Embed Size (px)
Citation preview

LEARNING FROM MULTIPLE RESULTS-
BASED FINANCING SCHEMES: AN ANALYSIS OF THE POLICY PROCESS FOR
SCALE-UP IN UGANDA (2003-2015).
Research report UGANDA
26-Oct-15
Assoc. Prof Freddie Ssengooba (MBChB, MPH, PhD)
Dr Elizabeth Ekirapa ( MBChB, MPH, MPH(HE),PhD)
Dr Timothy Musila (MBChB,MSc,MBA)
Dr Aloysius Ssennyonjo ( MBChB, MSc.,PGDM&E, AMRSPH)
Makerere University School of Public Health and Ministry of Health
This study is part of multicounty study titled “Implementation research: Taking Results Based
Financing from scheme to system” funded by the Alliance for Health Policy and Systems Research

i
ACKNOWLEDGEMENTS
This Policy analysis of Results-Based financing (RBF) development in Uganda has benefited
greatly from the contributions of a large number of individuals, groups and organizations. We
thank them all on behalf of the Study Team.
First, we wish to acknowledge the funding of the project by the Alliance for Health Policy and
Systems Research (AHSPR).Thanks are due to members of Technical Support team at
Institute of Tropical Medicine, Antwerp lead by Prof Bruno Meessen for their support.
The great contribution of the Project Consultants- Dr. Solome Bakeera and Mr. Aloysius
Mutebi is acknowledged and appreciated.
A range of stakeholder groups gave generously of their time, assistance and support,
particularly during data collection process. The special word of thanks goes, of course, to the
respondents who participated in the Study.
The energy and dedication of the research team (Ms. Racheal Bakubi, Jackie Mwendeze, Ms.
Prossy Aliweebwa, Ms. Resty Nakayima and Mr Victor Guma) in conducting and
transcribing the interviews as well as contributing during data analysis were tremendous.

ii
TABLE OF CONTENTS
Acknowledgements ..................................................................................................................... i
Table of Contents ....................................................................................................................... ii
List of illustrations ..................................................................................................................... v
Acronyms .................................................................................................................................. vi
Executive Summary ................................................................................................................. vii
CHAPTER 1: INTRODUCTION .............................................................................................. 1
1.1. Introduction: ................................................................................................................ 1
1.2. Background and rationale ............................................................................................ 1
1.3. Study Objectives .......................................................................................................... 2
1.4. Overview of Uganda’s Health system ......................................................................... 2
1.5. Key definitions ............................................................................................................ 3
1.6. Structure of the Report ................................................................................................ 4
CHAPTER 2: CONCEPTUAL FRAMEWORK ....................................................................... 5
2.1 Introduction ............................................................................................................ 5
2.2 Scaling up and integrating an RBF intervention: a multidimensional reality . 5
2.3 Descriptive work: Appreciating the progress of the RBF schemes (‘scale up
process’) ............................................................................................................................. 5
2.4 Analytical work ...................................................................................................... 7
CHAPTER 3: METHODOLOGY ............................................................................................. 9
3.0 Introduction ................................................................................................................. 9
3.1 Research Questions ...................................................................................................... 9
3.2 Research Design .......................................................................................................... 9
3.3 Instruments .................................................................................................................. 9
3.4 Sample ....................................................................................................................... 10
3.5 Data Collection .......................................................................................................... 10
3.5 Data Analysis ............................................................................................................. 11
3.6 Ethical considerations ................................................................................................ 11
3.7 Limitations ................................................................................................................. 11
CHAPTER 4: DESCRIPTION OF RESULTS-BASED FINANCING INITIATIVES IN
UGANDA. ................................................................................................................................ 13
Introduction: .............................................................................................................. 13 4.1
Types of RBF schemes implemented in Uganda (2003-2015) .................................. 13 4.2
Description of Supply side-RBF schemes in Uganda: .............................................. 13 4.3
4.3.1 The World Bank Performance-Based contracting (PBC) Study (2003-2005) .. 13

iii
4.3.2 The Cordaid project (2009-2015) ....................................................................... 15
4.3.3 The NuHealth project (2011-2015) .................................................................... 16
4.3.4 Strengthening Decentralization for Sustainability (SDS) (2010-2016) ............. 18
Evolution of Demand-side RBF Schemes ................................................................. 19 4.4
4.4.1 The World Bank Reproductive health Voucher Project (2006-2011) ................ 20
4.4.2 The Safe Deliveries Project (SDP) (2009-2011) ................................................ 21
4.4.3 The Saving Mothers Giving Life (SMGL) Initiative (2012-2017). ................... 23
Conclusion: ................................................................................................................ 29 4.5
CHAPTER5: THE MULTIDIMENSIONAL SCALE UP OF RBF IN UGANDA ................ 30
5.1 Introduction ............................................................................................................... 30
5.2 Population coverage .................................................................................................. 30
5.3 Service coverage ........................................................................................................ 32
5.4 Health systems integration ......................................................................................... 33
5.4.1 Areas of Integration ............................................................................................ 33
5.4.2 Depth of integration: .......................................................................................... 36
5.5 Scale up along Knowledge dimension ....................................................................... 39
5.5.1 Appreciation of the benefits of RBF towards improving Health systems
performance has progressed. ............................................................................................ 40
5.5.2 Cross learning among schemes has improved but slowly: ................................. 40
5.5.3 Progress in knowledge of key design and Implementation considerations: ....... 41
5.6 Conclusion ................................................................................................................. 42
CHAPTER 6: FACTORS AND ACTORS THAT INFLUENCED RBF DEVELOPMENT IN
UGANDA ................................................................................................................................. 43
6.1 Introduction ............................................................................................................... 43
6.2 Factors shaping RBF development in Uganda: ......................................................... 43
6.2.1 Contextual factors and their influence on national RBF scale-up. ..................... 43
6.2.2 Sharing and Utilisation of RBF evidence as determinant of buy-in and scale-up.
49
6.3 Prospects and recommendations for national RBF scale-up ..................................... 52
6.3.1 Prospects for RBF to become national policy .................................................... 52
6.3.2 Recommendation for RBF to become a national strategy: ................................ 53
6.4 Conclusion ................................................................................................................. 55
CHAPTER 7: DISCUSSION ................................................................................................... 57
7.1 Introduction ............................................................................................................... 57

iv
7.2 RBF Aspects that have moved/not moved and why? ................................................ 57
7.3 Progression of Implementation experience ............................................................... 58
7.4 Contextual Factors shaping RBF evolution ............................................................... 59
7.5 Future design considerations: .................................................................................... 60
CHAPTER 8: CONCLUSIONS AND RECOMMENDATIONS ........................................... 62
8.1 CONCLUSION ......................................................................................................... 62
8.2 RECOMMENDATIONS ........................................................................................... 63
List of References ..................................................................................................................... 65
Reviewed sources (Documents,websites ETC). ....................................................................... 67
Annex 1: List of Respondents .................................................................................................. 72
Annex 2: Consent form ............................................................................................................ 73
Annex 3: Generic interview guide .......................................................................................... 76
Annex 4: Coding framework for Document review ................................................................. 79

v
LIST OF ILLUSTRATIONS
Figure 1: Model for World Bank PBC study (Source: Authors). ............................................. 14 Figure 2: The Cordaid Project Model (Source: Authors) ......................................................... 16 Figure 3: NuHealth Pilot model (Source: authors) ................................................................... 17 Figure 4: SDS Program model (Source: Authors). .................................................................. 19 Figure 5: RHV Project Design (Source: Adapted from Project Operational Manual 2007; 6).
.................................................................................................................................................. 20 Figure 6: The Safe Deliveries Project Model ........................................................................... 22 Figure 7: The institutional design of the SMGL Project in Uganda (Source: Authors) ........... 24 Figure 8: Timeline for multi-dimensional scale up of RBF in Uganda.................................... 31
Table 1: Table showing categories of respondents .................................................................. 10 Table 2: Performance indicators for World Bank study........................................................... 14 Table 4: Design features of RBF schemes implemented in Uganda ........................................ 26
vi
ACRONYMS
AHPSR: Alliance for Health Policy and Systems Research.
BTC: Belgian Development agency.
CIDA: Canadian International Development Agency
DFID: Department of International Development
GBOBA: Global partnership for Output-based Aid
GoU: Government of Uganda
HFS: Health Financing Strategy
HSDP: Health Sector Development Plan
ITM Institute of Tropical Medicine, Antwerp
MakSPH: Makerere University School of Public Health
MoFPED: Ministry of Finance, Planning & Economic development
MOH: Ministry of Health
MoPS: Ministry of Public Service
NuHealth: Northern Uganda Project.
OBT: Output-Based Budgeting Tool
PBC: Performance-based Contracting
PBF: Performance-based financing
PNFP: Private-Not-For-Profit
RBF: Results Based Financing
RHV: Reproductive Health Voucher
SDP: Safe Deliveries Project
SDS: Strengthening Decentralization for Sustainability
SMGL: Saving Mothers Giving life Initiative
UCMB: Uganda Catholic medical Bureau.
UHC: Universal health Coverage
UNMHCP: Uganda National Minimum Health care Package
UNMHCP: Uganda National Minimum health care Package.
USAID: United States Agency for International Development
WB: World Bank
WHO: World Health Organisation

vii
EXECUTIVE SUMMARY
Background
Results-Based Financing (RBF) that links payments to providers or consumers to quantitative
or qualitative indicators has been increasingly used as a means to improve the performance of
health systems and help systems to move towards universal health coverage. However, in
many low-income countries like Uganda, little progress has been made in scaling up or
integrating RBF pilot projects into national health system. There is need for evidence on how
to foster scaling up of such RBF. This study is part of a multi-country research supported by
Institute of Tropical Medicine (ITM), Antwerp and the WHO Alliance for Health Policy and
System Research (AHPSR). It aims at documenting and analyzing the development (scaling
up) process of RBF in Uganda from Jan/2003 to March/2015 and draw lessons for further
scaling up and sustaining such initiative, nationally and internationally.
Methodology
This is a qualitative research and the data was collected through document/literature review,
key informant interviews and participant observation. The documentation part hinged on
descriptive work focused on scaling up as a policy process. First, a time line reporting the
different key steps in the scale up and the phenomena which triggered them was developed.
We then investigated the dynamics (process, context, content and actors) that enabled or
hindered the scaling up decision and/or implementation of the RBF. Thirty eight 38
individuals were interviewed and their current views on enablers, barriers, prospects and
prerequisites for scale up and integration of RBF into national health system and policy were
gathered. Additionally, participant observation was undertaken in early 2015 and proceeding
of the national multi-stakeholder national consultative meeting on RBF guided the analysis of
prospective role of RBF in Uganda‘s health sectors. Data was analysed manually for emergent
themes. Ethical review and approval from the Higher Degrees, Research and Ethics
Committee of Makerere University School of Public Health and the Uganda National Council
for Science and Technology (UNCST) and WHO Ethics Review committee was obtained
prior to primary data collection.
Key Findings
This study covered a total of 7 RBF initiatives that have been implemented in Ugandan health
sector since 2003. Table 3: Design features of RBF schemes implemented in Uganda)
elaborates the main feature of the various schemes. Generally, Uganda has seen both supply
side and demand side RBF schemes. The supply side schemes discovered included the World-
bank Study (2003-2005), the Cordaid Pilot (2009-2015), the NuHealth project (2011-2015),
and the proposed BTC/MoH Pilot project (2015-2019). Another program, the Strengthening
Decentralisation for Sustainability (SDS) is managed under Ministry of Local government and
provides performance-based grants to districts to deliver social services including health. On
the hand, several demand-side schemes (essentially vouchers) have been implemented in
Uganda. These Included the Reproductive Health Voucher Project by World bank (2006-
2011), the Safe deliveries project (2009-2011) and follow on Maternal & New-born study
(MANEST) (2011-2015), the Health Baby Voucher Project under Saving Mothers Giving
Life (SMGL) Initiative and proposed Reproductive health voucher project II (2014-2019).
This study covered the multidimensional evolution of RBF in Uganda. To capture this
complex phenomenon a timeline of the key milestones for RBF development over the last 12

viii
years is provided a long four dimensions of scale up namely service coverage, population
coverage, health system integration and Knowledge.
The scale-up in population coverage did not follow a systematic process and was contingent
on the specifications of the RBF schemes. Almost all regions in the country have had RBF
schemes but the western region has had the most number of pilots. Regarding service
coverage, it was noted that all demand side schemes offered package under Maternal and
Child Health services. Supply side pilots provided more comprehensive packages from the
UNMHCP. However, NCDS were notably unconsidered by all the schemes. There is also
little progress in implementing RBF in public facilities.
Regarding Health system integration, a mixed picture was found as some areas have
progressed compared to others. Regarding alignment with /governance structures, RBF has
worked closely with Districts bypassing the national level. RBF is still incompatible with the
public service Human resource systems. Furthermore, there is still need to consider how RBF
aligns with other financing reforms such as National Health insurance and Resource
allocation formula. On the other hand, RBF has resulted in progress in HMIS by encouraging
quality data management. Regarding institutionalisation, there are recent pointers to formal
institutionalisation processes such as setting up of Technical Working group at MOH and
explicit reference to RBF in the HSDP and Health financing Strategy.
Several contextual factors influencing RBF development in Uganda were given. These
contextual factors were divided into those external and internal to the country. The internal
factors were sub divided into those within and without the health sector. The subsequent
section summarised the emerging themes. External factors included Donor influence, the
global movement towards specific targets and policy transfer/importation of evidence.
Internal factors supportive of RBF included dissatisfaction of government about current poor
results and concern about rampant corruption scandals. Leadership/governance gaps and
health systems/ sector issues were noted to have a negative effect.
Regarding knowledge development & sharing, it was found that knowledge about the benefits
of RBF had improved however, mainly among implementers and academics. Several methods
of information sharing were noted. These included informal face to face interactions to more
formal multi sectoral meetings and field visits. Generally certain aspects have moved:
Knowledge about schemes that have been implemented in Uganda was very good among
academics and implementers but poor among national level policy makers. There has been
progress on dimension of knowledge regarding good practices under RBF design and
implementation. These included how to use resources/bonuses optimally, improvement of
robust information systems and establishment of correspondent with district leadership.
Consequently, implementation capacity has grown where implementation has taken place.
Interest at national level has also progressed evidenced by recent inclusion of RBF into HSDP
and Health Financing strategy. There was also evidence of action within government to
develop out-put based budgeting. However, these were noted to be deficient and not
practically framed based on RBF principles. There was some evidence that cross learning has
taken place where schemes learnt from others.
Conversely, it was noted that certain aspects such as establishing of complementary
institutions and public sector reforms have not moved and generally, the progression has been
slow. This was attributed to a number of reasons including the general lack of interest in RBF
among some policy makers despite evidence bring provided regarding the benefits of the
same. Other reason for low buy in included pointed to design issues. These included designs
being expensive, lack of effective mechanisms to share information, insufficient information

ix
especially on costs, and bias arising from failure of first schemes. There was also skepticism
that RBF can be a magic bullet to address the health systems constraints affecting
performance.
Two national workshops on RBF have been held in the country over the last two years. The
first was on March 16th
2014 and the second was held on 16-17th
February 2015. An overview
the key matters arising from the second national consultation workshop on RBF were
provided: RBF has to be discussed in light of UHC agenda. Despite the positive results, RBF
is not panacea and perverse effects should be anticipated and mitigated for. To advance, RBF
certain preconditions have to be met-such as ensuring that all facilities have adequate capacity
to function, filling the financing gap and separation of power, roles and responsibilities
especially under decentralised system. It was thus recommended that RBF implementation
should be supported by clear learning agenda. More so, central level coordinating Unit should
be established at MoH to steer the RBF agenda in Uganda.
The study also covered prospects and recommendations for RBF to become national policy.
Regarding RBF becoming integrated into national system, prospects were reported to be
generally good among the respondents but most indicated that adoption of RBF depends
greatly on sustained action being taken. The respondents also gave view on the aspects that
should be modified or taken into consideration as Uganda adopts RBF. These included Health
systems strengthening, capacity building, enacting policy changes (e.g permanent public
service contracts) and several design and implementation considerations. Key design issues
related to autonomy of facilities, performance tracking and separation and articulation of
roles.
Key Recommendations
We subsequently underscore several issues that need attention of the policy makers to ensure
that RBF works in the Ugandan context.
RBF has to be strategically debated as contributing the UHC agenda. The MoH should
develop an implementation plan that clearly articulates how RBF will be integrated/
combined with all strategies that the country will adopt as its path toward UHC.
Evidence/ information sharing efforts should be strengthened. The Ministry of Health and
her partners should create opportunities to share information on RBF.
The MOH has established a task force on RBF in the country. To institutionalise this
technical capacity, the MOH should set up an RBF technical unit in the MoH to
coordinate RBF efforts and synthesize evidence and lead stakeholder engagements.
The BTC/MOH project under development should have a clear and transparent research
agenda to ensure that the lessons learnt feed back into the decision making processes. This
should allow room for experimentation and flexibility to modify what may not work.
The accumulated local capacity should harness for example by setting up an
implementers’ forum or community of practice to ensure that the expert community is
continuously engaged.

x
MOH or government must develop strategy to uplift health facilities such that they reach
level of functionality. However, this must be informed by existing resource envelop.
Costing information on RBF is still dismal and yet this information is very important to
policy makers and technocrats in the ministry of finance to ensure that RBF is affordable
and sustainable. Costing of the benefit package should be done to inform decision making.
The prerequisite policy changes for RBF to take root in Uganda such as autonomy of
health facilities, separation of roles and revision of terms of reference under public service
have to be addressed.
Any future RBF model should be implemented within existing decentralized governance
structures. RBF initiatives should incentivize governance and leadership at both upstream
and downstream levels to reinforce the necessary complementary leadership and
governance systems.
1
CHAPTER 1 : INTRODUCTION
1.1. Introduction:
This section introduces the background and rationale for the study. It then gives the objectives
of the study. This is followed by the contextual background that mainly provides an overview
of Uganda’s health system. Finally, the structure of the report is given.
1.2. Background and rationale
Results-Based Financing (RBF) that links payments to providers or consumers to quantitative
or qualitative indicators has been increasingly used as a means to improve the performance of
health systems and help systems to move towards universal health coverage [1,2].For
example, Meessen et al (2010) [1] asserts that RBF “can address the problems of low
responsiveness, poor efficiency and inequity in the public health system.” They further note
that such reforms can lead to spillover effects outside the health system such as restructuring
of public finance management systems towards better performance.
In low and middle-income countries, while some of these mechanisms have successfully
scaled up nationwide and well integrated in the national health system as is the case in
Rwanda [1], many others remain at their early stage of implementation, as pilot or
demonstration projects [1,3].Further scaling up of these mechanisms requires better
understanding of the factors which enable or hinder such process.
While scaling up of effective health interventions or strategies is considered essential to
benefit more people, there is limited documented evidence on how to foster such scaling up
process, particularly on RBF. This seems to be the case in Uganda where a number of RBF
initiatives have been implemented as standalone projects with little integration of RBF into
the national health system [4,5, 6,7,8]
We contribute to bridge this evidence gap by conducting a case study, as part of a multi-
country research initiative supported by the Alliance for Health Policy and Systems Research
(AHPSR), to examine how RBF in Uganda has been developed (scaled up) and investigate the
extent to which RBF initiatives were successfully scaled up and why? We explored
evolutionary journey of all RBF schemes (hence force jointly referred to as RBF) that have
been implemented in Uganda over the last 10 years. The schemes studied included supply side
pilots and demand-side Voucher schemes.
Despite the general conclusion that RBF in Uganda did not attain optimal integration, we
view these schemes as actual opportunities that the country had (and still has for the ongoing
experience) to learn and move forward with the RBF agenda. We therefore intended to
understand the reasons why these schemes were not brought to scale at national level and the
extent to which the pilots themselves were barriers or enablers for the progress of the RBF
idea in Uganda. We also intended to identify major learning experiences by exploring the
changes that these schemes have elicited within the health system (more so among the
participating institutions and organizations) and the influence of these RBF initiatives on
national health policy.
In brief, this study aimed at documenting and analyzing the development process of RBF
in Uganda from Jan/2003 to March/2015 and draw lessons for future scaling up and
sustaining.
2
We then investigated the dynamics (process, context, content and actors) that enabled or
hindered the scaling-up decisions and/or implementation of the RBF. This work was
carried out in Uganda, but also in 10 other countries (by other research teams involved in this
research program). This large set of countries will allow drawing lessons from cross-country
comparisons.
The second component of our research is more specific to Uganda. There seems to be
growing momentum around RBF in Uganda. Two national consultation workshops have been
held on RBF. The first meeting was on 16th March 2014 and the second one on 16-17th
February 2015. We explored the determinants of dynamics around RBF in Uganda between
March 2014 and May 2015. We particularly deepened our understanding of current
determinants (enablers and barriers) to scale up by undertaking participant observation at a
multi-stakeholder national consultative meeting on RBF organized in February 2015. As
participant observers during this meeting, we were able to understand the current debates on
RBF and explanations for the same.
1.3. Study Objectives
1. To explore the evolution of RBF policy (2003 – 2015) with focus on the RBF
schemes, the actors involved, their motivation, cross linkage between schemes (cross
learning) and linkage into national health policy process.
2. To measure and understand the extent to which scale up has been achieved on several
dimensions in Uganda.
3. To understand the barriers and enablers for buy-in and integration of RBF into
national health policy and system.
4. To explore the determinants of the observed dynamics regarding RBF at national level
in Uganda between March 2014 to May 2015.
1.4. Overview of Uganda’s Health system
The overall stewardship of the Ugandan health sector is under the Ministry of Health (MoH)
which works in conjunction with other line ministers and local governments. The health
sector is composed of both public and private sub-sectors which play an important role in
delivery of health services with each reported to cover about 50% of the reported outputs
according to the Uganda demographic and health survey 2011 [ 9]. The Uganda National
Minimum health care Package (UNMHCP) was developed as basic package of health care
services to be provided through both sub-sectors. The Public health system consists of district
health system (including communities, Village health teams, health centres –HCs II, III and
IV and general Hospital) under the supervision of local governments and the semi-
autonomous Regional Referral Hospitals and National referral Hospitals [10]
The functionality of lower health facilities is still poor and is further undermined by
challenges across the health systems building blocks such as limited management capacity of
district health teams and Ministry of Health, inadequate funding, poor infrastructure and
shortage and low motivation of the health workforce. Stock outs of medicines and other health
supplies are also prevalent. There are also challenges in harnessing the potential of a
dominant yet diverse private health sector (comprising of both private for profit (PFPs) and
Private not for profit). In relation to public private partnerships, private not for profit (PNFPs)
facilities are enjoying a close collaboration with Government through their bureaus that
undertake self-regulation and coordination. However, it is much more difficult to deal with
the private for profit that is much diverse ranging from formal to informal health practitioners
and medicine-peddlers [11].

3
Regarding health financing, there are six sources of funds in Uganda including government
revenue, donor grants/loans, households, employers, philanthropic actors and NGOs [12]. In
terms of purchasing methods, public funds are used to pay for health services in the public
facilities and to subsidize in PNFP with salaries and line item budgets as the provider payment
methods. Such passive payment methods create no incentive for efficient use of resources but
a new government needs-based allocation formula that considers mortality indicators, number
of live births and population size as proxies is being piloted to determine disbursements to
districts and improve equitable resource distribution [11]. The private wings of public
hospitals, PNFP and Private Health Providers (PHP) are financed through user-fees which
undermine equity and efficiency in health financing [10]. Nabyonga, Criel et al (2011) [13]
reported that household surveys showed an increase in the out-of-pocket expenditures over
the period 2000 to 2006 despite abolition of user fees in Uganda in 2001.
In light of the above context, the Ugandan Health Systems Assessment 2011 [11] noted and
recommended a number of areas that need to be addressed to improve the performance of
health system namely: 1)re-alignment of resources in health sector to focus on the poor,2)
improve efficiency to reduce and control costs throughout the system,3) establish the required
institutions and systems to improve quality 4) Harness the potential of Uganda’s private
health sector to reduce inaccessibility to health care,5)strengthen coordination of all health
stakeholders to integrate the health system, 6) Tap into consumer power to advocate for
better health care.
In order to address the above critical intervention areas and to harness the benefits of RBF to
improve health systems performance, a number of RBF schemes have been implemented in
Uganda over the last decade. However, these have not resulted in the integration of RBF into
national health system. We therefore adopted a Policy analysis approach to understand the
slow progress towards integration of RBF into national system and policy. We explored
evolutionary journey all RBF schemes that have been implemented in Uganda over the last 10
years to understand what motivated the various actors, their experiences, the processes
followed and key decisions taken, cross learning among the schemes and linkages of schemes
into national policy processes.
1.5. Key definitions
Some of the key concepts used in this research are defined below:
We define Results Based Financing (RBF) as a purchasing mechanism that links payments
(to producers or consumers) to process or output measures (which may be quantitative or
quality measures or a mix of both) that can serve as indicators of, or proxies for, improved
health outcomes. (Fritsche et al. (2014) [18]). Our definition thus includes both supply side
mechanisms that have been alternatively labelled as Performance Based Financing (PBF) or
Pay for Performance (P4P), as well as demand side mechanisms such as vouchers that seek to
alter the demand for health services, by providing consumers with tangible benefits (cash) in
return for performing specific actions ( such as immunization, making ANC visits).
Health Policy refers to a broad statement of goals, objectives, and means that create a
framework for action. Health policy often takes the form of explicit written document but may
be implicit or unwritten [20].
Health policy analysis: examines the policy making process (prospectively or
retrospectively) with the aim of understanding the problem situation, context and the
4
stakeholders (their motivation and influence) in generating consensus on the goals, means,
values and rules to drive actions, implementation or evaluation of policy outcomes [21]
Scaling up: This study conceptualises scaling up as a complex and multi-dimensional and
often planned/guided process, as defined by Hartmann and Linn [22],“scaling up means
expanding, adapting and sustaining successful policies, programs or projects in different
places and over time to reach a greater number of people”. It further adopts ExpandNet
definition of scaling up as “deliberate efforts to increase the impact of successfully tested
health innovations so as to benefit more people and to foster policy and program development
on a lasting basis” [23]. These definitions highlight that scaling up is a guided process which
not only increases the coverage of an innovation, but also adapts and integrates it into the
national institution/system, and thus enhances its sustainability.
1.6. Structure of the Report
This report focuses on the findings of the of Policy analysis on the development of RBF in
Uganda. The report is comprised of seven chapters.
Chapter 1: describes the background of the study, the objectives, context for the study, the
key terminologies used and structure of the report.
Chapter 2: describes the conceptual framework that guided the study.
Chapter 3; presents the methodology of the study. It provides information on the research
questions, design, study instruments, data collection and analysis, ethical clearance and
limitations.
Chapter 4 covers the findings on the evolution of specific (7) RBF schemes that were
identified. .
Chapter 5 presents multidimensional scale up of RBF as a financing mechanism in general. A
timeline of the critical events along the various dimensions of scale up has been developed.
Chapter 6; presents views on determinants of RBF development at national level, RBF
prospects in Uganda and recommendations if RBF was to be adopted at the national level.
Chapter 7 provides a discussion of findings and their implications for RBF development in
Uganda.
Chapter 8 presents is the Conclusion and recommendations based on the findings of the study.

5
CHAPTER 2 : CONCEPTUAL FRAMEWORK
2.1 Introduction
A conceptual framework developed for the multi country analysis by the RBF research
support team at Institute of Tropical Medicine, Antwerp guided the data collection and
analysis process. In brief, a multidimensional understanding of RBF scale-up was adopted.
The framework is elaborated below:
2.2 Scaling up and integrating an RBF intervention: a multidimensional reality
Scaling up is often interpreted as increasing geographical coverage from a limited study area
to an entire region or country. In practice, scaling up is a complex and multi-dimensional and
often planned/guided process, as defined by Hartmann and Linn [22],“scaling up means
expanding, adapting and sustaining successful policies, programs or projects in different
places and over time to reach a greater number of people”. ExpandNet defines scaling up as
“deliberate efforts to increase the impact of successfully tested health innovations so as to
benefit more people and to foster policy and program development on a lasting basis” [23]1.
These definitions highlight that scaling up is a guided process which not only increases the
coverage of an innovation, but also adapts and integrates it into the national
institution/system, and thus, enhances its sustainability.
Beyond analyst consensus, there is a second strong reason to embrace a multidimensional
definition of scale up for this research. The object of the scale up, an RBF scheme, is not
‘just’ a health service intervention or a technological solution (e.g. a new treatment against a
disease) but a revision of the institutional arrangements shaping behaviors of various actors
already involved in the delivery of general health services to the population. This is reflected
by the definition of Performance-Based Financing proposed by Fritsche et al. (2014) [18] and
by Bertone & Meessen[24]. As argued by several experts, RBF not only requires several
structural reconfiguration of the institutional system (such as involvement of new actors,
distribution of new roles and reconfiguration of respective functions), but can also, through
spill-over, trigger some systemic changes [1].For this research, we have a dopted a broad
definition of scale up.
2.3 Descriptive work: Appreciating the progress of the RBF schemes (‘scale up process’)
As mentioned above, we developed a multidimensional definition for scale up. We further
elaborated these broad dimensions applied to this study as below.
Dimension 1-Population coverage: This is about covering more people. This can be
achieved by 1) expanding geographical or administrative area covered, 2) covering more
socio-economic groups (e.g. from poorest 20% to poorest 40%), 3) removing
demographic (age, gender) restrictions or 4) expanding the entitlement status (e.g.
extension to members of a specific voucher/insurance program)
Dimension 2-Service coverage: which can be increased by 1) covering more facilities, 2)
level of health facilities involved ( e.g from health centres only to referral hospitals as
well), 3) the range of affiliated health facilities (moving from private facilities only to
1 However, it is important to note that scaling up may not always be limited to programs that have
demonstrated themselves to be successful by any objective criterion. Programs may be scaled-up for reasons of political patronage independent of whether they are successful in reaching their stated or purported objectives.
6
include public ones), and 4) type of services (e.g. from family planning to all reproductive
health services or all types of services, including for example chronic non-communicable
diseases).
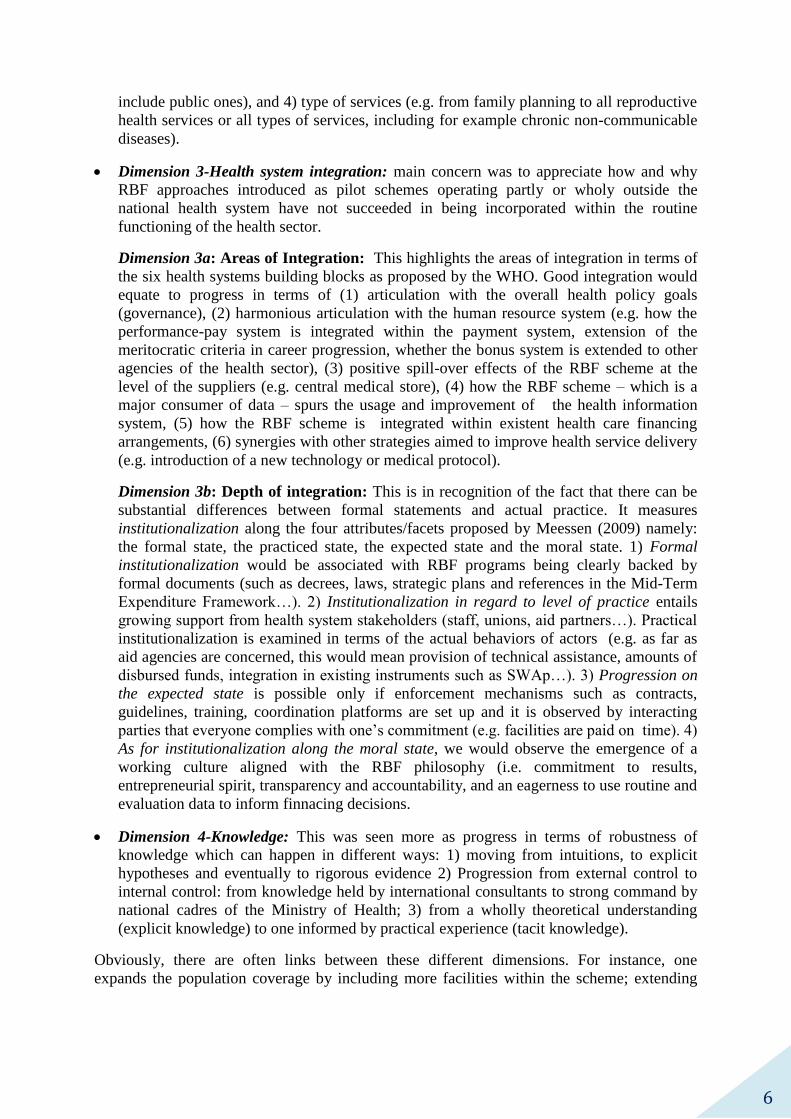
Dimension 3-Health system integration: main concern was to appreciate how and why
RBF approaches introduced as pilot schemes operating partly or wholy outside the
national health system have not succeeded in being incorporated within the routine
functioning of the health sector.
Dimension 3a: Areas of Integration: This highlights the areas of integration in terms of
the six health systems building blocks as proposed by the WHO. Good integration would
equate to progress in terms of (1) articulation with the overall health policy goals
(governance), (2) harmonious articulation with the human resource system (e.g. how the
performance-pay system is integrated within the payment system, extension of the
meritocratic criteria in career progression, whether the bonus system is extended to other
agencies of the health sector), (3) positive spill-over effects of the RBF scheme at the
level of the suppliers (e.g. central medical store), (4) how the RBF scheme – which is a
major consumer of data – spurs the usage and improvement of the health information
system, (5) how the RBF scheme is integrated within existent health care financing
arrangements, (6) synergies with other strategies aimed to improve health service delivery
(e.g. introduction of a new technology or medical protocol).
Dimension 3b: Depth of integration: This is in recognition of the fact that there can be
substantial differences between formal statements and actual practice. It measures
institutionalization along the four attributes/facets proposed by Meessen (2009) namely:
the formal state, the practiced state, the expected state and the moral state. 1) Formal
institutionalization would be associated with RBF programs being clearly backed by
formal documents (such as decrees, laws, strategic plans and references in the Mid-Term
Expenditure Framework…). 2) Institutionalization in regard to level of practice entails
growing support from health system stakeholders (staff, unions, aid partners…). Practical
institutionalization is examined in terms of the actual behaviors of actors (e.g. as far as
aid agencies are concerned, this would mean provision of technical assistance, amounts of
disbursed funds, integration in existing instruments such as SWAp…). 3) Progression on
the expected state is possible only if enforcement mechanisms such as contracts,
guidelines, training, coordination platforms are set up and it is observed by interacting
parties that everyone complies with one’s commitment (e.g. facilities are paid on time). 4)
As for institutionalization along the moral state, we would observe the emergence of a
working culture aligned with the RBF philosophy (i.e. commitment to results,
entrepreneurial spirit, transparency and accountability, and an eagerness to use routine and
evaluation data to inform finnacing decisions.
Dimension 4-Knowledge: This was seen more as progress in terms of robustness of
knowledge which can happen in different ways: 1) moving from intuitions, to explicit
hypotheses and eventually to rigorous evidence 2) Progression from external control to
internal control: from knowledge held by international consultants to strong command by
national cadres of the Ministry of Health; 3) from a wholly theoretical understanding
(explicit knowledge) to one informed by practical experience (tacit knowledge).
Obviously, there are often links between these different dimensions. For instance, one
expands the population coverage by including more facilities within the scheme; extending

7
the RBF scheme to hospitals will require adding new indicators, which may increase the
pressure for more synergies with the health information system.
As for the time dimension, our key instrument was a timeline. We used a simple software
solution (e.g. Excel) to situate key progresses in the RBF scale up.
2.4 Analytical work
We recognized RBF scale up as a policy process, which has a number of implicit and explicit
policy dimensions to be addressed when planning or assessing it [25].
There are a number of policy analysis frameworks, theories and models available in the
literature [26, 20]. Among these, the health policy triangle proposed by Walt and Gilson [21]
which comprises four components –policy process, content, context and actors–was
particularly relevant to this case study. However, this framework is highly simplified showing
the four components separately and may not entirely reflect the complex set of inter-
relationships in reality. Moreover, the aspect of knowledge translation throughout the RBF
scaling up may not be easily captured with this framework. Taking these limitations into
account, we employed this framework with slight adaptation to document and analyze RBF
scaling up process and identify enablers and barriers to the scale up process.
Our hypothesis is that RBF scaling up affects or is affected by the design features and
institutional arrangements of the RBF and the extent to which they are informed by (research-
based) knowledge and evidence (the policy content), key stakeholders involved in the scaling
up process, including those involved in the RBF conceptualization, design, implementation
and evaluation, and to a larger extent, those benefiting from or affected by RBF
implementation (the policy actors) and the context where RBF was implemented and scaled
up (the policy context).
2.4.1 Process
Among the four components, we put the scale up process at the heart of our descriptive work.
This was operationalised by developing a timeline. It was expected that as a tool, it would
facilitate : (1) the organization, visualization and triangulation of information collected from
key informants and document review, (2) reporting the multi-dimensional evolution of RBF
(the content), (3) mapping and relating actions taken by stakeholders in this process and (4)
building of the narrative of the case study; and (5) at a more analytical level (especially thanks
to cross-cases analysis), the identification of sequences of phenomena, which is a first step to
examining and establishing causal relationships.
On a timeline, we reported the multi-dimensional evolution of the content, which also
includes knowledge management processes, the related actions taken by the actors and the
phenomena at context level which affected the process. Through this adapted use of the Walt
& Gilson framework, we were able to report how RBF has been developed (scaled up) and
investigated why the RBF was (or was not) successfully scaled up by focusing on factors
influencing (enabling or hindering) such process.
2.4.2 The policy content
The policy content had a double status in our analysis: on one side, it is part of the outcomes
of the scale up process (see descriptive work above); on the other side, it is also one of the
factors which could have enabled or impeded the scale up. Too complex arrangements are
difficult to scale-up and too ambitious schemes may fail and discredit the strategy. In a recent
study, Spicer and colleagues [32] found designing scalable innovations and embedding the

8
scale-up in program design to be among key factors enabling the scaling up of the
innovations.
2.4.3 Actors
We paid particular attention to key stakeholders involved in the RBF scaling up process (the
policy actors), as they are at the center of the Walt & Gilson framework with free will and
agency power. These include individuals, groups of individuals or organizations, states or
governments.
We investigated how the actors interacted among them and exercised their power (financial,
political, technical, symbolic and normative power) to influence the scaling up related
decisions/actions and the reasons behind such decisions. We assumed that such
decisions/actions had been determined by the information at their disposal, their own interests
and constraints, including the overall context. The possible role of some ‘policy
entrepreneurs’ as a matter of interest.
2.4.4 Context
The policy context within which RBF was conceptualized, designed and implemented and
scaled up, according to Gilson and Raphaely [30], matters a lot and needs to be examined
carefully. The contextual factors can be political, economic and social. Theoretically, there
are many ways of categorizing contextual factors [20]. In this study, we included the global
context, the national context outside the health sector and the national health sector context.
We also tried to identify recent or current reforms, including decentralization processes and
their outcome, to examine to what extent they interacted with the proposed RBF reform. We
assumed that such contextual factors have been changing overtime along with other
components. Thus making the link with the timeline was particularly important to capture that
change.

9
CHAPTER 3 : METHODOLOGY
3.0 Introduction
This section on methodology provides an overview of the research questions, design, study
instruments, sampling, data collection and analysis approach. It further highlights the ethical
review process as well as the limitations of the study.
3.1 Research Questions
The study set out to answer the following study questions.
1. To what extent is scale up of RBF achieved in Uganda? What are the enablers and
barriers to buy-in and integration into national health policy processes?
a. How has RBF evolved in Uganda from 2003 to 2015? What were the drivers and
processes followed for various schemes?
b. Who were the actors and what was their motivation? To what extent were the
different schemes linked to national health policy process and build on evidence from
each scheme?
2. What are the determinants and explanations for observed dynamics regarding RBF
between March 2014 and March 2015 in Uganda?
3.2 Research Design
This is a case study research which is part of a multi-country analysis of RBF policy
processes in 11 countries. Specifically, it is both a retrospective and prospective analysis of
RBF policy process in Uganda and covers the period from January 2003 to May 2015. It
draws on work in health policy analysis and social sciences. This study drew on three main
sources of information: 1) the existing body of literature/documents on RBF in Uganda 2) key
informants among stakeholder institutions such as MOH, funders and RBF implementing
agencies and participating facility managers and 3) Participant observation at key meetings.
Through document review and interviews, analysis of the evolution of RBF from 2003 to
early 2015 has been carried to understand the barriers and facilitators for scale up.
Furthermore, as participant observers at 2nd
national consultative meeting on RBF, the study
explored the determinants of the new momentum around RBF in Uganda.
3.3 Instruments
A coding framework was developed for the document review (attached as annex 4).
For the interviews, a generic interview guide (attached as annex 3) was developed basing on
the conceptual framework that guided this study. The interviews sought information on how
the following themes explain the evolutionary process of RBF at national level:-Evidence
generation process, perception of success and failure by implementers, drivers and motivation
of implementers, cross learning over time, linkage to national policy process and coordination
of efforts. This was adapted to suit the different categories of respondents. Accordingly four
tools were used. The first guide was for implementers, second for health facility managers, the
third for decision makers (at national and district level) and development partners. The last
one was developed for representatives of the Ministry of Finance, Planning & Economic
development (MoFPED) and Ministry of Public Service (MoPS). These are appended as well.
10
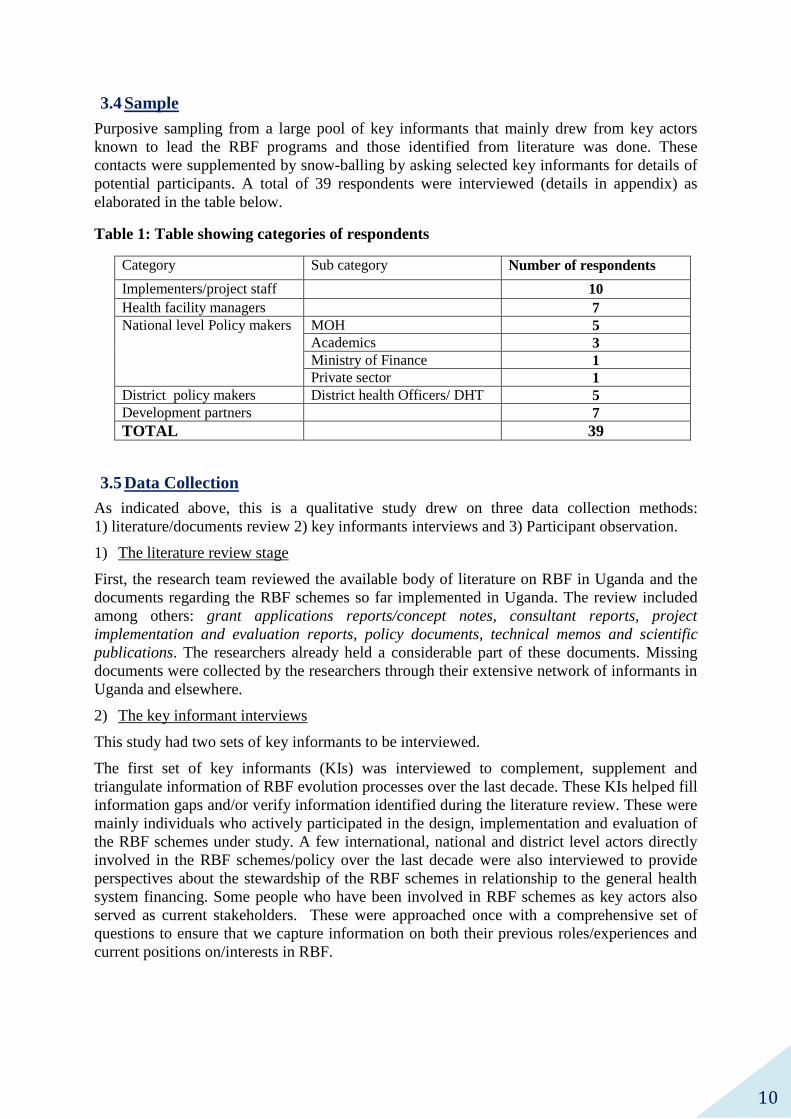
3.4 Sample
Purposive sampling from a large pool of key informants that mainly drew from key actors
known to lead the RBF programs and those identified from literature was done. These
contacts were supplemented by snow-balling by asking selected key informants for details of
potential participants. A total of 39 respondents were interviewed (details in appendix) as
elaborated in the table below.
Table 1: Table showing categories of respondents
Category Sub category Number of respondents
Implementers/project staff 10
Health facility managers 7
National level Policy makers MOH 5
Academics 3
Ministry of Finance 1
Private sector 1
District policy makers District health Officers/ DHT 5
Development partners 7
TOTAL 39
3.5 Data Collection
As indicated above, this is a qualitative study drew on three data collection methods:
1) literature/documents review 2) key informants interviews and 3) Participant observation.
1) The literature review stage
First, the research team reviewed the available body of literature on RBF in Uganda and the
documents regarding the RBF schemes so far implemented in Uganda. The review included
among others: grant applications reports/concept notes, consultant reports, project
implementation and evaluation reports, policy documents, technical memos and scientific
publications. The researchers already held a considerable part of these documents. Missing
documents were collected by the researchers through their extensive network of informants in
Uganda and elsewhere.
2) The key informant interviews
This study had two sets of key informants to be interviewed.
The first set of key informants (KIs) was interviewed to complement, supplement and
triangulate information of RBF evolution processes over the last decade. These KIs helped fill
information gaps and/or verify information identified during the literature review. These were
mainly individuals who actively participated in the design, implementation and evaluation of
the RBF schemes under study. A few international, national and district level actors directly
involved in the RBF schemes/policy over the last decade were also interviewed to provide
perspectives about the stewardship of the RBF schemes in relationship to the general health
system financing. Some people who have been involved in RBF schemes as key actors also
served as current stakeholders. These were approached once with a comprehensive set of
questions to ensure that we capture information on both their previous roles/experiences and
current positions on/interests in RBF.

11
To complement the above list of stakeholders, a small number of additional KIs were selected
basing on their current roles in relation to RBF and health financing policy in Uganda. They
were interviewed to understand their perception, interest in and position on RBF; highlighting
key areas of concern.
3) Participant Observation
Observation of RBF consultation processes at the national level during the period of Nov
2014 to March 2015 was done.
3.5 Data Analysis
The literature was analysed manually using a coding framework and a timeline was
developed.
The interviews were transcribed verbatim. An analysis guide was developed (attached) and
transcripts shared in advance with the study team. Analysis workshops were held to
consolidate the analysis.
3.6 Ethical considerations
The following measures will be taken to ensure adherence to ethical principles:
The study protocol and other standard operating procedures were submitted for review
and approval from the Higher Degrees, Research and Ethics Committee (HDREC) of
Makerere University School of Public Health and to the Uganda National Council for
Science and Technology (UNCST) and WHO Ethics Review committee (ERC).
All respondents consented for the study. The consent forms are attached as Annex 2.
3.7 Limitations
There are some issues that could have affected the results of the study.
1. Without an explicit policy on RBF, the study has been constrained by lack out outcomes
to assess. We looked at several diverse and distinct RBF projects that have not scaled up
at national level. Developing a timeline for RBF development in Uganda has thus been a
challenge. To address the above, all the schemes were considered to represent a
continuum of efforts towards RBF adoption in Uganda. Furthermore, an analytical
framework that captured the views of various stakeholders over the period of study was
adopted. Similarly, a prospective component of stakeholder analysis and observation were
added to ensure that this study informs future health policy reforms.
2. Relatedly, conceptualization of RBF and PBF has been a challenge across the study. There
is no uniform understanding of what RBF entails or does not among the respondents. The
schemes implementers have different conceptualization which has also led to the diverse
models being implemented in Uganda. This caused confusion among the respondents
especially those not very familiar with health financing concepts. This study adopted a
broad understanding of RBF as an umbrella term for several arrangements that link
performance/result to (financial/non-financial) rewards.
3. Developing a timeline was further complicated because of the difficulty to attach for
specific times/dates to the critical junctures in RBF development. This was partly offset
by triangulating information from various sources.

12
4. Time constraint was a challenge at the beginning of the study considering the long period
that was taken to obtain for ethical approval from the ERC of WHO. Reaching high level
policy makers and other important key informants for interviews was also challenging as
these were very busy people. Accordingly, efforts were made to make the research
manageable and feasible for the available study period. For example, the literature and
document review which did not require ethical approval was carried out right from the
start to create time for primary data collection.
13
CHAPTER 4 : DESCRIPTION OF RESULTS-BASED
FINANCING INITIATIVES IN UGANDA.
Introduction: 4.1
This chapter addresses objective 1 of the study and provides findings on the evolution of RBF
policy (2003 – 2015) with focus on description of the RBF schemes that have been
implemented in Uganda over the study period. These have been divided into supply side and
demand side schemes. The supply side schemes target mainly the service providers while the
demand side target primarily the consumers/users of health services. Never the less, there are
overlap and spill over effects among these two categories.
This descriptive part covers the general design and institutional arrangements, Population and
service coverage, key implementation issues and project closure/scale-up regarding each RBF
scheme.
Types of RBF schemes implemented in Uganda (2003-2015) 4.2
This study covered a total of 7 RBF initiatives that have been implemented in Ugandan health
sector since 2003. Table 3: Design features of RBF schemes implemented in
Ugandaelaborates the main feature of the various schemes. Generally, Uganda has seen both
supply side and demand side RBF schemes. The supply side schemes studied included the
World-bank PBC Study (2003-2005), the Cordaid Pilot (2009-2015) and the NuHealth project
(2011-2015). Another program, the Strengthening Decentralisation for Sustainability (SDS) is
managed under Ministry of Local government (MoLG) and provides performance-based
grants to districts to deliver social services including health. On the hand, three demand-side
schemes (essentially vouchers) have been implemented in Uganda. These included the
Reproductive Health Voucher Project by World Bank (2006-2011), the Safe Deliveries
Project (SDP) (2009-2011) and Saving Mothers Giving Life (SMGL) Initiative.
Description of Supply side-RBF schemes in Uganda: 4.3
This sub-section presents findings on the description of the Supply side RBF schemes that
have been implemented in Uganda over the 12 year study period.
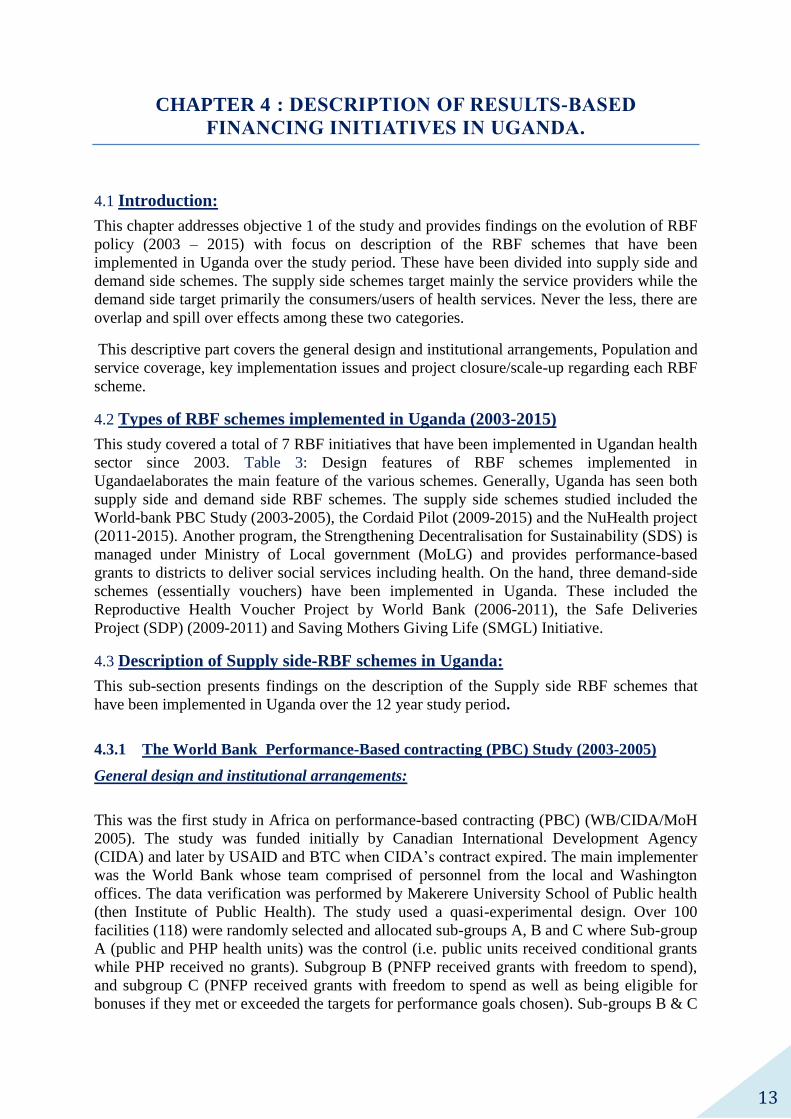
4.3.1 The World Bank Performance-Based contracting (PBC) Study (2003-2005)
General design and institutional arrangements:
This was the first study in Africa on performance-based contracting (PBC) (WB/CIDA/MoH
2005). The study was funded initially by Canadian International Development Agency
(CIDA) and later by USAID and BTC when CIDA’s contract expired. The main implementer
was the World Bank whose team comprised of personnel from the local and Washington
offices. The data verification was performed by Makerere University School of Public health
(then Institute of Public Health). The study used a quasi-experimental design. Over 100
facilities (118) were randomly selected and allocated sub-groups A, B and C where Sub-group
A (public and PHP health units) was the control (i.e. public units received conditional grants
while PHP received no grants). Subgroup B (PNFP received grants with freedom to spend),
and subgroup C (PNFP received grants with freedom to spend as well as being eligible for
bonuses if they met or exceeded the targets for performance goals chosen). Sub-groups B & C
14
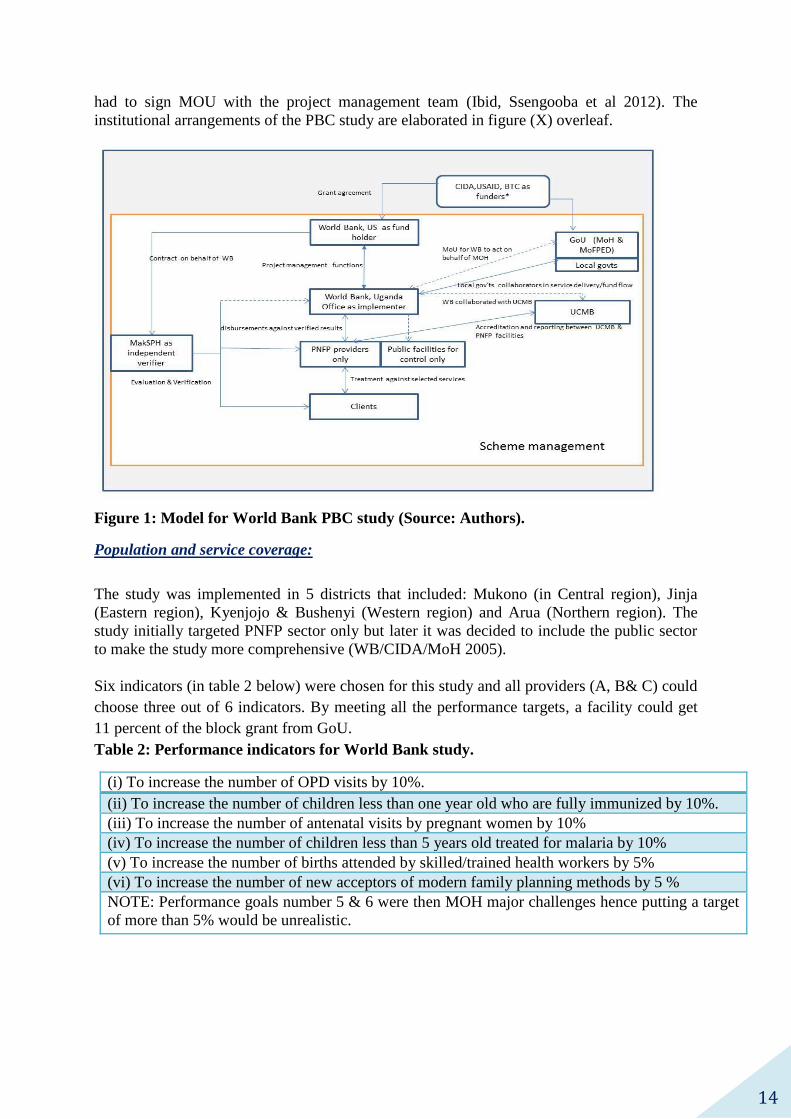
had to sign MOU with the project management team (Ibid, Ssengooba et al 2012). The
institutional arrangements of the PBC study are elaborated in figure (X) overleaf.
Figure 1: Model for World Bank PBC study (Source: Authors).
Population and service coverage:
The study was implemented in 5 districts that included: Mukono (in Central region), Jinja
(Eastern region), Kyenjojo & Bushenyi (Western region) and Arua (Northern region). The
study initially targeted PNFP sector only but later it was decided to include the public sector
to make the study more comprehensive (WB/CIDA/MoH 2005).
Six indicators (in table 2 below) were chosen for this study and all providers (A, B& C) could
choose three out of 6 indicators. By meeting all the performance targets, a facility could get
11 percent of the block grant from GoU.
Table 2: Performance indicators for World Bank study.
(i) To increase the number of OPD visits by 10%.
(ii) To increase the number of children less than one year old who are fully immunized by 10%.
(iii) To increase the number of antenatal visits by pregnant women by 10%
(iv) To increase the number of children less than 5 years old treated for malaria by 10%
(v) To increase the number of births attended by skilled/trained health workers by 5%
(vi) To increase the number of new acceptors of modern family planning methods by 5 %
NOTE: Performance goals number 5 & 6 were then MOH major challenges hence putting a target
of more than 5% would be unrealistic.

15
Key implementation issues:
The study designed included several data collection methods. For example several facility,
staff and exit surveys were conducted at the 118 health facilities. Household surveys in the
catchment areas of each facility were also conducted.
Several issues delayed the start of the project. These included changes in key project
personnel and delayed disbursements of funds due to the complexity of the design and
contractual arrangements (WB/CIDA/MoH 2005, Implementer). Mid-course, competing
national campaigns such as recruitment of health workers by public service, national mass
immunization and “Home Based treatment of fevers (HBF)” campaigns were noted to have
affected the project performance. For example, the malaria-related indicators could not be met
since children with malaria were being treated in the communities and few brought to health
units.
Project closure and scale-up
The project suffered budget shortfalls that constrained data collection. The data collection was
delayed and made less comprehensive (WB/CIDA/MoH 2005, Ssengooba et al 2012, KI).
Budget shortcomings were partly because CIDA’s contract ended prematurely. This in fact
further affected the bonus disbursements. Although, the project secured financial support from
other funders, the support was short lived. Ultimately, the project closed within 2 and half
years of implementation.
4.3.2 The Cordaid project (2009-2015)
General design and institutional arrangements:
The Cordaid project was the second supply side RBF project implemented in Uganda. It was
started in 2009, three years after the World Bank’s PBC study was concluded.
The project funder was Cordaid, a Dutch Catholic Non-governmental Organisation that had
been supporting the Uganda Catholic Medical Bureau (UCMB) for over a decade. The fund
holder was Jinja Catholic Diocese while the verification team include the diocesan team and
District health team headed by the DHO, Jinja. Later Community-based organisations were
recruited to do community verification and consumer satisfaction surveys. Figure 2 illustrates
the project model.
Population and service coverage:
The Cordaid project was implemented in a two phased approach. During phase I (2009-2013),
implementation covered only PNFP facilities in three eastern districts of Jinja, Kamuli and
Iganga. During phase II (2013-15), the project extended to public facilities on realising that
outputs in the public facilities were low (WHO & MoH 2014, KIIs). This adjustment made
the Cordaid pilot the first and only supply-side RBF to have been implemented in the public
sector in Uganda. Reportedly, the extension to the public sector stretched the available
financial resources. Hence, the geographical scope of the project’s intervention arm was
scaled down to cover only Kamuli district. The PNFP facilities in the neighbouring districts
acted as control facilities (WHO & MoH 2014.KIs).
Regarding services covered, the project covered 23 indicators based on services within the
UNMHCP.

16
Figure 2: The Cordaid Project Model (Source: Authors)
Key implementation issues:
The project set up support systems and health systems strengthening components to enhance
the project success. Notably, a procurement system was set up enable facilities to access
medical supplies from the Joint Medical Stores. Additionally, the data systems were initially
manual and when this was realised to impede timely generation and utilisation of data, a
computer-based information system was set up support data management functions.
The Key informants reported an initial challenge of low buy-in/ownership by the district
leadership. This was addressed through training district leaders to perform oversight. A
steering committee headed by DHO Jinja district was established to offer oversight and
perform supervisory roles.
Project closure and scale-up:
The project is expected to close in December 2015 after securing a six month extension.
However, over the last couple of years, Cordaid has been instrumental in promoting RBF in
through training and offering field visits to local, national and international actors. The
extension into the public sectors has given Cordaid leverage and national recognition. For
example, the in-charge of one of the public facilities implementing RBF received a national
award in 2014 as the best performing health facility manager in the country owing to using
RBF funds to improve the infrastructure and service delivery at his health centre.
4.3.3 The NuHealth project (2011-2015)
General design and institutional arrangements:
In 2011, another RBF project coded NuHealth was started in Northern Uganda. This 4 year
RBF project was started to support PNFP facilities in post conflict Acholi region in Northern
Uganda ‘to help poor people utilize health services” ( technical brief 2:X).
By design, NuHealth was a quasi-experimental study with intervention facilities (using RBF)
in Acholi while control facilities were in Lango sub region-also a post conflict region. Here,

17
input-based financing was maintained. The project organizational structure is elaborated in
figure below. In brief, the project has been funded by UKAid (formerly DFID). The
fundholding and project management team was led by Health partners International (HPI) and
Montrose. Verification was undertaken on quarterly basis by project management team and
DHTs. The funder was UKaid (former Department of International Development, DfID) and
the fund holder was NuHealth secretariat which was made up of Health Partners International
and Montrose as implementers. The project was implemented in PNFP facilities so NuHealth
worked closely with the Medical Bureaux. The district health teams in the intervention arm
were involved as data verification teams while regional bodies were set up to enhance shared
learning (NuHealth 2011,2013a,b,c and 2014). The institutional set up of the project is
illustrated in the figure below:
Figure 3: NuHealth Pilot model (Source: authors)
Population and service coverage:
Overall, there were 21 facilities from Acholi and 10 in Lango region. Regarding performance
measurement in Acholi, performance was gauged against 16 indicators selected from the
UNMHCP. The target beneficiaries were the general population in the project area.
Key Implementation issues:
Prior to project implementation, a baseline was undertaken to check readiness of the facilities.
The facilities received seed grant improve their level of functionality before start of RBF. The
IBF arm continued to receive conditional grants as per GoU arrangement. Throughout the
project life, all facilities were supported with essential medicines and health supplies from
JMS.

18
Verification was done quarterly by the NuHealth team and the District Health team.
Satisfactorily performance triggered payments to the facilities. Regarding oversight,
respondents indicated that a “hands-off approach’ where facilities were allowed to use the
funds as according to their own discretion was used under the RBF arm in Acholi region. On
the other hand, the facilities in the IBF arm were closely monitored by the NuHealth team to
ensure that they adhered to the business plans and existing financial systems.
Results from the project indicated that service utilisation increased in both arms but slightly
more in the RBF arm compared to the IBF segment (WHO& MOH 2014).
Project closure and scale-up
The NuHealth project had an independent impact evaluation assessment in September 2015
that was carried out by the Liverpool School of Tropical Medicine. The final dissemination is
expected soon. The project is expected to close at the end of October, 2015.
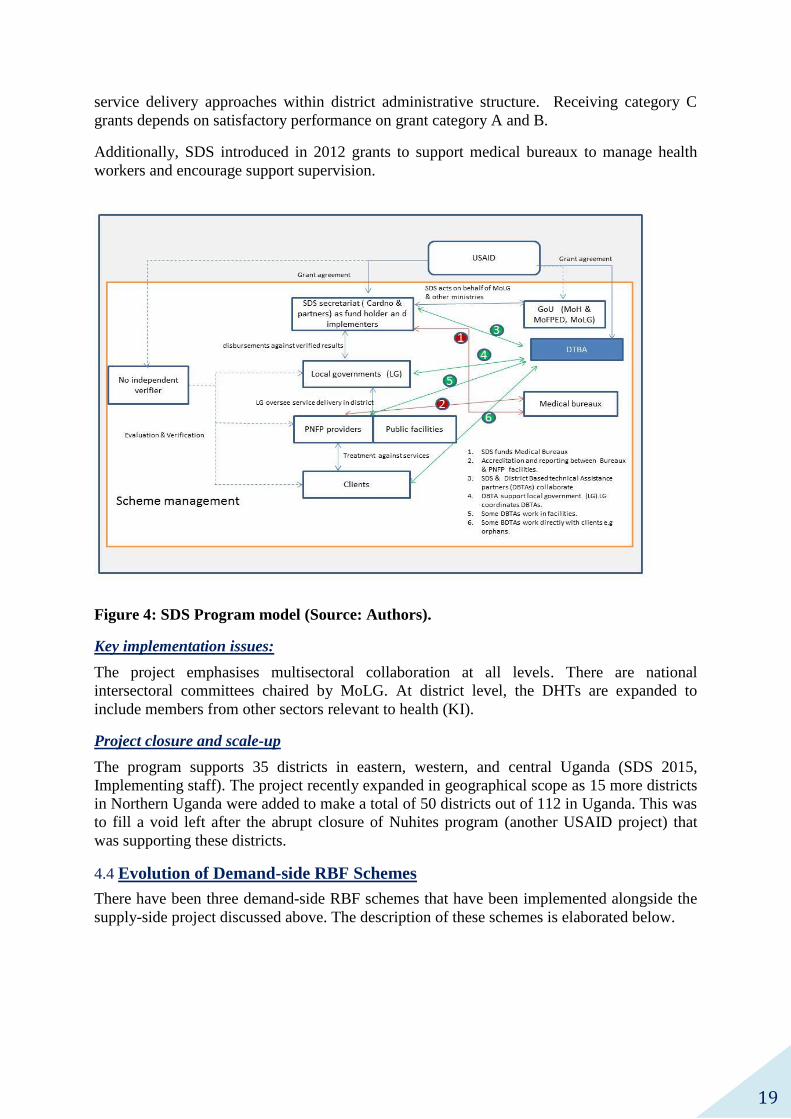
4.3.4 Strengthening Decentralization for Sustainability (SDS) (2010-2016)
General design and institutional arrangements:
In addition to the Supply-side RBF schemes so far discussed above, another RBF project
named Strengthening Decentralization for Sustainability (SDS) has been implemented in
Uganda since 2010. The SDS program supports local governments to improve social service
delivery, with emphasis on health, education, and services for orphans and vulnerable
children.
The project is funded by USAID and implemented by SDS Secretariat where the main player
is Cardno supported by the Urban Institute (UI), Development InfoStructure Inc. (Devis),
Infectious Disease Institute (IDI) and Tangaza Cinemas Ltd. The districts sign MoU with SDS
and receive performance-based grants to coordinate, plan, monitor and evaluate operations
that support services implemented by USAID District Based Technical Assistance (DBTA)
partners in health, HIV/AIDS, and for orphan and other vulnerable children (OVC). DBTAs
include Strengthening Tuberculosis and AIDS Response – South West (STAR-SW),
Strengthening Tuberculosis and AIDS Response – East Central (STAR-EC) and
Strengthening Tuberculosis and AIDS Response – East (STAR-E). The figure 4 below
illustrated the project set up.
Population and service coverage:
It was emphasised that SDS aims at addressing the coordination gap under decentralization.
Accordingly, SDS strives to empower the districts management teams to take authority in
coordinating Implementing partners (IPs) and assist with the integration of IP activities into
the district development plan (DDP). As such, the project uses governance and management
related-indicators to incentivize these important functions.
As reported by the implementing team, the SDS Programme has a comprehensive
performance-based grant structure (SDS 2015). Grant category A are called program support
grants. These are awarded annually to districts to facilitate non-wage expenditures such as
supplies, materials, vehicle operational costs, and staff per diems for travel and enhance
coordination of USAID partners. Grant Category B are called program management grants
and facilitate management functions such as planning, budgeting, monitoring and evaluation.
Receiving Grant B is contingent on satisfactory performance on grant A. Grant category C
(also known as innovation grant) were introduced in 2014 to build capacity for innovative
19
service delivery approaches within district administrative structure. Receiving category C
grants depends on satisfactory performance on grant category A and B.
Additionally, SDS introduced in 2012 grants to support medical bureaux to manage health
workers and encourage support supervision.
Figure 4: SDS Program model (Source: Authors).
Key implementation issues:
The project emphasises multisectoral collaboration at all levels. There are national
intersectoral committees chaired by MoLG. At district level, the DHTs are expanded to
include members from other sectors relevant to health (KI).
Project closure and scale-up
The program supports 35 districts in eastern, western, and central Uganda (SDS 2015,
Implementing staff). The project recently expanded in geographical scope as 15 more districts
in Northern Uganda were added to make a total of 50 districts out of 112 in Uganda. This was
to fill a void left after the abrupt closure of Nuhites program (another USAID project) that
was supporting these districts.
Evolution of Demand-side RBF Schemes 4.4
There have been three demand-side RBF schemes that have been implemented alongside the
supply-side project discussed above. The description of these schemes is elaborated below.

20
4.4.1 The World Bank Reproductive health Voucher Project (2006-2011)
General design and institutional arrangements:
In addition to the PBC study, the World Bank also implemented a demand-side vouchers
project in Western Uganda. As reported in the operational manual, the objective of this
intervention project was to reduce maternal and child mortality and decrease the burden of
sexually transmitted diseases (STDs):
“The project’s objective is to reduce the number of mothers and children dying or
being disabled due to absence or under-utilization of skilled medical attendance
during pregnancy and child delivery as well as to reduce the burden of sexually
transmitted diseases (STDs) through the introduction of a voucher system”, (Project
Operational manual, pg 5).
Regarding Institutional arrangements, several contracts were signed between varying parties.
The funder was global partnership for Output Based Aid (GPOBA) which was established in
2003 as a multi-donor trust fund administered by the World Bank. The partnership included
the United Kingdom’s Department for International Development (DFID), the International
Finance Corporation (IFC), the Dutch Directorate General for International
Cooperation (DGIS), the Australian Department for Foreign Affairs and Trade
(DFAT), the Swedish International Development Agency (Sida). (GPOBA 2015, Okwero et
al 2012).
At the same time, KfW was hired as the fiduciary agency while MarieStopes Uganda was
hired as the voucher management agency (VMA). The service providers were private
facilities while public health facilities were used for referral purposes only. KfW signed MoU
with GoU (MoH& MoFPED) but these did not have any active roles in project
implementation. PricewaterhouseCoopers (PwC) was hired as the independent verifier.
The project design is illustrated in the figure 5 below.
Figure 5: RHV Project Design (Source: Adapted from Project Operational Manual
2007; 6).

21
Population & Service Coverage:
The project started in 2006 as a pilot implemented by Kreditanstalt für Wiederaufbau (KfW)
and providing vouchers to treat sexually transmitted infections at selected private health
facilities within 5 districts in western Uganda.
On October 23, 2007, the World Bank as administrator of GPOBA) signed an agreement with
KfW worth four million three hundred thousand United States Dollars (US 4,300,000) to
scale-up the Reproductive Health Voucher (RHV) in Western Uganda Project. In early 2008
RHV was scale-up to cover 20 districts in the region. The target population in this area was 4-
5 million inhabitants (Okwero et al 2012).
The RHV project had four components namely Safe Motherhood Vouchers, STD treatment
vouchers, Fiduciary agent fee and Project Independent Verification Monitoring and Audit
(World Bank 2008:12).The Safe Motherhood vouchers catered for antennal care visits, normal
and complicated deliveries, one postnatal visits and costs associated with marketing and sale
of vouchers and voucher administration. The STD Treatment vouchers covered costs of
treating couples and covered costs of treatment of STDs and cost of marketing, selling and
administering the vouchers. KfW, the fiduciary agent received US390, 000 for costs
associated with administering the project funds.
Key implementation issues:
There were some disruptions that were well documented towards the end of implementation
that threatened continuity of the project and required innovative approaches (GPOBA 2012).
It was pointed out that national political campaigns lead to depletion of human resources
especially the Community Based vouchers which reduced voucher sales. Strategies included
extending the voucher redemption period and concentrating on towns and highly performing
health facilities and voucher distributors. This was in essence contraction of the scale-up
process.
Project closure & scale-up
The project ended in 2011. The impact evaluation (conducted in 2012) indicated positive
results on the poor (Bellows & Obare 2012, Kanya et al 2013). As follow on, a Reproductive
health voucher project Phase II worth USD 13,300,000 was agreed upon with the World Bank
and Government of Uganda. This is to be implemented in the western and eastern regions
effective 30th
October 2014 till 29th
December 2017. However, the project implementation has
delayed to start due to failure to determine the role of MoH in the scheme (policy maker,
MoH). As intimated by a policy maker at MoH, MarieStopes Uganda indicated interest in that
work but the administrative costs were very high. Accordingly, there is a plan to establish a
voucher management unit with MoH to build the institutional capacity.
4.4.2 The Safe Deliveries Project (SDP) (2009-2011)
General design and institutional arrangements.
As the World Bank implemented the RHV project in western Uganda, a team from Makerere
University School of Public Health as part of the Future Health systems consortium conceived
the SDP project to test innovative strategies to the improve the accessibility of the poor to
health services in eastern Uganda. The overall aim was to assess the effectiveness of a
demand side and supply side financing imitative using vouchers to increase institutional
deliveries. The SDP was a quasi-experimental study that was implemented in two districts of
Kamuli & Pallisa in the eastern region. Each district had one health sub district in intervention

22
and control arm. There intervention had two components-demand side (services and transport
vouchers) and supply side (health systems strengthening).
The MakSPH was the main implementer as the voucher management agency and funder
holder. The district leadership provided oversight while central government structured did not
have any active roles. Regarding the nature of health facilities,
The overall design of the SDP is elaborated below in figure 6:
Figure 6: The Safe Deliveries Project Model
Population and service coverage:
SDP was implemented in both public and private (for profit and not-for-profit) health
facilities. Noteworthy, this was the first RBF scheme to operate within public facilities in
Uganda. SDP was also the first project to introduce transport vouchers in Uganda. The VMA
signed contracts with the local transporters to provide free transport to mothers who had a
transport voucher
Regarding population coverage, the project covered all pregnant mothers within the
intervention areas. The covered services related to safe deliveries and included accessing
antenatal care and facility-based deliveries.
Key implementation issues:
The project underwent several phases namely design, pilot, implementation, evaluation and
dissemination phases. Design phase included sensitisation of leaders, needs assessment of

23
health facilities, survey of transport providers, exploratory research, updating knowledge of
service providers and design the vouchers.
Pilot started in December 2009 for 3 months in Buyende sub- district within Kamuli district.
The main activities included community sensitisations, distribution of vouchers and
payments. On review, the pilot showed tremendous utilisation of services and increased
demand on health systems. Moreover, the project incurred huge financial cost and the
decision was made to reduce the service package and transport fares (KI). Actual
implementation started in June 2010 for one year. The main activities included distribution of
vouchers, data collection, field supervision, making payments etc. This period was punctuated
with series of negotiations with service/transport providers to address implementation issues
(KI, Ekirapa et al 2013). Monitoring and evaluation was done through household surveys,
facility data collection and in-depth interviews of health workers, community leaders and
transporters.
Project closure and scale-up issues:
The main concern about the SDP project was the sustainability of results (Project manager).
Accordingly two follow –on projects were developed 1) The Maternal and New-born Study
(MANEST)-provides vouchers targeted for poor people who live beyond 5km from health
facilities. 2) Maternal and Neonatal implementation for Equitable Systems (MANIFEST) was
conceived to “generate evidence that can contribute to solving barriers to successful scale up
of these successful interventions...by investigating mechanisms of mobilizing and using
locally available resources in a sustainable manner for improving access to quality maternal
and newborn health care using existing structures” ( MANIFEST 20152)
4.4.3 The Saving Mothers Giving Life (SMGL) Initiative (2012-2017).
General design and institutional arrangements
Soon after RHV project ended in western Uganda, the SMGL initiative was introduced in
western Uganda in 2012. This initiative is a five year project that started in Uganda and
Zambia with a goal of supporting countries to rapidly reduce the alarming rates of women
dying during pregnancy and child birth. The initiative focuses on labour, delivery and the
immediate 24 hours after childbirth.
The SMGL has a complex web of players both at the international, national and subnational
levels. Regarding Funding, the project funders include US Global health Initiative (GHI) and
partners that included Merck/MSD, the American College of Obstetricians and
Gynaecologists, Every Mother Counts, ELMA foundation and the Government of Norway
(SMGL 2015b).
Pertaining implementers in Uganda, this project is being implemented (on behalf of the
Government of Uganda under the Ministry of Health) by several implementing partners with
Baylor Uganda and Infectious Disease Institute (IDI) as the lead agencies. Both Baylor
Uganda and the IDI leveraged their existing ongoing comprehensive HIV care programs in
their respective districts to implement and coordinate the SMGL project in their respective
districts. Baylor Uganda collaborated with professional bodies (Association of Obstetricians
& Gynaecologists of Uganda, Uganda (AOGU), Uganda Pediatric Association (UPA),
Uganda Society of Anesthesia (USoA)), the Infectious Diseases Institute (IDI,which leads
implementation in Kibaale district), STRIDES for Family Health, Marie Stopes-Uganda
2 http://hppm.musph.ac.ug/index.php/research/manifest-maternal-neonatal-implementation

24
(manages the Voucher program), ASSIST (Quality Assurance), UHMG (demand creation),
SDS (district coordination) ( SMGL 2015). An elaboration of the institutional arrangements
under SMGL initiative is provided in figure 7 below.
Figure 7: The institutional design of the SMGL Project in Uganda (Source: Authors)
Population and service coverage:
The SMGL project adopted a district wide approach in both public & private health facilities.
Interventions relate to systems strengthening, quality improvements and operations research.
Two types of vouchers were implemented:1) The transport voucher for transporting the
pregnant woman or sick new born to the nearest health facility and referral to next level of
health facility in case of emergency. Tricycle ambulances were procured in September 2012.
Secondly, a maternal health voucher program called Healthy Baby Voucher Program (HBVP)
was implemented in SMGL’s four priority districts in Western Uganda (Kyenjojo, Kabarole,
Kamwenge, and Kibaale).Poor pregnant women purchase the voucher for 3,000 Uganda
Shillings and receive access at no additional cost to the following services at accredited
providers. Altogether, 117 facilities received support from the SMGL initiative (CDC 2014).
Key implementation issues:
The project underwent some phases as explained below. The preparatory phase lasted
between 1st January to 31
st May 2012. The program was launched by former US Secretary of
State, Hillary Clinton in June 2012. The Pilot/proof of concept phase was between 1st June
2012 to 31st May 2013 in 4 selected districts of Kabarole, Kamwenge, Kyenjojo and Kibaale.
Phase II preparatory phase was between July to Sept 2013 and full Phase II implementation
started in October 2013 till 2017.. In 2014, the project extended to additional 6 districts in

25
northern Uganda and increased focus on newborn care (SMGL 2014, Centres for Disease
Control and prevention (CDC), 2014, SMGL 2015b).
Review of the project progress reports (SMGL 2013), indicated that this project benefited
from similar project in Zambia. There were opportunities to share lessons on best practices.
For example the Ugandan team visited Zambia in April 2013. More so, the study had strong
research component through several studies such as the Expenditure survey in August 2012,
pregnancy Outcomes measurement (POM) study undertaken in November 2012 and health
facility assessment in June 2013.
Project closure and scale-up
The project is mid-way and according to the mid-initiative report (SMGL 2015b), it has
respectively contributed 41% and 45% reduction in community and facility-based maternal
mortality ratios in the implementation areas.

26
Table 3: Design features of RBF schemes implemented in Uganda
3 Partners include Merck/MSD, the American College of Obstetricians and Gynaecologists, Every Mother Counts, ELMA foundation.
Project Feature World Bank Study Reproductive
Health vouchers
Project
Safe deliveries
Project (SDP)
Cordaid project NuHealth Project Health Baby
/SMGL Voucher
Project.
Strengthening
Decentralisation for
Sustainability (SDS)
Duration 2003-2005 July 2006- 2011 2009-2011 2009-2015 Sept 2011-2015 2012-to date 2010-to date
General study design Quasi-experimental
design, two
intervention groups
and a control
Intervention study Quasi-experiment
study
Interventional
design Quasi-experiment
study (RBF & input
based financing)
Intervention design Intervention design
Type of RBF Supply side Demand side Demand-side &
Supply side
Supply side
Supply side
Demand side with
health system
strengthening
components
Supply side
Funding source and external
support
CIDA,
USAID,BTC
KfW and the
GPOBA-World
Bank)
Bill and Melinda
Gates
Foundation and
WHO-AHPSR.
Cordaid
DFID
Saving mother giving
life initiative (funded
by US Global Health
Initiative (GHI) and
partners3.
USAID
Purchasing agent World Bank
through local
government.
MarieStopes Uganda
(MSU)
Makerere
University Schhol
of Public Health
(MaKSPH)
Jinja
Diocese/Cordaid
Health Partners
International (HPI)
&Montrose
International
Baylor-Uganda,
IDI,STRIDES froo
family health, MSU.
Cardno and supported by
the Urban Institute
(UI),Devis, Infectious
Disease Institute (IDI) and
Tangaza Cinemas Ltd
Fund holding agent World Bank MSU MaKSPH Cordaid HPI & Montrose SMGL initiative SDS program
Auditing/Verification agents MaKSPH
MSU
MakSPH Cordaid/DHTS and
CBOs
NU-Health and
District health teams
(DHTs)
Respective agencies SDS + District health
teams
Population
coverage
Geographical
scope
118 facilities (68
PNFPs) from five
pilot districts.
Evolved from 4 pilot
districts to 20
districts in south
western Uganda.
22 health facilities
in 2 districts in
Eastern Uganda.
Initially Jinja,
Kamuli & Iganga
districts. Later
restricted to Kamuli.
31 health centres in
12 northern Uganda
districts.
4 districts in Western
Uganda but scaled up
to 10( included 6
more districts in
Northern Uganda)
35 districts initially
increased to 50 in 2015
Populations
served
All resident within
reach of health
facilities
Women for STI and
SM
All resident
pregnant women,
transport providers,
health workers
All residents within
reach of facilities
All residents within
reach of facilities
All mothers within
districts
District councils and
Medical bureaux

27
Project Feature World Bank Study Reproductive
Health vouchers
Project
Safe deliveries
Project (SDP)
Cordaid project NuHealth Project Health Baby
/SMGL Voucher
Project.
Strengthening
Decentralisation for
Sustainability (SDS)
Service
coverage
Services
package
Six service
priorities (total
outpatient visits and
malaria,
immunization,
Antenatal visits,
attended births
and family
planning).
Subsidized vouchers
at 3,000 Uganda
shillings (US $1.40)
to access SM
services, STI
treatment.
-Demand side
(service and
transport vouchers)
for maternal health
services and
- Health system
strengthening
component to
deliver obstetric
care services.
All services
available at facilities
Range of services
especially maternal
and child health
services
ANC, delivery &
Post Natal care
Performance-based grants
to districts and Medical
bureaux incentivise
governance and
management functions.
Facilities Intervention group
included PNFP
only. Public, PFP
in control category.
PFP and PNFP.
Public were referral
points
Public, PFP and
PNFP facilities
Both Public and
Private
PNFP only. Private and Public
facilities
In regard to health services,
the facilities targeted were
those with bias to
HIV/AIDS and the PNFP
facilities
Transition from pilot Failed beyond pilot
but facility
autonomy adopted
by MoH.
From 4 pilot districts
for STI in 2006 to 20
districts for SM.
Successful pilot
informed
intervention phase.
New activities to
build sustainability.
Project had positive
results but to close
in Mid-2015
First pilot informed
phase II
2012-Had seed grants.
2014 introduced
performance grants and
innovation grant in 2015
Governance
roles
National MOH and the
World Bank
provided over all
stewardship
WB played oversight
role. MOH has no
active role.
National dialogue
conducted but MOH
has no active role
UCMB & MoH
offer oversight
Oversight by MOH
& regional
consultation groups.
MoH, professional
bodies are informed
Within Ministry of Local
government.
Have intersectoral
committees.
Within
district
Local government
manage grants on
and disburse to
facilities
VHTs used to
promote voucher
uptake. MOH
guidelines used.
Stakeholder
engagement
throughout the
project
DHTs supervise DHTs perform data
quality, output
audits. Annual
Regional
stakeholder
meetings.
DHTs supervise and
collaborate in service
delivery
Extended districts health
management committees.
District Based Technical
Assistance (DBTA)
partners support districts.
Facility level Intervention
facilities had
autonomy on
utilisation of
bonuses
Facilities determine
how funds are
utilised
Facility
management
structures decide on
fund utilisation
Guidelines on
splitting funds (60%
into operation &
40%) into bonus.
Facilities have
autonomy on using
budget for
operations.
In RBF arm-
facilities had
autonomy on fund
utilisation based on
business plans
In IBF arm-
government
financial systems
maintained.
Facility management
structure decide on
fund utilisation
Health facility
management structures
follow guidelines.

28
Source: Author
Project Feature World Bank
Study
Reproductive
Health vouchers
Project
Safe deliveries
Project (SDP)
Cordaid project NuHealth Project Health Baby
/SMGL Voucher
Project.
Strengthening
Decentralisation for
Sustainability (SDS)
Articulation with human
resource system
Some facilities
shared bonuses
with staff.
No direct benefit to
health workers
No direct benefits to
health workers
40% of funds
received were spent
on staff
In RBF, some
facilities gave
bonuses to staff
Bonuses to staff No direct funds to staff
Medical supplies systems PNFP facilities
procured supplies
form Joint medical
Stores (JMS)
PNFP facilities
received supplies
from JMS. Private
facilities were
allowed to procure
supplies from
accredited
pharmacies.
Public facilities
procured supplies
from National
Medical Stores
(JMS). PNFP
received supplies
from JMS
PNFP facilities
procured supplies
form JMS. Public
facilities received
autonomy to get
supplies outside
NMS.
PNFP facilities
procured supplies
from JMS
Private facilities
procure supplies from
JMS and accredited
pharmacies and
private facilities
recive supplies from
NMS
Public facilities receive
supplies from NMS while
PNFP facilities procure
supplies from JMS.
Health Management
information systems (HMIS)
Adopted HMIS
data
Separate reporting
registers for project
work
Adopted HMIS Adopted HMIS but
developed
computerised
systems. Also had
additional
Community based
verification done by
CBOs.
Use HMIS but have
additional
verification/audit
tools. Developed
computerised
systems.
Use HMIS and
additional project
verification tools
Verification tools used
designed for the project.
Capacity building (CB) One sensitisation
workshop of district
and facility
managers. Health
workers not trained.
Training in program
uptake. Standard
operating procedures
(SoPs)
Provided some
supplies for
obstetric care and
trainings of staff
CB for district
health management
teams
Support districts in:
Staff recruitment;
Essential medicines
Business planning.
Support supervision
Support districts in
development of plans
and implementation
arrangements.Facility
investements are
supported.
Support districts in
development of plans and
implementation
arrangements.
Social marketing Not included Voucher distributors;
Poverty grading.
Radio talk shows.@
voucher at 3000shs.
Community
engagement
meetings and
dialogues held
Community based
organisations as
verifiers.
Not applicable community structures
promote vouchers.
Not applicable
29
Conclusion: 4.5
In summary, this chapter looked at the description of a total of 7 RBF initiatives that have
been implemented in Ugandan health sector since 2003. These are diverse in many attributes
as elaborated in Table 3: Design features of RBF schemes implemented in Uganda. The
schemes differ in a substantial way in terms of results being secured, target populations, their
design and implementation arrangements (partnerships, performance audits and payments
systems).Some are supply side interventions while the others are majorly demand side
initiatives (voucher schemes).
Generally, Uganda has seen both supply side and demand side RBF schemes. The supply side
schemes covered included the World-bank Study (2003-2005), the Cordaid Pilot (2009-2015),
the NuHealth project (2011-2015), and the proposed BTC/MoH Pilot project (2015-2019).
Another program, the Strengthening Decentralisation for Sustainability (SDS) managed under
Ministry of Local government and provides performance-based grants to districts to deliver
social services including health was also described. On the hand, several demand-side
schemes (essentially vouchers) that have been implemented in Uganda were described. These
included the Reproductive Health Voucher Project by World Bank (2006-2011), the Safe
deliveries project (2009-2011) and follow on Maternal & New-born study and the Saving
Mothers Giving life (SMGL) initiative.
There are convergence and observable trends along certain dimensions of scale-up. These are
examined in depth in the next chapter 5. We were convinced that understanding linkages
between different initiatives and how and why the different models perform within the health
system would yield more robust evidence upon which policies and practices for national
scale-up, integration and sustainability of RBF mechanisms can be based. These various RBF
schemes also represented the major efforts between Government of Uganda, Donor and
development agencies (e.g World Bank, DFID and USAID), researchers and academic
institutions and other agencies such as Non-Governmental Organisations in the design,
implementation and evaluation of these initiatives. They hence provided a vantage point to
explore how various the factors and actors facilitated or hindered buy-in and integration of
RBF into national health system and policy (confer chapter 6).

30
CHAPTER 5 : THE MULTIDIMENSIONAL SCALE UP OF RBF
IN UGANDA
5.1 Introduction
The preceding chapter 4 described 7 diverse RBF pilots that have been implemented in
Uganda from 2003 to 2015. This chapter presents findings related to objective 2. That is, it
provides an examination of the extent to which the scale up of RBF has been achieved along
the various dimensions described in 2.3 above. It provides a synthesis of trends in design and
implementation of RBF schemes summarised in Table 3: Design features of RBF schemes
implemented in Uganda. A timeline (Figure 8: Timeline for multi-dimensional scale up of
RBF in UgandaFigure 8) has been developed to capture the key milestones for RBF
development over the last 12 years. These critical junctures are provided a long four
dimensions of scale up namely population coverage, service coverage, health system
integration and Knowledge. In the next sections, the main findings in each dimension are
presented.
5.2 Population coverage
The dimension of population coverage is about covering more people. This could be achieved
by 1) expanding geographical or administrative area covered, 2) covering more socio-
economic groups (e.g. from poorest 20% to poorest 40%), 3) removing demographic (age,
gender) restrictions or 4) expanding the entitlement status (e.g. extension to members of a
specific voucher/insurance program).
As shown in the timeline (figure 3), generally, there have been RBF schemes across all
regions in the country. However, this geographical coverage has not progressed
systematically. In absence of a national RBF scheme, the various schemes seem isolated as
each project has had to define its geographical scope depending on the factors elaborated
above under each project (in Chapter 4).
In terms of number of districts covered, some schemes had no change in area covered over
the course of implementation. For example, the first RBF scheme (the WB PBC study 2003-
2005) was implemented in 5 districts that included: Mukono (in Central region), Jinja
(Eastern region), Kyenjojo & Bushenyi (Western region) and Arua (Northern region).
NuHealth (2011-2015) has been implemented in 6 districts in Acholi Region and 4 districts in
Lango region since inception.
Some schemes, however, had expansion in geographical coverage over time. For instance, the
RHV project started in 2006 in 5 districts in western Uganda but expanded in 2008 to 20
districts (in the same region). The SDP (2009-2011) started as a pilot in one district but
implementation was expanded to 2 districts in eastern Uganda. Considering the Saving
Mothers Giving Life Initiative (SMGL), scale up was noted in 2013 when project expanded
from 4 districts in western Uganda to 10 after 6 districts in northern Uganda were added.
Recently (in early 2015), the SDS project increased geographical scope to 50 districts when
15 northern districts were added to the 35 districts that the project was covering in central,
western and eastern parts of the country. Whereas all the above cases point to schemes
expanding geographical coverage, the Cordaid project contracted geographical scope from 3
intervention districts to focus on one in 2013. Prospectively, BTC and MoH are proposing
implementing another RBF scheme in 15 districts covering two regions of Rwenzori and
West Nile. Furthermore, the RHV Phase II is planned to cover the eastern region in addition

31
to the western region covered in phase I. Basing on the above cases, it is difficult to anticipate
how these planned schemes will change over time.

Figure 8: Timeline for multi-dimensional scale up of RBF in Uganda
Population coverage
Practical institutionalization
Formal institutionalization
Service coverage
Knowledge

33
The above variation in geographical scope (and variation in service packages explained
below) meant that there has been much diversity in the population covered. In terms of
reaching out to particular groups of people, targeting the poorest individuals and households
was documented in a few projects. For example, some demand-side vouchers projects namely
the RHV project and MANEST (a follow-on voucher project from the SDP) had explicit
targeting of the poorest segments of the population. In other cases, geographical targeting was
used- where the entire population was considered poor. Such schemes intended to cover the
entire population within the geographical area covered under the scheme.
Reasons for expansion in population coverage:
Generally, schemes that have had successful pilots had expansion in geographical scope.
More so, availability (or lack thereof) of funds significantly influenced geographical scale-up
of several schemes. For instance, the World Bank PBC study was not scaled up because of
unsatisfactory results and the funds run out (WB/CIDA/MoH 2005, KIs). However, the World
Bank RHV project was scaled up from 5 districts to 20 districts after a successful pilot. The
expansion of this RHV Project I was also possible after a grant from GPOBA (a multi donor
trust fund administered by the WB) was secured in late 2007. In fact, the grant also led to
expansion of the service package from covering STI treatment only to provision of a more
comprehensive package of maternal and child health services (WHO/MoH 2014). The SMGL
was also expanded from 4 districts to additional 6 districts in northern Uganda because of the
success of the pilot (“proof of concept”) phase and obtaining additional funds from ELMA
foundation (SMGL 2015) in 2014.
Conversely, the case of Cordaid provides an example of shrinking in geographical scope from
three districts to one. This was also related to reduction in funds. After the scheme extended
to public facilities, it became very expensive to implement in all three districts as reported by
one DHO.
Initially it was Jinja, Mayuge, and Namanyigo [districts] but when the funding was
not adequate they zeroed on the population in Kamuli district. So the population that
we are using to calculate the targets for the agreed indicators is that of Kamuli
[district] [DHO].
Other reasons for change in geographical scope have been unique to the schemes. First, the
SDS program had its administrative scope extended to 15 districts in Northern Uganda to
cover a vacuum left when another USAID funded program (NuHites) closed abruptly in early
2015. Secondly, NuHealth was initiated in northern Uganda to generate evidence on the role
of RBF in strengthening health systems in the Post conflict region (NuHealth 2013a, 2012).
On the other hand, The SDP was initially in implemented two districts in eastern Uganda but
the number of districts changed to four (4) when Kamuli and Pallisa districts was split into
Buyende and Kibuku districts respectively. Population coverage (pregnant women and
transporters) is expected to have remained the same.
5.3 Service coverage
The dimension of service coverage is concerned with changes in aspects such as 1) covering
more facilities, 2) level of health facilities involved (e.g from health centres only to referral
hospitals as well), 3) the range of affiliated health facilities (moving from private facilities
only to include public ones), and 4) type of services (e.g. from family planning to all
reproductive health services or all types of services, including chronic non-communicable
diseases).

34
Regarding service packages, there has been some convergence on the benefit packages across
the two types of RBF schemes over the years. All the demand-side schemes (SDP, RHV
scheme and the SMGL) specifically provided Maternal and related child health care services.
On the other hand, the supply-side schemes (PBC study, NuHealth project and Cordaid
project) adopted a general service package from the Uganda national Minimum Health Care
package (UNMHCP). Similarly, the planned BTC/MOH project is expected to deliver the
UNMHCP. However, considering the indicators used in the schemes, there has not been a
specific focus on the Non-Communicable Diseases (NCDs). As an outlier, SDS targets
strengthening district leadership/ governance structure to enhance delivery of social services
including health. Never the less, SDS has specific focus on HIV/AIDS related health services.
Another finding in regard to service coverage is that involving the public sector in RBF
initiatives has progressed slowly as one respondent remarked;
“[RBF is] not at national level yet…but it’s been slow when it comes to bringing
public facilities on board” Academic.
Most RBF schemes have been implemented in the private sector especially private not for
profit (PNFPs) sector. In the first (WB) pilots, the public sector was minimally involved. The
public health facilities were just part of the control group (during the PBC study) or referral
points (in RHV project). In 2010, the SDP became the first RBF scheme to include public
health facilities among the service providers in their voucher project. On the supply side RBF,
it was only recently in 2013 that the Cordaid Pilot was extended to the public sector in Kamuli
district. In fact, Cordaid remains the only supply side RBF scheme to have been implemented
in Uganda’s public health sector. The reasons for the bias toward the private sector and
apparent avoidance of the public sector by the RBF schemes are discussed in the next chapter
6.
Regarding levels of health facilities, the findings indicated that all levels of health facilities
have been involved in the RBF project so far implemented in Uganda. These have ranged
from drug shops/pharmacies (for example under RHV project) through health centres II, III,
and IV to hospitals. Another set of providers in demand side RBF schemes were the
transporters hired to transport clients to health facilities. So far two voucher initiatives (SDP
& SMGL) have used transport vouchers to complement the service vouchers. The SDP was
the first project to introduce transport vouchers in 2009.
5.4 Health systems integration
The main concern under this dimension was to appreciate how and why RBF approaches
introduced as pilot schemes operating partly outside the national health system have not
succeeded in being incorporated within the routine functioning of the health sector. The
analysis also examines the readiness of the national context to embrace results orientation in
broader government systems.
5.4.1 Areas of Integration
This highlights the areas of integration in terms of the six health systems building blocks as
proposed by the WHO.
1) Regarding articulation of RBF with the overall health policy goals (governance), some
integration has been noted. In terms of aalignment with governance structures, RBF has
worked closely with districts bypassing the national level MOH. This was attributed to the
decentralised system of governance in Uganda which empowers districts to be

35
independent administrative units with responsibility over service delivery within their
jurisdiction. Progressively, RBF has been explicitly mentioned in the MOH strategic and
operational documents. For example the Health Sector Development Plan (HSDP)
(2015/16-2019/20) refers to RBF as the financing mechanisms for the plan (MoH 2015a).
The 20th
Joint Review Mission in 2014 adopted a resolution to have RBF as a financing
strategy for the HSDP. Furthermore, the Health Financing Strategy (HSF) 2015/16-
2024/25 emphasises RBF as the main pillar of the financing strategy for the next 10 years
in Uganda and proposes reforms to transform Uganda’s the financing mechanism from an
input to a results oriented focus in order to improve decision making and accountability.
This commitment is explicitly captured in the Draft HSF ( page 33):
The sector shall emphasise Results Based Financing (RBF)/Performance Based
Financing (PBF) as a mode of output based provider payment. This will be rolled out
systematically and progressively to cover the whole country by the end of this HFS
(MoH 2015b;33).
2) Harmonious articulation of RBF mechanisms with the existent human resource system has
not progressed much especially in the public sector. Well, some schemes like Cordaid had
explicit guidelines for how bonuses at facilities could be shared among the staff; these had
to be enforced through special memorandum of understanding with the facilities which
were outside the normal government arrangement. On the contrary, other schemes did not
offer any guidance regarding this matter and the decision on utilisation of funds from RBF
was left to the discretion of the health facility in-charges/health management committees
where they were functional. As result, some facilities invested in infrastructure while
others just organised social events. While it worked well under the SDP where there was
more investment in staff than other areas such as infrastructure, this lack of clarity created
disincentives and undermined performance of the schemes. This problem was highlighted
by the quotes below.
“The project also went wrong in one way or another because money was given to
hospital management who did not know how to use this money well. I mean they did
not make this money reach the health workers who were delivering the services”
Implementer.
“One time, XX hospital scored very well and got good money. The administration used
all the money to build the gate. The gate was very beautiful and yes, everybody
admired the gate but the gate was not the one that generated this money. It was the
staff. So instead of motivating the staff this demotivated them” Implementer.
Some attributes of human resource systems in public service were noted to be
incompatible with RBF arrangements. These included civil servants being ‘permanent and
pensionable’ with no performance management systems in place to align their
performance with the systemic goals, health facilities having no powers to recruit new
staff or fire underperforming staff and rigid staffing norms within public sector. The
following quote captures this reality:
“The moment you introduce this PBF, the health facilities are meant to be
autonomous- to take decisions on what priorities they want to fund, to hire staff, to fire
ifneedbebutourpublicsectorguidelinesandstandingordersdon’tofferthehealth
facilities with this autonomy that we need for PBF to effectively function”(DHO).
36
3) In regard to positive spill-over effects of the RBF schemes on supply chain for drugs and
medical supplies, the PNFP’s Joint Medical Stores featured prominently in the RBF
implementation. This was attributed to the fact that many schemes were implemented
within the PNFP sub-sector. On the other hand, government’s decision to grant monopoly
to National Medical Stores (NMS) as the sole supplier of all medical supplies to
government facilities was found to be constraining to RBF implementation in public
facilities. In particular, delays in supplies undermined the ability of facilities to promptly
address stock-outs in supplies. This issue was well summarised in the quote below:
“Weknowthatcurrentlygovernmenthas centralized the supply of drugs. But as far as
performance based financing is concerned, we needed to allow some leeway for the
service providers to identify other suppliers of these drugs. We appreciate that
National Medical Stores has improved the availability of medicines, but we are shy to
talk about [un]availability of equipment for example delivery kits at these facilities. So
if national medical stores are not providing the equipment and the facilities cannot
buy [these]somewhere else, then we are likely not to equally achieve improvement in
all areas” DHO.
4) Regarding integration of existing health information system into RBF, all schemes were
noted to use at least parts of the HMIS as a basis for computing results of service delivery
and rewarding facilities. However, it was very conspicuous that all schemes opted for
additional indicators which were not captured in the routine HMIS. This meant that either
the normal registers were expanded (Cordaid, NuHealth, World Bank study, SDP, SMGL)
or separate ones were created and used. For example, RHV &SDP introduced governance
indicators that were not in routine HMIS.
Furthermore, it was noted across all the schemes that additional data collection systems
were put in place to verify results. These included population based and facility surveys,
and needs assessments. Relatedly, a progression from manual/paper-based systems to
computerized information systems was noted over the 12 year study period. The recent
schemes (Cordaid, NuHealth and SMGL) all have computer-based information systems
compared to the first study that relied on paper-based system. Similarly, the trends in
general HMIS have moved to more computerised platforms.
Overall, there has been appreciation of the need for a functional health information system
for RBF to work.
“[There has been] realization that we need improved data or information system as a
pre-requisite [for RBF]” Academic.
5) Integration of RBF schemes within existent health care financing arrangements showed a
mixed picture between public and private sectors. Whereas compatibility of RBF with
PNFP sector was easy to achieve, it was rather hard in the public sector. The public
finance systems from Ministry of Finance created bureaucracies that undermined timely
and appropriate flow of funds. Prescriptive procurement guidelines in public sector are
often characterized by procurement delays. Conversely, the RBF funds reportedly fitted
well with the financing arrangements in the PNFP subsector by complementing the user
fee charges and government subsidies to these facilities. This compatibility of RBF within
PNFP set up was attributed to the flexibility in financial management systems in the
private sector. One respondent asserted:

37
“The private sector is more flexible than government; it can navigate [RBF] more
easily than government. In government they prescribe procedures and if you find a
road block you are supposed to stay there. In the Private Sector when you find a road
block, you can start changing direction and you might find a solution.” Policy Maker,
Private sector.
Another fundamental challenge reported was an aligning RBF reform with other financing
reforms in the health sector being pushed for at the same time. For example, some groups
were pushing for insurance systems while another one was working on resource-allocation
formula. Creating the right balance among these mechanisms was reported as a challenge. At
the 2nd
national consultation workshop, a participant from the UN local office observed the
fragmented reforms in health financing:
“The current dialogue is discussing different aspects of health financing (health
financing strategy, health insurance, PBF, allocation formula, etc.) in isolation, while
it will be opportune to have a comprehensive discussion encompassing all aspect of
health financing in function of the move towards UHC. ThereformeffortsinUganda’s
health sector like the National Health Insurance (NHI) Bill, the resource allocation
formula and the launch of purchasing mechanisms as RBF, need to be
harmonized”(BTC/MoH 2015:14).
5.4.2 Depth of integration:
This is in recognition of the fact that there can be substantial differences between formal
statements and actual practice. It measures institutionalization along the four attributes/facets
proposed by Meessen (2009) namely: the formal state, the practiced state, the expected state
and the moral state as elaborated in the conceptual framework in ( 2.2) above.
1) Formal institutionalization; There are recent efforts to formally institutionalise RBF in
Uganda. These have included two national consultation workshop on RBF held in March
2014 and February 2015. These efforts are complemented by recent articulation of RBF in
health sector documents -the HSDP & HFS.
A Technical working team (TWT) was set up at the MoH in May to steer the RBF policy
development. TWT is multisectoral team composed of members from stakeholder
constituencies for RBF. However, the TWT is yet to be functionalized as observed by lack
of any meetings four months since inception.
2) Institutionalization in regard to level of practice entails growing support from health
system stakeholders (staff, unions, aid partners). Practical institutionalization was
examined in terms of the actual behaviors of actors. In Uganda, the role of the
development partners in providing technical assistance and funds for RBF can be viewed
as building institutionalisation of RBF. It is obvious from Table 3: Design features of
RBF schemes implemented in Uganda that different donors are instrumental in advancing
RBF in the country. These include UN agencies especially the World Bank, bilateral
agencies such as USAID, CIDA, UKaid, BTC and international NGOs such as Cordaid,
MarieStopes Uganda, Montrose, Health Partners International and Pricewaterhouse
Coopers.

38
The sustained active involvement of international actors in RBF implementation using
external agencies has undermined the capacity of public systems to prepare for RBF
institutionalisation. This was particularly true regarding verification roles as one respondent
affirmed:
“Schemes havemoved slowly from external agencies such as MarieStopes to using
district officials and agencies for example schemes by NuHealth & Cordaid”
Academic.
Within government, sub national structures (districts) have recently played major roles in
RBF implementation. Recent schemes such as NuHealth and Cordaid have given districts
teams verification roles to monitor the projects which have greatly boosted the
implementation capacity at this level.
“Experience and capacity of implementing [RBF] has grown…the ministry is very
appreciative &supportive” Project Manager.
“There are many experiences of implementing [RBF] -so capacity to implement has
grown” Project manager.
Unlike local governments, central level MoH has been less involved in RBF implementation.
For example, it is documented that the PBC study recruited and positioned advisors for RBF
in MOH. These advisors left after the RBF pilot.
Academic institutions especially Makerere University School of Public Health have been very
active within RBF implementation in Uganda. They have contributed as implementers (for
WB study and SDP project) or providers of knowledge on RBF implementation (for example
Ssengooba et al 2012). This has contributed to institutionalisation by generating evidence at
local levels.
“Academicinstitutionsareimportantindesigningrobustdesignstogenerateconcrete
evidence. This is important to demonstrate that RBF works ornot”Academic
Respondents noted that RBF had created opportunities for business-oriented firms to
participate in health sector developments. Reference was made to activities like auditing
results and selling vouchers. Institutionalisation is rapid within the business firms that
implement RBF. One respondent argued that:
“RBF has brought many non-medical organizations whether you want to call them
entrepreneurs, to also be active in the health sector. You will hear Pricewaterhouse
Coopers is now a key player in RBF. You hear MarieStopes is getting money to
distribute vouchers. So in a sense, there are business opportunities RBF opened up at
many levels not necessarily within the service delivery chain but also outside of it.
Those who hold the money get some business. Those who provide technical assistance
get some business. So there are a lot of opportunities to build other businesses around
health”Academic.
3) Progression on the expected state is possible only if enforcement mechanisms such as
contracts, guidelines, training, and coordination platforms are set up and it is observed by
interacting parties that everyone complies with one’s commitment.

39
It was noted that all RBF schemes adopted Memoranda of Understanding with the various
players to formalize their relations. These have not been standardised because there is no
national model for scale-up.
4) As for institutionalization along the moral state, we considered the emergence of a
working culture aligned with the RBF philosophy (i.e. commitment to results,
entrepreneurial spirit, transparency and accountability, and an eagerness to use routine and
evaluation data to inform decisions. The findings were as follows:
Overall, there has been growth in interest in RBF in Uganda over the last decade. For
example, it was noted in the MTR for the Health Sector Strategic and Investment Plan
(HSSIP) 2009/10-2014/15 that MoH staff had “studied the Result Based Financing and
voucher system with a view to introducing performance based financing [in the sector]”
The interview respondents noted recent discussions between donors and government agencies
to adopt RBF as sign of advancement against the moral state. One respondent commented:
“PBF has caught attention of MoH and many donors. There is ongoing synthesis of
evidence and recently even discussions of one model” Development partner
Another respondent pointed out that a highly placed policy maker at MoH was in support of
RBF reforms:
“A high ranking official [XX] at MoH is talking about changing the financing system
toRBF” DHO.
The respondents further pointed to the fact that some district leaders and health facility in-
charges had started to openly advocate for RBF. Reference was made to request from leaders
in districts without RBF to have schemes extended to their areas:
“Managers like DHOs now advocating for it to be scale-up” Project Manager
“Buy in [is being realised] from everywhere even districts with no [project]
implementation”Project manager.
Beyond interest, there are recent efforts at regional level pushing Uganda to commit to
results-oriented management. For instance, Uganda is a member of the AfriK4R initiative of
the African Community of Practice (AfCoP) that “seeks to help accelerate regional
integration; establish effective public financial systems; facilitate trade; and improve the
business climate on the African continent through knowledge and best practice exchange on
results-based management between member states of COMESA and the West African
Economic and Monetary Union (WAEMU)” (African Development Bank Group AfDB
2015;1). In fact, a national workshop was held in late March 2015 to discuss this how Results-
oriented culture should be integrated into national programs: The workshop objective was
summarised as follows:
Spearheaded by the Office of the Prime Minister, the learning and planning event
[aims at ]consolidating country efforts at stimulating a results-oriented culture; while
positioning managing for development results (MfDR) as a change management
process for more results-focused and accountable programmes and implementation
structures (AfDB 2015;1, Monitor 2015)
Furthermore, there seemed concurrence within government to have performance contracts for
top civil servants in Uganda. For example New Vision 2013, reported that all top managers in
civil service were to receive three year contracts renewable on demonstrating satisfactory

40
performance. Subjecting top level managers to performance-based contracts was recently
reiterated during the launch of the second National Development Plan in June 2015:
“Government has institutionalized sector working groups, and will from henceforth
compel all accounting officers to sign performance contracts in line with the NDPII
results and targets” ( UNDP 2015;1)..
Generally, there was concurrence that the public sector management systems were not yet
configured to support RBF. However, result-oriented thinking is being introduced in the
budgeting frameworks In Uganda. The study found existing government-wide initiatives such
as Output-based Budgeting Tool (OBT).
“We can see attempts on the part of the government to begin to think about results
with the output based budgeting they are implementing through the OBT. And now,
they are talking about the Performance based budgeting. You can see in some sectors
they are doing the performance contracts. There is an attempt to begin holding people
accountable for the financing they are receiving”Development partner
However, some respondents indicated concerns that these government mechanisms are not
fully operationalized to ensure that budgeting is linked to results and that good performance is
rewarded. This renders OBT sub-optimal in enhancing performance culture as the remarks by
one policy maker below indicate:
“This [OBT] is notreallyperformancebasedinitiativeastheydon’tlinkperformance
to rewards. There are no mechanisms to utilize the information generated. They are
mimicking RBF” Policy maker, MoH.
The relevance of OBT to the health sector was also questioned. The unique nature of delivery
of health services was not addressed. For example 1) usually different teams have to work
together to deliver a certain result and 2) results may require prolonged interventions for
example chronic care services. One policy maker from MoH argued that:
“….. In fact, the[OBT]toolsdon’tcapturethepeculiarnatureofservices inhealth
sector where services are provided as packages and sometimes on a continuous basis”
Policy maker, MOH.
5.5 Scale up along Knowledge dimension
Scale-up of knowledge has progressed in terms of robustness of knowledge which can
happen in different ways: 1) moving from intuitions, to explicit hypotheses and eventually to
rigorous evidence 2) Progression from external control to internal control: from knowledge
held by international consultants to strong command by national cadres of the Ministry of
Health; 3) from a wholly theoretical understanding (explicit knowledge) to one informed by
practical experience (tacit knowledge). Knowledge generation, transfer and translation is
important to drive a health reform including the RBF agenda. This sub -section illuminates
the extent to which knowledge aspects regarding understanding RBF as a health financing
strategy in Uganda have progressed. Several aspects were explored as elaborated below.

41
5.5.1 Appreciation of the benefits of RBF towards improving Health systems
performance has progressed.
The respondents at the operational level pointed out several benefits of RBF. Reportedly, RBF
stimulated both demand and supply sides to perform better. On supply side, the respondents
indicated that bonuses were important in motivating staff at health facilities to be more
productive as one facility manager observed:
“… Staff attitude towards work improved because of direct financial benefit” Facility
manager
In some cases, RBF projects improved responsiveness of the management to the operational
needs at their facilities by supporting innovative solutions to management problems.
Respondents pointed noted that RBF stimulated infrastructural development at some facilities.
The funds were used to procure drugs and health supplies on time to prevent stock outs. The
following quotes from facility mangers reflect these views.
“We were able to meet our local needs-undertook renovations, bought facility
equipment; electricity was reinstalled after [paying] huge electricity bill” Facility
manager.
“We bought facility equipment like electric kettle, gum boots, aprons” Facility
Manager
“The RBF money got was used to buy drugs and [it] was not from government”
Facility manager
Demand side RBF was reported to have improved health seeking behaviours. This
improvement was attributed to several opportunities that RBF offered including making
facilities functional and further encouraging health education.
“[Through health education], the mother understood at least the three components of
maternal health that is ANC, delivery and PNC” Field staff
“[The Scheme made it] easy access to the facilities by the mothers so the mothers
were saved from the walking long distances. It was the responsibility of the
transporters to look for the mothers [to take to the facilities] as they were also
gaining” Field staff
5.5.2 Cross learning among schemes has improved but slowly:
Respondents observed some cross learning among the various schemes and some learning
from other schemes was reported by some implementers. The SDP reportedly visited the
RHV pilot to learn about voucher design and verification tools. NuHealth Project reportedly
learnt from Cordaid the payment systems. Prospectively, it was also reported that
accumulated evidence from other pilots is informing new RBF designs going forward. As one
respondent commented:
“The generated evidence from other schemes is being used to informed the BTC pilot
and national RBF model” Project manager
Recently, there have been opportunities to share learning on RBF at the national level. Two
national consultation workshops: the first in March 2014 organized by WHO & MoH and the
second workshop organized by MoH & BTC in February 2015 have been organised. These

42
workshops provided an opportunity to share evidence and experience from both near and far.
Evidence was presented from nation-wide RBF schemes in Rwanda, Burundi, Argentina and
Zimbabwe. Similarly, evidence from RBF research and pilot projects in Uganda – Cordaid in
Kamuli District and NU-Health project in Acholi region was also shared. These cross learning
opportunities have raised some awareness and interest in understanding how RBF works. As
reported by the key respondents.
“MoH has tried to bring different people who have done different schemes under one
rooftoshareexperiences” MoH policy maker.
“[I am] aware of other schemes much; we got to know them when WHO called us
together as mobilisers” Project manager.
“In the districts where they work, it [RBF] has been well understood and highly
appreciated. It has been appreciated in MOH and a number of discussions are going
on around it” Project manager.
However, knowledge about various RBF schemes varied across the various respondent
categories. It was generally good among academics, then district level staff and lowest among
national level policy makers. It was not surprising as many academics interviewed had
worked on RBF related research before.
“[I am aware of] Saving mothers giving lives (SMGL) in western Uganda, NU
Health,onedonebyCordaidinJinja,MarieStopes,there’salsooneIknowfundedby
the Catholic Church but I have forgotten the name” Academic.
5.5.3 Progress in knowledge of key design and Implementation considerations:
Generally, respondents reported that there has been progress regarding knowledge about
design and implementation of RBF and had enhanced implementation capacity among certain
players in the sector. This was mostly reported by previous implementers.
Respondents expressed knowledge that incentives and bonus structures adopted are important
for the success of any RBF initiative. For example as captured in the following quotes, they
pointed out that conflicts arise if the financial management system is not transparent and the
health workers do not directly benefit: or feel left out.
“[We have learnt that] streamlining financing system is very vital for success [of
RBF]” Project manager.
“Bonuses should not be all spent at facility level… not even on staff parties. To
appreciate RBF, people should feel the money make a difference in their pockets and
lives” Project manager.
Respondents recommended that RBF systems should reward team work and not leave out
certain categories of workers. Respondents highlighted the need to work closely with key
stakeholders and to actively engage them to promote buy-in. One respondent emphasised:
“It is important to sensitize the stakeholders during the planning phase to ensure that
your project succeeds.” Project manager.
The key informants emphasised the need to collaborate with local governments as very
important stakeholders under decentralized system of governance. One respondent

43
recommended that each scheme should have a focal person at the district to follow up
implementation activities while another observed:
“Using district officials as supervisors in a way brought about ownership to the
project. When these people to the lower units, they are forced to have an input”
Project manager.
The study participants pointed out more issues to consider during RBF design and
implementation. They observed that 1) bureaucracy leads to delays and affects performance in
decentralized system and 2) finding the right fit/model to satisfy the interest of every
stakeholder is impossible and leads to delays. They further pointed out the need to strengthen
the capacity of the health system before/alongside RBF to ensure that adequate functionality
exists at start. This would entail adopting learning agenda to generate evidence as the
implementation ensues. These issues are elaborated in next chapter under the section on
recommendations for RBF implementation in Uganda.
5.6 Conclusion
In conclusion, this chapter has examined the scale-up of RBF along four dimensions namely
population coverage, service coverage, health systems integration and knowledge. The scale-
up in population coverage did not follow a systematic process and was contingent on the
specifications and interests of funding agencies, not national/sector plans. Almost all regions
in the country have had RBF schemes but the western region has had the most number of
pilots. It is not clear why the region was elected or whether the services implemented were
the most needed. All demand side schemes offered packages under maternal and related child
health services. Supply side pilots provided more general packages from the UNMHCP and
targeted the entire population within reach of the facilities. However, NCDS were notably
unconsidered by all the schemes. There is also little progress in implementing RBF in public
facilities. Only three schemes (SDP, Cordaid pilot and to some extent the SMGL initiative)
have been implemented in public facilities.
A mixed picture was found regarding health system integration and some areas have
progressed compared to others. Pertaining alignment with governance structures, RBF has
worked closely with Districts bypassing the national level. RBF is still incompatible with
some aspects of human resource systems in Public service. The current health financing
reforms are fragmented and there is still need to align RBF with other financing reforms such
as National Health insurance and Resource allocation formula. On the other hand, RBF has
resulted in improvements in HMIS by encouraging quality data management based on
computerised systems and regular complementary verification/validation exercises. Regarding
institutionalisation, there are recent pointers to formal institutionalisation processes within the
health sector such as setting up of Technical working team at MOH and explicit reference to
RBF in the HSDP and Health financing Strategy. In regard to practical institutionalisation, the
development partners contributed to institutionalisation of RBF. Similarly, non-medical
organisations such as NGOs and Academic institutions have found increasing opportunities to
work in the sector by supporting RBF related processes. However, depending on non-state
agencies has undermined institutionalisation of RBF within the government entities.
Concerning knowledge, appreciation of the benefits of RBF and important design and
implementation issues was noted among some categories of respondents. Knowledge is
mostly at service provider level and less at systems or policy levels. This reflects the
implementation space where RBF has integrated with the health system. Recent efforts to
bring stakeholders together were noted to improve awareness among key stakeholders.

44
CHAPTER 6 : FACTORS AND ACTORS THAT INFLUENCED
RBF DEVELOPMENT IN UGANDA
6.1 Introduction
This chapter presents findings on the factors and actors that have influenced RBF
development in Uganda (objective 3). An effort has been made to consider drivers of RBF at
national level and hence the factors are general rather than specific to the schemes. As
indicated in the previous chapter, there has been progress along various dimensions but there
is yet to be a national RBF model/scheme in Uganda. However, there seems to be recent
momentum to adopt RBF nationally. This chapter further considers the factors that explain
these dynamics (objective 4). Despite these recent dynamics, it was noted that much more
needs to be done. Therefore, the chapter concludes with the views on prospects and
recommendations for national RBF scale-up.
6.2 Factors shaping RBF development in Uganda:
The major factors that have influenced RBF development in the country included 1)
contextual factors (external to the country, within government and internal to health sector)
and evidence-related (generation, sharing and utilisation).
6.2.1 Contextual factors and their influence on national RBF scale-up.
The respondents were requested to reflect on what they think could be the contextual factors
influencing RBF development in Uganda. These contextual factors were divided into those
external and internal to the country. The internal factors were sub divided into those within
and without the health sector. The emerging themes are summarised in the subsequent section.
6.2.1.1 Factors external to the country:
External contextual factors included donor influence, importation of evidence and policy
transfer, Global movement toward targets and frustration with failures of existing financing
mechanisms were noted to be important drivers for RBF. These are elaborated below.
6.2.1.1.1 Donor influence
Respondents identified donor influence as a very big driver of the RBF agenda in Uganda. All
RBF schemes have depended on donor support. As summarised in table 4, the funders of RBF
have been many and diverse. These included the World Bank, USAID, CIDA, UKaid
(formerly DFID), BTC, Cordaid etc. Reportedly, Uganda has a high dependence on donors for
funding the health sector which makes her susceptible to donor influence. As one respondent
highlighted, the donor funding has conditionalities, some of which pertain to use of results-
based financing mechanisms.
“[Donor] support comes already wired to RBF” Academic.
The increasing interest in RBF among donors was attributed to domestic forces within the
donor countries. Resources available for aid in developed countries reduced due to the 2009
global recession and heightened the need to demonstrate results within the donor countries.
“Ithinkthefactthattheresourceenvelopegloballyisalsogettingsmaller,thereis an
increased push for results. The tax payers are asking their governments whether there
is ‘value for money’ in the investments. They ask: where are you investing these

45
billions? Can you demonstrate the impact of our intervention? So [the] increased push
for results is a global trend due to increased scrutiny for ‘value for money’”
Development partner.
“[Donors]arebigproponentsandImustconfessthatit’snotonlybecausethey can see
that the RBF schemes are working in Uganda, but also that from their headquarters,
there is this push to drive their people here to push for RBF. There is a real push for
valueformoney” Development partner.
Some respondents observed that frustration with exiting financing modalities among the
donor community has been an important external driver of RBF agenda in Uganda. They
reported that input-based financing had not made a significant improvement in health system
performance hence the push for a performance-based system under RBF:
I think everyone……, the first and most important fact is that everyone can see that
inputbasedfinancingisnotgettingmuchdone.It’sveryclear” Development partner
“There is frustration about wastages and leakages at the moment. A lot is put in
without much comingout” Academic
Other respondents attributed the donor push for RBF to the emergence of evidence on the
extent of aid effectiveness or value for money from their development assistance. This view
was explained below:
“The motivation to adopt RBF is based on analysis of aid effective strategies and it is
widely acknowledged that handing out grants for which you seek only financial
accountability is not necessarily the best way for achieving development outcomes
.That puts aid effectiveness to a great stand still. So RBF is in response to some of the
dilemmas that donors face” Project manager.
6.2.1.1.2 Global Movement towards RBF
The respondents pointed out that there is a global movement pushing RBF across the world
to low and middle income countries and that RBF advancement in Uganda is a response to a
global phenomenon. One respondent asserted:
“Thereissomething[recommendation] from WHO about countries to develop Results
Based financing….so there is a global initiative to have results based financing
systemsinplace” Policy Maker, MoH
This interest in RBF was evident in the strategic documents of some donors. These documents
show that donors increasingly consider making aid results-oriented the preferred way of going
about the development work:
I want Payment by Results to be a major part of the way DFID works in the future. We
will develop a framework to ensure that all of our Payment by Results projects are
rigorous, independent with comparable evaluations in place so that we can learn more
about what works best, in what circumstances. We are committing to making those
evaluations public, so that others can learn from them too. DFID 2014;3
Several respondents reported that there are global initiatives that demand focus on achieving
certain targets that have been key in pushing the RBF agenda in Uganda. The Millennium
development Goals (MDGs) were reportedly important drivers of RBF pilots especially the

46
demand side projects in Uganda. The voucher schemes that have been implemented in
Uganda were mainly to improve MDG 4 (Reduce Child mortality) and MDG 5 (Improve
maternal health). One respondent observed:
“Yes, with the MDGs, I think [they have had an influence] especially within the last
five years when there was that push to accelerate progress towards achieving the
MDGs. They really made a case for RBF. And you can see, even in academia the
publications that are coming out especially in countries like Rwanda, RBF was
positioned as a particular tool that canhelptoachievetheMDG’s.So MDG influence
has really played a big role [in pushing RBF] particularly in the last 5 years”
Development partner
Respondents also mentioned that the Global Fund to Fight Malaria, Tuberculosis and
HIV/AIDS has a performance-based framework which is used as basis for subsequent
funding. Furthermore, the new health agenda of achieving Universal health coverage was
highlighted as an important driver for RBF in Uganda. One policy maker noted:
“I look at RBF as partof the ingredients of the universal health coverage. It’s not
really that they feed into each other;RBFfeedsintotheuniversalhealthcoverage.It’s
oneofthemechanismstoachieveUniversalHealthCoverage” Policy maker, MoH
Indeed, the UHC agenda seems to be a big driver for RBF going forward as was noted during
the national consultation workshop on RBF held in February 2015. The MoH’s Health Sector
Development Plan (HSDP 2015/16-2019/20) focuses on achieving Universal health coverage
(UHC). MoH incorporated RBF in the Health sector Development Plan (HSDP) as a major
financing strategy for the health sector and a tool to achieve UHC. This obviously has positive
implications for the RBF agenda. During this workshop, a top level MoH official emphasised
that RBF is a precursor for strategic purchasing which is mandatory under National health
insurance which is being considered as one of the initiatives towards UHC in Uganda.
6.2.1.1.3 Importation of evidence and policy transfer.
The respondents reported that evidence from other settings where RBF has been implemented
has been key in pushing the RBF agenda in Uganda. Reference was made to other countries as
justification for Uganda to adopt RBF. Rwanda was cited as one of the RBF success stories.
Now and again it was used to benchmark that Uganda needs RBF to improve its health sectors
performance. This was well capture below:
“IknowRwandahasdoneverywell[withRBF].Iwouldsayit’saveryimportanttool
as far as health reform is concerned. If you plan and implement it well, RBF is one of
the good approaches that could help improve the health sector. Asyou’reaware,the
MoH has tried so many tools to improve the quality of health services but many of
them are not working and of late people think that RBF can make a difference”
Project manager
“What you are seeing at international level in countries like Rwanda, Zimbabwe is
that RBF can have real effects on health systems performance. That alone is the
evidence [that RBF can work for Uganda]” Development partner
Review of documents, indicated that the RHV project was informed by lessons from other
projects that vouchers/contracting would lead to more efficiency in the health sector
compared to the input-based financing: “Contracting/voucher schemes in other countries have
shown a potential to increase efficiency over typical input-based public health care systems,

47
thus reaching a greater number of people with a given amount of public expenditure” the
project manual reads (WB 2007;3)
Lastly, respondents reported that training materials were developed (based on international
experiences and used to inform RBF initiative in Uganda. Reportedly, Cordaid developed a
curriculum on RBF that draws from its global experiences. These experiences informed the
design and implementation issues related to their RBF project in eastern Uganda.
6.2.1.2 Internal factors and their influence on RBF agenda in Uganda
Several factors in Uganda were noted to have influenced the development of RBF in Uganda.
These included: the focus on results by government, leadership/governance issues, health
systems/sectoral issues, Corruption scandals. Of these, government focus on results and
corruption scandals have been facilitators of interest in RBF in Uganda. Conversely, national
leadership/governance issues as well as sectoral issues have been hindrances to scale-up of
RBF.
6.2.1.2.1 Focus on results and lack of progress with current mechanisms
Frustration within government over the lack of progress in attaining national and global health
targets was reportedly a very important force for the recent push for RBF in the country. The
government is concerned about the poor quality of health services provided and the constant
complaints about health workers in public facilities. This has moved government to ponder
the possibility of using RBF to address these deficiencies.
“[RBF is being advanced] because government is tired of poor results” Policy Maker,
Non-MoH
“RBF [scheme] was introduced to support existing approaches such as integrated
supervision at district level” project manager.
6.2.1.2.2 Corruption scandals
Some respondents reported that the rampant cases of corruption in the country have been key
in galvanising the recent efforts to move from input based financing towards results-based
financing in Uganda. The following quotes captured these concerns:
“Corruption…corruption! Everyone is tired. We need to hold people accountable. In
fact,weshouldmovebeyondfinancialaccountability” Development partner
“It [RBF] also checks on corruption a lot. That’swhypeopleareembracingRBF a lot
……itencouragestransparencyalot.Sopeoplearejustwilling,thatifthisthingisthe
one now to transform us, they would rather go in for PBF” Field staff.
6.2.1.2.3 Configuration of Health Systems and Public sector as barriers to national RBF
scale-up.
Certain health systems factors that have shaped RBF development in the health sectors were
reported. Most of the RBF pilots have been implemented in the PNFP subsector. Two major
reasons were suggested for this ‘PNFP bias’. First was the need to support PNFP sector and
secondly, the difficulties of working within the public sector. These factors are elaborated
below.

48
6.2.1.2.3.1 Why RBF has concentrated in PNFP sector?
Many respondents emphasised that there has always been a need to support the PNFP
subsector in the country. The PNFP sector is usually needs external support to obtain
resources required to deliver of health services. One respondent pointed out one example;
“There was a need to support PNFP because government was paying better salaries
that led to traffic of health workers from PNFP to government” Field staff
The study found that the current government’s partnership in the private sector has been key
in advancing support for the PNFP sector. Reportedly, the World Bank PBC study was
possible because of the existing strong public private partnership in health in Uganda that
provided opportunities for resources to flow from government to the private sector in
exchange for provision of health services (WB/CIDA/MoH 2005, Morgan 2011). The end of
project report (WB/CIDA/MoH 2005: 22), emphasised the need for contractual arrangements
to ensure that government subsidies stimulated the desired results from the PNFP sector:
Giving grants without defining the expected outputs is not likely to promote efficiency,
equity, and effectiveness in health care delivery. It is a high time government and
private sector, especially PNFP, went into a contractual arrangement, defining the
volumes of services and expected outputs (performance-based) to match the funds
provided by the government, especially with emphasis to reaching the very poor and
other vulnerable groups.
As one key informant reported, the Cordaid Pilot was also started because the PNFP sector
wanted to demonstrate to government that their (government-PNFP) relationship could be
formalised through performance-based contracts which would explicitly specify each other’s
expectations.
[We advocated for PBF] because we wanted to demonstrate to government that the
funds they give us can be directly linked to performance” (Policy Maker, Private
sector).
6.2.1.2.3.2 Why public sector reforms supportive of RBF have been slow?
Most respondents highlighted several aspects of the public health systems that make it hard to
integrate the current RBF models as justification for working through the private sector. This
problem is well captured by Okal et al 2013; 3 in their assessment of opportunities and
challenges for public sector involvement in the maternal health voucher program in Uganda.
They observed that:
Public facilities were initially not contracted due to concerns that funds disbursements
and management would be pooled at the district level and that public facility
administrators lacked sufficient autonomy to effectively use the OBA reimbursements.
Some district and national level officials also viewed introducing the voucher program
in public health facilities, with vouchers nominally sold to poor clients, as in conflict
with the government policy of providing services at no cost.
Some respondents also took note of the above issue:
“But thepolicywehavecurrently is that inpublic facilities, thehealth servicesare
largely free apart from the private wings. So now as much as they (government)
appreciate the benefits of PBF, the (free health care) policy doesn’t fulfill the
requirements of theResults based financingwhere the user also has to contribute”
(DHO).
49
“Major public sector reforms to support RBF have not implemented” Development
Partner.
“The rules in the public sector do not allow autonomy to facilities” Academic.
On further probing, the slow reforms in public sector were attributed to several leadership and
governance issues. These were noted to influence RBF development but mostly in a negative
way as elaborated below:
First and foremost, RBF reforms introduce changes in institutional arrangements, property
rights and incentives of the actors in the health system (Bertone & Meessen 2012). This
reality seems to be a major determinant of buy-in for RBF in Uganda. The respondents noted
that the fear of loss of control over resource allocation processes in the sector among some
role bearers has been a stumbling block to RBF. Several quotes reflect those concerns:
“Most of our people might not be willing to change. The health system is structured is
in such a way that we have power centres at various levels yet the moment you
introduce this PBF, the health facilities are meant to be autonomous- to take decisions
on what priorities they want to fund, to hire staff, to fire if need be” DHO
“There is fear to venture into the unknown” Policy maker, MOH
“Top leaders controlling input based financing will not support RBF. People fear
being rendered irrelevant” Academic
Some respondents noted that the current resource allocation formula for the Primary health
care (PHC) grants to health facilities and districts favours certain units/districts was a reason
to resist change from current financing modalities. Reportedly PHC grant allocation formula
does not take into account the performance but just level of facility. As one respondent argued
those currently benefiting from modus operandi resist change to RBF:
The allocation formula for PHC funds is based on [health facility] level, butitdoesn’t
necessarily translate that the health centre 1V generates more and better outputs than
health centre III. So, some of the people who have benefited from that system of
allocating resources are reluctant to let go of RBF” DHO.
Furthermore, inadequate stewardship capacity to steer RBF within the health sector was
reported. Some key informants made reference to preference among some top MoH officials
to follow political directives to drive sector actions without regard to the strategic plans. This
has led to slow buy-in into the RBF agenda. One policy maker reported:
“The top (health ministry) management only want to listen to the president who makes
decisions without being guided by strategy of the sector. For example he orders;
‘Build a hospital here and a clinic there’; ‘Increase the pay of doctors at Health
centreIVmorethanothers’.Howdoyoupayonepersoninateam?” Policy Maker,
MoH.
Another fundamental barrier to scale-up of RBF pointed out was the very nature of the public
sector in Uganda where sectors plan and work in silos. Respondents observed that because of
this modus operandi; little engagement had gone on between Ministry of Health (health
sector) and other relevant key sectors such as local government, public service and Finance to
work out the necessary reforms. One policy maker at MoH emphasised that “Government
systems are disjointed to support RBF”. This was noted to be very big barrier because the

50
health sector relies on other sectors such as education, water & sanitation and labour to
address the social determinants of health.
Key informants noted that RBF had not taken root in the government planning and budgeting
system to facilitate its adoption in public sector which is a pre-requisite for national scale-up.
RBF is a financing reform that requires Ministry of Finance to be at centre stage. The Output
Budgeting tool currently used by Ministry of Finance (and within government) is an important
precursor for a result-based financial system. However, respondents observed that OBT is
sub-optimal. Public financing for health per capita was also reportedly low and does not meet
the minimum requirement needed under RBF. Some respondents argued that RBF would
require an increase in investments into the health sector which may not fit into the fiscal
space. The need for more investments by government was reportedly a disincentive for the
state to adopt RBF:
“There is the required minimum investment in terms of money per capita [under RBF].
ForinstanceaboutthreedollarsisrequiredtosupportthePBF.OurgovernmentI’m
sure is reluctant because our [government] funding per capita for health services is
not yet near the three dollars. So they are reluctant to quickly take it on”. DHO
Some respondents noted that the mandatory need for new reporting and accountability
obligations to the funder by the beneficiary creates a general hesitancy to adopt new
accountability systems associated with RBF reforms:
“PBF demands accountability at all levels-Some people are not willing to be
accountable to the donor”. DHO
6.2.2 Sharing and Utilisation of RBF evidence as determinant of buy-in and scale-up.
6.2.2.1 Inadequate information sharing as barrier to scale-up
Despite various stakeholder holder efforts such as undertaking national and international
study visits and organising national workshops, some respondents felt that buy-in into RBF
was still low at the national level.
“We undertook learning visits to Rwanda to share knowledge about RBF although
Ugandadoesn'tseeminterestedatleastatpolicylevel” Development partner.
“Have held [national consultation] workshops and I think people understand RBF
better but it is hard to change the mindset. However I believe that after 5 years it will
be embraced” Development partner.
On further probing, slow progress of RBF was partly attributed to inadequate engagement of
key stakeholder such as relevant ministries (health & Finance) and the politicians at the
national level. The following quotes succinctly capture this problem:
“Those with power have no information; those with information have no power”
Academic.
“Thosewhohave themoney, the politicians have not understood it…and that iswhy
they are dragging the scaling up process” Project Manager.
“Politicians have understood nothing generally… But they generally support where
they see personal gains .The politicians who work in the districts where the schemes are
know the benefits”.Project manager.

51
One respondent noted that knowledge sharing has concentrated among researchers pointing to
ineffective translation of knowledge on RBF:
“Cross fertilization of knowledge [on RBF] is only a domain of research institutions
like School of Public health... Sharing knowledge about PBF has not been very
optimal” Policy maker, MoH
Recently, efforts have been made to bridge the knowledge gap. However, as one respondent
who had participated in the workshops observed, few people from MoH participated in these
national engagements.
“[RBFhasmoved] to a small extent citing the two consultative meetings that we held
but policy makers were not there as there were few people from the Ministry of
Health” Project manager.
6.2.2.2 Inconclusive Evidence on RBF as barrier to buy-in
One further probing, we found that the inconclusive evidence on RBF impacts has to some
extent been a major barrier to buy –in to RBF. The study found that the inconclusive results
from the first RBF study influenced people’s perception towards RBF negatively. One key
informant noted that
“The study did not reach conclusion and so did not generate evidence that RBF works. The
failure of first pilot biased certain people against RBF” Project Manager.
The next sub section explores how various views about RBF have influence buy-in.First is the
belief that RBF is not a panacea and secondly, there expression by policy makers that more
information on implementation is needed before scale-up. These aspects are expounded on
below.
6.2.2.2.1 Understanding that RBF is not a Panacea
First and foremost, some respondents attributed slow buy in into RBF to skepticism that RBF
may not be all that Uganda’s health sector needs to improve its performance. The respondents
emphasised other structural challenges in the sectors that need to be worked on to ensure that
the system is functional enough to start demanding results from health facilities. The
following quotes reflect these aspects.
“Thereisan understanding that RBF is not a magic bullet to all the problems in our
system” Academic
“RBF is seen as a solutionwithout fully understanding the problem” Development
partner.
Consensus on how to achieve results seemed inadequate in government. One key informant
observed that the Ministry of Finance holds a different view on how results should be
achieved; and this is not through RBF:
“TheMinistryofFinance is interested in increasing value for money and increasing
effectiveness and from their point of view, the kind of guidelines and the planning tools
they put in place are gearing towards that. So they do not understand when you try to
push for the shift to RBF because they think that their approach is the way that should
be giving them the results. But unfortunately, when you evaluate the success of their
approach, it almost endsupbeingbusinessasusual”Development Partner

52
The “RBF is not panacea” perspective was further emphasised during the 2nd
national
consultation workshop on RBF. For example, evidence presented from Burundi reported that
there was no differential effect of PBF on addressing equity across socio-economic groups.
Presenters from Uganda also reported experiencing perverse effects and risks of PBF such as
including neglect of non-purchased services that are beneficial, reduced quality, irregular
payments and falsification and manipulation of health information data. Considering the
results of PBF in Uganda and abroad, the workshop participants concluded that PBF as an
innovative fund allocation mechanism can accelerate progress and address some of Uganda’s
problems in the health sector through the strategic purchasing of health services. However,
they emphasised that PBF is not a magic bullet that could solve all problems within the
system.
Related to the above, the participants at the two national consultation workshops on RBF
pointed out several preconditions for RBF to be rolled out nationally. For example, during the
2nd
national consultation workshop on RBF, the delegates emphasised that RBF is a health
system strengthening tool that needs to be carefully combined with other financing
mechanisms (input-based financing, user fees, and insurance schemes) and that requires some
preconditions in place at different levels in order to be successful. As participant observers at
this workshop, we captured the following concerns:
All health facilities need to have a certain minimum level of operational capacity
before being taken up in a RBF scheme. RBF cannot solve structural problems, but is
only able to capitalize on existing productive facilities to improve service delivery
capacity with a more efficient utilization of the available assets. In other words,
productive assets at health facility level need to be in place before introducing RBF.
(BTC/MOH 2015).
Furthermore, one participant from the development partners’ community highlighted a very
significant financial gap at almost every health facility level in Uganda. He asserted that this
gap undermined significantly the funding of basic operational costs and that RBF would not
be able to cover this gap. Hence RBF might fail to improve service delivery and performance.
Accordingly, the workshop participants agreed that there is need to address the extent and
nature of Uganda’s financial gap in the health sector and for the GoU to come up with a
strategy to uplift the facilities with bottlenecks and supports them in reaching a minimum
required level of functionality. In summary, it was agreed that is only a concerted action of
many different funding sources aligned to GoU efforts that can ensure the scale up of RBF to
national coverage ( BTC/MoH 2015, Participant observation).
6.2.2.2.2 Knowledge gaps as barrier to buy-in:
Some study participants noted that some gaps in knowledge regarding RBF implementation
have undermined opportunities for national RBF is scaled-up. Reportedly, the isolated nature
of the schemes so far implemented created reservations on roll out of national program. One
development partner noted that “some schemes have been implemented as vertical stand-
aloneprojectsandnotintegrated[intoexistingSystems]”.He argued that “Patchypilotsall
over the country make it difficult to scale up.”
Some respondents highlighted concerns about sustainability of RBF. All RBF pilots depended
on donor support. This factor undermined transparent sharing of information on the costs of
implementing RBF at national level. Some respondents were concerned that RBF schemes are
very expensive to implement yet little information is being shared on the cost of

53
implementation. Indeed, we found only one publication on the costs of implementing a
voucher scheme ( Mayora et al 2014). Policy makers expressed keen ness to know the costs of
national roll-out yet little is forthcoming from the schemes:
“Scale up may be hard because it is costly and the funding may be limited”
Development Partner.
“Dependency on donor funding to reward output, when delayed or no funding is
provided affects the scale up of the scheme” Development Partner
“Morelightneeds to be put on resources required for implementation” DHO
“Not enough is sharedonhowmuchRBFcosts…yet it is hard todemonstrateRBF
effectiveness. ExpensivedesignsofRBFaren’tsustainableoncethefunderspullout”
Academic.
6.3 Prospects and recommendations for national RBF scale-up
The following section present results on the prospects and recommendations for scale-up of
RBF as national policy.
6.3.1 Prospects for RBF to become national policy
Most respondents felt that the prospects of RBF becoming a national strategy were good.
However, they were quick to point out that more need to be done and current efforts
sustained;
“[Prospectsare]goodandIwouldrecommenditbecauseof thebenefitsofRBFof
improved quality and value for money” Policy maker, MoH
“Prospects are high if continuous discussions are held” Field staff
“Thereishope…MOHisonboardbuttheyneedtounderstand before pushing for it”
Project manager.
Observation of events between January and May 2015 indicated that the prospects of RBF
becoming national strategy in Uganda are generally now better than ever before considering
some important events over this time. Key events include:
The 2nd
national consultation workshop on RBF organized between 16-17th
February
2015. During the workshop BTC outlined a long term vision- of progressively
building up a universal public health insurance scheme that starts with RBF schemes
at limited scale and evolve towards a basket fund to finance the insurance. The plan is
gradual nation-wide extension of the RBF system in the mid-term, to lead in the long
run to a national trust fund that finances a nationally managed contracting and
insurance system. In such a system there will be a real purchaser-provider split with
the GoU responsible for regulating and providing stewardship, and the national trust
responsible for managing the resources. Noteworthy, although BTC plans to start with
PNFP facilities, it will progress to the Public sector in the second year of the project.
Another important development during the RBF workshop was the commitment form
MoH that the time of piloting RBF in Uganda’s health sector had come to an end and
that with the support of BTC’s PNFP Project, a national RBF model would be

54
designed. In fact, MoH promised to set up a coordination unit in the MoH to execute
this task. A Technical working team was set up in May 2015.
RBF has recently been well articulated as a financing strategy in the new Health
Sector Development Plan (HSDP 2014/15-2019/20) and the health financing strategy
(2015/16-2014/25).
Despite the above developments, some respondents were skeptical of RBF taking root
nationally considering the barriers highlighted already. One key informant remarked:
“Itwon’tbeeasy…MinistryofFinanceisnotinthedrivingseatyetithasthepowerto
drive the reform” Development Partner.
6.3.2 Recommendation for RBF to become a national strategy:
When asked what they thought should be done for RBF to work in Uganda. The study
respondents highlighted several issues that need to be considered. These range from
preconditions (such as other supportive public sector reforms, health systems strengthening),
design issues and other implementation considerations. Several suggestions were presented as
elaborated below:
6.3.2.1 Preconditions for RBF Success
1) Health systems strengthening
Most respondents emphasised that health systems strengthening should be done
simultaneously to ensure that RBF reforms achieve the intended objectives. Specifically, it
was recommended that there is need to harness benefits of decentralization by involving local
governments throughout the processes. Human resource strategies such as recruiting more
health workers, revising job contracts to permit contracting of health workers and changing
mindsets of health workers. Furthermore, it was evident that other health systems building
blocks should be considered. Examples suggested included increasing government funding for
health, government needs to upscale / help improve facilities to get facilities functional,
accreditation of facilities and stakeholder engagement.
2) Capacity Building
Building the capacity of the implementing individuals and entities was an important
component suggested for successful implementation of RBF. Particularly, the respondents
suggested:
- Empowerment of the local government to be able to do the monitoring.
- Training local government to RBF concepts.
- Conducting good assessment of the capacity of existing facilities to deliver services.
- Boosting the capacity of MOH to supervise and support the institutions.
3) Policy changes
Some policy changes within the public sector were proposed as prerequisites for RBF to work
in Uganda. However, it was noted that putting such reforms in place is likely to be a
challenging process. Some specific policy suggestions were captured as below:

55
“Autonomyoffacilitiesshouldbethoughtabout” Academic
“Contracts in public service should be revised such that civil servants sign contracts
thatshowdeliverables”Fieldstaff
“Theremustbeaprovisionoffiringofnon-performers” Policy maker, MoH
6.3.2.2 Design Issues
Several suggestions were provided on the design issues. These included general and specific
design issues. Under general design issues, the respondents suggested that:
- RBF rates should take into account difference in characteristics of the districts.
- Facilities should have to meet a certain minimum standard before being brought on
board.
The first among the specific design issues was how to tracking performance. Specific design
changes suggested pertained to tracking outcomes instead of outputs. It was noted that
tracking results may be challenging but never the less it is indispensable under RBF
arrangements. Some of the suggestions were as follows:
“Performance should move from output to outcome hence measure changes in
behaviorpracticesandsystemsnotvolumesofservices” Project manager
“Robustmeasurementsandinformationsystemsshouldbeestablished” Development
partner
Relatedly, respondents emphasized that for RBF to proceed in Uganda there must be
separation of roles. Obviously this would entail creating new structures to perform
fundholding, validation, and purchasing at national and subnational levels. This would also
necessitate breaking the monopoly of the National Medical Stores, the only permitted supplier
of medical supplies to the public sector. These aspects are captured below:
“Government needs to get out of service provision and focus more on purchasing”
Development partner
“Government should allow new service providers and public facilities to identify
other suppliers of drugs” DHO
“Financing should go somewhere else. DHO's office should remain purely on
supervisory roles” DHO
Relatedly, some respondents suggested having a semi-autonomous public body to manage and
oversee RBF initiatives in the country. One respondent recommended:
“Uganda should develop appropriate institutional arrangements and come up with
body that will becontrollingthefunds” Development partner
6.3.2.3 Implementation issues:
Several ideas were generated from the study regarding consideration for RBF implementation
in Uganda. This included revisiting criteria for allocation of resources. Other suggestions
included: Ensuring that RBF implementation follow phased approach such that lessons can be
incorporated into subsequent stages and that corruption at local government level must be
fixed. The beneficiaries organisations should need to have different accounts for RBF funds
so they can feel the need to work hard when there is no money coming in through RBF.

56
6.3.2.4 Summary of recommendations
We noted the recommendations from the second RBF workshop which we participated in as
participant observers. These were similar to those suggested by the key informant. Some of
the recommendations were as follows:
A learning and documentation process should be set up alongside the implementation of
RBF. Such a process would feed into the design and development of a national RBF
model and roadmap towards UHC, including testing and learning new ideas.
Policy level reform efforts in the health sector like NHI, RBF, and resource allocation
formula need to be harmonized. It is essential to link the current RBF dialogue with the
development of a Health Financing Strategy.
The implementation of RBF requires the formulation of a structured theory of change
based on sound assumptions. An operational manual on RBF should be developed to
clarify on the direction to take.
GoU should articulate a strategy to uplift public health facilities with operational
bottlenecks to reach a specific level of functionality in order to avoid being left out of the
RBF model.
Overall, the RBF reform architects were urged to stick to the good practices and principles of
RBF implementation.
“The problem we have is that there are many people masquerading to have RBFs and
that’swheretheproblemis.Thisisbecausepeopledon’tknow.Ideally, any good RBF
should be designed and well implemented within the principles consistent with RBF.
We should not name other things RBF when they are not. That causes confusion and
many people who are not very much conversant with RBF will be thinking that those
arealsoRBFswhentheyarenot”. Development partner
6.4 Conclusion
The various RBF schemes covered in this study represented the major efforts between
Government of Uganda, Donor and development agencies (e.g World Bank, DFID and
USAID), researchers and academic institutions and other agencies such as Non-Governmental
Organisations in the design, implementation and evaluation of these initiatives. They hence
provided a vantage point to explore how various the factors and actors facilitated or hindered
buy-in and integration of RBF into national health system and policy. Donor influence,
growing global movement towards RBF, transfer of Knowledge from other countries and
changing aid architecture were suggested as external forces pushing RBF in Uganda.
Frustration with corruption and inefficiencies in exiting input-based financing were reported
as factors advancing RBF in the country. However, several issues within the public sector
were noted as barriers for scale-up. These included disjointed government systems, weak
stewardship of the sector and inadequate engagement of the key constituencies for RBF.
Similarly, knowledge was considered both as product of and factor for RBF scale-up. It has
been argued that knowledge on RBF has not been sufficient to convince some key policy

57
makers that RBF is the way to go. This pointed to need for generation of robust evidence that
should be well disseminated to foster buy-in across government entities.
Several recommendations were made in respect precondition for RBF to work in Uganda.
These included health system strengthening initiatives, undertaking complementary public
sector reforms such a financing and human resource systems and ensuring a phased
implementation approach that would take into account learning during implementation.

58
CHAPTER 7 : DISCUSSION
7.1 Introduction
While scaling up of effective health interventions or strategies is considered essential to
benefit more people, there is limited documented evidence on how to foster such scaling up
process, particularly on RBF. This seems to be the case in Uganda where a number of RBF
initiatives have been implemented as standalone projects with little integration of RBF into
the national health system [4,5, 6,7,8]
Scaling up is noted to be a complex and multi-dimensional and often planned/guided process,
as defined by Hartmann and Linn [22],“scaling up means expanding, adapting and sustaining
successful policies, programs or projects in different places and over time to reach a greater
number of people”. Accordingly, scaling up is a guided process which not only increases the
coverage of an innovation, but also adapts and integrates it into the national
institution/system, and thus, enhances its sustainability.
In brief, this study aimed at documenting and analysing the development process of RBF in
Uganda from Jan/2003 to March/2015 and it draw lessons for future scale up and
sustainability of initiatives. It has covered a total of 7 diverse RBF initiatives that have been
implemented in Uganda since 2003. This section discusses the results and draws out
implication for policy in Uganda and other similar countries.
7.2 RBF Aspects that have moved/not moved and why?
The respondents pointed out certain RBF aspects that they considered to have moved at
national level. For instance, knowledge about benefits of RBF had progressed. As such, they
reported that RBF schemes led to improved staff motivation, health systems responsiveness,
better health seeking behaviors and health outcomes ultimately. However, perverse effects
arising from incoherence of incentives were also reported and that these could be detrimental
to performance. It was noted that implementation experience has improved. This
improvement in knowledge could be explained by the fact that many of the respondents have
been involved in RBF in one way or another. Conversely, knowledge about other RBF
schemes was notably still low and knowledge about design and implementation
considerations was concentrated among those who have been implementing the schemes and
the scholars of RBF. This points to either inadequate or ineffective information sharing
efforts. Therefore, more active stakeholder engagements should be developed. One
opportunity to be considered is to bring them together under one roof. Moreover, the low
cross learning among the schemes was blamed on the lack of such experience sharing
platforms. The establishment on RBF technical unit in the MoH would go a long way in
consolidating the lessons and coordinating RBF efforts.
Several reasons for low buy in were suggested. These included high costs, having patchy pilot
with diffuse effect and dependence on donor funds who earmark their resources to certain
ventures. On the other hand, some respondents hinted that Uganda doesn’t need to pilot RBF
anymore. Accordingly, they urged BTC/MOH to come up with a national model outright.
However, this means coming up with a scalable model. This is very important considering
that negative experiences with first schemes were noted to have biased people against RBF.
Never the less, as one respondent argued, developing a model that satisfies every stakeholder
may not be feasible in reality. In that case, any RBF initiative henceforth should adopt a clear
and transparent learning agenda where evidence feeds back into decision-making processes.

59
Health system and sector issues were also notable barriers to RBF advancement. The evidence
that RBF can work in the public sector is little as a result low involvement of public facilities
yet these contribute almost half of health services in the country (MOH). On a positive note,
some efforts to extend RBF to the public sector have been noted to be successful. As a result,
they should be supported and lessons on good practices learnt. On a broader scale, this implies
investing in health system strengthening as was emphasised by all respondents. RBF requires
that all health facilities have a basic level of functionality. Accreditation may be used to
screen facilities that meet the standards. However, the good practices that were documented
across some schemes must be encouraged. For example, NuHealth provided seed grants to
facilities while the safe deliveries project introduced a grant for health systems strengthening
after the pilot. Therefore, if MOH or government is to adopt RBF, she must develop strategy
to uplift health facilities such that they reach a level of functionality. Otherwise, it will be
unfair and counterproductive to punish a facility or indeed the beneficiaries for upstream
factors beyond their control.
One important barrier for accepting RBF in Uganda was the concern that RBF is very costly
and unsustainable in the long run. This concern has not been eliminated owing to the dearth of
information on the actual cost of the RBF projects. Indeed, we found only one publication on
the costs of implementing a voucher scheme (Mayora et al 2014). It was noted that there has
been little sharing on the actual costs of RBF implementation to enable policy makers to
estimate the financial gap for Uganda’s health sector. Moreover, costing of the service
package is greatly needed for further reference especially during negotiations with the
Ministry of Finance. This is rather paradoxical considering that even the implementers who
have made considerable efforts to disseminate the findings that RBF works wonders have not
been forthcoming on this. Could this be due to the fact that RBF is very costly or just the
shortcomings of the reporting mechanisms in these arrangements? Whatever the case, the
slow buy-in underscores the urgent need for transparency among the implementing agencies
to share with the stakeholder their implementation costs. This would help inform the design of
the most viable model for the Ugandan market
7.3 Progression of Implementation experience
It was noted that both demand side and supply side initiatives have been implemented in the
country across different localities and during various periods. Evidence provided emphasised
a need to think about both sided during the design of RBF arrangements. For example, the
evidence from the Safe deliveries project indicated that introducing transport and service
vouchers led to a drastic increase in service utilization. This stretched and overwhelmed
system to the detriment of quality. They had to introduce a health systems strengthening
component. Similarly, evidence from Cordaid indicated that where the functionality of health
facilities improved, an influx of clients was experienced stretching the facilities further. This
implies that any national RBF arrangement should consider the unintended effects of RBF on
health systems capacity and plan for both demand-side and supply-side components.
Related to capacity building, it was noted that many schemes have relied on external business-
oriented agencies to perform the management or verification functions. However, it was noted
that some progress has been made in using local structures. NuHealth and Cordaid used the
District health teams (DHT) for verification. Another, notable example is the SDS program
that has expanded the composition of the DHT to include all heads of departments at districts
to foster harmonization of planning at district level. This is an important aspect since
production of health requires collective effort. This points to a need for RBF initiatives to
incentivize governance and leadership practices as a way to engender a results-oriented
culture at both upstream and downstream governance and implementation levels.

60
In light of the above capacity challenge, the observation that the current government “version
of RBF” in form of OBT has notable design and implementation gaps has far reaching
implications. These systems use output indicators and do not serve any purpose other than
guiding the budgeting process. This could be attributed to the fact that currently there are no
mechanisms to ensure feedback from OBT informs strategic decision making. This renders
these arrangements “academic” as was argued by one respondent. Furthermore, it alludes to
lack of adequate experience with RBF within government agencies. As such, capacity around
performance management needs to be strengthened in the public sector.
7.4 Contextual Factors shaping RBF evolution
It has been noted that RBF has recently been captured in health sector strategic documents
such as the HSDP 2015/16-2019/20 and the new HFS 2015/16-2024/25. Considering that the
development of these documents has been guided by evidence, stakeholder consultation and
analysis of available options, this implies that Uganda is progressively moving towards
implementing RBF. However, this calls for careful planning on how to operationalize the
different aspects recommended in the documents. Currently, the global development
community agenda is about achieving sustainable development goals and Universal Health
Coverage (UHC). This means that RBF has to be strategically debated as contributing to the
UHC agenda. There is knowledge that RBF is not panacea and that it has to work alongside
other mechanisms to achieve UHC. This calls for a careful process of integrating all strategies
that the country will adopt as its path toward UHC. This process should be iterative and
informed by evidence and learning as implementation progresses.
There have been many factors and actors that have influenced RBF scale up in Uganda. These
were both external and internal to the country and the health sector. First and foremost, donor
influence through conditional grants was a notable driver of RBF initiatives. This was coupled
with the general interest in the developed countries to demonstrate aid effectiveness as part of
accountability to the tax payers. More so, positive evidence from other countries where RBF
has been adopted nationally was used to urge Uganda to adopt RBF. Unsurprisingly, some
respondents suggested donors as the champions for RBF in Uganda although one policy
maker hinted that this is quickly changing. This implies that any future efforts to integrate
RBF in Uganda’s system should strategically engage the donor community since they provide
a good lot of money to the sector. BTC/MoH model provided a framework to think about
donor involvement- that is the progressive movement towards donor basket to fund health
initiatives geared towards achieving UHC. However, for this to materialize, concerted efforts
of the government in general and MoH would be warranted.
Relatedly, other external contextual factors that have shaped RBF development in Uganda
were reported. These included the global movement towards achievement of certain targets.
The Millennium development goals (MDGs) were noted to be a key factor that has shaped
RBF initiatives and the service packages therein. Understandably, this should not be
surprising considering that Uganda has been lagging to achieve all the MDGs except the one
on poverty (MoFPED 2013,iii). In fact, many of the schemes emphasised mainly Maternal
and child health services. This implies that RBF agenda in Uganda should be cognizant of
these global influences and work towards harnessing their benefits while mitigating their
negative impacts. On a practical note, the following issues are important. First, defining the
benefit package in Uganda will be challenge considering that the existing UNMHCP is
considered too big and vague. BTC/MoH model considers offering the UNMHCP in its
current form hence this will require careful scrutiny to avoid ambiguities during
implementation. Secondly, that the country has committed to the UHC agenda, RBF should

61
be discussed in light of this now domesticated global agenda to ensure alignment of RBF with
the strategic direction of the sector.
Back home, focus on results and displeasure within government about the slow the progress
with current financing mechanisms were suggested as facilitating factors for RBF
development. This implies that if harnessed well, this situation could be a fertile ground for
RBF advocates to push for reforms. However, several leadership/governance gaps were noted
as being barriers towards RBF. These include the uncertainty about what will happen to the
current role bearers if RBF is introduced. As such fear of loss of power was pointed out as a
cause for resistance to change. This calls for thorough stakeholder analysis and development
of strategies to engage the necessary stakeholders both within and outside MOH and to
manage the transition process. In fact, the lack of involvement of key stakeholders in MOH
and MoFPED were reported to have contributed to the sloth in adoption of RBF.
7.5 Future design considerations:
There has been slow involvement of public facilities in the RBF schemes. This is partly due to
the lack of the effective public sector machinery to support RBF reforms. Conversely, lack of
anational RBF model could have delayed emergence of the necessary reform. It was noted
that to adopt RBF, certain policies have to change. These included interalia autonomy of
health facilities, separation of roles and revision of terms of reference under public service to
move from permanent to performance-based contracts. Such massive reforms require a
carefully directed process. For example, autonomy of facilities implies empowering local
management and community structures. It also means that stewardship and capacity should be
strengthened to ensure that resources are optimally utilized. Guidance will be important
considering cases where bonuses to facilities ended up being counterproductive and became a
disincentive to good performance. It was highlighted during the consultation workshop that in
light of governance gaps in the sector, a total hands–off management strategy may not be
helpful. This implies strengthening the capacity at the center and progressively empowering
the local institutions.
It was noted that some RBF projects evolved as a way of sustaining the results achieved. For
instance, the Safe deliveries project evolved into two projects coded MANEST and
MANIFEST. The former aims at increasing access for the poor through targeted vouchers
while the latter to addresses sustainability through community mobilization efforts for saving.
On the other hand, components of the Reproductive Health Voucher under the World Bank
were incorporated into Saving Mother Giving life (SMGL) initiative. This has positive
implications as the implementing agencies have remained relatively stable in both sets of
initiatives. This implies that there is institutional memory and capacity at least in those
regions and agencies that have been involved. This is important because these can provide
technical capacity if Uganda is to scale up RBF. For example, some individuals can act as
trainers of trainers where they can share experience and build capacity of others. Therefore,
there should be a strategy on how the local capacity can be harnessed for RBF scale up.
Related to the above is the fact that sharing of evidence and information has been slow which
has undermined buy-in across key sectors and actors such as Ministry of Finance. It was noted
that although knowledge about certain aspects of RBF such as benefits and implementation
experience have grown over time, it was mainly concentrated within implementers and
scholars. This underscores a need for more efforts to engage other stakeholders who have not
been actively involved in RBF implementation so far. In fact, it was noted that some people
have not accepted RBF just out of sheer lack of interest. This further emphasizes the need for
active and continuous stakeholder involvement. Strategies such as establishing intersectoral

62
collaboration committees and conducting field visits were reported to improve people’s
perceptions and understanding of RBF. As such these approaches should be strengthened.
At further scrutiny, the indicators being used are mainly output-based. This is partly
understandable because using and measuring outcome health indicators is challenging under
RBF. However, the SDS has moved a step further and uses outcome indicators which offer
lessons while adopting performance indicators under any national level RBF. Noteworthy,
there are several factors that affect performance of health facility or districts. These may be
specific to local contextual factors such as the geographical landscape. This points to the
need to reflect on the indicators to adopt to ensure that they serve the purpose of enhancing
performance of the health systems.

63
CHAPTER 8 CHAPTER 8: CONCLUSIONS AND
RECOMMENDATIONS
8.1 CONCLUSION
This study contributed to bridging the evidence gap on scale up of RBF in developing
countries by examining how RBF in Uganda has been developed (scaled up) and investigating
the extent to which RBF initiatives were successfully scaled up and why? We explored
evolutionary journey of all RBF schemes that have been implemented in Uganda over the last
10 years. The schemes studied included supply side pilots and demand-side Voucher schemes.
Generally, Uganda has seen both supply side and demand side RBF schemes. The supply side
schemes covered included the World-bank Study (2003-2005), the Cordaid Pilot (2009-2015),
the NuHealth project (2011-2015), and the proposed BTC/MoH Pilot project (2015-2019).
Another program, the Strengthening Decentralisation for Sustainability (SDS) managed under
Ministry of Local government and provides performance-based grants to districts to deliver
social services including health was also described. On the hand, several demand-side
schemes (essentially vouchers) that have been implemented in Uganda were described. These
included the Reproductive Health Voucher Project by World Bank (2006-2011), the Safe
deliveries project (2009-2011) and follow on Maternal & New-born study and the Saving
Mothers Giving life (SMGL) initiative.
Convergence and observable trends along certain dimensions of scale-up have been noted
when we examined the scale-up of RBF along four dimensions namely population coverage,
service coverage, health systems integration and knowledge. The scale-up in population
coverage did not follow a systematic process and was contingent on the specifications and
interests of funding agencies, not national/sector plans. Almost all regions in the country have
had RBF schemes but the western region has had the most number of pilots. It is not clear
why the region was elected or whether the services implemented were the most needed. All
demand side schemes offered packages under maternal and related child health services.
Supply side pilots provided more general packages from the UNMHCP and targeted the entire
population within reach of the facilities. However, NCDS were notably unconsidered by all
the schemes. There is also little progress in implementing RBF in public facilities. Only three
schemes (SDP, Cordaid pilot and to some extent the SMGL initiative) have been implemented
in public facilities.
A mixed picture was found regarding health system integration and some areas have
progressed compared to others. Pertaining alignment with governance structures, RBF has
worked closely with Districts bypassing the national level. RBF is still incompatible with
some aspects of human resource systems in Public service. The current health financing
reforms are fragmented and there is still need to align RBF with other financing reforms such
as National Health insurance and Resource allocation formula. On the other hand, RBF has
resulted in improvements in HMIS by encouraging quality data management based on
computerised systems and regular complementary verification/validation exercises. Regarding
institutionalisation, there are recent pointers to formal institutionalisation processes within the
health sector such as setting up of Technical working team at MOH and explicit reference to
RBF in the HSDP and Health financing Strategy. In regard to practical institutionalisation, the
development partners contributed to institutionalisation of RBF. Similarly, non-medical
organisations such as NGOs and Academic institutions have found increasing opportunities to

64
work in the sector by supporting RBF related processes. However, depending on non-state
agencies has undermined institutionalisation of RBF within the government entities.
Concerning knowledge, appreciation of the benefits of RBF and important design and
implementation issues was noted among some categories of respondents. Knowledge is
mostly at service provider level and less at systems or policy levels. This reflects the
implementation space where RBF has integrated with the health system. Recent efforts to
bring stakeholders together were noted to improve awareness among key stakeholders.
Understanding linkages between different initiatives and how and why the different models
performed (or not performed) within the health system has yielded more robust evidence upon
which policies and practices for national scale-up, integration and sustainability of RBF
mechanisms can be based. The various RBF schemes covered in this study represented the
major efforts between Government of Uganda, Donor and development agencies (e.g World
Bank, DFID and USAID), researchers and academic institutions and other agencies such as
Non-Governmental Organisations in the design, implementation and evaluation of these
initiatives. They hence provided a vantage point to explore how various the factors and actors
facilitated or hindered buy-in and integration of RBF into national health system and policy.
Donor influence, growing global movement towards RBF, transfer of Knowledge from other
countries and changing aid architecture were suggested as external forces pushing RBF in
Uganda. Frustration with corruption and inefficiencies in exiting input-based financing were
reported as factors advancing RBF in the country. However, several issues within the public
sector were noted as barriers for scale-up. These included disjointed government systems,
weak stewardship of the sector and inadequate engagement of the key constituencies for RBF.
Similarly, knowledge was considered both as product of and factor for RBF scale-up. It has
been argued that knowledge on RBF has not been sufficient to convince some key policy
makers that RBF is the way to go. This pointed to need for generation of robust evidence that
should be well disseminated to foster buy-in across government entities.
Several recommendations were made in respect precondition for RBF to work in Uganda.
These included health system strengthening initiatives, undertaking complementary public
sector reforms such a financing and human resource systems and ensuring a phased
implementation approach that would take into account learning during implementation.
Despite the general conclusion that RBF in Uganda did not attain optimal integration into
national systems, these schemes should be viewed as actual opportunities that the country had
(and still has for the ongoing experience) to learn and move forward with the RBF agenda.
Thus, we have explored the reasons why these schemes were not brought to scale at national
level and the extent to which the pilots themselves were barriers or enablers for the progress
of the RBF idea in Uganda. We also identified major learning experiences by exploring the
changes that these schemes have elicited within the health system and among the participating
institutions and organizations) and the influence of these RBF initiatives have on national
health policy.
8.2 RECOMMENDATIONS
We subsequently underscore several issues that need attention of the policy makers to ensure
that RBF works in the Ugandan context.
The health sector in HSDP 2015/16-2019/20 has committed to achieving UHC. This
means that RBF has to be strategically debated as contributing the UHC agenda. The

65
MoH should develop an implementation plan that clearly articulates how RBF will be
integrated/ combined with all strategies that the country will adopt as its path toward
UHC.
Evidence/ information sharing efforts should be strengthened. The Ministry of Health and
her partners should create opportunities to share information on RBF. Approaches could
include a policy dialogue, consultation workshops and field visits where possible.
The MOH should set up an RBF technical unit in the MoH to coordinate RBF efforts and
synthesize evidence and lead stakeholder engagements. The unit should develop a national
model and ensure that any future initiatives conform to this standard. This task force wil
be responsible for engaging the donor community on priority indicators to purchase under
a common basket.
The BTC/MOH project under development should have a clear and transparent research
agenda to ensure that the lessons learnt feed back into the decision making processes.
Efforts to harness the accumulated local capacity should be strengthened. This may
include setting up an implementers’ forum or community of practice to ensure that the
expert community is continuously engaged.
If MOH or government is to adopt RBF, she must develop strategy to uplift health
facilities such that they reach level of functionality. However, this must be informed by
existing resource envelop.
One important barrier for accepting RBF in Uganda was the concern that RBF is very
costly and unsustainable in the long run. Costing of the benefit package should be done to
inform decision making.
The prerequisite policy changes have to address for RBF to take root in Uganda. These
included interalia autonomy of health facilities, separation of roles and revision of terms
of reference under public service to move from permanent to performance-based
contracts. Such massive reforms require a carefully directed process involving all relevant
ministries and agencies.
Any future RBF model should be implemented within existing decentralized governance
structures. RBF initiatives should incentivize governance and leadership at both upstream
and downstream levels.

66
CHAPTER 9 CLIST OF REFERENCES
1. Meessen B, Soucat A, Sekabaraga C: Performance-based financing: just a donor fad or a
catalyst towards comprehensive health-care reform?Bull World Health Organ 2011,
89:153-156.
2. Morgan, Lindsay and Rena Eichler. December 2011. Performance-Based Incentives in Sub-
Saharan Africa: Experiences, Challenges, Lessons. Bethesda, MD: Health Systems 20/20, Abt
Associates.
3. Robert Soeters, Peter Bob Peerenboom, Pacifique Mushagalusa,Célestin Kimanuka.(2011).
Performance-Based Financing Experiment Improved Health Care In The Democratic Republic
Of Congo. Health Affairs. vol. 30 no. 8 1518-1527. doi: 10.1377/hlthaff.2009.0019
4. Morgan, Lindsay 2010. Some Days Are Better Than Others: Lessons Learned from
Uganda’s First Results-Based Financing Pilot.
https://www.rbfhealth.org/system/files/RBF_FEATURE_Uganda.pdf
5. NU Health 2014. Frequently asked questions & answers. http://www.healthpartners-
int.co.uk/our_projects/documents/NUHealthFAQs.pdf
6. Ekirapa-Kiracho et al 2011: Increasing access to institutional deliveries using demand and
supply side incentives: early results from a quasi-experimental study. BMC International
Health and Human Rights 2011 11(Suppl 1):S11.
7. Okal et al. 2013. An assessment of opportunities and challenges for public sector
involvement in the maternal health voucher program in Uganda. Health Research Policy
and Systems 2013, 11:38 Page 2 of 11. http://www.health-policy
systems.com/content/11/1/38.
8. Kanya L, Obare F, Abuya T, Okal J, Njuki R, Warren C, Askew I, Bellows B: Safe
Motherhood Voucher Coverage in Western Uganda: Addressing Finance Related Access
Barriers. Health Policy and Planning; 2013:1–8. doi:10.1093.
9. The 2011 Uganda Demographic and Health Survey (2011 UDHS). Uganda Bureau of
Statistics (UBOS) http://www.ubos.org/onlinefiles/uploads/ubos/UDHS/UDHS2011.pdf
10. The Second National Health Policy (NHPII) 2010.Ministry of Health, Kampala.
11. MoH 2012. Uganda Health System Assessment 2011. Kampala, Uganda and Bethesda, MD:
Health Systems 20/20 project, Abt Associates Inc. http://health.go.ug/docs/hsa.pdf
12. Ministry of Health (MOH) 2011. 2009/10 Health Financing Review. Ministry of Health
Uganda. http://www.who.int/providingforhealth/countries/ugandahealthfinreview.pdf.
13. Nabyonga Orem J, Mugisha F, Kirunga C, Macq J, Criel B. Abolition of user fees: the
Uganda paradox. Health Policy Plan. 2011 Nov;26 Suppl 2:ii41-51. doi:
10.1093/heapol/czr065. PubMed PMID: 22027918.
14. NU Health program 2013. Technical Brief 2 July 2013: Early Implementation Experiences in
NU Health.
http://www.healthpartnersint.co.uk/our_projects/documents/NUHealthY2Q3TechnicalBrief.pd
f
15. NU Health 2011.Program brief.
http://www.healthpartnersint.co.uk/our_projects/documents/NUHealthProgrammebrief.pdf
16. Ssengooba, F., McPake, B., & Palmer, N. (2012). Why performance-based
contracting failed in Uganda–An “open-box” evaluation of a complex health
system intervention. Social science & medicine, 75(2), 377-383.

67
17. Reproductive Health Vouchers Evaluation Team 2014. http://www.rhvouchers.org/ [ Accessed
on Monday Nov 10 2014 at 19:07hrs]
18. Fritsche G SR, Meessen B: Performance-Based Financing Toolkit. Washington, DC: The
World Bank; 2014.
19. David H. Peters, Nhan. T. Tran, Taghreed Adam. 2013. Implementation Research in
Health: a practical guide. Alliance for Health Policy and Systems Research, World Health
Organisation.
20. Buse K, Mays N, Walt G: Making Health Policy. London: Open University Press, London
School of Hygiene and Tropical Medicine; 2005.
21. Walt G, Gilson L: Reforming the health sector in developing countries: the central role of
policy analysis.Health Policy Plan 1994, 9:353-370.
22. Hartmann A LJ: Scaling up: a framework and lessons for development and effectiveness
from literature and practices. Washington DC: Wolfensohn Center for Development, The
Brookings Global Economy and Development; 2008.
23. Nine steps for developing a scaling up strategy. Geneva: WHO/ExpandNet; 2010.
24. Bertone MP, Meessen B: Studying the link between institutions and health system
performance: a framework and an illustration with the analysis of two performance-
based financing schemes in Burundi.Health Policy Plan 2013, 28:847-857.
25. Hardee KA, L.; Rottach, E.; Jolivet, R.; Kiesel, R.: The policy dimensions of scaling up
health initiatives. Washington, DC: Futures Group, Health Policy Project; 2012.
26. Walt G, Shiffman J, Schneider H, Murray SF, Brugha R, Gilson L: 'Doing' health policy
analysis: methodological and conceptual reflections and challenges.Health Policy Plan
2008, 23:308-317.
27. Ir P, Bigdeli M, Meessen B, Van Damme W: Translating knowledge into policy and action
to promote health equity: The Health Equity Fund policy process in Cambodia 2000-
2008.Health Policy 2010, 96:200-209.
28. Brugha R, Varvasovszky Z: Stakeholder analysis: a review.Health Policy Plan 2000,
15:239-246.
29. Varvasovszky Z, Brugha R: A stakeholder analysis.Health Policy Plan 2000, 15:338-345.
30. Gilson L, Raphaely N: The terrain of health policy analysis in low and middle income
countries: a review of published literature 1994-2007.Health Policy Plan 2008, 23:294-307.
31. Everybody's business: strengthening health systems to improve health outcomes.
WHO's framework for action Geneva: World Health Organization; 2007.
32. Spicer N, Bhattacharya D, Dimka R, Fanta F, Mangham-Jefferies L, Schellenberg J, Tamire-
Woldemariam A, Walt G, Wickremasinghe D: 'Scaling-up is a craft not a science':
Catalysing scale-up of health innovations in Ethiopia, India and Nigeria.Soc Sci Med
2014, 121C:30-38
68
CHAPTER 10 REVIEWED SOURCES (DOCUMENTS,WEBSITES
ETC).
1) Ekirapa-Kiracho et al 2011: Increasing access to institutional deliveries using demand and
supply side incentives: early results from a quasi-experimental study. BMC International
Health and Human Rights 2011 11(Suppl 1):S11.
2) Barnes A, Brown G, Harman S, Papamichail A, Banda P, Hayes R, Muliamba C (2014)
‘African participation and partnership in performance-based financing: A case study in
global health policy’, EQUINET Discussion Paper 102, EQUINET: Harare.
3) Morgan, Lindsay 2010. Some Days Are Better Than Others: Lessons Learned from
Uganda’s First Results-Based Financing Pilot.
https://www.rbfhealth.org/system/files/RBF_FEATURE_Uganda.pdf
4) NuHealth 2013. Technical Brief: Setting up a Results-Based Financing Scheme –
Experiences in NU Health.
5) NU Health 2014. Frequently asked questions & answers. http://www.healthpartners-
int.co.uk/our_projects/documents/NUHealthFAQs.pdf
6) Okal et al. 2013. An assessment of opportunities and challenges for public sector
involvement in the maternal health voucher program in Uganda. Health Research Policy
and Systems 2013, 11:38 Page 2 of 11. http://www.health-policy
systems.com/content/11/1/38.
7) Bellows, B and Hamilton, M. Vouchers for Health: Increasing Utilization of Facility-
Based STI and Safe Motherhood Services in Uganda. Health Systems 20/20. June 2010.
Available at: http://www.healthsystems2020.org/content/resource/detail/2576/
8) Bellows, B and Obare, F (2012). Population level impact of vouchers on access in
Uganda. Presentation of Impact Evaluation Findings Workshop. Kampala, Uganda.
9) Kanya L, Obare F, Abuya T, Okal J, Njuki R, Warren C, Askew I, Bellows B (2013). Safe
Motherhood Voucher Coverage in Western Uganda: Addressing Finance Related Access
Barriers. Health Policy and Planning; 2013:1–8. doi:10.1093.
10) Bellows, N, Bellows, B, and Warren, C. The Use of Vouchers for Reproductive Health
Services in Developing Countries: Systematic Review. Tropical Medicine and
International Health. Available at: http://onlinelibrary.wiley.com/doi/10.1111/j.1365-
3156.2010.02667.x/full
11) The 2011 Uganda Demographic and Health Survey (2011 UDHS). Uganda Bureau of
Statistics (UBOS) http://www.ubos.org/onlinefiles/uploads/ubos/UDHS/UDHS2011.pdf

69
12) Ministry of Health (2010). The Second National Health Policy (NHPII) 2010. Kampala.
13) MoH 2012. Uganda Health System Assessment 2011. Kampala, Uganda and Bethesda,
MD: Health Systems 20/20 project, Abt Associates Inc. http://health.go.ug/docs/hsa.pdf
14) Ministry of Health (MOH) 2011. 2009/10 Health Financing Review. Ministry of Health
Uganda. http://www.who.int/providingforhealth/countries/ugandahealthfinreview.pdf .
15) Okwero P,Villegas L, Monay C, Johannes L (2012). Providing Safe Delivery Services
With Vouchers: The Reproductive Healthcare Voucher Project (RHVP) in Western and
Southern Uganda. Smart Lessons. IFC, World Bank.
16) NU Health program 2013. Technical Brief 2 July 2013: Early Implementation
Experiences in NU Health.
http://www.healthpartnersint.co.uk/our_projects/documents/NUHealthY2Q3TechnicalBri
ef.pdf
17) NU Health 2011.Program brief.
http://www.healthpartnersint.co.uk/our_projects/documents/NUHealthProgrammebrief.pdf
18) Ssengooba, F., McPake, B., & Palmer, N. (2012). Why performance-based contracting
failed in Uganda–An “open-box” evaluation of a complex health system intervention.
Social science & medicine, 75(2), 377-383.
19) Reproductive Health Vouchers Evaluation Team 2014. http://www.rhvouchers.org/ [
Accessed on Monday Nov 10 2014 at 19:07hrs]
20) World Bank/ CIDA 2006. Performance Based Contracting Study in Uganda. World
Bank/CIDA/MoH Project. End of Project Report - Policy Component
21) Lundberg M ( 2008). Client Satisfaction and the Perceived Quality of Primary Health
Care in Uganda. Chapter 14 in Are you being served? : New tools for measuring service
delivery edited by Samia Amin, Jishnu Das, Markus Goldstein. The World Bank.
22) Lars Johannes, Patrick Mullen, Peter Okwero and Miriam Schneidman ( 2008).
Performance-based contracting in health: The experience of three projects in Africa.
OBApproaches, Note Number 19
23) Monitor 2015.ADB gives Uganda Shs3 billion. http://www.monitor.co.ug/Business/ADB-
Uganda-finance/-/688322/2678528/-/69ts61z/-/index.html [accessed on 15th
September
2015 at 10:23 pm]
24) Africa Development Bank ( afDB) 2015. Uganda to hold Managing for Development
Results meeting. http://www.afdb.org/en/news-and-events/article/uganda-to-hold-
managing-for-development-results-meeting-14089/ [ accessed on 15th
September 2015 at
11:00pm]

70
25) UNDP in Uganda (2015). Government of Uganda launches new UNDAF and second 5-
year National Development Plan.
http://www.ug.undp.org/content/uganda/en/home/presscenter/articles/2015/06/11/govern
ment-of-uganda-jointly-launches-undaf-and-5-year-national-development-plan-.html [
Accessed on 15th
September 2015 at 11:36pm].
26) WHO/MOH 2014. Report of the National Consultative Workshop on Performance Based
Financing. 26th March 2014, Kabira Country Club
27) MoH 2015a. Health Sector Development Plan 2015/16-2019/20.
28) MoH 2015b, Draft Health financing strategy 2015/16-2024/24.
29) MOH 2013. Midterm Review Report of the Health Sector Strategic and Investment Plan
(HSSIP) 2010/11 - 2014/15 (VOLUME: 1). http://library.health.go.ug/publications/health-
workforce-human-resource-management/performance-management/midterm-review-
report
30) Mayora C, Ekirapa-Kiracho E, David D, Peters HD , Okui O & Baine SO (2014). Incremental cost of increasing access to maternal health care services: perspectives from a
demand and supply side intervention in Eastern Uganda. Cost Effectiveness and Resource
Allocation 2014, 12:14 http://www.resource-allocation.com/content/12/1/14
31) Namazzi et al (2013). Stakeholder analysis for a maternal and newborn health project in
Eastern Uganda. BMC Pregnancy and Childbirth, 13:58
http://www.biomedcentral.com/1471-2393/13/58
32) NuHealth 2013a. Technical Brief 2 July 2013: Early Implementation Experiences in NU
Health.
33) Department of International Development (DFID) (2014). Sharpening incentives to
perform: DFID’s Strategy for Payment by Results.
34) NuHealth 2013b. Acholi Regional Consultative Group (17th
and 18th
September, 2013).
Meeting Minutes: A summary of key points discussed and action points.
35) NuHealth 2013c. Lango Regional Consultative Group (19th
September, 2013). Meeting
Minutes: A summary of key points discussed and action points.
36) The World Bank (2014). Report No: 84295-UG. Project Appraisal Document on a
Proposed Grant From The Global Partnership On Output-Based Aid (GPOBA) in the
Amount Of Us$ 13.3 Million to the Republic Of Uganda for a Scale Up: Uganda
Reproductive Health Voucher Project (RHVP-II). Health Nutrition Population.
37) Namayanja C, Semujju R & Odong J ( 20XX). Assessing the need of integrating Family
Planning into the Reproductive Health Voucher project. MariesStopes Uganda Output-
Based Aid Project.

71
38) MarieStopes Uganda (201X). Improving access to quality maternal health services
through SHOPS project in Western Uganda – “From a garage to a maternity home”- a
health systems strengthening achievement.
39) Global Partnership on Output-based Aid (2007). Grant Agreement. Reproductive Health
Vouchers in Western Uganda Project.
40) Arur, Aneesa, Nelson Gitonga, Barbara O’Hanlon, Francis Kundu, Maggie Senkaali, and
Richard Ssemujju. November 2009. Insights from Innovations: Lessons from Designing
and Implementing Family Planning/Reproductive Health Voucher Programs in Kenya and
Uganda. Bethesda, MD: Private Sector Partnerships-One project, Abt Associates Inc.
41) Global Partnership on Output-based Aid (2012). Uganda Reproductive Health Voucher
Scheme. Lessons Learnt. Note Number 1.
42) Arben Fetai (2010). Outputs Based Aid as a Way to Provide Reproductive Health Access
to Vulnerable Populations. Seminar on Fertility and Poverty: Micro and Macro Linkages .
University of Southampton.
43) GPOBA (2007). Operations Manual: Reproductive Health Vouchers in Western Uganda.
44) Saving Mothers Giving Lives (SMGL) (2013).Making pregnancy & Childbirth Safer in
Uganda & Zambia. Annual Report 2013.
45) Saving Mothers Giving Lives (SMGL) (2014).Phase 2 Launch Report. August 2014.
46) SMGL (2015a): Saving mothers Giving Life project description.
http://savingmothersgivinglife.org/our-work/uganda.aspx [Accessed July 23rd 2015 at
4:45 pm)
47) SMGL 2015b. Reducing Maternal Mortality In Sub-Saharan Africa: Delivering Results.
Mid-Initiative Report. http://savingmothersgivinglife.org/docs/SMGL-mid-initiative-
report.pdf
48) Centers for Disease Control and Prevention (CDC) 2014. Saving Mothers, Giving Life
Phase 1 Monitoring and Evaluation Findings: Executive Summary. Atlanta, GA: Centers
for Disease Control and Prevention, US Department of Health and Human Services.
http://www.cdc.gov/reproductivehealth/global/publications/pdfs/saving-mothers-giving-
life-phase1.pdf
49) Bellows MN (2012). Vouchers for reproductive health care services in Kenya and
Uganda. Approaches supported by Financial Cooperation. Discussion Paper. KfW.

72
50) Boler T and Harris, L (2010). Reproductive Health Vouchers: from Promise to Practice”.
London: Marie Stopes International.
51) Morgan, Lindsay and Rena Eichler (2011). Performance-Based Incentives in Sub-Saharan
Africa: Experiences, Challenges, Lessons. Bethesda, MD: Health Systems 20/20, Abt
Associates.
52) Gorter AC, Ir P and Meessen B (2013). Evidence Review, Results-Based Financing of
Maternal and Newborn Health Care in Low- and Lower-middle-Income Countries,
February 2013, study commissioned and funded by the German Federal Ministry for
Economic Cooperation and Development (BMZ) through the sector project PROFILE at
GIZ – Deutsche Gesellschaft für Internationale Zusammenarbeit.
53) Witter S (2013). Pay for performance for strengthening delivery of sexual and
reproductive health services in low- and middle-income countries. Evidence synthesis
paper. The World Bank.
54) Pearson M, Johnson M and Ellison R (2010). Review of major Results Based Aid (RBA)
and Results Based Financing (RBF) schemes. Final report. UKaid.
55) Grainger C, Gorter A, Okal J and Bellows B ( 2014). Lessons from sexual and
reproductive health voucher program design and function: a comprehensive review.
International Journal for Equity in Health 2014, 13:33
http://www.equityhealthj.com/content/13/1/33
56) Ministry of Finance, Planning and Economic development (MoFPED) 2013. Drivers of
MDG Progress in Uganda and the Implications for the Post-2015 Development Agenda.
http://www.ug.undp.org/content/dam/uganda/docs/UNDPUg-
2013MDGProgress%20Report-Oct%202013.pdf

73
CHAPTER 11 ANNEX 1: LIST OF RESPONDENTS

74
CHAPTER 12 ANNEX 2: CONSENT FORM
Informed Consent Form for RBF study
Informed Consent Form for Key Informants who have been involved in Results based financing policy
process in Uganda and who we are inviting to participate in the RBF study, titled: Learning from
Multiple Results-Based Financing Schemes: An analysis of the policy process for Scale-up in
Uganda (2003-2015)
Name of Principle Investigator (PI): Prof. Freddie Ssengooba
Name of Organization: Makerere University School of Public Health (MakSPH)
Name of Sponsor: The Alliance for Health Policy and Systems Research (AHPSR)
Name of Project Support team: Institute of tropical medicine (ITM), Antwerp.
This Informed Consent Form has two parts:
• Information Sheet (to share information about the study with you)
• Certificate of Consent (for signatures if you choose to participate)
You will be given a copy of the full Informed Consent Form
Part I: Information Sheet
Introduction
I am__________, working with Makerere University School of Public Health. We are doing research as
part of a multicountry study looking at using financing strategy that links payments to services provided by
health facilities or consumed by service users as one way to improve the performance of health systems.
The purpose of this form is to provide you with information about this study and secondly to seek you
participation in the interview. The interview takes about 60 – 90 minutes.
Purpose of the research
Results-Based Financing (RBF) that links payments to services provided or consumed has been
increasingly used as a means to improve the performance of health systems. Whereas RBF has been
adopted in some countries as a national approach to financing the health sector, in some countries like
Uganda, RBF has not progressed beyond pilot projects. There is need to generate evidence to understand
why the slow progress. This study aims at documenting and analysing the development of RBF in Uganda
from Jan/2003 to March/2015 and draw lessons for decision making. We seek to understand the sequence
of events relating to RBF and to identify factors that have enabled or hampered the process of RBF scale-
up in Uganda over the study period.
Participant Selection
You are being invited to participate in this study because of your experience, knowledge and roles (direct
or indirect) in implementation of RBF in the past or in the future. We shall also ask you views about how
evidence from RBF schemes has shaped policy interest in RBF in Uganda.
Voluntary Participation
Your participation in this research is entirely voluntary. Your participation will have no bearing on your job
or on any work-related evaluations or reports. You are free to stop at any time during the interview or to
decline responding to some questions you do not wish to answer.
Procedures
During the interview, I ask questions from the prepared list and also some that may arise from your

75
responses. The information will be recorded on a digital recorder for accurate transcription later. If you do
not agree to being recorded, then written notes will be taken. Only the core research team members will
have access to the information recoded and transcribed. The tape and other materials will be reviewed to
make that anonymous before analysis. All research materials will be kept in a secure place under the
custodianship of the PI.
Risks The questions we seek to ask you are from your experience of RBF activities or about the prospect for RBF
in Uganda. We do not envisage any personal risk in the answers you provide. Your name and that of your
institution will not be used in any output of this research process. Furthermore to ensure confidentiality,
identifiers of professional position will be removed. All your responses will remain anonymous outside of
the core research team.
Benefits
There are no direct benefits for your participation but the information you provide will form a useful basis
for future RBF policy process in Uganda and add to available evidence in international literature. There are
no monetary incentive for taking part in this research.
Ethics Review and Approval
This proposal has been reviewed and approved by the Higher Degrees, Research and Ethics Committee
(HDREC) of Makerere University School of Public Health and the Uganda National Council for Science
and Technology (UNCST) which are committees whose task is to make sure that research participants are
protected from harm. This study has also been reviewed by the Ethics Review Committee of the World
Health Organization (WHO), which is supporting this and similar studies in other countries.
Who to Contact
If you have any questions, you can ask them now or later. If you wish to ask questions later, you may
contact the leader of the research team Dr. Freddie Ssengooba at Makerere University. He can be reached
at: Tel: +256772509316/ [email protected].
If you wish to find about more about the ethical conduct of research, please contact the HDREC
Chairperson Dr. Suzanne Kiwanuka on Tel No: +256701-888 163 or +256 312-291 397).
76
Part II: Certificate of Consent
I have been invited to participate in research Results based financing policy process in Uganda.
I have read the foregoing information, or it has been read to me. I have had the opportunity to ask
questions about it and any questions I have been asked have been answered to my satisfaction. I
consent voluntarily to be a participant in this study.
Print Name of Participant__________________
Signature of Participant ___________________
Date ___________________________
Day/month/year
Statement by the researcher/person taking consent
I have accurately read out the information sheet to the potential participant, and to the best
of my ability made sure that the participant understands that the following will be done:
1. An Interview will be conducted with the participant on understanding the process of
scale-up of results based financing in Uganda.
2. The interview will be recorded.
3. The views expressed in the interview will be confidential and will be used as specified
in the information sheet.
I confirm that the participant was given an opportunity to ask questions about the
study, and all the questions asked by the participant have been answered correctly and to
the best of my ability. I confirm that the individual has not been coerced into giving consent,
and the consent has been given freely and voluntarily.
A copy of this ICF has been provided to the participant.
Print Name of Researcher/person taking the consent________________________
Signature of Researcher /person taking the consent__________________________
Date ___________________________
Day/month/year

77
CHAPTER 13 ANNEX 3: GENERIC INTERVIEW GUIDE
Draft RBF Key informant Interview guide-Uganda
SECTION 1: Consent and Introduction
Note:
Start by introducing yourself and the purpose. If agreeable to interview, proceed to the
consent form
Request to record interview and make sure the tape recorder is switched on to the start
of the interview.
Ice breaker
1. What role(s) have you played in result based financing (“RBF” for short) in Uganda or
elsewhere?
2. For how long have you played this/these role(s)?
3. From your own understanding, what is Results based financing?
4. From your experience, what benefits do you see in using RBF in Uganda’s health
system?
SECTION 2: CONTEXT.
I want to start by asking how the external factors or how CONTEXT has influenced the
evolution of RBF in Uganda. This can be global context, national context outside the health
sector and within the health sector?
In your experience, what are the main external that factors have influenced the
evolution of RBF in Uganda?
Probe:
1. What contextual elements external to the country that may have had main influence on
the RBF policy
(Look out for Millennium Development Goals, the Universal Health Coverage
donor interest in RBF?)
Where did RBF come from?
What were the key policy makers preoccupied with?
For donors, where did RBF come from within your organisation?
2. At the national level outside the health sector, what could be the main sources of
influence supportive of RBF or against RBF?
3. Within the health sector, what are the contextual factors that may have influence on
RBF and how it has evolved?
o How did the RBF evolution interact with events in the health financing
calendar over the study period – e.g. development of HSSIP I, and II and
midterm review of these plans?

78
4. What policy could have helped RBF to become institutionalized following your
experience and who had the power to make it?
SECTION3: CONTENT
A. Regarding the RBF scheme you were part of:
1. What were the key milestones in RBF scheme evolution especially in terms of
concept, implementation, and dissemination of findings, other research uptake
activities?
2. What could be the causes of this evolution of RBF schemes?
Is it available scientific evidence (at national and international problem)?
Is it the possible need to simplify the policy to allow rapid scale up or buy-in
by a key stakeholder?
Is it the reform vision underlying the RBF program?
Was it because of the need to have a well-functioning policy, including by
finding the right fit with other policies and systems?
Was there a need to address a newly identified health problem?
3. In your opinion, what is the relevance that the changes brought to the content of the
policy? Were the changes (for instance adoption to obtain support from a stakeholder)
an improvement or not?
4. How do you think the RBF scheme design feature and institutional arrangements
influenced performance of RBF and eventual buy in from wider stakeholders?
Probe about: the objectives, target population or beneficiaries and methods to
identify them, benefit package, health service providers, contractual
arrangements, incentivized outputs/indicators with related price to be paid for,
management structure, including agency, commissioning/funding agencies,
monitoring and evaluation framework.
B. Use of evidence
5. How has understanding of RBF evolved over time and how has this influenced the
scale up process?
Probe:
How was the generated knowledge and evidence managed, shared and utilised?
How has the prevailing understanding of RBF influenced buy in or scale up of
RBF at national level?
6. To what extent do you think RBF has moved to national health policy?
Probe:
What aspects have moved or not moved and why?
What areas have moved forward?
Why do you think so?
Are you aware of other schemes that have been implemented?
What motivated them to start?

79
Has there been cross learning among the different schemes?
In your experience, what worked in terms of moving RBF to national policy?
What do you consider as opportunities missed/not seized?
SECTION 4: ACTORS
1. Regarding the role you played in the RBF scheme, how easy was it to relate with other
agencies/institutions or providers?
Probe:
What was easy and why?
What was difficult and why?
How did you adjust?
Did the changes bring any benefits?
To what extent did the capacity of others agencies influence your work?
2. Who were the key stakeholders related to the RBF scheme/policy? Who could be
considered the ‘RBF policy champion or entrepreneurs’ in Uganda?
3. How did the actors interact among themselves and how did they exercise their power
(financial, political, technical, symbolic and normative power) to influence the scaling
up related decisions/actions and the reasons behind such decisions.
4. Who was influential in moving nor not moving the RBF agenda forward? How and
why was this position taken?
5. To what extent do you think that such decisions/actions have been determined by the
information at their disposal, their own interests and constraints, including the overall
context?
6. What strategies were adopted to address the needs/interests of various stakeholders?
SECTION 5: CONCLUSION
1. In your observations, what are the prospects of RBF becoming a government policy in
Uganda? Probe by asking why? (For any key factor given).
2. Would you recommend RBF as financing strategy in Uganda? Why? Probe: How has
your perception about this changed overtime and why?
3. What aspects of RBF they would have loved to change if RBF was to become policy?
Thank you very much once again for taking part in this Interview

80
CHAPTER 14 ANNEX 4: CODING FRAMEWORK FOR
DOCUMENT REVIEW
RBF-Draft Coding Framework.
Only code with these two levels
Area Parent Node Child node Description of node
A.1: Pilot coverage
progression
a. Population coverage Time of events Timeline for change in population
coverage
Change communication How was change message
packaged
Justification for change What was reason for change
Content/ Target of change
and in which way.
Any particular population was
targeted? How?
Effects of change Outcomes of the population
coverage changes.
b. service coverage Time of events Timeline for change in service
coverage
Change communication How was change message
packaged?
Justification for change What was reason for change
Target of change and in
which way.
Any particular service coverage
was targeted? How?
Effects of change Outcomes of the service coverage
changes.
c. Geographical
coverage
Time of events Timeline for change in service
coverage
Change communication How was change message
packaged
Justification for change What was reason for change
Target of change and in
which way.
Any particular localities was
targeted? How?
Effects of change Outcomes of the geographical
coverage changes.
A.2: Pilot Institutional
arrangements
progression
a. Health service
providers
Time of events Timeline for change in health
service providers
Change communication How was change message
packaged?
Justification for change What was reason for change
Content/Target of change
and in which way.
Any particular health provision
arrangement changed? How?
Effects of change Outcomes of the changes in
health service providers.
b. Contractual
arrangements (other than
with health service
providers)
Time of events Timeline for change in
contractual arrangements.
Change communication How was change message
packaged?
Justification for change What was reason for change
Content/Target of change
and in which way.
Any particular contractual
arrangement changed? How?

81
Effects of change Outcomes of the changes in
contractual arrangements.
c. Monitoring and
Evaluation (M&E)
framework e.g
Incentivized
outputs/indicators
Time of events Timeline for change in M&E
framework.
Change communication How was change message
packaged?
Justification for change What was reason for change
Content/Target of change
and in which way.
Any elements of M&E (e.g
incentivised outputs/ indicators)
changed? How?
Effects of change Outcomes of the changes in M&E
framework.
d. Management structure
(including
funding/commission
agencies)
Time of events Timeline for change in
management structure.
Change communication How was change message
packaged?
Justification for change What was reason for change
Content/Target of change
and in which way.
Any particular elements of
management structure changed?
How?
Effects of change Outcomes of the changes in
management structure.
B.1.Institutionalisation
and RBF Policy
prospects.
a. Pilot to pilot cross
learning
Elements What aspects were cross learned
from one scheme to another?
Locality Was leaning from schemes within
country or other countries.
Reasons Reasons why the lessons were
picked
Challenges What challenges in implementing
lessons
Effects of cross learning Outcomes of cross learning on
design/implementation of
schemes
Best practices What are key lessons to take
forward from experiences
b. Health Systems
changes
What changes What changes has RBF induced
in health systems? Which health
systems function is affected?
Level What level are the changes e.g
district, national, community,
Public vs Private etc.
Mechanisms In what way are the health
systems changes induced?
c. Other public sector
changes
What changes What changes has RBF induced
in Public sector?
Level In what sectors are the changes
e.g Public service/public
financing systems?

82
Mechanisms In what way are the changes in
public sectors induced?
d. Policy prospects. Current impact What is impact on health policy
in Uganda so far?
Facilitators What are enabling factors for
RBF policy development
Barriers What are the barriers for buy-in
for RBF by policy makers?
Future prospects What are opportunities and
challenges for policy adoption?
Process of policy influence How are actors trying to influence
policy?
B.2 Practice
perspectives and
systems readiness
a.Capacity building Reasons for CB Why it was arranged/not
arranged?
Type of CB What type of personal and /or
group capacity-building was
included in RBF?
Process of CB How was it arranged?
Effects of CB Perceived usefulness of CB
b. Costing Costing methods How were costs arrived at?
Content How was costing arranged?
Effects of costing methods Perceived effect of costing
methods on project performance
or buy in?
Challenges What were the challenges in
costing?
Solutions How were costing problems
addressed?
c. Information systems Preceding information
systems
Which information systems were
being used prior to start of RBF
scheme?
Type Which information systems were
adopted for RBF?
Reasons Why was it adopted?
Process How was system arranged?
Effects Perceived usefulness of system
d. Accountability Type What accountability approaches
were used by scheme? E.g
auditing and reports
Reasons Why was it arranged/or not?
Process How was it arranged?
Performance determinants What factors facilitate or hinder
performance?
Effects Perceived usefulness of the
accountability mechanisms.
e. Donor harmonisation
of aid systems
Reasons Why was it arranged/or not?
s Process How was it arranged?
Performance determinants What factors facilitate or hinder
performance?
Effects Perceived usefulness of the aid
harmonisation mechanisms.