Embed Size (px)
Citation preview

545
CL I N I C A L AS P E C T S O FVI S I O N A N D HE A R I N G
CHAPTER CONTENTS
How Can Vision Become Impaired?
Focusing Problems
Decreased Transmission of Light
Damage to the Retina
Optic Nerve Damage: Glaucoma
The Eye Examination
How Can Hearing Become Impaired?
Conductive Hearing Loss
Sensorineural Hearing Loss
The Ear Examination and Hearing Evaluation
Managing Hearing Loss
T H E P L A S T I C I T Y O F P E R C E P T I O N :
Decrease in Cortical Function Due to Aging
A C R O S S T H E S E N S E S : Deafness and Visual Attention
SOME QUESTIONS WE WILL CONSIDER
■ What are the major causes of impaired vision andhearing? (546, 564)
■ Can a person be legally blind but have 20/20 vision?(551)
■ How can diseases of the ear and eye be treated? (552,567)
Although it is obvious that the man in Figure 16.1 isexamining the woman’s eye, most people do notunderstand exactly what he is seeing or what he islooking for. Even though most Americans have hadtheir eyes and ears examined because of problemswith either vision or hearing or just as part of a routinephysical examination, few people understand exactly
what is going on during these examinations. One ofthe purposes of this chapter is to demystify what goeson during examinations of the eye and the ear.
Before we can understand what eye and ear spe-cialists look for during an examination, we mustunderstand the major problems that can cause impair-ments in vision and hearing. We therefore begin this
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 545
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

2. Light is blurred as it enters the eye. Scarring of thecornea or clouding of the lens blurs light as itenters the eye. Specific problems: corneal injuryor disease, cataract.
3. There is damage to the retina. The retina can bedamaged by disruption of the vessels that supply itwith blood, by its separation from the blood supply,
546
Retinaldamage
Optic nervedamage
Focus and blurproblems
Figure 16.2 Places in the eye where visual problems can occur.
chapter by describing a number of the most commonvisual problems and how they are treated to improveor restore vision. After we understand the nature of themost common causes of visual problems, we willdescribe how a routine eye examination detects theseproblems. Following our discussion of vision, we takethe same approach for hearing.
V I S U A L I M P A I R M E N T
HOW CAN VISION BECOMEIMPAIRED?
Four major types of problems can cause poor vision(Figure 16.2):
1. Light is not focused clearly on the retina. Problemsin focusing light can occur because the eyeball istoo short or too long or because the cornea or thelens does not function properly. We will describethe following specific problems: myopia (near-sightedness), hyperopia (farsightedness), presby-opia (“old eye”), and astigmatism.
Figure 16.1 Ophthalmologist examining patient.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 546
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

and by diseases that attack its receptors. Specificproblems we will discuss include macular degen-eration, diabetic retinopathy, detached retina, andhereditary retinal degeneration.
4. There is damage to the optic nerve. The opticnerve can degenerate. When this degeneration isdue to a pressure buildup inside the eyeball, thecause is glaucoma. In addition, degeneration canbe caused by poor circulation, toxic substances, orthe presence of a tumor. We will focus on glau-coma in our discussion.
We begin by considering a problem that affectsmore people than all the others combined: an inabil-ity to adequately focus incoming light onto the retina.
FOCUSING PROBLEMS
In Chapter 2, we described the optical system of theeye—the cornea and the lens—which, if everything isworking properly, brings light entering the eye to asharp focus on the retina. We also described theprocess of accommodation, which adjusts the focus-ing power of the eye to bring both near and far objectsinto focus.
We will now consider the conditions myopia,hyperopia, presbyopia, and astigmatism, four prob-lems that affect a person’s ability to focus an image onthe retina.
MyopiaMyopia, or nearsightedness, is an inability to see dis-tant objects clearly. The reason for this difficulty,which affects over 70 million Americans, is illustratedin Figure 16.3a: In the myopic eye, parallel rays oflight are brought to a focus in front of the retina so thatthe image reaching the retina is blurred. This problemcan be caused by either of two factors: (1) refractivemyopia, in which the cornea and/or the lens bends thelight too much, or (2) axial myopia, in which the eye-ball is too long. Either way, light comes to a focus infront of the retina, so that the image on the retina isout of focus, and far objects look blurred. (See Chapter15 for a discussion of how myopia develops.)
How can we deal with this problem? One way tocreate a focused image on the retina is to move thestimulus closer. This pushes the focus point furtherback (see Figure 2.10), and if we move the stimulusclose enough, we can push the focus point onto theretina (Figure 16.3b). The distance at which the spotof light becomes focused on the retina is called thefar point, and when our spot of light is at the far
547 Clinical Aspects o f Vis ion and Hearing
Figure 16.3 Focusing of light by the myopic (nearsighted) eye.(a) Parallel rays from a distant spot of light are brought to afocus in front of the retina, so distant objects appearblurred. (b) As the spot of light is moved closer to the eye,the focus point is pushed back until, at the far point, therays are focused on the retina, and vision becomes clear.Vision is blurred beyond the far point. (c) A corrective lens,which bends light so that it enters the eye at the same angleas light coming from the far point, brings light to a focus onthe retina. Angle A is the same in (b) and (c).
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 547
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

point, a myope can see it clearly. Although a personwith myopia can see nearby objects clearly (which iswhy a myopic person is called nearsighted), objectsbeyond the far point are still out of focus (see the leftcolumn of Table 16.1). The solution to this problemis well known to anyone with myopia: corrective eye-glasses or contact lenses. These corrective lensesbend incoming light so that it is focused as if it wereat the far point (Figure 16.3c). Notice that the lensplaced in front of the eye causes the light to enter theeye at exactly the same angle as light coming fromthe far point in Figure 16.3b.
Before leaving our discussion of myopia, let’sconsider the following question: How strong must acorrective lens be to give the myope clear far vision?To answer this question, we have to keep in mindwhat is required of a corrective lens: It must bend par-allel rays so that light enters the eye at the same angleas a spot of light positioned at the far point. Figure16.4 shows what this means for two different locationsof the far point. When the far point is close, as inFigure 16.4a, we need a powerful corrective lens tobend the light in the large angle shown in Figure16.4b. However, when the far point is distant, as inFigure 16.4c, we need only a weak corrective lens tobend the light in the small angle shown in Figure16.4d. Thus, the strength of the corrective lensdepends on the location of the far point: A powerfullens is needed to correct vision when the far point isclose, and a weak lens is needed to correct visionwhen the far point is distant.
When ophthalmologists or optometrists write aprescription for corrective lenses, they specify thestrength of the lens in diopters, using the followingrelationship: number of diopters � 1/far point inmeters. Thus, a slightly myopic person with a far
548
Table 16.1Comparisons of focusing problems associated with the farpoint and the near point
Far Point (Farthest Distance Near Point (Closest Distancefor Clear Vision) for Clear Vision)
Problem: In myopia, the far point Problem: In presbyopia, the is close to the eye, and vision is near point moves away fromblurred beyond the far point. the eye, and vision is blurred
closer than the near point.
Figure 16.4 The strength of a lens required to correct myopic vision depends on the location of the far point. (a) A close far point requiring(b) a strong corrective lens. (c) A distant far point requiring (d) a weak corrective lens.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 548
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

point at 1 meter (100 cm) requires a 1-diopter correc-tion (diopters � 1/1 � 1.0). However, a very myopicperson with a far point at 2/10 of a meter (20 cm)requires a 5-diopter correction (diopters � 1/0.2 �5.0). This relationship between the distance of the farpoint and the required number of diopters of correc-tion is shown in Figure 16.5.
Although glasses or contact lenses are the majorroute to clear vision for the myope, surgical proce-dures in which lasers are used to change the shape ofthe cornea have been introduced that enable peopleto experience good vision without corrective lenses.The first widely used laser procedure, photorefrac-tive keratotomy (PRK), was introduced in the UnitedStates around 1980. In this procedure, a type of lasercalled an excimer laser, which does not heat tissue,sculpts the cornea to give it either less power (formyopia; Figure 16.6a) or more power (for hyperopia;Figure 16.6b). This procedure appears to be mosteffective for myopia.
Recently, PRK has been largely replaced withanother laser procedure, laser-assisted in situ kerato-mileusis (LASIK). This procedure also involvessculpting the cornea with an excimer laser, but beforethe cornea is sculpted, a small flap, less than the thick-ness of a human hair, is cut into the surface of thecornea. The flap is folded out of the way, the cornea issculpted by the laser, and the flap is then folded backinto place. This procedure results in faster healingand less discomfort than the PRK procedures.
549 Clinical Aspects o f Vis ion and Hearing
(a)
Lens
(b)
Lens
Cornea
Figure 16.6 In the laser photorefractive keratotomy operation, anexcimer laser is used to reshape the cornea, as shown by thedashed lines. (a) Reducing the curvature of the cornea onthe myopic eye reduces the focusing power of the cornea sothat the focus point moves back. (b) Increasing the curva-ture of the cornea in the hyperopic eye increases the focus-ing power of the cornea so that the focus point movesforward.
Figure 16.5 The number of diopters of lens power needed to correct myopic vision for different far points. Without a corrective lens, vision isblurred at distances greater than the far point. A far point of 10 cm represents severe myopia, and a far point of 100 cm repre-sents mild myopia.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 549
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license
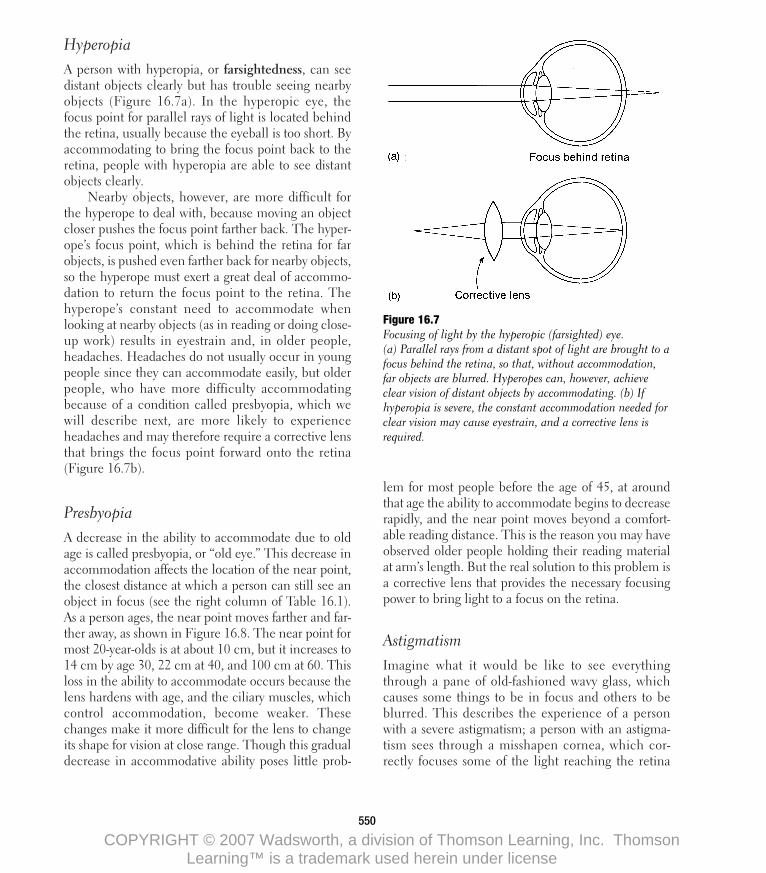
HyperopiaA person with hyperopia, or farsightedness, can seedistant objects clearly but has trouble seeing nearbyobjects (Figure 16.7a). In the hyperopic eye, thefocus point for parallel rays of light is located behindthe retina, usually because the eyeball is too short. Byaccommodating to bring the focus point back to theretina, people with hyperopia are able to see distantobjects clearly.
Nearby objects, however, are more difficult forthe hyperope to deal with, because moving an objectcloser pushes the focus point farther back. The hyper-ope’s focus point, which is behind the retina for farobjects, is pushed even farther back for nearby objects,so the hyperope must exert a great deal of accommo-dation to return the focus point to the retina. Thehyperope’s constant need to accommodate whenlooking at nearby objects (as in reading or doing close-up work) results in eyestrain and, in older people,headaches. Headaches do not usually occur in youngpeople since they can accommodate easily, but olderpeople, who have more difficulty accommodatingbecause of a condition called presbyopia, which wewill describe next, are more likely to experienceheadaches and may therefore require a corrective lensthat brings the focus point forward onto the retina(Figure 16.7b).
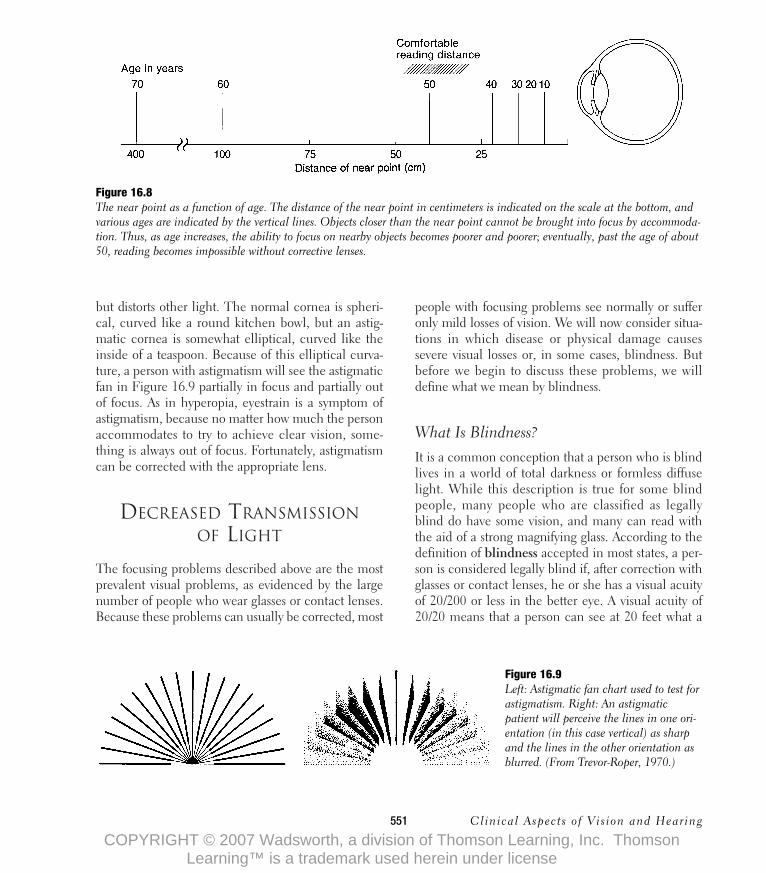
PresbyopiaA decrease in the ability to accommodate due to oldage is called presbyopia, or “old eye.” This decrease inaccommodation affects the location of the near point,the closest distance at which a person can still see anobject in focus (see the right column of Table 16.1).As a person ages, the near point moves farther and far-ther away, as shown in Figure 16.8. The near point formost 20-year-olds is at about 10 cm, but it increases to14 cm by age 30, 22 cm at 40, and 100 cm at 60. Thisloss in the ability to accommodate occurs because thelens hardens with age, and the ciliary muscles, whichcontrol accommodation, become weaker. Thesechanges make it more difficult for the lens to changeits shape for vision at close range. Though this gradualdecrease in accommodative ability poses little prob-
lem for most people before the age of 45, at aroundthat age the ability to accommodate begins to decreaserapidly, and the near point moves beyond a comfort-able reading distance. This is the reason you may haveobserved older people holding their reading materialat arm’s length. But the real solution to this problem isa corrective lens that provides the necessary focusingpower to bring light to a focus on the retina.
AstigmatismImagine what it would be like to see everythingthrough a pane of old-fashioned wavy glass, whichcauses some things to be in focus and others to beblurred. This describes the experience of a personwith a severe astigmatism; a person with an astigma-tism sees through a misshapen cornea, which cor-rectly focuses some of the light reaching the retina
550
Figure 16.7 Focusing of light by the hyperopic (farsighted) eye.(a) Parallel rays from a distant spot of light are brought to afocus behind the retina, so that, without accommodation,far objects are blurred. Hyperopes can, however, achieveclear vision of distant objects by accommodating. (b) Ifhyperopia is severe, the constant accommodation needed forclear vision may cause eyestrain, and a corrective lens isrequired.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 550
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license
but distorts other light. The normal cornea is spheri-cal, curved like a round kitchen bowl, but an astig-matic cornea is somewhat elliptical, curved like theinside of a teaspoon. Because of this elliptical curva-ture, a person with astigmatism will see the astigmaticfan in Figure 16.9 partially in focus and partially outof focus. As in hyperopia, eyestrain is a symptom ofastigmatism, because no matter how much the personaccommodates to try to achieve clear vision, some-thing is always out of focus. Fortunately, astigmatismcan be corrected with the appropriate lens.
DECREASED TRANSMISSIONOF LIGHT
The focusing problems described above are the mostprevalent visual problems, as evidenced by the largenumber of people who wear glasses or contact lenses.Because these problems can usually be corrected, most
people with focusing problems see normally or sufferonly mild losses of vision. We will now consider situa-tions in which disease or physical damage causessevere visual losses or, in some cases, blindness. Butbefore we begin to discuss these problems, we willdefine what we mean by blindness.
What Is Blindness?It is a common conception that a person who is blindlives in a world of total darkness or formless diffuselight. While this description is true for some blindpeople, many people who are classified as legallyblind do have some vision, and many can read withthe aid of a strong magnifying glass. According to thedefinition of blindness accepted in most states, a per-son is considered legally blind if, after correction withglasses or contact lenses, he or she has a visual acuityof 20/200 or less in the better eye. A visual acuity of20/20 means that a person can see at 20 feet what a
551 Clinical Aspects o f Vis ion and Hearing
Figure 16.8 The near point as a function of age. The distance of the near point in centimeters is indicated on the scale at the bottom, andvarious ages are indicated by the vertical lines. Objects closer than the near point cannot be brought into focus by accommoda-tion. Thus, as age increases, the ability to focus on nearby objects becomes poorer and poorer; eventually, past the age of about50, reading becomes impossible without corrective lenses.
Figure 16.9 Left: Astigmatic fan chart used to test forastigmatism. Right: An astigmaticpatient will perceive the lines in one ori-entation (in this case vertical) as sharpand the lines in the other orientation asblurred. (From Trevor-Roper, 1970.)
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 551
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

person with normal vision can see at 20 feet. However,a person with an acuity of 20/200 needs to be at a dis-tance of 20 feet to see what a person with normalvision can see from a distance of 200 feet.
When we define blindness in terms of visual acu-ity, we are evaluating a person’s ability to see with hisor her fovea (which, as we saw in Chapter 2, is thecone-rich area of the retina that is responsible fordetail vision). While poor foveal vision is the mostcommon reason for legal blindness, a person withgood foveal vision but little peripheral vision may alsobe considered legally blind. Thus, a person with nor-mal (20/20) foveal vision but little or no peripheralvision may be legally blind. This situation, which iscalled tunnel vision, results from diseases that affectthe retina, such as advanced glaucoma or retinitis pig-mentosa (a form of retinal degeneration), whichaffect peripheral vision but leave the foveal conesunharmed until the final stages, when central visioncan also be affected.
We begin our discussion of problems caused bydisease or injury by considering some conditions thataffect both peripheral and central vision because theyaffect the perception of light at the beginning of thevisual process, as light enters the eye through thecornea and the lens.
Corneal Disease and InjuryThe cornea, which is responsible for about 70 per-cent of the eye’s focusing power (Lerman, 1966), isthe window to vision because light first passesthrough this structure on its way to the retina. Inorder for a sharp image to be formed on the retina,the cornea must be transparent, but this transparencyis occasionally lost when injury, infection, or allergicreactions cause the formation of scar tissue on thecornea. This scar tissue decreases visual acuity andsometimes makes lights appear to be surrounded by ahalo, which looks like a shimmering rainbow. Inaddition, corneal disease and injury can also causepain. Drugs, which often bring the cornea back to itstransparent state, are the first treatment for cornealproblems. If drugs fail, however, clear vision canoften be restored by a corneal transplant operation.
The basic principle underlying a corneal trans-plant operation is shown in Figure 16.10. The scarredarea of the cornea, usually a disk about 6 to 8 mm indiameter, is removed and replaced by a piece ofcornea taken from a donor. For best results, this donorshould be a young adult who died of an acute diseaseor of an injury that left the corneal tissue in good con-dition. In the past, a major problem with this opera-tion was the necessity of transplanting the donorcornea within a few hours after the donor’s death.Now, however, donor corneas are preserved by low-temperature storage in a specially formulated solution.
Of the over 10,000 corneal transplants performedevery year, about 85 percent are successful. Remem-ber, however, that a corneal transplant operationinvolves only a small piece of the eye—there is nosuch thing as an eye transplant. Indeed, the problemsinvolved in transplanting a whole eye are overwhelm-ing. For one thing, the optic nerve and the retina aresensitive to lack of oxygen, so that, once the circula-tion is cut off, irreversible damage occurs within min-utes, just as is the case for the brain. Thus, keeping thedonor’s eye alive presents a serious problem. And evenif it were possible to keep an eye alive, there is theproblem of connecting the 1 million optic nerve fibersof the donor’s eye to the corresponding nerve fibers ofthe patient’s optic nerve. At this point, whole eyetransplants are purely science fiction.
552
Figure 16.10 Corneal transplant operation. The scarred part of thecornea has been removed, and the donor cornea is about tobe sutured in place.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 552
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license
Clouding of the Lens (Cataract)
Like the cornea, the lens is transparent and is importantfor focusing a sharp image on the retina. Clouding ofthe lens, which is called a cataract, is sometimes pres-ent at birth (congenital cataract), may be caused by aneye disease (secondary cataract), or may be caused byinjury (traumatic cataract), but the most commoncause of cataract is old age (senile cataract). Cataractsdevelop, for reasons as yet unknown, in 75 percent ofpeople over 65 and in 95 percent of people over 85.
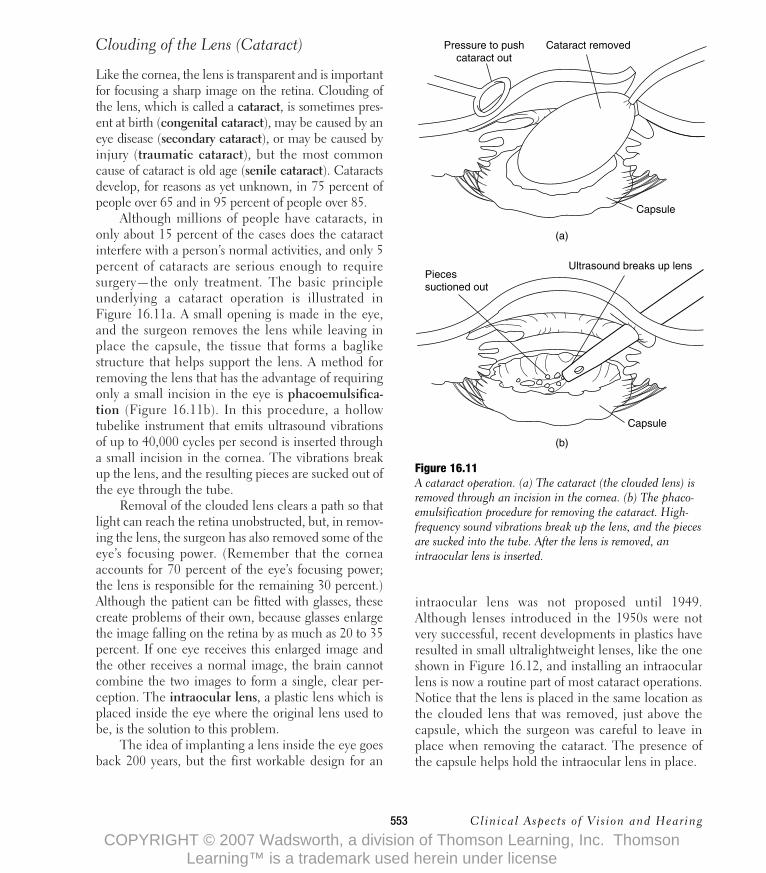
Although millions of people have cataracts, inonly about 15 percent of the cases does the cataractinterfere with a person’s normal activities, and only 5percent of cataracts are serious enough to requiresurgery—the only treatment. The basic principleunderlying a cataract operation is illustrated inFigure 16.11a. A small opening is made in the eye,and the surgeon removes the lens while leaving inplace the capsule, the tissue that forms a baglikestructure that helps support the lens. A method forremoving the lens that has the advantage of requiringonly a small incision in the eye is phacoemulsifica-tion (Figure 16.11b). In this procedure, a hollowtubelike instrument that emits ultrasound vibrationsof up to 40,000 cycles per second is inserted througha small incision in the cornea. The vibrations breakup the lens, and the resulting pieces are sucked out ofthe eye through the tube.
Removal of the clouded lens clears a path so thatlight can reach the retina unobstructed, but, in remov-ing the lens, the surgeon has also removed some of theeye’s focusing power. (Remember that the corneaaccounts for 70 percent of the eye’s focusing power;the lens is responsible for the remaining 30 percent.)Although the patient can be fitted with glasses, thesecreate problems of their own, because glasses enlargethe image falling on the retina by as much as 20 to 35percent. If one eye receives this enlarged image andthe other receives a normal image, the brain cannotcombine the two images to form a single, clear per-ception. The intraocular lens, a plastic lens which isplaced inside the eye where the original lens used tobe, is the solution to this problem.
The idea of implanting a lens inside the eye goesback 200 years, but the first workable design for an
intraocular lens was not proposed until 1949.Although lenses introduced in the 1950s were notvery successful, recent developments in plastics haveresulted in small ultralightweight lenses, like the oneshown in Figure 16.12, and installing an intraocularlens is now a routine part of most cataract operations.Notice that the lens is placed in the same location asthe clouded lens that was removed, just above thecapsule, which the surgeon was careful to leave inplace when removing the cataract. The presence ofthe capsule helps hold the intraocular lens in place.
553 Clinical Aspects o f Vis ion and Hearing
(a)
Pressure to pushcataract out
Cataract removed
Capsule
Ultrasound breaks up lens
(b)
Piecessuctioned out
Capsule
Figure 16.11 A cataract operation. (a) The cataract (the clouded lens) isremoved through an incision in the cornea. (b) The phaco-emulsification procedure for removing the cataract. High-frequency sound vibrations break up the lens, and the piecesare sucked into the tube. After the lens is removed, anintraocular lens is inserted.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 553
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

DAMAGE TO THE RETINA
The retina receives nourishment from the retinal cir-culation and from the pigment epithelium on whichit rests. All four conditions described below cause aloss of vision because of their effects on the retinal cir-
culation and on the relationship between the retinaand the pigment epithelium.
Diabetic RetinopathyBefore the isolation of insulin in 1922, most peoplewith severe diabetes, a condition in which the bodydoesn’t produce enough insulin, had a life expectancyof less than 20 years. The synthesis of insulin (whichwon the 1923 Nobel Prize for its discoverers) greatlyincreased the life expectancy of diabetics, but oneresult of this greater life expectancy has been a greatincrease in an eye problem called diabetic retinopa-thy. Of the 10 million diabetics in the United States,about 4 million show some signs of this problem.
Figure 16.13 shows what happens as the diseaseprogresses. At first, the capillaries swell, and althoughmost cases of diabetic retinopathy stop here, a largenumber of diabetics suffer vision losses even when thedisease stops at this point. The disease’s further pro-gression, which occurs in a small percentage ofpatients, involves a process called neovascularization.Abnormal new blood vessels are formed (Figure16.13b), which do not supply the retina with adequateoxygen and which are fragile and so bleed into the vit-reous humor (the jellylike substance that fills the eye-ball); this bleeding interferes with the passage of lightto the retina. Neovascularization can also cause scar-ring of the retina and retinal detachment (see below).
554
(b)
(a)
Wire loop Intraocular lens(behind iris)
Cornea
Wire loop
Iris
Lens beinginsertedthrough pupil
Figure 16.12Installing an intraocular lens in the eye after the cataracthas been removed. (a) The lens is inserted through an inci-sion in the cornea. Notice that it is being inserted throughthe pupil so that it will be positioned where the originallens was, behind the iris and just above the capsule.(b) Frontal view, showing the lens in place behind the iris.The small wire loops hold the lens in place.
(a) (b)
Figure 16.13 Blood vessels in diabetic retinopathy. (a) In early stages ofthe disease, the blood vessels swell and leak slightly. (b) Inlater stages, in a process called neovascularization, abnor-mal new blood vessels grow on the surface of the retina.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 554
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license
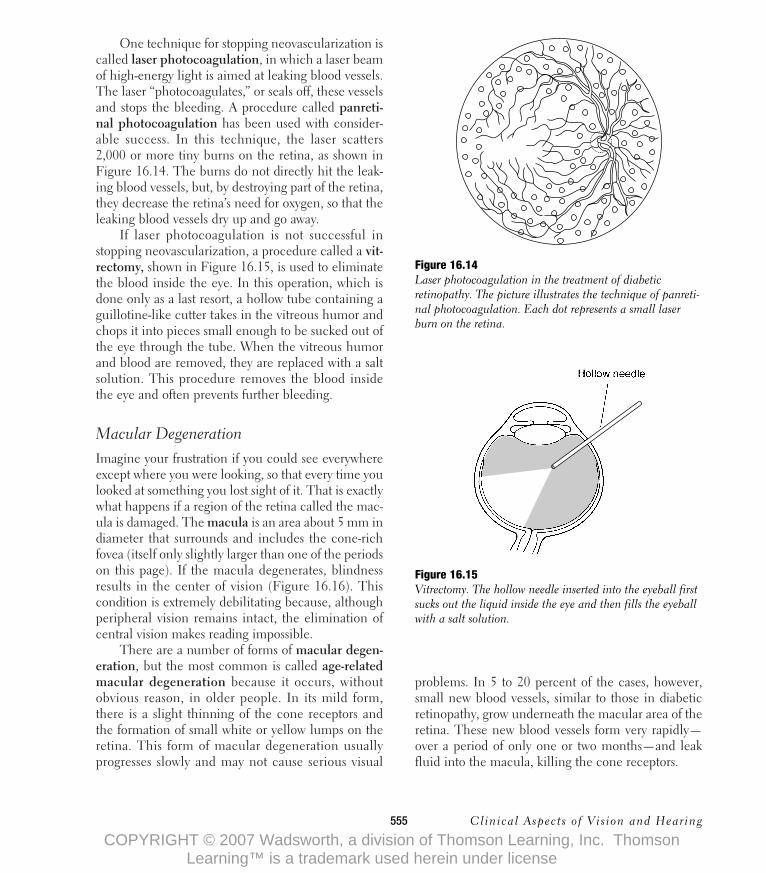
One technique for stopping neovascularization iscalled laser photocoagulation, in which a laser beamof high-energy light is aimed at leaking blood vessels.The laser “photocoagulates,” or seals off, these vesselsand stops the bleeding. A procedure called panreti-nal photocoagulation has been used with consider-able success. In this technique, the laser scatters2,000 or more tiny burns on the retina, as shown inFigure 16.14. The burns do not directly hit the leak-ing blood vessels, but, by destroying part of the retina,they decrease the retina’s need for oxygen, so that theleaking blood vessels dry up and go away.
If laser photocoagulation is not successful instopping neovascularization, a procedure called a vit-rectomy, shown in Figure 16.15, is used to eliminatethe blood inside the eye. In this operation, which isdone only as a last resort, a hollow tube containing aguillotine-like cutter takes in the vitreous humor andchops it into pieces small enough to be sucked out ofthe eye through the tube. When the vitreous humorand blood are removed, they are replaced with a saltsolution. This procedure removes the blood insidethe eye and often prevents further bleeding.
Macular DegenerationImagine your frustration if you could see everywhereexcept where you were looking, so that every time youlooked at something you lost sight of it. That is exactlywhat happens if a region of the retina called the mac-ula is damaged. The macula is an area about 5 mm indiameter that surrounds and includes the cone-richfovea (itself only slightly larger than one of the periodson this page). If the macula degenerates, blindnessresults in the center of vision (Figure 16.16). Thiscondition is extremely debilitating because, althoughperipheral vision remains intact, the elimination ofcentral vision makes reading impossible.
There are a number of forms of macular degen-eration, but the most common is called age-relatedmacular degeneration because it occurs, withoutobvious reason, in older people. In its mild form,there is a slight thinning of the cone receptors andthe formation of small white or yellow lumps on theretina. This form of macular degeneration usuallyprogresses slowly and may not cause serious visual
problems. In 5 to 20 percent of the cases, however,small new blood vessels, similar to those in diabeticretinopathy, grow underneath the macular area of theretina. These new blood vessels form very rapidly—over a period of only one or two months—and leakfluid into the macula, killing the cone receptors.
555 Clinical Aspects o f Vis ion and Hearing
Figure 16.14 Laser photocoagulation in the treatment of diabeticretinopathy. The picture illustrates the technique of panreti-nal photocoagulation. Each dot represents a small laserburn on the retina.
Figure 16.15 Vitrectomy. The hollow needle inserted into the eyeball firstsucks out the liquid inside the eye and then fills the eyeballwith a salt solution.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 555
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

Until recently, there was no treatment for age-related macular degeneration. However, a study bythe National Eye Institute indicates that, if the prob-lem can be caught at an early stage in some patientswith the more severe form of the disease, laser photo-coagulation can stop or greatly reduce leakage of thenewly formed vessels.
Detached RetinaDetached retina, a condition in which the retinabecomes separated from the underlying pigmentepithelium (Figure 16.17), has occurred in a numberof athletes because of traumatic injuries to the eye orthe head. Sugar Ray Leonard, the former welter-weight boxing champion, retired temporarily fromboxing because of a detached retina. He returned toboxing a number of years later amid much discussionabout whether returning to the ring was worth therisk of losing his sight in one eye. As it turned out,Leonard won both the fight and the gamble with hissight, apparently escaping without further damaginghis eye.
A detached retina affects vision for two reasons:(1) For good image formation, the retina must lie
smoothly on top of the pigment epithelium, and(2) when the retina loses contact with the pigmentepithelium, the visual pigments in the detached areaare separated from enzymes in the epithelium neces-sary for pigment regeneration. When the visual pig-ment can no longer regenerate, that area of the retinabecomes blind.
The treatment for a detached retina is an opera-tion to reattach it. The basic idea behind this opera-tion is to cause the formation of scar tissue inside theeye that will attach itself to the retina and anchor it inplace. This process is accomplished by applyingeither a cooling or a heating probe to exactly the rightplace on the outside of the eyeball. Figure 16.17bshows the procedure used to determine where toapply the probe. While looking into the eye with aspecial viewing device, the surgeon presses on theoutside of the eyeball, which causes an indentationthat can be seen inside the eye. The surgeon pressesat a number of points, until the indentation inside theeyeball matches the location of the tear or hole in theretina, where the detachment originated.
Once the point where the detachment hasoccurred is located, it is marked on the outside of theeyeball, and that point is cooled or heated to create an
556
Figure 16.16 Macular degeneration causes a loss ofcentral vision.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 556
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

inflammatory response. The retina must then bepushed flush with the wall of the eyeball. This isaccomplished by placing a band around the outside ofthe eyeball that creates a dumbbell-shaped eye. Then,with the retina pressed against the wall of the eye, theinflammation causes scarring that “welds” the retinaback onto the pigment epithelium. If the area ofdetached retina is not too big, there is a 70 to 80 per-cent chance that this procedure will work. In mostcases, it restores vision, although vision is sometimesnot restored even though the retina is successfullyreattached. The larger the detached area, the lesslikely it is that this operation (or others, which we willnot describe here) will work. Sometimes, if a retinaltear can be caught at an early stage, before fluid hasgotten through it and caused the retina to detach, it ispossible to prevent detachment by surrounding thetear with laser burns. This is a quick procedure thatcan be carried out in the ophthalmologist’s office andrequires no surgery.
Hereditary Retinal DegenerationThe most common form of hereditary retinal degen-eration is a disease called retinitis pigmentosa, adegeneration of the retina that is passed from onegeneration to the next (although not always affectingeveryone in a family). We know little about what actu-ally causes the disease, although one hypothesis is thatit is caused by a problem in the pigment epithelium.
A person with retinitis pigmentosa usually showsno signs of the disease until reaching adolescence. Atthis time, the person may begin to notice some diffi-culty in seeing at night, since the disease first attacksthe rod receptors. As the person gets older, the diseaseslowly progresses, causing further losses of vision inthe peripheral retina. Then, in its final stages, whichmay occur as early as a person’s 30s or as late as the50s or 60s (depending on the strain of the disease),retinitis pigmentosa also attacks the cones, and theresult is complete blindness.
OPTIC NERVE DAMAGE:GLAUCOMA
A leading cause of blindness in the United States isglaucoma, which causes nerve fibers in the opticnerve to degenerate and therefore prevents the nerveimpulses generated by the retina from being transmit-ted to the brain.
Although the end result of glaucoma is damageto the optic nerve, the source of the problem is at thefront of the eye. We can understand how damage tothe front of the eye affects the optic nerve by lookingat the cross section of the eye in Figure 16.18a.Under normal conditions, the aqueous humor (theliquid found in the space between the cornea and thelens), which is continuously produced at A, passesbetween the iris and the lens following the path indi-cated by the arrows; it then drains from the eye at B.In glaucoma, the drainage of aqueous humor is par-tially blocked. Closed-angle glaucoma is a rare formof glaucoma in which a pupillary block (Figure16.18b) constricts the opening between the iris andthe lens and causes a pressure buildup that pushesthe iris up, thereby closing the angle between the
557 Clinical Aspects o f Vis ion and Hearing
Figure 16.17 (a) A detached retina. (b) Procedure for reattaching theretina. To locate the site of detachment, a probe pushes theeyeball from outside while the surgeon, at S, looks into theeye. Once the site of the detachment is located, the outsideof the eye is marked, and a cooling or heating probe isapplied at the marked point.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 557
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

cornea and the iris and blocking the area at B wherethe aqueous humor leaves the eye.
In open-angle glaucoma, which is the mostcommon form of the disease, the eye looks normal(Figure 16.18a), but the drainage area at B is partiallyblocked, so that it is more difficult for the aqueous
humor to leave the eye. The blocks that occur inboth closed- and open-angle glaucoma result in alarge resistance to the outflow of aqueous humor,and since the aqueous humor continues to be pro-duced inside the eye, the intraocular pressure—thepressure inside the eyeball—rises. This increase inintraocular pressure presses on the head of the opticnerve at the back of the eye. This pressure cuts off cir-culation to the head of the optic nerve, which resultsin the degeneration of the optic nerve fibers thatcauses blindness.
The increase in pressure that occurs in closed-angle glaucoma usually happens very rapidly and isaccompanied by pain. The treatment for this type ofglaucoma is an operation called an iridectomy, inwhich a small hole is created in the iris with a laser(Figure 16.18b). This hole opens a channel throughwhich the aqueous humor can flow and releases thepressure on the iris. With the pressure gone, the irisflattens out and uncovers the area at B so that aque-ous humor can flow out of the eye.
Intraocular pressure increases more slowly inopen-angle glaucoma, so the patient may be unawareof any symptoms. In many cases, visual loss is so grad-ual that much of the patient’s peripheral vision isgone before its loss is noticed. For that reason, oph-thalmologists strongly recommend that people over40 have their eyes checked regularly for glaucoma,since early detection greatly enhances the chances ofeffective treatment by medication. In 5 to 10 percentof the cases of open-angle glaucoma, medications donot decrease the pressure, and an operation becomesnecessary. The goal of this operation is to cut anopening in the wall of the eyeball that creates a newroute for fluid to leave the eye.
THE EYE EXAMINATION
So far, we have described some of the things that cango wrong with the eye and how these problems aretreated. In this part of the chapter, we will describethe procedures used to uncover some of these prob-lems. Before describing the eye examination, we willconsider who examines the eyes.
558
Figure 16.18 (a) Arrows indicate the flow of aqueous humor in the nor-mal eye. The aqueous humor is produced at A and leavesthe eye at B. In open-angle glaucoma, the aqueous humorcannot leave the eye because of a blockage at B. (b) Inclosed-angle glaucoma, the raised iris hinders the flow ofaqueous humor from the eye. An iridectomy—cutting a holein the iris—can provide a way for the aqueous humor toreach B.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 558
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

Who Examines Eyes?Three types of professionals are involved in eye care:ophthalmologists, optometrists, and opticians.
1. An ophthalmologist is an M.D. who has com-pleted undergraduate school and four years ofmedical school, which provide general medicaltraining. In order to become an ophthalmologist, aperson needs four or more years of training aftergraduation from medical school to learn how totreat eye problems medically and surgically. Someophthalmologists receive even further training andthen specialize in specific areas, such as pediatricophthalmology (practice limited to children), dis-eases of the cornea, retinal diseases, or glaucoma.Most ophthalmologists, however, treat all eye prob-lems, as well as prescribing glasses and fitting con-tact lenses.
2. An optometrist has completed undergraduateschool and, after four years of additional study, hasreceived a doctor of optometry (O.D.) degree.Optometrists can examine eyes and fit and pre-scribe glasses or contact lenses. In some states,optometrists have won the right to include medicaltreatment using drugs for some eye conditions.Surgery, however, is still done exclusively by oph-thalmologists.
3. An optician is trained to fabricate and fit glassesand, in some states, contact lenses, on the pre-scription of an ophthalmologist or an optometrist.
What Happens During an Eye Exam?The basic aims of an eye exam are (1) to determinehow well the patient can see, (2) to correct vision if itis defective, (3) to determine the causes of defectivevision by examining the optics of the eye and check-ing for eye diseases, and (4) to diagnose diseases thatthe patient may not even be aware of. To accomplishthese aims, an examination by an eye specialist usuallyincludes the following.
Medical History The first step in an eye exam is totake a medical history. This history focuses on any eyeproblems that the patient may have had in the past, on
any current eye problems, and on any general medicalproblems that may be related to the patient’s vision.
Visual Acuity This is the familiar part of the eyeexam, in which you are asked to read letters on an eyechart like the one in Figure 15.1. The old version ofthe eye chart, which most people are familiar with,had a large E at the top. This new version results inmore accurate measurements of acuity because thereare the same number of letters on each line and thespacing between the letters is proportional to the sizesof the letters. The top row of letters is the 20/400 line.This means that a person with normal vision shouldbe able to see these letters from a distance of 400 feet.Since the eye chart is usually viewed from about 20feet, people with normal vision see these letters easily.When asked to read the smallest line he or she cansee, the patient usually picks a line that is easily read.With a little encouragement, however, most patientsfind that they can see lines smaller than the one theyoriginally picked, and the examiner has the patientread smaller and smaller lines until letters are missed.The smallest line a person can read indicates his orher visual acuity, with normal vision defined as anacuity of 20/20. A person with worse than normalacuity—say, 20/40—must view a display from a dis-tance of 20 feet to see what a person with normal acu-ity can see at 40 feet. A person with better thannormal acuity—say, 20/10—can see from a distanceof 20 feet what a person with normal vision can seeonly at 10 feet.
The visual acuity test described above tests onlyfoveal vision, since the patient looks directly at eachletter, so the image of that letter falls on the fovea.Thus, as mentioned earlier, a person who scores20/20 on a visual acuity test may still be classified aslegally blind if he or she has little or no peripheralvision. Testing peripheral vision is usually not part ofa routine eye exam, but when peripheral vision prob-lems are suspected, a technique called perimetry isused, in which the patient is asked to indicate thelocation of small spots of light presented at differentlocations in the periphery. This test locates blindspots (called scotomas) that may be caused by retinaldegeneration, detachment of the retina, or diseasessuch as glaucoma.
559 Clinical Aspects o f Vis ion and Hearing
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 559
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license
In addition to using the eye chart to test farvision, it is also customary to test near vision, espe-cially in older patients who may be experiencing theeffects of presbyopia. This testing is done by deter-mining the smallest line of a card like the one inFigure 16.19 that the patient can see from a comfort-able reading distance.
Refraction A score of 20/60 on a visual acuity testindicates worse than normal acuity but does not indi-cate what is causing this loss of acuity. Acuity couldbe decreased by one of the diseases described earlieror by a problem in focusing: myopia, hyperopia, pres-byopia, or astigmatism. If the problem lies in thefocusing mechanism of the eye, it is usually easilycorrected by glasses or contact lenses. Refraction isthe procedure used to determine the power of thecorrective lenses needed to achieve clear vision.
The first step in refraction is a retinoscopy exam,an examination of the eye with a device called aretinoscope. This device projects a streak of light intothe eye that is reflected into the eye of the examiner.The examiner moves the retinoscope back and forth
and up and down across the eye, noticing what thereflected light looks like. If the patient’s eye is focus-ing the light correctly, the examiner sees the wholepupil filled with light, and no correction is necessary(in this case, the patient will usually have tested at20/20 or better in the visual acuity test). If, however,the patient’s eye is not focusing the light correctly, theexaminer sees a streak of light move back and forthacross the pupil as the streak of light from theretinoscope is moved across the eye.
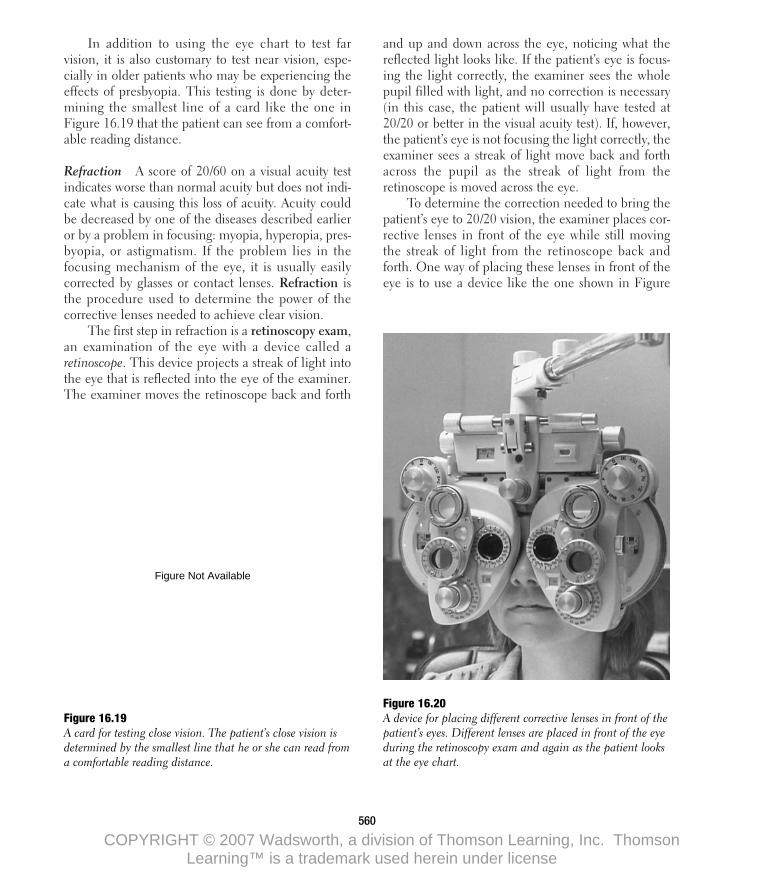
To determine the correction needed to bring thepatient’s eye to 20/20 vision, the examiner places cor-rective lenses in front of the eye while still movingthe streak of light from the retinoscope back andforth. One way of placing these lenses in front of theeye is to use a device like the one shown in Figure
560
Figure 16.19 A card for testing close vision. The patient’s close vision isdetermined by the smallest line that he or she can read froma comfortable reading distance.
Figure 16.20 A device for placing different corrective lenses in front of thepatient’s eyes. Different lenses are placed in front of the eyeduring the retinoscopy exam and again as the patient looksat the eye chart.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 560
Figure Not Available
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

16.20. This device contains a variety of lenses thatcan be changed by turning a dial. The examiner’sgoal is to find the lens that causes the whole pupil tofill up with light when the retinoscope is moved backand forth. This lens brings light to a focus on theretina and is usually close to the one that will be pre-scribed to achieve 20/20 vision.
The retinoscopy exam results in a good firstapproximation of the correct lens to prescribe for apatient, but the ultimate test is what the patient sees.To determine this, the examiner has the patient look atthe eye chart and places lenses in front of the patient’seyes to determine which one results in the clearestvision. When the examiner determines which lensresults in 20/20 vision, he or she writes a prescriptionfor glasses or contact lenses. To fit contact lenses afterdetermining the prescription, the examiner mustmatch the shape of the contact lens to the shape of thepatient’s cornea.
Refraction is used to determine the correctionneeded to achieve clear far vision. Using a procedurewe will not describe here, the examiner also deter-mines whether a correction is needed to achieveclear near vision. This determination is particularlyimportant for patients over 45 years old, who mayexperience reading difficulties due to presbyopia.
External Eye Exam In an external eye exam, theexaminer uses a variety of tests to check the conditionof the external eye. The examiner checks pupillaryreaction by shining light into the eye, to see if thepupil responds by closing when the light is presentedand by opening when the light is removed. The exam-iner also checks the color of the eye and the sur-rounding tissues. “Red eye” may indicate that aninflammation is present. The movement of the eyes ischecked by having the patient follow a moving target,and the alignment of the eyes is checked by havingthe patient look at a target. If the eyes are aligned cor-rectly, both eyes will look directly at the target, but, ifthe eyes are misaligned, one eye will look at the tar-get, and the other will veer off to one side.
Slit-Lamp Examination The slit-lamp examina-tion checks the condition of the cornea and the lens.The slit lamp, shown in Figure 16.21, projects a nar-row slit of light into the patient’s eye. This light can beprecisely focused at different places inside the eye, andthe examiner views this sharply focused slit of lightthrough a binocular magnifier. This slit of light is likethe sharp edge of a knife that cuts through the eye.
What does the examiner see when looking at the“cutting edge” of light from the slit lamp? By focusing
561 Clinical Aspects o f Vis ion and Hearing
Figure 16.21 A patient being examined with a slitlamp. The examiner is checking the con-dition of the lens and the cornea by view-ing the slit of light through a binocularmagnifier.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 561
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

the light at different levels inside the cornea and lens,the examiner can detect small imperfections—placeswhere the cornea or the lens is not completelytransparent—that cannot be seen by any othermethod. These imperfections may indicate cornealdisease or injury or the formation of a cataract.
Tonometry Tonometry measures intraocular pres-sure, the pressure inside the eye, and is therefore thetest for glaucoma. Nowadays, an instrument called atonometer is used to measure intraocular pressure,but before the development of this device, it wasknown that large increases of intraocular pressure,which accompany severe cases of glaucoma, causethe eye to become so hard that this hardness could bedetected by pushing on the eyeball with a finger.
There are several types of tonometers, whichmeasure the intraocular pressure by pushing on thecornea. The Schiotz tonometer is a hand-held devicethat consists of a small plunger attached to a cali-brated weight. The weight pushes the plunger andindents the cornea. If the intraocular pressure is high,the plunger causes a smaller indentation than if theintraocular pressure is normal. Thus, intraocular pres-sure is determined by measuring the indentation ofthe cornea. (Though this procedure may sound ratherpainful, it is not, because the examiner applies a few
drops of anesthetic to the cornea before applying thetonometer.)
The applanation tonometer, shown beingapplied to a patient’s cornea in Figure 16.22, is amore sophisticated and accurate instrument than theSchiotz tonometer. After a few drops of anesthetic areapplied to the cornea, the flat end of a cylindricalrod, called an applanator, is slowly moved against thecornea by the examiner, who watches the applana-tor’s progress through the same magnifiers used forthe slit-lamp exam (Figure 16.22). The examinerpushes the end of the applanator against the corneauntil enough pressure is exerted to flatten a small areaon the cornea’s curved surface. The greater the forcethat must be exerted to flatten the cornea, the greaterthe intraocular pressure.
Ophthalmoscopy So far, we have looked at the out-side of the eye (external eye exam), examined the lensand cornea (slit-lamp exam), and measured theintraocular pressure (tonometry), but we have yet tolook at perhaps the most important structure of all:the retina. Since there is a hole (the pupil) in thefront of the eye, it should be simple to see the retina;we only have to look into the hole. Unfortunately, it’snot that simple; if you’ve ever looked into a person’spupil, you realize that it’s dark in there. In order to
562
Figure 16.22 An applanation tonometer being applied toa patient’s cornea.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 562
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

see the retina, we must find some way to light up theinside of the eye. This is accomplished by the oph-thalmoscope, which was first developed by Hermannvon Helmholtz, of the Young-Helmholtz theory ofcolor vision, in 1850.
The principle underlying Helmholtz’s ophthal-moscope is shown in Figure 16.23. A light off to theside is directed into the patient’s eye with a half-silvered mirror. The half-silvered mirror reflects someof the light and transmits the rest, so that an examinerpositioned as shown in Figure 16.23 can see throughthe mirror and into the patient’s eye. Actual ophthal-moscopes are much more complicated than the onediagrammed here, since they include numerouslenses, mirrors, and filters, but the basic principleremains the same as that of the original ophthalmo-scope designed by Helmholtz in 1850.
Figure 16.24 is a patient’s-eye view of an examina-tion with an ophthalmoscope, although the examineris actually very close, as shown in Figure 16.1. Figure16.25 shows a close-up of what the ophthalmologist
563 Clinical Aspects o f Vis ion and Hearing
Figure 16.23 The principle behind the ophthalmoscope. Light is reflectedinto the patient’s eye by the half-silvered mirror. Some ofthis light is then reflected into the examiner’s eye (along thedashed line), allowing the examiner to see the inside of thepatient’s eye.
Figure 16.24 Patient’s-eye view of an ophthalmoscopic exam.
Figure 16.25 Close-up view of the head of the optic nerve and the retinalcirculation as seen through an ophthalmoscope.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 563
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

sees if the patient has a normal retina. The mostprominent features of this view of the retina are theoptic disk, the place where the ganglion cell fibersleave the eye to form the optic nerve, and the arteriesand veins of the retina. In this examination, the oph-thalmologist focuses on these features, noting anyabnormalities in the appearance of the optic disk andthe retinal circulation. For example, the ophthalmolo-gist may detect the presence of diabetic retinopathy bynoticing a number of very small blood vessels (neovas-cularization). In fact, all the retinal injuries and dis-eases described above cause some change in theappearance of the retina, which can be detected bylooking at the retina with an ophthalmoscope.
Our description of an eye examination has cov-ered most of the tests included in a routine exam. Theexaminer may decide to carry out other tests if a prob-lem is suggested by the routine tests. For example, atechnique called fluorescein angiography is used to
564
Figure 16.26 Fluorescein angiograph of a normal eye. In this view, thehead of the optic nerve is on the far right, just outside thepicture. The fovea is in the dark space near the middle ofthe picture. In the normal eye, the blood vessels stand out insharp contrast to the background. (Photograph courtesy ofEye and Ear Hospital of Pittsburgh.)
examine more closely the retinal circulation inpatients with diabetic retinopathy. A fluorescent dye isinjected intravenously into the arm, and when thisdye reaches the retina, it sharply outlines the retinalarteries and veins, as shown in Figure 16.26. Only bythis technique can we observe the leakage of fluid thatoccurs in the abnormal neovascularized blood vesselsthat accompany diabetic retinopathy. Determiningthe location of the leakage identifies areas that are tobe treated with photocoagulation.
Other tests, which we will not describe here,include the electroretinogram, which measures theelectrical response of the rod and cone receptors andis therefore useful in diagnosing such retinal degener-ation as retinitis pigmentosa, and the cortical evokedpotential, which measures the electrical response ofthe visual cortex and is useful for diagnosing visionproblems caused by head injuries or tumors.
See Summary Table 16.1 for an overview of thematerial we have discussed so far.
H E A R I N G I M P A I R M E N T
In our consideration of the clinical aspects of vision,we saw that visual functioning can be impairedbecause of problems in delivering the stimulus to thereceptors, because of damage to the receptors, andbecause of damage to the system that transmits signalsfrom the receptors toward the brain. An analogous sit-uation exists in hearing, as we will see by consideringthe various causes of hearing impairment.
HOW CAN HEARING BECOMEIMPAIRED?
In considering the question “How can hearing becomeimpaired?” it is important to distinguish betweenimpairments in the auditory system and what effectsthese impairments have on a person’s hearing. A hear-ing impairment is a deviation or change for the worsein either the structure or the functioning of the audi-tory system. A hearing handicap is the disadvantagethat a hearing impairment causes in a person’s ability
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 564
Image Not Available
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

quencies above 6,000 Hz, and would therefore havesome impact on the person’s quality of life.
Problems can develop in the auditory system forthe following reasons: (1) problems in delivering thesound stimulus to the receptors, (2) damage to thereceptors, (3) damage to the transmission system, and(4) damage to the auditory cortex (Figure 16.27). Thefollowing is a list of the types of things that can gowrong in the auditory system within each of thesecategories:
1. Sound is not properly transmitted to the receptors.Problems in delivering sound to the receptors canoccur because of problems such as blockage of the
565 Clinical Aspects o f Vis ion and Hearing
Focusing ProblemsFocusing problems connected with incorrect bending of the light bythe cornea and lens or an eyeball that is too long or short includemyopia and hyperopia. The power of a lens needed to correctmyopia is expressed in diopters, which is 1 divided by the far point.PRK and LASIK are two laser surgery techniques that can be used toreduce or eliminate myopia or hyperopia. Other focusing problemsare presbyopia, decreased ability to accommodate that occurswhen a person gets older, and astigmatism, blurring of stimuli insome orientations due to a misshapen cornea.
What Is Blindness?Blindness is legally defined in terms of either reduced acuity orreduced visual fields.
Decreased Transmission of LightConditions that decrease the amount of light that is transmitted tothe retina include corneal disease or injury and cataracts. Problemsthat cause clouding or scarring of the cornea can be treated withdrugs or corrected with a corneal transplant operation. Cataract, aclouding of the lens, can be treated by removal of the lens andreplacement with an intraocular lens.
Damage to the RetinaDiabetic retinopathy and macular degeneration cause a loss ofvision because of their effects on the retinal circulation. Diabetic
retinopathy is a swelling of the capillaries and, in more extremecases, neovascularization. One treatment is laser photocoagulation.Macular degeneration is a degeneration of the area around thefovea. It is related to old age and can sometimes be treated withlaser photocoagulation. Detached retina causes problems becausethe retina becomes detached from the enzyme-rich pigment epithe-lium. It can be reattached through surgery. Hereditary retinaldegenerations like retinitis pigmentosa attack the receptors.
Optic Nerve DamageGlaucoma, a leading cause of blindness in the United States, is usu-ally connected with a blockage of drainage of the aqueous humorout the front of the eye. This blockage results in increased intraoc-ular pressure, which can led to blindness by pushing on the circula-tion that enters the eye at the optic nerve. Treatments include drugsand surgery to restore the flow by eliminating the blockage.
The Eye ExaminationOphthalmologists, optometrists, and opticians are all professionalsinvolved in eye care. In general, ophthalmologists and optometristsare trained to both fit glasses and also detect abnormalities of theeye. The eye exam consists of the following components: medicalhistory, visual acuity test (far and near), refraction, external eyeexam, slit-lamp examination, tonometry, ophthalmoscopy, andsometimes techniques such as fluorescein angiography.
S U M M A R Y T A B L E 1 6 . 1
to communicate or in the person’s daily living. The dis-tinction between an impairment and a handicapmeans that a hearing impairment does not alwayscause a large hearing handicap. For example, althougha person who has lost the ability to hear all soundsabove 6,000 Hz has lost a substantial portion of his orher range of hearing, this particular hearing loss has lit-tle effect on the person’s ability to hear and understandspeech. We can appreciate this when we realize that,even though telephones transmit frequencies onlybetween about 500 and 3,000 Hz, most people haveno trouble using the telephone for communication.Such a hearing impairment would, however, change aperson’s perception of music, which often contains fre-
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 565
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

outer ear or damage to the system that transmitsvibrations through the middle ear. These types ofproblems result in conductive hearing losses.
2. The hair cells are damaged, so they can’t generateelectrical signals. This problem and the one belowresult in sensorineural hearing losses.
3. There is damage to the auditory nerve or thebrainstem that keeps signals that are generatedfrom being transmitted to the auditory area of thebrain. Damage at the brainstem level can interferewith the listener’s ability to integrate the signalscoming from the left and right ears.
4. There is damage at the auditory cortex, so whenthe signal reaches the cortex, it is not processedproperly.
We will describe some of the major ways inwhich these problems occur in the auditory system,focusing on the first two categories above: conductivehearing loss and sensorineural hearing loss.
CONDUCTIVE HEARING LOSS
A conductive hearing loss is one in which the vibra-tions that would normally be caused by a sound stim-ulus are not conducted from the outer ear into the
cochlea. This kind of loss can occur in either theouter ear or the middle ear.
Outer-Ear DisordersSound can be blocked at the ear canal by the buildupof excessive cerumen (ear wax) or by the insertion ofobjects, as might occur when children decide itwould be fun to put beans or wads of paper into theirears. A more serious problem occurs in children whoare born with outer- or middle-ear malformations thatprevent sound from traveling down the outer-earcanal and through the middle ear. Blockage may alsooccur because of a swelling of the canal caused byinfection by microorganisms, a situation that oftenoccurs in swimmers when water is trapped in the ear,hence the name “swimmer’s ear.”
Another problem occurs if the tympanic mem-brane at the end of the outer ear is ruptured either bya very loud noise such as an explosion or by the inser-tion of a sharp object too far into the ear. Such a rup-ture may allow microorganisms into the middle earthat may cause infection. Also, once the tympanicmembrane is ruptured, it does not efficiently set theossicles into vibration, which may cause hearing loss.Problems of the outer ear are generally treated withmedication or surgery. Normal hearing is oftenrestored after these treatments.
566
Sound transmission problems(conductive hearing loss)
Auditory nerve damage(sensorineural hearing loss)
Hair cell damage(sensorineural hearing loss)
Figure 16.27 Places in the ear where hearingproblems can occur.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 566
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

Middle-Ear DisordersMost people have experienced otitis media, middle-ear infection, at some time. Middle-ear infections arecaused by bacteria that cause swelling of the eusta-chian tube, the passageway that leads from the middleear to the pharynx, which normally opens when a per-son swallows. This natural opening allows the pressurein the middle ear space to equalize with the pressurein the environment. However, if the eustachian tubeis blocked, the pressure in the middle ear starts todecrease. With the eustachian tube closed, the bacte-ria have a nice, warm place to grow inside the middleear space, and this growth eventually produces fluid inthe middle ear, which prevents the tympanic mem-brane and the ossicles from vibrating properly.
Repeated exposure to middle-ear infections maycause a tissue buildup in the middle ear called a cho-lesteatoma. This growth interferes with the vibrations ofthe tympanic membrane and the ossicles and must besurgically removed. If a person does not seek treatmentfor a middle-ear infection, the fluid may build up untilthe tympanic membrane ruptures in order to releasethe pressure. An infection that is left untreated also maydiffuse through the porous mastoid bone, which createsthe middle-ear cavity. This is a very serious conditionand must be treated immediately before the infectionis allowed to spread to the brain. Luckily, diffusionthrough the mastoid bone rarely occurs if middle-earinfections are promptly treated by antibiotics.
Otosclerosis is a hereditary condition in whichthere is a growth of bone in the middle ear. Usually,the stapes becomes fixed in place, so it can’t transmitvibrations to the inner ear. This was the conditionthat caused Beethoven to become so deaf that, late inhis career, he was unable to hear his own music.Today, this condition can be successfully treated by asurgical procedure called stapedectomy, in which thestapes is replaced with an artificial strut.
SENSORINEURAL HEARING LOSS
Sensorineural hearing loss is caused by a number offactors that have in common their site of action in theinner ear.
PresbycusisThe most common form of sensorineural hearing lossis called presbycusis, which means “old hearing”(remember that the equivalent term for vision is pres-byopia, for “old eye”). This loss of sensitivity, which isgreatest at higher frequencies, accompanies agingand affects males more severely than females. Figure16.28 shows the progression of loss as a function ofage. The most common complaint of people withpresbycusis is that they have difficulty hearing peopletalking when there is noise or when other people aretalking at the same time. Presbycusis is treated by theamplification provided by hearing aids and by teach-ing people more effective communication strategies.
Unlike the visual problem of presbyopia, which isan inevitable consequence of aging, presbycusis isapparently caused by factors in addition to aging,since people in preindustrial cultures, who have notbeen exposed to the noises that accompany industrial-ization or to drugs that could damage the ear, often donot experience a decrease in high-frequency hearingin old age. This may be why males, who are exposedto more workplace noise than females, as well as tonoises associated with hunting and wartime, experi-ence a greater presbycusis effect. Because of its link toenvironmental conditions, presbycusis is also calledsociocusis.
Noise-Induced Hearing LossNoise-induced hearing loss occurs when loud noisescause degeneration of the hair cells. This degenera-tion has been observed in examinations of thecochleas of people who have worked in noisy envi-ronments and have willed their ear structures to med-ical research. Damage to the organ of Corti is oftenobserved in these cases. For example, examination ofthe cochlea of a man who worked in a steel mill indi-cated that his organ of Corti had collapsed and noreceptor cells remained (Miller, 1974). Apparently,this kind of damage also occurs in people who haveexposed themselves to loud music for extended peri-ods of time. Because of this exposure to loud music,rock musicians such as Steven Stills and PeterTownsend have become partially deaf and have urged
567 Clinical Aspects o f Vis ion and Hearing
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 567
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

musicians and concertgoers to wear earplugs (Acker-man, 1995). In fact, members of many symphonyorchestras, including the Chicago Symphony, wearear protection to preserve their hearing.
Acoustic trauma caused by implosive noises,such as explosions or machines that create a loudimpact, also can result in sensorineural hearing loss.An example is a 21-year-old college student who wasin the process of raiding a rival fraternity house whena firecracker exploded in his hand, 15 inches from hisright ear. The result was a hearing loss of over 50 dBat frequencies above 3,000 Hz. In addition, the stu-dent also experienced a ringing sensation in his earthat was still present two years after the accident(Ward & Glorig, 1961).
TinnitusRinging in the ears, which is known as tinnitus (ti-NYE-tus or TIN-ni-tus, from the Latin for “tinkling”),affects more than 36 million Americans, nearly 8 mil-lion of them severely. The most common cause oftinnitus is exposure to loud sounds, although thiscondition also can be caused by certain drugs, earinfections, or food allergies.
Whatever causes tinnitus, it is an extremelydebilitating condition. According to Jack Vernon,
director of the Kresge Hearing Research Laboratoryat the University of Oregon, tinnitus is the third worstthing that can happen to a person, ranking onlybelow intractable severe pain and intractable severedizziness. In its most serious form, the constant noiseof tinnitus is totally incapacitating, making it impossi-ble for people to maintain their concentration longenough to complete a task and, in some cases, evendriving people to suicide.
Is there a cure for tinnitus? Unfortunately, formost people the answer to this question is no. Somepeople, however, can gain relief by using a devicecalled a tinnitus masker. The masker, which is wornin the ear like a hearing aid, produces noise thatsounds like a waterfall. This externally producednoise masks the internal noise of tinnitus, making lifebearable for some tinnitus sufferers. Also, tinnitus suf-ferers who use a hearing aid to compensate for a lossof hearing sometimes find that they are unaware ofthe tinnitus while using the hearing aid and for sev-eral hours after taking the hearing aid off.
Meniere’s DiseaseAnother cause of sensorineural hearing loss isMeniere’s disease, a debilitating condition that iscaused by an excessive buildup of the liquid that fills
568
Figure 16.28 Hearing loss in presbycusis as afunction of age. All of the curves areplotted relative to the 20-year curve,which is taken as the standard.(Adapted from Bunch, 1929.)
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 568
Figure Not Available
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

the cochlea and the semicircular canals. The symp-toms of the disease include fluctuating hearing loss,tinnitus, and severe vertigo (dizziness) that is oftenaccompanied by nausea and vomiting. By the end ofthe disease, the vertigo subsides, but some people areleft with a sensorineural hearing loss. Physiciansattempt a variety of treatments to relieve the symptomsand to treat the increase in fluid, but no one treatmentis effective for all patients. The fluctuating hearingloss can be helped by a flexible hearing aid that can bereprogrammed as the hearing loss changes.
Neural Hearing LossAll of the conditions described above have theireffects primarily in the inner ear and on the haircells. A type of sensorineural hearing loss called neu-ral hearing loss may be caused by tumors on the audi-tory nerve along the auditory pathways in thebrainstem. These tumors generally grow slowly andare benign. However, when they are surgicallyremoved, the patient is often left with some hearingloss. In addition, neural hearing loss also can becaused by tumors or damage further along the audi-tory pathway.
THE EAR EXAMINATION ANDHEARING EVALUATION
We begin our description of the ear examination andhearing evaluation by considering the types of profes-sionals involved in the care of the ear and in helpingpeople maintain their hearing.
Who Examines Ears and Evaluates Hearing?A number of types of professionals examine the earand test hearing. The two main categories are oto-rhinolaryngologists and audiologists.
1. An otorhinolaryngologist is an M.D. who has spe-cialized in the treatment of diseases and disordersaffecting the ear, nose, and throat, and so thename of this specialty is often abbreviated ENT,
for “ear, nose, and throat.” ENT specialists carryout physical examinations of the ear, nose, andthroat and provide treatment through drugs andsurgery. Some physicians with ENT training spe-cialize in one area. For example, an otologist is anotorhinolaryngologist whose practice is limited toproblems involving the auditory and vestibular(balance) system.
2. An audiologist is a professional with a master’s ordoctoral degree who measures the hearing abilityof children and adults and identifies the presenceand severity of any hearing problems. If a hearingloss is identified, the audiologist can fit the personwith a hearing aid to make sound audible and alsomay work with the person on a long-term basis toteach communication strategies such as speechreading (also called lipreading) and other tech-niques for more effective communication. Theaudiologist may also recommend assistive devicessuch as telephone amplifiers and alerting systems.When hearing loss is found in children, the audi-ologist works with other professionals to make surethat the child develops a communication system(speech or sign language) and has access to appro-priate schooling.
ENT specialists and audiologists often worktogether in dealing with hearing problems and theear. For example, sometimes a person has a problemthat needs medical treatment by a physician and atthe same time sees an audiologist who helps the per-son deal with the hearing loss.
What Happens During an Ear Examinationand Hearing Evaluation?The basic aims of the ear examination and hearingevaluation are to assess hearing and to determinethe cause of defective hearing so it can be treated.The basic components of the examination are thefollowing.
Medical History The medical history focuses onhearing problems that the patient now has or mayhave had in the past, on general medical problems
569 Clinical Aspects o f Vis ion and Hearing
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 569
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license
that could affect the person’s hearing, on medicationsthat may be responsible for a hearing loss, and onnoisy work environments or hobbies, such as hunt-ing, that could affect hearing.
Otoscopy The purpose of otoscopy is to examinethe tympanic membrane. To do this, the physicianlooks into the ear using an otoscope, which, much inthe manner of the ophthalmoscope used to see theinside of the eye, illuminates the ear and makes itpossible to view the illuminated area. The physician
inspects the ear canal for foreign objects and signs ofdisease, notes the color of the tympanic membrane,and inspects it for evidence of tears.
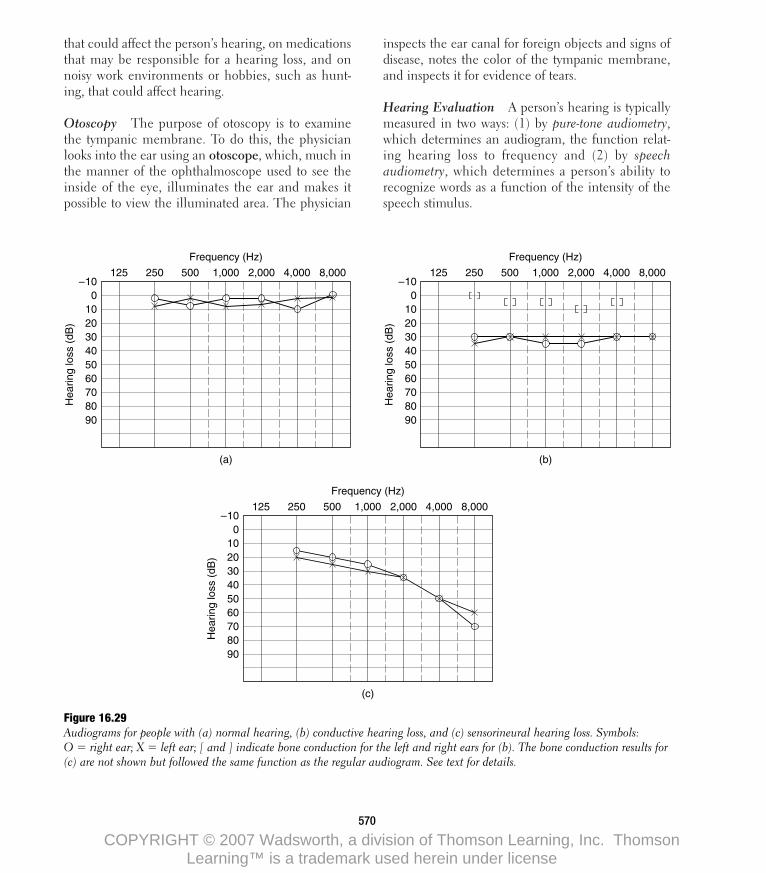
Hearing Evaluation A person’s hearing is typicallymeasured in two ways: (1) by pure-tone audiometry,which determines an audiogram, the function relat-ing hearing loss to frequency and (2) by speechaudiometry, which determines a person’s ability torecognize words as a function of the intensity of thespeech stimulus.
570
Hea
ring
loss
(dB
)
–100
125
102030405060708090
250 500 1,000
(a)
Frequency (Hz)
2,000 4,000 8,000
Hea
ring
loss
(dB
)
–100
125
102030405060708090
250 500 1,000
(c)
Frequency (Hz)
2,000 4,000 8,000
Hea
ring
loss
(dB
)
–100
125
102030405060708090
250 500 1,000
(b)
Frequency (Hz)
2,000 4,000 8,000
Figure 16.29 Audiograms for people with (a) normal hearing, (b) conductive hearing loss, and (c) sensorineural hearing loss. Symbols:O � right ear; X � left ear; [ and ] indicate bone conduction for the left and right ears for (b). The bone conduction results for(c) are not shown but followed the same function as the regular audiogram. See text for details.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 570
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

Pure-tone audiometry is typically measured by adevice called an audiometer, which can present puretone stimuli at different frequencies and intensities.The audiologist varies the intensity of the test toneand instructs the patient to indicate when he or shehears it. When the person’s threshold has been deter-mined at a number of frequencies, the audiometercreates an audiogram, a plot of degree of hearingloss (compared to normal) versus frequency. Figure16.29a shows the audiogram of a patient with normalhearing, and the audiograms in Figures 16.29b and16.29c are of a patient with about a 30-dB loss ofhearing at all frequencies and a patient with high-frequency loss, respectively. Audiograms are plottedso the curve for a person with normal hearing fallsbetween the zero line and 15-dB hearing loss for allfrequencies, and any hearing loss is indicated by sym-bols below the 15-dB hearing loss line.
The pattern of hearing loss sometimes providesinformation regarding the nature of the patient’s prob-lem. For example, the audiogram in Figure 16.29b, inwhich the hearing loss is approximately the sameacross the range of hearing, is typical of a patient witha conductive hearing loss. The record in Figure16.29c, in which hearing becomes progressivelyworse at high frequencies, is typical of sensorineuralhearing loss. Hearing loss due to exposure to noisetypically shows a maximum loss at about 4,000 Hz.
The way to differentiate between sensorineuraland conductive hearing losses is to compare a person’shearing when the stimulation is presented through theair, as when sound is heard from a loudspeaker orthrough earphones, and when it is presented by vibrat-ing the mastoid bone, which is located just in back ofthe ear. Bone conduction is measured by means of anaudiometer connected to an electronic vibrator thatpresents vibrations of different frequencies to the mas-toid. The person responds to the bone-vibrated signalin the same way as to air-conducted signals, andthresholds for bone conduction hearing are plotted onthe audiogram. If air-conduction hearing is worsethan bone-conduction hearing, this result indicatesthat something must be blocking sound in the outer ormiddle ear. If the bone conduction and air conduc-tion results are the same, the problem must be beyondthe outer and middle ear. The bracket symbols ([ and
]) in Figure 16.29b indicate normal bone conductionin the patient with conductive hearing loss.
Another way to measure hearing, which is partic-ularly important in people with sensorineural loss, isto measure their word recognition ability. To do this,the audiologist presents a series of tape-recordedwords at different intensities, and the patient is askedto identify the words that are spoken. The result is anarticulation function like the one in Figure 16.30,which plots the percentage of words identified cor-rectly versus the intensity of the sound. Patients withconductive losses tend to have articulation functionsthat are shifted to higher intensities, but, if the inten-sity is high enough, they can understand the words.Patients with sensorineural loss have functions thatare also shifted to higher intensities, but they oftenfail to reach 100 percent performance. Thus, in sen-sorineural hearing loss, many words cannot be con-sistently identified, no matter what their intensity.
Other diagnostic techniques, which we will notdescribe here, include tympanometry, in which a
571 Clinical Aspects o f Vis ion and Hearing
0
Per
cent
age
corr
ect
100
–20
Hearing level (dB)
100
80
60
40
20
0 20 40 60 80
Figure 16.30 Articulation functions for a patient with conductive hearingloss (solid line) and a patient with sensorineural hearingloss (dashed line). Both curves are shifted to the right com-pared to normal, indicating that the patient requires greaterthan normal intensity to recognize the words. Also, noticethat the curve for sensorineural hearing loss never reaches100 percent, no matter what the intensity.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 571
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

device called a tympanometer is used to measurehow well the tympanic membrane and the middle-ear bones are responding to sound vibrations, andmeasurement of the acoustic reflex threshold. Theacoustic reflex is the activation of the middle-earmuscles in response to high-intensity sounds. Thisactivation stiffens the chain of ossicles and dampenstheir vibration, perhaps to protect the inner ear frombeing overstimulated. The acoustic reflex can bemeasured with the tympanometer.
In addition to these diagnostic techniques thataccess hearing and the functioning of structures inthe ear, there are also tests that measure the electricalresponses of the auditory nerve and the auditory cor-tex, which are important if there is a hearing loss
even though the structures of the ear seem to be oper-ating normally. These electrophysiological measurescan therefore be useful in determining the location ofsensorineural hearing loss.
MANAGING HEARING LOSS
Hearing loss covers a very large continuum, from theindividual with mild hearing loss to someone who istotally deaf and cannot make use of sound for thepurpose of communication (Figure 16.31). Differentindividuals need different types of technology andstrategies in order to communicate effectively.
572
120
90
80
70
60
50
40
30
sth
ph
chio
z v
J m dnng
eu
l
b a r
0
Hea
ring
loss
(dB
)
8,0004,0002,0001,000
Frequency in cycles per second
500250125
k
f
sh
g
20
10
100
110
Figure 16.31 Audiogram showing the frequenciesand degree of hearing loss that causedifficulties in the perception of variousenvironmental sounds. The letters rep-resent spoken sounds. For example, aperson with a hearing loss of 100 dBaround 250 Hz will not be able tohear the lawn mower. (From Northern& Downs, 1978.)
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 572
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

The majority of individuals with conductivehearing loss receive medical treatment for their con-dition, and the hearing loss is eliminated as soon asthe disease process is eliminated. Patients who cannotor do not choose to take advantage of surgical or med-ical procedures may use an amplification system suchas a hearing aid to help them hear. As we noted whendescribing word recognition tests, as long as the soundis loud enough, these patients can hear quite well.
Individuals with sensorineural hearing loss gen-erally use some kind of amplification. Hearing aidshave changed drastically since the beginning of the1990s, with the development of smaller hearing aidsthat can be automatically programmed to work effec-tively in different listening situations. Almost all indi-viduals with sensorineural hearing loss can benefitfrom a hearing aid, which is fitted by an audiologist.
Hearing-impaired individuals also may receivetraining in speech reading (often called lipreading)and communication strategies. This type of training isoften called aural rehabilitation and is conducted byan audiologist. Some individuals have so much hear-ing loss that they cannot benefit from amplification.Many of these individuals consider themselves part ofthe deaf culture and are happy to communicate usingsign language. However, most people who lose theirhearing after being able to hear for the majority oftheir lives wish to continue to be connected to thehearing world. For these people, a new technologycalled the cochlear implant is available.
A cochlear implant is a device in which elec-trodes are inserted in the cochlea to create hearing byelectrically stimulating the auditory nerve fibers. Thisdevice offers the hope of regaining some hearing tosome people who have lost their hearing because ofdamaged hair cells, so that hearing aids, which canamplify sound but can’t cause that sound to be trans-lated into electrical signals in the hair cells, areineffective.
The cochlear implant bypasses the damaged haircells and stimulates auditory nerve fibers directly. Thefollowing are the basic components of a cochlearimplant (Figure 16.32):
• The microphone (1), which is worn behind theperson’s ear, receives the speech signal, transforms
it into electrical signals, and sends these signals tothe speech processor.
• The speech processor (2), which looks like a smalltransistor radio, shapes the signal generated by themicrophone to emphasize the information neededfor the perception of speech by splitting the rangeof frequencies received by the microphone into anumber of frequency bands. These signals are sent,in the form of an electrical code, from the proces-sor to the transmitter. Newer versions of cochlearimplants now package the entire speech processorin what looks like a behind-the-ear hearing aid.
• The transmitter (3), mounted on the mastoid bone,just behind the ear, transmits the coded signalsreceived from the processor through the skin to thereceiver.
• The receiver (4) is surgically mounted on the mas-toid bone, beneath the skin. It picks up the codedsignals from the transmitter and converts the codeinto signals that are sent to electrodes implantedinside the cochlea (5).
The implant makes use of Békésy’s observation,which we described in Chapter 10, that there is atonotopic map of frequencies on the cochlea, highfrequencies being represented by activity near thebase of the cochlea and low frequencies being repre-sented by activity at the apex of the cochlea. Themost widely used implants therefore have a multi-channel design, which uses a number of electrodes tostimulate the cochlea at different places along itslength, depending on the frequencies in the stimulireceived by the microphone. This electrical stimula-tion of the cochlea then causes signals to be sent tothe auditory area of the cortex, and hearing results.
What does a person using this system hear? Theanswer to this question depends on the person. Mostpatients are able to recognize a few everyday sounds,such as horns honking, doors closing, and waterrunning. In addition, many patients are able to per-ceive speech. In the best cases, patients can perceivespeech on the telephone, but it is more common forcochlear-implant patients to use the sounds perceivedfrom their implant in conjunction with speech read-ing. In one test, 24 patients scored 54 percent on a
573 Clinical Aspects o f Vis ion and Hearing
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 573
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

test of speech reading alone and 83 percent whenspeech reading was combined with sound from theimplant. In addition, the implant enabled patients totrack speech much more rapidly—16 words perminute using speech reading alone, and 44 words perminute with speech reading plus the implant (Brown,Dowell, & Clark, 1987; Owens, 1989). In another testit was found that deaf children who received acochlear implant before the age of 5 years were ableto learn to produce speech more easily than childrenwho received the implant when they were older (Tye-Murray, Spencer, & Woodworth, 1995).
As of 1995, over 10,000 people had receivedcochlear implants. The best results occur for postlin-gually deaf individuals—people who were able to per-ceive speech before they became deaf. These peopleare most likely to be able to understand speech withthe aid of the implant because they already know how
to connect the sounds of speech with specific mean-ings. Thus, these people’s ability to perceive speechoften improves with time, as they again learn to linksounds with meanings.
To place a more human face on the effects of thecochlear implant operation, we will end by relatingthe story of Gil McDougald, the standout New YorkYankee infielder who played in eight World Series inthe 1950s. McDougald, who in 1995 was 66 yearsold, had gradually gone deaf in both ears after anaccident in which he was hit by a line drive duringbatting practice in 1955. He was almost completelydeaf for about 20 years, being able to make out somesounds but no intelligible words. His deafness cuthim off from other people. He could no longer talkon the telephone, and he stopped attending “old-timers’” functions with ex-teammates like Yogi Berraand Mickey Mantle because he was unable to com-
574
2
1
3 4 5
Electrode Cochlea
Figure 16.32 Cochlear implant device. See text for details.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 574
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

municate with them. At family functions, he wouldleave the table because of his frustration at not beingable to hear what was going on.
McDougald heard about the implant operationand, in 1995, called implant specialist Noel Cohen atNew York University Medical Center. After testinghad determined that he was a good candidate for animplant, he underwent the operation. Six weeks afterthe operation, he went to see Betsy Bromberg, anaudiologist, to have the apparatus programmed andactivated (Figure 16.33). The following is an excerptfrom a newspaper account of what transpired in heroffice (Berkow, 1995):
In the office, McDougald sat at a desk with a com-puter on it. Bromberg sat across from him. His wife,Lucille, and daughter, Denise, sat within arm’slength.
A small microphone was set behind his ear, anda transmitter with a magnet was placed over the siteof the implant. A cable was extended from themicrophone to a speech processor the size of a handcalculator that can be worn on a belt or placed in abreast pocket.
Then Bromberg began the test that woulddetermine how much McDougald’s hearing hadimproved.
Bromberg covered her mouth with a sheet ofpaper so he could not lip read.
“Tell me,” she said, “what you hear.”She said, “aah.” He hesitated. “Aah,” he
answered. She went, “eeeh.” He said, “eeeh.”“Hello,” she said. “Hello,” he said. “I’m going
to count to five,” she said. “Do you hear me?”“Oh yeah!” he said. “Wow! This is exciting!”His wife and daughter stared, hardly moving.Bromberg wrote down four words on a pad of
paper and said them: “football,” “sidewalk,” “cow-boy,” and “outside.” “Now Gil,” she said, “I’m goingto mix up the word order and cover my mouth andyou tell me the word I say.”
“Cowboy,” she said. “Cowboy,” he said.“Outside,” she said. “Outside,” he said. And then hebegan to flush. Tears welled in his eyes.
“This is the first time in . . .” Lucille said andthen choked up, unable to finish her sentence. “It’sunbelievable.”
“It’s a miracle,” said Denise.Both began crying.Bromberg said, “It’s O.K. Everybody cries at
times like this.” And then mother and daughterembraced. And they hugged Gil. And they huggedBromberg, and hugged the director of the unit,Susan Waltzman, who had been observing. . . .
575 Clinical Aspects o f Vis ion and Hearing
Figure 16.33Gil McDougald trying out his cochlearimplant for the first time, with audiologistBetsy Bromberg. In the office, McDougaldsat at a desk with a computer on it.Bromberg sat across from him. His wife,Lucille, and daughter, Denise, sat withinarm’s length.
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 575
Figure Not Available
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

Last night, the McDougald household wasbursting with children and grandchildren.“Everyone,” said Lucille McDougald, “has come towatch grandpa hear.” (p. B8)
Cochlear implantation is an impressive demon-stration of how basic research yields practical benefits.Advances such as this, which have proven to be effec-tive in bringing deaf adults and children into theworld of hearing (Kiefer et al., 1998; Tye-Murray etal., 1995), are the end result of discoveries that beganin perception or physiology laboratories many yearsearlier. In this case, it was George von Békésy’sresearch on how the vibration of the basilar mem-brane depends on the frequency of the sound that
provided the knowledge about the operation of theear that made implants possible. Systems also havebeen proposed for restoring vision to people who areblind, by stimulating their visual cortex (Dobelle,1977; Dobelle, Mladejovsky, & Girvin, 1974; Dobelleet al., 1976), and for guiding blind people through theenvironment by applying the principles of auditorylocalization to the design of a “personal guidance sys-tem” (see Chapter 11, page 379).
It is clear that the study of both the psycho-physics and the physiology of perception has yieldednot only knowledge about how our senses operate butalso ways to apply this knowledge to create new per-ceptual worlds for people like Gil McDougald andcountless others.
576
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 576
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

577 Clinical Aspects o f Vis ion and Hearing
T H E P L A S T I C I T Y O F P E R C E P T I O N
Decrease in Cortical Function Due to Aging
As people age they experience decreases in visualacuity, contrast sensitivity, motion sensitivity, andwavelength sensitivity. We’ve seen that some ofthese decreases can be attributed to problems atthe “front end” of the visual system, such as cata-racts, the clouding of the lens that causes blurredvision. Another problem that occurs in the eye ispresbyopia, the loss of the ability to accommodate.Both of these problems involve a disruption of theprocesses that normally focus light as it enters theeye. However, these problems cannot totallyexplain the degree of decline in acuity and otherfunctions that occurs with aging. To understandthe overall effect of the aging process in vision, weneed to consider how aging affects the brain.
Matthew Schmolesky and coworkers (2000)investigated cortical changes due to aging, byrecording from neurons in area V1 of the monkeyand determining how the neurons’ tuning for ori-entation changes with age. They found that thefairly narrow orientation tuning observed in mostof the neurons of the young monkeys was lesscommon in the older monkeys.
Figure 16.34 shows the orientation tuning fortwo neurons recorded from old monkeys. Curve(a) is a narrowly tuned neuron and curve (b) is abroadly tuned neuron. Only 42 percent of theneurons in the older monkeys were narrowlytuned, compared to 90 percent in young mon-keys. Schmolesky and coworkers suggest that asmonkeys age they lose the inhibitory connectionsbetween neurons that are needed to create orien-tation tuning.
What might be going on for the old monkeysmay be similar to what happens when kittens oryoung monkeys are raised in environments thatcontain just one orientation (see page 100). Inthese selective rearing experiments, neurons thatnormally respond to the orientations that areabsent lose their ability to respond to those orien-tations. A similar thing may be occurring in aging,except that the properties that change rapidlywhen young animals are visually deprived orreared in selective environments change slowly,over a much longer period of time, during aging.
Figure 16.34 Orientation tuning of neurons inarea V1 of an older monkey: (a) atuned neuron that responds betterto some orientations than othersand (b) a nonselective neuron thathas broad tuning, respondingalmost equally well to all orienta-tions. (From Schmolesky et al.,2000.)
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 577
Figure Not Available
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

578
A C R O S S T H E S E N S E S
dren with normal hearing or children who havesome hearing, because of a cochlear implant?Although we don’t know the answer to this question,we can guess that it may have something to do withhow the ability to hear might affect attention in gen-eral. A person hears a sound and turns his headtoward it. A person in a crowded room that is pulsat-ing with many conversations directs her attention tothe one person with whom she is talking. A personsitting in a coffee house alive with conversation andmusic has learned to focus his attention on the bookhe is reading. Each of these examples involves boththe focusing of attention and hearing. Because deaf
DE A F N E S S A N DVI S UA L AT T E N T IO N
There is evidence supporting the idea that the sensesare linked to each other during development (Smith& Katz, 1996). According to this idea, both seeingand hearing develop in tandem with one another, sothat if one sense becomes deficient during develop-ment, it is possible that the other will be deficient aswell. Alexandra Quittner and her coworkers (1994)tested the idea that loss of hearing causes a change inthe capacity for visual attention by testing threegroups of children, a deaf group, a deaf group whohad received cochlear implants, and a group withouthearing impairment. Subjects in each of thesegroups were shown a sequence of numbers presentedvisually, one after another, and were told to push abutton every time they saw a 9 after a 1. This task,which requires that the subject pay close attention tothe numbers at all times, is used to identify childrenwith serious attentional deficits.
The results of this experiment, shown in Figure16.35, supported the idea of a link between visionand hearing. The deaf subjects had the poorest per-formance, those with the cochlear implant did bet-ter, and the hearing subjects performed best of all.Thus, the better the subjects could hear, the betterthey performed on a task that was purely visual.
Quittner checked this result in another way bytesting the visual attention of subjects after they hadbeen using a cochlear implant for 10 months andthen testing them again at 18 months. When theycompared their performance to a group of deaf sub-jects who were tested at the same time intervals, theyfound that there was no difference at 10 months butthat by 18 months the cochlear implant group wasless likely to commit “false alarms”—that is theywere less likely to say the target (the 9) was therewhen it actually wasn’t.
Why should deaf children be more likely to bedistracted from a visual attention task than are chil-
Figure 16.35 Performance of deaf subjects, subjects who had been using acochlear implant, and hearing subjects on a visual atten-tion test. (Adapted from Quittner et al., 1994.)
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 578
Figure Not Available
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

ability in one sense might in an indirect way cause adecrease in a person’s ability in another sense.
579 Clinical Aspects o f Vis ion and Hearing
people do not have any of these experiences, they aremissing opportunities that might help them becomebetter at focusing their attention. Thus, the loss of
Conductive Hearing LossConductive hearing loss is associated with reduced transmission ofsound stimuli into the cochlea. Outer-ear disorders include damagedue to putting objects in the ear, infection, and rupturing of the tym-panic membrane. Middle-ear disorders include the infection otitismedia, a condition in which tissue builds up called cholesteatoma,and otosclerosis, a hereditary condition in which there is a growthof bone in the middle ear.
Sensorineural Hearing LossSensorineural hearing loss is associated with damage to the innerear. Presbycusis is a loss of high-frequency sensitivity that is con-nected with aging. Noise-induced hearing loss occurs when loudnoises cause degeneration of the hair cells. This can occur due tolong-term exposure or implosive noises such as explosions. Tinnitusis a ringing in the ears that can be extremely debilitating. Meniere’sdisease is caused by excessive buildup of the liquid that fills thecochlea. All of the sensorineural conditions described above affectthe inner ear and the hair cells. Neural hearing loss describes con-ditions caused by damage to the auditory nerve or other auditorysystem structures.
The Ear Examination and Hearing EvaluationEar examinations are carried out by otorhinolaryngologists (ear,nose, and throat specialists) and audiologists. The ear examination
and hearing evaluation consist of the following components: med-ical history; otoscopy, to check the integrity of the tympanic mem-brane; hearing evaluation, measured by pure-tone audiometry orword recognition tests; and tympanometry, to check the response ofthe tympanic membrane.
Managing Hearing LossHearing loss can be managed by using hearing aids and training inspeech reading. For people whose hair cells are damaged, installa-tion of a cochlear implant is an option for partially restoring hearing.
Plasticity: Decrease in Cortical Function Due to AgingA number of visual functions decrease as a consequence of aging.The cause of this decrease can be traced to problems with the eyeand also to changes in the visual cortex. Research on monkeysshows that many of the neurons in area V1 of older monkeys havelost their orientation tuning.
Across the Senses: Deafness and Visual AttentionIn a test of visual attention, deaf subjects had the poorest perform-ance, those with cochlear implants did better, and hearing subjectsperformed best of all. The reason for this may be that in hearingsubjects sound often helps orient visual attention.
S U M M A R Y T A B L E 1 6 . 2
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 579
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license

How Can Vision Become Impaired?
1. What are the four major types of problems that cancause poor vision? (546)
Focusing Problems
Myopia
2. What is myopia? How are parallel rays of light broughtto a focus in the myopic eye? What are the two possi-ble causes for this incorrect focusing? (547)
3. How can we cause the point of focus to fall on theretina of a myopic eye without using corrective lenses?(547)
4. What is the far point? Where does the focus point fallif an object is farther from the eye than the far point?At the far point? Closer to the eye than the far point?Can a myope bring faraway objects into focus byaccommodation? (548)
5. How must a corrective lens bend light so that a myopecan see clearly? (548)
6. What is a diopter? Be able to calculate the correctionin diopters if you are given the distance of the far point.(548)
7. What are two surgical procedures involving lasers thatcan correct myopic vision? (549)
Hyperopia
8. What is hyperopia? How are parallel rays of lightbrought to a focus in the hyperopic eye? How is thiscondition corrected? (550)
Presbyopia
9. What is presbyopia? What is the near point? What hap-pens to the near point as a person ages? (550)
Astigmatism
10. What is astigmatism? What causes it? How is this con-dition corrected? (550)
Decreased Transmission of Light
What Is Blindness?
11. What is the legal definition of blindness? Can a personwho is legally blind have 20/20 vision? Explain youranswer. (551)
Corneal Disease and Injury
12. The cornea is responsible for about percent ofthe eye’s focusing power. (552)
13. What can cause corneal diseases or injury? What is thefirst treatment for corneal disease or injury? If thistreatment fails, what is the next alternative? (552)
14. Describe a corneal transplant operation. Exactly whatis transplanted? What is the success rate of cornealtransplants? (552)
Clouding of the Lens (Cataract)
15. What is a cataract? What is the most common kind ofcataract, and what percentage of people over the age of65 have cataracts? What percentage of cataracts areserious enough to interfere with a person’s normalactivities? What percentage require surgery? (553)
16. Describe a cataract operation. (553)
17. When we remove the lens in a cataract operation, wedecrease the focusing power of the eye. Why areglasses an unacceptable solution to this problem?What is the solution to this problem? (553)
Damage to the Retina
Diabetic Retinopathy
18. What is the tissue upon which the retina rests? (554)
19. Describe what happens to the retinal circulation inmild and severe cases of diabetic retinopathy. (554)
20. Describe a procedure that has been used to stop neo-vascularization. (555)
21. What is a vitrectomy operation? What does it accom-plish? (555)
580
STUDY QUESTIONS
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 580
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license
Macular Degeneration
22. Describe the mild and severe types of macular degen-eration. What is a treatment that can be successfullyused in some patients? (555)
Detached Retina
23. What is a detached retina? What are two reasons that adetached retina can affect vision? (556)
24. Describe the procedure used to reattach a detachedretina. (556)
Hereditary Retinal Degeneration
25. What is retinitis pigmentosa? (557)
Optic Nerve Damage: Glaucoma
26. Describe the two forms of glaucoma. How are thesetwo types treated? (557)
The Eye Examination
Who Examines Eyes?
27. Describe the training and capabilities of ophthalmolo-gists, optometrists, and opticians. (558)
What Happens During an Eye Exam?
28. What are the four basic aims of an eye examination?(559)
29. How is visual acuity determined? What does it mean tosay that a person has 20/200 vision? (559)
30. What is visual perimetry? (560)
31. What is the purpose of the refraction part of the eyeexamination? What are the two steps in the refractionexam? (561)
32. What is the purpose of the external eye examination?(561)
33. What is the purpose of the slit-lamp examination?(561)
34. What does the tonometry exam measure? For what dis-ease does it test? What is the basic principle behind thetonometry exam? (561)
35. What is the basic principle behind an ophthalmo-scope? Be able to draw a diagram of an ophthalmo-scope. (563)
36. What does the examiner look for in an ophthalmo-scopic exam? (563)
37. What is fluorescein angiography, and what does itaccomplish? (564)
How Can Hearing Become Impaired?
38. What is the difference between a hearing impairmentand a hearing handicap? (564)
39. What are the four types of things that can go wrong inthe auditory system? (565)
Conductive Hearing Loss
40. What is conductive hearing loss? (566)
41. Describe outer-ear disorders and middle-ear disorders.(566)
Sensorineural Hearing Loss
42. What is sensorineural hearing loss? (567)
43. What is the most common form of sensorineural hear-ing loss? Describe the role of aging and environmentalexposure in causing this condition. (567)
44. Where is the main damage in noise-induced hearingloss? (567)
45. What is tinnitus? How can it be treated? (568)
46. Describe Meniere’s disease. (568)
47. What is neural hearing loss? (569)
The Ear Examination and Hearing Evaluation
Who Examines Ears and Evaluates Hearing?
48. Describe the training and capabilities of otorhino-laryngologists and audiologists. (569)
581
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 581
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license
What Happens During an Ear Examinationand Hearing Evaluation?
49. What is the purpose of otoscopy, and how is it con-ducted? (570)
50. Describe pure-tone audiometry. What is an audio-gram? Describe how the pattern of hearing loss canprovide information regarding the nature of a patient’sproblem. (570)
51. Describe how vibration of the mastoid bone can beused to differentiate between sensorineural hearingloss and conductive hearing loss. (571)
52. What is the articulation function? (571)
53. Describe tympanometry and the acoustic reflex. (571)
Managing Hearing Loss
54. What types of treatment are used for conductive hear-ing loss and sensorineural hearing loss? (572)
55. What is aural rehabilitation? (573)
56. Describe how a cochlear implant operates. How suc-cessful have cochlear implants been in restoring hear-ing? (573)
The Plasticity of Perception: Decrease in Cortical Function Due to Aging
57. What kinds of decreases in vision occur due to aging?(577)
58. How do problems in the eye contribute to these visualdecreases? (577)
59. What is the evidence from monkey recording experi-ments that aging affects neurons in area V1? (577)
Across the Senses: Deafness and Visual Attention
60. Describe the experiment of Quittner and coworkersthat tested the idea that a loss of hearing causes achange in the capacity for visual attention. (578)
61. Describe Quittner’s other experiment in which sheused subjects who had been using a cochlear implant.(578)
62. What is a possible explanation for the fact that deafchildren are more easily distracted from a visual atten-tion task than children with normal hearing or chil-dren with a cochlear implant? (578)
582
4730_ch016_545-582.qxd 1/27/04 2:11 PM Page 582
COPYRIGHT © 2007 Wadsworth, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license


![Novel of the nearsighted adolescent This project has been funded with support from the European Commission. This publication [communication] reflects the](https://img.dokumen.tips/doc/110x75/56649e895503460f94b8df4a/novel-of-the-nearsighted-adolescent-this-project-has-been-funded-with-support.jpg)