Embed Size (px)
Citation preview

KUMC CLINICAL CULTURE AND DIVERSITY SERIES
UNIVERSITY OF KANSASAPRIL 21, 2015
Religion and Culture

Objectives
1. What is culture?2. What is cultural competence3. Where does religion come in?4. What are some important things to think
about?5. What are some important things to do?

What is culture?
a : the integrated pattern of human knowledge, belief, and behavior that depends upon the capacity for learning and transmitting knowledge to succeeding generations
b : the customary beliefs, social forms, and material traits of a racial, religious, or social group; also : the characteristic features of everyday existence shared by people in a place or time <popular culture> <southern culture>
c : the set of values, conventions or social practices associated with a particular field, activity, or societal characteristic <studying the effect of computers on print culture> <changing the culture of materialism will take time — Peggy O'Mara>

Defining “culture”
Everything we do in our normal, day-to-day life that feel so natural that we forget them

2-x-2 differences
In groups of 2 for 5 minutes: identify as many characteristics or experiences you have in common and which are different?

2-x-2 differences
In groups of 2 for 5 minutes: identify as many characteristics or experiences you have in common and which are different?
In Larger group: What was easy to talk about? What surprised you? What was hard to talk about?

Belief Structure: Religion
Religion typically does three things:1. It confirms to us the role of “the gods” (pc-
speak: the ‘elemental forces at work in the universe’) and helps us understand how the universe and nature work (ontology).
2. It provides important stories that help us understand how to live as individuals and communities (morality).
3. It provides rituals (such as prayer and worship) intended to ask the gods to intervene on our behalf, including in matters of health and well-being (hope).

Western Two-Tiered Cosmology
Religion & Personal beliefs
Science & Fact
FaithMoral ProblemsSacred-Personal
Sight and ExperienceNatural OrderThis-Worldly ProblemsSecular-Public
Excluded Middle
Non-western cosmologies often assert that there is a parallel universe peopled by spirits
Seee http://rationalrevolution.net/articles/history_of_the_separation_of_chu.htmi).
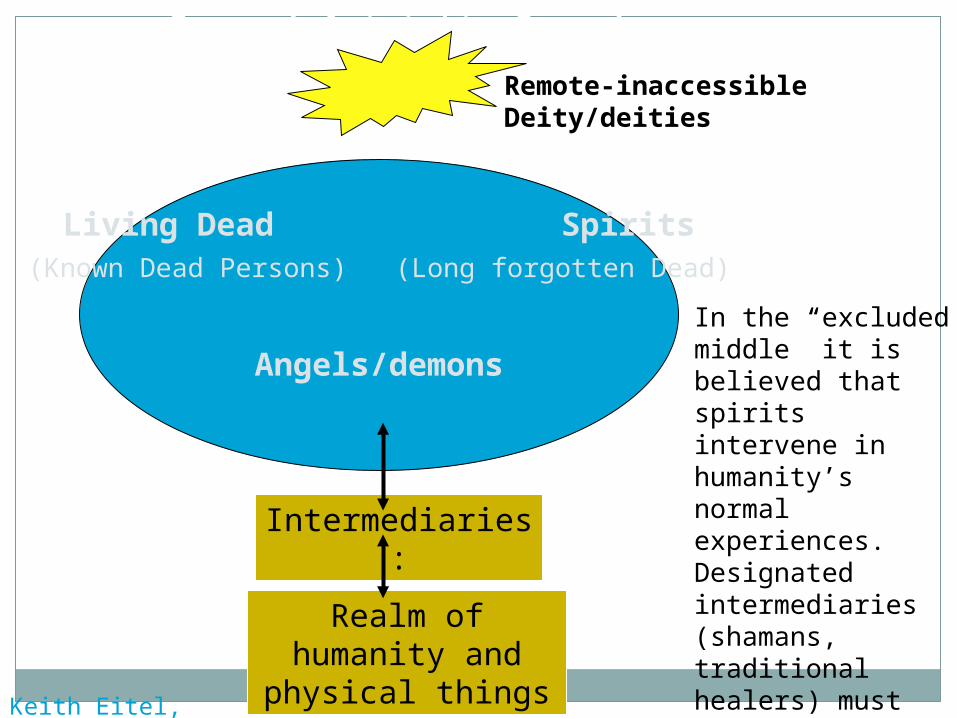
General Animistic Cosmology
Remote-inaccessible Deity/deities
Living Dead Spirits(Known Dead Persons) (Long forgotten Dead)
Angels/demons
Intermediaries:
Realm of humanity and physical things
In the “excluded middle” it is believed that spirits intervene in humanity’s normal experiences. Designated intermediaries (shamans, traditional healers) must appease these forces to heal/sustain life.Keith Eitel, Missiology
Cultural Competence Definition
Cultural Competence – Definition
A set of congruent behaviors, practices, attitudes and policies that come together in a system or agency or among professionals, enabling effective work to be done in cross-cultural situations

Cultural Competence Definition
Cultural Competence – What it isn’t:An in-depth study of a number of common cultures
you may encounter in practice, their characteristics, cultural health practices and beliefs and how to best approach them
“Culturalism” Assuming that, because we know about cultural
beliefs and practices, we are fully-prepared to intervene.
Knowledge without self-discovery may lead to even more bias, stereotyping and discrimination.

Patient Safety and Healthcare Quality: what can go wrong in LEP populations
Among 1,083 adverse incident reports from six Joint Commission-accredited hospitals for English speaking vs. LEP (Limited English Patients) over 7 months in 2005: A greater percentage of LEP patients (49%)
experienced physical harm versus English-speaking patients (30%).
LEP patients also experienced higher levels of physical harm ranging from moderate temporary harm to death, 47% and 24% respectively.
Divi C, Koss RG, Schmaltz SP, Loeb JM. Language proficiency and adverse events in US hospitals: a pilot study. Int J Qual Health Care. Apr 2007;19(2):60-67

The Cultural Competence Continuum

Cultural Destructiveness
Examples Genocide or Ethnocide Exclusion Laws Shun/Avoid certain curriculum topics “We know it when we see it”
“When we redistrict we can get rid of THAT neighborhood!”
“If we could get rid of the special needs students, our scoreswould improve.”
Using one’s power to eliminate the culture of another.
“See the difference; stomp it out.”
Cultural Blindness
Examples Discomfort in noting difference Beliefs/actions that assume world is fair and achievement is based on merit
“Our school does not need to focus on multicultural education- we have no diversity.”
“Everyone learns the same.”
“We have nothing against their religion, we just don’t know anything about it so we ignore it, because we don’t want to offend.”
“I’m not prejudiced. I don’t see color in my students.”
Acting as if cultural differences do not matter or as if there are not differences among/between cultures.
“See the difference; act like you don’t.”

Cultural Proficiency
Five essential elements:
1. Assessing culture
2. Valuing Diversity
3. Managing the Dynamics of Difference
4. Adapting to Diversity
5. Institutionalizing Cultural KnowledgeExamples Interdependence Personal change and transformation Developing alliances with groups other than one’s own
Esteem culture; knowing how to learn about organizational culture; interacting effectively in a variety of cultural groups.
“See the difference; respond positively. Engage and adapt.”

Cultural Proficiency
Esteem culture; knowing how to learn about organizational culture; interacting effectively in a variety of cultural groups.
“See the difference; respond positively. Engage and adapt.”

Does it matter what you think about the Excluded Middle?
We each have beliefs about ‘what is out there’.
If we believe that what we think is “true” and the other person is “uneducated” (or other label) unconscious biases are communicated (feeling).
It may be useful to think about what we might say or do if they ask.
I don’t know is an OK response. “I believe this and so should you” probably is
not. Our role is as “professional helpers” and that
requires being respectful, genuine and beneficent. “Primum non nocere”

Kleinman’s Nine Questions
One assessment tool for clinicians to better understand patients
Developed by Arthur Kleinman, MD, MA, a physician and anthropologist
“Culture, Illness and Care: Clinical Lessons from Anthropologic and Cross-Cultural Research,” Annals of Internal Medicine, 1978
Reference: http://depts.washington.edu/fammed/predoc/clerkship/resources/cultKlein
Kleinman’s Questions
1. What do you think has caused your problem?2. Why do you think it started when it did?3. What does your sickness do to you; how does it work? 4. How severe is your sickness? 5. Will it have a short or long duration? 6. What kind of treatment should you receive? 7. What are the most important results you hope to receive from this treatment? 8. What are the chief problems your sickness has caused you? 9. What you do you fear about your sickness?

Story of Bhutanese refugee community
150,000 (20% of Bhutan’s population), Nepali-speaking majority language
1989: Minority ruling-elite outlawed Nepali language and dress
1990-94 Dissent quashed, lands-finances seized, rape-torture-murder, followed by mass exodus and 18 years in Nepali refugee camps Gross National Happiness and ethnic cleansing: read
Thapa 2011 http://www.wavemag.com.np/issue/article3775.html

Story of Bhutanese Refugee community
UNHCR unable to secure repatriationUS agrees to give asylum to 60,000 by
Dec. 2013 (~50,000 have arrived)3 months of re-settlement assistance8 months of Medicaid then medical
indigence if un-employed (exceptions for families with children and some medically disabled)



Learn to anticipate the un-expected
Source: Doug Hall, “The Cat and the Toaster”

Lessons learned by 1 provider
1. Every person is different/thinks differently: generalizations don’t help
2. I am the one who needs to learn the most3. Relationships and mutual understanding
takes time to develop.4. Every community and person has a path
that is unique, and worthy to celebrate5. It will not “just happen”: it is important to
be intentional, “learning to learn well”


Getting there is half the fun…

A grid to think about your growth
Your practic
e
Partners
System
Community
Knowledge
Attitude
SkillsClinical Behavior





























