Embed Size (px)
Citation preview

RESEARCH PAPER
Lies tell the truth about cognitive dysfunctionin essential tremor: an experimental deceptionstudy with the guilty knowledge taskF Mameli,1,2 E Tomasini,1,2 E Scelzo,3 M Fumagalli,1,2 R Ferrucci,1,2 L Bertolasi,4
A Priori1,3
1Centro Clinico per laNeurostimolazione, leNeurotecnologie ed i Disordinidel Movimento, FondazioneIRCCS Ca’Granda–OspedaleMaggiore Policlinico, Milan,Italy2Servizio di NeuropsicologiaClinica, Fondazione IRCCSCa’Granda–Ospedale MaggiorePoliclinico, Milan, Italy3Dipartimento di FisiopatologiaMedico-Chirurgica e deiTrapianti, Università degli Studidi Milano, Milan, Italy4Dipartimento ad AttivitàIntegrata di Neuroscienze,Azienda OspedalieraUniversitaria Integrata,Verona, Italy
Correspondence toProfessor Alberto Priori, CentroClinico per laNeurostimolazione, leNeurotecnologie ed i Disordinidel Movimento, FondazioneIRCCS Ca’ Granda OspedaleMaggiore Policlinico, Universityof Milan, Via F. Sforza 35,Milan 20122, Italy;[email protected]
Received 27 November 2012Revised 22 February 2013Accepted 20 March 2013Published Online First17 April 2013
To cite: Mameli F,Tomasini E, Scelzo E, et al.J Neurol NeurosurgPsychiatry 2013;84:1008–1013.
ABSTRACTBackground Research conducted in the past decadechallenges the traditional view that essential tremor (ET)is characterised exclusively by movement disorder, andincreasingly shows that these patients have deficits incognitive and behavioural functioning. The availableevidence suggests that this impairment might arise fromdysfunction in either the fronto-subcortical or cortico-cerebellar circuits. Although abnormalities in the fronto-subcortical circuits could imply difficulty in lying, nostudy has investigated deception in patients with ET.Aims To examine the cognitive functions regulatingdeception in patients with ET, we used a computerisedtask, the Guilty Knowledge Task (GKT). We also tested agroup of patients with Parkinson’s disease (PD), adisease associated with a known difficulty in lieproduction, and a group of healthy subjects (HS).Results In the GKT for deception, patients with ETresponded less accurately than HS (p=0.014) butsimilarly to patients with PD (p=0.955). No differencesbetween groups were found in truthful responses(p=0.488).Conclusions Besides confirming impaired deception inpatients with PD, our results show a lie productiondeficit in patients with ET also. These findings suggestthat difficulty in lying is an aspecific cognitive feature inmovement disorders characterised by fronto-subcorticalcircuit dysfunction, such as PD and ET. Currentknowledge along with our new findings in patients withET—possibly arising from individually unrecognisedextremely mild, cognitive difficulties—should help indesigning specific rehabilitative programmes to improvecognitive and behavioural disturbances in patients.
INTRODUCTIONLying comes under regulation by complex cognitiveprocesses, each supported by distinct neural corre-lates.1–4 From a neurobiological perspective, lyingmay be considered as an exercise in behaviouraland cognitive control. Deception involves multiplemental processes including attention, memory, setshifting, inhibition (the truthful response must beblocked) and conflict monitoring (conflict betweenthe automatic truthful and the lie response).2 5 Innormal everyday circumstances liars are calledupon to do at least two things simultaneously: theymust build a new informative item (the lie) whilewithholding a factual item (the truth), assumingthat they know and understand what constitutes the‘correct’ information. Within such a theoretical
framework the truthful response apparently com-prises a form of baseline, or prepotent response.5
Neuroimaging studies show that responding with alie demands additional cognitive processing, whichengages frontal and parietal cortex, cerebellum,striatum, insula and thalamus.6 7 This additionalwork leads to longer reaction times (RTs) for lyingresponses than for telling the truth and primarilyinvolves prefrontal cortex functions.5
Deception being a complex cognitive process, inclinical conditions that impair cognitive or behav-ioural functioning lying might be impaired inexperimental tasks requiring false responses.8–10
Patients with Parkinson’s disease (PD) have greaterdifficulty than healthy controls in making deceptiveresponses8 probably owing to dysfunctions in theprefrontal system. This finding seems importantgiven the increased attention to non-motor symp-toms in movement disorders.11–13
Of interest are data from a study on essentialtremor (ET)—one of the most common movementdisorders– traditionally considered as a pure motordisorder.14 Neuropsychological research challen-ging the traditional view shows that patients withET frequently have deficits in executive functions,verbal fluency, memory and attention, including set-shifting.11 Their cognitive deficits might arise fromdysfunction in either fronto-subcortical13 15 orcortico-cerebellar circuits.16 17 Although fronto-subcortical abnormalities in ET could imply diffi-culty in lying, no studies have investigated impairedlying in patients with ET.In this study, to investigate whether deceptive
responses are impaired in ET, we tested patientswith the Guilty Knowledge Task (GKT),2 4 asimple, fast, computerised paradigm specificallyassessing the ability to lie. We also tested a groupof patients with PD, a disease associated with aknown difficulty in lie production,8 and a controlgroup of healthy subjects (HS).
MATERIALS AND METHODSSubjectsThe participants were 20 patients with ET, 24patients with idiopathic PD, and 17 HS matchedfor age and score on the Mini-Mental StateExamination (MMSE).18 The demographic charac-teristics of the groups are summarised in table 1.All patients were recruited from the MovementDisorders Center of Fondazione IRCCS Ca’Granda, Policlinico Hospital of Milan, and the
1008 Mameli F, et al. J Neurol Neurosurg Psychiatry 2013;84:1008–1013. doi:10.1136/jnnp-2012-304674
Movement disorders
group.bmj.com on October 6, 2014 - Published by jnnp.bmj.comDownloaded from

Movement Disorders Center of the Policlinico G.B. RossiHospital of Verona. The patients’ motor disturbances were eval-uated using Hoehn and Yahr staging19 and the UnifiedParkinson’s Disease Rating Scale (part III)20 for patients withPD, and with the Tremor Rating Scale21 and the MovementsDisorders Society criteria22 for patients with ET. Scores wererated while patients were ‘on’ medication. The inclusion criteriawere age between 45 and 85 years, age at onset older than40 years, an MMSE score of 24 or higher, and Hoehn and Yahrstage from 1 to 3 for patients with PD. The exclusion criteriawere a medical history of central nervous system diseases notdirectly related to PD or ET (eg, stroke, brain injury, epilepsy),concurrent psychiatric illness such as schizophrenia or manicdepression, a documented or suspected history of drug abuse oralcoholism, diabetes mellitus, cerebral infarction or tumour. Allpatients with PD were taking levodopa or dopamine agonists, orboth (table 1), whereas only eight patients with ETwere takingdisease-related drugs (seven patients β-adrenergic blockers andone patient an anticonvulsant medication). All subjects providedinformed consent. The procedures were approved by the institu-tional review board (ethics committee by Fondazione IRCCSCa’ Granda-Policlinico Hospital of Milan) and were conductedin accordance with the Declaration of Helsinki.
EXPERIMENTAL PROTOCOLAll subjects participated in an experimental session lasting about70–80 min during which they underwent cognitive screeningand an experimental evaluation.
Cognitive screeningFor all patients and controls, in addition to the MMSE, a set ofstandard neuropsychological tests was used to preliminarilyexclude cognitive deficits (table 1). Frontal lobe functions wereassessed with the Digit Span test,23 the Verbal Fluency test,24
and the Trail Making test (TMT).25 To investigate response
inhibition we used a computerised version of the Go/No-Gotask (E-Prime-Psychology Software Tools, Inc.), a responseinhibition task in which a motor response must either be exe-cuted or inhibited and may provide successful and alternativemethods for investigating complex constructs such as impulsivity(or lack of inhibition) and inattention. During this task, partici-pants were required to look at a series of letters displayed onthe screen and respond to a target letter by pressing a button. Inour computerised task, the fixation point appeared on thescreen followed by the stimulus for 2 s and then randomly 40stimuli, which could be either ‘X’ or ‘O’. Participants had topress the corresponding key on the keyboard (B) when ‘X’
appeared, otherwise they pressed no key. The dependent vari-ables measured to investigate response inhibition were RTs andaccuracy (number of correct responses).
Deception taskTruthful and deceptive responses were evaluated using acomputer-controlled procedure (E-Prime-Psychology SoftwareTools, Inc.), a simplified version of the GKT.2 4 Subjects werefirst required to select 5 pictures from a set of 10. To avoidspurious response variations due to stimulus memorisability, the10 pictures were selected to have a similar familiarity (averagefamiliarity=5.54; SD=1.5), frequency (average fre-quency=2.33; SD=0.3), and age of acquisition (average age ofacquisition=2.89; SD=0.6). The pictures and the correspondingstatistical parameters were taken from a database collected onItalian subjects.26 Subjects were then requested to answer truth-fully or lie to the question ‘Do you have this picture?’ referringto a picture randomly presented on the computer screen: 50%of the times the picture was one of those selected and 50% ofthe times it was one of those not selected, with a total of 80trials. Of the 80 stimuli presented, 40 required a truthfulresponse and 40 stimuli required the subject to lie. Before eachpicture was presented, the computer instructed the participant
Table 1 Demographic variables and neuropsychological test performance
Essential tremor (=15) Parkinson’s disease (=20) Healthy controls (=17) p Values
Demographic characteristicsAge (years) 70.26 (10.93) 66.86 (9.37) 61.29 (7.21) p=0.181Sex (male/female) 5/10 16/4 7/10Education (years) 10.26 (4.57) 12.45 (4.48) 10.88 (3.94) p=0.559Duration of disease (years) 7.27 (8.33) 6.10 (3.67) –
Levodopa equivalent dose (mg/day) – 592.25 (318.42) –
UPDRS III (motor part) – 19.18 (8.86) –
Hoehn and Yahr stage – 2.15 (0.72) –
Tremor Rating Scale 13.30 (7.66) – –
Screening assessmentMMSE 28.41 (1.31) 28.18 (1.52) 28.65 (1.19) p=0.579TMTA
(time required/seconds) 43.10 (19.13) 30.03 (16.07) 30.85 (16.98) p=0.065TMTB
(time required/seconds) 73.27 (58.57) 70.15 (60.58) 50.00 (61.28) p=0.482TMTA−B
(time required/seconds) 28.43 (41.23) 40.13 (50.01) 19.71 (50.96) p=0.436Digit span 6.65 (1.07) 6.70 (0.99) 6.54 (1.10) p=0.902PAL 11.73 (3.89) 12.38 (3.04) 12.93 (2.84) p=0.588Verbal fluency
Phonetic 34.14 (9.55) 33.31 (10.94) 38.91 (7.52) p=0.278Semantic 38.64 (7.73) 41.15 (7.52) 44.71 (4.81) p=0.052
GO/NO-GO Task (Accuracy) 38.60 (2.64) 38.85 (1.60) 39.35 (0.86) p=0.480GO/NO-GO Task (Reaction time; ms) 624.88 (229.61) 532.26 (234.20) 456.78 (85.31) p=0.060
UPDRS, Unified Parkinson’s Disease Rating Scale; MMSE, Mini Mental State Examination; TMT, Trial Making Test; PAL, Paired Associate Learning; ms, milliseconds; p values, statisticalsignificance at ANOVA; all values are expressed as mean (SD).
Mameli F, et al. J Neurol Neurosurg Psychiatry 2013;84:1008–1013. doi:10.1136/jnnp-2012-304674 1009
Movement disorders
group.bmj.com on October 6, 2014 - Published by jnnp.bmj.comDownloaded from
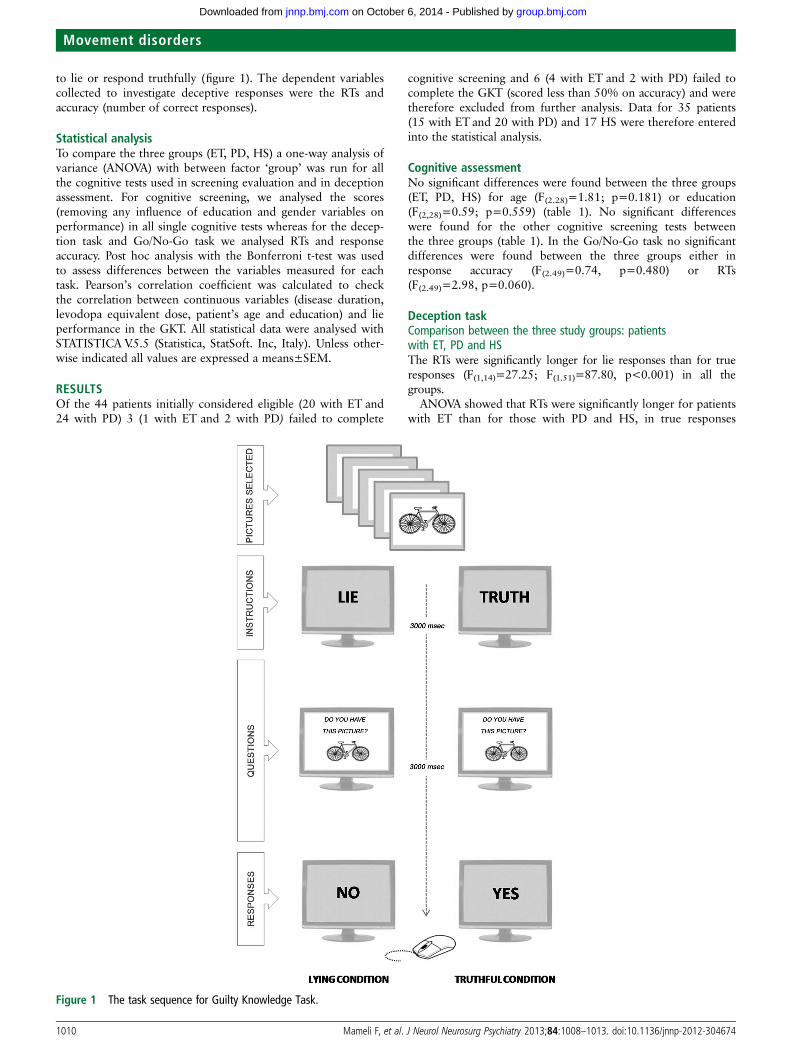
to lie or respond truthfully (figure 1). The dependent variablescollected to investigate deceptive responses were the RTs andaccuracy (number of correct responses).
Statistical analysisTo compare the three groups (ET, PD, HS) a one-way analysis ofvariance (ANOVA) with between factor ‘group’ was run for allthe cognitive tests used in screening evaluation and in deceptionassessment. For cognitive screening, we analysed the scores(removing any influence of education and gender variables onperformance) in all single cognitive tests whereas for the decep-tion task and Go/No-Go task we analysed RTs and responseaccuracy. Post hoc analysis with the Bonferroni t-test was usedto assess differences between the variables measured for eachtask. Pearson’s correlation coefficient was calculated to checkthe correlation between continuous variables (disease duration,levodopa equivalent dose, patient’s age and education) and lieperformance in the GKT. All statistical data were analysed withSTATISTICA V.5.5 (Statistica, StatSoft. Inc, Italy). Unless other-wise indicated all values are expressed a means±SEM.
RESULTSOf the 44 patients initially considered eligible (20 with ET and24 with PD) 3 (1 with ET and 2 with PD) failed to complete
cognitive screening and 6 (4 with ET and 2 with PD) failed tocomplete the GKT (scored less than 50% on accuracy) and weretherefore excluded from further analysis. Data for 35 patients(15 with ET and 20 with PD) and 17 HS were therefore enteredinto the statistical analysis.
Cognitive assessmentNo significant differences were found between the three groups(ET, PD, HS) for age (F(2.28)=1.81; p=0.181) or education(F(2,28)=0.59; p=0.559) (table 1). No significant differenceswere found for the other cognitive screening tests betweenthe three groups (table 1). In the Go/No-Go task no significantdifferences were found between the three groups either inresponse accuracy (F(2.49)=0.74, p=0.480) or RTs(F(2.49)=2.98, p=0.060).
Deception taskComparison between the three study groups: patientswith ET, PD and HSThe RTs were significantly longer for lie responses than for trueresponses (F(1,14)=27.25; F(1.51)=87.80, p<0.001) in all thegroups.
ANOVA showed that RTs were significantly longer for patientswith ET than for those with PD and HS, in true responses
Figure 1 The task sequence for Guilty Knowledge Task.
1010 Mameli F, et al. J Neurol Neurosurg Psychiatry 2013;84:1008–1013. doi:10.1136/jnnp-2012-304674
Movement disorders
group.bmj.com on October 6, 2014 - Published by jnnp.bmj.comDownloaded from
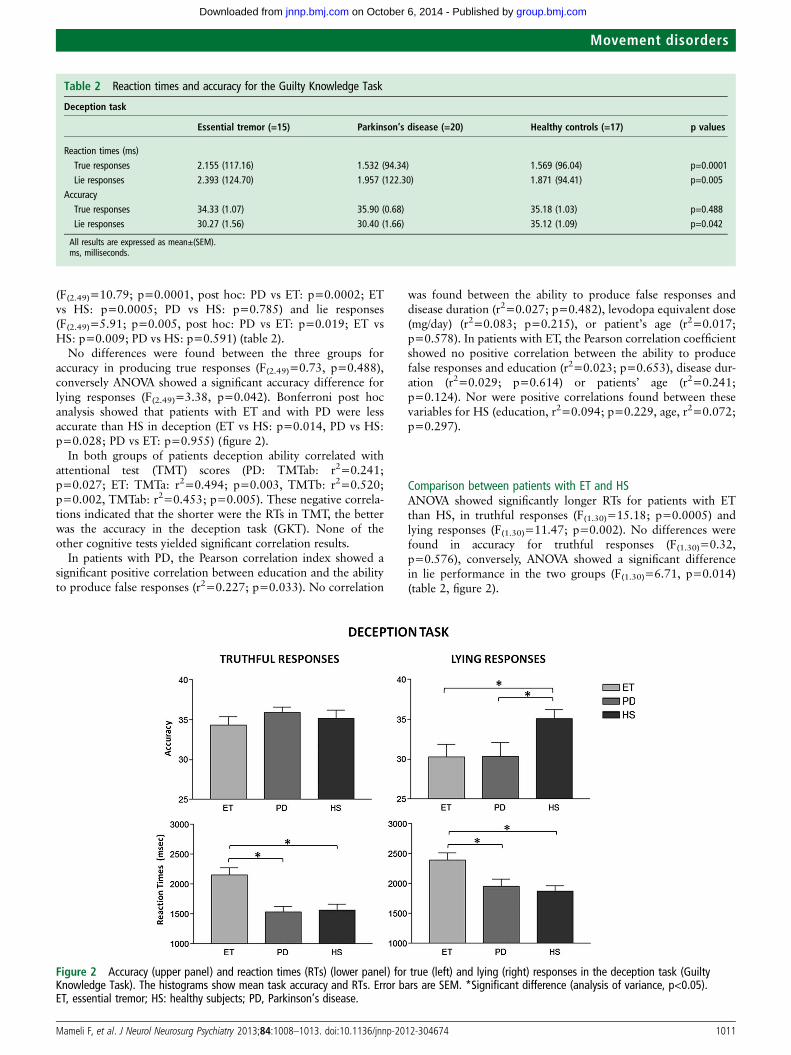
(F(2.49)=10.79; p=0.0001, post hoc: PD vs ET: p=0.0002; ETvs HS: p=0.0005; PD vs HS: p=0.785) and lie responses(F(2.49)=5.91; p=0.005, post hoc: PD vs ET: p=0.019; ET vsHS: p=0.009; PD vs HS: p=0.591) (table 2).
No differences were found between the three groups foraccuracy in producing true responses (F(2.49)=0.73, p=0.488),conversely ANOVA showed a significant accuracy difference forlying responses (F(2.49)=3.38, p=0.042). Bonferroni post hocanalysis showed that patients with ET and with PD were lessaccurate than HS in deception (ET vs HS: p=0.014, PD vs HS:p=0.028; PD vs ET: p=0.955) (figure 2).
In both groups of patients deception ability correlated withattentional test (TMT) scores (PD: TMTab: r2=0.241;p=0.027; ET: TMTa: r2=0.494; p=0.003, TMTb: r2=0.520;p=0.002, TMTab: r2=0.453; p=0.005). These negative correla-tions indicated that the shorter were the RTs in TMT, the betterwas the accuracy in the deception task (GKT). None of theother cognitive tests yielded significant correlation results.
In patients with PD, the Pearson correlation index showed asignificant positive correlation between education and the abilityto produce false responses (r2=0.227; p=0.033). No correlation
was found between the ability to produce false responses anddisease duration (r2=0.027; p=0.482), levodopa equivalent dose(mg/day) (r2=0.083; p=0.215), or patient’s age (r2=0.017;p=0.578). In patients with ET, the Pearson correlation coefficientshowed no positive correlation between the ability to producefalse responses and education (r2=0.023; p=0.653), disease dur-ation (r2=0.029; p=0.614) or patients’ age (r2=0.241;p=0.124). Nor were positive correlations found between thesevariables for HS (education, r2=0.094; p=0.229, age, r2=0.072;p=0.297).
Comparison between patients with ET and HSANOVA showed significantly longer RTs for patients with ETthan HS, in truthful responses (F(1.30)=15.18; p=0.0005) andlying responses (F(1.30)=11.47; p=0.002). No differences werefound in accuracy for truthful responses (F(1.30)=0.32,p=0.576), conversely, ANOVA showed a significant differencein lie performance in the two groups (F(1.30)=6.71, p=0.014)(table 2, figure 2).
Table 2 Reaction times and accuracy for the Guilty Knowledge Task
Deception task
Essential tremor (=15) Parkinson’s disease (=20) Healthy controls (=17) p values
Reaction times (ms)True responses 2.155 (117.16) 1.532 (94.34) 1.569 (96.04) p=0.0001Lie responses 2.393 (124.70) 1.957 (122.30) 1.871 (94.41) p=0.005
AccuracyTrue responses 34.33 (1.07) 35.90 (0.68) 35.18 (1.03) p=0.488Lie responses 30.27 (1.56) 30.40 (1.66) 35.12 (1.09) p=0.042
All results are expressed as mean±(SEM).ms, milliseconds.
Figure 2 Accuracy (upper panel) and reaction times (RTs) (lower panel) for true (left) and lying (right) responses in the deception task (GuiltyKnowledge Task). The histograms show mean task accuracy and RTs. Error bars are SEM. *Significant difference (analysis of variance, p<0.05).ET, essential tremor; HS: healthy subjects; PD, Parkinson’s disease.
Mameli F, et al. J Neurol Neurosurg Psychiatry 2013;84:1008–1013. doi:10.1136/jnnp-2012-304674 1011
Movement disorders
group.bmj.com on October 6, 2014 - Published by jnnp.bmj.comDownloaded from

Comparison between patients with PD and ETANOVA showed that RTs were significantly longer in patientswith ET than in those with PD, for truthful responses(F(1.33)=17, p=0.0002) and lying responses (F(1.33)=6.02,p=0.019). Conversely, no significant difference was found inaccuracy (truthful responses: F(1.33)=1.66, p=0.206; lyingresponses: (F(1.33)=0.00, p=0.955) (see table 2, figure 2).
Comparison between patients with PD and HSNo significant differences were found between groups in RTs,for truthful responses (F(1.35)=0.08, p=0.785) or lyingresponses (F(1.35)=0.29, p=0.591). Similarly, no differenceswere found in accuracy for truthful responses (F(1.35)=0.36,p=0.552), conversely, ANOVA showed a significant differencein lie accuracy F(1.35)=5.20, p=0.028) (see table 2, figure 2).
DISCUSSIONOur main finding is that when tested with the GKT, a procedureassessing the ability to lie, patients with ET produce normaltruthful responses, but are less accurate than HS in producingdeception. As expected in accordance with a previous report,the GKT disclosed a similar difficulty in producing deceptiveresponses in patients with PD. Confirming previous studies inpatients with PD,8 this finding therefore demonstrates that ourexperimental paradigm provides reliable results and the GKT isa valid tool for testing the ability to lie.
An intriguing finding is that patients with ET were slowerthan HS and patients with PD in truthful and lying responses.This finding seems surprising given that one would haveexpected patients with PD to be slower. A possible explanationis that kinetic tremor makes it hard for patients with ET toreach the target on the keyboard and choose the right key.Conversely, patients with PD would be less prone to slowingbecause they predominantly have rest tremor. Among otherfactors possibly contributing to the prolonged response latencyin patients with ET is their reported oculomotor deficit.27 28 Inparticular, a study testing eye–hand coordination in patientswith ET disclosed abnormal kinematical changes in pointingmovements.28
The absence of executive dysfunction in routine clinical cog-nitive assessment and frontal-type test results in the patients westudied seems to contradict our initial hypothesis that a failurein deception mechanisms could depend on frontal-striatal (orfronto-cerebellar in ET) circuit derangement. The executive testsused in screening assessment nevertheless differ from the decep-tion task, whereas the GKT simultaneously involves frontal abil-ities such as set shifting, working memory, inhibition process(the truthful response must be blocked) and conflict monitoring(conflict between the automatic truthful response and the lieresponse required by the instructions). Equally important, therandom deceptive condition requires participants to monitortheir long-term response patterns strategically to accommodatea deceptive strategy. These cognitive functions could be definedas ‘high-functioning frontal skills’. In particular, the anterior cin-gulate cortex is a frontal brain area involved in monitoringactions and resolving problems with conflicting responses.29 Wetherefore speculate that our patients’ impaired lying abilitycould reflect the intense cognitive load required by the decep-tion task. Complex experimental paradigms, such as those weadministered in our study, can detect alterations in cognitivefunctioning or subclinical deficits. Computerised tasks that testseveral cognitive functions simultaneously also allow evaluatingpatients’ cognitive abilities, simulating a real-life situation in
which the environment issues multiple requests and requires fastresponses. The GKT focuses precisely on these cognitive pro-cesses2 4 and requires the subject to make an intense cognitiveeffort to overcome the high cognitive load the task demands.The cognitive complexity related to the deception task may helpto explain the GKT abnormality in patients with ET and PD, inwhom subtle cognitive dysfunctions—per se clinically andbehaviourally irrelevant—may serially cumulate, ultimatelyresulting in impaired lying.
Although the difficulty in lying is common to ET and PD,movement disorders characterised by fronto-subcortical circuitdysfunction, in the brain areas implicated15 30 might differ inthe two conditions. Whereas in PD the corticostriatal loopinvolvement implicates the connections between the neocortexand striatum,30 the circuit implicated in the pathophysiology ofET is the cerebello-frontal loop.15 Neuropsychological data indi-cate that dysfunctions in this circuit might contribute to the cog-nitive deficits in ET.11 In addition, functional neuroimagingstudies, in conjunction with neuropsychological investigations,increasingly point to a cerebellar role in cognitive functionssuch as attention, executive functions, verbal fluency andmemory31 32 and document pathways connecting the cerebel-lum with the thalamus and cortex.33 A growing interest in cere-bellar function and its involvement in higher cognition haveprompted research in recent years.34 Of special importance arefindings on functional connectivity and cognitive networks inET describing disrupted functional coupling between the cere-bellum and the executive control circuit (dorsolateral prefrontalcortex, thalamus, inferior parietal cortex). Also, neuroimagingstudies during deception in HS show activation in the dorsolat-eral prefrontal cortex (a brain area involved in PD), and in thecerebellum (an area involved in ET).5 6
Finally, evidence from functional studies on neuronal net-works show that the cerebellum plays a regulatory role betweencompetitive cognitive networks.35 Poor cognitive control inpatients with ET may reflect abnormalities in switching from adefault mode network to an executive control circuit, particu-larly when task demands are elevated.35
Some help in explaining the abnormal deception disclosed inpatients with PD and ET could come from emerging knowledgeon abnormal subcortical network oscillations. Research intomovement disorders is now opening up a new area of interestinvestigating local field potentials (LFP) (EEG recorded directlyfrom subcortical structures) in patients.36 LFP studies in humansin the past 10 years have disclosed unknown subcortical func-tions in patients with ET and PD doing motor, cognitive andbehavioural tasks showing that a ‘code’ exists in LFP oscillationsand corresponds to the patient’s status.37 Probably, severalcomplex cognitive functions rely on specific brain oscillatoryrhythms in the cortico-subcortical network and their abnormal-ity can interfere widely with brain function, ultimately impairingdeception.
Of importance when interpreting our results, we emphasisethat the sample size, though small, matches patient numbers inprevious cognitive studies in ET and PD.13 16 38 Second, weinvestigated patients with different motor disorders that are dif-ficult to compare in terms of disease stages and severity. Third,because we instructed our participants to tell a lie, this experi-mental laboratory condition prevents us from automaticallyextending our findings to the patient’s real life. Also, becauseour testing procedure specifically focuses on the cognitive com-ponents that characterise complex lies, for example executivecontrol, further studies will need to investigate deception abilityin more ‘ecological’ experimental settings.
1012 Mameli F, et al. J Neurol Neurosurg Psychiatry 2013;84:1008–1013. doi:10.1136/jnnp-2012-304674
Movement disorders
group.bmj.com on October 6, 2014 - Published by jnnp.bmj.comDownloaded from

CONCLUSIONExtending current knowledge on the psychological features inmovement disorders, the impaired deception we describe inpatients with ET and PD may reflect poor cognitive flexibilityand insidious neuropsychological changes that might underliespecific personality traits. Parkinsonian patients with PD are‘honest’ in that they tend not to deceive others.39 40 Ratherthan choosing not to tell lies, they may actually have difficultyin lying owing to cognitive deficits resulting from pathologicalchanges or dysfunctions in certain brain regions.8 Impairment inthe prefrontal executive system can prevent people exhibitingthe flexible and goal-directed behaviours that are consideredessential human behavioural features. These new insights intothe complex cognitive processes in patients with ET and PDcould be useful in designing novel specific approaches for cogni-tive and behavioural rehabilitation.
Contributors FM: principal investigator, conception and design,cognitive-behavioural assessment, analysis and interpretation of data and draftingthe article; ET: cognitive-behavioural assessment, analysis and interpretation of data;ES: patients enrolment, revising article critically for important intellectual content;MF: cognitive-behavioural assessment, data collection and analysis andinterpretation of data; RF: cognitive-behavioural assessment, revising article criticallyfor important intellectual content; LB: experimental procedures monitoring, revisingarticle critically for important intellectual content, scientific dissemination of results;AP: conception and design, experimental procedures monitoring, revising articlecritically for important intellectual content, final approval of the version to bepublished.
Competing interests None.
Patient consent Obtained.
Ethics approval Fondazione IRCCS Ca’Granda–Ospedale Maggiore Policlinico,Milan, Italy.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1 Ganis G, Kosslyn SM, Stose S, et al. Neural correlates of different types of
deception: an fMRI investigation. Cereb Cortex 2003;13:830–6.2 Mameli F, Mrakic-Sposta S, Vergari M, et al. Dorsolateral prefrontal cortex
specifically processes general—but not personal—knowledge deception: Multiplebrain networks for lying. Behav Brain Res 2010;211:164–8.
3 Nunez JM, Casey BJ, Egner T, et al. Intentional false responding shares neuralsubstrates with response conflict and cognitive control. Neuroimage2005;25:267–77.
4 Priori A, Mameli F, Cogiamanian F, et al. Lie-specific involvement of dorsolateralprefrontal cortex in deception. Cereb Cortex 2008;18:451–5.
5 Spence SA, Hunter MD, Farrow TF, et al. A cognitive neurobiological account ofdeception: evidence from functional neuroimaging. Philos Trans R Soc Lond B BiolSci 2004;359:1755–62.
6 Langleben DD, Loughead JW, Bilker WB, et al. Telling truth from lie in individualsubjects with fast event-related fMRI. Hum Brain Mapp 2005;26:262–72.
7 Langleben DD, Schroeder L, Maldjian JA, et al. Brain activity during simulateddeception: an event-related functional magnetic resonance study. Neuroimage2002;15:727–32.
8 Abe N, Fujii T, Hirayama K, et al. Do parkinsonian patients have trouble telling lies?The neurobiological basis of deceptive behaviour. Brain 2009;132:1386–95.
9 Baron-Cohen S. Out of sight or out of mind? Another look at deception in autism.J Child Psychol Psychiatry 1992;33:1141–55.
10 Oswald DP, Ollendick TH. Role taking and social competence in autism and mentalretardation. J Autism Dev Disord 1989;19:119–27.
11 Bermejo-Pareja F. Essential tremor—a neurodegenerative disorder associated withcognitive defects? Nat Rev Neurol 2011;7:273–82.
12 Demakis GJ. The neuropsychology of Parkinson’s disease. Dis Mon 2007;53:152–5.
13 Gasparini M, Bonifati V, Fabrizio E, et al. Frontal lobe dysfunction in essentialtremor: a preliminary study. J Neurol 2001;248:399–402.
14 Elble RJ. Diagnostic criteria for essential tremor and differential diagnosis. Neurology2000;54:S2–6.
15 Higginson CI, Wheelock VL, Levine D, et al. Cognitive deficits in essentialtremor consistent with frontosubcortical dysfunction. J Clin Exp Neuropsychol2008;30:760–5.
16 Lombardi WJ, Woolston DJ, Roberts JW, et al. Cognitive deficits in patients withessential tremor. Neurology 2001;57:785–90.
17 Troster AI, Woods SP, Fields JA, et al. Neuropsychological deficits in essentialtremor: an expression of cerebello-thalamo-cortical pathophysiology? Eur J Neurol2002;9:143–51.
18 Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method forgrading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189–98.
19 Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology1967;17:427–42.
20 Fahn S ER, Members of the UPDRS Development Committee. In: Fahn S, Marsden CD,Calne DB, Goldstein M.eds Recent developments in Parkinson’s disease. Vol 2. FlorhamPark, NJ. Macmillan Health Care Information, 1987: 293–304.
21 Fahn S, Tolosa E, Concepcion M. Clinical rating scale for tremor. In: Jankovic J,Tolosa E, eds. Parkinson’s disease and movement disorders. 2nd edn. Baltimore:Williams and Wilkins, 1993: 271–80.
22 Deuschl G, Bain P, Brin M, et al. Consensus statement of the Movement DisorderSociety on Tremor. Ad Hoc Scientific Committee. Mov Disord 1998;13Suppl3:2–23.
23 Orsini A, Grossi D, Capitani E, et al. Verbal and spatial immediate memory span:normative data from 1355 adults and 1112 children. Ital J Neurol Sci1987;8:539–48.
24 Novelli G, Papagno C, Capitani E, et al. Tre test clinici di memoria verbale a lungotermine. Taratura su soggetti normali. Arch Psicol Neurol Psichiatria1986;47:278–96.
25 Giovagnoli AR, Del Pesce M, Mascheroni S, et al. Trail making test: normativevalues from 287 normal adult controls. Ital J Neurol Sci 1996;17:305–9.
26 Dell’Acqua R, Lotto L, Job R. Naming times and standardized norms for the ItalianPD/DPSS set of 266 pictures: direct comparisons with American, English, French,and Spanish published databases. Behav Res Methods Instrum Comput2000;32:588–615.
27 Helmchen C, Hagenow A, Miesner J, et al. Eye movement abnormalities in essentialtremor may indicate cerebellar dysfunction. Brain 2003;126:1319–32.
28 Trillenberg P, Fuhrer J, Sprenger A, et al. Eye-hand coordination in essential tremor.Mov Disord 2006;21:373–9.
29 Johnson R Jr, Barnhardt J, Zhu J. The contribution of executive processes todeceptive responding. Neuropsychologia 2004;42:878–901.
30 Owen AM. Cognitive dysfunction in Parkinson’s disease: the role of frontostriatalcircuitry. Neuroscientist 2004;10:525–37.
31 Ferrucci R, Marceglia S, Vergari M, et al. Cerebellar transcranial direct currentstimulation impairs the practice-dependent proficiency increase in working memory.J Cogn Neurosci 2008;20:1687–97.
32 Schmahmann JD, Caplan D. Cognition, emotion and the cerebellum. Brain2006;129:290–2.
33 Benito-Leon J, Louis ED, Bermejo-Pareja F. Population-based case-control study ofcognitive function in essential tremor. Neurology 2006;66:69–74.
34 Keren-Happuch E, Chen SHA, Moon-Ho Ringo Ho, et al. A meta-analysis ofcerebellar contributions to higher cognition from PET and fMRI studies Brain Mapp2012. doi:10.1002/hbm.22194
35 Dosenbach NU, Fair DA, Cohen AL, et al. A dual-networks architecture of top-downcontrol. Trends Cogn Sci 2008;12:99–105.
36 Priori A, Giannicola G., Rosa M, et al. Deep brain electrophysiological recordingsprovide possible clues to what is wrong in Tourette syndrome. Neurosci BiobehavRev 2013. doi:10.1016/j.neubiorev Not available
37 Pedrosa DJ, Reck C, Florin E, et al. Essential tremor and tremor in Parkinson’sdisease are associated with distinct ‘tremor clusters’ in the ventral thalamus.Exp Neurol 2012;237:435–43.
38 Cerasa A, Passamonti L, Novellino F, et al. Fronto-parietal overactivation in patientswith essential tremor during Stroop task. Neuroreport 2010;21:148–51.
39 Ishihara L, Brayne C. What is the evidence for a premorbid parkinsonian personality:a systematic review. Mov Disord 2006;21:1066–72.
40 Menza M. The personality associated with Parkinson’s disease. Curr Psychiatry Rep2000;2:421–6.
Mameli F, et al. J Neurol Neurosurg Psychiatry 2013;84:1008–1013. doi:10.1136/jnnp-2012-304674 1013
Movement disorders
group.bmj.com on October 6, 2014 - Published by jnnp.bmj.comDownloaded from
doi: 10.1136/jnnp-2012-304674online April 17, 2013
2013 84: 1008-1013 originally publishedJ Neurol Neurosurg Psychiatry F Mameli, E Tomasini, E Scelzo, et al. knowledge taskexperimental deception study with the guiltydysfunction in essential tremor: an Lies tell the truth about cognitive
http://jnnp.bmj.com/content/84/9/1008.full.htmlUpdated information and services can be found at:
These include:
References http://jnnp.bmj.com/content/84/9/1008.full.html#ref-list-1
This article cites 36 articles, 7 of which can be accessed free at:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
CollectionsTopic
(601 articles)Parkinson's disease � (1730 articles)Drugs: CNS (not psychiatric) �
(731 articles)Movement disorders (other than Parkinsons) � Articles on similar topics can be found in the following collections
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on October 6, 2014 - Published by jnnp.bmj.comDownloaded from




























