Embed Size (px)
Citation preview

Multi-Trauma and Complex Injuries
Hannah Gift, OTR/L, CHT, COMT, CEAS
St. Louis, MOApril 27-29, 2018
Learning Objectives
• Understand all systems involved and multi-system approach to mutilating hand injuries
• Identify healing phases, considerations and relationships within each tissue system and between multiple systems
• Understand complex balance between tissue systems and appropriate advancement through healing phases
• Understand principles and phases of Early Protective Motion
Introduction
Trauma to multiple anatomic systems of the hand resulting in a varied and complex
clinical picture
Photos by Gary Soloman, Nora Barrett
Systems (Tissues) • Therapist Hierarchy for Tissues
Vascular
Skin Coverage
Bone Stability
Nerve
Muscle/TendonTamai S. JHS, 1982, 7(6): 549‐556.
Vascular Structures &Considerations
Pictures provided by Nora Barrett
Vascular Structures
• Arteries- carry blood AWAY from the heart• Compromise- pale or white (“dusky”), cold
feeling, slow capillary refill
• Veins- carry blood back to the heart• Compromise- blue or purple in color, edema,
rapid capillary refill

• Redness—> extreme (mark area to track)• Heat—> increased temp• Pain or swelling—> sudden increase• Debris—> pus• Odor• Non-healing/new breakdown• Exposed bone
Inflammation vs. Infection
Pictures provided by Nora Barrett
• Elevation• At what level?
• Active exercise• Consider what is appropriate
• Compression• Contraindicated with vessel
repair until 6 weeks
• Physical agents
Managing Edema
Pictures provided by Nora Barrett
Manual Edema Mobilization
• MEM vs. MLD• Steps
• Diaphragmatic breathing • “Clear” exercises • Light skin traction• Massage Elbow Lymph nodes• “Flow” exercises
Picture from Howard & Krishnagiri, 2001).
Compartment Syndrome• 4 Ps:
• Pain (with passive stretch)• Paresthesias• Pallor• Pulselessness
• Compartments• Forearm- dorsal, volar, and mobile wad • Hand- interosseous, thenar, hypothenar, adductor
• Critical pressures: >30mm Hg, normal 8-10mm Hg
• Decompression
Pictures provided by Nora Barrett
Skin Coverage/Wound/Scarand Considerations
Pictures provided by Nora Barrett
Skin Coverage
• Types of Wound Closure • Primary Intention
• Secondary Intention
• Delayed Primary Closure
• Tensile Strength • Increases from day 5-30• By week 3: 15-20%• Healed wound 80%
Pictures provided by Nora Barrett
Whirlpool Guidelines• Whirlpools may be utilized for cleansing and
debridement of superficial necrotic tissue
• May stimulate granulation tissue, soften necrotic tissue and increase circulation
• Temperature- goal is 94*
Photo from prohealthcareproducts.com
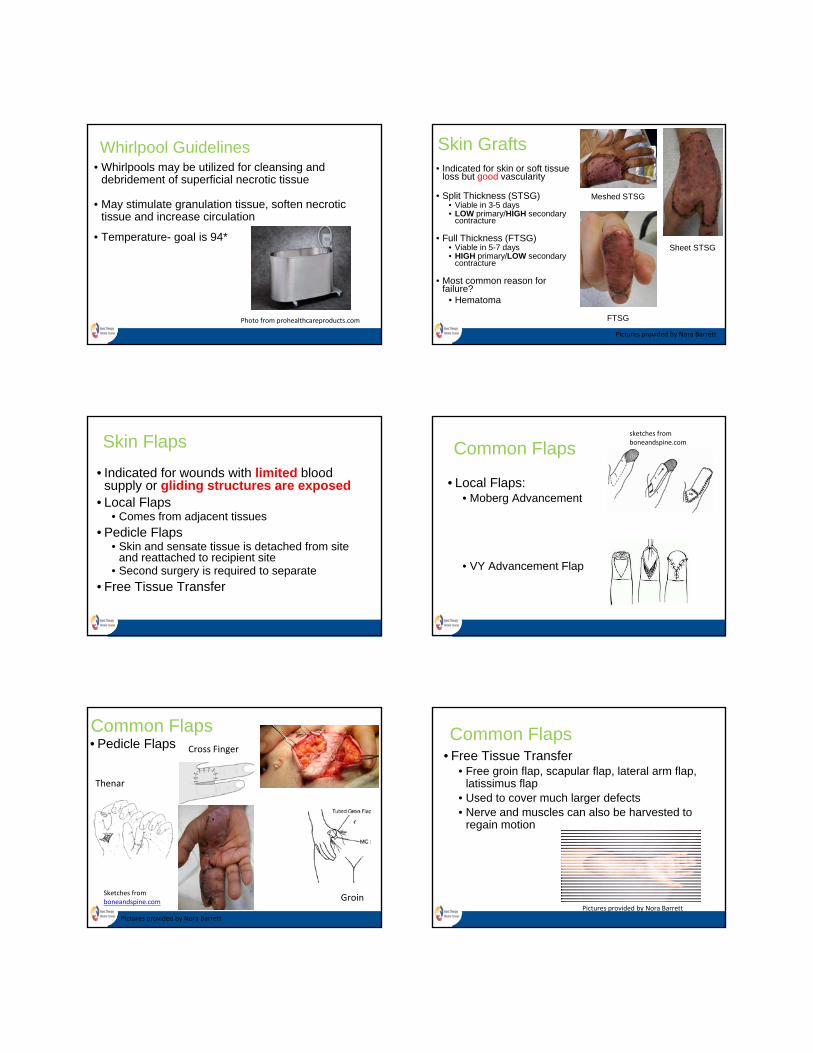
Skin Grafts • Indicated for skin or soft tissue
loss but good vascularity
• Split Thickness (STSG)• Viable in 3-5 days• LOW primary/HIGH secondary
contracture
• Full Thickness (FTSG)• Viable in 5-7 days• HIGH primary/LOW secondary
contracture
• Most common reason for failure?
• Hematoma
Meshed STSG
Sheet STSG
FTSG
Pictures provided by Nora Barrett
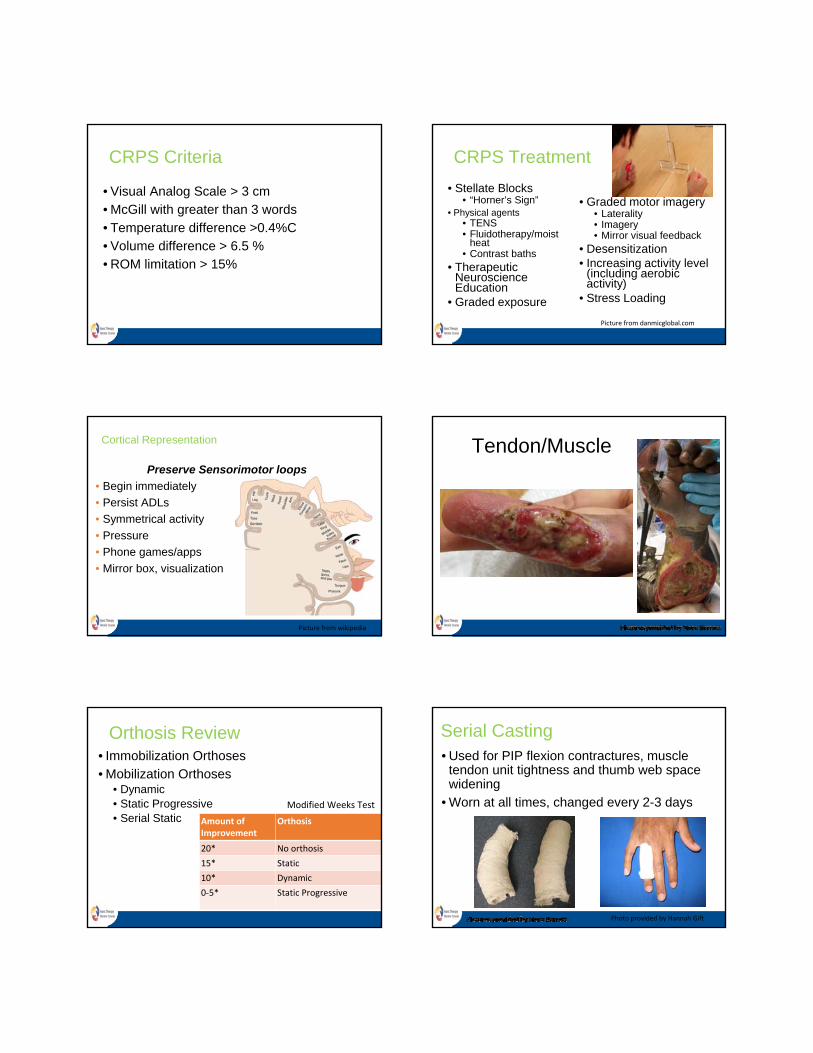
Skin Flaps
• Indicated for wounds with limited blood supply or gliding structures are exposed
• Local Flaps • Comes from adjacent tissues
• Pedicle Flaps• Skin and sensate tissue is detached from site
and reattached to recipient site• Second surgery is required to separate
• Free Tissue Transfer
Common Flaps
• Local Flaps:• Moberg Advancement
• VY Advancement Flap
sketches from boneandspine.com
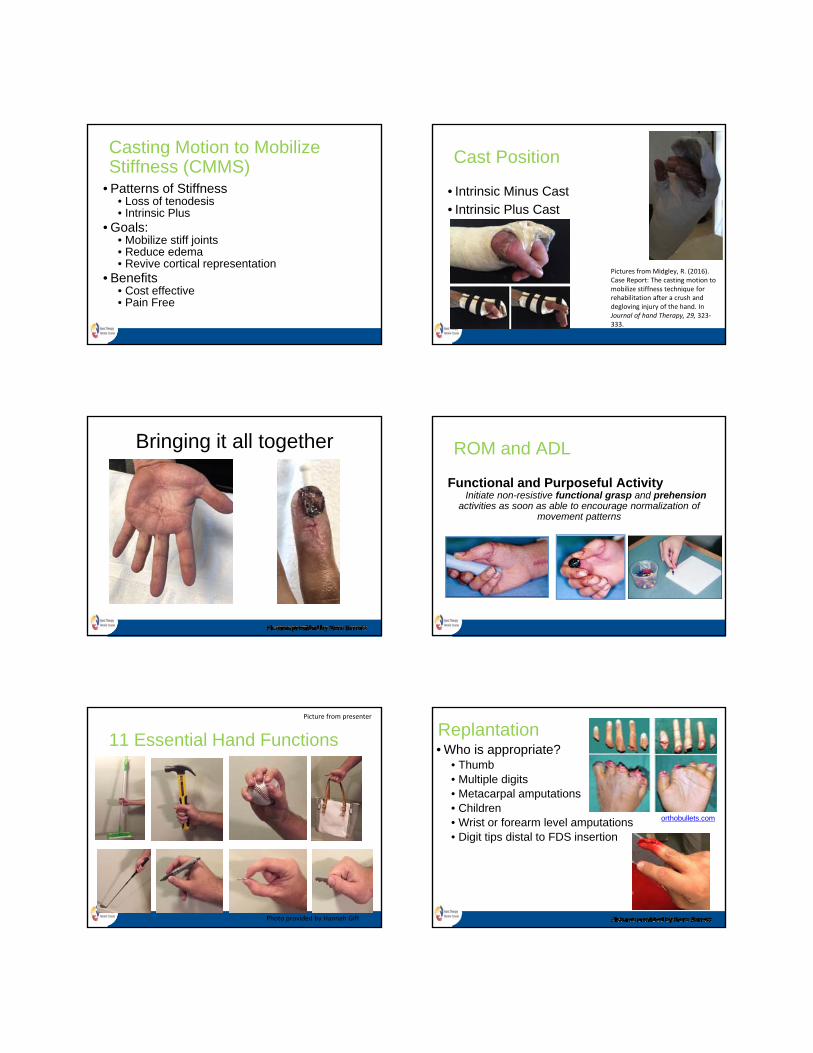
Common Flaps• Pedicle Flaps
Sketches from boneandspine.com
Thenar
Cross Finger
Groin
Pictures provided by Nora Barrett
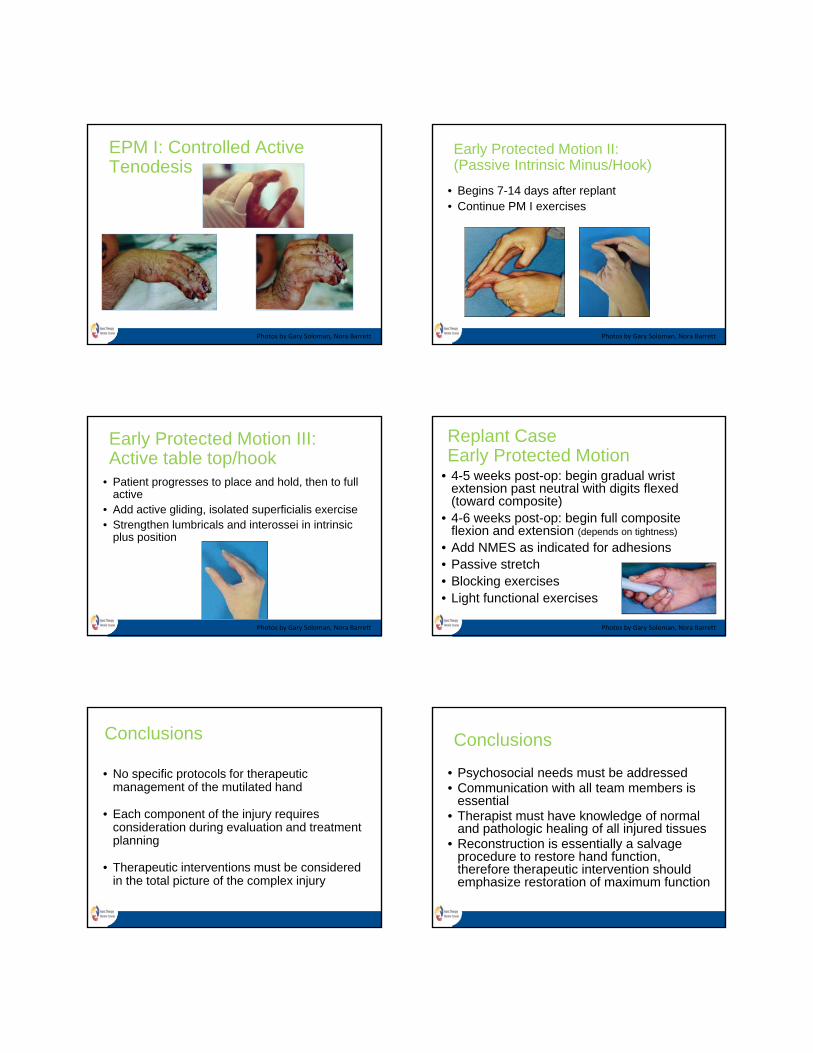
Common Flaps• Free Tissue Transfer
• Free groin flap, scapular flap, lateral arm flap, latissimus flap
• Used to cover much larger defects• Nerve and muscles can also be harvested to
regain motion
Pictures provided by Nora Barrett

ScarsHypertrophic• Bulky, elevated above
skin
• Occur soon post injury
• Severity of injury determines scar
• Found in areas of motion
• Associated with wound tension and timing
• Will improve with therapy and flatten in 1-2 years
Scars
Keloid• Beyond original injury site
• 15X higher in darker pigments
• Occurs from superficial or deep injuries
• May occur within first month, year, or several years
• Medications, radiation, surgical excision
Scar Management • Controlled motion• Transverse Friction Massage
• Continuous Pressure Garments
• Silicone Gel Sheeting, Paper tape
• Scar molds
• Orthoses
• Physical agents
Burns
• Causes of Injury:• Cutaneous • Cold• Chemical• Electrical
• Common Complications: • Edema• Joint deformities• Sensory impairment • Restricted use of the hand• Compartment syndrome
Depth of Burns• Epidermal
• Sunburn
• Partial Thickness• Superficial• Deep
• Full Thickness
• 4th degree• Circumferential burns
Burn Treatment• Biological Dressings/Wound Closures • Edema Management
• Range of Motion • Positioning • Physical Agents
• Scar Management • Pressure Therapy

Burn Orthosis OptionsBurns • Most common deformities
• Thumb web space contracture• PIP joint flexion contracture • Boutonniere deformity• Swan neck• “Claw hand”• Burn syndactyly• Palmar cupping
Skeletal System Amputation Levels • Finger• Partial Hand• Wrist Disarticulation• Trans-Radial• Elbow Disarticulation• Trans Humeral• Shoulder Disarticulation• Forequarter• Bilateral
Prosthetic Basics
1. No Prosthesis2. Passive
3. Body Power4. External Power5. Hybrid
6. Activity Specific
Pics from upperlimbprostheticsinfo.com
Residual Limb Care
• Performed with complete amputations or fingertip injuries
• Stump wrapping for shaping and edema control
• Desensitization for stump hypersensitivity
www.rehabmart.com
Photo from ncmedical.com

Nerves/PainPain
• “An unpleasant sensory and emotional experience associated with actual or potential tissue damage.” IASP
• CRPS is characterized by severe pain, swelling, stiffness, discoloration, and decreased function in an entire extremity or single digit.
Types of CRPS
• Type I: • Previously RSD• Develops after noxious event• DOES NOT have an identifiable nerve lesion
• Type II: • Previously causalgia• INCLUDES Injury to peripheral nerve or branch
Types of CRPS
• Sympathetically Independent Pain (SIP)• Occurring in the initial onset of the syndrome
• Sympathetically Maintained Pain (SMP)• “A symptom of CRPS but not a clinical entity”• Occurs after a period of time
CRPS Criteria • Criteria: 1. Presence of an inciting noxious event or a
cause of immobilization 2. Continuing pain, allodynia, or hyperalgesia
with which pain is disproportionate to an inciting event
3. Evidence at some time of edema, changes in blood flow, or abnormal sudomotor activity
4. Excluding existence of other condition which would cause similar symptoms
CRPS Criteria Symptom Sign
Sensory Hyperesthesia, allodynia Hyperalgesia, allodynia to light touch, movement, pressure
Vasomotor Temperature/skin asymmetry/color changes/asymmetry
Temperature asymmetry, skin color changes
Sudomotor/Edema Edema, hyperhidrosis, sweating changes asymmetry
Edema, sweating changes
Motor/Trophic Decreased ROM, motor dysfunction, trophic changes
Decreased ROM, motor dysfunction, trophic changes
CRPS Criteria
• Visual Analog Scale > 3 cm • McGill with greater than 3 words
• Temperature difference >0.4%C• Volume difference > 6.5 %• ROM limitation > 15%
CRPS Treatment
• Stellate Blocks• “Horner’s Sign”
• Physical agents• TENS• Fluidotherapy/moist
heat• Contrast baths
• Therapeutic Neuroscience Education
• Graded exposure
• Graded motor imagery • Laterality• Imagery • Mirror visual feedback
• Desensitization • Increasing activity level
(including aerobic activity)
• Stress Loading
Picture from danmicglobal.com
Cortical Representation
Preserve Sensorimotor loops
• Begin immediately
• Persist ADLs
• Symmetrical activity
• Pressure
• Phone games/apps
• Mirror box, visualization
Picture from wikipedia
Tendon/Muscle
Orthosis Review • Immobilization Orthoses • Mobilization Orthoses
• Dynamic• Static Progressive• Serial Static Amount of
ImprovementOrthosis
20* No orthosis
15* Static
10* Dynamic
0‐5* Static Progressive
Modified Weeks Test
Serial Casting • Used for PIP flexion contractures, muscle
tendon unit tightness and thumb web space widening
• Worn at all times, changed every 2-3 days
Photo provided by Hannah Gift
Casting Motion to Mobilize Stiffness (CMMS)
• Patterns of Stiffness• Loss of tenodesis• Intrinsic Plus
• Goals: • Mobilize stiff joints• Reduce edema• Revive cortical representation
• Benefits • Cost effective • Pain Free
Cast Position
• Intrinsic Minus Cast• Intrinsic Plus Cast
Pictures from Midgley, R. (2016). Case Report: The casting motion to mobilize stiffness technique for rehabilitation after a crush and degloving injury of the hand. In Journal of hand Therapy, 29, 323‐333.
Bringing it all together
Functional and Purposeful ActivityInitiate non-resistive functional grasp and prehension
activities as soon as able to encourage normalization of movement patterns
ROM and ADL
11 Essential Hand Functions
Picture from presenter
Photo provided by Hannah Gift
Replantation• Who is appropriate?
• Thumb• Multiple digits• Metacarpal amputations• Children• Wrist or forearm level amputations• Digit tips distal to FDS insertion
orthobullets.com

Replantation • Common order for replant:
• Clean wound• Skeletal system/periosteum• Extensor tendons• Flexor tendons• Nerves• Artery• Vein• Skin
Thumb Amputation
Photos by Gary Soloman, Nora Barrett
Thumb Replantation
Photos by Gary Soloman, Nora Barrett
Early Protective Motion(Silverman, 1989)
Rationale: Early Protected Motion (EPM)
Differential glide of tendons• Joint movement• Protection to hand from composite
motion which may disrupt repairs• Give enough tendon gliding without
tension to prevent adhesions
EPM Phases
• I• Controlled Active Tenodesis • Day 4-14
• II• Passive Intrinsic Minus• Day 7-14
• III • Active Intrinsic Minus• Day 14
Orthosis
Photos by Gary Soloman, Nora Barrett
EPM I: Controlled Active Tenodesis
Photos by Gary Soloman, Nora Barrett
Early Protected Motion II: (Passive Intrinsic Minus/Hook)
• Begins 7-14 days after replant• Continue PM I exercises
Photos by Gary Soloman, Nora Barrett
• Patient progresses to place and hold, then to full active
• Add active gliding, isolated superficialis exercise• Strengthen lumbricals and interossei in intrinsic
plus position
Early Protected Motion III: Active table top/hook
Photos by Gary Soloman, Nora Barrett
• 4-5 weeks post-op: begin gradual wrist extension past neutral with digits flexed (toward composite)
• 4-6 weeks post-op: begin full composite flexion and extension (depends on tightness)
• Add NMES as indicated for adhesions• Passive stretch • Blocking exercises• Light functional exercises
Replant CaseEarly Protected Motion
Photos by Gary Soloman, Nora Barrett
Conclusions
• No specific protocols for therapeutic management of the mutilated hand
• Each component of the injury requires consideration during evaluation and treatment planning
• Therapeutic interventions must be considered in the total picture of the complex injury
Conclusions
• Psychosocial needs must be addressed• Communication with all team members is
essential• Therapist must have knowledge of normal
and pathologic healing of all injured tissues• Reconstruction is essentially a salvage
procedure to restore hand function, therefore therapeutic intervention should emphasize restoration of maximum function

Acknowledgements
• Gary Solomon, MS, OTR/L, CHT• Nora Barrett, MS, OTR/L, CHT
• Hannah Gift, OTR/L, CHT
• Chan S & LaStayo P. (2003). Hand Therapy Management Following Mutilating Hand Injuries. In Hand Clinics, 19(1):133-148.
• Chee, N. Complex Traumatic Injuries. In Test Prep for the CHT Exam, 3rd Edition.
• Chung K & Alderman A. (2002). Replantation of the Upper Extremity: Indications and Outcomes. In Journal of the American Society for Surgery of the Hand, 2(2):78-94.
• Colditz, J. Therapist’s Management of the Stiff Hand. In Rehabilitation of the Hand and Upper Extremity, 6th edition. Skirven, Osterman, Fedorczyk & Amadio. Elsevier/Mosby: Philadelphia 2011.
• Hannah S. (2011). Psychosocial issues after a traumatic hand injury: facilitating adjustment. In Journal of Hand Therapy, 24(2):95-103.
• Hay, D., Taras, J. & Yao, J. Vascular Disorders of the Upper Extremity. In Rehabilitation of the Hand and Upper Extremity, 6th edition. Skirven, Osterman, Fedorczyk & Amadio. Elsevier/Mosby: Philadelphia 2011.
• Howard, S. & Krishnagiri, S. (2001). The use of manual edema mobilization for the reduction of persistent edema in the upper limb. In Journal of Hand Therapy, 14(4), 291-301.
• Jones NF, Chang J & Kashani P. The Surgical and Rehabilitative Aspects of Replantation and Revascularization of the Hand. In Rehabilitation of the Hand and Upper Extremity, Sixth Edition. Skirven, Osterman, Fedorczyk & Amadio. Elsevier/Mosby: Philadelphia 2011.
• Levin LS. Management of Skin Grafts and Flaps in Rehabilitation of the Hand and Upper Extremity, Sixth Edition. Skirven, Osterman, Fedorczyk & Amadio. Elsevier/Mosby: Philadelphia 2011.
References
• McVeigh, K., Herman, M. & Laney, B. Wound Healing. In Test Prep for the CHT Exam, 3rd Edition.
• Midgley, R. (2016). Case Report: The casting motion to mobilize stiffness technique for rehabilitation after a crush and degloving injury of the hand. In Journal of hand Therapy, 29, 323-333.
• Monroe, B. Amputations and Prosthetics. In Test Prep for the CHT Exam, 3rd Edition.
• Neumeister M. & Brown R. (2003). Mutilating Hand Injuries: principles and management. In Hand Clinics 19(1): 1-15.
• Pettengill K. Therapist’s Management of the Complex Injury in Rehabilitation of the Hand and Upper Extremity, Sixth Edition. Skirven, Osterman, Fedorczyk & Amadio. Elsevier/Mosby: Philadelphia 2011.
• Rizzo M. Complex Injuries of the Hand in Rehabilitation of the Hand and Upper Extremity, Sixth Edition. Skirven, Osterman, Fedorczyk & Amadio. Elsevier/Mosby: Philadelphia 2011.
• Silverman P., Willette-Green V & Petrilli J (1989). Early Protective Motion in Digital Revascularization and Replantation. In Journal of Hand Therapy, 2:84-101.
• Stanton, D., Pigott, R.. Orthotic Fabrication and Biomechanics. In Test Prep for the CHT Exam, 3rd edition.
• Thurlow, M. & Anderson, P. Burns. In Test Prep for the CHT Exam, 3rd Edition.
• Villeco J. Edema: Therapist’s Management in Rehabilitation of the Hand and Upper Extremity, Sixth Edition. Skirven, Osterman, Fedorczyk & Amadio. Elsevier/Mosby: Philadelphia 2011.
• Westlake K. & Byl N. (2013). Neural plasticity and implications for hand rehabilitation after neurological insult. In Journal of Hand Therapy, 26(2):87-93.
63















![Intentional Replantation: An Updated Protocols in ... · conventional treatment, and accidental avulsion (unintentional replantation) [8]. On the other hand, contraindications of](https://img.dokumen.tips/doc/110x75/5ed55ef56933f508e973f125/intentional-replantation-an-updated-protocols-in-conventional-treatment-and.jpg)










![[PVG] Hannah Montana - Hannah Montana 3](https://img.dokumen.tips/doc/110x75/56d6bf381a28ab30169562c0/pvg-hannah-montana-hannah-montana-3.jpg)


