Embed Size (px)
Citation preview

1
School of Health Sciences, Jönköping University
Foodwork and meals in everyday life among
persons with dementia and their partners
LINDA JOHANSSON
DISSERTATION SERIES NO. 45, 2013
JÖNKÖPING 2013

2
© Linda Johansson, 2013
Publisher: School of Health Sciences Print: Intellecta Infolog
ISSN 1654-3602
ISBN 978-91-85835-44-7

Abstract
The aim of this thesis was to explore and describe foodwork and meals for older persons with dementia and their partners in ordinary homes.
Descriptive and explorative designs were used in the four papers this thesis is based on. Longitudinal data, including older home-living unlike-sex twins, were analysed using descriptive and analytical statistics. An ethnographic approach was used to describe everyday life for persons with dementia. Interviews with partners and staff were analysed using thematic analysis and qualitative content analysis, respectively.
The results revealed that, among home-living older persons, there is an association between a person’s cognitive ability and nutritional status; i.e. low cognitive ability leads to increased risk of malnutrition. For home-living persons with dementia and their partners, foodwork and meals sometimes changed, meaning that shopping, preparing food and eating as well as social interaction become complicated, which seemed to lead to transitions in roles, routines and relations. There was foodwork that the persons with dementia could perform, and participants expressed a desire that abilities and independence be preserved. However, support was sometimes needed, and it was emphasized that this was based on the person’s needs, wishes and problems.
In conclusion, there is an association between decreased cognitive ability and increased risk of malnutrition. Furthermore, foodwork and meals affected both persons with dementia and their partners. Therefore, early intervention whereby both partners in a couple get individually adjusted support is of importance. Consequently, a person-centred care approach can be useful in arranging the support.

Original papers
The thesis is based on the following papers, which are referred to by their Roman numerals in the text:
Paper I Johansson L, Sidenvall B, Malmberg B & Christensson L (2009): Who will become malnourished? A prospective study of factors associated with malnutrition in older persons living at home. The Journal of Nutrition, Health and Aging 13, 855-861.
Paper II Johansson L, Christensson L & Sidenvall B (2011): Managing mealtime tasks: told by persons with dementia. Journal of Clinical Nursing 20, 2552-2562.
Paper III Johansson L, Sidenvall B, Björklund A & Christensson L: Dancing on a slack tightrope: spouses’ experiences of food activities and meals with a partner suffering from dementia. Submitted.
Paper IV Johansson L, Björklund A, Sidenvall B & Christensson L: Staff views on improving foodwork and meals for home-living persons with dementia. Submitted. Papers I and II have been reprinted with the kind permission of the respective journals.

Contents
Acknowledgements ....................................................................................... 8 Introduction ................................................................................................ 10 Background ................................................................................................. 11
The home as the arena for care ................................................................. 11 Everyday life when living with dementia ................................................. 12
Everyday life for persons with dementia .............................................. 13 Being the partner of a person with dementia and sharing everyday life .............................................................................................................. 14 Formal caregiving using a person-centred perspective ........................ 15
Foodwork and meals at home ................................................................... 16 Traditions, routines and roles ............................................................... 17 Dependence and independence applied to the activities of foodwork and meals ..................................................................................................... 18 Nutritional problems among home-living older persons ...................... 19
Foodwork and meals when living with dementia ..................................... 20 Being a person with dementia and its effect on foodwork and meals .. 20 Changes in foodwork and meals experienced by partners ................... 21 The Life Nourishment Theory .............................................................. 22 Support in foodwork and meals ............................................................ 23
Rationale for the thesis ............................................................................... 25 Aim of the thesis ......................................................................................... 26 Method ......................................................................................................... 27
Design ....................................................................................................... 27 Participants and setting ......................................................................... 29
Data collection .......................................................................................... 36 Quantitative data................................................................................... 36
Instruments ....................................................................................... 36 Supplementary variables .................................................................. 37
Qualitative data .................................................................................... 37

Individual interviews ........................................................................ 37 Focus group interviews .................................................................... 38
Data analyses ............................................................................................ 38 Quantitate data ...................................................................................... 38 Qualitative data .................................................................................... 39
Thematic analysis ............................................................................. 39 Content analysis ............................................................................... 41
Ethical considerations .............................................................................. 42 Findings ....................................................................................................... 44
Cognitive ability as an associated factor for malnutrition among home-living older men and women (I) ............................................................... 44 Changes that occur in the couples regarding foodwork and meals (II, III) .................................................................................................................. 45 Activities of importance to uphold regarding foodwork and meals (II, III, IV) ............................................................................................................ 46 Adjusting foodwork and meals to cognitive changes (II, III, IV) ............ 47
Discussion .................................................................................................... 50 Reflection on the findings ........................................................................ 50
Decreased cognitive ability increases risk of problems with nutritional status and foodwork ............................................................................. 50 Transition in roles, routines and relationships ...................................... 52 The importance of staying independent ............................................... 55 Using a person-centred care approach is essential in foodwork and meals .................................................................................................... 56
Methodological considerations ................................................................ 58 Validity and reliability ......................................................................... 58 Trustworthiness .................................................................................... 60
Conclusions and implications ................................................................... 63 Svensk sammanfattning ............................................................................. 65 References ................................................................................................... 67
Appendices 1-2 ............................................................................................ Appendix 1: Questions Paper I ..................................................................... Appendix 2: Interview guides ......................................................................

8
Acknowledgements
When I read a thesis this is usually were I start, and it is often also the only part I actually read. However, I do hope that when you are finished reading this section you will at least read the abstract to get an understanding of what this thesis is actually about. I namely believe that we owe it to the people who have offered their time and let me into their homes to share their stories of everyday life and thus made it possible to increase the knowledge about foodwork and meals when living with dementia. To all of you who participated, I want to express my sincere gratitude.
Many people have contributed in different ways to make this thesis possible, and more than anyone I would like to thank my supervisors for believing in me and encouraging me.
Lennart Christensson, my main supervisor: Thank you for always being there for me. You’ve played a big part in making my time as a PhD student fantastic.
My co-supervisors: Birgitta Sidenvall, thank you for all your passion and interest in my research, as well as for your way of always making me feel good; and Anita Björklund, for joining my supervising team at a time when I needed you the most. Your constructive advice and quick responses have been invaluable.
Bo Malmberg: Thank you for letting me use data from the Gender study, and for being a co-author on Paper I with all your expertise in data and statistics.
Further, I am most grateful to the School of Health Sciences at Jönköping University, the Dementia Association in Sweden, Futurum – the Health Care Academy in the Jönköping County Council, KP-Stiftelsen and the Swedish Society of Nursing, for financial support.
Thank you to the professionals who were involved in the participant inclusion procedure for the project, and to Hertha Ljungman for helping me with the data collection.
9
Heather Keller: Thank you for letting me use, and also for reading and commenting on, the paragraph about the Life Nourishment Theory.
My wonderful colleagues, past and present, at the Research School of Health and Welfare. You have made my days, and I’m really going to miss our fantastic discussions about research, methods and theories. Especially Marit and Marie, thank you for all the time and effort you’ve put into my thesis, but also for all the laughter and memories – I want you to know how much I’ve missed you this past year and a half! Tomas, thanks for all the ‘pre-fika’ moments; and Annette, thank you for running alongside me this final year – it’s been a pleasure! Paula, coordinator of the Research School, you have helped me more than anyone could have expected. I’m really going to miss asking you things instead of looking them up myself on the Web…
Finally, I would like to thank my family and friends. Not because you’ve helped me write this thesis but because you’ve made sure that my time as a PhD student was not a lifestyle but just work, which has always been my motto. Firstly, thanks to HIF for all the running hours; especially Anna and Ulrika – you’re the best! Secondly, my parents and mostly my mom, for making sure I got myself a university degree. I’m not sure you really meant that I have to go on forever, but I know you’re proud of me. Lastly, but first in my heart, I would like to thank my beloved family: Per, Lukas and Ellie. Spending time with you has really made me forget about work. I love you all!
Jönköping, April 2013
Linda Johansson

10
Introduction
Traditionally, the provision of food and fluids to patients has been considered to be in the area of nursing, and already in the 1850s Nightingale wrote “Every careful observer of the sick will agree in this that thousands of patients are annually starved in the midst of plenty” (p. 37). Further, she described how nurses could help the patient eat and what kind of food was preferable (Nightingale, 1992). About 100 years later Henderson (2004) described that, in nursing, it is important to have knowledge about not only nutrition but also families’ social and cultural standards regarding food. However, even though it is quite common to assess nutritional status among older persons today, the phenomenon of meals is often overlooked; i.e. how older persons choose, prepare, serve and eat food (Amella & Aselage, 2011). Further, the Swedish Society of Nursing points out that intervention studies are needed, with persons’ problems and wishes serving as the basis in planning for care and meals (Swedish Society of Nursing, 2013).
It is reasonable to believe that Nightingale and Henderson were thinking about persons receiving hospital care when writing their theories. In our time, however, it is a different scenario: the number of beds in hospitals has decreased (McKee, 2004), and policies favour caring for older persons at home (Genet et al., 2011). This is also true for persons with dementia, and as the disease is increasing in the world (Alzheimer’s Association, 2013) it is important to further develop the care for these persons. Regarding meals in the home context among persons with dementia, little is known and further research is needed and called for (Aselage & Amella, 2010). Paying attention to, and increasing, the knowledge about meals is of great importance as it contributes to health and quality of life (Amella & Aselage, 2011). Therefore, the aim of this thesis is to explore and describe foodwork and meals for home-living older persons with dementia and their partners.

11
Background
The home as the arena for care
In Sweden, the national policy is that older persons should stay in their ordinary homes as long as possible (Ministry of Health and Social Affairs, 2003:91). Living in one’s own home is also what older people themselves have expressed as important (Tanner, Tilse, & De Jonge, 2008). In Sweden, many older people live in their own household, and this is also common among people with dementia (National Board of Health and Welfare, 2006b). However, when suffering from a dementia disease the ability to stay in one’s ordinary home is affected (Luppa et al., 2010), and persons with dementia tend to move to special housing earlier compared to others (National Board of Health and Welfare, 2005). To be able to stay in their ordinary home many older persons rely on support; approximately 250,000 older persons (>65 years) in Sweden use some kind of assistance (National Board of Health and Welfare, 2012). For persons with dementia, help and support from others becomes successively necessary, and cognitive impairment is associated with an increased use of home-help service (Meinow, Kåreholt, & Lagergren, 2005). In Sweden, formal dementia care involves staff from both the municipality and the county council, depending on what kind of care a person needs (National Board of Health and Welfare, 2010).
The Ädelreform took effect in 1992, changing the organization of care for older persons by giving municipalities the main responsibility for the care (Thorslund, Bergmark, & Parker, 1997). This is stressed in the Health and Medical Services Act and the Social Services Act, in which it can be read that the municipalities should provide for people to live independently in their own household, and are responsible for delivering good quality care to those in need (Ministry of Health and Social Affairs, 1982:763; 2001:453). These acts do not further describe the care to be delivered, or what is to be offered to those in need of support. In a European study, differences in home care have been found to be related to its organization and finances (Genet et al., 2011). In Sweden, it is common that municipalities have local guidelines

12
regarding available assistance (Blomberg, 2004; Trydegård, 2000). Care managers in Sweden have expressed that they try to meet the older person’s needs but that this is not always possible because of limitations in the service (Dunér & Nordström, 2010), and they tend to make decisions – i.e. suggest assistance – that agree with local guidelines (Dunér & Nordström, 2006). This might be one explanation for why food distribution has increased in municipalities whilst support regarding food preparation in the home has decreased (County Administration Boards of Sweden, 2009). According to Larsson (2006), the total use of formal services decreased in the older population in Sweden between the 1980s and the 2000s. Instead, it is most common that those in need of help in the home receive informal care (Nordberg, Von Strauss, Kåreholt, Johansson, & Wimo, 2005; Sundström & Johansson, 2005) – despite the fact that the family’s efforts in caregiving are supposed to be a supplement to public care (Lagergren, 2002). However, this depends on the person’s social network, and those living alone receive less informal care compared to those living with someone, and single-living persons seem to receive a higher level of formal care (Larsson & Thorslund, 2002).
Everyday life when living with dementia
Approximately 36 million people worldwide have dementia (World Health Organization [WHO] and Alzheimer’s Disease International, 2012) and it is estimated that this number will double every 20 years, with the highest increase occurring in the developing countries (Ferri et al., 2006). Dementia mainly affects older people (WHO, 2012), and as the number of older people is rising around the world, more will develop a dementia disease (Alzheimer’s Association, 2013). For instance, approximately 1% of people have dementia at the age of 65 compared to over 50% of those in their 90s (Swedish Council on Technology Assessment in Health Care, 2008). Dementia is a syndrome that includes several diseases, the most common are Alzheimer’s disease, vascular dementia, dementia with Lewy bodies, and frontotemporal dementia. However, it is common for individuals to have mixed types. A dementia leads to a deterioration in cognitive function and affects, for instance, memory, orientation, learning ability, language and judgment. It is not only the individual who has dementia who is affected;
13
families, caregivers and society are all influenced physically, psychologically, socially and economically by the disease (WHO, 2012).
Everyday life for persons with dementia
Persons with dementia have described that they associate the disease with feelings of loss (Ostwald, Duggleby, & Hepburn, 2002), which can be related to the assertion that having a dementia can lead to difficulties performing daily activities (Agüero-Torres, Thomas, Winblad, & Fratiglioni, 2002; WHO and Alzheimer’s Disease International, 2012). Further, one’s ability to live independently can be affected (Luppa et al., 2010). Additionally, difficulties in managing the home situation increase gradually (von Kutzleben, Schmid, Halek, Holle, & Bartholomeyczik, 2012), with practical skills diminishing and problems performing ordinary activities arising along with problems dealing with new situations and activities (Steeman, de Casterlé, Godderis, & Grypdonck, 2006). In order to accomplish everyday activities, persons with dementia have described that they sometimes avoid certain situations (Gillies, 2000) and that their own expectations of what they are able to do decrease (De Boer et al., 2007). Further, relying on others (Steeman, Godderis, Grypdonck, De Bal, & De Casterlé, 2007), minimizing or denying what is happening, and comparing oneself with others who have more severe problems have also been described (De Boer et al., 2007). However, this does not mean persons with dementia per se become passive when experiencing problems; instead, it has been described how people actively try to find strategies for managing the situation (Nygård, 2004; von Kutzleben et al., 2012; Öhman, Josephsson, & Nygård, 2008). Keeping notes and writing in diaries are examples of such strategies (De Boer et al., 2007). Consequently, suffering from the same disease does not mean that the experiences are the same for all individuals with dementia. In an interview study, it was found that experiences ranged from those who did not feel it was “such a big deal” to those who described life as hell (Hulko, 2009).
Even though dementia is a progressive disease, positive aspects have been expressed. People with dementia usually try to uphold their life as much as possible by maintaining daily routines and activities (De Boer et al., 2007), by trying to live in the present (von Kutzleben et al., 2012) and by focusing

14
on their remaining abilities instead of the severities (Steeman et al., 2007). Feelings like optimism, satisfaction and appreciation have been expressed in descriptions of what it means to live with the disease (Ostwald et al., 2002). Further, relationships with others have been described in terms of love, affection and closeness (Steeman et al., 2007).
Being the partner of a person with dementia and sharing everyday life
Being the partner of a person with dementia has been experienced as a changed situation in which several aspects of daily life are affected. Even so, positive experiences appeared, and doing things together, for instance, could result in closeness and meaningfulness (Persson & Zingmark, 2006); it has also been described that there is still affection, love and closeness within the relationship (Hellström, Nolan, & Lundh, 2007). In a review examining relationships between family caregivers and persons with dementia, even increased closeness, warmth and mutual affection were found (Ablitt, Jones, & Muers, 2009). The importance of doing things without the person with dementia has also been expressed, as this offers time to rest, even though it was difficult to get this time alone. Conflicts arose when choosing between the needs of the person with dementia and one’s own needs (Persson & Zingmark, 2006).
A transition in the relationship is commonly described, whereby a couple moves from being equal partners towards a situation in which the healthy spouse becomes more of a caregiver than a partner (Walters, Oyebode, & Riley, 2010). Still, involving the person with dementia in activities has been described as important (Butcher, Holkup, & Buckwater, 2001). For example, in studies of wives caring for their husbands with dementia it has been found that they took over their husband’s old responsibilities but at the same time tried to include them in activities with fewer risks, like domestic work, to make them feel like they were contributing something (Hellström, Nolan, & Lundh, 2007). The transition resulted in partners giving up most of their own life to be able to take care of the person with dementia (Jansson, Nordberg, & Grafström, 2001). Making all the decisions for the couple can lead to feelings of loneliness and abandonment (Persson & Zingmark, 2006). This might result in feelings of stress and burden, as well as declined health

15
(Brodaty & Donkin, 2009; Etters, Goodall, & Harrison, 2008), which have been found to be reasons for the person with dementia moving to special housing (O’Malley & Croucher, 2005). However, pride at achieving activities while caring for the partner with dementia has been described among husbands (Sanders & Power, 2009). Furthermore, appreciating the small pleasures in life and trying to find the positive things in life as well as living in the present can be ways to preserve the relationship (Hellström, Nolan, & Lundh, 2007).
Formal caregiving using a person-centred perspective
To be able to treat and care for persons with dementia within their life situation, a bio-psycho-social perspective is needed in health care. One way to achieve this would be through person-centred care. Kitwood (1997) was the first to articulate the importance of using a person-centred care as a response to the biomedical view that had previously been central in dementia care. There is no consensus regarding person-centred care but several researchers, like Brooker (2004), Edvardsson, Winblad, & Sandman (2008) and Slater (2006), have tried to describe the meaning of the concept. At least there seems to be an agreement that the concept includes several dimensions, and that the focus is on the person behind the disease instead of on the disease itself, whereby the person’s subjective experiences are of great importance (Brooker, 2004, 2007; Edvardsson et al., 2008; Slater, 2006). According to a review by Edvardsson et al. (2008), person-centred care includes: considering the personhood concealed but not lost; acknowledging the personhood in all aspects of care; creating a personalized care and environment; sharing decision-making; understanding behaviours from the subjective world of the person; and prioritizing relation and care tasks equally (Edvardsson et al., 2008). A recent study, in which persons with dementia, family and staff were interviewed, highlights the importance of including the family in the care (Edvardsson, Fetherstonhaugh, & Nay, 2010), the previous neglect of which has been pointed out in criticism of the concept. Nolan, Davies, Brown, Keady and Nolan (2004) highlight that this probably has to do with the individualistic focus of person-centred care.
In Sweden, person-centred care has not had as much clinical impact as in other countries (Edvardsson, 2011). However, Ekman et al. (2011) assert

16
that formal caregivers today broadly acknowledge the meaning and importance of this concept for care. Recently, national guidelines were developed for health care professionals working with persons with dementia, whereby person-centred care is also advocated (National Board of Health and Welfare, 2010). One might argue that person-centred care is also important when caring for person with poor nutritional status, as research shows that an individualized nutritional programme based on a person’s problems, desires and resources can improve nutritional status (Lorefält & Wilhelmsson, 2012) health and cognitive ability (Wikby, Ek, & Christensson, 2009).
Foodwork and meals at home
There is no overall definition of nutrition, but it has usually been described from a biological perspective (Beauman et al., 2005), which can be distinguished, for instance, in the WHO’s (2013) definition: “Nutrition is the intake of food, considered in relation to the body’s dietary needs”. However, this perspective has been questioned (Beauman et al., 2005), which might be related to the fact that using a biomedical perspective in health care has been found to be insufficient. Instead, it is important to understand an individual within his/her surrounding context, i.e. have a bio-psycho-social perspective on the person (Engel, 1977). In studying meals the social and cultural aspects are included, i.e. how older persons choose, prepare, serve and eat food (Amella & Aselage, 2011). The definition of meal is complex, and in English it means both what is eaten and the event of eating (Meiselman, 2008). Oltersdorf, Schlettwein-Gsell and Winkler (1999), based on other researchers’ definitions, have described criteria for what comprises a meal, stating that meals can be defined based on the time of the day of the intake, the amount and combination of food, and whether or not there is social interaction between people. Sobal (2000) stresses that the meal is as much a social activity as it is a situation for easing hunger and thirst. Further, Fjellström (2004) and Mäkälä (2000) write that meals are social acts and something we share together with others and, depending on habits and values in a certain society or group, that people have notions of what constitutes a proper meal. The food included in the meal has been found to describe a person’s class, ethnic group or lifestyle affiliation, as well as other

17
social positions she/he holds, and is associated with one’s family and home (Anderson, 2005). Meals are preceded by planning and shopping as well as the preparation of food, which can be performed by the eater him/herself or by others; such activities have been described as foodwork (Bove & Sobal, 2006), and this term will be used in this thesis to describe such activities.
Traditions, routines and roles
Foodwork has traditionally been associated with a female role (DeVault, 1991), and women usually have the main responsibility for preparing food; this is especially true for older women (Gustafsson, Andersson, Andersson, Fjellström, & Sidenvall, 2003). According to a British study (Caraher, Dixon, Lang, & Carr-Hill, 1999), men tend to learn how to cook later in life and learn this from their partner more often compared to females, whilst women usually learn it at younger ages from their mothers. Similar results have been found in some Swedish studies, in which it has been found that women felt comfortable in these activities and that foodwork was not something they had to think about, but rather something they had always done and, therefore, were able to perform (Gustafsson et al., 2003; Sidenvall, Nydahl, & Fjellström, 2001). However, older women have described that they are anxious about becoming ill and losing their ability to carry out foodwork (Gustafsson et al., 2003). Further, divorced women and widows have expressed that their role and identity as a food provider ceased and resulted in feelings of loss (Sydner, Sidenvall, Fjellström, Raats, & Lumbers, 2007). In interviews with older men who had previously lived in a partnership, the opposite was revealed: this was often a new responsibility (Kullberg, Björklund, Sidenvall, & Åberg, 2010), and was difficult to perform due to lack of knowledge. Changes in roles in a couple could arise as the older woman became ill or frail, and when the change was slow the wife helped and taught the husband as he successively took on these responsibilities. However, these could be changes of a more natural character, like a result of retirement, which meant that foodwork was carried out as teamwork, with the woman still having the main responsibility and the husband being a helper (Sydner et al., 2007).

18
Dependence and independence applied to the activities of foodwork and meals
A disease like dementia might lead to severities in performing activities and make help from others necessary, for example during foodwork and meals. Using the concepts of dependence and independence regarding meals has recently been described by Fjellström and Mattsson Sydner (2013). The authors problematized the degree to which autonomy and independence should be promoted, since for persons who to some extent lack insight concerning their need of support it is a dilemma to preserve their independence and simultaneously make sure they attain a healthy food intake (Fjellström & Mattsson Sydner, 2013).
Both dependence and independence have previously been used and discussed together with ageing, which might be a result of ageing itself involving various kinds of dependence, like becoming financially dependent after retirement and the increased risk of becoming dependent on others as a result of disability and morbidity (Gibson, 1998). Dependence is usually described as negative and as something to be prevented, as well as a shameless and stigmatic concept, whilst both independence and autonomy are described as the opposite (Fine & Glendinning, 2005; Munnichs, 1976).
Dependence has been defined from a biomedical view, meaning that it has to do with the person’s ability to perform daily activities (Wilkin, 1987). However, it has also been emphasized that the concept includes a social dimension, meaning that relationships between people are important (van den Heuvel, 1976). Further, dependence can be understood as something that brings people together as humans (Sennett, 2004), which offers a more positive view of the concept. Still, dependence has previously been described as being related to ageism. This might be related to dependence usually being described together with not only old age but also childhood, which might be understood as an assertion that older persons should be treated the same way as children, since within both age groups people are recognized as being dependent on others. Further, the population of old persons, as well as their dependence, is rising and will likely continue increasing in the future, which also reinforces ageism (Bond & Cabrero, 2007).

19
Independence, on the other hand, means that one does not depend on anyone else; i.e., the concept actually excludes social relationships. One might argue that it is not possible to be totally independent of others. There is a third concept – interdependence – which emphasizes that there is a social world in which people meet and relationships are created, and that in some ways we are all dependent on each other (Munnichs, 1976). However, in a health care context independence is commonly used and described in a way that includes social relations in the concept (Bonikowski, Musto, Suteu, MacKenzie, & Dennis, 2012; Tamaru, McColl, & Yamasaki, 2007), which is in accordance with how the concept of independence is understood in this thesis.
In interview studies with older persons regarding foodwork and meals, independence and dependence seemed to be related to the ability to perform such activities. Moreover, independence seems to be highly valued and older women have expressed the importance of being independent from others and preserving meals and foodwork (Andersson & Sidenvall, 2001; Gustafsson et al., 2003; Kullberg et al., 2010; Sidenvall et al., 2001). The ability to cook has been described as being associated with the ability to live on one’s own (Porter, 2007). As independence is of great importance, if function decreases and cooking becomes difficult it can result in deficient meals (Gustafsson, 2002).
Nutritional problems among home-living older persons
Malnutrition occurs when food and nutrient intake do not meet an individual’s nutrient requirements (Skipper, 2012). With such a definition, a person might have an intake that is either lower or higher than the requirements. However, when it comes to older people the concepts of malnutrition and undernutrition are usually used interchangeably (Hickson, 2006). In a concept analysis among older people, malnutrition was found to mean “faulty or inadequate nutritional status; undernourishment characterized by insufficient dietary intake, poor appetite, muscle wasting and weigh loss” (Chen, Schilling, & Lyder, 2001, p. 139). In the clinical setting, a person with at least two of the following characteristics is considered to be undernourished: insufficient food intake; loss of weight, muscle or fat mass; fluid accumulation; or decreased hand grip strength

20
(Skipper, 2012). Approximately 2% of older persons living at home are malnourished, and 24% are at risk of malnutrition (Guigoz, 2006). The consequences of malnutrition are poorer physical capacity (Ödlund Olin, Koochek, Ljungqvist, & Cederholm, 2005), decreased subjective health (Keller, Østbye, & Goy, 2004), increased risk of illness, and mortality (Akner & Cederholm, 2001).
Several factors, which can be of a physical, social or psychological nature, have an impact on older persons’ nutritional status. Older persons tend to contract illnesses more often than others do, and disabilities and decreased physical activity can lead to reduced food intake (Hickson, 2006) as it can affect the ability to cook and eat food (Pirlich & Lochs, 2001). As a consequence of illness, prescribed drugs are used, and these drugs often have side effects such as dry mouth and loss of appetite (Alibhai, Greenwood, & Payette, 2005). Further, older people often do not meet fluid intake requirements, even though fluid is one of the most important components in maintaining good nutritional status (Elsner, 2002). All these factors can be considered to be of a physical nature. Factors of a social nature can be related to, for instance, living arrangements. Living alone and receiving help seems to affect nutritional status negatively (Söderhamn, Christensson, Idvall, Johansson, & Bachrach‐Lindström, 2012), which can be a result of decreased enjoyment in arranging the meal (Gustafsson & Sidenvall, 2002). Factors of a psychological nature include depression (Söderhamn et al., 2012) loneliness and stress which can lead to malnutrition (Hickson, 2006). Further, decreased cognitive ability is associated with malnutrition (Fagerström, Palmquist, Carlsson, & Hellström, 2011; HaeKwan, Kim, ByoungHoon, & ChanHyong, 2009).
Foodwork and meals when living with dementia
Being a person with dementia and its effect on foodwork and meals
Eating difficulties are common among persons with dementia (Manthorpe & Watson, 2003). Even persons in a mild stage of dementia seem to lose weight, which appears to be related to poor food intake (Holm &
21
Söderhamn, 2003). In a study including home-living persons with dementia it was found that almost 50% of the participants were malnourished or at risk of malnutrition (Roqué, Salva, & Vellas, 2013).
There are several factors that contribute to malnutrition in people with dementia. Most research aiming to describe problems regarding meals have been carried out in hospitals and special housing, and research among home-living persons with dementia is called for. Lack of appetite, a lost ability to recognize food, and eating things that are not appropriate or in small sizes are some of the problems that can occur when one suffers from dementia, which might lead to malnutrition (Aselage & Amella, 2010). Keller et al. (2008) have found that some of the problems described concerning eating in special housing or hospitals are also experienced by people living in ordinary homes. But, there are also other problems that might arise when a person lives in his/her own household, including challenges in buying and cooking food (Keller, Edward, & Cook, 2007; Keller et al., 2008). A recent study revealed that critical incidents regarding grocery shopping took place in the home of the person with Alzheimer’s disease, on the way to and from the grocery shop, as well as in the grocery shop. To manage the situation, participants used several strategies like double-checking, planning ahead or avoiding certain situations (Brorsson, Öhman, Cutchin, & Nygård, 2013).
Changes in foodwork and meals experienced by partners
Sharing meals has been referred to as a social activity, something enjoyable and a highlight of the day in interviews with family members of persons with dementia. However, changes and difficulties can arise, and it has previously been described that family members experience frustration, stress and conflict as a result of these changes (Keller et al., 2007). A few studies have focused on how foodwork and meals change, and as a result of this it has also been revealed that roles and routines in the families are affected. One study showed that female caregivers experienced a transition from working as a team to instead having the main responsibility and doing things alone; i.e., they had extended their current role as food provider. Male caregivers, however, described that as a result of their partner’s disease they had been forced to take over the responsibility and that it had become a challenge to perform these activities (Fjellström et al., 2010). Another study described

22
that when adjusting to living with a person with dementia men shifted from a passive role to an active one as food provider, whilst their female partners with dementia instead became increasingly passive as a result of a decreased capacity to manage activities. At the beginning of the process, the wife with dementia was the expert and the husband needed her knowledge to carry out foodwork and meals, but this shifted over time (Atta-Konadu, Keller, & Daly, 2011). Male caregivers have also stressed that when taking over this responsibility they learned that preparing meals is much more than just cooking, and that it was harder than their female partner had made it seem (Russell, 2001). Even though it might be a struggle to manage these new responsibilities, male spouses have expressed pride in achieving foodwork while caring for their partner (Sanders & Power, 2009).
The Life Nourishment Theory
Recently, the Life Nourishment Theory (LNT) was developed based on longitudinal studies including interviews with families in Canada living with dementia. According to this theory, meals are mirrors that reflect who we are, and studying meal situations may be one way to capture families’ experiences of overall daily life when a family member is suffering from dementia. There are three interrelated concepts that further explain the theory: being connected, honouring identity, and adapting to an evolving life (Genoe et al., 2012; Genoe et al., 2010; Keller et at., 2010). Being connected includes how relationships can be preserved, and help families stay united and interact both within the family as well as with others. Different parts promote the connection: being face to face, which means that people physically create meals together; participating psychologically, i.e. cognitive and emotional engagement; and getting and giving support, which could be of both a physical nature (for example helping with foodwork) and a psychological nature (like discussing problems and finding solutions) (Keller et al., 2010). Honouring identity means that both the individual and family identities are honoured by preserving dignity and autonomy, and by helping persons feel they are important. This process includes protecting dignity while struggling for autonomy, which has to do with having respect for oneself and for others, as well as being accepted for who you are. Having meaningful roles of importance for the person contributes to maintaining his/her identity. Reaffirming a sense of self in the world can be about, for

23
instance, preserving routines and traditions (Genoe et al., 2010). Adapting to an evolving life refers to the process of being aware of changes during meals and foodwork, and adjusting and adapting to these changes as the dementia continues to progress (Genoe et al., 2012).
Support in foodwork and meals
Aselage and Amella (2010) argue that there is a lack of research when it comes to supporting home-living persons with dementia regarding meals and preserving or improving nutritional status in the home environment. This can be one explanation for why nutritional guidelines are seldom used (Persenius, Hall-Lord, Bååth, & Larsson, 2008), as well as why nutritional interventions were only used in about 20% of the cases in a Dutch study among malnourished older persons receiving home-help (Meijers, Halfens, van Bokhorst-de van der Schueren, Dassen, & Schols, 2009). In a review of interventions to prevent malnutrition in people with dementia, those living in their ordinary homes were excluded, which was motivated with the explanation that these people have different problems that require other interventions compared to those in special housing or hospitals (Jackson, Currie, Graham, & Robb, 2011). However, one might argue that some of the interventions emphasized in the review can also be applicable to home-living persons, like educating caregivers, adjusting the environment and giving individual support. In the national guidelines for care in cases of dementia, which target persons in both ordinary and special housing, individualized care using several interventions is highlighted (National Board of Health and Welfare, 2010).
A study including both a literature review and focus groups interviews revealed that environmental modifications might be needed for home-living persons with dementia. Such interventions, which could help them participate in foodwork as much as possible with minimum risk, include installing timers, providing a place in the kitchen where they can sit and carry out foodwork, and making things visible so it is clear what and where they are (van Hoof, Kort, van Waarde, & Blom, 2010). For persons who are not able to prepare meals independently, food distribution (e.g. meals-on-wheels) can be used. However, a recent Swedish qualitative study among professionals involved in such a service revealed that it was found to be a

24
deficient intervention as the staff did not know what actually happened after they delivered the food; it would have been preferable to stay while the person ate (Pajalic, Persson, Westergren, & Skovdahl, 2012).

25
Rationale for the thesis
Previous research has shown that older persons highly value independence and living in their own household, which is in agreement with national policies. This can be jeopardized, however, if a person has insufficient nutritional intake. Nutrition should be understood from more than just a biomedical perspective; meals can be studied with a focus on social and cultural aspects of the phenomenon. However, there is a lack of knowledge regarding meals for home-living persons, not least among those with dementia. To be able to identify problems and develop evidence-based interventions for this group, whereby the person’s own problems and wishes serve as the basis when planning for care and meals, it is essential to explore the experiences of both the person with dementia and his/her partner as well as staff.

26
Aim of the thesis
The aim of this thesis was to explore and describe foodwork and meals for older persons with dementia and their partners in ordinary homes. The research questions were:
How is nutritional status affected by cognitive impairment among home-living older men and women? (Paper I)
Which changes occur in couples regarding foodwork and meals? (Papers II and III)
Which functions are important to uphold regarding foodwork and meals? (Papers II, III and IV)
How can foodwork and meals be adjusted to the cognitive changes? (Papers II, III and IV)

27
Method
Design
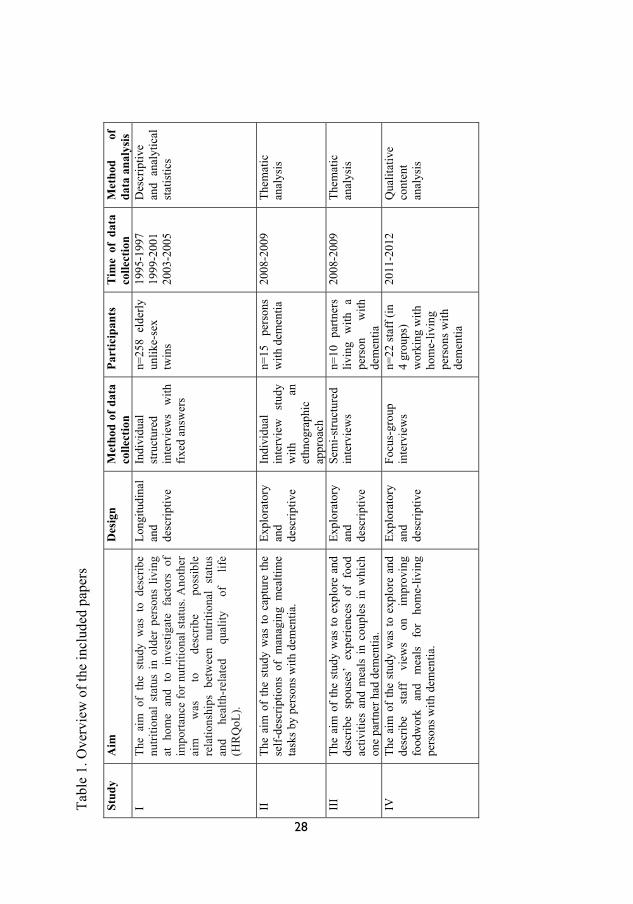
Several designs were used when performing the four studies on which the thesis is based. An overview of the studies is found in Table 1. The results from the longitudinal descriptive study among home-living unlike-sex twins (Paper I) showed the need for further research on foodwork and meals for persons with dementia living at home. Since little is known (Aselage & Amella, 2010), qualitative methods were chosen to highlight this phenomenon (Polit & Beck, 2012). Thereafter, two studies focusing on the experiences of living with dementia were conducted (Papers II and III). In the study including persons with dementia (Paper II) an ethnographic approach was used which, according to Wolcott (2008), entails studying customary social behaviours to learn about the culture in a specific group of people. Further, this method can be used to describe people’s actions in everyday life (Hammersley & Atkinson, 1995). Therefore, in ethnographic studies data need to be collected in the natural setting, which makes it possible to study certain aspects of people’s daily life. Fieldwork is highly valued, and preferred data collection includes observations and interviews (Wolcott, 2008). In Paper II the results are based mainly on interviews but also include observations. The explorative and descriptive studies including persons with dementia (Paper II) and their partners (Paper III) revealed several challenges as well as a need for support to manage the complex situations they were facing. Since little is known about this, another qualitative study (focus group interviews) was conducted with staff (Paper IV) to describe and explore their views on how meals can be improved. Data collected in the interviews (Papers II and III), together with observations from the home visits, were used to create vignettes. These vignettes were further used as a basis for the discussions during the focus group interviews with staff (Paper IV).
Tabl
e 1.
Ove
rvie
w o
f the
incl
uded
pap
ers
28
Stud
y A
im
Des
ign
Met
hod
of d
ata
colle
ctio
n Pa
rtic
ipan
ts
Tim
e of
dat
a co
llect
ion
Met
hod
of
data
ana
lysi
s I
The
aim
of
the
stud
y w
as t
o de
scrib
e nu
tritio
nal
stat
us i
n ol
der
pers
ons
livin
g at
hom
e an
d to
inv
estig
ate
fact
ors
of
impo
rtanc
e fo
r nut
ritio
nal s
tatu
s. A
noth
er
aim
w
as
to
desc
ribe
poss
ible
re
latio
nshi
ps b
etw
een
nutri
tiona
l st
atus
an
d he
alth
-rel
ated
qu
ality
of
lif
e (H
RQ
oL).
Long
itudi
nal
and
desc
riptiv
e
Indi
vidu
al
stru
ctur
ed
inte
rvie
ws
with
fix
ed a
nsw
ers
n=25
8 el
derly
un
like-
sex
twin
s
1995
-199
7 19
99-2
001
2003
-200
5
Des
crip
tive
and
anal
ytic
al
stat
istic
s
II
The
aim
of
the
stud
y w
as to
cap
ture
the
self-
desc
riptio
ns o
f m
anag
ing
mea
ltim
e ta
sks b
y pe
rson
s with
dem
entia
.
Expl
orat
ory
and
desc
riptiv
e
Indi
vidu
al
inte
rvie
w
stud
y w
ith
an
ethn
ogra
phic
ap
proa
ch
n=15
pe
rson
s w
ith d
emen
tia
2008
-200
9 Th
emat
ic
anal
ysis
III
The
aim
of
the
stud
y w
as to
exp
lore
and
de
scrib
e sp
ouse
s’ e
xper
ienc
es o
f fo
od
activ
ities
and
mea
ls in
cou
ples
in w
hich
on
e pa
rtner
had
dem
entia
.
Expl
orat
ory
and
desc
riptiv
e
Sem
i-stru
ctur
ed
inte
rvie
ws
n=10
par
tner
s liv
ing
with
a
pers
on
with
de
men
tia
2008
-200
9 Th
emat
ic
anal
ysis
IV
The
aim
of
the
stud
y w
as to
exp
lore
and
de
scrib
e st
aff
view
s on
im
prov
ing
food
wor
k an
d m
eals
fo
r ho
me-
livin
g pe
rson
s with
dem
entia
.
Expl
orat
ory
and
desc
riptiv
e
Focu
s-gr
oup
inte
rvie
ws
n=22
staf
f (in
4
grou
ps)
wor
king
with
ho
me-
livin
g pe
rson
s with
de
men
tia
2011
-201
2 Q
ualit
ativ
e co
nten
t an
alys
is

29
Participants and setting
In Paper I the sample consisted of unlike-sex twins from the Swedish Twin Register, and more specifically from the national project “Aging in women and men: a longitudinal study of gender differences in health behaviour and health among elderly”. Inclusion criteria have previously been described in detail (Gold, Malmberg, McClearn, Pedersen, & Berg, 2002). A total of 249 twin pairs, or 498 persons, were interviewed at home by experienced research nurses during the period 1995-1997, i.e. Occasion 1 (OC1). This was a structured interview including sociodemographic background data, cognitive testing, health examination, drug registration and blood sampling. Two repeated interviews were carried out during 1999-2001 (Occasion 2 [OC2]) and 2003-2005 (Occasion 3 [OC3]). At OC3, an assessment of nutritional status (Mini Nutritional Assessment [MNA]) was conducted on 258 persons, and the sample in this study consists of these persons, who all still lived in their ordinary homes. Of these 258 persons, 128 were men and 130 women, and ultimately a total of 65 twin pairs had stayed intact (Figure 1).
A comparison of those at OC3 who participated (n=258) in Paper I and those who did not (n=48) showed that those who were excluded had significantly lower Mini-Mental State Examination (MMSE) scores (p<0.001) and Activity of Daily Living (ADL) functioning (p<0.001). No significant differences were found regarding sex or age.

30
Figure 1. Flowchart of participants in Paper I.
OC1 (Occasion 1) 1995-1997 n=498 persons (249 twin pairs) Aged: 71-80
58 persons died. 60 dropped out: illness, frailty, unwillingness to participate.
OC3 2003-2005 n=306 persons
OC2 1999-2001 n=380 persons
Participants in Paper I n=258 Aged: 79-88
62 persons died. 12 dropped out: illness, frailty, unwillingness to participate.
47 persons did not complete MNA. One person lived in special housing.

31
All data for Papers II, III and IV were collected in the same municipality in southern Sweden, with approximately 130,000 residents. All individuals received written and oral information about the interview study they were asked to participate in (Papers II, III and IV).
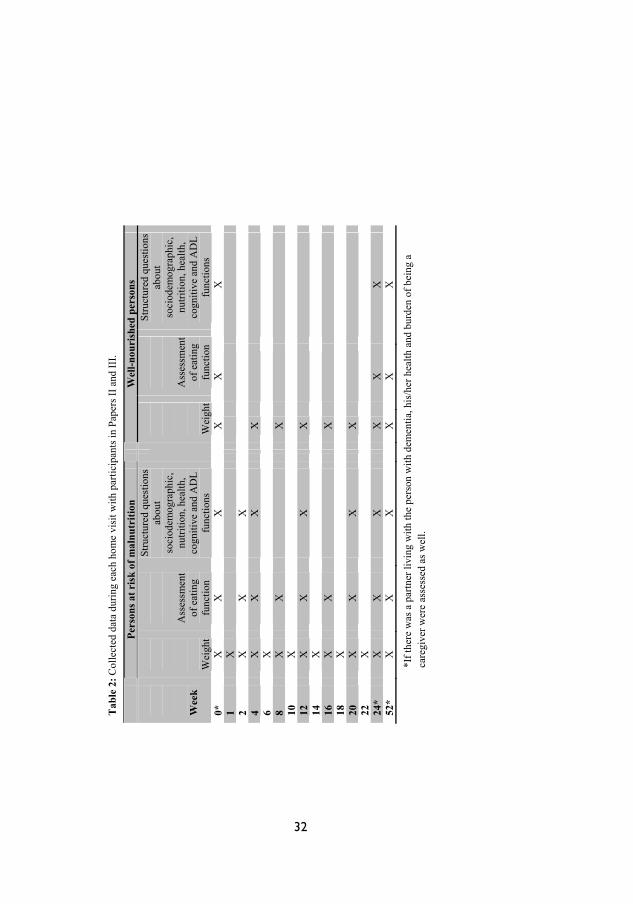
Participants in Papers II and III participated in a project called Food, Exercise and Memory Loss. The main aim of the project was to examine whether or not individual exercise and food interventions could improve health-related quality of life. Both qualitative and quantitative data were collected during the years 2008–2009 among home-living persons with dementia and their partners. Persons diagnosed with dementia by a physician 6–12 months prior to the time of data collection were asked to participate in the project by a public health nurse or similar, specialized in persons with dementia. If the person wanted to participate the primary nurse passed on contact information to the researcher, who contacted the person and gave him/her further information about the study. At least eight visits were conducted in each home, where the researcher and the person discussed food and meals. However, this depended on the person’s nutritional status, and in some cases 15 home visits were performed (Table 2). Notes were made after each visit, based on what was discussed and observed. A total of 35 persons with dementia were included in the project.
Fifteen persons with dementia were asked to participate in an interview study with an ethnographic approach (Paper II), since they were considered to be able to communicate verbally to an adequate extent. They all agreed to participate. All partners (11 persons) participating in the project were asked to participate in a separate interview study, and all but one gave consent (Paper III). Participants’ characteristics are presented in Tables 3 and 4, and the relationship between participants in Papers II and III are presented in Table 5.
32
Tab
le 2
: Col
lect
ed d
ata
durin
g ea
ch h
ome
visi
t with
par
ticip
ants
in P
aper
s II a
nd II
I.
*If t
here
was
a p
artn
er li
ving
with
the
pers
on w
ith d
emen
tia, h
is/h
er h
ealth
and
bur
den
of b
eing
a
care
give
r wer
e as
sess
ed a
s wel
l.
Pe
rson
s at r
isk
of m
alnu
triti
on
W
ell-n
ouri
shed
per
sons
W
eek
W
eigh
t
A
sses
smen
t of
eat
ing
func
tion
Stru
ctur
ed q
uest
ions
ab
out
soci
odem
ogra
phic
, nu
tritio
n, h
ealth
, co
gniti
ve a
nd A
DL
func
tions
Wei
ght
A
sses
smen
t of
eat
ing
func
tion
Stru
ctur
ed q
uest
ions
ab
out
soci
odem
ogra
phic
, nu
tritio
n, h
ealth
, co
gniti
ve a
nd A
DL
func
tions
0*
X
X
X
X
X
X
1 X
2
X
X
X
4 X
X
X
X
6 X
8
X
X
X
10
X
12
X
X
X
X
14
X
16
X
X
X
18
X
20
X
X
X
X
22
X
24*
X
X
X
X
X
X
52
* X
X
X
X
X
X

Tab
le 3
: Per
sons
with
dem
entia
cha
ract
eris
tics b
ased
on
quan
titat
ive
and
qual
itativ
e da
taA
ge
Gen
der
Liv
ing
stat
us
MN
A
MM
SE
Food
wor
k 82
Fe
mal
e Li
ves a
lone
in fl
at.
24.5
25
B
uys g
roce
ries h
erse
lf. R
ecei
ves m
eals
-on-
whe
els f
rom
the
hom
e-he
lp se
rvic
e.
84
Fem
ale
Live
s with
par
tner
in c
o-op
erat
ive
flat.
25
.5
22
Buy
s gro
cerie
s and
coo
ks h
ome-
mad
e fo
od to
geth
er w
ith
her p
artn
er.
77
Mal
e Li
ves a
lone
in h
ouse
. 24
.0
26
Buy
s gro
cerie
s and
war
ms u
p pa
rtly
or re
ady-
cook
ed m
eals
hi
mse
lf.
71
Mal
e Li
ves w
ith p
artn
er in
flat
. 22
.0
30
Buy
s gro
cerie
s tog
ethe
r with
par
tner
. Par
tner
coo
ks h
ome-
mad
e fo
od.
69
Mal
e Li
ves w
ith p
artn
er in
hou
se.
24.0
16
Pa
rtner
buy
s gro
cerie
s and
coo
ks h
ome-
mad
e fo
od.
78
Fem
ale
Live
s alo
ne in
co-
oper
ativ
e fla
t. 21
.0
29
Buy
s gro
cerie
s her
self.
Rec
eive
s mea
ls-o
n-w
heel
s fro
m th
e ho
me-
help
serv
ice.
86
Fe
mal
e Li
ves a
lone
in c
o-op
erat
ive
flat.
23.0
21
B
uys g
roce
ries a
nd c
ooks
hom
e-m
ade
food
her
self.
77
M
ale
Live
s with
par
tner
in h
ouse
. 19
.0
21
Partn
er b
uys g
roce
ries a
nd c
ooks
hom
e-m
ade
food
. 80
Fe
mal
e Li
ves a
lone
in c
o-op
erat
ive
flat.
24.5
21
B
uys g
roce
ries h
erse
lf. R
ecei
ves m
eals
-on-
whe
els f
rom
the
hom
e-he
lp se
rvic
e.
79
Fem
ale
Live
s with
par
tner
in c
o-op
erat
ive
flat.
25.0
27
B
uys g
roce
ries a
nd c
ooks
hom
e-m
ade
food
her
self.
85
Fe
mal
e Li
ves a
lone
in fl
at.
24.0
22
B
uys g
roce
ries a
nd c
ooks
hom
e-m
ade
food
her
self.
80
Fe
mal
e Li
ves a
lone
in fl
at.
27.5
23
B
uys g
roce
ries a
nd c
ooks
hom
e-m
ade
food
her
self.
77
M
ale
Live
s alo
ne in
hou
se.
26.0
28
R
ecei
ves g
roce
ries a
nd m
eals
-on-
whe
els f
rom
the
hom
e-he
lp se
rvic
e.
85
Fem
ale
Live
s alo
ne in
hou
se.
24.0
29
B
uys g
roce
ries t
oget
her w
ith so
n. R
ecei
ves m
eals
-on-
whe
els f
rom
the
hom
e-he
lp se
rvic
e.
79
Fem
ale
Live
s with
par
tner
in fl
at.
26.0
25
B
uys g
roce
ries t
oget
her w
ith p
artn
er, c
ooks
hom
e-m
ade
food
her
self.
33

34
Tab
le 4
: Par
tner
s’ c
hara
cter
istic
s bas
ed o
n qu
antit
ativ
e an
d qu
alita
tive
data
Age
G
ende
r L
ivin
g st
atus
Fo
odw
ork
70
Fem
ale
Mar
ried
and
lives
with
hu
sban
d in
hou
se.
Res
pons
ible
for c
ooki
ng e
ven
befo
re p
artn
er w
as d
iagn
osed
with
dem
entia
. Now
coo
ks
hom
e-m
ade
food
and
buy
s gro
cerie
s her
self.
80
Fe
mal
e M
arrie
d an
d liv
es w
ith
husb
and
in fl
at.
Res
pons
ible
for c
ooki
ng e
ven
befo
re p
artn
er w
as d
iagn
osed
with
dem
entia
. Now
coo
ks
hom
e-m
ade
food
alo
ne, a
nd b
uys g
roce
ries t
oget
her w
ith h
er p
artn
er.
83
Fem
ale
Mar
ried
and
lives
with
hu
sban
d in
flat
. R
espo
nsib
le fo
r coo
king
eve
n be
fore
par
tner
was
dia
gnos
ed w
ith d
emen
tia. N
ow c
ooks
ho
me-
mad
e fo
od a
nd b
uys g
roce
ries h
erse
lf.
79
Fem
ale
Mar
ried
and
lives
with
hu
sban
d in
flat
. R
espo
nsib
le fo
r coo
king
eve
n be
fore
par
tner
was
dia
gnos
ed w
ith d
emen
tia. N
ow c
ooks
ho
me-
mad
e fo
od a
lone
, and
buy
s gro
cerie
s tog
ethe
r with
her
par
tner
. 73
Fe
mal
e M
arrie
d an
d liv
es w
ith
husb
and
in h
ouse
. R
espo
nsib
le fo
r coo
king
eve
n be
fore
par
tner
was
dia
gnos
ed w
ith d
emen
tia. N
ow c
ooks
ho
me-
mad
e fo
od a
nd b
uys g
roce
ries h
erse
lf.
76
Fem
ale
Mar
ried
and
lives
with
hu
sban
d in
hou
se.
Res
pons
ible
for c
ooki
ng e
ven
befo
re p
artn
er w
as d
iagn
osed
with
dem
entia
. Now
coo
ks
hom
e-m
ade
food
and
buy
s gro
cerie
s her
self.
78
M
ale
Mar
ried
and
lives
with
w
ife in
hou
se.
Res
pons
ible
for c
ooki
ng e
ven
befo
re p
artn
er w
as d
iagn
osed
with
dem
entia
1 . Now
co
oks h
ome-
mad
e fo
od a
lone
, and
buy
s gro
cerie
s tog
ethe
r with
his
par
tner
. 86
M
ale
Mar
ried
and
lives
with
w
ife in
terr
ace
hous
e.
Partn
er u
sed
to b
e re
spon
sibl
e fo
r coo
king
bef
ore
bein
g di
agno
sed
with
dem
entia
1 . N
ow c
ooks
hom
e-m
ade
food
and
buy
s gro
cerie
s tog
ethe
r with
par
tner
. 86
M
ale
Mar
ried
and
lives
with
w
ife in
terr
ace
hous
e.
Partn
er u
sed
to b
e re
spon
sibl
e fo
r coo
king
bef
ore
diag
nose
d w
ith d
emen
tia. N
ow
rece
ives
mea
ls-o
n-w
heel
s fro
m th
e ho
me-
help
serv
ice
and
buys
gro
cerie
s him
self.
63
M
ale
Live
s with
par
tner
in
co-o
pera
tive
flat.
Res
pons
ible
for c
ooki
ng e
ven
befo
re p
artn
er w
as d
iagn
osed
with
dem
entia
. Now
coo
ks
hom
e-m
ade
food
alo
ne, a
nd b
uys g
roce
ries t
oget
her w
ith h
is p
artn
er.
1 In th
ese
case
s the
par
ticip
ants
had
take
n ov
er th
e m
ain
resp
onsi
bilit
y la
ter i
n lif
e, e
.g. a
fter r
etire
men
t.
35
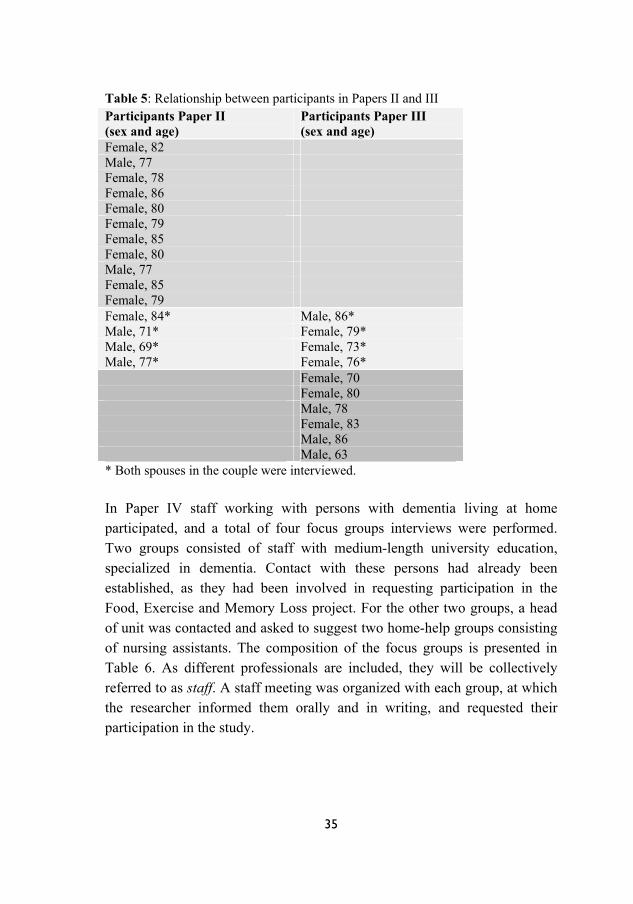
Table 5: Relationship between participants in Papers II and III Participants Paper II (sex and age)
Participants Paper III (sex and age)
Female, 82 Male, 77 Female, 78 Female, 86 Female, 80 Female, 79 Female, 85 Female, 80 Male, 77 Female, 85 Female, 79 Female, 84* Male, 86* Male, 71* Female, 79* Male, 69* Female, 73* Male, 77* Female, 76* Female, 70 Female, 80 Male, 78 Female, 83 Male, 86 Male, 63 * Both spouses in the couple were interviewed. In Paper IV staff working with persons with dementia living at home participated, and a total of four focus groups interviews were performed. Two groups consisted of staff with medium-length university education, specialized in dementia. Contact with these persons had already been established, as they had been involved in requesting participation in the Food, Exercise and Memory Loss project. For the other two groups, a head of unit was contacted and asked to suggest two home-help groups consisting of nursing assistants. The composition of the focus groups is presented in Table 6. As different professionals are included, they will be collectively referred to as staff. A staff meeting was organized with each group, at which the researcher informed them orally and in writing, and requested their participation in the study.

36
Table 6: Background data on participants in Paper IV
Data collection
Quantitative data
In Paper I instruments measuring nutritional status and cognitive function, as well as questions that may have an impact on nutritional status, were used.
Instruments
The full Mini Nutritional Assessment (MNA) (Guigoz, Vellas, & Garry, 1994/1995) is the most commonly used tool in screening for nutritional status among older persons, and is also considered to be the most appropriate (Secher, Soto, Villars, van Kan, & Vellas, 2007). The MNA was developed to assess the nutritional status of frail older persons and consists of 18 items (anthropometric measurements, general assessment, dietary assessment, subjective assessment), with a maximum total score of 30. A score of less than 17 indicates that a person is malnourished, between 17 and 23.5 that the person is at risk of malnutrition, and above 23.5 that the person is well-nourished (Vellas et al., 1999).
Focus group Age (range)
Education Working years in elderly care (range)
Dementia team 1 (6 persons)
39-60 University degree: nurse (2), social worker (2), occupational therapist (2)
15-30
Dementia team 2 (5 persons)
40-62 University degree: specialist nurse with focus on public health nursing (5)
14-45
Nursing assistants 1 (6 persons)
21-62 Less than upper secondary school (2), upper secondary school (4)
1-24
Nursing assistants 2 (5 persons)
25-52 Upper secondary school (5) 7-29

37
The Mini-Mental State Examination (MMSE) was used to screen for cognitive function (Folstein, Folstein, & McHugh, 1975). The MMSE is commonly used both clinically and in research studies during diagnosis and screening (Tombaugh & McIntyre, 1992). Scores range between 0 and 30 (Folstein et al., 1975); how they should be interpreted is not definite, but Jönsson and Wimo (2009) suggest that 20 points or more be considered mild dementia, 10-19 moderate, and less than 10 severe.
Supplementary variables
The longitudinal study (Paper I) included questions on aspects that might have an impact on the nutritional status (Appendix A). In the thesis, two questions about health were dichotomized and used during the statistical analysis. A question about cognitive function was used in a similar way, hereafter referred to as memoryDL.
Qualitative data
Individual interviews
In Papers II and III, individual semi-structure interviews (Polit & Beck, 2012) were performed at the participants’ homes during 2008-09. This meant that interview guides (Appendix B) covering different aspects of meals and foodwork were used, inspired by previous studies about meals (e.g. Andersson & Sidenvall, 2001; Sidenvall et al., 2001) and by one of the researchers’ (B. Sidenvall) knowledge in this research area. Although an interview guide was used when interviewing the persons with dementia (Paper II), these interviews can best be described as conversations in which the researcher adjusted to the person. The interviews were performed at the third home visit or later, when the researcher and participants had established a relationship. The author conducted all interviews in the participants’ homes. In Paper II, one person with dementia was interviewed at an occasion when the partner was not at home. In the interviews with partners (Paper III), two informants chose to be interviewed when their spouses were away from home. In all other cases, if there was a partner, he/she was at home but in a different room from where the interviews were performed. Field notes were made by the author after all interviews, including both observations and thoughts. Detailed observations were made

38
of the present setting and the participants’ behaviours during the interviews with the persons with dementia (Paper II). Each participant was interviewed once, and each interview lasted 15 to 60 minutes (Paper II) and 13 to 45 minutes (Paper III).
Focus group interviews
During 2011-2012 focus group interviews were performed with staff, during which the participants read and discussed two vignettes. These vignettes were based on data from Papers II and III (Appendix A, Paper IV). Before being used in the focus groups, these vignettes were discussed with a public health nurse and a nursing assistant to ensure that the situations felt authentic, and it was determined that they did. The focus groups interviews started with everyone introducing themselves, and then the first vignette was distributed to the participants. All interviews were led by a moderator (me) and an assistant, as described by Krueger and Casey (2009). The moderator was responsible for the interviews, ensuring that everyone was involved in the interviews, and asking follow-up questions like “What do you mean by…” or, “Can you please tell us more about…”. The assistant was responsible for practical tasks, taking notes during the interviews, and summarizing each vignette at the end of the discussion. Each focus group lasted about an hour. All interviews (Papers II, III and IV) were recorded and transcribed verbatim.
Data analyses
Quantitate data
In Paper I parametric tests (Student’s t-test) were used for Body Mass Index (BMI) and MMSE, and non-parametric tests (Chi-2 tests) were used for all other variables. In the thesis, MMSE was instead analysed using non-parametric tests. In the logistic regression analysis (uni- and multivariate), the nutritional status was used as the dependent variable. Persons at risk of malnutrition or who were malnourished (PAR) were combined during the analysis and compared with those who were well-nourished (WN). Variables consisting of more than two possible responses were dichotomized. In the
39
logistic regression analyses, MMSE was dichotomized using the commonly used cutoff point of 23/24 (Aevarsson & Skoog, 2000; Grut, Fratiglioni, Viitanen, & Winblad, 1993). Tests for dependent variables were used to analyse differences over time (ANOVA [Paper I], Friedman’s test, Cochran´s Q test). Data have been analysed as both independent and dependent groups as the participants are unlike-sex twins, but since the results are similar the independent variables are presented. SPSS 19.0 was used to perform the statistical analysis in the thesis. Significant levels were set at p<0.05.
Qualitative data
Qualitative data were analysed using thematic analysis (Papers II and III) and qualitative content analysis (Paper IV).
Thematic analysis
Thematic analysis seeks to find repeated patterns and meanings across a data set (Braun & Clarke, 2006). Spradley (1979) describes thematic analysis as a method in ethnography whereby the theme is associated with the culture, whilst Field and Morse (1995, p. 139) do not relate to the cultural aspect but instead describe it as a “search for and identification of common threads that extend throughout an entire interview or set of interviews”. This distinction is quite good for describing the two different thematic analyses performed here. In paper II, the analysis was performed in accordance with ethnographic thematic analysis described by Wolcott (1994). Meanwhile, the analysis in Paper III was based on Braun and Clarke’s (2006) step-by-step guide for inductive thematic analysis, which rather agrees with Field and Morse’s (1995) definition of thematic analysis.
Wolcott (1994) describes three categories for transforming collected data in an ethnographic study, which were used as a basis for the analysis of Paper II: description, analysis and interpretation. Description involves presenting what is going on in the setting and orienting the reader. In the analysis, data should be structured to allow for the identification of patterns and the presentation of facts. Interpretation is a way to understand and draw conclusions from the data. It is part of the analysis process, but it is important to discuss the extent to which interpretation has occurred

40
(Wolcott, 1994). In Paper II this way of transforming data was used as guidance during the analysis, which meant that notes from the observations were first written as vignettes to describe and increase the understanding of the settings and informants. The analysis started with reading the interviews several times and marking all text concerning foodwork and meals, as well as writing short summaries of all interviews. The summaries and the marked text from the first five interviews were used to find patterns and meanings and to create preliminary themes that agreed with the content of the data. These preliminary themes were then discussed with a co-author, and when agreement had been reached an analysis including all 15 interviews were performed whereby the themes were tested if they fit the whole data set. This was done by checking both whether the marked text in the remaining ten interviews fit the themes and whether the meaning of the whole data set seemed to be described in the themes. This meant that two of the authors in the paper discussed the themes continuously. Finally, three main themes with associated subthemes were created. To make sense of the findings, they were interpreted by referring to theories and previous research. Further, findings were critically reviewed and discussed with other researchers.
In Paper III the analysis began with writing summaries based on the interviews and field notes for each participant, which were then discussed with each participant during a second home visit. These were also recorded and transcribed and used in the analysis. In one case the second home visit was not carried out because of illness in the family, but data from the interview were included in the analysis. Braun and Clarke (2006) have identified six phases for a thematic analysis, but these should not be understood as a linear process; instead, there is a constant moving between them. The phases include the researcher becoming familiar with the data set (1), creating initial codes (2), searching for themes (3), reviewing themes (4), defining and labelling the themes (5) and finally writing the results (6) (Braun & Clarke, 2006). After all data were transcribed, the text was first read several times to get an overview of the content of the interviews. Data including spouses’ experience of foodwork and meals were labelled with a code. The codes were then sorted into potential subthemes, which were tested and reworked when necessary, and there was a constant moving between the data as a whole and the codes to search for patterns and

41
meanings. Finally, the analysis resulted in three subthemes describing how things used to be, what kind of changes had occurred, and how these changes were managed. During the analysis a metaphor used by one of the informants, ‘dancing on a slack tightrope’, was observed to capture a central feature of all interviews, and suited the content of the three subthemes. The metaphor made it possible not only to see how informants’ experiences fit together but also to highlight the diversities, and was therefore used to label the theme. The metaphor was found to consist of three components that further explained it and that suited the content of the three subthemes. Hence, these components were used to label the subthemes: Being on the platform, Being on the tightrope, and Using a balance pole. This metaphor was used when writing the report. It has previously been described that metaphors can be used in qualitative studies to structure data and give them meaning (Bonner & Greenwood, 2005; Carpenter, 2008; Sandelowski, 1998).
Content analysis
Content analysis can be described as a systematic technique used to find patterns in a text (Krippendorff, 2012). The description by Elo and Kyngäs (2008) of inductive content analysis was used during the analysis, which entails the selection of the unit of analysis, a massive reading of the text to make sense of the data, the performance of an open coding, the creation of categories through interpretation and an abstraction of the categories to the degree possible (Elo & Kyngäs, 2008). In Paper IV the analysis started with reading the transcribed interviews several times to get an overview of the data. The notes from the focus group interviews made by the assistant were also read through. The software program Atlas TI 6.2 was used for the coding and categorization process. Since the aim was to describe and explore staff views on improving foodwork and meals for home-living persons with dementia, all text about foodwork and meals was marked with a code; i.e. the open coding process was performed. During this process some codes were named slightly differently even though their content was similar; therefore, they were merged during the process. The final codes were then sorted depending on their content, and subcategories were created. Then, through abstraction, five categories were developed from these subcategories, and one main category was identified.

42
Ethical considerations
Regional Ethical Review Boards approved Papers I, II and III (dnr 95:53, 98:381, 03:124 Paper I, dnr M15-08 Papers II-III). The Declaration of Helsinki (World Medical Association [WMA], 2008) and the Ethical guidelines for nursing research in the Nordic countries (Northern Nurses’ Federation, 2003) were used as an ethical standpoint regarding confidentiality, information letter, informed consent and storage of collected data. When it comes to ethical considerations regarding Paper III, one must consider that the partners might have found it difficult not participating in the interview study since their spouse, the person with dementia, was already participating in the Food, Exercise and Memory Loss project. However, participation in the interview was voluntary, and the partners were asked separately about participation. Focus group interviews were performed with staff, who were informed about the study during a staff meeting, and additionally the interview was performed at the workplace, which might have affected their consent and participation (Paper IV). No formal approval was needed for Paper IV, but the Research Ethics Committee of the School of Health Sciences, Jönköping University, reviewed the study and raised no objections from an ethical point of view (7/2-12).
Several ethical issues arise when research includes persons with dementia (Paper II), and according to the WMA (2008) research on vulnerable groups should be avoided. On the other hand, the constant exclusion of people with dementia might lead not only to stigmatization in society as it signals that they lack the capacity to share their experiences (Wilkinson, 2001) but also to a stagnation in the development regarding nursing care for them (Northern Nurses’ Federation, 2003). A fundamental aspect of referring to persons with dementia as vulnerable is related to informed consent, as the disease might affect one’s ability to receive information and therefore also one’s ability to give informed consent (Slaughter, Cole, Jennings, & Reimer, 2007). However, the within-group differences are great, and it is therefore likely that people’s abilities also vary (Hellström, Nolan, Nordenfelt, & Lundh, 2007). It was experienced that the cognitive capacity differed between the participants. Among other things, this seemed to be related to whether the person lived alone or with a partner. For those living with a partner, both were always informed about the study, but the person with dementia was the

43
one who chose whether or not to participate. Single-living persons who remembered that the researcher was going to contact them and were also able to express the aim of the study were considered to be able to decide themselves whether or not to participate in the study. In some cases the researcher or primary nurse informed adult children about the study, after receiving consent from the person with dementia. The persons were able to live in their ordinary homes, and it was considered important to preserve their autonomy and prevent them from feeling offended. One example of such a situation was a woman who was informed and asked to participate by the public health nurse, and wanted to participate. The nurse asked if she could contact the woman’s adult child about the study, but the woman answered that she was capable of deciding such a thing herself. During each home visit the persons were informed and asked to participate, which has been described as important since a dementia can fluctuate from one occasion to the next (Hellström, Nolan, Nordenfelt et al., 2007). It should be clarified that significant others, and sometimes home-care staff and/or the public health nurse, were informed when a person was assessed as being at risk of malnutrition, but only after the person him/herself was informed of this.
Repeated visits have been described as important for a trustful relationship to be built between the participant and the researcher. As mentioned before, repeated visits were made to the person’s home and the interviews were carried out during the third visit at the earliest. However, even though the importance of building a relationship has been pointed out, there is a lack of research regarding ending a research project (Cowdell, 2006), which was found to be difficult. The number of home visits varied, but usually between eight and 15 visits were performed. This resulted in the emergence of relationship, making it possible to collect data. This relationship can be regarded as unequal, since the researcher had an agenda for the relationship and decided when to end it, but this of course affected the researcher’s feelings. Even more, it seemed to affect the participants, and some expressed sadness during the last home visit since this meant that the data collection was finished and that the home visits and relationship would now end.

44
Findings
Cognitive ability as an associated factor for malnutrition among home-living older men and women (I)
According to the MNA, 42 persons were assessed as being at risk of malnutrition and one as being malnourished. The median MNA score for persons at risk (PAR) of malnutrition was 22 [Q1 20.0 Q3 23.5], and 26.5 [Q1
25.0 Q3 27.5] for the well-nourished (WN).
Comparisons (OC3) between the persons at risk and the well-nourished showed that cognitive ability was significantly lower for those at risk compared to the well-nourished (MMSE: PAR md 27.0 [Q1 24.0 Q3 29.0], WN md 29.0 [Q1 27.0 Q3 30.0], p=0.018; memoryDL: PAR 26%, WN 7%, p=0.001). Using a cutoff point of 23/24 for MMSE revealed that of those at risk, 19% had an MMSE score of 23 or lower compared to 6% among well-nourished (p=0.004). Statistically significant differences in cognitive ability were also found four years earlier (OC2) (MMSE: PAR md 28.0 [Q1 25.0 Q3
29.0], WN md 29.0 [Q1 27.0 Q3 29.0], p=0.021; memoryDL: PAR 16% versus WN 6%, p=0.023).
Univariate logistic regression at OC3 showed that decreased cognitive ability had a significant impact on the odds of being at risk of malnutrition (MMSE: OR 5.0, p<0.001; memoryDL: OR 4.3, p=0.001). A multivariate logistic regression analysis including the variables MMSE (dichotomized), memoryDL, health poorer compared to four years ago, and hospital stay during the past two months showed that MMSE had the greatest impact on the odds of being at risk of malnutrition (OR 5.3 p<0.001). Performing within-group tests over the three test occasions, cognitive ability decreased over time in those at risk (MMSE p=0.02; memoryDL p=0.04) but not in the well-nourished.
A comparison of men and women regarding nutritional status (MNA) at OC3 showed no significant differences. Men at risk of malnutrition had

45
lower cognitive ability compared with well-nourished men (MMSE: md 26.0 [Q1 22.5 Q3 29.0], md 29.0 [Q1 28.0 Q3 30.0], p=0.001); this was not found in women. A multivariate logistic regression on the same variables as for the whole group, i.e. MMSE (dichotomized), memoryDL, health poorer compared to four years ago, and hospital stay during the past two months was performed. The outcome showed that the odds of being at risk of malnutrition increased with cognitive impairment (MMSE: OR 13.8, p<0.001), as well as with perceiving poorer health compared to four years ago (OR 5.0, p=0.011) for men. For women, recent hospital care (OR 6.4, p=0.042) and decreased cognitive ability (memoryDL: OR 5.1, p=0.030) were predictors for being assessed as being at risk of malnutrition.
Changes that occur in the couples regarding foodwork and meals (II, III)
The persons with dementia usually described that memory loss was not something that affected them during foodwork, and usually no difficulties in preparing or eating were expressed (II); partners also described how foodwork and meals were the same as before the disease. The dementia disease could fluctuate, though, and what had worked one day for the person with dementia might be a problem the next (III).
Some persons with dementia experienced that they did have some problems with their memory and that this affected the foodwork (II), and this was also expressed by partners (III). Changes that occurred concerned the person with dementia having trouble managing the shopping (II, III), as well as setting the table and cooking the food. The persons with dementia were no longer able to take the initiative regarding what to eat, chose to stay out of the kitchen, and were referred to as someone who no longer had an interest in foodwork or meals. As a result of the dementia, they were no longer able to cook since they could not handle the complex situation and, for instance, the food would turn out too spicy or some ingredients would be forgotten. The partners were not sure if the person with dementia understood this themselves (III).
46
Persons with dementia described how they had changed their ways of living as a result of their inability to perform foodwork on their own, and how they missed performing these activities (II). Partners described an increased responsibility for foodwork and meals since their spouses’ ability to prepare food had been affected by the disease. Only male partners mentioned this as new activities. It could be a problem when the person with dementia, who used to be in charge of the foodwork, no longer had the ability to prepare food (III). Changes also had to do with a new routine for meals whereby the person with dementia left home for the day care centre and ate his/her meals there a couple of days a week (II, III). This created a feeling of loss for the partner, even though it was not described as a problem (III).
Changes in eating also arose for the person with dementia as a result of the disease, which included having trouble remembering what one had eaten the day before (II) or forgetting to eat. Decreased appetite and a lack of feeling hungry were also described, as was eating constantly. For the partner, this could result in blaming him/herself for the person’s decreased food intake. Changed eating behaviour in persons with dementia was also noted, like avoiding certain foods, enjoying desserts more or imitating what the partner ate (III).
Another change, only mentioned by female partners, was the lack of conversation during meals, for instance resulting in spouses no longer receiving appreciation for the food they had prepared. Overall they talked less with each other, and partners found it hard to sustain conversation around the kitchen table (III).
Activities of importance to uphold regarding foodwork and meals (II, III, IV)
There was foodwork that the persons were able to carry out and perform independently, such as shopping, baking, cooking food, setting the table, peeling vegetables and washing the dishes (II, III). It was described that the persons with dementia wanted to do these things and preserve their independence (II). Staff also felt it was important to preserve the person’s own abilities and independence, and therefore that meals should be prepared

47
at the person’s own home. This also entailed that the person’s ability to eat independently or shop on his/her own was preserved, as it could result in the person feeling that he/she was competent and needed, as well as participating and contributing (IV). Partners who had taken over the responsibility in order to maintain a stable situation and uphold the couple’s routines mentioned that the knowledge and experience of the person with dementia were needed, because of the partner’s insecurity about how things should be done to prepare food and create proper meals (III).
Adjusting foodwork and meals to cognitive changes (II, III, IV)
Foodwork and meals sometimes had to be adjusted as changes occurred, which meant that persons with dementia found their own strategies and routines in order to be able to continue with these activities (II). Further, both family members and formal caregivers could help and support the person when needed (III, IV), and it was recommended that support be structured based on the person’s needs, wishes and problems (IV).
To be able to continue shopping, persons with dementia used shopping lists. One woman explained that she was able to remember what she needed to buy as long as she did not talk to people while she walked around the supermarket (II). Getting help from others with buying and bringing the groceries home could be used as a means of getting food (II, III, IV).
If a person was considered unable to perform foodwork independently, meals could be created together with him/her, and this help could come from either family members (II, III, IV) or formal caregivers. This meant giving support and help during foodwork, including being there and supervising but not taking over (IV). Giving orders or delegating tasks can help people with dementia take part in foodwork. To make them involved and aware in foodwork and meals, they could be verbally reminded of what was going to happen (III), and a menu of the meals for the whole week could help them get an overview (II).

48
Supervising included making sure the person used the right amount of ingredients, such as spices, or that he/she did not burn anything (IV). When ingredients were set out, the person with dementia recognized and understood what they were supposed to do (III), and after ingredients were used they could be put away to minimize the risk of using them twice (II). Technical devices could be used as an aid in maintaining foodwork. This meant that a timer could be used for the stove (II, IV) and that watches could also be used – not only ordinary watches to keep track of the time and to know when it was time to eat (II), but also special watches designed to help persons with memory loss. It was expressed that during more advanced activities the responsibility should be given to someone else (IV).
Occasionally, persons with dementia had to simplify the cooking to be able to manage. This meant preparing uncomplicated food or buying partly or ready-cooked meals that only need to be heated (II), or decreasing the workload by only being responsible for breakfast or the evening meal instead of all meals. Maintaining meals in the home meant that someone else had to take over the main responsibility for foodwork to ensure that the person received proper meals (IV). It was sometimes also a necessary strategy, for the partner to be able to prepare food, to exclude the person with dementia from the kitchen (III). For partners to learn how to manage these new activities, food classes allowing them not only to learn to cook but also to meet others in the same situation could be a solution (IV).
New habits and solutions were other ways of managing meals, and helped not only the person with dementia but also the partner. Meals-on-wheels, as well as eating at day care centres or restaurants, was described (II, III, IV), and assistance could be given to ensure that the person had access to mobility service or that someone accompanied him/her to the restaurants. Replacing ordinary meals with meals-on-wheels or pre-packaged products was expressed by staff as something frequently used today, but it was asserted that the meals should be cooked in the person’s home (IV). However, moving meals outside the home helped decrease the partner’s workload (III, IV). Even if there had been changes, home-like and familiar meals should be made, which meant that the food served should be what the person was used to eating and should taste like a home-cooked meal (IV); people could also find ways to preserve old habits, like serving the food like

49
in the past (II). The surrounding environment, such as when to eat and other old routines, should also be considered to make the meal as familiar as possible. However, staff expressed that some people actually liked trying new tastes (IV).
Eating sometimes needed attention as a result of changes. To make sure the person obtained adequate food intake, the food prepared should be dishes the person liked (III, IV), and products containing more fat could be used (III). Pedagogical meals in appetizing atmospheres were suggested (IV). If the person with dementia imitated food behaviour, one could put more food on one’s plate to make the person also took a larger portion (III). Attending and supervising during the meal made it possible to ensure that the person started eating as well as finished the meal (IV).
Since changes in conversation sometimes occurred, certain tricks were used to make the person with dementia converse during meals. Choosing to discuss things that happened in the old days, or in this very second, could make it possible to have a conversation. Partners described having adjusted to the silence, which meant either accepting it or using the radio to break the silence (III).

50
Discussion
Reflection on the findings
The main results from the four papers revealed that cognitive ability affects nutritional status, i.e. low cognitive ability leads to increased risk of malnutrition. Persons with dementia and their partners experienced that foodwork and meals were affected, and expressed transitions in roles, routines and relations. It was described that there was foodwork that the persons with dementia could perform, and that abilities and independence should be preserved if possible. Support was sometimes needed, and it was emphasized that this was based on the person’s needs, wishes and problems. Meals-on-wheels was commonly described as a solution when foodwork and meals deteriorated.
Decreased cognitive ability increases risk of problems with nutritional status and foodwork
The results show that low cognitive ability is associated with malnutrition among home-living older persons. Looking at the respective MMSE scores for those at risk of malnutrition and the well-nourished, there is a slight difference in median MMSE score (I), which raises questions of whether these differences are actually of clinical relevance. However, using a cutoff point of 23/24 clarifies such a difference as it is 19% among those at risk compared with 6% of well-nourished people who had an MMSE score lower than 23 at OC3 (I). Using such a cutoff point is common (Aevarsson & Skoog, 2000; Grut et al., 1993), but lacks the sensitivity needed for use as a diagnostic tool for dementia; i.e. the instrument tends to result in false positives. However, it is suggested that it be used as a screening tool (Grut et al., 1993). Furthermore, the subjective question regarding whether their memory affects daily life also showed that those at risk of malnutrition experienced that it affected their daily life to a higher extent compared with the well-nourished (I). One might argue, though, that this is just a single
51
question about cognitive ability. However, such a subjective question should not be neglected as it has been found to be associated with cognitive decline as well as dementia, especially in predicting future decline (Jonker, Geerlings, & Schmand, 2000). As in these results (I), an association between nutritional status and cognitive status has also been found (Fagerström et al., 2011; HaeKwan et al., 2009). Consequently, paying attention to persons with decreased cognitive ability is important in order to prevent nutritional problems: when assessing home-living persons with dementia, as many as 43% were assessed to be at risk of malnutrition and another 2% as malnourished (Roque et al., 2013). This suggests that insufficient attention is paid to improving nutritional status in home care or outpatient care, but might also be a result of the fact that when nutritional problems occur it is hard to improve the status among home-living persons. In a recent literature review including intervention studies between 2004 and 2012 on mealtime difficulties among persons with dementia, only two studies had been carried out in an outpatient care setting. In these studies, in which nutritional supplements and training/education programmes for physicians, caregivers and patients were given, some improvement was noted; however, there is insufficient evidence and research on this matter, not least in a Swedish context (Liu, Cheon, & Thomas, 2013).
The longitudinal study (I) showed that cognitive ability was lower even four years earlier for those at risk of malnutrition compared to the well-nourished, which indicates that as soon as a person experiences or is observed to have decreased cognitive ability, nutritional status should be assessed. Perhaps it should be standard that nutritional status is measured for all persons during the dementia assessment. Assessing nutritional status in all persons receiving in-hospital care, primary care or care provided by the municipality have been highlighted in the national quality register Senior Alert. Yet, the degree to which municipalities and county councils assess and register nutritional status varies (Senior Alert, 2013 ). This has been confirmed in interviews with nurses and nursing mangers in Sweden, who described that nutritional assessment tools were seldom used (Persenius et al., 2008). Besides, as Watson (2011) states, assessing nutritional status does not mean it will improve. Instead, it should be understood as a first step towards being able to improve nutritional status when necessary.

52
Transition in roles, routines and relationships
Changes in foodwork and meals were described, and seemed to be related to which member of the couple used to be in charge of these activities (II, III). In the Life Nourishment Theory (LNT), adjusting to an evolving life is described as experiencing changes in a family in which a person has dementia, explained as a process by which the family becomes aware of, gives meaning to, and finally responds to the changes (Genoe et al., 2012). Evans and Lee (2013) used the transition concept to explain such changes in everyday life, in a review study including couples in which one partner had dementia. When it comes to roles in couples, this transition means that the person with dementia steps back from his/her ordinary duties and responsibilities whilst the partner takes on new ones (Evans & Lee, 2013). Using gender roles to explain the transitions in roles that occur in couples as a result of the dementia might be troublesome, as the results indicate that this probably has more to do with who used to be in charge of these activities rather than gender. However, these things seem to be intertwined when it comes to foodwork and meals. In Paper III it was male partners who described that having the main responsibility was something new, something they had learned later in life. Similar results were found in the study by Fjellström et al. (2010), in which particularly men described an unfamiliar situation regarding foodwork and meals even though they had sometimes played a peripheral role in the past. Persons previously not in charge of foodwork can have trouble performing such activities, as described by Russel (2007). However, husbands taking over these responsibilities have expressed pride at achieving activities while caring for their partner (Sanders & Power, 2009), and experienced well-being when cooking (Kullberg et al., 2010). A study including men caring for their wives revealed that both partners in the couple were sliding into new food roles. For the caregiving husbands, this meant that they gradually performed more preparation and ultimately came to be in control of these activities, whilst the partners with dementia moved towards doing less (Atta-Konadu et al., 2011). In Paper II a majority of the interviewed persons with dementia were females, and when it was no longer possible for them to perform foodwork they missed doing it (II). This is in accordance with results from other studies, which have shown that older women link the inability to perform foodwork with feelings of

53
sadness (Sydner et al., 2007) as well as guilt and frustration (Sidenvall et al., 2001). Perhaps females find these activities important, which might be related to their thinking of foodwork as part of their identity. Foodwork has traditionally been connected to female roles (DeVault, 1991), and a recent study showed that women preferred to engage in activities related to cooking/eating more often than men did (Menne, Johnson, Whitlatch, & Schwartz, 2012). A Canadian study also revealed that interviewed older women with dementia found household chores, such as foodwork, extremely important since such activities constituted their personhood and helped them retain a sense of their personal identity (Phinney, Chaudhury, & O’Connor, 2007).
Meal routines were also transformed, and for some this meant that less foodwork was carried out in the home and instead that meals-on-wheels, day care centres and restaurants came to be more frequently used (II, III). It has previously been described that changes in routines were due to the healthy partner not finding it appropriate to take on activities formerly performed by the person with dementia, or the healthy partner not having an interest in these activities but instead finding other ways to manage (Atta-Konadu et al., 2011). Eating out can be one way to reduce foodwork and demands, not least for the person who has taken over the foodwork. For single-living persons with dementia, moving meals outside the home can help them increase their social interaction (Cassolato et al., 2010). However, family caregivers have regretted simplifying and changing routines, expressing that it made them feel like their meal standards were slipping (Keller et al., 2007). Single-living persons have also associated changes in routines with feelings of a negative nature, e.g. dependence and loneliness, even though they were grateful to receive meals-on-wheels (Pajalic, Persson, Westergren, Berggren, & Skovdahl, 2012).
Relationships and social interaction with others are highlighted in the meal concept (Oltersdorf et al., 1999; Sobal, 2000). According to LNT, meals create opportunities to relate to and connect with the self, as a couple and also within a wider perspective, i.e. within social networks. Further, they can make it easier for families to stay together as a unit and be connected (Keller et al., 2010). However, this can be troublesome as the ability to speak sometimes changes due to the disease (Alzheimer's Association, 2013).
54
Partners of people with dementia expressed that the communication during meals was not the same as it used to be; the person with dementia became quieter or was not always able to follow on-going dialogue (III). Loss of conversation has previously been found to change the pattern of daily life within couples (Walters et al., 2010), and has been considered to be one aspect that can make a partner see his/her loved one with dementia as a different person than before, which could lead to a disruption of marital closeness (Boylstein & Hayes, 2012). In previous studies, partners have described that the relationship changes from an equal situation to one in which the healthy spouse becomes more of a caregiver than a partner (Walters et al., 2010). Partners learned ways to help the person with dementia participate in a dialog when he/she had trouble communicating (III), which is also described in the LNT. However, verbal communication is not the only way to be connected; things like hugs and laughter can also be helpful in connecting (Keller et al., 2010). Non-verbal communication has also been previously described as useful in helping persons with dementia remain part of the communicative world when they lost the ability to converse (Hubbard, Cook, Tester, & Downs, 2002).
Foodwork and meals worked quite well, according to persons with dementia as well as their partners (II, III). Perhaps performing these activities can serve as a hub for preserving relationships in everyday life, as this is actually something that has not changed. The LNT describes that sharing foodwork and meals can promote connections (Keller et al., 2010), and it has previously been described that foodwork includes shared activities that can help couples stay engaged with one another (Hellström, Nolan, & Lundh, 2005). However, when changes occurred, persons with dementia and their partners adjusted and found strategies for managing foodwork and meals (II, III). Using different strategies to compensate for memory loss is common, and has previously been described as helping persons with dementia to manage (Nygård, 2004; Öhman et al., 2008). This is similarly described in the LNT, which further explains that these strategies can be something the person with dementia and their families obtain through both experience and research. Further, trial and error are commonly used to learn how to deal with changes (Genoe et al., 2012). Hence, passing along results from studies like this one can help other couples in similar situations increase their

55
knowledge, and the LNT advocates that support groups and networks can be helpful for families (Genoe et al., 2012).
The importance of staying independent
It was important for persons with dementia to remain independent (II), and formal caregivers also expressed that the person’s own abilities and independence should be preserved (IV). In a study on healthy eating, including older persons from several European countries, a strong desire to manage oneself was expressed (Lundkvist, Fjellström, Sidenvall, Lumers, & Raats, 2010), and similar results have been found among older women in Sweden (Andersson & Sidenvall, 2001; Sidenvall et al., 2001). Actually, doing things oneself has previously been described as being so important that people have tried to manage themselves even though they actually needed support, which resulted in deficient food intake (Gustafsson, 2002). An explanation for why foodwork is so important for older persons might be related to the results of a study by Haak, Fänge, Iwarsson, and Ivanoff (2007), i.e. that being able to perform daily activities is one way to preserve your image as independent. Further, Porter (2007) found that older women associated the ability to cook with the ability to live on their own. The desire to be independent can also be related to current policies reflecting that independence is something to strive for (Ministry of Health and Social Affairs, 2003:91), and people of today have likely been socialized to value independence. Dependence, on the other hand, is a stigmatized concept (Fine & Glendinning, 2005; Munnichs, 1976) and can create a fear of not being seen as a respected member of society.
Support from partners or formal caregivers during foodwork and meals is sometimes necessary (III, IV). As capacities decrease (WHO and Alzheimer’s Disease International, 2012), dementia affects the ability to stay independent and increases the need to rely on others (Steeman et al., 2007). However, according to the LNT, focusing on foodwork and meals can preserve one’s own identity and dignity as it provides an opportunity to choose what to eat and with whom, and how foodwork should be managed, which can help a person with dementia gain control over life when his/her capacities change (Genoe et al., 2010). Furthermore, in health care

56
independence is more than just the competence to perform daily activities; it instead includes autonomy and the ability to have control and make one’s own decisions (Tamaru et al., 2007), which strengthens the results suggesting that the person should do as much as possible him/herself (IV). Perhaps becoming more and more dependent results in a need to feel useful and that one is contributing in some way, as highlighted in the LNT (Genoe et al., 2010). Staff mentioned that including the person with dementia, instead of just taking over, could help the person feel like he/she was competent and needed as well as that participating and contributing (IV). The LNT explains that it is a balancing act between respecting the person and making foodwork safe (Genoe et al., 2010). Fjellström and Mattsson Sydner (2013) also highlight the problem of providing autonomy and at the same time protecting the person, as independence could endanger his/her health and quality of life. Technical devices were described as something that could make it possible to maintain foodwork, like using a timer for the stove (II, IV), which also increased the person’s safety. Hence, independence should be understood as a continuum including several levels and one might need assisting devices, for instance; but this decreases the independence of others, which was also found in a review by Bonikowsky et al. (2012). This is important from a partner perspective as well, since they might struggle with changes themselves, and by upholding the person’s functions it might actually be possible to decrease the burden on the partner. Hence, as described in the LNT, the partner can be the one who becomes dependent (Genoe et al., 2010) as he/she needs help from the person with dementia to perform foodwork, as mentioned in Paper III. This also highlights what Munnichs (1976) writes about dependence and independence: that there is a social world in which people meet and relationships are created, i.e. in some ways we are all dependent on each other. Instead, the focus should be on creating care that has its starting point within the person, which is in accordance with person-centred care (Edvardsson et al., 2008).
Using a person-centred care approach is essential in foodwork and meals
In Paper IV, staff described several means for improving foodwork and meals for persons with dementia who were in need of support, including
57
supporting the person at home, eating at restaurants and providing pre-packaged food (IV). These findings are significant; there is little knowledge about how to support persons with dementia and their families at home, as most research has been carried out in special housing or hospitals (Aselage & Amella, 2010). However, as more older persons tend to live at home longer more of them develop dementia (Ferri et al., 2006), and an increased need of home care is to be expected (Genet et al., 2011). The problems and support needed may differ between persons with dementia living at home and those cared for in special housing or hospitals (Jackson, Currie, Graham, & Robb, 2011). However, one might argue that some of the interventions can be applicable to both home-living persons and those in special housing and hospitals; such results have been found by Keller et al. (2008). According to Amella, Grant and Mulloy (2008), who tested interventions for persons with moderate- to late-stage dementia, the ultimate goal is to enhance their meal experience and quality of life, preserve their independence and dignity, engage them in social interaction, and give meaning to every meal. For this to be possible, the person must be understood based on his/her context and experiences, which is in agreement with the meaning of person-centred care. The quality of the relationship with the person with dementia may also increase when spending time in the person’s home, which is significant in person-centred care as well as nursing care (Edvardsson et al., 2008). Further, a benefit when working in the home environment is that the chances of getting to know the person are enhanced since being in the person’s own context offers an understanding of his/her life and routines (Öresland, Määttä, Norberg, Jörgensen, & Lutzén, 2008). Having access to such information probably makes it easier to offer support based on the person’s individual needs and wishes, which is advocated as the foundation of supporting a person (IV). In other Swedish studies in which older persons have been interviewed, the importance of receiving help on one’s own terms was emphasized (Dunér & Nordström, 2010), and regarding receiving meals distributed by the municipality older persons themselves had suggestions about how the service could be improved (Pajalic, Persson, Westergren, Berggren et al., 2012)). This highlights the benefit of including the persons themselves when designing services, and is in accordance with person-centred care, which underlines personalized care and shared decision-making (Edvardsson et al., 2010). The national

58
guidelines for persons with dementia also highlight that care and nutritional interventions should be individualized (National Board of Health and Welfare, 2010). The causes of malnutrition can be many; therefore, several interventions can be needed and these should be based on the person’s needs, resources and problems, as this has previously been found to be effective (Lorefält & Wilhelmsson, 2012; Wikby et al., 2009). Yet, there are very few published research studies on person-centred care, and even fewer that identify benefits (McCormack, 2004). Further, even though person-centred care is promoted (National Board of Health and Welfare, 2006a, 2010) it is not always achieved (Docteur & Coulter, 2012). This is also in accordance with the results revealing that there were several means for improving foodwork and meals depending on the individual’s needs and resources, yet meals-on-wheels were often offered (IV). This is supported in the findings by County Administration Boards of Sweden (2009), that food distribution has increased whilst food preparation at home has decreased. Further, what is offered seems to depend on local guidelines rather than the person’s preferences (Dunér & Nordström, 2010). Food distribution, i.e. meals-on-wheels, can naturally be used when suitable. However, a recent Swedish qualitative study among professionals involved in food distribution service revealed that it was a deficient intervention, with staff not knowing what actually happened after they delivered the food, and that a preferable way would have been to stay while the person ate (Pajalic, Persson, Westergren, & Skovdahl, 2012).
Methodological considerations
Validity and reliability
Validity and reliability need to be considered in order to draw clear conclusions from quantitative studies (Kazdin, 2003).
A threat to internal validity is related to the design used when including participants (Kazdin, 2003; Polit & Beck, 2012). The same sample as in the study by Takkinen et al. (2004) was used in Paper I. From a survey including unlike-sex twins (Gold et al., 2002), a sample of 382 twin pairs were invited to participate in in-person testing. Of this sample, a total of 266 persons did

59
not participate because they: did not want to participate (n=114); had died (n=30); or were excluded because their twin declined participation or had died (n=106); further, 16 persons could not be contacted. Therefore, the sample at OC3 consisted of 249 unlike-sex twin pairs (498 persons) (Taakinen et al., 2004). This indicates that the sample is not similar to the normal population as they were probably healthier. However, many persons decided to take part in the study at all three test occasions; i.e. those participants in Paper I grew frailer over time as a result of ageing. It is fair to believe that in the normal population, a higher rate of people died during the longitudinal data collection as a result of frailty, with the result that the healthiest persons survived. Consequently, the sample (I) and the normal population look more equal over time. Further, the attrition rate can be affected in longitudinal studies, meaning that dropouts may differ to some degree compared to those included in the sample. In Paper I, 60 persons between OC1 and OC2 and another 12 between OC2 and OC3 chose not to participate, which can have affected the results. Even so, many persons decided to take part in the study at all three test occasions. At OC3, 48 persons were excluded because they lacked a complete MNA score or lived in special housing. A comparison of those participating at OC3 (n=258) and those who did not (n=48) showed that those who were excluded had significantly lower MMSE scores and Activity of Daily Living (ADL) functioning, which indicates that those who participated were healthier.
The participants in Paper I were unlike-sex twins, which could be a threat to external validity. However, according to Simmons et al. (1997), twin pairs in older age groups are comparable to non-twins in the same age groups. Further, using statistical analysis for independent or dependent groups, i.e. treating them as matched pairs, gave similar results, which indicates that the relationship between the twins did not affect the results, which can therefore be generalized to other groups of older people as well.
Low statistical power can be a threat to statistical conclusion validity (Kazdin, 2003). In Paper I power was not calculated, but the sample included 258 persons and significant differences were found in the analysis. A recommendation for decreasing the risk of bias includes standardizing procedures, as neglecting to do so can threaten statistical conclusion validity (Kazdin, 2003). Here, a few experienced research nurses collected all data

60
using standardized questionnaires (I). Further, in-person testing has been proven to have positive effects on response rate (Polit & Beck, 2012).
For the instruments used (I), satisfactory reliability was found for both MMSE (Tombaugh & McIntyre, 1992) and MNA. For MNA this is also true for validity (Guigoz, 2006). MMSE shows good construct validity, and is a commonly used instrument for testing cognitive impairment. Yet, it has low sensitivity regarding mild degrees of cognitive impairment (Tombaugh & McIntyre, 1992). Both MMSE (Grut et al., 1993) and MNA (Guigoz, 2006) are commonly used in a Swedish context. A disadvantage is that the supplementary questions have not been tested for validity or reliability. However, a strength is that the variables have remained basically unchanged over the three occasions of data collection.
The use of parametric tests for MMSE in Paper I can be criticized, as non-parametric tests should be used for ordinal variables and for ratio scale variables that are not normally distributed (Thorne, 2003). Therefore non-parametric tests were used in this thesis. However, this did not affect the results with regard to statistical significance, even though the p-value increased when non-parametric testing was used. For instance, testing for differences in MMSE at OC3 between persons at risk and those who were well-nourished resulted in a p-value <0.001 compared to p-value 0.018. Further, meals-on-wheels were used as an independent variable in the multivariate logistic regression analysis in Paper I. However, one might argue that this is likely a dependent variable. Therefore, this variable was not included in the multivariate logistic regression analysis in this thesis.
Trustworthiness
Lincoln and Guba (1985) describe that trustworthiness in qualitative data can be attained using the four criteria of credibility, transferability, dependability and confirmability, which have been considered in Papers II, III and IV.
Paper II, including persons with dementia, was inspired by ethnography. Using an ethnographic approach means that fieldwork and observations are important in performing a study (Wolcott, 2008). However, here mainly interview data were collected and used in the analysis, which can be seen as

61
a limitation of the study and could affect its credibility. However, Wolcott (2008) writes that, after observation, interviews are the next best way to gather data in an ethnographic study. Further, he explains that it is better to conduct one in-depth interview than several only on the surface (Wolcott, 2008). However, the dementia disease affected the possibility to gain deep information. Hence, even though the persons with dementia were able to express their views, they seldom gave detailed descriptions. Instead, their answers were often short and they sometimes had trouble remembering words, lost focus or repeated themselves. Even though persons with dementia are able to contribute in a meaningful way in interviews (Moore & Hollett, 2003), they can have trouble distinguishing the present from how things used to be (Edvardsson & Nordvall, 2008), and can normalize or deny problems (Howorth & Saper, 2003). Therefore, it would probably have been good to include observations during foodwork and meals in the data collection. Another way would have been to interview the couples together. However, this could have led to the healthy partner’s voice being given greater importance and regarded as being closer to the truth; also, healthy partners tend to talk for the couple, as described by Hellström, Nolan, Nordenfelt et al. (2007). Besides, the purpose was to hear the person’s own experiences (II, III) and it therefore seemed appropriate to hold individual interviews. Also, those living alone would have been excluded in such an approach.
Papers II and III have similarities, but there is a distinction. It was namely determined that when interviewing persons with dementia, all data should be collected in the home, and this resulted in a greater understanding of the person’s daily life. This is also in agreement with ethnographic methods in which the importance of the context and setting is highlighted (Wolcott, 2008). Further, giving a thick description of the context can strengthen transferability (Lincoln & Guba, 1985). A threat to the credibility is that accessibility determined which persons participated. It was public health nurses who asked about participation in the Food, Exercise and Memory Loss project, and only a few people were asked to participate. Among these, everyone who the researcher considered to be able to communicate verbally about foodwork and meals was included (II). Further, in cases in which the persons in the project had a partner, they were also asked to participate in a
62
separate interview study (III). However, a benefit of including persons from the project was that several hours were spent at each home and a trustful relationship had been established already before the interviews were conducted, which hopefully allowed the participants to talk openly about their foodwork and meals, and rich information was obtained. This can be understood as prolonged engagement, which is one way to gain credibility (Lincoln & Guba, 1985). Establishing a trustful and relaxed relationship before collecting data is important when including persons with dementia in research (Hellström, Nolan, Nordenfelt et al., 2007).
A similar procedure was used to include staff (Paper IV): it was likely those who were the most interested in the topic who volunteered. However, since the aim was to capture staff views on how foodwork and meals could be improved, this hopefully gave the richest descriptions. Further, the participants in each focus group knew each other before the interviews, which can be an advantage since they shared experiences of incidents and could relate to each other when discussing things (Kitzinger, 1995). The focus group technique is considered to be a good method to use when the purpose is to capture opinions on a specific topic, and makes it possible to include more participants in a short time compared to interviewing one participant at a time (Polit and Beck, 2012). However, using focus group interviews might affect the participants and prevent them from fully expressing their opinions (Kitzinger, 1995; Polit & Beck, 2012), and people can become silent or dominant in the discussion (Polit & Beck, 2012). To avoid this, the moderator tried to include everyone during the interviews, which is in accordance with the method (Krueger & Casey, 2009). Further, to attain credibility and dependability, the assistant summarized the content after each vignette in order to try to prevent misunderstanding (IV). Partners were given a brief summary of the interview during a second home visit to ensure that everything had been understood correctly, and were asked follow-up questions (III).
The researcher’s own experience with persons with dementia was limited before these studies, which might have had an impact on the interviews. However, this might have had both positive and negative consequences, as it probably meant that different questions were asked compared to what someone familiar with the disease and how it affects people suffering from it
63
would have asked. Interviews with persons with dementia (II) as well as their partners (III) were performed continuously as participants were included, and this therefore should not have affected the interviews. However, the analysis of data from persons with dementia was completed before the analysis including data from partners was conducted. This can have had an influence on the analysis of data from partners, and might have affected the confirmability. To minimize such risks, a dialogue was maintained between the researchers during the whole research process (II, III, IV), and especially during different phases of the analyses continuous discussions were held to ensure that there was agreement regarding the content. The final results were discussed with other researchers as well, at seminars and conferences. According to Lincoln and Guba (1985), this strengthens credibility, dependability and confirmability. In Paper III, a metaphor was used during the analysis. The benefit of using metaphors is that, because of their richness and complexity, it is possible to go further in the analysis to form new meanings and understandings of the data. Moreover, metaphors can also put separate bits together and create a whole (Polit & Beck, 2012). Other researchers have used metaphors in a similar way as in the present study, i.e. to understand processes and relationships in the data (Bonner & Greenwood, 2005; Drury, Francis, Chapman, & Chapman, 2008; Öhlén, Bengtsson, Skott, & Segesten, 2002). There is a risk that the credibility was negatively affected, though, since using metaphors can simplify or overshadow the results. The data in Paper III were not forced to fit the metaphor; instead, it helped the researchers reach an understanding of the data, and hopefully also clarify the partners’ experiences for the reader.
Conclusions and implications
The results revealed that there is an association between cognitive ability and nutritional status, which indicates that for persons with dementia there is a need to assess nutritional status and to intervene early when risk is identified. This thesis has contributed knowledge about what kinds of difficulties home-living persons with dementia and their partners struggle with regarding foodwork and meals. The persons with dementia as well as their partners usually experienced that these activities worked, but as a result of the

64
dementia transitions regarding roles, routines and relationships were distinguished. This meant that partners took on greater responsibility whilst persons with dementia performed less foodwork and their dependence on others increased. This highlights the importance of supporting both partners in a couple in which one has dementia. Further, deepened knowledge was obtained concerning the importance of formal caregivers helping the person feel independent, autonomous and competent during support. Person-centred care is one approach that can help in accomplishing this, and the person’s own needs, wishes and problems should be the foundation when structuring the support.
Future research should focus on intervention studies aiming to improve foodwork and meals at home. That means designing interventions based on personal needs, wishes and resources, using a person-centred care approach during the whole research process, i.e. including older persons with dementia and their partners when planning and implementing such studies.
The researchers who developed the LNT request that it be tested in different contexts to further develop the theory (Lam & Keller, 2012). Here, the LNT was used to increase the understanding of the results, and it would be interesting to test the theory in a Swedish context using a deductive approach, to further confirm whether the LNT is transferable to this context. Besides, the LNT has its basis in the family, and not every person with dementia lives with someone. Single-living persons are probably more vulnerable than others when their abilities decrease, which means that the formal caregiver has a responsibility to make them feel connected and that their identity is being honoured while helping them adjust to the changed situation. Hence, it would be interesting to investigate how staff can facilitate this.

65
Svensk sammanfattning
Att kunna bo kvar i det egna hemmet och vara oberoende av andra har i tidigare studier visat sig vara viktigt för äldre personer. Detta överensstämmer väl med den nationella policyn som poängterar att äldre personer ska bo hemma så länge som möjligt. Att äta bra är en viktig faktor för att äldre ska kunna hålla sig friska och bo kvar i det egna hemmet. Trots det saknas kunskap om måltidsrelaterade aktiviteter och måltider bland hemmaboende personer, inte minst bland de som har en demenssjukdom vilka löper ökad risk för undernäring. Genom att undersöka de erfarenhet som personer med demens, deras partners och personal har rörande måltidsrelaterade aktiviteter och måltider skulle problem kunna identifieras och evidensbaserade interventioner utvecklas.
Syftet med denna avhandling var att undersöka och beskriva måltidsrelaterade aktiviteter och måltider för äldre personer med demens och deras partners i eget boende.
För de fyra studierna som avhandlingen bygger på användes utforskande och beskrivande design Delstudie I är en kvantitativ longitudinell studie bland hemmaboende olikkönade äldre tvillingar där data analyserades med hjälp av beskrivande och analytisk statistik. I delstudie II, III och IV har kvalitativa metoder används för att undersöka måltidsrelaterade aktiviteter och måltider för äldre personer med demens och deras partners. I studien där personer med demens deltog användes en etnografisk ansats (II). Individuella intervjuer genomfördes med partners och analyserades med hjälp av tematisk analys (III). I delstudien där personal deltog samlades data in genom fokusgruppintervjuer och analyserades med kvalitativ innehållsanalys (IV).
Resultaten visade att bland hemmaboende äldre personer finns det ett samband mellan en persons kognitiva förmåga och näringsstatus, d.v.s. låg kognitiv förmåga ger ökad risk för undernäring. Personer med demens och deras partners beskrev att måltidsrelaterade aktiviteter och måltider ibland

66
hade förändrats, vilket innebar att inhandla, tillaga och äta ibland kunde vara svårt. Förändringar som påverkade den sociala interaktionen beskrevs också, där personen med demens hade svårt att medverka vid samtal under måltider. Detta sammantaget tycktes kunde leda till förändringar i roller, rutiner och relationer. Det fanns måltidsrelaterade aktiviteter som personerna med demens kunde utföra och en önskan om att bevara oberoende och förmågor uttrycktes. Dock behövdes stöd och hjälp ibland och det betonades att detta skulle bygga på personens behov, önskemål och problem.
Sammanfattningsvis visar studierna att det finns ett samband mellan minskad kognitiv förmåga och ökad risk för undernäring. Förändringar rörande måltidsrelaterade aktiviteter och måltider påverkar både personer med demens och deras partners. Därför är det viktigt att tidigt stödja både personen med demens och partner. För att möta individuella behov, önskemål och problem skulle personcentrerad vård kunna användas som utgångspunkt vid planering av stödinsatser.

67
References
Ablitt, A., Jones, G.V., & Muers, J. (2009). Living with dementia: A systematic review of the influence of relationship factors. Aging & Mental Health, 13(4), 497-511.
Aevarsson, O., & Skoog, I. (2000). A Longitudinal Population Study of the Mini-Mental State Examination in the Very Old: Relation to Dementia and Education. Dementia and Geriatric Cognitive Disorders, 11(3), 166-175.
Agüero-Torres, H., Thomas, V.S., Winblad, B., & Fratiglioni, L. (2002). The impact of somatic and cognitive disorders on the functional status of the elderly. Journal of Clinical Epidemiology, 55(10), 1007-1012.
Akner, G., & Cederholm, T. (2001). Treatment of protein-energy malnutrition in chronic nonmalignant disorders. American Journal of Clinical Nutrition, 74 (1), 6-24.
Alibhai, S.M.H., Greenwood, C.E., & Payette, H. (2005). An approach to the management of unintentional weight loss in elderly people. Canadian Medical Association Journal, 172(6), 773-780.
Alzheimer's Association. (2013). 2013 Alzheimer's disease facts and figures. Alzheimer’s & Dementia, 9(2), 1-69.
Amella, E.J., & Aselage, M.B. (2011). Mealtime difficulties. In A. O'Meara, T.T. Fulmer, D. Zwicker, & M. Boltz (Eds.), Evidence-Based Geriatric Nursing Protocols for Best Practice (4 ed., pp. 453-468). New York: Springer Pub.
Amella, E.J., Grant, A.P., & Mulloy, C. (2008). Eating behavior in persons with moderate to late-stage dementia: assessment and interventions. Journal of the American Psychiatric Nurses Association, 13(6), 360-367.
Anderson, E.N. (2005). Everyone Eats. Understanding Food and Culture. New York: New York University Press.
Andersson, I., & Sidenvall, B. (2001). Case studies of food shopping, cooking and eating habits in older women with Parkinson's disease. Journal of Advanced Nursing, 35(1), 69-78.
Aselage, M.B., & Amella, E.J. (2010). An evolutionary analysis of mealtime difficulties in older adults with dementia. Journal of Clinical Nursing, 19(1‐2), 33-41.
Atta-Konadu, E., Keller, H.H., & Daly, K. (2011). The food-related role shift experiences of spousal male care partners and their wives with dementia. Journal of Aging Studies, 25(3), 305-315.
Beauman, C., Cannon, G., Elmadfa, I., Glasauer, P., Hoffmann, I., Keller, M., Krawinkel, M., Lang, T., Leitzmann, C., Lötsch, B., Margetts,

68
B.M., McMichael, A.J., Meyer-Abich, K., Oltersdorf, U., Pettoello-Mantovani, M., Sabaté, J.,Shetty, P., Sória, M., Spiekermann, U., Tudge, C., Vorster, H.H., Wahlqvist, M., & Zerilli-Marimò, M. (2005). The principles, definition and dimensions of the new nutrition science. Public Health Nutrition, 8(6a), 695-698.
Blomberg, S. (2004). Specialiserad biståndshandläggning inom den kommunala äldreomsorgen. Genomförandet av en organisationsreform och dess praktik [Swedish]. (Dissertation), Lund University, Lund.
Bond, J., & Cabrero, G.R. (2007). Health and dependency in later life. In J. Bond, S. Peace, F. Dittman-Kohli, & G. Westerhof (Eds.), Ageing in Society, (3 ed., pp. 113-141). London: Sage Publication Ltd.
Bonikowsky, S., Musto, A., Suteu, K.A., MacKenzie, S., & Dennis, D. (2012). Independence: an analysis of a complex and core construct in occupational therapy. The British Journal of Occupational Therapy, 75(4), 188-195.
Bonner, A., & Greenwood, J. (2005). Producing the magnum opus: a metaphor for nephrology nursing expertise acquisition. Journal of Advanced Nursing, 51(1), 64-72.
Bove, C.F., & Sobal, J. (2006). Foodwork in newly married couples: Making family meals. Food, Culture and Society: An International Journal of Multidisciplinary Research, 9(1), 69-89.
Boylstein, C., & Hayes, J. (2012). Reconstructing Marital Closeness While Caring for a Spouse With Alzheimer’s. Journal of Family Issues, 33(5), 584-612.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101.
Brodaty, H., & Donkin, M. (2009). Family caregivers of people with dementia. Dialogues in Clinical Neuroscience, 11(2), 217-228.
Brooker, D. (2004). What is person-centred care in dementia? Reviews in Clinical Gerontology, 13(3), 215-222.
Brooker, D. (2007). Person-centred dementia care: making services better. London: Jessica Kingsley Publications.
Brorsson, A., Öhman, A., Cutchin, M., & Nygård, L. (2013). Managing critical incidents in grocery shopping by community-living people with Alzheimer's disease. Scandinavian Journal of Occupational Therapy, 1-10. doi:10.3109/11038128.2012.752031.
Butcher, H.K., Holkup, P.A., & Buckwalter, K.C. (2001). The experience of caring for a family member with Alzheimer’s disease. Western Journal of Nursing Research, 23(1), 33-55.
Caraher, M., Dixon, P., Lang, T., & Carr-Hill, R. (1999). The state of cooking in England: the relationship of cooking skills to food choice. British Food Journal, 101(8), 590-609.

69
Carpenter, J. (2008). Metaphors in qualitative research: Shedding light or casting shadows? Research in Nursing & Health, 31(3), 274-282.
Cassolato, C.A., Keller, H.H., Dupuis, S.L., Schindel Martin, L., Edward, H.G., & Genoe, M.R. (2010). Meaning and experience of “eating out” for families living with dementia. Leisure/Loisir, 34(2), 107-125.
Chen, C.C.H., Schilling, L.S., & Lyder, C.H. (2001). A concept analysis of malnutrition in the elderly. Nursing Theory and Concept Develoment or Analysis, 36(1), 131-142.
County Administration Boards of Sweden (2009). Socialtjänsten och de äldre. Länsstyrelsernas redovisning för iakttagelser som gjorts i tillsynen inom äldreomsorgen under 2008 [Swedish]. Retrieved from http://www.lansstyrelsen.se/Skane/SiteCollection/Documents/sv/publikationer/2009/aldreomsorg_lstgem3.pdf
Cowdell, F. (2006). Preserving personhood in dementia research: a literature review. International Journal of Older People Nursing, 1(2), 85-94.
De Boer, M.E., Hertogh, C.M.P.M., Dröes, R.M., Riphagen, I.I., Jonker, C., & Eefsting, J.A. (2007). Suffering from dementia–the patient's perspective: A review of the literature. International Psychogeriatrics, 19(06), 1021-1039.
DeVault, M. (1991). Feeding the family. Chicago: University of Chicago Press.
Docteur, E., & Coulter, A. (2012). Patient-centeredness in Sweden’s health system – an external assessment and six steps for progress. Report 2012:3. Stockholm: TMG Sthlm.
Drury, V.B., Francis, K., & Chapman, Y. (2008). The crusade–a metaphorical explication of the journey made by mature female undergraduate nursing students. Rural and Remote Health, 8(3), 978-978.
Dunér, A., & Nordström, M. (2006). The discretion and power of street-level bureaucrats: an example from Swedish municipal eldercare. European Journal of Social Work, 9(4), 425-444.
Dunér, A., & Nordström, M. (2010). The desire for control: negotiating the arrangement of help for older people in Sweden. Journal of Aging Studies, 24(4), 241-247.
Edvardsson, D. (2011). Personcentrerad omvårdnad - definition, mätskalor och hälsoeffekter. In D. Edvardsson (Ed.), Personcentrerad omvårdnad i teori och praktik. Lund: Studentlitteratur.
Edvardsson, D., & Nordvall, K. (2008). Lost in the present but confident of the past: experiences of being in a psycho‐geriatric unit as narrated by persons with dementia. Journal of Clinical Nursing, 17(4), 491-498.
Edvardsson, D., Fetherstonhaugh, D., & Nay, R. (2010). Promoting a continuation of self and normality: person‐centred care as described

70
by people with dementia, their family members and aged care staff. Journal of Clinical Nursing, 19(17‐18), 2611-2618.
Edvardsson, D., Winblad, B., & Sandman, P.O. (2008). Person-centred care of people with severe Alzheimer's disease: current status and ways forward. The Lancet Neurology, 7(4), 362-367.
Ekman, I., Swedberg, K., Taft, C., Lindseth, A., Norberg, A., Brink, E., Carlsson, J., Dahlin-Ivanoff, S., Johansson, I-L., Kjellgren, K., Lidén E., Öhlén, J., Olsson, L-E., Rosén, H., Rydmark, M., & Stibrant Sunnerhagen, K. (2011). Person-centered care—Ready for prime time. European journal of cardiovascular nursing, 10(4), 248-251.
Elo, S., & Kyngäs, H. (2008). The qualitative content analysis process. Journal of Advanced Nursing, 62(1), 107-115.
Elsner, R.J. (2002). Changes in eating behavoir during the aging process. Eating Behaviors, 3, 15-43.
Engel, G.L. (1977). The need for a new medical model: a challenge for biomedicine. Science, 196(4286), 129-136.
Etters, L., Goodall, D., & Harrison, B.E. (2008). Caregiver burden among dementia patient caregivers: a review of the literature. Journal of the American Academy of Nurse Practitioners, 20(8), 423-428.
Evans, D., & Lee, E. (2013). Impact of dementia on marriage: A qualitative systematic review. Dementia. doi:10.1177/1471301212473882
Fagerström, C., Palmqvist, R., Carlsson, J., & Hellström, Y. (2011). Malnutrition and cognitive impairment among people 60 years of age and above living in regular housing and in special housing in Sweden: A population-based cohort study. International Journal of Nursing Studies, 48(7), 863-871.
Ferri, C.P., Prince, M., Brayne, C., Brodaty, H., Fratiglioni, L., Ganguli, M., Huang, Y. (2006). Global prevalence of dementia: a Delphi consensus study. The Lancet, 366(9503), 2112-2117.
Field, P.A., & Morse, J.M. (1995). Qualitative research methods for health professionals. Thousand Oaks, California: Sage Publications.
Fine, M., & Glendinning, C. (2005). Dependence, independence or inter-dependence? Revisiting the concepts of 'care' and 'dependency'. Ageing and Society, 25(4), 601-622.
Fjellström, C. (2004). Mealtime and meal patterns from a cultural perspective. Scandinavian Journal of Food & Nutrition, 48(4), 161-164.
Fjellström, C., & Mattsson Sydner, Y. (2013). Dependence and individualism: The influence of modern ideologies on older people´s food security. In C. Phellas (Ed.), Aging in European Societies: Healthy Aging in Europe (pp. 47-60). New York: Springer.
Fjellström, C., Starkenberg, Å., Wesslén, A., Tysén Bäckström, A.C., & Faxén-Irving, G. (2010). To Be a Good Food Provider: An

71
Exploratory Study Among Spouses of Persons With Alzheimer’s Disease. American Journal of Alzheimer's Disease and Other Dementias, 25(6), 521-526.
Folstein, MF., Folstein, SE., & McHugh, PR. (1975). "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12, 189-198.
Genet, N., Boerma, W.G.W., Kringos, D.S., Bouman, A., Francke, A.L., Fagerström, C., Melchiorre, M.G., Greco, C., & Devillé, W. (2011). Home care in Europe: a systematic literature review. BMC health services research, 11(1), 207. doi:10.1186/1472-6963-11-207
Genoe, M.R., Keller, H.H., Martin, L.S., Dupuis, S.L., Reimer, H., Cassolato, C., & Edward, G. (2012). Adjusting to Mealtime Change within the Context of Dementia. Canadian Journal on Aging/La Revue canadienne du vieillissement, 1(1), 1-22.
Genoe, R., Dupuis, S.L., Keller, H.H., Martin, L.S., Cassolato, C., & Edward, H.G. (2010). Honouring identity through mealtimes in families living with dementia. Journal of Aging Studies, 24(3), 181-193.
Gibson, D. (1998). Aged care: Old policies, new problems. Cambridge: Cambridge University Press.
Gillies, B.A. (2000). A memory like clockwork: accounts of living through dementia. Aging & Menatl Health, 4(4): 366-374.
Gold, C.H., Malmberg, B., McClearn, G.E., Pedersen, N.L., & Berg, S. (2002). Gender and Health: A study of Older Unlike-Sex Twins. Journal of Gerontology, 57(3), 168-176.
Grut, M. , Fratiglioni, L., Viitanen, M., & Winblad, B. (1993). Accuracy of the Mini-Mental Status Examination as a screening test for dementia in a Swedish elderly population. Acta Neurololgica Scandinavica, 87(4), 312-317.
Guigoz, Y. (2006). The mini nutritional assessment (MNA). Review of the literature-what does it tell us? . The Journal of Nutrition, Health & Aging, 10(6), 466-477.
Guigoz, Y., Vellas, B., & Garry, P.J. (1994/1995). Mini Nutritional Assessment: a practical tool for grading the nutritional state of elderly patients. Facts and Research in Gerontology, (2 ed.). Paris: Serdi Publishing.
Gustafsson, Kerstin. (2002). Meals and food in older women : health perceptions, eating habits, and food management. (Dissertation), Uppsala University, Uppsala.
Gustafsson, K., Andersson, I., Andersson, J., Fjellström, C., & Sidenvall, B. (2003). Older women's perceptions of independence versus dependence in food-related work. Public Health Nursing, 20(3), 237-247.

72
Gustafsson, K., & Sidenvall, B. (2002). Food-related health perceptions and food habits among older women. Journal of Advanced Nursing, 39(2), 164-173.
Haak, M., Fänge, A., Iwarsson, S., & Ivanoff, S.D. (2007). Home as a signification of independence and autonomy: experiences among very old Swedish people. Scandinavian Journal of Occupational Therapy, 14(1), 16-24.
HaeKwan, C., Kim, E.A., ByoungHoon, O., & ChangHyung, H. (2009). Nutritional risk and cognitive impairment in the elderly. Archives of gerontology and geriatrics, 48(1), 95-99.
Hammersley, M., & Atkinson, P. (1995). Ethnography. Principles in Practise (2 ed.). London: Routledge.
Hellström, I., Nolan, M., & Lundh, U. (2005). 'We do things together': A case study of 'couplehood' in dementia. Dementia. 4(1), 7-22.
Hellström, I., Nolan, M., & Lundh, U. (2007). Sustaining 'couplehood': Spouses' strategies for living positively with dementia. Dementia, 6(3), 383-409.
Hellström, I., Nolan, M., Nordenfelt, L., & Lundh, U. (2007). Ethical and Methodological Issues in Interviewing Persons With Dementia. Nursing Ethics, 14(5), 608-619.
Henderson, Virginia. (2004). ICN basic principles of nursing care. Geneva: International council of nurses.
Hickson, M. (2006). Malnutrition and ageing. Postgraduate Medical Journal, 82(963), 2-8.
Holm, B., & Söderhamn, O. (2003). Factors associated with nutritional status in a group of people in an early stage of dementia. Clinical Nutrition, 22(4), 385-389.
Howorth, P., & Saper, J. (2003). The dimensions of insight in people with dementia. Aging and Mental Health, 7(2), 113-122.
Hubbard, G., Cook, A., Tester, S., & Downs, M. (2002). Beyond words: Older people with dementia using and interpreting nonverbal behaviour. Journal of Aging Studies, 16(2), 155-167.
Hulko, W. (2009). From ‘not a big deal’ to ‘hellish’: experiences of older people with dementia. Journal of Aging Studies, 23(3), 131-144.
Jackson, J., Currie, K., Graham, C., & Robb, Y. (2011). The effectiveness of interventions to reduce undernutrition and promote eating in older adults with dementia: A systematic review. The Joanne Briggs Institute Library of Systematic Reviews, 9(37), 1509-1549.
Jansson, W., Nordberg, G., & Grafström, M. (2001). Patterns of elderly spousal caregiving in dementia care: an observational study. Journal of Advanced Nursing, 34(6), 804-812.
Jonker, C., Geerlings, M.I., & Schmand, B. (2000). Are memory complaints predictive for dementia? A review of clinical and population‐based
73
studies. International Journal of Geriatric Psychiatry, 15(11), 983-991.
Kazdin, A.E. (2003). Research Design in Clinical Psychology (4 ed.). Boston: Allyn & Bacon.
Keller, H.H., Edward, G.H., & Cook, C. (2007). Mealtime Experiences of Families With Dementia. American Journal of Alzheimer's Disease and Other Dementias, 21(6), 431-438.
Keller, H.H., Østbye, T., & Goy, R. (2004). Nutritional risk predicts quality of life in elderly community-living Canadians. The Journals of Gerontology. Series A, Biololgical Sciences and Medical Sciences, 59(1), 68-74.
Keller, H.H., Schindel Martin, L., Dupuis, S., Genoe, R., Edward, H.G., & Cassolato, C. (2010). Mealtimes and being connected in the community-based dementia context. Dementia, 9(2), 191-213.
Keller, H.H., Smith, D., Kasdorf, C., Dupuis, S., Schindel Martin, L., Edward, G.H., Cook, C., & Genoe, R. (2008). Nutrition education needs and resources for dementia care in the community. American Journal of Alzheimer's Disease and Other Dementias, 23(1), 13-22.
Kitwood, Tom. (1997). Dementia reconsidered: The person comes first: Buckingham: Open University Press.
Kitzinger, J. (1995). Qualitative research: introducing focus groups. Bmj, 311(7000), 299-302.
Krippendorff, K. (2012). Content analysis: An introduction to its methodology. Thousands Oaks, California: Sage Publications.
Krueger, R.A., & Casey, M.A. (2009). Focus groups: A practical guide for applied research: Thousands Oaks, California: Sage Publication.
Kullberg, K., Björklund, A., Sidenvall, B., & Åberg, A.C. (2010). ‘I start my day by thinking about what we’re going to have for dinner’–a qualitative study on approaches to food‐related activities among elderly men with somatic diseases. Scandinavian Journal of Caring Sciences, 25(2), 227-234.
Lagergren, M. (2002). The systems of care for frail elderly persons: the case of Sweden. Aging clinical and experimental research, 14(4), 252-257.
Lam, I.T.Y., & Keller, H.H. (2012). Honoring Identity Through Mealtimes in Chinese Canadian Immigrants. American Journal of Alzheimer's Disease and Other Dementias. doi:10.1177/1533317512449727.
Larsson, K. (2006). Care needs and home-help services for older people in Sweden: does improved functioning account for the reduction in public care? Ageing and Society, 26(03), 413-429.
Larsson, K., & Thorslund, M. (2002). Does gender matter? Differences in patterns of informal support and formal services in a Swedish urban elderly population. Research on Aging, 24(3), 308-336.

74
Lincoln, Y.S., & Guba, E.G. (1985). Naturalistic inquiry. Newbury Park, California: Sage Publication.
Liu, W., Cheon, J., & Thomas, S.A. (2013). Interventions on mealtime difficulties in older adults with dementia: A systematic review. International Journal of Nursing Studies. doi: 10.1016/j.ijnurstu. 2012.12.021
Lorefält, B., & Wilhelmsson, S. (2012). A multifaceted intervention model can give a lasting improvement of older peoples’ nutritional status. The Journal of Nutrition, Health & Aging, 16(4), 378-382.
Lundkvist, P., Fjellström, C., Sidenvall, B., Lumbers, M., & Raats, M. (2010). Management of healthy eating in everyday life among senior Europeans. Appetite, 55(3), 616-622.
Luppa, M., Luck, T., Weyerer, S., König, H.H., Brähler, E., & Riedel-Heller, S.G. (2010). Prediction of institutionalization in the elderly. A systematic review. Age and Ageing, 39(1), 31-38.
Manthorpe, J., & Watson, R. (2003). Poorly served? Eating and dementia. Journal of Advanced Nursing, 41(2), 162-169.
McCormack, B. (2004). Person‐centredness in gerontological nursing: an overview of the literature. Journal of Clinical Nursing, 13(1), 31-38.
McKee, M. (2004). Reducing hospital beds: what are the lessons to be learned? (Vol. 6): WHO Regional Office for Europe.
Meijers, J.M.M., Halfens, R.J.G., van Bokhorst-de van der Schueren, M.A.E., Dassen, T., & Schols, J.M.G.A. (2009). Malnutrition in Dutch health care: Prevalence, prevention, treatment, and quality indicators. Nutrition, 25(5), 512-519.
Meinow, B., Kåreholt, I., & Lagergren, M. (2005). According to need? Predicting the amount of municipal home help allocated to elderly recipients in an urban area of Sweden. Health & Social Care in the Community, 13(4), 366-377.
Meiselman, H.L. (2008). Dimensions of the meal. Journal of Foodservice, 19(1), 13-21.
Menne, H.L., Johnson, J.D., Whitlatch, C.J., & Schwartz, S.M. (2012). Activity Preferences of Persons With Dementia. Activities, Adaptation & Aging, 36(3), 195-213.
Ministry of Health and Social Affairs (1982:763). The health and medical service act.
Ministry of Health and Social Affairs (2001:453). The Social Services Act. Ministry of Health and Social Affairs (2003:91). Äldrepolitik för framtiden.
100 steg till trygghet och utveckling med en åldrande befolkning [Swedish]. Retrieved from http://www.regeringen.se/sb/d/108/a/2611.
Moore, T.F., & Hollett, J. (2003). Giving voice to persons living with dementia: The researcher’s opportunities and challenges. Nursing Science Quarterly, 16(2), 163-167.
75
Munnichs, J.M.A. (1976). Dependency, interdependency and autonomy: an introduction. In J.M.A. Munnichs, & van den Heuvel, W.J.A. (Eds.) Dependency or interdependency in old age (pp.3-8). The Hague: Nijhoff.
Mäkälä, J. (2000). Cultural definitions of the meal. In H.L. Meiselman (Ed.), Dimensions of the meal: the science, culture, business, and art of eating (pp. 7-18). Gaithersburg: Aspen Publishers.
National Board of Health and Welfare. (2005). Boende och vårdinsatser för personer med demenssjukdom [Swedish]. Retrieved from http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/10107/2005-123-5_20051235.pdf
National Board of Health and Welfare. (2006a). God vård – om ledningssystem för kvalitet och patientsäkerhet i hälso- och sjukvården [Swedish]. Retrieved from http://www.socialstyrelsen.se /lists/artikelkatalog/attachments/9406/2006-101-2_20061012.pdf
National Board of Health and Welfare. (2006b). Äldre: vård och omsorg år 2005. Kommunala insatser enligt socialtjänstlagen samt hälso- och sjukvårdslagen. [Swedish]. Retrieved from http://www.socialstyrelsen .se/publikationer2006/2006-44-3
National Board of Health and Welfare. (2010). Nationella riktlinjer för vård och omsorg vid demenssjukdom 2010 – stöd för styrning och ledning [Swedish]. Retrieved from http://www.socialstyrelsen.se /Lists /Artikelkatalog /Attachments/18012/2010-5-1.pdf.
National Board of Health and Welfare. (2012). Äldre – vård och omsorg den 1 april 2012. Kommunala insatser enligt socialtjänstlagen samt hälso- och sjukvårdslagen [Swedish]. Retrieved from http://www.Social styrelsen.se/ Lists/Artikelkatalog/Attachments/18862/2012-10-19.pdf
Nightingale, F. (1992). Notes on nursing: What it is and what it is not. Philadelphia: Lippincott.
Nolan, M.R., Davies, S., Brown, J., Keady, J., & Nolan, J. (2004). Beyond ‘person‐centred’ care: a new vision for gerontological nursing. Journal of Clinical Nursing, 13(1), 45-53.
Nordberg, G., Von Strauss, E., Kåreholt, I., Johansson, L., & Wimo, A. (2005). The amount of informal and formal care among non‐demented and demented elderly persons—results from a Swedish population‐based study. International Journal of Geriatric Psychiatry, 20(9), 862-871.
Northern Nurses´ Federation. (2003). Ethical guidelines for nursing research in the Nordic Countries. Vård i Norden, 4(70), 1-19.
Nygård, L. (2004). Responses of persons with dementia to challenges in daily activities: a synthesis of findings from empirical studies. The American Journal of Occupational Therapy, 58(4), 435-445.

76
O'Malley, L., & Croucher, K. (2005). Housing and dementia care–a scoping review of the literature. Health and Social Care in the Community, 13(6), 570-577.
Oltersdorf, U., Schlettwein-Gsell, D., & Winkler, G. (1999). Assessing eating patterns - An emerging research topic in nutritional sciences: Introduction to the symposium. Appetite, 32(1), 1-7.
Ostwald, S.K., Duggleby, W., & Hepburn, K.W. (2002). The stress of dementia: view from the inside. American Journal of Alzheimer's Disease and Other Dementias, 17(5), 303-312.
Pajalic, Z., Persson, L., Westergren, A., Berggren, V., & Skovdahl, K. (2012). The experiences of elderly people living at home related to their receiving meals distributed by a municipality in Sweden. Journal of Food Research, 1(1), 68-78.
Pajalic, Z., Persson, L., Westergren, A., & Skovdahl, K. (2012). Public home care professionals’ experiences of being involved in food distribution to home-living elderly people in Sweden: a qualitative study with an action research approach. Journal of Nursing Education and Practice, 2(2), 41-51.
Persenius, M.W., Hall‐Lord, M.L., Bååth, C., & Larsson, B.W. (2008). Assessment and documentation of patients’ nutritional status: perceptions of registered nurses and their chief nurses. Journal of Clinical Nursing, 17(16), 2125-2136.
Persson, M., & Zingmark, K. (2006). Living with a person with Alzheimer's disease: Experiences related to everyday occupations. Scandinavian Journal of Occupational Therapy, 13(4), 221-228.
Phinney, A., Chaudhury, H., & O’Connor, D.L. (2007). Doing as much as I can do: The meaning of activity for people with dementia. Aging and Mental Health, 11(4), 384-393.
Pirlich, M., & Lochs, H. (2001). Nutrition in the elderly. Best Practice & Research Clinical Gastroenterology, 15(6), 869-884.
Polit, D.F., & Beck, C.T. (2012). Nursing research: generating and assessing evidence for nursing practice (9 ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
Porter, E.J. (2007). Problems with preparing food reported by frail older women living alone at home. Advances in Nursing Science, 30(2), 159-174.
Roqué, M., Salva, A., & Vellas, B. (2013). Malnutrition in community-dwelling adults with dementia (Nutrialz trial). The Journal of Nutrition, Health & Aging, 17(4), 295-299.
Russel, R. (2007). The Work of Elderly Men Caregivers: From Public Careers to an Unseen World. Men and Masculinities, 9(3), 298-314.
Sandelowski, M. (1998). Writing a good read: Strategies for re-presenting qualitative data. Research in Nursing & Health, 21(4), 375-382.

77
Sanders, S., & Power, J. (2009). Roles, responsibilities, and relationships among older husbands caring for wives with progressive dementia and other chronic conditions. Health and Social Work, 34(1), 41-51.
Secher, M., Soto, M.E., Villars, H., van Kan, G.A., & Vellas, B. (2007). The Mini Nutritional Assessment (MNA) after 20 years of research and clinical practice. Reviews in Clinical Gerontology, 17(4), 293-310.
Senior Alert (2013) [Swedish] Retrieved from http://www.lj.se/senioralert Sennett, R. (2004). Respect: the formation of character in an age of
inequality. London: Penguin. Sidenvall, B., Nydahl, M., & Fjellström, C. (2001). Managing food shopping
and cooking: the experiences of older Swedish women. Ageing and Society, 21 (02), 151-168.
Simmons, S.F., Johansson, B., Zarit, S.H., Ljungqvist, O., Plomin, R., & McClearn, G.E. (1997). Selection Bias in Samples of Older Twins? Journal of Aging and Health, 9(4), 553-567.
Skipper, A. (2012). Agreement on Defining Malnutrition. Journal of Parenteral and Enteral Nutrition, 36(3), 261-262.
Slater, L. (2006). Person-centredness: a concept analysis. Contemporary Nurse, 23(1), 135-144.
Slaughter, S., Cole, D., Jennings, E., & Reimer, M.A. . (2007). Consent and Assent to Participate in Research from People with Dementia. Nursing Ethics, 14(1), 27-40.
Sobal, J. (2000). Sociability and meals: facilitation, commensality, and interaction. In H. Meilselman (Ed.), Dimensions of the Meal The Science, Culture, Business, and Art of Eating (pp. 119-133). Gaithersburg: Aspen Publishers.
Spradley, J.P. (1979). The etnographic interview. Orlando, Florida: Harcourt Brace Jovanovich College Publishers.
Steeman, E., de Casterlé, B.D., Godderis, J., & Grypdonck, M. (2006). Living with early-stage dementia: a review of qualitative studies. Journal of Advanced Nursing, 54(6), 722-738.
Steeman, E., Godderis, J., Grypdonck, M., De Bal, N., & De Casterlé, B.D. (2007). Living with dementia from the perspective of older people: Is it a positive story? Aging & mental health, 11(2), 119-130.
Sundström, G., & Johansson, L. (2005). The changing balance of government and family in care for the elderly in Sweden and other European countries. Australasian Journal on Ageing, 24(s1), S5-S11.
Swedish Council on Technology Assessment in Health Care. (2008). Dementia – Etiology and Epidemiology. A Systematic Review. Retrieved from http://www.sbu.se/upload/Publikationer /Content1/ 1/Dementia_vol1.pdf
Swedish Society of Nursing. (2013). Kunskapsluckor inom omvårdnad - en första inventering [Swedish]. Stockholm: Swedish Society of Nursing.

78
Sydner, Y.M., Sidenvall, B., Fjellstrom, C., Raats, M., & Lumbers, M. (2007). Food habits and foodwork: the life course perspective of senior Europeans. Food, Culture and Society: An International Journal of Multidisciplinary Research, 10(3), 367-387.
Söderhamn, U., Christensson, L., Idvall, E., Johansson, A., & Bachrach‐Lindström, M. (2012). Factors associated with nutritional risk in 75‐year‐old community living people. International Journal of Older People Nursing, 7(1), 3-10.
Takkinen, S., Gold, C., Pedersen, N.L., Malmberg, B., Nilsson, S., & Rovine, M. (2004). Gender differences in depression: a study of older unlike-sex twins. Aging & Mental Health, 8, 187-195.
Tamaru, A., McColl, M.A., & Yamasaki, S. (2007). Understanding 'Independence': Perspectives of occupational therapists. Disability & Rehabilitation, 29(13), 1021-1033.
Tanner, B., Tilse, C., & De Jonge, D. (2008). Restoring and sustaining home: The impact of home modifications on the meaning of home for older people. Journal of Housing for the Elderly, 22(3), 195-215.
Thorne, B.M. (2003). Statistics for the behavioral sciences (4 ed.). New York: McGraw-Hill Higher Education.
Thorslund, M., Bergmark, Å., & Parker, MG. (1997). Difficult decisions on care and services for elderly people: the dilemma of setting priorities in the welfare state. Scandinavian Journal of Social Welfare, 6(3),197-206.
Tombaugh, T.N., & McIntyre, N.J. (1992). The mini-mental state examination: a comprehensive review. Journal of the American Geriatrics Society. 40(9), 922-935.
Trydegård, G.B. (2000). Tradition, change and variation: past and present trends in public old-age care. (Dissertation), Stockholm university, Stockholm.
Walters, A.H., Oyebode, J.R., & Riley, G.A. (2010). The dynamics of continuity and discontinuity for women caring for a spouse with dementia. Dementia, 9(2), 169-189.
van den Heuvel, W.J.A. (1976). The meaning of dependency. In J.M.A. Munnichs, & van den Heuvel, W.J.A. (Eds.) Dependency or interdependency in old age (pp. 162-173). The Hague: Nijhoff.
van Hoof, J., Kort, H.S.M., van Waarde, H., & Blom, M.M. (2010). Environmental interventions and the design of homes for older adults with dementia: an overview. American Journal of Alzheimer's Disease and Other Dementias, 25(3), 202-232.
Watson, Roger. (2011). Editorial: Nutrition and older people with dementia. Journal of Clinical Nursing, 20(3‐4), 303-304.
Vellas, B., Guigoz, Y., Garry, P.J., Nourhashemi, F., Bennahum, D., Lauque, S., & Albarede, J-L. (1999). The Mini Nutritional Assessmant (MNA)

79
and Its Use in Grading the Nutritional State of Elderly Patients. Nutrition, 15(2), 116-122.
Wikby, K., Ek, A.C., & Christensson, L. (2009). Implementation of a nutritional programme in elderly people admitted to resident homes. Scandinavian journal of Caring Sciences, 23(3), 421-430.
Wilkin, D. (1987). Conceptual problems in dependency research. Social Science & Medicine, 24(10), 867-873.
Wilkinson, H. (2001). Including people with dementia in research. Methods and motivations. In H. Wilkinson (Ed.), The perspective of People with Dementia. Research Methods and Motivations (pp. 2-24). London: Jessica Kingsley Publishers.
Wolcott, H.F. (1994). Transforming qualitative data; description, analysis, and interpretation. Thousand Oaks: Sage Publications.
Wolcott, H.F. (2008). Ethnography: A way of seeing (2nd ed.). Lanham: AltaMira Press.
von Kutzleben, M., Schmid, W., Halek, M., Holle, B., & Bartholomeyczik, S. (2012). Community-dwelling persons with dementia: What do they need? What do they demand? What do they do? A systematic review on the subjective experiences of persons with dementia. Aging & Mental Health, 16(3), 378-390.
World Health Organization [WHO]. (2012). Dementia. Fact sheet N°362. Retrieved from http://www.who.int/mediacentre/factsheets/fs362/en/
World Health Organization [WHO]. (2013). Health Topics - Nutrition. Retrieved from http://www.who.int/topics/nutrition/en/
World Health Organization [WHO] and Alzheimer’s Disease International. (2012). Dementia- a public health priority. Retrieved from http://whqlibdoc.who.int/publications/2012/9789241564458_eng.pdf
World Medical Association [WMA]. (2008). WMA Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects. Retrieved from www.wma.net/en/30publications/ 10policies /b3/17c.pdf
Ödlund Olin, A., Koochek, A., Ljungqvist, O., & Cederholm, T. (2005). Nutritional status, well-being and functional ability in frail elderly service flat residents. European Journal of Clinical Nutrition, 59(2), 263-270.
Öhlén, J., Bengtsson, J., Skott, C., & Segesten, K. (2002). Being in a lived retreat-embodied meaning of alleviated suffering. Cancer Nursing, 25(4), 318-325.
Öhman, A., Josephsson, S., & Nygård, L. (2008). Awareness through interaction in everyday occupations: experiences of people with Alzheimer's disease. Scandinavian Journal of Occupational Therapy, 15(1), 43-51.

80
Öresland, S., Määttä, S., Norberg, A., Jörgensen, M.W., & Lützén, K. (2008). Nurses as guests or professionals in home health care. Nursing Ethics, 15(3), 371-383.

Appendices 1-2
Appendix 1: Questions Paper I The Questions Responses Dichotomized
variables Variable names in Paper I
MNA items that have been dichotomized:
Har Du ätit mindre de senaste 2-3 månaderna p.g.a. försämrad aptit, matsmältningsproblem, tugg- eller sväljsvårigheter?
Ja, minskat avsevärt (0) Ja, minskat något (1) Nej, ingen förändring (2)
0+1=minskat matintag 2=ingen förändring
Declined food intake over the past 3 months
(Om minskning) Hur mycket har du gått ner de senaste 2-3 månaderna?
Mer än tre kilo (0) Vej ej (1) Mer än ett mindre än tre kilo (2) Nej, ingen viktförlust (3)
0-2= Viktminskning 3= ingen viktminskning
Weight loss during the past 3 months
Intar mer än tre ordinerade läkemedel dagligen?
Ja (0) Nej (1)
0=Ja 1=Nej
Takes more than 3 prescribed drugs per day
Har trycksår eller hudsår
Nej (0) Ja (1)
0=Nej 1=Ja
Pressure sores or skin ulcer

Äter eller dricker du vanligtvis
Minst en mejeriprodukt dagligen (mjölk/ost/yoghurt) Ja (1), Nej (0) Två eller fler ägg per vecka. Ja (1) Nej (0) Fisk, fågel eller kött varje vecka. Ja (1) Nej (0)
Noll eller ett ja svar=lågt intag av protein Två eller tre ja-svar= tillräckligt proteinintag
Small amount of protein intake
Äter du själv utan problem?
Behöver mycket hjälp/matas (0) Behöver lite hjälp (1) Äter själv utan problem (2)
0+1=behöver hjälp 2=äter självständigt
More or less assistance during meals
Äter du minst två frukter eller två portioner med grönsaker dagligen?
Ja (1) Nej (0)
0=Nej 1=Ja
Consumes less than 2 servings of fruits or vegetables per day
Hur mycket dricker du dagligen? (vatten/jouice/kaffe/te/mjölk/öl)
Mindre än tre glas/muggar (0) 3-5 glas/muggar (1) Mer än 5 glas/muggar (2)
0+1=för litet intag 2=tillräckligt intag
Doesn’t meet fluid requirement
Tycker du att du får i dig den mat du behöver?
Svårt undernärd (0) Osäker om näringstillståndet (1) Har inga näringsproblem (2)
0+1= har näringsproblem 2=har inga näringsproblem
Views self as being malnourished or uncertain about nutritional status

Questions asked about aspects that might have an impact on nutritional status: Hur bedömer du din hälsa jämför med för fyra år sedan?*
Bättre (1) Ungefär likadant (2) Sämre(3)
1+2= bra 3=sämre
Health poorer compared with 4 years ago
Har du under de senaste två månaderna varit inlagd på sjukhus (akutvård/rehab)*
Nej (0) Ja (antalet tillfällen)
0=nej 1=ja
Hospital stay during the past 2 months
Har du under de senaste två månaderna besökt/haft besök av läkare (exkl. sjukhusvård)
Nej (0) Ja (antalet tillfällen)
0=nej 1=ja
Contact with physicians during the past 2 months
Får du någon hjälp i hemmet?
Ja (1) Nej (0)
1=ja 0=Nej
Municipal home-help service
Hemsänd mat Nej (0) Sällan (1) 1 gång/månad (2) 1 gång/14 dag (3) 1 gång/vecka (4) Flera gånger/vecka (5) Dagligen (6)
0=Nej 1-6=Ja
Meals-on-wheels
Färdtjänst Nej (0) Sällan (1) 1 gång/månad (2) 1 gång/14 dag (3) 1 gång/vecka (4) Flera gånger/vecka (5) Dagligen (6)
0=Nej 1-6=Ja
Special transport services

Tycker du att du har några problem med minnet som försvårar det dagliga livet?*
Nej, inte alls (1) Nej, knappast (2) Svårt att ta direkt ställning till (3) Ja, viss utsträckning (4) Ja, i hög grad (5)
1+2= Nej 3-5=Ja
Memory impairment affecting ADL (called MemoryDL in the thesis)
ADL-funktion: Summerad skattning
Totalt nedsatt ADL-kapacitet. Behöver hjälp dygnet runt. (1) Starkt nedsatt ADL-kapacitet. Behöver hjälp varje dag men inte nödvändigtvis hela dagen eller natten med många av sysslorna. (2) Måttligt nedsatt ADL-kapacitet. Kräver regelbunden hjälp med åtminstone 4 stycken sysslor men klarar någon enstaka utan hjälp, eller behöver regelbundet hjälp med matlagning (3) Lätt nedsatt ADL-kapacitet. Kan klara alla utom 1-3 av de dagliga sysslorna. Hjälp krävs för 1-3 sysslor, dock ej dagligen. Kan klara en dag utan hjälp. Klarar att laga sin egen mat. (4) God ADL-kapacitet. Kan utföra alla dagliga sysslor utan hjälp. (5) Utomordentlig ADL-kapacitet. Kan utföra alla dagliga sysslor lätt utan hjälp. (6)
1-4=nedsatt ADL-kapacitet 5-6= God ADL-kapacitet
Reduced ADL function
_____________________________________________________________
Questions marked with * are included in the thesis

Appendix 2: Interview guides
Interview guide: person with dementia (Paper II)
Opening question: Can you please tell me what you have eaten today? Or: What do you think is really good food? Areas:
Shopping Cooking Eating Meal environment
Interview guide: partner (Paper III)
Opening question: Can you please tell me what your food and meals look like; what have you eaten today? Areas:
Shopping Cooking Eating Meal environment Highlight/problem situations

School of Health Sciences Dissertation Series
1. Linddahl, Iréne. (2007). Validity and Reliability of the Instrument DOA; A Dialogue about Working Ability. Licentiate Thesis. School of Health Sciences Dissertation Series No 1. ISBN 978-91-85835-00-3 2. Widäng, Ingrid. (2007). Patients’ Conceptions of Integrity within Health Care Illuminated from a Gender and a Personal Space Boundary Perspective. Licentiate Thesis. School of Health Sciences Dissertation Series No 2. ISBN 978-91-85835-01-0 3. Ernsth Bravell, Marie. (2007). Care Trajectories in the oldest old. Doctoral Thesis. School of Health Sciences Dissertation Series No 3. ISBN 978-91-85835-02-7 4. Almborg, Ann-Helene. (2008). Perceived Participation in Discharge Planning and Health Related Quality of Life after Stroke. Doctoral Thesis. School of Health Sciences Dissertation Series No 4. ISBN 978-91-85835-03-4 5. Rosengren, Kristina. (2008). En hälso- och sjukvårdsorganisation i förändring – från distanserat till delat ledarskap. Doctoral Thesis. School of Health Sciences Dissertation Series No 5. ISBN 978-91-85835-04-1 6. Wallin, Anne-Marie. (2009). Living with diabetes within the framework of Swedish primary health care: Somalian and professional perspectives. Doctoral Thesis. School of Health Sciences Dissertation Series No 6. ISBN 978-91-85835-05-8 7. Dahl, Anna. (2009). Body Mass Index, Cognitive Ability, and Dementia: Prospective Associations and Methodological Issues in Late Life. Doctoral Thesis. School of Health Sciences Dissertation Series No 7. ISBN 978-91-85835-06-5 8. Einarson, Susanne. (2009). Oral health-related quality of life in an adult population. Licentiate Thesis. School of Health Sciences Dissertation Series No 8. ISBN 978-91-85835-07-2 9. Harnett, Tove. (2010). The Trivial Matters. Everyday power in Swedish elder care. Doctoral Thesis. School of Health Sciences Dissertation Series No 9. ISBN 978-91-85835-08-9 10. Josefsson, Eva. (2010). Immigrant background and orthodontic treatment need - Quantitative and qualitative studies in Swedish adolescents. Doctoral Thesis. School of Health Sciences Dissertation Series No 10. ISBN 978-91-85835-09-6 11. Lindmark, Ulrika. (2010). Oral Health and Sense of Coherence - Health Behaviours, Knowledge, Attitudes and Clinical Status. Doctoral Thesis. School of Health Sciences Dissertation Series No 11. ISBN 978-91-85835-10-2

12. Pihl, Emma. (2010). The Couples’ Experiences of Patients’ Physical Limitation in Daily Life Activities and Effects of Physical Exercise in Primary Care when having Chronic Heart Failure. Doctoral Thesis. School of Health Sciences Dissertation Series No 12. ISBN 978-91-85835-11-9 13. Nilsson, Stefan. (2010). Procedural and postoperative pain management in children - experiences, assessments and possibilities to reduce pain, distress and anxiety. Doctoral Thesis. School of Health Sciences Dissertation Series No 13. ISBN 978-91-85835-12-6 14. Algurén, Beatrix. (2010). Functioning after stroke - An application of the International Classification of Functioning, Disability and Health (ICF). Doctoral Thesis. School of Health Sciences Dissertation Series No 14. ISBN 978-91-85835-13-3 15. Kvarnström, Susanne. (2011). Collaboration in Health and Social Care - Service User Participation and Teamwork in Interprofessional Clinical Microsystems. Doctoral Thesis. School of Health Sciences Dissertation Series No 15. ISBN 978-91-85835-14-0 16. Ljusegren, Gunilla. (2011). Nurses’ competence in pain management in children. Licentiate Thesis. School of Health Sciences Dissertation Series No 16. ISBN 978-91-85835-15-7 17. Arvidsson, Susann. (2011). Health promoting factors in people with chronic musculoskeletal pain or with rheumatic diseases: a descriptive and interventional study. Doctoral Thesis. School of Health Sciences Dissertation Series No 17. ISBN 978-91-85835-16-4 18. Berggren, Elisabeth. (2011) Identity construction and memory after Subarachnoid Haemorrhage - Patients’ accounts and relatives’ and patients’ statements in relation to memory tests. Licentiate Thesis. School of Health Sciences Dissertation Series No 18. ISBN 978-91-85835-17-1 19. Ericsson, Iréne. (2011) Välbefinnande och demens - Aspekter på välbefinnande hos äldre personer med måttlig till svår demenssjukdom. Doctoral Thesis. School of Health Sciences Dissertation Series No 19. ISBN 978-91-85835-18-8 20. Silén, Marit. (2011) Encountering ethical problems and moral distress as a nurse - Experiences, contributing factors and handling. Doctoral Thesis. School of Health Sciences Dissertation Series No 20. ISBN 978-91-85835-19-5 21. Munck, Berit. (2011) Medical technology and its impact on palliative home care as a secure base experienced by patients, next-of-kin and district nurses. Doctoral Thesis. School of Health Sciences Dissertation Series No 21. ISBN 978-91-85835-20-1
22. Jacobsson, Brittmarie. (2011) On Oral Health in Young Individuals with Foreign and Swedish Backgrounds. Licentiate Thesis. School of Health Sciences Dissertation Series No 22. ISBN 978-91-85835-21-8 23. Bergsten, Ulrika. (2011) Patients’ and healthcare providers’ experiences of the cause, management and interaction in the care of rheumatoid arthritis. Doctoral Thesis. School of Health Sciences Dissertation Series No 23. ISBN 978-91-85835-22-5 24. Wilińska, Monika. (2012) Spaces of (non-)ageing - A discursive study of inequalities we live by. Doctoral Thesis. School of Health Sciences Dissertation Series No 24. ISBN 978-91-85835-23-2 25. Wagman, Petra. (2012) Conceptualizing life balance from an empirical and occupational therapy perspective. Doctoral Thesis. School of Health Sciences Dissertation Series No 25. ISBN 978-91-85835-24-9 26. Golsäter, Marie. (2012) Hälsosamtal som metod att främja barns och ungdomars hälsa – en utmanande uppgift. Doctoral Thesis. School of Health Sciences Dissertation Series No 26. ISBN 978-91-85835-25-6 27. Celsing Fåhraeus, Christina. (2012) Övervikt/fetma hos barn, ungdomar och unga vuxna i relation till vikt, viktutveckling och kariesförekomst. Licentiate Thesis. School of Health Sciences Dissertation Series No 27. ISBN 978-91-85835-26-3 28. Åhnby, Ulla. (2012) Att möjliggöra äldre människors delaktighet i vardagen - Framtidsverkstad som idé och metod. Licentiate Thesis. School of Health Sciences Dissertation Series No 28. ISBN 978-91-85835-27-0 29. Ståhl, Ylva. (2012) Documentation in Child and School Health Services Mapping health information from a biopsychosocial perspective using the ICF-CY. Doctoral Thesis. School of Health Sciences Dissertation Series No 29. ISBN 978-91-85835-28-7 30. Åkerman, Eva. (2012) Assessment and tools for follow up of patients’ recovery after intensive care. Doctoral Thesis. School of Health Sciences Dissertation Series No 30. ISBN 978-91-85835-29-4 31. Pietilä, Sirpa. (2012) Tvillingskap genom livet - individualitet och relation i äldre tvillingars livsberättelser. Doctoral Thesis. School of Health Sciences Dissertation Series No 31. ISBN 978-91-85835-30-0 32. Gimbler Berglund, Ingalill. (2012) Nurse anaesthetist’s interactions and assessment of children’s anxiety. Licentiate Thesis. School of Health Sciences Dissertation Series No 32. ISBN 978-91-85835-31-7

33. Fristedt, Sofi. (2012) Occupational participation through community mobility among older men and women. Doctoral Thesis. School of Health Sciences Dissertation Series No 33. ISBN 978-91-85835-32-4 34. Andersson, Bodil. (2012) Radiographers’ Professional Competence - Development of a context-specific instrument. Doctoral Thesis. School of Health Sciences Dissertation Series No 34. ISBN 978-91-85835-33-1 35. Siouta, Eleni. (2012) Communication Patterns in Consultations Between Patients with Atrial Fibrillation and Health Professionals. Licentiate Thesis. School of Health Sciences Dissertation Series No 35. ISBN 978-91-85835-34-8 36. Selander, Helena. (2012) Driving assessment and driving behavior. Doctoral Thesis. School of Health Sciences Dissertation Series No 36. ISBN 978-91-85835-35-5 37. Sjölander, Catarina. (2012) Consequences for family members of being informal caregivers to a person with advanced cancer. Doctoral Thesis. School of Health Sciences Dissertation Series No 37. ISBN 978-91-85835-36-2 38. Anastassaki Köhler, Alkisti. (2012) On temporomandibular disorders – Time trends, associated factors, treatment need and treatment outcome. Doctoral Thesis. School of Health Sciences Dissertation Series No 38. ISBN 978-91-85835-37-9 39. Berggren, Elisabeth. (2012) Daily life after Subarachnoid Haemorrhage – Identity construction, patients’ and relatives’ statements about patients’ memory, emotional status and activities of living. Doctoral Thesis. School of Health Sciences Dissertation Series No 39. ISBN 978-91-85835-38-6 40. Sigurðardóttir, Sigurveig H. (2013) Patterns of care and support in old age. Doctoral Thesis. School of Health Sciences Dissertation Series No 40. ISBN 978-91-85835-39-3 41. Larsson, Ingrid. (2013) Person-centred care in rheumatology nursing for patients undergoing biological therapy: an explorative and interventional study. Doctoral Thesis. School of Health Sciences Dissertation Series No 41. ISBN 978-91-85835-40-9 42. Josephson, Iréne (2013) Utrymme för deltagande. Beslutsprocesser i möten mellan patienter med ospecifika ländryggsbesvär och sjukgymnaster i primärvård. Doctoral Thesis. School of Health Sciences Dissertation Series No 42. ISBN 978-91-85835-41-6 43. Strand, Anne-Sofie (2013) Truancy from student and school perspectives. An interview and document study. Doctoral Thesis. School of Health Sciences Dissertation Series No 43. ISBN 978-91-85835-42-3

44. Nygårdh, Annette (2013) A quality improvement project on empowerment in chronic kidney care – an interactive research approach. Doctoral Thesis. School of Health Sciences Dissertation Series No 44. ISBN 978-91-85835-43-0 45. Johansson, Linda (2013) Foodwork and meals in everyday life among persons with dementia and their partners. Doctoral Thesis. School of Health Sciences Dissertation Series No 45. ISBN 978-91-85835-44-7