Embed Size (px)
Citation preview

Jones Fractures
Selene G. Parekh, MD, MBAAssociate Professor
North Carolina Orthopaedic ClinicDepartment of Orthopaedic Surgery
Adjunct Faculty Fuqua Business SchoolDuke University
Durham, NC919.471.9622
www.seleneparekhmd.com@seleneparekhmd

5th Metatarsal Fractures
• Consider in Zones
Jones fx
Diaphysealfx

Jones Fracture
• Fracture of the metaphyseal-diaphyseal junction• Must enter the 4/5 intermetatarsal articulation

Mechanism of Injury
• Vertical and mediolateral forces concentrated over the 5th MT
• Forced adduction• Can result in a fracture between shaft and
immobile base
• Greater propensity • Forefoot supination• Knee/ankle/hindfoot varus

Anatomy
• Peroneus brevis
• Peroneus tertius
• Abductor digiti minimi
• Lateral band of plantar fascia
• Plantar and dorsal interosseous
• Flexor digiti minimi brevis

Vascular Water-Shed
•Periosteal plexus
•Nutrient artery•Enters medial aspect of 5th MT at junction of proximal and middle third of bone
•Metaphyseal and diaphyseal vessels

Jones Fracture: Non-Op
• Indications• Elderly• Non-athletic• Low-demand
• Protocol• NWB cast 4-8 weeks
• 100 Fractures of 5th MT: Naval base• 72% union (avg. time 21.2 wks)Clapper, ClinOrth 1995

Jones Fracture: Non-Op
• Protocol• Orthotic
• No data

Jones Fracture: Operative
• Indications• Athlete
• Acute/stress fx• Active adult• Nonunion• Refracture• Cavovarus = lateral overload

Jones Fracture: Operative
• Operative goals• Expedite healing• Quicker recovery; easier rehab• Decrease nonunion rate• Decrease refracture risk

Jones Fracture: Operative
• Operative options• K-wiring and cast• Tension band wiring• IM curettage and casting• Mini-fragment screws• Low profile plates• IM screw fixation
• Open• Percutaneous

Jones Fracture: Operative
•Screw Fixation• Screw choices
• 4.5 mm malleolar (Synthes)• 5.0 mm cannulated (ACE/DePuy) • 6.5 mm short thread (Synthes)

Jones Fracture: Operative
•Nonunion after percutaneous screw fixation are all with Cannulated Screws or Small Screws

Jones Fracture: Operative
• Percutaneous Screw Fixation• Solid screw
• Large fragment screws
• Dedicated system• Cannulated bone preparation• Solid screw fixation

Jones Fracture: Set-up
• Supine
• Ankle block
• Mini C-arm• Flex knee and place foot on base

Jones Fracture: Approach
• Incision through skin only• 1 fingerbreadth proximal to base of 5th MT• Parallel to peroneals
• Mosquito through wound to base of 5th MT

Jones Fracture: Approach
• Solid screw into a curved bone

Jones Fracture: Approach
• Guide pin• Entry site extremely important• Start “high and inside”• Central in the canal on AP and lat views

Jones Fracture: Technique
• Entry drill• Tap to the correct screw diameter
• 4.5, 5.5, 6.5mm• Feel the 5th MT head torsional forces

Jones Fracture: Technique
• Measure length• Remove pin and drill guide• Place solid screw
• Chose the largest solid screw that comfortably” fits the canal
• Do not attempt to place down the entire MT

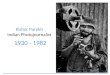
Insert Screw “High and Inside”
HIGH & INSIDE

Jones Fracture: Technique
• Failure to start “high and inside”• Prominent screw head• Perforation of medial cortexstress riser

Jones Fracture: Technique
• Avoid the headless tapered screw• Difficult to remove
• Avoid plate• Prominent• If removed refracture

Jones Fracture
• Postop management• NWB x 2 weeks• WBAT in boot x 4 weeks• Physical therapy

Jones Fracture
• Begin running in modified shoewear at 6-8 weeks if clinically nontender

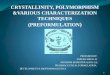
Jones Fracture
• Follow radiographs• Healing may not be evident for 12 weeks
12 wks p.o.

Jones Fracture
• Leave screw forever!

Pitfalls of IM Screw
• Infection• Delayed wound healing• Distal perforation (stress riser)• Sural neuritis/neuroma• Peroneal tendinitis• Persistent nonunion

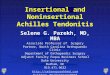
Jones Fracture Nonunion
• Hardware fatigue a sign of trouble

Jones Fracture Nonunion
• Cavovarus?• Adequate fixation?

Jones Fracture Nonunion
• If uncertain obtain CT

Jones Fracture Nonunion
• Open Surgical technique• Remove hardware• Open bone graft
• Iliac crest vs. allograft vs. substitutes vs. BMP• Re-fixation with largest screw

Jones Fracture Nonunion
• Dwyer for varus

RE ECT
the ankle
the foot