Embed Size (px)
Citation preview
REVIEW
Laparoscopic treatment of Mirizzi syndrome: a systematic review
Stavros A. Antoniou Æ George A. Antoniou ÆCharalambos Makridis
Received: 16 January 2009 / Accepted: 22 April 2009 / Published online: 23 May 2009
� Springer Science+Business Media, LLC 2009
Abstract
Background This article reviews the feasibility of the
laparoscopic treatment of Mirizzi syndrome and determines
the associated risks and complications of this technique.
Methods An electronic search of the literature between
1989 and 2008 was undertaken to identify relevant articles.
Studies comprising at least four patients treated by lapa-
roscopy and reporting on the preoperative diagnosis rate
and analytical conversion and complication data were
considered for inclusion.
Results From 66 abstracts reviewed, 10 eligible studies
were identified. Conversion, complication, and reoperation
rates were 41%, 20%, and 6%, respectively. The risks for
open conversion and procedure-related complications were
similar for patients with type I and type II Mirizzi syn-
drome. However, patients of studies reporting a high pre-
operative diagnosis rate had a significantly lower risk for
conversion (p \ 0.05), procedure-related complications
(p \ 0.05), and reoperation (p \ 0.05), when compared
with studies with a low preoperative diagnosis rate.
Conclusion Current evidence suggests that laparoscopic
treatment of Mirizzi syndrome cannot be recommended as
a standard procedure. Preoperative diagnosis of the syn-
drome seems an important predicting factor of technical
success.
Keywords Mirizzi syndrome � Cholecystobiliary fistula �Laparoscopy � Laparoscopic cholecystectomy � Review
Mirizzi syndrome (MS) is an uncommon complication of
gallstone disease, with a reported incidence between 0.06%
and 5.7% in patients undergoing cholecystectomy [1, 2].
The condition was originally described by Kehr in 1905
[3], but it was named after Pablo Mirizzi several years
later, who defined the syndrome as a benign common
hepatic duct obstruction due to gallstone impaction in the
gallbladder neck resulting in local inflammation and bile
duct spasm [4]. As it was eventually recognized that there
is no physiological sphincter of the hepatic duct, MS was
finally attributed to extrinsic compression of the common
hepatic duct by gallstones impacted in the cystic duct or the
gallbladder neck [5]. Bile duct wall necrosis and sub-
sequent cholecystobiliary fistula caused by chronic
inflammation is a rare sequence of the disease.
The most widely accepted classification of MS was
proposed by McSherry et al. [6], who described two types:
type I includes partial or complete obstruction of the
common hepatic duct due to external compression; type II
refers to the formation of a communication between the
gallbladder neck or the cystic duct and the common hepatic
duct. Csendes et al. further subclassified cholecystobiliary
communication into three types according to the diameter
of the biliary fistula [7]. In this classification, type II is a
cholecystobiliary fistula that involves less than one-third of
the circumference of the bile duct, type III is a fistula that
involves up to two-thirds of the bile duct circumference,
and type IV is a fistula with complete bile duct destruction.
The classification suggested by McSherry et al. was used in
this systematic review.
This review will be presented in the 9th Panhellenic Congress of
Laparoendoscopic Surgery and International Symposium
‘‘Collaboration for Surgery Evolution’’ May 21–23, 2009, Athens,
Greece.
S. A. Antoniou (&) � G. A. Antoniou � C. Makridis
First Surgical Department, Papageorgiou General Hospital,
Thessaloniki Ring Road, 564 29 Thessaloniki, Greece
e-mail: [email protected]
123
Surg Endosc (2010) 24:33–39
DOI 10.1007/s00464-009-0520-5

The treatment of MS is mainly surgical and consists of
partial or complete cholecystectomy with or without com-
mon bile duct exploration. Choledochoplasty with a gall-
bladder flap and T-tube placement may be required in
complex cases, but extensive erosions of the bile duct are
best managed with a bilioenteric anastomosis [5, 8]. Endo-
scopic retrograde cholangiopancreaticography (ERCP) may
be the only option for poor surgical candidates. Electrohy-
draulic and extracorporeal shock wave lithotripsy have also
been described as alternatives to surgical therapy [9, 10].
Shortly after the advent of laparoscopy in the treatment
of gallbladder diseases, Rust et al. suggested that MS may
be a contraindication for laparoscopic cholecystectomy
[11]. In 1992, Paul et al. reported the first successful lap-
aroscopic treatment of type I MS [12]. Several cases were
described thereafter; this new method, however, has not
gained wide acceptance, partly because of the lack of large
series due to the rarity of the syndrome and the contro-
versial results of different reports.
The purpose of the present study was to systematically
review the literature in order to analyze the preoperative
investigation methods, the outcome, and the complications
of the laparoscopic treatment of MS.
Methods
Search strategy
A public-domain database (MEDLINE) was searched using
a web-based search engine (PubMed) for articles published
between December 1989, when the technique of laparo-
scopic cholecystectomy was first described, and December
2008. The literature search was confined to studies pub-
lished in English and German. The keywords used were
‘‘Mirizzi syndrome AND laparoscopy’’ and ‘‘Mirizzi syn-
drome AND laparoscopic cholecystectomy.’’ Abstracts of
the articles found were scrutinized to identify the original
articles. The full text of each original article was then
obtained. Manual cross-referencing was also carried out,
based on the bibliography of articles identified in the pri-
mary search, to ensure inclusion of all possible studies. The
literature search, study selection, and data extraction from
the relevant studies were performed by two independent
authors (S.A.A., G.A.A.).
Study selection
Studies were considered for inclusion based on the fol-
lowing criteria: (1) they included at least four patients with
MS who were treated by laparoscopy, (2) they reported on
the preoperative diagnosis rate, and (3) they reported on
analytical conversion and complication data.
Data abstraction and statistical analysis
Data abstracted, where available, from individual studies
were: type of study (prospective or retrospective), number
of patients with MS, number of patients with MS treated by
laparoscopy, duration of follow-up, demographic charac-
teristics of the study population, MS type I/MS type II
ratio, preoperative diagnosis rate, sensitivity of each diag-
nostic tool, conversion rate, conversion rate according to
type of MS, reason for conversion, complication rate,
complication rate according to type of MS, reoperation
rate, reoperation rate according to type of MS, and days of
in-hospital stay.
The statistical analysis was performed using the two-
tailed Fisher’s exact probability test, in order to compare
the outcome between study groups with a high or low
preoperative diagnosis rate of MS. The same statistical test
was used to compare the outcome between MS type I and
MS type II patients. A p value less than 0.05 was consid-
ered statistically significant.
Results
Search results
Sixty-six abstracts were initially located, and 15 relevant
articles were retrieved. Ten of these articles fulfilled the
inclusion criteria [13–22]. The reasons for rejection were:
non-English and non-German articles (20), fewer than four
patients treated laparoscopically (20), open or other types
of treatment (4), inadequate complication data (3), reviews
(1), letters to the editor (1), and not related articles (7)
(Fig. 1). The ten recruited studies with details on their
characteristics are summarized in Table 1.
Fig. 1 Flow chart of search history
34 Surg Endosc (2010) 24:33–39
123
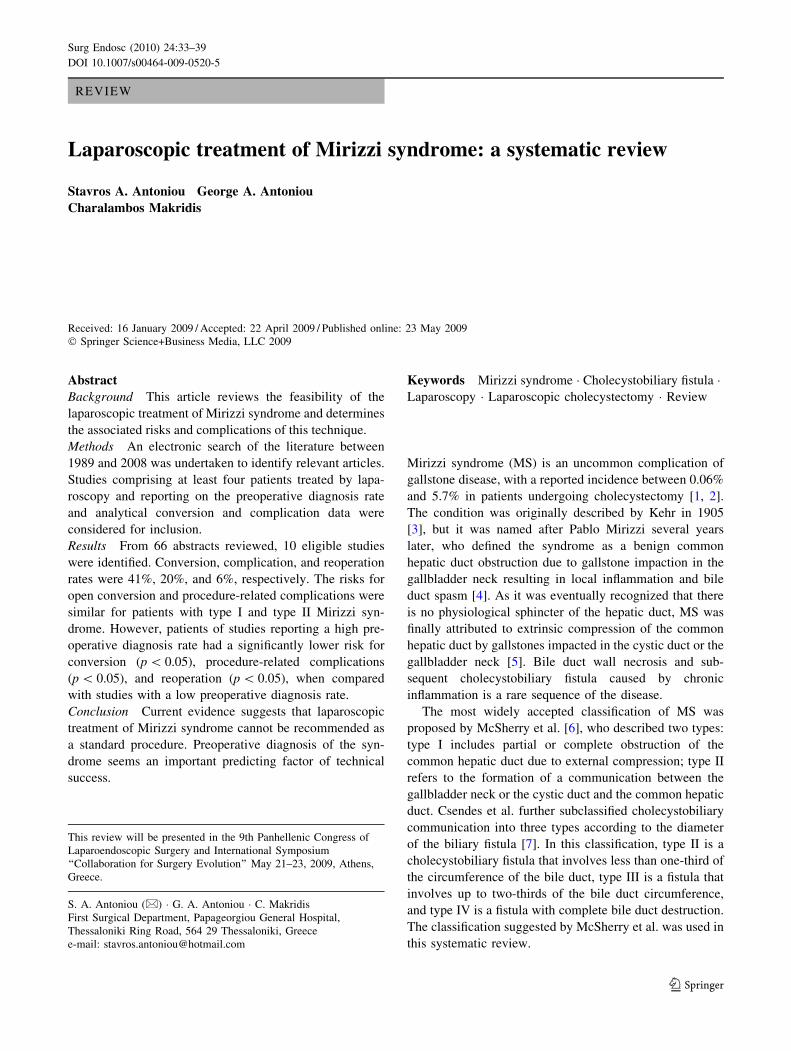
Characteristics of the study population
The ten manuscripts identified 135 patients with MS; lap-
aroscopic treatment was attempted in 124 of these patients.
In one study, a patient with unspecified type of MS was
excluded from the laparoscopic approach [13]. In another
study, all patients with type II MS were subjected to open
cholecystectomy and were excluded from further analysis
[22]. MS type I/MS type II ratio varied substantially among
different reports (Table 2). The male/female ratio was
1:3.2 in the eight publications providing data on patient
sex. The median age in the nine studies providing data on
age was 61 years (range 44–68 years). It is clear from
Table 3 that there is significant heterogeneity in the pre-
operative diagnosis rate of MS among the different studies.
Most studies reported the use of ERCP and/or ultraso-
nography in order to confirm the diagnosis of MS; ERCP
was proved to be the most reliable assessment tool and
identified MS in 76.2%.
Technical success
Of a total of 124 patients, laparoscopic treatment of MS
was successful in 73 patients (59%); conversion was
required for 51 (41%) (Table 4). Seven studies provided
information on conversions for each MS subtype. Con-
version to open surgery was required in 32 of 68 patients
with type I MS (47%) and in 7 of 16 patients with type II
MS. Table 5 summarizes the reasons for open conversion
sorted by frequency. The most common reason for con-
version was adhesions around the Calot’s triangle, fol-
lowed by uncertain or abnormal biliary anatomy.
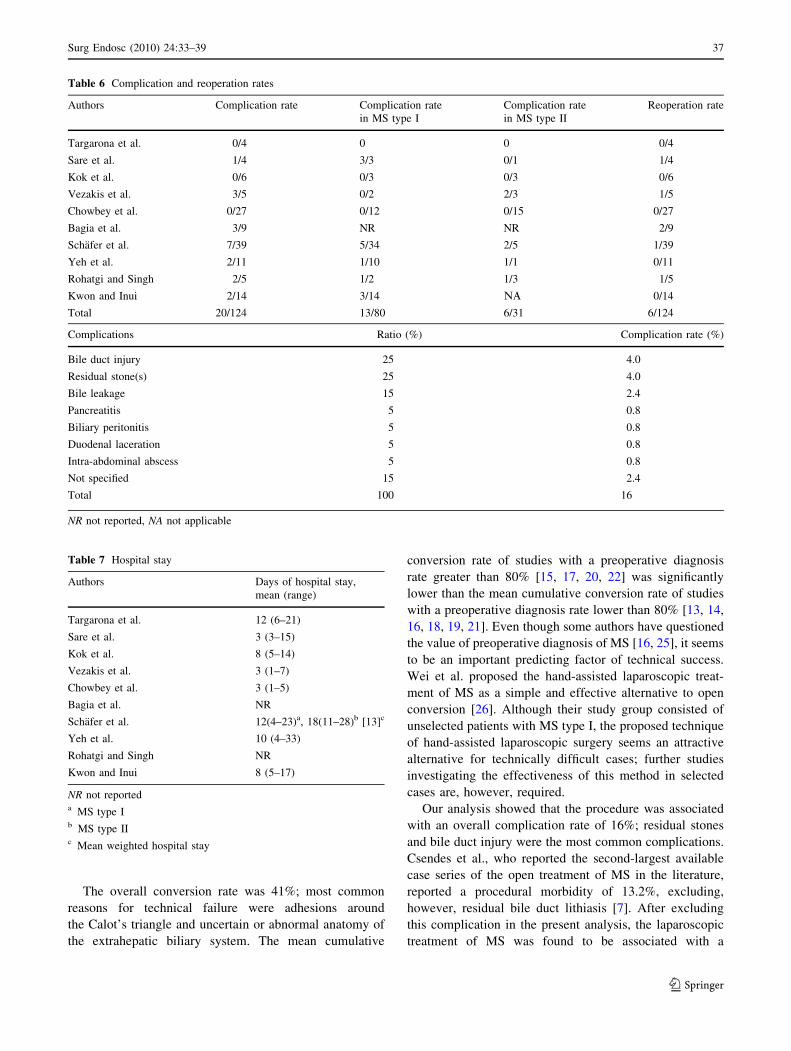
Complications and reoperations
Table 6 shows the complication and reoperation rate for
each individual study. The mean complication rate was 20
of 124 (16%). Additionally, Table 6 shows the procedure-
related complications sorted by frequency. Bile duct injury
and residual lithiasis were the most common complica-
tions, occurring in five patients each. Minor bile leakage
complicated three cases. Isolated incidents of pancreatitis,
biliary peritonitis, duodenal laceration, and intra-abdomi-
nal abscess were also reported. One procedure-related
death was reported in the literature [14], due to biliary
peritonitis and septic shock, accounting for a mortality rate
of 0.8%.
Reoperation was required in 6 of 124 patients: in 2
patients for a major bile duct injury, in another 2 patients
for the management of biliary peritonitis, in 1 patient to
extract a residual bile duct stone, and in another patient to
excise a gallbladder carcinoma, resulting in a reoperation
rate of 5% (Table 6). Most studies did not report on the
reoperation rate for each type of MS; therefore, the risk for
secondary intervention of each MS subgroup could not be
Table 1 Study characteristics
Authors Year Study type No. of patients
with MS
No. of patients treated
by laparoscopy
Duration of
follow-up (months)
Targarona et al. [13] 1997 Retro 5 4 3–36/mean 19
Sare et al. [14] 1998 Retro 4 4 NR
Kok et al. [15] 1998 Retro 6 6 8–17/mean 12
Vezakis et al. [16] 2000 NR 5 5 26–61/mean 37
Chowbey et al. [17] 2000 Retro 27 27 Mean 26
Bagia et al. [18] 2001 Prosp 9 9 NR
Schafer et al. [19] 2003 Prosp 39 39 NR
Yeh et al. [20] 2003 Retro 11 11 NR
Rohatgi and Singh [21] 2006 Retro 5 5 NR
Kwon & Inui [22] 2007 NR 24 14 NR
Total 135 124
NR not reported
Table 2 Patient characteristics
Authors Male
(%)
Age (mean),
years
MS type I
(n)
MS type II
(n)
Targarona et al. 40 54 NR NR
Sare et al. 25 59 3 1
Kok et al. 50 64 3 3
Vezakis et al. NR 68 2 3
Chowbey et al. NR NR 12 15
Bagia et al. 22 44 8 1
Schafer et al. 36 61 34 5
Yeh et al. 36 51 10 1
Rohatgi and Singh 20 66 2 3
Kwon and Inui 63 63 14 0
NR not reported
Surg Endosc (2010) 24:33–39 35
123
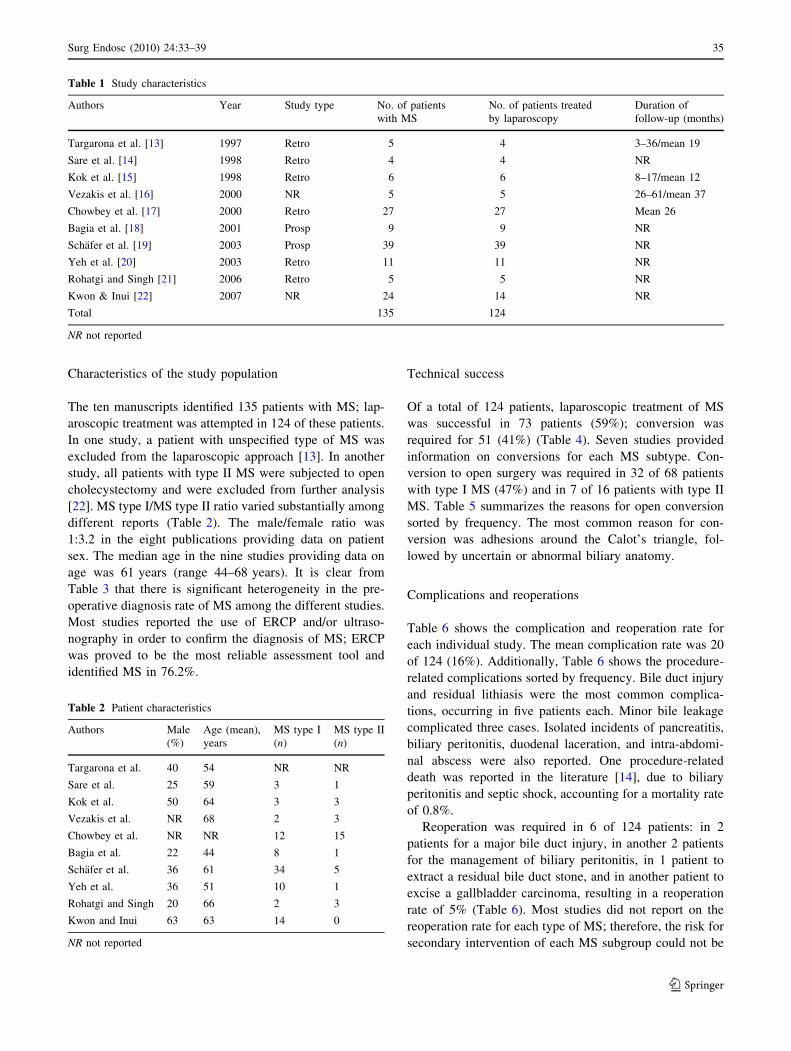
evaluated. Details on the length of hospital stay were
available in eight studies (Table 7); the median hospital
stay was 8 days (range 3–13 days).
As shown in Table 8, patients of studies reporting a high
preoperative diagnosis rate ([80%) had a significantly
lower risk for conversion (p \ 0.05), when compared with
studies with a low preoperative diagnosis rate (\80%).
Additionally, they had a lower risk for suffering procedure-
related complications (p \ 0.05), or undergoing reopera-
tion (p \ 0.05). Furthermore, MS type II patients did not
have a higher risk for conversion or procedure-related
complications, compared with the MS type I subgroup.
Discussion
The difficult surgical management of MS is due to the
presence of an intense fibrotic process and/or communi-
cation between the gallbladder and the common hepatic
duct. Since laparoscopic cholecystectomy became a routine
procedure in the early 1990s, only a few studies have been
published describing their experience with the laparoscopic
technique for the treatment of MS. They were all case
reports or case series; a randomized controlled study
comparing the open with the laparoscopic approach is
currently lacking in the surgical literature. The objectives
of this review were, therefore, to examine the feasibility of
the laparoscopic treatment of MS and to determine the
associated risks and complications.
The mean preoperative diagnosis rate was 66.1%. Most
authors reported ERCP as the preferred diagnostic proce-
dure when MS is suspected; this assessment tool had a
satisfactory mean sensitivity rate of 76.2%. Interestingly,
Kwon and Inui reported a 100% sensitivity rate for spiral
computed tomography after infusion cholangiography,
which was used in 11 of their patients [22]. This exami-
nation, however, is not widely utilized, because the contrast
agents often cause significant nausea on administration
[23]; additionally, the technique is only effective in
patients with serum bilirubin greater than 2 mg/dl [24].
Table 3 Preoperative diagnosis rates
Authors Preoperative
diagnosis
rate (%)
ERCP sensitivity
rate
U/S sensitivity
rate
PTC sensitivity
rate
CT sensitivity
rate
MRCP sensitivity
rate
SCT sensitivity
rate
Targarona et al. 3/4 (75) 3/4 0/5 – 0/1 – –
Sare et al. 3/4 (75) 2/4 0/3 1/1 – – –
Kok et al. 6/6 (100) 6/6 NR – – – –
Vezakis et al. 0/5 (0) 0/3 0/5 – – – –
Chowbey et al. 22/27 (82) 22/27 NR – – – –
Bagia et al. 3/9 (33) 0/3 2/9 – – – –
Schafer et al. 18/39 (46) NR NR – – – –
Yeh et al. 11/11 (100) 11/11 5/11 – 3/3 2/2 –
Rohatgi and Singh 2/5 (40) 1/2 1/5 – – 0/2 –
Kwon and Inui 14/14 (100) 3/3 NR – – – 11/11
ERCP endoscopic retrograde cholangiopancreaticography, U/S ultrasound, PTC percutaneous transhepatic cholangiography, CT computed
tomography, MRCP magnetic resonance cholangiopancreaticography, SCT spiral computed tomography after infusion cholangiography
Table 4 Conversion rates
Authors Conversion
rate
Conversion rate
in MS type I
Conversion rate
in MS type II
Targarona et al. 4/4 NR NR
Sare et al. 1/4 0/3 1/1
Kok et al. 1/6 1/3 0/3
Vezakis et al. 0/5 0/2 0/3
Chowbey et al. 6/27 NR NR
Bagia et al. 2/9 NR NR
Schafer et al. 29/39 24/34 5/5
Yeh et al. 4/11 3/10 1/1
Rohatgi and Singh 0/5 0/2 0/3
Kwon and Inui 4/14 4/14 NA
Total 51/124 32/68 7/16
NR not reported, NA not applicable
Table 5 Reasons for conversion
Reason for conversion Ratio (%) Conversion rate (%)
Adhesions 40.9 10.6
Uncertain/abnormal anatomy 31.8 8.2
Unsuccessful stone retrieval 13.6 3.5
Gallbladder carcinoma 4.5 1.2
Bleeding 4.5 1.2
Unsuccessful T-tube insertion 4.5 1.2
Total 100 –
36 Surg Endosc (2010) 24:33–39
123
The overall conversion rate was 41%; most common
reasons for technical failure were adhesions around
the Calot’s triangle and uncertain or abnormal anatomy of
the extrahepatic biliary system. The mean cumulative
conversion rate of studies with a preoperative diagnosis
rate greater than 80% [15, 17, 20, 22] was significantly
lower than the mean cumulative conversion rate of studies
with a preoperative diagnosis rate lower than 80% [13, 14,
16, 18, 19, 21]. Even though some authors have questioned
the value of preoperative diagnosis of MS [16, 25], it seems
to be an important predicting factor of technical success.
Wei et al. proposed the hand-assisted laparoscopic treat-
ment of MS as a simple and effective alternative to open
conversion [26]. Although their study group consisted of
unselected patients with MS type I, the proposed technique
of hand-assisted laparoscopic surgery seems an attractive
alternative for technically difficult cases; further studies
investigating the effectiveness of this method in selected
cases are, however, required.
Our analysis showed that the procedure was associated
with an overall complication rate of 16%; residual stones
and bile duct injury were the most common complications.
Csendes et al., who reported the second-largest available
case series of the open treatment of MS in the literature,
reported a procedural morbidity of 13.2%, excluding,
however, residual bile duct lithiasis [7]. After excluding
this complication in the present analysis, the laparoscopic
treatment of MS was found to be associated with a
Table 6 Complication and reoperation rates
Authors Complication rate Complication rate
in MS type I
Complication rate
in MS type II
Reoperation rate
Targarona et al. 0/4 0 0 0/4
Sare et al. 1/4 3/3 0/1 1/4
Kok et al. 0/6 0/3 0/3 0/6
Vezakis et al. 3/5 0/2 2/3 1/5
Chowbey et al. 0/27 0/12 0/15 0/27
Bagia et al. 3/9 NR NR 2/9
Schafer et al. 7/39 5/34 2/5 1/39
Yeh et al. 2/11 1/10 1/1 0/11
Rohatgi and Singh 2/5 1/2 1/3 1/5
Kwon and Inui 2/14 3/14 MA 0/14
Total 20/124 13/80 6/31 6/124
Complications Ratio (%) Complication rate (%)
Bile duct injury 25 4.0
Residual stone(s) 25 4.0
Bile leakage 15 2.4
Pancreatitis 5 0.8
Biliary peritonitis 5 0.8
Duodenal laceration 5 0.8
Intra-abdominal abscess 5 0.8
Not specified 15 2.4
Total 100 16
NR not reported, NA not applicable
Table 7 Hospital stay
Authors Days of hospital stay,
mean (range)
Targarona et al. 12 (6–21)
Sare et al. 3 (3–15)
Kok et al. 8 (5–14)
Vezakis et al. 3 (1–7)
Chowbey et al. 3 (1–5)
Bagia et al. NR
Schafer et al. 12(4–23)a, 18(11–28)b [13]c
Yeh et al. 10 (4–33)
Rohatgi and Singh NR
Kwon and Inui 8 (5–17)
NR not reporteda MS type Ib MS type IIc Mean weighted hospital stay
Surg Endosc (2010) 24:33–39 37
123

complication rate of 12%. Bile leakage complicated only 3
of 124 cases treated by laparoscopy; however, biliary
peritonitis led to septic shock and death in one case,
resulting in an overall mortality rate of 0.8% [14]. The in-
hospital mortality of the open procedure was reported to be
6.8% [7]. However, the above comparative results should
be approached with caution, because the aforementioned
study examined a population with a lower MS type I/MS
type II ratio.
Reoperation was required in six patients (5%); further-
more, higher preoperative suspicion index of MS was also
associated with a lower risk for reoperation (p \ 0.05). The
literature search for the open procedure did not provide
adequate data to allow comparative evaluation of risk for
reoperation. The mean weighted in-hospital stay was
8.4 days. This result could also not be comparatively
evaluated, as we did not identify any large series of the
open procedure reporting data on hospital stay.
The physiopathology of MS has been adequately
described during the past two decades [6, 7]. Cholecy-
stobiliary fistula is now considered an evolving stage of
longstanding gallstone disease [27]. Additionally, Beltran
et al. recently recognized cholecystoenteric fistula as a
further complication of chronic cholecystolithiasis [2]. The
reverse of the MS type I/MS type II ratio (2.1:1) observed
in the present review in contrast to several studies pub-
lished before the advent of laparoscopy [2, 7, 28] can be
attributed to the early diagnosis and treatment of patients
with gallstone disease in the laparoscopic era, and thus the
fall of the incidence of severe complications of the disease.
Csendes et al. reported a significantly higher morbidity for
patients with MS type III and IV (Csendes classification)
treated with the open procedure, when compared with the
other groups [7]. This may be explained by the physiopa-
thology of the syndrome, as cholecystobiliary fistula rep-
resents a complex sequence of MS type I, impairing the
physiological anatomic structures and making bile duct
dissection hazardous. Nevertheless, in the present review of
laparoscopic treatment of MS, there was no statistical
significance in the conversion and complication rates
between the MS subtypes, as would be expected.
From the literature reviewed, it appears that the outcome
of laparoscopic treatment of MS is not inferior to that of
open surgery, but it carries a significant conversion rate.
However, preoperative diagnosis of the syndrome is asso-
ciated with a decrease of the conversion and complication
rates to 45% and 54%, respectively. This evidence suggests
that patients with clinical suspicion of MS should undergo
an intensive diagnostic algorithm. Desai and Smink have
recommended preoperative ERCP in all patients with
jaundice and elevated liver function tests, and intraopera-
tive cholangiography in case of a negative result [29]. In
the era of minimally invasive treatment, we would suggest
solely the use of intraoperative cholangiography; if cathe-
terization of the cystic duct is unfeasible or the common
bile duct cannot be visualized, we would consider MS as a
potential diagnosis and perform intraoperative ERCP, if
available. A study comparing the aforementioned tools for
the diagnosis of MS would be of great interest.
The moderate technical success rate of the laparoscopic
treatment of MS suggests that it cannot be recommended as
a standard procedure. A stronger emphasis should be given
to the preoperative diagnosis of the syndrome, as it seems
to be associated with significantly lower risks for conver-
sion, procedure-related complications, and reoperation.
However, at least one randomized controlled trial com-
paring conventional open and laparoscopic treatment of
MS is required to consolidate these conclusions.
References
1. Becker CD, Hassler H, Terrier F (1984) Preoperative diagnosis of
the Mirizzi syndrome: limitations of sonography and computed
tomography. AJR 143:591–596
2. Beltran MA, Csendes A, Cruces KS (2008) The relationship of
Mirizzi syndrome and cholecystoenteric fistula: validation of a
modified classification. World J Surg 32:2237–2243
3. Kehr H (1905) Die in meiner Klinik geubte Technik der Galle-
steinoperationen mit einem Hinweis auf die Indikationen und die
Dauererfolge. JF Lehman, Munich
4. Mirizzi PL (1948) Sindrome del conducto hepatico. J Int Chir
8:731–777
5. Abou-Saif A, Al-Kawas FH (2002) Complications of gallstone
disease: Mirizzi syndrome, cholecystocholedochal fistula, and
gallstone ileus. Am J Gastroenterol 97:249–254
6. McSherry CK, Ferstenberg H, Virshup M (1982) The Mirizzi
syndrome: suggested classification and surgical therapy. Surg
Gastroenterol 1:219–225
Table 8 Comparison of outcome according to preoperative diagnosis rate and type of MS
Preoperative diagnosis rate p Type of MS p
[80% \80% Type I Type II
Conversion rate (%) 15/58 (25.9) 36/66 (54.5) 0.043 32/68 (47.0) 7/16 (43.8) NS
Complication rate (%) 4/58 (6.9) 16/66 (24.2) 0.029 13/80 (16.3) 6/31 (19.4) NS
Reoperation rate (%) 0/58 (0) 6/66 (9.1) 0.033 – – –
NS not significant
38 Surg Endosc (2010) 24:33–39
123

7. Csendes A, Dias JC, Burdiles P, Maluenda F, Nava O (1989)
Mirizzi syndrome and cholecystobiliary fistula: a unifying clas-
sification. Br J Surg 76:1139–1143
8. Bower TC, Nagorney DM (1988) Mirizzi syndrome. HPB Surg
1:67–76
9. Binmoeller KF, Thonke F, Soehendra N (1993) Endoscopic treat-
ment of Mirizzi’s syndrome. Gastrointest Endosc 39:532–536
10. Benninger J, Rabenstein T, Farnbacher M, Keppler J, Hahn EG,
Schneider HAT (2004) Extracorporeal shockwave lithotripsy of
gallstones in cystic duct remnants and Mirizzi syndrome. Gas-
trointest Endosc 60:454–459
11. Rust KR, Chancy TV, Warren G, Mertesdorf J, Maxwell JG (1991)
Mirizzi syndrome: a contraindication to coelioscopic cholecys-
tectomy. J Laparoendosc Surg 1:133–137
12. Paul MG, Burris DG, McGuire AM, Thorfinnson HD, Schonekas
H (1992) Laparoscopic surgery in the treatment of Mirizzi syn-
drome. J Laparoendosc Surg 2:157–163
13. Targarona EM, Andrade E, Balague C, Ardid J, Trıas M (1997)
Mirizzi’s syndrome: diagnostic and therapeutic controversies in
the laparoscopic era. Surg Endosc 11:842–845
14. Sare M, Gurer S, Taskin V, Aladag M, Hilmioglu F, Gurel M
(1998) Mirizzi syndrome: choice of surgical procedure in the
laparoscopic era. Surg Laparosc Endosc 8:63–67
15. Kok KYY, Goh PYM, Ngoi SS (1998) Management of Mirizzi
syndrome in the laparoscopic era. Surg Endosc 12:1242–1244
16. Vezakis A, Davides D, Birbas K, Ammori BJ, Larvin M, McMahon
MJ (2000) Laparoscopic treatment of Mirizzi syndrome. Surg
Laparosc Endosc Percutan Tech 10:15–18
17. Chowbey PK, Sharma A, Mann V, Khullar R, Baijal M, Vashistha
A (2000) The management of Mirizzi syndrome in the laparoscopic
era. Surg Laparosc Endosc Percutan Tech 10:11–14
18. Bagia JS, North L, Hunt DR (2001) Mirizzi syndrome: an extra
hazard for laparoscopic surgery. ANZ J Surg 71:394–397
19. Schafer M, Schneiter R, Krahlenbuhl L (2003) Incidence and
management of Mirizzi syndrome during laparoscopic chole-
cystectomy. Surg Endosc 17:1186–1190
20. Yeh C-N, Jan Y-Y, Chen M-F (2003) Laparoscopic treatment for
Mirizzi syndrome. Surg Endosc 17:1573–1578
21. Rohatgi A, Singh KK (2006) Mirizzi syndrome: laparoscopic man-
agement by subtotal cholecystectomy. Surg Endosc 20:1477–1481
22. Kwon A-H, Inui H (2007) Preoperative diagnosis and efficacy of
laparoscopic procedures in the treatment of Mirizzi syndrome. J
Am Coll Surg 204:409–415
23. Freitas ML, Bell RL, Duffy AJ (2006) Choledocholithiasis:
evolving standards for diagnosis and management. World J Gas-
troenterol 12:3162–3167
24. Memel DS, Balfe DM, Semelka RC et al (1998) The biliary tract.
In: Lee JKT, Sagel SS, Stanley RJ (eds) Computed body tomog-
raphy with MRI correlation, 3rd edn. Lippincot-Raven, Philadel-
phia, pp 779–884
25. Curet MJ, Rosendale DE, Congilosi S (1994) Mirizzi syndrome
in a native American population. Am J Surg 168:616–621
26. Wei Q, Shen L-G, Zheng H-M (2005) Hand assisted laparoscopic
surgery for complex gallstone disease: a report of five cases.
World J Gastroenterol 11:3311–3314
27. Safioleas M, Stamatakos M, Safioleas P, Smyrnis A, Revenas C,
Safioleas C (2008) Mirizzi syndrome: an unexpected problem of
cholelithiasis. Our experience with 27 cases. Int Semin Surg
Oncol 5:12
28. Rao PS, Tandon RK, Kapur BM (1988) Biliobiliary fistula:
review of nine cases. Am J Gastroenterol 83:652–657
29. Desai DC, Smink RD (1997) Mirizzi syndrome type II: is lapa-
roscopic cholecystectomy justified? JSLS 1:237–239
Surg Endosc (2010) 24:33–39 39
123