Embed Size (px)
Citation preview

Lonafarnib and Peginterferon Lambda: First-in-class Drugs for
HDV Infection in Late-Stage Clinical Development
Robert G. Gish, MDPrincipal, Robert G Gish Consultants LLCMedical Director, Hepatitis B Foundation

Introduction
• Key points from the Phase 2 POC and LOWR 1-4 studies
- Patients dosed with lonafarnib with and without RTV, with and without PEG-IFN-alfa-2a
- Data results from the Phase 2 POC resulted in the Phase 3 study design and initiation which we will discuss at the end of the presentation
- Data from the phase II lambda interferon monotherapy study has led to a phase II combination study that we will discuss today
3
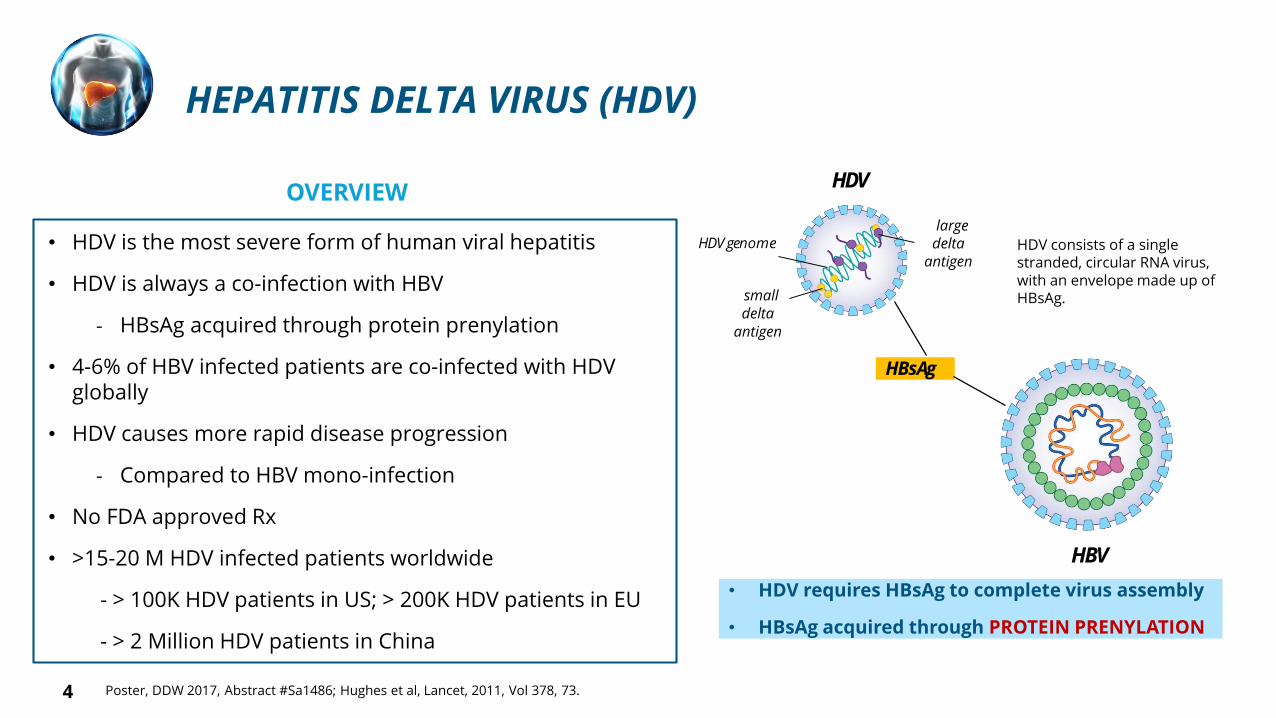
HEPATITIS DELTA VIRUS (HDV)
OVERVIEW
• HDV is the most severe form of human viral hepatitis
• HDV is always a co-infection with HBV
- HBsAg acquired through protein prenylation
• 4-6% of HBV infected patients are co-infected with HDVglobally
• HDV causes more rapid disease progression
- Compared to HBV mono-infection
• No FDA approved Rx
• >15-20 M HDV infected patients worldwide
- > 100K HDV patients in US; > 200K HDV patients in EU
- > 2 Million HDV patients in China
large delta
antigen
small delta
antigen
HDV
HBsAg
HBV
HDV genome HDV consists of a single stranded, circular RNA virus, with an envelope made up of HBsAg.
Poster, DDW 2017, Abstract #Sa1486; Hughes et al, Lancet, 2011, Vol 378, 73.
• HDV requires HBsAg to complete virus assembly
• HBsAg acquired through PROTEIN PRENYLATION
4

HDV: MOST RAPID PROGRESSION OF VIRAL HEPATITIS
50% of HDV-Infected Patients are Cirrhotic at Diagnosis
Transplant
Westbrook et al, J Hepatology 2014 Fattovich et al, Seminars in Liver Diseases 2003 Nourredin et al, Curr. Gasterol. Rep 2013
Progression to Cirrhosis
HCV 10-20% within 20 Years
HBV 20% within 5 Years
HDV 70% within 5-10 Years
5
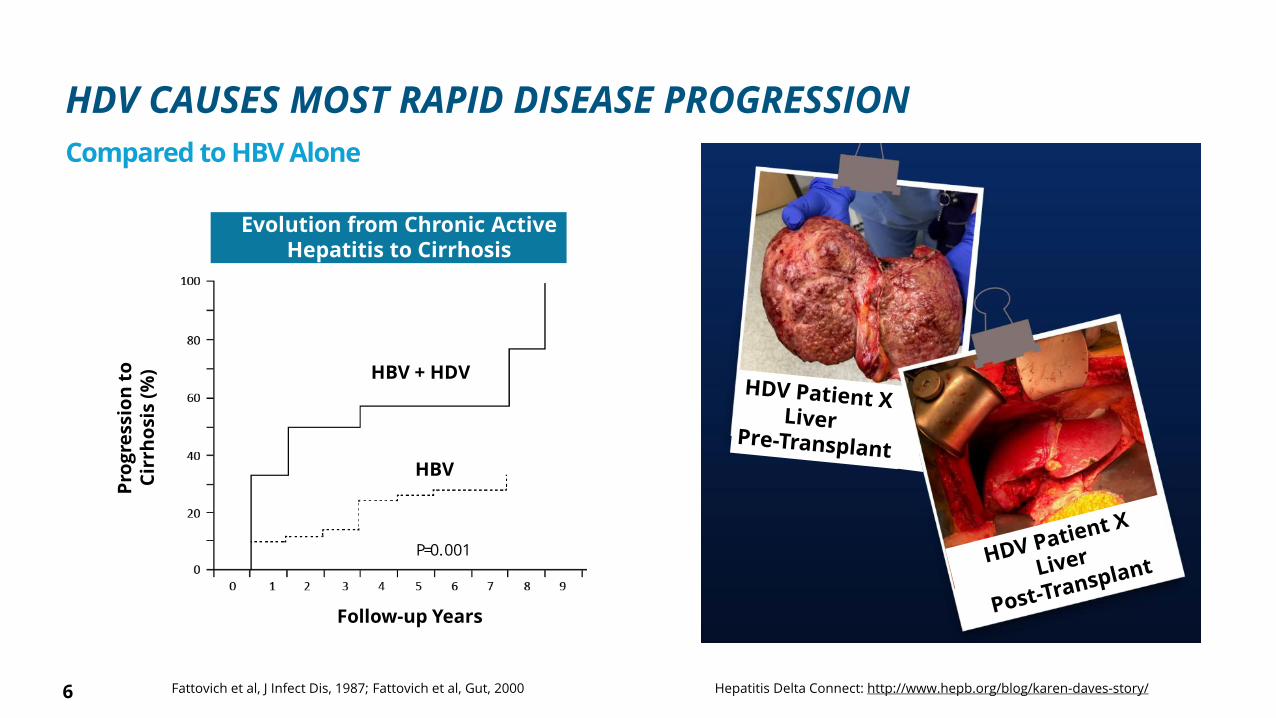
HDV CAUSES MOST RAPID DISEASE PROGRESSION
Compared to HBV Alone
Fattovich et al, J Infect Dis, 1987; Fattovich et al, Gut, 2000
Evolution from Chronic ActiveHepatitis to Cirrhosis
Pro
gre
ssio
nto
C
irrh
osi
s(%
) HBV + HDV
HBV
P=0.001
Follow-up Years
Hepatitis Delta Connect: http://www.hepb.org/blog/karen-daves-story/6

Years
HBV and HDV1
6 8 10 122 4 14 160
P=0.0002
1.0
0.8
0.6
0.4
0.2
0.0
SURVIVAL: HDV VS CANCER
Colorectal Cancer2
102 4 6 8
Years
1.0
0.8
0.6
0.4
0.2
0.0
Su
rviv
al
Years
1.0
0.8
0.6
0.4
0.2
0.01 52 43
Resected NSCLC3
1Serrano et al, EASL 2011; 2Cancer Causes Control, 2012, 23:1421–1428; 3Cerfolio et al, Ann Thorac Surg, 2007, 84:182–907
HBV + HDV
HBV

• Small molecule, first-in-class, oral, prenylation inhibitor, by blocking farnesyltransferase
• Well-characterized through Phase 3
- >2,000 patients dosed in oncology program by Merck (Schering)
- Dose limiting toxicity is GI (class effect)
• Over 120 HDV patients dosed across international sites to date
• US & EU Orphan Designation, FDA Breakthrough Designation, EMA PRIME Designation
• Issued patent covering broad range of lonafarnib + ritonavir doses and durations
- US, Europe, Japan, China and South Korea
NO
N NH2
O
N
Br
Br
Cl
LONAFARNIB FOR HDV
8
First and Only Oral Agent in Development for chronic HDV infection

0
0 4 8 12
Week
16 20 24
Change in Log HDV-RNA
LNF 50 mg BID + RTV
(N=12) *
LNF 50 mg BID + RTV + PEG IFN-alfa-2a
(N=4) *
100 Fold
Increase
Antiviral
Activity
20182019
PEG IFN-alfa-2a
(N=15) **
Compared to PEG-IFN-alfa-2a Alone
+
* Yurdaydin et al, LOWR HDV 2 Study; EASL 2018, PS-161; J. Hepatology, 2018, Vol 68, S89** Wedemeyer et al, Myr201 Study; EASL 2019, G-13; J. Hepatology, 2019, Vol 70, e81
-0.5
-1
-1.5
-2
-2.5
-3
-3.5
-4
9
LONAFARNIB PHASE 2 HDV PROGRAM: ANTIVIRAL ACTIVITY
Using the same RoboGene assay 1.1 log LLQ = 14 IU,

LONAFARNIB PHASE 2 HDV PROGRAM
All-oral: Lonafarnib boosted with Ritonavir
33% (6 of 18) patients ≥ 2 log decline or BLQ at Week 24
47% (7 of 15) patients normalized ALT at Week 24
Composite endpoint: 29% (4 of 14)
Combination: Lonafarnib boosted with Ritonavir + PEG IFN-alfa-2a
78% (7 of 9) patients ≥ 2 log decline or BLQ at Week 24
88% (7 of 8) patients normalized ALT at Week 24
Composite endpoint: 63% (5 of 8)
Predominant AEs were GI-related (mild / moderate)
10 Yurdaydin et al, LOWR HDV 2 Study; EASL 2018, PS-161; J. Hepatology, 2018, Vol 68, S89 Most common reported AEs: nausea, diarrhea, fatigue, weight loss, anorexia, vomiting
2018
Presented
Dose, Combinations and Endpoints Defined

Lonafarnib 50 mg BID
Ritonavir 100 mg BID
Lonafarnib 50 mg BID
Ritonavir 100 mg BID
PEG IFN-alfa-2a
Placebo
PEG IFN-alfa-2a
All patients will be maintained on background HBV nucleoside therapy.
N = 175
Primary Endpoint at Week 48
• ≥ 2 log decline in HDV RNA
+
Normalization of ALT
Secondary Endpoint at Week 48
• Histologic improvement
o > 2-point improvement in HAI inflammatory score
o No progression in fibrosis
• Improvement of fibrosis
N = 125
N = 50
N = 50
On-treatment48
weeks24
weeks
Post-treatment
Follow Up
Follow Up
Follow Up
Follow Up
**
* biopsy
: PHASE 3 INTERNATIONAL STUDY
Superiority over PEG IFN-alfa-2a not required.
Nuc
Nuc
Nuc
Nuc
12-24weeks
Run-In
Quest Diagnostics, LLOQ = 40 IU/mL
Delta-Liver Improvement and Virologic Response in HDV
11

20 COUNTRIES | 105 SITES
12

HDV RNA quantification and HBV/HDV
• Reflex test for RNA PCR testing at Quest
Patient and physician outreach
• 600,000 diagnosed HBV patients provide readily identifiable HDV market
• HDV patients clustered in major metro hotspots
U.S. HDV PATIENT IDENTIFICATION PROGRAM
13

QUEST DIAGNOSTICS: COMMERCIAL HDV RNA TEST
• Leading provider of diagnostic services
• Over 2,200 patient service centers across the U.S.
• Eiger HDV testing program for HBV+ patients
• HDV RNA quantification and HBV/HDV reflex testing
• HDV RNA QUEST quantification threshold current: 40 IU/mL
HDV RNA Quantification is Gold Standard in HDV Diagnosis and Management
14

U.S. MAJOR METRO HOTSPOTS IDENTIFIED
Martins et al, DDW 2017
Top 10 U.S. Cities in 2016
1. Chicago, Illinois
2. Berwyn, Illinois
3. Brooklyn, New York
4. Corona, New York
5. Waukegan, Illinois
6. New York, New York
7. Bronx, New York
8. Jamaica, New York
9. Lombard, New York
10. Aurora, Illinois
HDV Geographic Footprint is Growing
15

• A novel first in class Type III interferon
• Binds to a unique receptor separate from Type I interferons
- Type III interferon receptor is highly expressed on hepatocytes
- Lambda receptors have limited expression on hematopoietic cells and CNS cells
• Uses similar downstream signaling pathway as Type I interferons
• Greater than 3,000 patients in 17 clinical trials (HCV / HBV)
• Comparable antiviral activity with less of the typical IFN alfa related side effects*
PEGINTERFERON LAMBDA
* Chan, HLY et al, J Hepatology 2016
A Better Tolerated Interferon
16

LIMT: PHASE 2 LAMBDA MONOTHERAPY STUDY
Arm 1N = 19
Arm 2N = 14
Follow-up
On-treatment
48 weeks 24 weeks
Post-treatment
Study Complete
201920182017
Primary Endpoint:
• Evaluate Safety, Tolerability, Efficacy
Secondary Endpoint:
• Proportion of Patients with HDV RNA BLQ 24 weeks after EOT
Lambda 120 mcg QW
Lambda 180 mcg QW Follow-up
A Better Tolerated Interferon for Monotherapy
17

-2
-2.5Lambda 180 mcg QW*
-3
-1.5
0
-0.5
-1
0 4 8 12 16 20 24
Week
28 32 36 40 44 48
Lambda 120 mcg QW*
2019
Lo
gH
DV
RN
AIU
/mL
* Randomization dose, dose reductions allowed; Etzion et al, EASL 2019, PS-052: J. Hepatology, 2019, Vol. 70, e32.Robogene® 2.0 HDV RNA PCR assay used for Pegasys and Lambda data sets, LLOQ = 14 IU/mL
Lambda 180 mcg better response compared to Lambda 120 mcg
HDV-RNA REDUCTION WITH LAMBDA THRU WEEK 48
18

-2
-2.5Lambda 180 mcg QW*
-3
-1.5
-1
0
-0.5
0 4 8 12 16 20 24 28 32
Week
36 40 44 48
Alfa 180 mcg QW**
Lambda 120 mcg QW*
2019
Lo
gH
DV
RN
AIU
/mL
* Randomization dose, dose reductions allowed; Etzion et al, EASL 2019, PS-052: J. Hepatology, 2019, Vol. 70, e32.** Wedemeyer EASL 2019, G-13: J. Hepatology, 2019, Vol 70, e81
Robogene® 2.0 HDV RNA PCR assay used for Lambda and Alfa data sets, LLOQ = 14 IU/mL
HDV-RNA REDUCTION WITH LAMBDA THRU WEEK 48
Lambda 180 mcg Better than Alfa 180 mcg with Improved Tolerability
19

5/1436%
BLQ
Week 48End of Treatment
Week 72End of Follow-up
BLQ
10
20
30
40
5/1436%
%Patients
2/1414%
5/1436%
ALTNormalization
ALTNormalization
DVR = BLQ at 24 Weeks Post-TreatmentEtzion et al, EASL 2019, PS-052: J. Hepatology, 2019, Vol. 70, e32.
* Compared to Alfa = 0%
SVR
Wedemeyer EASL 2019
2019
Robogene® 2.0 HDV RNA PCR assay used for Pegasys and Lambda data sets, LLOQ = 14 IU/mL
DVR Endpoint with Lambda Monotherapy to Be Discussed with Regulatory Agencies
20
4/14 were BLD at week 72
LIMT STUDY: 36% DURABLE VIROLOGIC RESPONSE (DVR)*

* biopsy
Primary Endpoint:
• ≥ 2 Log HDV RNA reduction at EOT
Secondary Endpoint:
• Histological Improvement: baseline compared to Week 48 (24 weeks off treatment)
(biopsy confirmed)
N=26Lambda 180 mcg QW
Lonafarnib 50 mg BID
Ritonavir 100 mg BID
24 Weeks
Follow Up
24 Weeks*
On-treatment Post-treatment
• Post Treatment Data Q4’19
Koh et al, AASLD 2019, LO-8Quest Diagnostics, LLOQ = 40 IU/mL
LIFT: PHASE 2 LAMBDA COMBO WITH LONAFARNIB STUDY
A Better Tolerated Interferon for Combination
21
*

• Adverse events: mostly mild to moderate; included GI related weight loss, hyperbilirubinemia, and anemia
• Therapy was dose reduced in 3 patients and discontinued in 4 patients
Week 12(N=21/26)
Week 24(N=19/26)
Mean Log10 HDV RNA decline -3.6 -3.4
from Baseline (p<0.0001) (p<0.0001)
% Patients HDV RNA≥ 2 log10 decline
-- 95% (18/19)
% Patients HDV RNA 24% 16%
Below Limit of Quantification (5/21) (3/19)
% Patients HDV RNA 24% 37%
Undetectable (5/21) (7/19)
LIFT: PHASE 2 LAMBDA COMBO WITH LONAFARNIB/RTV STUDY
Interim Results
22Koh et al, AASLD 2019, LO-8Quest Diagnostics, LLOQ = 40 IU/mL

Lonafarnib
Lonafarnib / Ritonavir+
PEG IFN Lambda
PEG IFN Lambda
“All Oral”
Therapy
“Mono Therapy” Sub Q
“Combination Therapy”
FIRST-IN-CLASS TREATMENTS IN DEVELOPMENT FOR HDV
Multiple Options to Treat HDV
23
PEG IFN Lambda
Lonafarnib/ Ritonavir

THANK YOU!
Acknowledgements:
Ingrid Choong, PhD, Eiger Senior VP Clin Dev
Eiger Development Team
Jeff Glenn, MD, PhD
Cihan Yurdaydin, MD
Christopher Koh, MD
All Investigators and Patients
on the LOWR, LIMT and LIFT Studies24






























