Embed Size (px)
Citation preview

Global perspective
Prevalence of overweight and obesity (weight-for-height ≥ 2SD) among children under age 5 years, 2014, WHO

Life-course perspective – women’s health

1850 1900 1950 2000 2050 2100
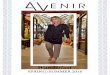
104.5
119.8
89.1 96.8
108.9
98.1
time series
forecast mean
95% approx.conf. interval
time series
forecast mean
95% approx.conf. interval
120
110
100
90
80
70
60
50
40
Forecast of record life expectancy
Source: Vaupel
In 2015: Japan 84 (Men 80, women 87)

Top global causes of death
WHO 2015
Causes of death Deaths in Millions
CHD 8.9
Stroke 6.3
COPD 3.2
Low resp. infections 2.7
Lung cancers 1.7

Non-communicable diseasesInfectious diseases
LE=30 ys LE=50 ys LE=70 ys
Demographic & Epidemiologic Transition

Top global causes of death
WHO 2015
Causes of death Deaths in Millions
CHD 8.9
Stroke 6.3
COPD 3.2
Low resp. infections 2.7
Lung cancers 1.7
Top risk factors?

Global risk factors

Malnutrition?

Malnutrition
Malnutrition = inadequate/unbalanced nutrition
• Undernutrition
• Protein-energy malnutrition
• Micronutrient deficiencies
• Overnutrition

Overweight/obesity
2.1 billion adults
~a third of the world population
Marie Ng, et al. Lancet, 2014

Obesity – a worldwide problem
• Overweight and obesity are linked to more deaths worldwide than underweight
Prevalence of overweight and obesity, GBD, 2013

Childhood obesity – a worldwide problem
• 43 million overweight and obese preschoolers (<5 y) in the world
• 35 million live in developing countries
de Onis M, Blossner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr. 2010;92:1257-64.

Consequences of childhood obesity
• In childhood:- Can harm heart, lungs, muscles, bones, kidneys and GI tract- Disturbances in hormones that control blood sugar and puberty- Social and emotional problems
• Risk for later life: overweight children are likely to : - become obese adults, overweight ‘tracks’- develop diabetes and CVD at a younger age

• Developed countries: increases in obesity began in the 1980s; since 2006, the increase has slowed down
• Developing countries: obesity rates continue to rise
Obesity – a worldwide problem – trends
WHO, 2014

World health in transition
• Demographic transition (Warren Thompson, 1929) population ageing
• Epidemiological transition (Abdel Omran, 1971) changes in global disease burden
• Nutrition transition (Barry Popkin, 1993) changes in diet and physical activity

Nutrition transition
The shift in dietary consumption and energy expenditure that coincides with economic, demographic, and epidemiological changes

Pattern 1 – Hunter Gatherer
• Highly active lifestyles• Hunting and foraging for food• Diets rich in fibrous plants and protein from lean wild
animals• Diets low in fat

Pattern 1 – Hunter Gatherer
• Highly active lifestyles• Hunting and foraging for food• Diets rich in fibrous plants and protein from lean wild
animals• Diets low in fat

Pattern 2 – Early Agriculture
• Famine is common• Slowing individuals’ growth• Scarcity • Low variation of the food supply

Pattern 2 – Early Agriculture
• Monoculture: low variation of the food supply• Nutrient deficiencies• Famine is common• Scarcity • Short stature

Pattern 3 – End of Famine
• Famine recedes • Income rises • Nutrition improves: more fruits, vegetables, and animal
protein

Pattern 3 – End of Famine
• Famine recedes • Income rises • Nutrition improves: more fruits, vegetables, and animal
protein

Pattern 4 – Overeating, Obesity-Related Diseases
• Incomes continue to rise• Access to an abundance of high-calorie foods• Diets high in total fat, cholesterol, sugar; and low in
PUFAs and fiber • Increasingly sedentary lifestyle • Increases in obesity • Increase in obesity-related chronic diseases, such as
diabetes and heart disease

Pattern 4 – Overeating, Obesity-Related Diseases
• Incomes continue to rise• Access to an abundance of high-calorie foods• Diets high in total fat, cholesterol, sugar; and low in
PUFAs and fiber • Increasingly sedentary lifestyle • Increases in obesity and related chronic diseases, such as
diabetes and heart disease

Pattern 5 – Behavior Change
• Response to increasing rates of obesity and obesity-related chronic diseases
• Individuals change their behavior• Communities promote behavior changes

Pattern 5 – Behavior Change
• Response to increasing rates of obesity and obesity-related chronic diseases
• Individuals change their behavior• Communities promote behavior changes

Nutrition transition
1. Hunter-gatherer: collecting food, diets high in carbohydrates, low in fat, fat was mainly unsaturated
2. Early agriculture: famine, scarcity, reduced variation of the food supply
3. End of famine: more fruits, vegetables, and animal protein
4. Overeating, obesity-related diseases: diets high in total fat, cholesterol, sugar; and low in PUFAs and fiber; often accompanied by an increasingly sedentary lifestyle
5. Behavior change: to prevent or delay degenerative diseases
Barry Popkin, 1993

Nutrition transition
• Currently, most low- and middle-income countries are rapidly moving from pattern 3 (end of famine) to pattern 4 (processed foods)
Popkin BM. Am J Clin Nutr. 2006; 84:289–98.
Shift from traditional to Western-style diets

Nutrition and epidemiologic transition
• Different stages of transition within:– Countries– Regions– Families– Individuals
Double burden

Double burden in countries
Low-middle income countries battle with:
food insecurity, undernutrition, infectious diseases
AND
obesity, heart disease, hypertension, stroke, and diabetes.
Example: South Africa
• Significant levels of stunting, but declining levels of underweight
• In adults, overweight and obesity are more serious than underweight.
• Rising incidence of CVD, diabetes and cancer, but also of TB and HIV/AIDS.

• Overweight in combination with micronutrient deficiencies (e.g., vitamin A)
• Early-life under nutrition, stunting + adulthood obesity
Double burden within individuals

Double burden within families
• Pregnant women -> children
Risks of undernutrition during pregnancy for the child: LBW, mental retardation, death
But also More NCD later in life (Barker)
Barker, 1995, BMJ

The Dutch Hunger Winter Study
Rooseboom et al. 2001 & 2006
Poor maternal nutrition during pregnancy may lead to increased disease susceptibility in later life
↑ Obesity ↑ Type 2 diabetes↑ Coronary heart disease↑ Kidney disease
Similar effects for overnutrition/ obesity during pregnancy!

Maternal obesity
• The Generation R Study
• Adverse offspring outcomes of maternal obesity during pregnancy:
Fetal outcomes Childhood outcomes Adult outcomes
StillbirthNeonatal deathCongenital anomaliesLGA at birthNeonatal hypoglycemiaReferral to neonatal intensive care unit
ObesityAdverse body compositionHigh blood pressureDyslipidemiaIncreased inflammatory markersImpaired insulin/glucose homoeostasis
ObesityHigh blood pressureDyslipidemiaInsulin resistancePremature mortality

Developmental Origins of Health and Disease (DOHaD)
“The DOHaD concept describes how, during early life
(at conception, and/or during fetal life, infancy, and early childhood),
the environment induces changes in development that have long term
impact on later health and disease risk.”
International Society for Developmental Origins of Health and Disease

Childhood obesity
• 43 million overweight and obese preschoolers (<5 y) in the world• 35 million live in developing countries
• Affects child’s health, quality of life• Tacks to later life
Covered by the MDGs?
de Onis M, Blossner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr. 2010;92:1257-64.

WHO
On Jan 25, 2016, the
Commission on Ending
Childhood Obesity
(ECHO) presented its
report to the Director-
General of WHO

Ending Childhood Obesity (ECHO)

Childhood obesity: global and lifecourse perspective

Gynecologic and ObstetricConsequences of Obesity in
Adolescent Girls:THE FACTS
Leticia Elizondo-Montemayor, M.D.
Director of the Clinical Nutrition and Obesity Research Center.

Introduction
Obesity: most prevalent nutritional problem in children and adolescentsin the US. (Ogden, Carroll, Kit, & al, 2012)
The prevalence of overweight in children and adolescents has increased by more than half, and that of obesity has doubled. (Ogden, Carroll, Kit, & al, 2012)
50 – 77% of obese adolescents will become obese adults. (De Silva, Helmrath, Klish, 2007) (In-Iw, Biro, 2011)
In Mexico, 1 in every 3 children and adolescents is overweight orobese. (Gutierrez, Rivera-Dommarco, Shamah-Levy, & al, 2012)

Obesity rates
OECD estimates based on national health surveys. Leticia Elizondo-Montemayor Tecnológico de Monterrey, México

International Association for theStudy of Obesity, 2013; Bös et al. (2004), Universität Karlsruhe and Ministères de l’Educationnationale et de la Santé forLuxembourg; and KNHANES 2011 for Korea.
Overweight(includingobesity) amongchildrenaged 5-17, 2010 ornearest year

National prevalence of overweight and obesity in infants less than 5 years
old in Mexico, EN88, ENN1999, ENSANUT 2006,
ENSANUT 2012
National prevalence of overweight and obesity in children 5 to 11 years old in Mexico, ENSANUT 2012
National prevalence of overweight and obesity in adolescents of 12-19 years old in Mexico, ENSANUT 2012

Effects of obesity on the life courseof women’s health
Cardiovascular
• Hypertension
• Dyslipidemia
• Atherosclerosis
• Congestive heart failure
• Intima thickening
• Left ventricular hypertrophy
• Peripheral vascular disease
• Pulmonary embolism
Metabolic
• Insulin Resistance
• Glucose Intolerance
• DM type 2
• Metabolic syndrome
• Gout
• Vitamin D deficiency
Pulmonary
• Obstructive sleep spnea
• Hypoventilation syndrome
• Pulmonary hypertension
• Dyspnea
• Asthma exacerbation
Hepatic
• Nonalcoholic fatty liver disease
• Nonalcoholic Steatohepatitis
• Cirrhosis
Genitourinary
• Polycystic ovarian syndrome
• Hyperandrogenism
• Infertility
• Irregular menstruation
• Urinary incontinence
• Impotence
Neurologic
• Embolism
• Idiopatic intracraneal hypertension
• Lower back pain
(Elizondo, Hernández, Zamora, 2011)

Cancer
• Breast
• Colon
• Prostate
• Endometrial
Orthopedic
• Osteoarthritis
• Blount disease
Gastrointestinal
• Cholelitiasis
• GERD
• Hernias
Dermatologic
• Acanthosis nigricans
• Hirsutism
• Stretch marks
• Venous stasis
• Cellulite
• Intertrigo
Renal
• Microalbuminuria
• Terminal renal disease
• Obesity related glomerulopathy
Psychological
• Depression
• Anxiety
• Low self esteem
• Suicide
• Low quality of life
• Years of life lost
Effects of obesity on the life courseof women’s health
(Elizondo, Hernández, Zamora, 2011)

Metabolic and life impact of obesity in girls• Childhood and adolescent adiposity are good predictors of MetS, both in
adolescence and adulthood. (In-Iw, Biro, 2011) (Morrison, Friedman, Wang, & al, 2008)
• Based on the degree of overweight adolescents, younger adults have a tendency to have greater years of life lost than older adults. (De Silva, Helmrath, Klish, 2007)
(Li, Chen, Srinivasan, & al, 2012)(Zeller, Modi, 2006)(Finkelstein, Brown, Wrage, & al, 2010)
Consequences Risk/prevalence
Metabolic Syndrome 27.8% prevalence
Diminished health related quality of life 5.5 times more likely
Years of life lost 5-9 years

Psychological Impact of obesity in adolescence
Low self-esteem
• Twice more likely to have low self-esteem, especially females. (McClure, Tanski, Kingsbury, & al, 2010) (Kelly, Barlow, Rao, & al, 2013)
Depression
• Positive correlation between depressive symptoms and obesity in adolescents, especially the severely obese. (Liem, Sauer, Oldehinkel, & al, 2008) (Anderson, Cohen, Naumova, & al, 2006)
• Depression rates of 30% in severely obese adolescents. (Kelly, Barlow, Rao, & al, 2013) (Zeller, Roehrig, Modi, & al, 2006)
There is also
• Stigmatization
• Altered cognitive performance
• Low self-worth
• Frustration
• Emotional disorders.

Effects of obesity on puberty
Early pubertyHigh BMI was positively correlated with early maturation, starting puberty earlier. (Buyken, Karaolis-Danckert, Remer, 2009) (Wang, 2002)
(Biro, Huang, Morrison, & al, 2010)
Cohort study
10 year length
1,141 girls
9 years of age
Earlier maturation in thosewith higher fat mass,
waist-to-height ratio, ratio of fat mass to fat-free mass
Population based cohort
Danish
135,000
7 year old girls
Large pre-pubertal BMI associated with growth
spurt and peak highvelocity at an earlier age
(Aksglaede, Juul, Olsen, & al, 2009)

Effects of obesity on puberty
Early menarche
(Castillo, Nucci, 2015)
(Lee, Appugliese, Kaciroti, & al, 2007)
Cross-sectional
study
Brazilian
1,671 girls
7-18 years old
Overweight girls presentedwith earlier menarche.
American Longitudinal study
354 girls
36 months
to 12 years old
Larger BMI, as early as 3 yearsold Earlier breast
development and menarche.

Effects of obesity on reproductive function
Risk of infertility
Fertility disorders are stronger when obesity has an early onset during the adolescent years.
(Hartz, Barboriak, Wong, & al, 1979) (Norman, Clark, 1998)
597 anovulatory women VS. 1,695 primiparous controls
Increased risk of infertilitydue to obesity in both groups
3-fold higher risk of infertility
Internet -based prospective cohort study
Danish
Overweight, obese and and women who gained
excess weight since age 17
Reduced fertility
(Grodstein, Goldman, Cramer, 1994) (Wise, Rothman, Mikkelsen, & al, 2010)

Effects of obesity on reproductive function
Obese women submitted to in-vitro fertilization in which exogenous gonadotropins were used:
• Had lower odds of conception than non-obese women. (Gesink, Maclehose, Longnecker, 2007)
• Required longer gonadotropin stimulation and higher amounts than normal weightwomen to produce a similar number of follicles. (Practice Comm of Am- Society for Reprod Medicine, 2008)
Likelihood of clinical pregnancy and live birth with in vitro fertilization were 50% lower in women with BMI over 40. (Shah,
Missmer, Berry, & al, 2011)
Embryos derived from oocytes of obese women are of poorer quality than those from normal-weight women. (Metwally, Cutting, Tripton, & al, 2007)
Influence on assisted reproductive technology (ART)

Disorders of menstruation in adolescets with obesity
Irregular menstruation• Obese women are twice more likely to have irregular
menstruation. (Wei, Schmidt, Dwyer, & al, 2009)
• The same goes for obese adolescents. (Hillman, Miller, Inge, 2011)
(Hillman, Miller, Inge, 2011)
American Cohortstudy
25 severelyobese
adolescents(BMI 51.4)
bariatric surgery
Mean age 17.4 years
High prevalenceof irregular
mensescycles
28% Menorrhagia
32% Oligomenorrhea

Disorders of menstruation in adolescents with obesity
Irregular menstruation
• Oligomenorrhea
• irregular menstrual bleeding
• Amenorrhea
• heavy menstrual bleeding. (Seif, Diamond, Nickkho-Amiry, 2015)
Cross-sectional
Serbian
835 post-menarcheal
girls
Irregular cycles: higher weight, BMI, fat percentage and
larger ovaries.
Predisposingfactor for
polycystic ovarysyndrome.
Prospectivepopulation-
based
Finnish
2,033 subjects
Menstrual irregularity and/orelevated androgenlevels at 16 years.
Associated withsymptoms of PCOS
and infertilityproblems at age 26.
(Radivojevic, Lazovic, Kravic-stevovic, & al, 2014)
(West, Lashen, Bloigu, & al, 2014)

Dysmenorrhea in adolescents with obesity
Negative correlation
Cross-sectional
study
Turkish
800 students
17-32 years old
Dysmenorrhea 1.5 times higher in underweight people than in
overweight/obese.
Cross-sectional
study
Japanese
2,282 females
18-21 years old
Higher prevalence in the underweightgroup (BMI <19.8).
(Ozerdogan, Sayiner, Ayranci, & al, 2009)(Hirata, Kumabe, Inoue, 2002)
Consider these are UNDERWEIGHT, not normal weight adolescents
The effect of obesity on dysmenorrhea is still CONTROVERSIAL

Dysmenorrhea in adolescents with obesity
No association
Cross-sectional
study
Nigerian
1,399 adolescents
Primarydysmenorrhea 85.4%.
BMI and level of adiposity (based
on WC) werenot associated.
Review
15 longitudinal, case-control,
cross-sectionalstudies
Increased risk High stress, family history of
dysmenorrhea.
InconclusiveObesity, diet,
smoking.
(Maruf, Ezenwafor, Moroof, & al, 2013)(Ju, Jones, Mishra, 2014)

Dysmenorrhea in in adolescents with obesity
Positive correlation
American cohort study
Severely obese adolescents
40% withdysmenorrhea.
Australian Longitudinal Studyon Women’s Health
14, 247 women 18-23 years
13 year follow up
Obesity was more common among
those withdysmenorrhea.
Longitudinal study
Australian
9,688 women
22-27 years old
U- shapedassociation
betweendysmenorrhea and
BMI.
(Hillman, Miller, Inge, 2011)
(Ju, Jones, Mishra, 2014)

Sexual behavior in in adolescents with obesity
Less likely to be sexually active. (Ratcliff, Jenkins, Reiter-Purtill, & al, 2011) (Ali, Rizzo, Amialchuk, & al, 2014)
For each point increase in BMI the probability of having a romanticrelationship decreased by 6%. (Halpem, King, Oslak, & al, 2005)
Higher odds ratio for unsafe sexual behavior:(Leech, Dias, 2012; Ratcliff, Jenkins, Reiter-Purtill, & al, 2011; Chang, Davis, Kusonoki, & al, 2015)
• Unprotected sex.
• Sex under the effects of alcohol or drugs.
• Casual sex.
• Numerous partners.
• Lack of contraceptive use.
One study proved no influence of weight sexual behavior or contraceptive use. (Akers, Lynch, Gold, & al, 2009)

Contraception weight gain in obesity
Fear of weight gain
Use hormonal contraceptives less frequently
Depend on less efective forms or no contraception. (Shaw, Edelman, 2013)
Population-based longitudinal study with 900 teens 18 to 19 years oldproved this. (Chang, Davis, Kusunoki, & al, 2015)
Teens who experience weight gain while taking COC attribute it to theCOC and discontinue their use. (Coney, Washenik, Langley, & al, 2001)
(Gallo, López, Grimes, & al, 2014)
Cochrane reviewNo relationship between COC or a combination skin patch
and weight change.
COC related weight gain in adolescents

Contraception weight gain in obesityCOC related weight gain in adolescents
Adolescents using hormonal inyectable contraceptives gain more weight tan COC users. (Beksinska, Smit, Kleinschmidt, & al, 2010)
Placebo-controlled, randomized
trial
700 adolescentswomen >14
years
Low dose COC (20mg EE/100 mg LNG)
did not cause weight gain, because of the low dose.
Longitudinal study
12- 21 yearsold
Using COC for more
than 1 year.
4.2% increase in weight;
12.5% increase in body fat.
(Coney, Washenik, Langley, & al, 2001)(Bonny, Britto, Huang, & al, 2004)

Contraception weight gain in obesityDMPA related weight gain
• Depotmedroxyprogesterone (DMPA) is more associatedwith weight gain than other hormonal contraceptives.
• Those overweight at the start of DMPA were more likelyto gain weight during the first year of use. (Mangan, Larsen, Hudson, 2002)
(Beksinska, Smit, Kleinschmidt, & al, 2010)
Longitudinal study
15-19 yearsold
Use DMPA orNET-EN
gain 6.2kg compared to
2.3kg with COC.

Contraception Failure in obesityCOC effectiveness
• COC and the patch• higher failure rates in obese adolescents. (Greydanus,2009)
• Progestin Long Acting Reversible Contraceptives (LARC) Etonorgestrel implant and levonorgestrel IUD• Safer and more effective.
Retrospective cohort analysis
18-39 years old
1.6 increased risk of COC failure.
Associated with the highest weightquartile among very low dose COC users (<35mcg ethinyl estradiol).
Case control study
Risk of pregnancy 60% higher in women with BMI >27.3.
>70% higher in BMI >32.2 and weight >74kg.
Doubled with weight > 86kg. (Holt, Scholes, Wicklund, & al, 2005)
(Holt, Cushing-Haugen, Daling, 2002)

Contraception Failure in obesity
Emergency contraception effectiveness
• Overweight and obese women taking LNG were 4 times more likely to get pregnant. (Mody, Han, 2014)
Meta-analysis of 2 randomized
controlled trials
comparing UPA vs LNG
>16 yearsold
Obese women are 3 times as likely to get pregnant as those with normal BMI for either method. (Glasier, Cameron,
Blithe, & al, 2011)
Cohort of Europeanwomen,
using COCswith CMA
Increased BMI and weightassociated with higher
rate of failure.
CMA Lipophilic. (Dinger, Cronin,
Möhner, & al, 2009)

Polycystic Ovary Syndrome in obesityObesity increases the risk of PCOS in adolescents. Odds ratio of being obese or extremely obese was 4.0 for adolescents with diagnosedPCOS. (Christensen, Black, Smith, & al, 2013)
50% of adolescents and adults with PCOS are obese. (Messinis, Messini, Anifandis, & al, 2015) (Azziz, Woods, Reyna, & al, 2004)
Overweight and obesity amplify the severity of PCOS and increase the risk of metabolic alterations. (Franks, 2008)
•Girls aged 14 with a high BMI in childhood increased risk of oligomenorrhea and diagnosis of PCOS in young adulthood. (Glueck, Morrison, Daniels, & al, 2011)
Girls with premature puberty (obese) have been linked to PCOS.

Polycystic Ovary Syndrome in obesity
• Metabolic alterations• Overweight and obese girls with PCOS have a 3-fold
increased risk of developing type 2 diabetes. (O’Brien, Emans, 2008) (Palmert, Gordon, Kartashov, & al, 2002)
• PCOS in obese adolescents is associated with MetS.
Study in obese adolescent females
15.4% Elevatedaminotransferase levels,
suggestive of non-alcoholicsteatohepatitis.
43.6% MetS
10.2% Both. (Barfield, Liu, Kessler, & al, 2009)
Study of severely obese, obese, overweight adolescents
37% girls with PCOS hadMetS.
5% with normal weight
Girls with PCOS were4.5 times more likely to
have MetS. (Coviello, Legro, Dunaif, 2006)

Mineralization and Bone density in adolescents with obesity
Positive or no effect
Correlational study
200 adolescents
and children,
4-20 yearsold.
Obesity during childhood and adolescence Increased vertebral bone density, increased whole bodybone dimensions and mass. (Leonard,
Shults, Wilson, & al, 2004)
865 children and
adolescents
Obese children (% body
fat)
Did not have lower BMC compared with leaner
children. (Petit, Beck, Shults, & al, 2005) (Ellis,
Shypailo, Wong, & al, 2003)

Mineralization and Bone density in adolescents with obesity
Negative effect
Obesity impeds acquisition and promotes loss of bone mass. (Mosca, Silva, Goldberg, 2013)
200 female adolescents
Negative correlationsbetween % body fat
and femur and lumbar spine BMD
Excess fat mass can be detrimental to theattainment of bonemass. (Mosca, Goldberg, da
Silva, & al, 2014)
300 adolescents
3-19 years old
Lower bone mass and bone area for theirtotal body weight.
(Goulding, Taylor, Jones, & al, 2000)
Children and young adults, 4-20 years old.
Proximal femur bonestrength in overweight wasadapted to lean mass and
height. Bone strengthadjusts to muscle forces
Fat mass did not havea positive influenceon bone strength
(static load). (Petit, Beck,
Shults, & al, 2005)
In obese teens, as thenumber of cardio-metabolic risk factorsincreased, their BMD decreased. (Pollock, Bernard, Gutin, & al, 2011)

Macromastia in adolescents withobesityAdolescent girls with macromastia
• Overweight 35%
• Obese 35% (Cruz-Korchin,
Korchin, González-Keelan, & al, 2001)
Most frequent complaints
• back pain, shoulder pain, and intertrigo.
• shoulder grooving from bra straps, upper extremity parestesias, headaches and thoracic kyphosis. (Wolfswinkel, Lemaine, Weathers, 2013)
Adolescents <21 withmacromastia reported
• lower HRQOF
• lower self-esteem
• more eating disorders(Cerrato, Webb, Rosen, & al, 2012)
The demand for breastreduction among
adolescent girls has recently increased.
(Larson, Gosain, 2012)

Breast Cancer in obesity
A greater BMI contributes to increasing incidence of breast cancer. (Gewefel, Salhia, 2014) (Porter, 2008)
Birth weight impacts the risk and progression of breast cancer.
• Women born >4kg 2-fold higher risk than those <3kg. (dos Santos, de Stavola, Hard, & al, 2004) (Perks, Holly, 2011)
Adult obese women have increased risk for postmenopausal breast cancerbut not premenopausal. (Neuhoser, Aragaki, Prentice, & al, 2015)
Obese women with a family history of breast cancer have an increased risk of developing postmenopausal breast cancer. (Carpenter, Ross, Paganini-Hill, & al, 2003)
Increased risk

Breast cancer in obesity
Premenopausal breast cancer exhibits an inverse associationwith BMI and body fat in childhood and adolescence. (Harris,
Tamimi, Willett, & al, 2011) (Michels, Terry, Willett, 2006)
Early life adiposity had a protective effect whencorrelating body fatness at young ages and risk of breast cancer. (Baer, Tworoger, Hankinson, & al, 2010)
Once a woman has developed breast cancer, beingoverweight or obese has adverse consequences. (Perks, Holly, 2011)
Decreased risk

Endometrial cancer in obesity5% of endometrial cancer is diagnosed in women
younger than 40 years old. (Creasman, 2014) (Madison, Schottenfeld,
James, & al, 2004)
Earlier onset of puberty and sexual development in obese adolescents is associated with an increase in
hormone-dependent cancers in adulthood.
Obesity is a risk factor for endometrial cancer with a relative risk between 2 to 5-fold. (Brinton, Lacey, Devesa, & al, 2004)
Adolescents with PCOS are particularly vulnerable. (Hardiman, Pillay, Atiomo, 2003)

Endometrial cancer in obesity
Obesity as a risk factor
Japanese case-control studyand American case control
study
Weight gain >35% in early adulthood
trend to developendometrial cancer10 years earlier than
subjects withoutweight change. (Hosono,
Matsuo, Hirose, & al, 2011) (Lu, Risch, Irwin, & al, 2011)
American cohort
76, 569 women
5% increase in weightfrom baseline
(age 25)
greater risk of postmenopausal
endometrial cancer. (Han, Stevens, Truesdale, & al, 2014)
American subcohort study
33, 057 postmenopausalwomen not using
hormones for 17 years.
High BMI at age18 was
associated withendometrial
cancer risk. (Stevens,
Jacobs, Patel, & al, 2014)

Endometrial cancer in obesity
Obesity not as a risk factor
American prospective
study and Koreanretrospective
study
There wasn’t a strongassociation between BMI
at a young age and endometrial hyperplasiaor cancer. (Lee, Kim, Ahn, & al, 2009)
(Dougan, Hankinson, Vivo, & al, 2015)

Pregnancy complications in adolescentswith obesity
Retrospective case-control study
4, 822 females <19 years old
3-fold increased risk for gestational
diabetes mellitus.
1.8-fold increased risk for pregnancy induced
hypertension.
1.7-fold increased riskfor preeclampsia. (Sukalich,
Mingione, Glantz, 2006)
Retrospective cohort
Primiparous adolescents<20 years old
Overweight and obese gained more
weight than recommended.
1.5 to 1.9-fold risk for
preeclampsia. (Harper, Chang, Macones,
2011)
Population based cohortretrospective study
34, 648 overweight and obeseteenagers
11-17 years old.
1.5 times more likely to have
pregnancyrelated
hypertension. (Halloran, Marshall,
Kunovich, & al, 2012)

Obstetric Consequences of Obesity
(Sukalich, Mingione, Glantz, 2006) (Shaw, Wise, Mayo, 2014) (Harper, Chang, Macones, 2011) (Halloran, Marshall, Kunovich, & al, 2012)
Consequences Impact : increased risk
Pre-term delivery >1.2 - 2.7 fold
Pregnancy induced hypertension 1.8 fold
Post-term delivery >1.8 fold
Preeclampsia 1.7 - 1.9 fold
Primary cesarean delivery 1.6 fold
Failure to progress/ cephalopelvicdisproportion
1.6 fold
Labor induction 1.4-fold
Early spontaneous preterm birth 1.2 - 2.7
Large for gestational age infant 2 - 3 fold
Perinatal adverse outcomes in obese adolescents

Obstetric consequences of obesity
Consequences Impact: increased risk
Birth trauma 1.4 - 4 fold
Meconium aspiration syndrome 1.4 - 4 fold
Respiratory distress syndrome 1.4 - 4 fold
Low Apgar scores 1.4 - 4 fold
Premature rupture of membranes 1.4 - 4 fold
Length of stay >5 days 1.4 - 4 fold
Stillbirth 2 - 3 fold
(Sukalich, Mingione, Glantz, 2006)(Shaw, Wise, Mayo, 2014)(Harper, Chang, Macones, 2011) (Halloran, Marshall, Kunovich, & al, 2012)(Warshak, Wolfe, Russell, 2013)
Perinatal adverse outcomes in obese adolescents

Lifestyle factors which affect bodycomposition and obesity
Diet• Fatty foods: higher BMI.
• Sugary drinks lead to higher BMI.
• Bigger portions of food.
• Higher variety of refined foods.
Lack of exercise
• Lessens total energy expenditure and basal energy expenditure.
• Exercise is inversely related to body weight, BMI and degree of obesity.
Sleep deprivation
• Less energy expenditure
• Thermogenesis disturbance
• Increased fatigue
• More time to eat(Elizondo, Hernández, Zamora, 2011)

Take home messagesObese teens have a wide range of psychological, metabolic, gynecological and obstetric consequences
• Psycological and social distress
• Cardio-metaboliccomplications
• Risky sexual behaviour
• Earlier sexual maturation
• Reproductive dysfunction
• Dysmenorrhea
• Disorders of menstruation
• Contraception failure
• PCOS
• Mineralization and bonedensity alterations
• Macromastia
• Increased risk of breastand endometrial cancer
• Pregnancy and obstetriccomplications
• Perinatal complications
• Neonatal complications

Take home messages
• Ask about social behavior, bullying, social isolation, self-esteem, and anxiety during routine consultations.
• Apply a simple depression screening questionnaire.
• Refer to psycologist or psychiatrist if necessary.
Psycologicaland social
distress
• Inform patients and parents about CM risks
• Perform simple anthropometric measurements such as WC, and W/Ht ratio.
• Assess for fasting glucose, HOMA index, lipid profile.
Cardiometabolic
complications
• Gain the patient´s confidence.
• Ask about sexual behaviour, drugs, alcohol and contraceptive use during routine consultations or any.
• Give advice as patient provides information.
Risky sexual behaviour

Take home messages• Early physical examination and clinical history.
The greater the BMI percentile, the sooner.
• Talk to them about uncomfortable physical changes, greater risk of early sexual maturation: give reassurance
• Be ready to talk to the patient and parents aboutclothing issues, and how to handle sports and P.E. class.at school-
Earlier sexual maturation
• Explain to the patient and parents the increased risk of annovulatory cycles and infertility and decreasedeffectivness of ART if obesity continues.
• Assess for fasting glucose, HOMA index, hormonal profile.
Reproductivedysfunction
• The effect in a girl´s daily life of dealing withdysmenorrhea can be quite cumbersome and distressful.
• Provide the necessary care.
• Referral if needed to improve this condition.
Dysmenorrhea

Take home messages
• Patients should be counseled that weight loss mightameliorate the problem, including heavy menstrual bleeding.
• Investigate and consider how it disturbs daily life.
• Advise weight loss through healthy nutrition and physical activity.
Disorders of menstruation
• Emphasize with patients the higher risk they are at.
• Offer safer and more effective methods such as progestin long-acting reversible contraceptives(etonorgestrel implant and LNG IUD).
ContraceptionFailure
• Thorough screening to identify patients at risk, provideopportune diagnosis, and offer the needed care, evenbefore they undergo puberty.
• Screen for cardiometabolic abnormalities: glucose, HOMA, lipids
PCOS

Lifestyle factors which improve body composition and obesity
Diet• Balanced hypocaloric diet.
• Weight loss or maintainance.
• Avoid fatty foods, sugared drinks and sweets.
• Smaller portions of food.
• Higher variety of fruits and vegetables.
Physical Activity and Screen Time
• As recommended by tha AAP
Alcohol• Limit alcohol consumption to reduce caloric intake
Sleep Balance
• Children 8-9 hours
• Adolscents 7-8 hours(Elizondo, Hernández, Zamora, 2011)
Take home messages

Guidelines for treatment of Obesity according to AHA
Children 2-4 years oldwith obesity
Reduce BMI to achieve a weight gain rate of <1kg/2cm of linear growth
Children >4 years old withoverweight (BMI 85-95%) Children >4 years old withobesity (BMI >= 95%), no comorbidities
Reduce BMI to <85th percentile to mantain thepresent BMI;
or weight maintenance through linear growth.
Children > 4 years oldwith obesity (BMI >= 95 percentile), withcomorbidities
Individual approach based on the severity of comorbidities.When weight loss is necessary, it should be progressive and slow. If weight loss is big or quick, there will be a slowing-down of growth that will not be recovered further on.
Adolescents with obesitythat have completedlinear growth
More aggressive weight loss, similar to the one foradults.
Take home messages
(Daniels, Arnett, Eckel, & al, 2005)

Guidelines for treatment of Obesity according to AAP
2-5 years old 6-11 years old 12-18 years old
BMI 85-94th percentileMaintain weight up to a BMI <85th percentile ordiminish weight gain(deflection of BMI curve)
BMI 85-94th percentileMaintain weight up to a BMI <85th percentile ordiminish weight gain(deflection of BMI curve)
BMI 85-94th percentileMaintain weight up to a BMI <85th percentile ordiminish weight gain(deflection of BMI curve)
BMI >= 95th percentileMaintain weight up to a BMI <85th percentile; ifthere is weight loss withhealthy diet it should notbe over 500g/per month
BMI >= 95th percentileMaintain weight up to a BMI <85th percentile orgradual weight loss of 500g/per month
BMI >= 95th percentileWeight loss up to a BMI< 85th percentile, not over1kg per week
BMI >21 kg/m2 (rare)Gradual weight loss, notover 500g/ per month
BMI >= 99th percentileWeight loss, an average of 1kg per week
BMI >= 99th percentileWeight loss, an average of 1kg per week
Adapted from Spear BA et al. Recommendations for Treatment of Child and Adolescent Overweight and Obesity. Pediatrics. American Academy of Pediatrics,2007;120;S254-S288
Take home messages

Exercise recommendations in obesity
According to the AAP and the American College of Sports Medicine, adolescents and children should have:
• 60 minutes of physical activity, daily.
• Less than 2 hours per day of screen time (TV, videogames, computer). (Council on Sports Medicine and Fitness, 2006)
The activity should be enjoyable in the long run (Cycling, skating, jumping the rope, dancing, hiking).
Resistence training is not recommended in prepuberal children that haven’t achieved physical and bone maturity.
(Elizondo, Hernández, Zamora, 2011)
Take home messages

References• WHO. Childhood overweight and obesity. Available at: http://www.who.int/dietphysicalactivity/childhood/en/. Accessed
2015
• Ogden C, Carroll M, Kit B, et al: Prevalence of obesity and trends in body mass index among US children and adolescents, 1999-2010. JAMA 2012; 307:483
• Gutiérrez J, Rivera-Dommarco J, Shamah-Levy T et al: Encuesta Nacional de Salud y Nutrición 2012. Resultados Nacionales. Cuernavaca, México: Instituto Nacional de Salud Pública (MX), 2012
• De Silva N, Helmrath M, Klish W: Obesity in the Adolescent Female. J Pediatr Adolesc Gynecol 2007; 20:207
• In-Iw S, Biro F: Adolescent Women and Obesity. J Pediatr Adolesc Gynecol 2011; 24: 58
• Morrison J, Friedman L, Wang P, et al: Metabolic syndrome in childhood predicts adult metabolic syndrome and type 2 diabetes mellitus 25 to 30 years later. J Pediatr 2008; 152:201
• Li S, Chen W, Srinivasan S, et al: Relation of childhood obesity/cardiometabolic phenotypes to adult cardiometabolicprofile: The Bogalusa Heart Study. Am J Epidemiol 2012; S142
• Zeller M, Modi A: Predictors of health-related quality of life in obese youth. Obesity Silver Spring, Md 2006; 14:122
• Finkelstein E, Brown D, Wrage L, et al: Individual and Aggregate Years-of-life-lost Associated with Overweight and Obesity. Obesity (Silver Spring) 2010; 18:333
• Trandafir L, Anton-Paduraru D, Miron I, et al: Psychosocial Implications of Childhood Obesity. Revista de Cercetare si Interventie Sociala 2015; 49:205
• McClure A, Tanski S, Kingsbury J, et al: Characteristics associated with low self-esteem among US adolescents. AcadPediatr 2010; 10: 238
• Kelly A, Barlow S, Rao G, et al: Severe obesity in children and adolescents: identification, associated health risks, and treatment approaches: a scientific statement from the American Heart Association. Circulation 2013; 128:1689

References
• Liem E, Sauer P, Oldehinkel A, et al: Association between depressive symptoms in childhood and adolescence and overweight in later life: review of the recent literature. Arch Pediatr AdolescMed 2008; 162:981
• Anderson S, Cohen P, Naumova E, et al: Association of depression and anxiety disorders with weight change in a prospective community-based study of children followed up into adulthood. Arch Pediatr Adolesc Med 2006; 160:285
• Richardson L, Davis R, Poulton R, et al: A longitudinal evaluation of adolescent depressionand adult obesity. Arch Pediatr Adolesc Med 2003; 157:739
• Pine D, Goldstein R, Wolk S: The association between childhood depression and adulthood body mass index. Pediatrics 2001; 107:1049
• Hillman J, Dorn L, Bin Huang: Association of anxiety and depressive symptoms and adiposity among adolescent females, using dual energy X-ray absorptiometry. Clin Pediatr 2010; 49: 671
• Goodman E, Must A: Depressive Symptoms in Severely Obese Compared to Normal Weight Adolescents: Results from a Community-Based Longitudinal Study. J Adolesc Health 2011; 49:64
• Boutelle K, Hannan P, Fulkerson J, et al: Obesity as a prospective predictor of depression in adolescent females. Health Psychol 2010; 29:293
• Zeller M, Roehrig H, Modi A, et al: Health-related quality of life and depressive symptoms in adolescents with extreme obesity presenting for bariatric surgery. Pediatrics 2006; 117:1155
• Stice E, Presnell K, Shaw H, Rohde P: Psychological and behavioral risk factors for obesity onset in adolescent girls: a prospective study. J Consult Clin Psychol 2005; 73:195

References
• Merten M, Wickrama K, Williams A: Adolescent obesity and young adult psychosocial outcomes: Gender and racial differences. J Youth Adolescence 2008; 37:1111
• Kaplowitz P: Link between body fat and the timing of puberty. Pediatrics 2008; 121 Suppl 3:S208
• Biro F, Greenspan L, Galvez M: Puberty in Girls of the 21st Century. J Pediatr Adolesc Gynecol 2012; 25:289
• Buyken A, Karaolis-danckert N, Remer T: Association of prepubertal body composition in healthy girls and boyswith the timing of early and late pubertal markers. Am J Clin Nutr 2009; 89:221
• Castilho S, Nucci L: Age at menarche in schoolgirls with and without excess weight. J Pediatr 2015; 91:75
• Lee J, Appugliese D, Kaciroti N, et al: Weight status in young girls and the onset of puberty. Pediatrics 2007; 119:e624
• Biro F, Huang B, Morrison J, et al: Body mass index and waist-to-height changes during teen years in girls are influenced by childhood body mass index. J Adolesc Health 2010; 46:245
• Davison K, Susman E, Birch L: Percent body fat at age 5 predicts earlier pubertal development among girls at age 9. Pediatrics 2003; 111:815
• Wang Y: Is obesity associated with early sexual maturation? A comparison of the association in American boys versus girls. Pediatrics 2002; 110:903
• Crocker M, Stern E, Sedaka N, et al: Sexual dimorphisms in the associations of BMI and body fat with indices of pubertal development in girls and boys. J Clin Endocrinol Metab 2014; 99:E1519
• Aksglaede L, Juul A, Olsen L, et al: Age at puberty and the emerging obesity epidemic. PloS One 2009; 4:e8450
• Bordini B, Rosenfeld R: Normal pubertal development, part I: the endocrine basis of puberty. Pediatr Rev 2011; 32:223

References
• Bordini B, Rosenfeld R: Normal pubertal development: part II: clinical aspects of puberty. Pediatr Rev 2011; 32:281
• Sanfilippo J: Hershey Kiss and Puberty?: J Pediatr Adolesc Gynecol 2015; 28:285
• Jasik C, Lustig R: Adolescent obesity and puberty: the "perfect storm". Ann N Y Acad Sci 2008; 1135:265
• Pasquali R: Obesity and androgens: fact and perspectives: Fertil Steril 2006; 85:1319–40
• Hillman J, Dorn L, Loucks T, Berga S: Obesity and the hypothalamic-pituitary-adrenal axis in adolescent girls. Metab Clin Exp 2012; 61:341
• Shalitin S, Phillip M: Role of obesity and leptin in the pubertal process and pubertal growth-- a review. Int J Obes Relat Metab Disord 2003; 27:869
• Sanchez-Garrido M, Tena-Sempere M: Metabolic control of puberty: roles of leptin and kisspeptins. HormBehav 2013; 64:187
• Catli G, Anik A, Tuhan H, et al: The relation of leptin and soluble leptin receptor levels with metabolic and clinical parameters in obese and healthy children. Peptides 2014; 56:72
• Błogowska A, Rzepka-górska I, Krzyzanowska-swiniarska B: Body composition, dehydroepiandrosterone sulfate and leptin concentrations in girls approaching menarche: J Pediatr Endocrinol Metab 2005; 18:975
• Smith J, Coolen L, Kriegsfeld L, et al: Variation in kisspeptin and RFamide-related peptide (RFRP) expression and terminal connections to gonadotropin-releasing hormone neurons in the brain: a novel medium for seasonal breeding in the sheep. Endocrinology 2008; 149: 5770
• Skorupskaite K, George J, Anderson R: The kisspeptin-GnRH pathway in human reproductive health and disease. Hum Reprod Update 2014; 20:485

References• Dungan H, Clifton D, Steiner R: Minireview: kisspeptin neurons as central processors in the regulation of gonadotropin-
releasing hormone secretion. Endocrinology 2006; 147:1154
• Cortes M, Carrera B, Rioseco H, et al: The role of kisspeptin in the onset of puberty and in the ovulatory mechanism: a mini review. J Pediatr Adolesc Gynecol 2015; 28:286
• Castellano J, Bentsen A, Sánchez-garrido M, et al: Early metabolic programming of puberty onset: impact of changes in postnatal feeding and rearing conditions on the timing of puberty and development of the hypothalamic kisspeptinsystem. Endocrinology 2011; 152:3396
• Pita J, Barrios V, Gavela-pérez T, et al: Circulating kisspeptin levels exhibit sexual dimorphism in adults, are increased in obese prepubertal girls and do not suffer modifications in girls with idiopathic central precocious puberty. Peptides 2011; 32:1781
• Ahmed M, Ong K, Dunger D: Childhood obesity and the timing of puberty. Trends Endocrinol Metab 2009; 20:237
• Wood P, Bauman D: Gynaecological issues affecting the obese adolescent. Best Pract Res Clin Obstet Gynaecol 2015; 29:453
• Pinkney J, Streeter A, Hosking J, et al: Adiposity, chronic inflammation, and the prepubertal decline of sex hormone binding globulin in children: evidence for associations with the timing of puberty (Earlybird 58). J Clin Endocrinol Metab2014; 99:3224
• Ibáñez L, De zegher F: Puberty and prenatal growth. Mol Cell Endocrinol 2006; 22:254
• Embleton N: Early nutrition and later outcomes in preterm infants. World Rev Nutr Diet 2013; 106:26
• Aksglaede L, Sorensen K, Petersen J, et al: Recent decline in age at breast development: The Copenhagen Puberty Study. Pediatrics 2009; 123:e932
• Buck Louis G, Gray L, Marcus M, et al: Environmental factors and puberty timing: Expert panel research needs. Pediatrics 2008; 121(Suppl 3):S192

References• Buck Louis G, Gray L, Marcus M, et al: Environmental factors and puberty timing: Expert panel research needs. Pediatrics
2008; 121(Suppl 3):S192
• Wolff M, Teitelbaum S, Pinney S, et al: Investigation of relationships between urinary biomarkers of phytoestrogens, phthalates, and phenols and pubertal stages in girls. Environ Health Perspect 2010; 118:1039
• Grodstein F, Goldman M, Cramer D: Body mass index and ovulatory infertility. Epidemiology 1994; 5:247
• Klenov V, Jungheim E: Obesity and reproductive function: a review of the evidence. Curr Opin Obstet Gynecol 2014;26:455
• Shaw K, Edelman A: Obesity and oral contraceptives: a clinician's guide. Best Pract Res Clin Endocrinol Metab 2013; 27:55
• Talmor A, Dunphy B: Female obesity and infertility. Best Pract Res Clin Obstet Gynaecol 2015; 29:498
• Hartz A, Barboriak P, Wong A, et al: The association of obesity with infertility and related menstrual abnormalities in women. Int. J. Obesity 1979; 3:57
• Norman R, Clark A: Obesity and reproductive disorders: a review. Reprod. Fertil. Dev 1998; 10:55
• Wise L, Rothman K, Mikkelsen E, et al: An internet-based prospective study of body size and time-to-pregnancy. Hum Reprod2010; 25:253
• Gesink D, Maclehose R, Longnecker M: Obesity and time to pregnancy. Hum Reprod 2007; 22:414
• Shah D, Missmer S, Berry K, et al: Effect of obesity on oocyte and embryo quality in women undergoing in vitro fertilization. Obstet. Gynecol 2011; 118:63
• Practice Committee of American Society for Reproductive Medicine. Obesity and reproduction: an educational bulletin. FertilSteril 2008; 90:S21
• Sutton-McDowall M, Gilchrist R, Thompson J: The pivotal role of glucose metabolism in determining oocyte developmental competence. Reproduction 2010; 139: 685

References• Metwally M, Cutting R, Tipton A, et al: Effect of increased body mass index on oocyte and embryo quality in IVF patients.
Reprod Biomed Online 2007; 15:532
• Brannian J, Hansen K: Leptin and ovarian folliculogenesis: implications for ovulation induction and ART outcomes. Semin ReprodMed 2002; 20:103
• Jungheim E, Moley K: Current knowledge of obesity’s effects in the pre and periconceptional periods and avenues for future research. Am J Obstet Gynecol 2010; 203:525
• Chabrolle C, Tosca L, Ramé C, et al: Adiponectin increases insulin-like growth factor I762 induced progesterone and estradiol secretion in human granulosa cells. Fertil Steril 2009; 92:1988
• Reverchon M, Ramé C, Bertoldo M, et al: Adipokines and the female reproductive tract. Int J Endocrinol 765 2014; 2014:232454
• Gamundi-segura S, Serna J, Oehninger S, et al: Effects of adipocyte-secreted factors on decidualized endometrial cells: modulation of endometrial receptivity in vitro. J Physiol Biochem 2015; 7:537
• Takemura Y, Osuga Y, Yamauchi T, et al: Expression of adiponectin receptors and its possible implication in the human endometrium. Endocrinology 2006; 147:3203
• Michalakis K, Segars J: The role of adiponectin in reproduction: from polycystic ovary syndrome to assisted reproduction. FertilSteril 2010; 94:1949
• Michala L, Creighton S: Adolescent gynaecology. Obstetrics, gynaecology and reproductive medicine 2014; 24:74
• Jamieson M: Disorders of Menstruation in Adolescent Girls. Pediatr Clin North Am 2015; 62:943
• Talib H, Coupey S: Excessive uterine bleeding. Adolesc Med State Art Rev 2012; 23:53
• Fisher M, Lara-Torre E: Update on Key Topics in Adolescent Gynecology. J Pediatr Adolesc Gynecol 2013; 26:51
• Wei S, Schmidt M, Dwyer T, et al. Obesity and menstrual irregularity: associations with SHBG, testosterone, and insulin. ObesitySilver Spring 2009; 17:1070

References
• Seif M, Diamond K, Nickkho-amiry M: Obesity and menstrual disorders. Best Pract Res Clin Obstet Gynaecol 2015; 29:516
• Hillman J, Miller R, Inge T: Menstrual concerns and intrauterine contraception among adolescent bariatric surgery patients. J Womens Health. 2011; 20:533
• Radivojevic U, Lazovic G, Kravic-stevovic T, et al: Differences in anthropometric and ultrasonographic parameters between adolescent girls with regular and irregular menstrual cycles: a case-study of 835 cases. J Pediatr Adolesc Gynecol 2014; 27:227
• West S, Lashen H, Bloigu A, et al: Irregular menstruation and hyperandrogenaemia in adolescence are associated with polycystic ovary syndrome and infertility in later life: Northern Finland Birth Cohort 1986 study. Hum Reprod 2014; 29:2339
• Marcovecchio M, Chiarelli F: Obesity and growth during childhood and puberty. World Rev Nutr Diet 2013; 106:135
• Yoo R, Dewan A, Basu R, et al: Increased luteinizing hormone pulse frequency in obese oligomenorrheic girls with no evidence of hyperandrogenism. Fertil Steril2006; 85:1049
• Tang T, Glanville J, Hayden C, et al: Combined lifestyle modification and metformin in obese patients with polycystic ovary syndrome. A randomized, placebo-controlled, double blind multicentre study. Hum Reprod 2006; 21:80
• Ozerdogan N, Sayiner D, Ayranci U, et. al: Prevalence and predictors of dysmenorrhea among students at a university in Turkey. Int J Gynaecol Obstet 2009; 1:107
• Hirata M, Kumabe K, Inoue Y: Relationship between the frequency of menstrual pain and bodyweight in female adolescents. Nihon Koshu Eisei Zasshi 2002; 49:516
• Maruf F, Ezenwafor N, Moroof S, et al: Physical activity level and adiposity: are they associated with primary dysmenorrhea in school adolescents? Afr J ReprodHealth 2013; 4:1
• Ju H, Jones M, Mishra G: The prevalence and risk factors of dysmenorrhea. Epidemiol Rev 2014; 36:104
• Council on Sports Medicine and Fitness, Council on SchoolHealth. Active healthy living: prevention of childhood obesity through increased physical activity. Pediatrics,2006;117:1834–42
• Elizondo, L., Hernández, C., & Teresa, Z. M. (2011). Terapia Nutricia Médica en Ginecología y Obstetricia. México: McGraw Hill.












![3LD D GH FDSLWDO vQ ± ZZZ SZF FRP SHUVSHFWLYH · pog hxur pog hxur &dslwdol]duhdexuvlhu d frpsdqlloruurpkqh gwl olvwdwh od %9% vq 1xp uxo frpsdqlloru olvwdwh od exuv vq &uh gwhuhd](https://img.dokumen.tips/doc/110x75/604d47635cd63b31d17dbfd4/3ld-d-gh-fdslwdo-vq-zzz-szf-frp-shuvshfwlyh-pog-hxur-pog-hxur-dslwdolduhdexuvlhu.jpg)
![Article 6 Faizan Rai-Neu-Pak-ME-18 Aug 2020-ED-SSA · )dl]dq 5dl 9ro 1rv shuvshfwlyh rq 3dnlvwdq¶v 0(1$ srolf\ xowlpdwho\ ghprqvwudwlqj wkdw wkhuh h[lvwv dq rvfloodwlrq dqg rffdvlrqdo](https://img.dokumen.tips/doc/110x75/60bb49d9ece6b5038943b64b/article-6-faizan-rai-neu-pak-me-18-aug-2020-ed-ssa-dldq-5dl-9ro-1rv-shuvshfwlyh.jpg)


![Application of modern imaging methods in diagnosis of ...hera.ugr.es/doi/16518391.pdf · eases such as cholelitiasis or chronic cholecystitis [3]. Nevertheless, a better understanding](https://img.dokumen.tips/doc/110x75/5e6dfa0ae74cf20491555e89/application-of-modern-imaging-methods-in-diagnosis-of-heraugresdoi-eases.jpg)














