Embed Size (px)
Citation preview

NIHR SouthamptonBiomedical Research Centre
The Southampton Biomedical Research Centre is funde d by the National Institute for Health Research (NI HR) andis a partnership between University Hospital Southa mpton Foundation Trust and the University of Southa mpton
Life Course Factors, Nutrition and Body Composition
Alan A Jackson
Stockholm 18-19th April 2013

Global Health Problems
Barker Hypothesis
Catch-up growth
Conclusions

Global Health Problems
Barker Hypothesis
Catch-up growth
Conclusions

Europe: Secular Increase in Height
Plateau ~1.8 m:Denmark, Sweden, Norway, Netherlands ?genetic potential
Increasing: Belgium, Spain, Italy, Portugal
Larnkjaer et al Acta Paediatrica 2006

Europe: secular increase in height:
Stopped, 18 years following post-neonatal mortality
around 4/1000 deliveries.
Improving socio-economic conditions
better nutrition – healthier diet
decrease in infectious diseases

Brazil Costa Rica Guatemela Haiti Jamaica Nigeria India Ho ng Kong108
112
116
120
124
Martorell, 1985Martorell, 1985Martorell, 1985Martorell, 1985
- 50th- 50th- 50th- 50th
- 25 th- 25 th- 25 th- 25 th
- 10 th- 10 th- 10 th- 10 th
- 5 th- 5 th- 5 th- 5 th
NCHSNCHSNCHSNCHS
percentilepercentilepercentilepercentilehe
ight
, cm
Mean height for 7 year old boysMean height for 7 year old boysMean height for 7 year old boysMean height for 7 year old boys
high socio-economic statushigh socio-economic statushigh socio-economic statushigh socio-economic status
low socio-economic statuslow socio-economic statuslow socio-economic statuslow socio-economic status
Social Determinants of Length

STUNTING: low height for age
More common than wasting (thinness, severe acute malnutrition)
Obesity more common than wasting
↑ mortality
↑ morbidity
↓ physical work performance
↓ intellectual function
↓ Lifelong earning capability

Stunting: by 2 years of ageDeprivation: poor neurocognitive development, obesity
length
weight
weight for length
Shrimpton 2001

Global epidemic of obesity
300 million BMI>30
1.5 billion BMI>25
1.7 billion BMI>23
200 m school-age children overweight
35 m under 5yrs overweight
““““The epidemic of obesity, with its attendant comorbidities --- heart disease, hypertension, stroke, and diabetes --- is not a problem limited to industrialized countries”””” – WHO TRS 916

Prevalence of obesity among children < 5 yrs de Onis & Blossner AJCN
2005

Hillary Clinton Launches 1,000 Days MovementSeptember 2010
Double Burden of Malnutrition:
Malnutrition in All its Forms
Underweight, Overweight, Micronutrient Deficiencies

Global Action Plan for Scaling Up Nutrition (SUN)
Scaling up of evidence-based,high priority nutrition interventions
Focusing primarily on the window of opportunity conception to 24 months
Multisectoral: underlying socio-economic, intersectoral causes
Integrate: health systems, agriculture and food security and social safety nets


Body Mass Index
U-shaped relationshipall cause mortality
Preferred range 22-25 kg/m2

Global Health Problems
Barker Hypothesis
Catch-up growth
Conclusions

Barker hypothesis:Fetal Origins of Chronic Disease:
Coronary heart disease,
Stroke,
Type 2 diabetes
Hypertension
Developmental Model for Disorders

Fetal Origins Hypothesis of Chronic Disease
Disorders originate through Developmental Plasticity
Poor nutrient exposure: early life (fetus, infant, early childhood)
Permanent change in structure and function: - tissues and organs
Vulnerable period: timing, intensity, duration

Coronary heart diseaseStandardised mortality ratios (SMR) in 10141 men & 5585 women
20
40
60
80
100
120
-5.5 -6.5 -7.5 -8.5 -9.5 >9.5
Birthweight (pounds)
SMR
20
40
60
80
100
120
-5.5 -6.5 -7.5 -8.5 -9.5 >9.5
Birthweight (pounds)
SMR
MEN WOMEN
BMJ 1993;307:1519-24
Variable risk across the rangeacross the rangeacross the rangeacross the range of weight at birth & at age one year, which is not a feature of the extremes of the ranges, very low or very high.
Barker Hypothesis

Early Life origins of disease:
Evidence from wide range of internationalstudies
Metabolic changes already
evident in childhood by
5 years of age
Birthweight Tertile andPrevalence of Insulin Resistance Syndrome
Valdez et al, Diabetologia 1992
1 2 3
Birthweight tertile
0
2
4
6
8
10
12
14
16
IRS
per
cent
age
Non-hispanic American
Mexican American
Birthweight Tertile, Adult BMI and Insulin Resistance Syndrome
Valdez at al, Diabetologia 1994
1 2 3
Birthweight Tertile
0
5
10
15
20
25
30
IRS
Pre
vale
nce
BMI Tertile1
23

Adults who had coronary heart disease
Growth in childhood – to 11 years
Mean z scores for height, weight and body mass index
Barker et al Ann Hum Biol 2009;36:445-458
Finnish Studies

Coronary Heart Disease: Finnish menCoronary Heart Disease: Finnish menCoronary Heart Disease: Finnish menCoronary Heart Disease: Finnish menForsen et al, BMJ 1997, 315, 837-40Forsen et al, BMJ 1997, 315, 837-40Forsen et al, BMJ 1997, 315, 837-40Forsen et al, BMJ 1997, 315, 837-40
< 25< 25< 25< 25 - 27- 27- 27- 27 - 29- 29- 29- 29 > 29> 29> 29> 290000
25252525
50505050
75757575
100100100100
125125125125
150150150150
maternal ht > 1.58mmaternal ht > 1.58mmaternal ht > 1.58mmaternal ht > 1.58m
maternal ht < 1.58mmaternal ht < 1.58mmaternal ht < 1.58mmaternal ht < 1.58m
ponderal index of baby, kg/mponderal index of baby, kg/mponderal index of baby, kg/mponderal index of baby, kg/m3333
sta
nd
ard
ise
d m
ort
ali
ty r
ate
sta
nd
ard
ise
d m
ort
ali
ty r
ate
sta
nd
ard
ise
d m
ort
ali
ty r
ate
sta
nd
ard
ise
d m
ort
ali
ty r
ate

Coronary Heart Disease: Finnish menForsen et al BMJ 1997, 315, 837-40Forsen et al BMJ 1997, 315, 837-40Forsen et al BMJ 1997, 315, 837-40Forsen et al BMJ 1997, 315, 837-40
< 24< 24< 24< 24 - 26- 26- 26- 26 - 28- 28- 28- 28 - 30- 30- 30- 30 > 30> 30> 30> 300000
50505050
100100100100
150150150150maternal ht > 1.58m
maternal ht < 1.58mmaternal ht < 1.58mmaternal ht < 1.58mmaternal ht < 1.58m
maternal BMI, kg/m 2
stna
dard
ised
mor
talit
y ra
te

Coronary heart disease: mother < 1.58 mCoronary heart disease: mother < 1.58 mCoronary heart disease: mother < 1.58 mCoronary heart disease: mother < 1.58 m
standardised mortality ratestandardised mortality ratestandardised mortality ratestandardised mortality rate
Forsen et al, BMJ 1997; 315: 837-840
Ponderal index Ponderal index Ponderal index Ponderal index of babyof babyof babyof baby
< 24< 24< 24< 24 -26-26-26-26 -28-28-28-28 -30-30-30-30 > 30> 30> 30> 30 AllAllAllAll
<25<25<25<25 55555555 106106106106 168168168168 170170170170 224224224224 131131131131
-27-27-27-27 55555555 70707070 146146146146 113113113113 134134134134 104104104104
-29-29-29-29 26262626 54545454 31313131 137137137137 149149149149 75757575
> 29> 29> 29> 29 0000 63636363 26262626 55555555 75757575 48484848
AllAllAllAll 43434343 73737373 88888888 114114114114 136136136136 90909090
BMI of motherBMI of motherBMI of motherBMI of mother

Stunting and overweight in children Countries in transition
Popkin, Public Health Nutrition 1998, 1, 5-21
High rates of lower birth weights
High rates of stunting in childhood (15-35%)
Increased prevalence of obesity
Changes in dietary habits
Reduced levels of activity associated with urbanization
Increased prevalence of heart disease and type 2 diabetes

Global trend towards increase weight and height:
generally desirable:
BUT
increase in weight achieved - before increase in height
Increase in childhood overweight and adiposity
Increased risk of shortness/stunting and obesity

The Thin-Fat Indian Baby
Pune: newborn baby
Weight 2,800g
Thin: reduced lean mass.
Relatively adipose: central fat
Small Baby: shortness and fatnessIncreased risk type 2 diabetes

Standard: how children should grow
All children grow similarly

Low birth wt High birth wt20
22
24
26
28
30
32
34
% b
ody
fat
% fat in low and high birth weight groups (mean + sem), adjusted for BMI (27.9 kg/m2)
4.85%(P<0.004)
Kensara et al, 2005
Age 62-75 years

23 24 25 26 27 28 29 30 31 3220
22
24
26
28
30
32Low birth wt
High birth wt
Body mass index (kg/m 2)
% f
at
4. 85%(p <0.004)
ANCOVA BMI v % fat (r = 0.67; p <0.001)
Kensara et al, 2005

For the same weight or BMI at 70 years of age
Lower birth weight
- less muscle- more fat- more central fat
- function difference
- altered cellular nutrient environment

Systolic Blood PressureMaternal Exposure to Protein Diet
6% 9% 12% 18%100
120
140
160
180
casein content of maternal diet during pregnancy
syst
olic
blo
od p
ress
ure,
mm
Hg

Fetus:
reset of central set-point for key hormonal axes
hypothalamo - pituitary-adrenal
growth hormone – IGF – insulin
thyroid axis
sex steroid axis
- response to diet- response to stressors

Glycine and folic acid supplementation prevent hypertension
Blood pressure at 4 weeks in females
18% 9%
9% +
glyc
ine
50
70
90
110
130*
Maternal diet
Sys
tolic
blo
od p
ress
ure
(mm
Hg)
Jackson et al. 2002, Torrens et al. 2006
Blood pressure at 4 weeks in females
18% 9%
Folic a
cid su
pplem
ente
d
50
70
90
110
130
*
Maternal dietS
ysto
lic b
lood
pre
ssur
e(m
m H
g)

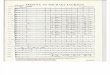
Control Low protein LP with folic acid50
75
100
dietary group
DN
A m
ethy
latio
n
Control Low protein LP with folic acid0
100
200
300
400
dietary group
mR
NA
con
cent
ratio
n
Hepatic Glucocorticoid Receptor: methylation of promoter region of gene and gene expression

Epigenetics
Stable change in DNA structure
Modifies expression
Carried between generations
Variable methylation (protein and folate)
Selective methylation of promoter region

Values are means + SEM
10.0
15.0
20.0
25.0
-40% -60% -80% >80%
Godfrey, et al. Diabetes 2011
Umbilical cord RXRASH amp1 CpG13 methylation
Methylation promoter RETINOIC ACID RECEPTOR gene umbilical cord
Association adiposity 9 years of age: ‘explains’ >25 % of later adiposity;

Global Health Problems
Barker Hypothesis
Catch-up growth
Conclusions

Catch-up growth
- rapid growth, rate greater than normal
- altered efficiency of growthgreater tissue gain per unit energy
- Altered pattern of tissue deposition

Cost of Growth in relation to Change in Body Compos itionduring recovery from severe malnutrition
Jackson, 1977
0 10 20 30 40 50 60 70 80 90 1000.0
2.5
5.0
7.5
10.0
(change in muscle mass) x 100/(change in body mass) , %
cost
of w
eigh
t gai
n, k
cal/g plus
Zinc
minusPotassiumMagnesiumPhosphate

Effect of removing potassium from parenteral
nutrition on nitrogen balanceRudman et al, 1975
-150
-100
-50
0
50
100
150
200 Full Regimen
Full Regimen, 2.4 mmol K+/kg
Plasma K+ 4.6 mmol/L
No potassium
Plasma K+, 2.5 mmol/L
Nitro
gen
Balanc
e, m
g/kg
/d

Pattern of nutrients retainedNutrient requirements for net deposition:
- bone- lean tissue- adipose (by default)
Nutrient availability – altered pattern tissue deposition:
- energy- macronutrients
dietarily essential, conditionally essential- micronutrients

Non-essential or conditionally essential Nutrients:- do not have to be provided preformed in diet.
Required for metabolism - formed from precursors usually readily available in diet.
Amino acids
Longer chain polyunsaturated Fatty acids
High rates of formation
Regulated rates of formation

Diet:
Quantity:energy[macronutrients, carbohydrate, lipid (fat), protein]
Quality:Nutrients[CHO, lipid (essential fatty acids), amino acids, minerals, vitamins, trace elementswater, oxygen]
FOOD/NUTRIENT INSECURITY
Activity: Inflammation

Global Health Problems
Barker Hypothesis
Catch-up growth
Conclusions

Life course
CHRONIC
DISEASEMother’’’’s diet &
body composition
Fetal growth &
development
Infant feeding,
growth, adiposity
Childhood diet,
activity, adiposity
Adult diet, activity
other risk factors
What happens in the short term matters in the long term Life course approach to chronic disease
Standing Committee on Nutrition, United Nations System:
Chronic disease: impending global burden of ill-health
Window of vulnerability: preconception to 2 years of age

Molecular:genetic, epigentic
Cellular:membrane structure and functionreceptor functionsignalling, replication, differentiation
Tissue, organHead circumference: brain Renal size:nephron numberAbdominal circumference: hepatic architecture
Body shape:height, lean, adipose
Structure/function
Structure and function inextricably linked

height weight
Central fat
Fat mass
Lean mass
Visceral lean
Muscle mass
Peripheral fat
Widdowson - “Harmony of Growth”
pace and proportion, partitioning of nutrients
Quantity and Quality