Embed Size (px)
Citation preview

11
Lessons Learned: Tobacco Cessation and Health
Systems Change
May 24, 2017

22
Speakers
Anne DiGiulio, Manager,
Lung Health Policy,
American Lung Association
Megan Whittet,
Senior Cessation
Manager, Clearways,
MinnesotaSM
Joy Leuthard, Manager,
Health Improvement
Programs, Oklahoma
Hospital Association

33
• Introduction
• Setting the Stage
• The Oklahoma Experience
• The Minnesota Experience
• Question and Answer
Overview

4FOR INTERNAL USE ONLY DO NOT DISTRIBUTE. Confidential and proprietary property of the American Lung Association, all rights reserved. 4
What is a Comprehensive Cessation Benefit?

55
Cessation Coverage
• 7 Medications
– 5 NRTs (Gum, Patch, Lozenge, Nasal
Spray, Inhaler)
– Bupropion
– Varenicline
• 3 Types of Counseling
– Individual (face-to-face)
– Group
– Phone
Comprehensive Benefit

66
Cessation Coverage
• Cost Sharing (Co-Pays)
• Prior Authorization
• Stepped Care Therapy
• Required Counseling
• Duration Limits
• Annual (or Lifetime) Limits
• Dollar Limits
Common Barriers to Access Care
7FOR INTERNAL USE ONLY DO NOT DISTRIBUTE. Confidential and proprietary property of the American Lung Association, all rights reserved. 7
WHY HEALTH SYSTEMS CHANGE?

88
Why Systems Change?
• Over 2/3 of smokers want to quit
• In 2015, only half of smokers received advice to quit from a health professional and made a quit attempt
• Fewer than 1 in 10 smokers quit successfully
• In Medicaid, only 10 percent of current smokers received cessation medication
Smokers want to Quit

99
• Tobacco-caused disease is
costly in terms of lives and
money
• Quality Measures
– HEDIS
– Joint- Commission
• MACRA
Value and Payment
Why Systems Change?

Hospitals Helping Patients Quit:
Advancing Tobacco Treatment
Oklahoma Hospital Association
JOY L LEUTHARD, MS, LSWA
MANAGER, HEALTH IMPROVEMENT INITIATIVES
10AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Oklahoma Hospital Association
Established in 1919; represents over 135 hospitals/health systems –
85% of all hospitals
Advocacy at state & federal levels, industry communication,
educational programs, information and data analysis,
patient quality& safety resources, health improvement
Promotes health and welfare of all Oklahomans by leading and assisting
member organizations to provide high quality, safe and valued
health care services to their communities
Hospitals play a vital role in helping to advance the overall state of
health for their patients and the public
Uniquely positioned to promote tobacco treatment
11AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Hospital Helping Patients Quit
Funding - Okla. Tobacco Settlement Endowment Trust - MSA $$
Staffing - 3.5 FTE’s – 1 Manager, 2 Coordinators, ½-time assistant
Launched in 2009, serving OHA hospital members
Touched over 50 hospitals and health systems statewide
Measure # referrals to Helpline ; % acceptance; % tobacco free
Helpline & HHPQ evaluation - Oklahoma Tobacco Research Center and the University of Oklahoma, College of Public Health
October 2010 – March 2017:
- Referrals to Oklahoma Tobacco Helpline – 20,189 / 50% e-Referrals
- 29% acceptance rate for services
- 35% of those receiving counseling and pharmacotherapy remain quit at 7 mos
12AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Hospital Helping Patients Quit
Comprehensive system changes – tobacco-free culture:
◦ Policy driven
◦ Comprehensive tobacco-free property – inside and outside
◦ Tobacco treatment/cessation support for:
- Patients, Family and Employees
Sustainable system changes embedded in processes
◦ Clinical Process – evidence-based clinical guidelines – 5A’s
◦ Workflow – integrate clinical protocol into EMR, include e-Referral
13AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017
Why Hospitals/Clinics
Appropriate time and setting
• Health system! Treat the whole person!
• Majority of tobacco users visit a health system annually
• Teachable moment – motivated due to hospitalization
• Tobacco free campus / culture – supports cessation
• Opportunity for positive experience with adequately
dosed medication and supportive treatment
14AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Why Hospitals/Clinics?
Growing Quality Measure in the Healthcare Sector
Recommendation of National Quality Forum
Joint Commission Tobacco Measures
Increasingly Adopted – 14 Hospitals in Oklahoma
CMS Requirement for Inpatient Behavioral Health
Meaningful Use
15
TOB-1• Tobacco Use
Screening
TOB-2
• Tobacco Use Treatment at Visit
TOB-3
• Tobacco Use Treatment at Discharge
AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Embedding Best Practice
Clinical Workflow
In EMRs
16AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Clinical Practice Guidelines 5A’s Best Practice
ASK - screen all patients
ADVISE - to quit tobacco and tie to health issues
ASSESS - readiness to make a quit attempt
ASSIST - provide adequately dosed NRT
ARRANGE - referral to the Oklahoma TobaccoHelpline / follow-up
17
USPHS Clinical Practice Guidelines: Treating Tobacco Use and Dependence – 2008 Update
AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Tobacco Use Screening (RN/LPN/MA)
• Screens all patients for tobacco use via the
screening questions in embedded in EMR
• Arranges for medication
• EMR prompts designated staff for
completion of cessation intervention
Bedside Intervention (3–5 minutes)
• Motivational Interview
• Assess tobacco users interest in quitting
• Assess desire for helpline support
• Assess for comfort with medication
Tobacco
status
documented
in record
Visit with
Physician
RRT
Case Mgt.
Soc. Work
RN
EMR
EMR
Ask
Advise &
Assess
Assist &
Arrange
E-Referral /
Fax referral
Outcome report
Tobacco Treatment Workflow
Optum
AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017 18

Case Studies:
Four Oklahoma
Health Systems
AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017 19

Case Study:INTEGRIS Health
First system-wide implementation / began with fax referrals
Launched in Oct 2010 / 10 hospitals/1,650 beds & 20+ clinics
Took 18 months to implement / hospitals first
Required 1 FTE coordinator - 3 yr contract w/ HHPQ – shared cost
2016 - implementing new EMR – Epic /clinics & 4 hospitals / 24 mos
As of March 2017 – 10,480 referrals!
- 7,980 inpatient / 2,083 outpatient/ 261 employees / 86 community health
20AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Case Study:
Chickasaw Nation Medical Center
Oklahoma has the 2nd largest Native Americanpopulation in numbers & percent - nearly 300,000 / 9.1% *
First Oklahoma hospital to implement e-Referrals / 18 mos to complete
Utilize IHS EMR – RPMS
(Resource and Patient Management System)
Launch: Hospital - Nov 2014 / 4 clinics - Feb 2015
* U.S. Census Bureau, July 2015 / Kaiser Family Foundation, 2015
21AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Case Study:
Chickasaw Nation Medical Center
Total Referrals: 2,136 Clinics – 1,825; Hospital – 311
Adapted RPMS work around / SFTP – Secure File Transfer Protocol
◦ Batch referral files to be sent to Quitline / Encrypt them / Drag & drop from their server to the Helpline server
◦ Outcome reports – returned to hospital via SFTP encrypted/server to server
22AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Case Study:Mercy Health System
23
Already had an integrated EMR in hospitals and clinics – Epic
2½ years to build e-Referral capability into Epic / 5 years overall
65 clinics launched first – April 2015 launch - 1,640 referrals
Employee Wellness – Jan-March 2016 launch – 102 referrals
9 hospitals – 825 inpatient beds – 696 referrals
- Mercy OKC – 2015
- 5 rural hospitals – 2016
- 3 rural hospitals – 2017
Total Helpline e-referrals - 2,438
Required 1 FTE coordinator – shared cost with OHA/TSET
AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017
Case Study:OUMC Children’s Hospital,Perinatal-Neonatal Program
Part of University of Oklahoma Medical Center and O.U. Health Sciences Center
Level III NICU – 90 beds
Receives infants statewide and from Kansas
Large Medicaid population
Improve infant exposure to secondhand smoke upon discharge and improve post discharge healing
Requires 1 FTE coordinator/.5 FTE social worker/shared cost w/HHPQ
April 2016 – launched protocol in NICU
o screen neonatal parents and caretakers - best practice protocol embedded in NICU EMR – ‘CribNotes’
o E-fax - no need for outcome reports - family returns to local PCP
24AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Case Study:OUMC Children’s Hospital,Perinatal-Neonatal Program Screened over 780 parents/caretakers
85% of NICU admission parents/caretakers were screened for tobacco use
Of those, 49% received cessation services by NICU staff and referred to Helpline
Expanded to Prenatal Diagnostic Center 2017 – high risk pregnant patients
- 38 OB patients screened/assessed / 27 – Helpline referral
2017-2018 – expanding to Pediatric Cardiothoracic Surgery and Oklahoma Infant Transition Center
25AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017
Lessons Learned
When you’ve worked with one health
system,,,,,,
you’ve worked with one health system
26AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Lessons Learned
Tobacco treatment in health care settings must be embedded in
electronic medical records to be sustainable and include:
- Clinical workflow – best practice 5A’s
- FDA approved pharmacotherapy with dosing information
- Electronic referrals to quitlines – preferably direct messaging
- Returned outcome reports from quitlines to patient record
Large system implementation requires internal system resources
- Accountable administrative oversight
- Multi-disciplinary implementation committee
- Full time coordinator
- IT EMR support expertise
27AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

Lessons Learned
Permanent changes in health systems requires focused effort with funding and dedicated staff consulting and supporting – HHPQ/ TSET
Provider associations:
- are credible, trusted resources to help health providers
- help reduce hospital costs in making permanent changes
Support to health systems requires expertise in best practice, technology, and funding.
Resources are essential - staffing resources inside health systems
- financial support & external expertise to guide the process
Greatest impact is through larger multi-service health systems -includes urban and rural providers
Patience, patience, patience…….. this work takes time!
28AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017

HHPQ Staff
Contact Information
Joy L Leuthard, MS, LSWA
Manager, Health Improvement Initiatives
Eric Finley, MPH
Jennifer Roysdon, MS, TTS
Tobacco Treatment Systems Coordinators
Oklahoma Hospital Association
405.427.9537
29AMERICAN LUNG ASSOCIATION WEBINAR / MAY 24, 2017
Health Systems Change Initiative
Megan Whittet, MPH, Senior Cessation Manager
May 24, 2017

31
Overview
• Brief review on our approach to health
systems change
• Update on Health Systems Change Grants
• Update on Capacity Building Project

32
Health Systems Change
Support health systems to implement
changes to make tobacco dependence
treatment a standard and expected part of
health care

33
Health System Change Efforts
• Health Systems Change Grants
• Capacity Building Initiative
• Policy Initiatives

Health Systems Change Grants

35
Health Systems Change Grants
Fiscal Year 2014 Fiscal Year 2015
36
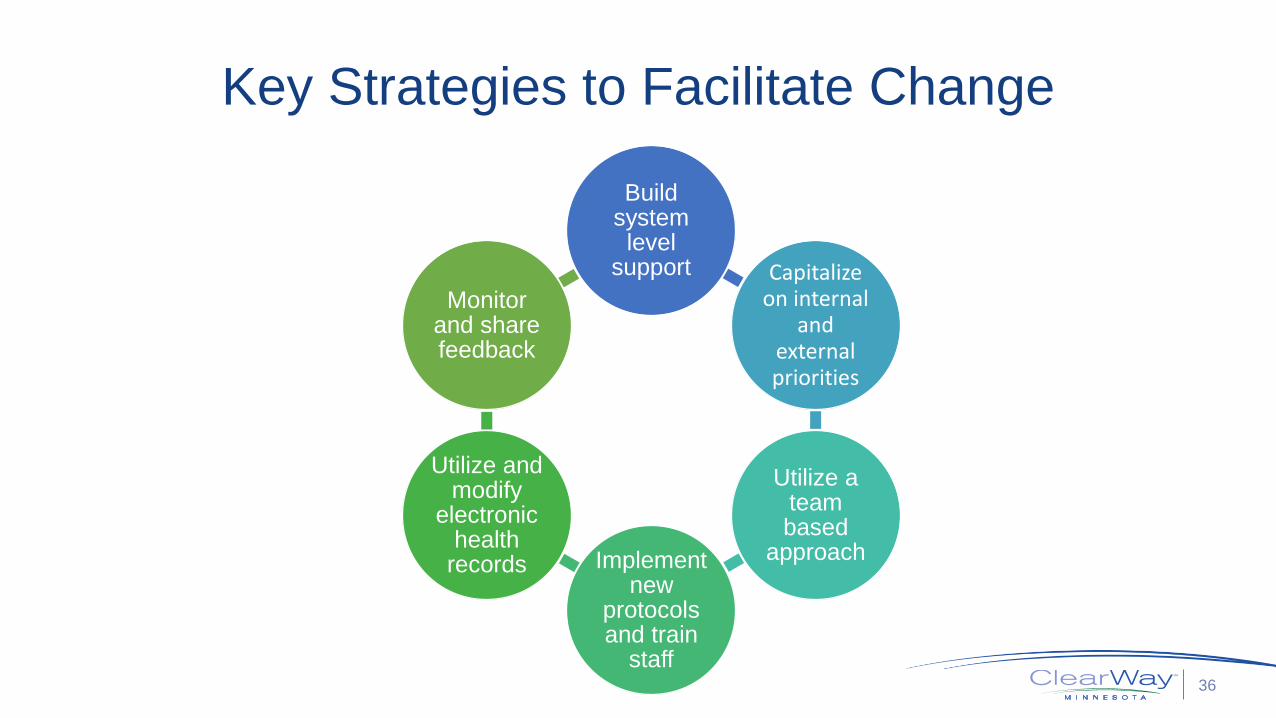
Key Strategies to Facilitate Change
Build system level
support Capitalize on internal
and external priorities
Utilize a team based
approachImplement new
protocols and train
staff
Utilize and modify
electronic health
records
Monitor and share feedback

37
Success!

38
Success Continued!

39
Key Challenges and Solutions
• Implementing Electronic Health Record (EHR) elements
– Work closely with IT staff from the beginning
– Pilot the EHR elements
• Reaching all staff, including new staff
– Use multiple repeated forms of communication
– Utilize new employee orientations
• Lack of funding for training staff and prioritizing systems
change
– Utilize current resources and processes
– Share existing data to help prioritize work among leadership

40
Sustaining the Work

41
Case Studies
http://clearwaymn.org/policy/cessation-policy/

Capacity Building Project

43
Capacity Building Initiative

44
Year One Activities
• Interest Group
• Trainings
• Practice Facilitation Coaching
• Communication and Resources

45
Interest Group
• 23 participants from a variety of:
– Health Systems and Clinics
– Health Plans
– State-wide Organizations
– State Agencies (i.e. DHS, MDH)
• Share insights and help inform the
capacity building activities

46
Rally Around Health Systems Change for Treating
Tobacco Dependence
• Almost 100 participants
• WHAT is health systems change and WHY
is it important
• 90% agreed or strongly agreed that they
gained an idea they will take back to their
organization or community

47
Regional
Workshops
• Total of 49 Participants
• Provide effective methods to help health
systems identify next steps to advance
tobacco systems change efforts

48
Practice Facilitation Coaching

49
Tobacco Systems Change Website
https://www.icsi.org/dissemination__implementation/practice_facilitation/tobacco_systems_change/

50
• Goes out to over 170
participants
• Every other month
• Includes a variety of
information and
resources

51
Reach Summary
• 159 Participants– 18 Who have been involved in more than one activity
• 66 Organizations – 18 Health Systems or Clinics
– 7 Community Health Centers/ FQHC
– 6 Native American Focus
– Others include Health Plans, State/Local Health &
Human Services, and Mental Health Organizations

52
Telling Our Story

53

5454
QUESTIONS?

5555
Contact:
Anne DiGiulio,
Manager, Lung Health Policy
202-719-2814