, Kassab GS, Lanir Y (2010) Mechanisms of my-ocardium-coronary vessel interaction. Am J Physiol Heart CircPhysiol 298:H861-873
11. Spaan JA, Breuls NP, Laird JD (1981) Diastolic-systolic coronaryflow differences are caused by intramyocardial pump action inthe anesthetized dog. Circ Res 49:584-593
12. Panting JR, Gatehouse PD, Yang G-Z, et al (2002) Abnormalsubendocardial perfusion in cardiac syndrome X detected by car-diovascular magnetic resonance imaging. N Engl J Med346:1948-1953
13. Plein S, Schwitter J, Suerder D, Greenwood JP, Boesiger P, Koz-erke S (2008) k-Space and time sensitivity encoding-acceleratedmyocardial perfusion MR imaging at 3.0 T: comparison with 1.5T. Radiology 249:493-500
14. Plein S, Ryf S, Schwitter J, Radjenovic A, Boesiger P, KozerkeS (2007) Dynamic contrast-enhanced myocardial perfusion MRIaccelerated with k-t sense. Magnetic Resonance in Medicine: of-ficial journal of the Society of Magnetic Resonance in Medi-cine/Society of Magnetic Resonance in Medicine 58:777-785
15. Morton G, Ishida M, Schuster A, et al (2012) Perfusion cardio-vascular magnetic resonance: comparison of an advanced,
high-resolution and a standard sequence. Journal of Cardio-vascular Magnetic Resonance 14:34:1-1
16. Chiribiri A, Bettencourt N, Nagel E (2009) Cardiac magnetic res-onance stress testing: results and prognosis. Curr Cardiol Rep11:54-60
17. Nandalur KR, Dwamena BA, Choudhri AF, Nandalur MR, CarlosRC (2007) Diagnostic performance of stress cardiac magneticresonance imaging in the detection of coronary artery disease:a meta-analysis. J Am Coll Cardiol 50:1343-1353
18. Patel AR, Antkowiak PF, Nandalur KR, et al (2010) Assessmentof advanced coronary artery disease. J Am C 56:561-569
19. Jerosch-Herold M, Wilke N, Stillman A (1998) Magnetic reso-nance quantification of the myocardial perfusion reserve with aFermi function model for constrained deconvolution. Med Phys25:73–84.
20. Jerosch-Herold M (2010) Quantification of myocardial perfusionby cardiovascular magnetic resonance. Journal of CardiovascularMagnetic Resonance 12:57
21. Morton G, Jogiya R, Plein S, Schuster A, Chiribiri A, Nagel E(2012) Quantitative cardiovascular magnetic resonance perfusionimaging: inter-study reproducibility. European Heart Journal –Cardiovascular Imaging 13:954-960
22. Ishida M, Schuster A, Morton G, et al (2011) Development of auniversal dual-bolus injection scheme for the quantitative as-sessment of myocardial perfusion cardiovascular magnetic res-onance. J Cardiovasc Magn Reson 13:28
23. Zarinabad N, Chiribiri A, Hautvast GLTF, et al (2012) Voxel-wisequantification of myocardial perfusion by cardiac magnetic res-onance. Feasibility and methods comparison. Magnetic Reso-nance in Medicine: official journal of the Society of Magnetic Res-onance in Medicine/Society of Magnetic Resonance in Medicine68:1994-2004
24. Chiribiri A, Schuster A, Ishida M, et al (2013) Perfusion phantom:an efficient and reproducible method to simulate myocardialfirst-pass perfusion measurements with cardiovascular mag-netic resonance. Magnetic Resonance in Medicine: official jour-nal of the Society of Magnetic Resonance in Medicine/Society ofMagnetic Resonance in Medicine; 69:698–707.
25. Hautvast GLTF, Chiribiri A, Lockie T, Breeuwer M, Nagel E, PleinS (2011) Quantitative analysis of transmural gradients in my-ocardial perfusion magnetic resonance images. Magnetic Res-onance in Medicine: official journal of the Society of MagneticResonance in Medicine/Society of Magnetic Resonance in Med-icine 66:1477-1487
26. Chiribiri A, Hautvast GLTF, Lockie T, et al. Assessment of coro-nary artery stenosis severity and location: quantitative analysis oftransmural perfusion gradients by high resolution magnetic res-onance versus fractional flow reserve. J Am Coll Cardiol Img.2013;():. doi:10.1016/j.jcmg.2012.09.019
27. Pijls N, Vanschaardenburgh P, Manoharan G, et al (2007) Percuta-neous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER Study. J Am Coll Cardiol 49:2105-2111
28. Tonino PAL, De Bruyne B, Pijls NHJ, et al (2009) Fractional flowreserve versus angiography for guiding percutaneous coronaryintervention. N Engl J Med 360:213-224
29. De Bruyne B, Pijls NHJ, Kalesan B, et al (2012) Fractional flowreserve-guided PCI versus medical therapy in stable coronarydisease. N Engl J Med 367:991-1001
30. Hussain ST, Paul M, Plein S, et al (2012) Design and rationale ofthe MR-INFORM study: stress perfusion cardiovascular magneticresonance imaging to guide the management of patients withstable coronary artery disease. J Cardiovasc Magn Reson 14:65
Heart Metab. (2013) 59:14-19 19
METABOLIC IMAGING - AMEDEO CHIRIBIRI
14_VA_1008_BA_INTERIEUR_Heart&Metabolism 21/05/13 23:52 Page19





























