Embed Size (px)
Citation preview

Inr. J. Radiation Oncology Bml. Phys Vol. 9. pp. 1191. II94 036~3016/83/081191-04103.00/0 Printed in the U.S.A. All rights reserved. CopyrIght 6 1983 Pergamon Press Ltd
0 Original Contribution
LATE BREAST RECURRENCE AFTER LUMPECTOMY AND IRRADIATION
JOHN M. KURTZ, M.D.,’ JEAN-MAURICE SPITALIER, M.D.’ AND ROBERT AMALRIC, M.D.3
‘The Swedish Hospital Tumor Institute, Seattle Washington, The Departments of ‘Surgery and ‘Radiotherapy of the Cancer Institute, Marseille, France
For 276 patients with early breast cancer followed from lo-21 years after lumpectomy and radiotherapy, the recurrence rate in the treated breast was 15.6%, and 7.2% developed contralateral breast cancer. Only 63% of breast recurrences occurred within 5 years, and the remainder were “late failures,” with 5 of the 43 recurrences observed after 10 years. The proportion of failures occurring late was greater for T, than for T, tumors (53% vs 25 % ). Twenty-six percent of early recurrences were inoperable, and an adverse impact of early recurrence on 1 O-year survival was clearly demonstrable. Late recurrences were all operable and did not appear to be associated with decreased survival. Only 16 of the 36 patients (44%) with operable breast recurrence ever developed metastatic disease, and 5 year survival following salvage therapy was 62%. Although the treated breast remains at continuous cancer risk even beyond 5 years, the prognosis of late recurrence appears quite similar to that of contralateral breast cancer. We do not consider the phenomenon of late recurrence to lend support to a policy of primary mastectomy, just as the existence of contralateral breast cancer does not justify routine “prophylactic” contralateral mastectomy.
Breast cancer, Primary radiation therapy, Local recurrence, Salvage surgery.
INTRODIJCTION The combination of limited surgery and irradiation is gaining increasing acceptance as an alternative to modi- fied radical mastectomy in the primary therapy of early breast cancer. Although data from both long-term retro- spective studies’,4*i’ as well as two ongoing randomized trials”,is suggest that survival is not adversely affected by breast-conserving therapy, the literature provides little data regarding the fate of the treated breast itself 5, 10 or 15 years after primary radiotherapy. There is a wide- spread tendency to apply to the intact breast the same expectations derived from the postoperative irradiation of the mastectomized patient, namely that (a) 4500-5000 cGy in 5 weeks will sterilize more than 90% of subclinical breast cancer, and (b) 75% of recurrences occur within 3 years, recurrences after 5 years being rare.’ This study was undertaken in order to determine recurrence rates in patients followed for many years after lumpectomy and irradiation, to describe the chronology of mammary recurrence, to investigate the effectiveness of salvage treatment, and to elucidate the ultimate prognosis of local failure.
METHODS AND MATERIALS
Between June 1960, and December 197 1, 276 patients with early breast cancer (T,.,, N&,) were treated by
lumpectomy and radiotherapy at the Cancer Institute and associated clinics in Marseille. Only 6% of these patients were lost to follow-up. Criteria for patient selection as well as treatment techniques have been previously described in detai1.‘6.‘7 Briefly, all patients had histologi- cally-verified breast carcinoma with a clinical diameter of 5 cm or less, with minimal or no palpable axillary adenopathy. During the time period in question, radio- therapy was delivered almost exclusively using a telece- sium unit encompassing both the breast and the regional lymph nodes. Breast doses were typically 5000-6000 cGy with boost to the primary tumor area employing reduced cesium fields at short distance. Total doses to the tumor bed were usually between 7000 and 9000 cGy. Therapy was delivered 5 days per week without treatment breaks, ordinarily at a weekly dose rate between 850 and 1050 cGy per week. Prior to 1968, however, 65 patients were treated with a protracted treatment course of IO weeks or more, sometimes with weekly dose rates as low as 400- 600 cGy per week.
During the time period of this study, primary limited surgery consisted almost exclusively of simple lumpecto- my. No special effort was made to obtain a wide margin of grossly normal tissue around the tumor. Limited axil- lary dissection was performed in only 13 patients. Adju- vant chemotherapy was not employed, but selected
Presented at the 24th Annual Meeting of the American Society of Therapeutic Radiologists, Orlando, Florida, October 27, 1982.
Reprint requests to: John M. Kurtz, M.D., The Swedish
Hospital Tumor Institute, 1221 Madison St., Seattle, WA 98104.
Accepted for publication 23 March 1983.

1192 Radiation Oncology 0 Biology 0 Physics August 1983, Volume 9, Number 8
premenopausal patients with poor prognostic features descriptions were available, the majority (27, or 87%) underwent surgical oophorectomy. After primary treat- were in the vicinity of the original tumor. There appeared ment, patients were followed at regular intervals, with to be a greater tendency for the late failures to be “new mastectomy held in reserve in the event of apparent local tumors,” with 25% being either multiple or clearly sepa- or regional failure. rate from the original site.
RESULTS
With follow-up ranging from 10 to 21 years, 43 of the 276 patients (15.6%) have developed proven cancer in the treated breast. In addition, 20 patients (7.2%) have developed contralateral breast cancer, 4 of whom also had ipsilateral recurrence. Five patients had isolated axillary recurrence without failure in the breast. The frequency of mammary recurrence was slightly higher for larger tumors with 19/ 139 (13.3%) of T, and 24/ 137 (17.5%) of T, tumors ultimately failing in the breast. Of 47 patients having treatment protracted at dose rates less than 800 cGy/week, the mammary recurrence rate was 27.6%, whereas the breast failure rate in the remainder of the patient population was 12.8%.
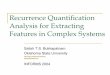
The chronology of mammary recurrences is described in Figure 1. Only 27 (63%) occurred by 5 years, the remainder being considered “late failures,” 5 recurrences (12%) being documented between 10 and 14 years. No failures were noted beyond 14 years, but only 29 patients were alive to be at risk for local failure at 15 years. Late failure was more common for smaller tumors, with 1 O/ 19 (53%) of T, mammary recurrences occurring after 5 years in contrast to only 6/24 (25%) of Tz breast failures. For comparison, contralateral breast cancers are also represented in Figure 1. They show a similar distribution in time to the ipsilateral recurrences but occur at approxi- mately half the rate; e.g., during the first 5 years, the actuarial risks of ipsilateral recurrence and contralateral cancers are about 2% per year and 1% per year respec- tively.
An attempt was made to determine from the patients’ records whether the recurrent tumor was located at or near the primary excision site or whether it was clearly separate. In 12 instances, such a determination could not be made. However, in the 31 patients where adequate
Results of salvage therapy Of the 43 mammary recurrences, 7 were inoperable, 2
because of distant metastases and 5 because of rapid local growth. All of the inoperable patients were in the early recurrence group and all died of metastatic breast cancer within 3 years of local failure. All 16 late failures were operable, although 1 patient refused further surgical treatment and is alive and well on hormonal therapy 81/z years after recurring in the breast.
Salvage surgery most often consisted of a classical radical or modified radical mastectomy, although more conservative operations were employed in 5 instances. Of the 35 patients who had salvage operations, histologically positive axillary nodes were documented in 17 patients (49%), with a similar frequency in both early and late cases. Among 26 operable patients with adequate follow- up time after salvage treatment, 16 (62%) survived for at least 5 years following mammary recurrence. The 5 year survival following salvage surgery is essentially identical for both early and late failures. A second local recurrence was documented in only 3 patients following salvage surgery, which was thus effective in providing ultimate local control in 9 1% of operable mammary failures.
Table 1 illustrates the prognosis of breast recurrence. Early and late failures differ principally because of the 26% inoperability rate among the patients recurring prior to 5 years. The 10 year survival of the 36 operable patients is 72%, which does not differ from that of patients experiencing either no breast recurrence or those develop- ing contralateral carcinoma. However, if one includes the inoperable patients in the statistics, it becomes clear from both 10 year survival and from the incidence of treatment failure that early recurrences are associated with an unfavorable prognosis. The prognosis of late recurrence is distinctly more favorable, with operability and 10 year survival rates similar to those of patients developing
Years After 0 1 2 3 4 Primary Treatment
Ipsil ateral Breast 7 1 7 5 7 43/276 (15.6%)
5
.
.
.
.
.
.
.
.
.
.
.
6 7 a 9 10 11 12 13 14 15 . . . . .
2 1 3 2 3:2 0 1 2 0:O
Contralateral Breast 3 4 4 1 1 20/276 (7.2%)
. .
.
. .
0 0 1 2 2:1 0 0 0 0:1 . . . .
Fig. I, Mammary failures and contralateral cancers in 276 consecutive patients with minimum IO year follow-up after lumpectomy and radiotherapy.

Late breast recurrence 0 J. M. KURTZ et al. 1193
Table 1. Prognosis of mammary failure
Operability %
1 O-year survival following primary
treatment (So)
Treatment failure (follow-up 1 O-2 1 years)
(%)
Early mammary failure (~5 yr) N = 21
Late mammary failure (>5 yr) N = 16
Contralateral breast cancer N = 20
No mammary failure N = 233
14 41 59
100 94 50
100* 75 30
76 13
*Although anatomically operable, almost all patients were treated with breast conserving therapy. Treatment failure = distant metastases or uncontrolled local disease.
contralateral breast cancer but with a somewhat higher treatment failure rate.
DlSCUSSION
This long-term analysis of a large cohort of patients treated following lumpectomy with adequate doses of radiotherapy serves to allow the formation of conclusions regarding the frequency, time course and prognosis of breast recurrence. It is apparent that the concept of “subclinical” deposits of breast cancer derived from the irradiation of the mastectomized patient cannot be applied in a straightforward fashion to the intact breast following simple lumpectomy. The 15% recurrence rate seen in this series is considerably greater than the 5510% expected following the application of 4500-5000 cGy in 5 weeks in the post-mastectomy setting,’ and yet the total doses which our patients received were considerably higher than those theoretically required to sterilize “sub- clinical disease.” That these moderately-high doses were beneficial in minimizing breast recurrence is suggested by the significantly higher recurrence rate of 28% in the subgroup receiving biologically lower equivalent doses as well as the somewhat higher breast failure rates reported by other groups employing lower mammary dosesI no boost therapy,6 or minimal boost therapy.6
Contrary to expectations derived from post-mastec- tomy radiation therapy, it is quite apparent from the present study, as well as from the limited number of other long-term studies,3.6.‘3 that the risk of recurrent cancer in the treated breast remains significant even beyond 10 years. The phenomenon of late recurrence, i.e., recur- rence beyond the 5th year, is particularly striking for T, lesions, with 53% of breast failures.observed after 5 years in our series. The seemingly higher proportion of late failure in T, tumors may at least in part be due to the longer survival expectancy of the earlier stage patients.
The continuing risk of breast recurrence would be of grave concern were it not for the observation that mam- mary failure has a markedly more favorable prognosis
than local recurrence post mastectomy.’ Numerous clini- cal studies have documented that even “isolated” local recurrences following radical surgery have a poor outlook, with SO-90% of such patients developing further recur- rence or distant metastases.2.5 In contrast, only 44% of patients with operable breast recurrence eventually devel- oped metastatic disease, and 5 year survival following salvage treatment was 62%. Although inoperable local failure was uniformly fatal, inoperability was diagnosed in only 16% of patients, and all late failures were opera- ble. In addition, salvage therapy was very successful in assuring permanent local control in more than 90% of operable local failures. Even including the 7 inoperable failures, only 3.3% of the 276 patients suffered uncon- trolled local disease. This illustrates that, as a result of the effectiveness of salvage surgery, the ultimate local control provided by lumpectomy and irradiation is at least as good as that achieved by modified radical mastectomy.
Curative radiation therapy results not only for tumor cell death but also in massive destruction of lobules and ducts.” However, the irradiated breast is not a biologi- cally inert mass of tissue. The fact that some recurrences are multiple, or are at some distance from the original primary, illustrates that the phenomenon of multicentrici- ty,14 or “new” tumor formation plays at least some role in mammary failure. Although the percentage of clearly new sites was low in our series (16%), new tumor forma- tion may partially explain why the irradiated breast remains subject to a continuing cancer risk which is at least as high as that of the contralateral breast.
However, since the majority of breast failures are at least anatomically true recurrences, more aggressive treatment of the involved quadrant might be expected to yield superior local control. Current therapy at Marseille employs wedge resection in place of simple lumpectomy; alternative approaches include interstitial implanta- tion8.12 or, in the extreme, quadrantectomy.‘* These mea- sures, coupled with scrupulous radiation therapy tech- nique, should reduce the mammary failure rate well below the 15% reported here. However, we expect that the

1194 Radiation Oncology 0 Biology 0 Physics August 1983, Volume 9, Number 8
phenomenon of late recurrence will continue to be recog- be clearly specified in reporting recurrence rates in order nized, and that the proportion of failures occurring after 5 for statistics to be meaningful. The importance of long- years will remain relatively constant. The continuing risk term follow-up of conservatively-treated patients cannot of breast recurrence mandates that the follow-up interval be overemphasized.
REFERENCES I. Amalric, R., Santamaria, F., Robert, F., Seigle, J., Alt-
schuler, C., Kurtz, J.M., Spitalier, J.M., Brandone, H., Ayme, Y., Pallet, J.F., Burmeister, R., Abed, R.: Radiation therapy with or without primary limited surgery for opera- ble breast cancer: A 20-year experience at the Marseille Cancer Institute. Cancer 49: 30-34, 1982.
2. Bedwinek, J.M., Lee, J., Fineberg, B., Ocwieza, M.: Prog- nostic indicators in patients with isolated local-regional recurrences of breast cancer. Cancer 47: 2232-2235, I98 1.
3. Calle, R., Pilleron, J.P.: Radiation therapy, with and with- out lumpectomy, for operable breast cancer. Breast S(4): 2-6, 1979.
4. Calle, R., Pilleron, J.P., Schlienger, P., Vilcoq, J.R.: Con- servative management of operable breast cancer. Ten years’ experience at the Foundation Curie. Cancer 42: 204552053, 1978.
5. Chu, F.C.H., Lin, F., Kim, J.H., Huh,S.H.,Gormatis, C.J.: Locally recurrent carcinoma of the breast: Results of radia- tion therapy. Cancer 37: 26777268 I, 1976.
6. Clark, R.M., Wilkinson, R.H., Mahoney, L.J., Reid, J.G., MacDonald, W.D.: Breast cancer: A 2l-year experience with conservative surgery and radiation. Int. J. Radiaf. Oncol. Biol. Phys. 8: 967-975, 1982.
7. Fletcher, G.H., Montague, E., Nelson, A.J.: Combination of conservative surgery and irradiation for cancer of the breast. Am. J. Roentgenoi. 162: 216-22, 1976.
8. Hellman, S., Harris, J.R., Levene, M.B.: Radiation therapy of early carcinoma of the breast without mastectomy. Cancer 46: 988-994, 1980.
9. Kurtz, J.M., Spitalier, J.M., Amalric, R.: Results of salvage surgery for local failure following conservative therapy of operable breast cancer. In Frontiers of Radiation Therapy and Oncology. Vol. 17, Vaeth, J.M. (Ed.). Basel, Karger. 1983, pp. 84-90.
IO. Moss, W.T., Brand, W.N., Battifora, H.: Radiation Onco- logy. 5th Edition. St. Louis, C.V. Mosby Co. 1979, pp. 289-294.
I I. Peters, M.V.: Wedge resection with or without radiation in early breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2: 1151-l 156, 1977.
12. Pierquin, B., Owen, R., Maylin, C., Otmezguine, Y., Ray- nal, M., Mueller, W., Hannoun, S.: Radical radiation therapy of breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 6: 17-24, 1980.
13. Rissanen, P.M.: A comparison of conservative and radical surgery combined with radiotherapy in the treatment of Stage I carcinoma of the breast. Br. J. Radiol. 42: 423-426, 1969.
14. Rosen, P.P., Fracchia, A.A., Urban, J.A., Schottenfeld, D., Robbins, G.F.: “Residual” mammary carcinoma following simulated partial mastectomy. Cancer 35: 739-747, 1975.
15. Sarrazin, D., Le, M., Fontaine, F., Arriagada, R.: Conser- vative treatment versus mastectomy in T, or small T, breast cancer (Abstract). Proceedings of European Society for Therapeutic Radiology and Oncology, June 28, 1982, p. IO.
16. Spitalier, J.M., Amalric, R.: Treatment of operable mam- mary carcinomas with conservation of the breast at the Cancer Institute of Marseille. In Breast Disease. New York, Grune & Stratton, Inc. 1979, pp. 222-25 I.
17. Spitalier, J., Brandone, H., Ayme, Y., Amalric, R., Santa- maria, F., Seigle, J.: Cesium therapy of breast cancer. A five-year report on 400 consecutive patients. In?. J. Radial. Oncol. Biol. Phys. 2: 231-235, 1977.
18. Veronesi, U., Sacozzi, R.. DelVecchio, M., Banfi, A. et al.. Comparing radical mastectomy with quadrantectomy, axil- lary dissection and radiotherapy in patients with small cancers of the breast. New Eng. J. Med. 305: 6-l I, 198 1.