Embed Size (px)
Citation preview

INTRODUCTION
The knee joint is a common site for sports injuries,particularly ligamentous injuries, because ligaments con-tribute a great deal to knee joint stability. A solidknowledge of knee anatomy and biomechanics isnecessary to properly assess the injury and devise arehabilitation program that creates the best environmentfor healing. Criterion-based rehabilitation protocols areused because they outline milestones that must be metfor progression, eliminating subjectivity. The rate ofprogression can differ between athletes and is dependenton the individual rate of healing and the demands of theathlete’s activity level. Within each phase of the protocol,clinicians must choose therapeutic exercises that gra-dually introduce stresses to the healing tissue and thatare tailored to preparing the athlete to return to thedemands of the sport. Only after completing all phases ofrehabilitation and meeting functional testing criteria areathletes allowed to return to sport activities.
ANATOMY AND BIOMECHANICS
BONY STRUCTURE
The tibiofemoral joint is created by the interface of thedistal femur and proximal tibia. The distal femur ischaracterized by two bony prominences, the medial andlateral condyles, which are separated by an intercondylarnotch. Both condyles are rounded inferiorly and projectposteriorly, but the medial femoral condylar projection islonger. The longer projection of the medial femoralcondyle partially dictates the biomechanics of the kneejoint. The greater surface area of the medial condylerequires greater accessory motion in the medial half ofthe knee in comparison to the lateral half. Thus, when theknee is flexed, the tibiofemoral joint undergoes a small
CHAPTER CONTENTS
Introduction 379
Anatomy and biomechanics 379Bony structure 379Ligaments 380Menisci 381
Knee examination 381General guidelines 381Ligament testing 382
Medial collateral ligament 382Posterior oblique ligament 382Lateral collateral ligament 382Anterior cruciate ligament 383Posterior cruciate ligament 383Arcuate complex 384
Meniscal tests 384Effusion 384Special topics related to knee evaluation 385
Arthrometer testing 385Quadriceps strength testing 385Hop testing 386Self-report questionnaires 386
Rehabilitation of common sports-related injuries 386General rehabilitation guidelines 386Phases of rehabilitation 386
Acute phase 386Advanced phase 387Return-to-play phase 388
Anterior cruciate ligament 388Mechanism of injury 388Non-operative treatment 388Operative treatment 389Postoperative treatment 390
Medical collateral ligament 390Mechanism of injury 390Non-operative treatment 390Operative treatment 390Postoperative treatment 390
Menisci 391Mechanism of injury 391Non-operative treatment 391Operative treatment 391Postoperative treatment 391
Rehabilitation of less common injuries 391Posterior cruciate ligament and posterolateral corner injuries
391Mechanism of injury 391Non-operative treatment 392Operative treatment 392Postoperative treatment 392
Tibial plateau fracture 393Mechanism of injury 393Non-operative treatment 393Operative treatment 394Postoperative treatment 394
Arthritis and the athlete 394Non-operative treatment for osteoarthritis 394Operative treatment 395Postoperative treatment 395
Summary 396
379
20
KneeTerese L Chmielewski Ryan L MiznerWilliam Padamonsky II Lynn Snyder-Mackler
F07154-20.qxd 3/9/02 1:28 PM Page 379

but significant amount of internal rotation to sustaincongruency between the condyles. When the kneeapproaches full extension, the tibiofemoral joint under-goes a subsequent external rotation, as the medial aspectof the knee must exhibit greater motion to maintain jointcongruency.
When viewed from above, the proximal tibia appearsflattened with a raised central region that divides thesurface into medial and lateral components. The centralregion is known as the intercondylar region, or tibialeminence, and serves as a ligamentous attachment site.The tibial eminence protrudes into the correspondingintercondylar notch of the femur. On either side of thetibial eminence lie the medial and lateral tibial plateaus.The tibial plateaus articulate with their respectivefemoral condyles.
Surrounding the tibiofemoral joint is a joint capsule,which runs along the femoral condyles proximally andattaches distally around the circumference of the tibia.The joint capsule travels more superiorly on the anterioraspect of the femur and much closer to the joint line as itmoves posteriorly. The capsule is deficient posteriorly atthe lateral femoral condyle to allow passage of thepopliteus tendon. The knee joint capsule is lined with asynovial membrane that surrounds, but does notencompass, the cruciate ligaments. The superior projec-tion of the synovial membrane, anteriorly, is called thesuprapatellar pouch. On the posterior aspect of the knee,the synovium projection is not as extensive, as it isdictated by the capsular insertion closer to the joint line.
Slightly distal to the lateral aspect of the tibial plateauis the proximal tibiofibular joint, composed of the fibularhead and the fibular notch located on the lateral tibia.This articulation is mentioned here due to its proximity tothe tibiofemoral joint. The tibiofibular joint has its ownjoint capsule and is not continuous with the tibiofemoraljoint.
LIGAMENTS
Ligaments of the tibiofemoral joint serve to providestructural stability and to guide knee motion. Theligaments can be subclassified as capsular, intracapsular,and extracapsular, based on the relationship of theligament to the joint capsule. Capsular ligaments aredistinct thickenings of the joint capsule, intracapsularligaments are located within the joint capsule, and extra-capsular ligaments are located outside of the jointcapsule. The medial collateral ligament (MCL), posterioroblique ligament (POL), and arcuate ligament are allcapsular ligaments of the tibiofemoral joint. The lateralcollateral ligament (LCL) is a capsular ligament at itssuperior end; however, distally it is extracapsular. Theanterior cruciate ligament (ACL), posterior cruciate
ligament (PCL), and meniscofemoral ligaments are allintracapsular ligaments.
The MCL is located on the medial aspect of the kneeand is composed of both superficial and deep fibers (Fig. 20.1). The superficial fibers of the MCL extend fromthe medial femoral condyle, anterior to the adductortubercle, to the anteromedial aspect of the tibial plateau.The deep fibers of the MCL travel from the same origin toinsert onto the medial meniscus. On the posteromedialaspect of the knee lies the POL, which originates from theadductor tubercle and inserts onto the posterior aspect ofthe capsule.
On the lateral side of the knee joint, the LCL coursesbetween the lateral femoral condyle to the fibular head(Fig. 20.1). The arcuate ligament arises from the posteriorfibular head and spans the posterolateral aspect of theknee, inserting on the intercondylar region of the tibiaand the posterior region of the lateral femoral condyle(Fig. 20.2). The LCL, the arcuate ligament, the popliteustendon, and the lateral head of the gastrocnemius arecollectively considered the arcuate complex.
The ACL originates on the posteromedial aspect of thelateral femoral condyle and inserts on the tibial ridge ofthe tibial plateau (Fig. 20.1). The ACL is composed offascicles that can be divided into two bundles: ananteromedial bundle and a posterolateral bundle. Thesignificance of the bundles is that they each are taut indifferent portions of the range of motion, allowingtension to be produced in the ACL throughout the fullrange. The posterolateral bundle is taut when the knee isextended, whereas the anteromedial bundle becomestight as the knee is flexed.
The PCL has a more vertical orientation, originating onthe medial aspect of the intercondylar notch andinserting on the tibial ridge of the tibial plateau, justposterior to the ACL (Fig. 20.1). The PCL is comprised oftwo bundles, an anterolateral bundle and a postero-
380 REGIONAL SPORT AND EXERCISE INJURY MANAGEMENT
Posteriorcruciateligament
Anteriorcruciateligament
Medialmeniscus
Patellarsurface
Popliteustendon
Lateralmeniscus
Lateralcollateralligament
Medialcollateralligament
Patellarligament
Figure 20.1 Anterior view of the knee with the patella removed.
F07154-20.qxd 3/9/02 1:28 PM Page 380

medial bundle. Similar to the ACL, the bundles are tightin reciprocal fashion. The anterolateral bundle becomestight when the knee is flexed, and the posteromedialbundle is tight with knee extension.
The meniscofemoral ligaments, the ligament ofHumphries and the ligament of Wrisberg, are accessoryligaments that surround and augment the PCL (Heller &Langman 1964). These ligaments are variably present;however, at least one ligament has been found in70–100% of knees (Girgis et al 1975, Heller & Langman1964). When present, these ligaments are located in theintercondylar notch, forming an attachment between theposterior horn of the lateral meniscus and the lateralborder of the medial femoral condyle. The ligament ofHumphries is located anterior to PCL, and the ligamentof Wrisberg is located posteriorly.
MENISCI
The menisci, located on the surface of the tibial plateaus(Fig. 20.1), are vascularized by the genicular arteries atbirth; however, this vascularity recedes with increasingage until only the peripheral 10–30% is vascularized(Arnoczky & Warren 1982, Clark & Ogden 1983). Themenisci are slightly concave superiorly, increasing thecongruity between the tibia and femur interface, andcreating a greater contact area for distribution of load.The menisci further assist in load transmission throughtheir compression.
The amount of movement during knee motion differsbetween the medial and lateral menisci. Both menisci aresecured to the anterior tibial plateau through attachmentscalled coronary ligaments. The medial meniscus,however, has firm attachments through extensions of thejoint capsule, whereas the capsular attachments to thelateral meniscus are less firm. Consequently, the medialmeniscus translates about 2–5 mm on the tibial plateauduring knee motion, and the lateral meniscus about 9–11mm (Fu & Baratz 1994).
Femoral contact on the menisci changes during kneemotion. With increasing knee flexion, there is greatercontact on the posterior part, or posterior horn, of themensici. Conversely, as the knee moves into extension,the femur contacts the anterior aspect, or anterior horn(Fu & Baratz 1994).
KNEE EXAMINATION
GENERAL GUIDELINES
Every knee examination begins with a patient interviewduring which information is gathered about themechanism of injury and the location and severity ofpain. The patient interview assists the clinician ingenerating a hypothesis about which structure has beeninjured. This hypothesis guides the examination, helpingthe examiner avoid superfluous testing and in thedevelopment an examination sequence. Tests that mayprovoke pain in the structure that is hypothesized to beinjured are typically performed near the end of theevaluation, since pain can cause muscle guarding whichin turn, can confound the results of subsequent testingprocedures.
In most sport injury evaluations, three basic principlescan be used to improve the accuracy and validity of thephysical examination. First, the patient should bepositioned comfortably during the examination. If thepatient is not relaxed, muscle contraction may obviateproper technique during testing maneuvers. Second, theknee examination tests should be performed on thecontralateral side before testing the injured side. Testingthe contralateral side first reveals the amount of normallaxity inherent to the individual, to form a baselineagainst which the injured side can be compared. Also,patients are more likely to be relaxed when they knowwhat to expect during testing. Finally, examination testsmust isolate a structure to conclusively test the integrityof the structure. Structures that contribute the majority ofthe restraint against a force in a given direction are calledprimary restraints. Secondary restraints are structuresthat contribute less to counteracting forces in a specificdirection or structures that become a more significant
KNEE 381
Medial head ofgastrocnemius
muscle Lateral head ofgastrocnemius
muscle
Arcuate poplitealligament
Fibular collateralligament
Popliteus muscle
Posterior ligamentof head of fibula
Figure 20.2 Posterior view of the knee.
F07154-20.qxd 3/9/02 1:28 PM Page 381

restraint only after the primary restraint is injured. Themost sensitive examination procedure is one in which thetested structure is the primary restraint.
Many knee examination tests are designed to assess theintegrity of a ligament. A positive ligamentous test isindicated either by pain in the ligament when force isapplied, or an increase in laxity compared to theuninjured side. The examiner may also evaluate ligamentintegrity by the quality of the end feel in comparison tothe other side.
Grading scales are often used to allow clinicians tocommunicate information about the severity of ligamentcompromise. A scale that assigns a grade based on theamount of laxity during testing is grade 1+ = 0–5 mm,grade 2+ = 5–10 mm, and grade 3+ = 10–15 mm(Hughston & Andrews 1976). The principle considerationconcerning grading scales is that clinicians that worktogether must use a common scale to ensure clearcommunication.
LIGAMENT TESTING
Medial collateral ligament
The medial collateral ligament (MCL) is best suited toprotect the knee against valgus forces because of itslocation on the medial side of the knee. When the knee isin full extension, the superficial and deep portions of theMCL share the role of primary restraint against valgusstress (Grood et al 1981, Inoue et al 1987). With the kneein 30° of flexion, the superficial portion of the MCL, theportion most commonly injured, is the primary restraint.
To perform a valgus stress test, the patient is posi-tioned supine with the leg to be tested near the edge ofthe examining table (Fig. 20.3). The examiner faces thepatient, supporting the lateral aspect of the distal femurand the medial aspect of the distal tibia, with the knee
joint in approximately 30° of flexion. The distal femur isheld in position while a laterally directed force is appliedto the distal tibia, producing a valgus force at the kneejoint.
Posterior oblique ligament
The posterior oblique ligament (POL) contributes toresisting valgus stress when the knee is extended, andbecomes slack when the knee is in 30° of flexion (Groodet al 1981). External rotation of the tibia moves the POLfrom a posteromedial position to nearly a pure medialarrangement. Once the POL is in this medial position,applying a valgus stress with the knee in extension cantest POL integrity.
Lateral collateral ligament
The lateral collateral ligament (LCL) is well suited toresist varus forces at the knee secondary to its laterallocation. At full knee extension, the LCL shares theprotective role with the arcuate complex (Gollehon et al1987, Grood et al 1981), however as the knee becomesmore flexed, the LCL becomes a primary restraint (Groodet al 1981).
For varus stress testing, the patient is positionedsupine, with the test leg close to the edge of the table(McGee 1992). The examiner faces the patient andabducts the leg to allow the examiner to stand betweenthe edge of the table and the test leg (Fig. 20.4). The distalfemur is supported medially, and the distal tibia issupported laterally, with the knee flexed to approximately30°. While firmly stabilizing the femur, the examinerapplies a medially directed force to the distal tibia toproduce varus force at the knee joint. An alternate way toperform this test, in order to improve femur stabilization,is to hold the distal femur against the edge of the table
382 REGIONAL SPORT AND EXERCISE INJURY MANAGEMENT
Figure 20.3 Valgus stress test for the knee. Figure 20.4 Varus stress test for the knee.
F07154-20.qxd 3/9/02 1:28 PM Page 382

while applying the force at the distal tibia, using the edgeof the table as a fulcrum to cause a varus stress at theknee joint.
Anterior cruciate ligament
The anterior cruciate ligament (ACL) is the primaryrestraint against anterior displacement of the tibia on thefemur. With the knee flexed to 30°, the ACL provides 87%of the restraint against anterior displacement (Butler et al1980). In addition, the ACL acts as a secondary restraintfor valgus stress at full extension (Inoue et al 1987,Markolf et al 1990).
Many tests have been described to test the integrity ofthe ACL. The Lachman test has been found to be bothsensitive and specific for testing the ACL (Liu et al 1995).To perform a Lachman test, the patient is positionedsupine (McGee 1992). The examiner stands facing thepatient, supporting the lateral aspect of the distal femurand grasping the medial aspect of the proximal tibia,keeping the knee flexed to approximately 20° (Fig. 20.5).The examiner then pulls the proximal tibia anteriorly,keeping the femur stabilized. If the femur is adequatelystabilized, the applied stress will not be localized to theknee. The examiner should also palpate the hamstringswhile stabilizing the femur, to ensure that the anteriorpull is not being impaired by hamstring contraction.
Another test to assess injury to the ACL is the pivotshift test (Galway et al 1972). This test reproduces the‘giving way’ sensation of the knee; therefore patientrelaxation is problematic. A greater percentage of positiveresults in ACL deficient knees are obtained during testingunder anesthesia (Donaldson et al 1985). To perform apivot shift test, the examiner holds the patient’s lower legwith one hand and applies a valgus stress at the lateralaspect of the knee joint with the other hand while the
patient’s knee is in a fully extended position (Fig. 20.6). Inthis position, the valgus force produces a rotationalsubluxation of the lateral tibia. The examiner then movesthe knee into approximately 30° of flexion, maintainingthe valgus stress at the knee joint. A positive pivot shifttest will be perceived as a ‘sliding’ motion of the tibia asthe knee reaches approximately 20–30° of flexion, whichis actually a reduction of the tibia. The tibial reduction iscaused by the pull of the iliotibial band, which becomes aknee flexor at approximately 20° of flexion.
Posterior cruciate ligament
The posterior cruciate ligament (PCL) is the primaryrestraint to posterior displacement of the tibia on thefemur (Fukubayashi et al 1982, Gollehon et al 1987), thusmost examination tests involve the measurement ofposterior laxity. The PCL additionally acts as a secondaryrestraint to varus stress at 0° and 30° knee flexion(Gollehon et al 1987).
Injury to the PCL can be assessed by many tests. Onetest is called the posterior drawer (Veltri & Warren 1993).To perform the posterior drawer test, the patient ispositioned supine with the knee flexed to 90° (Fig. 20.7)The examiner grasps the proximal tibia with both hands,with the thumbs on the anterior aspect of the tibia, andapplies a posteriorly directed force. Position of the tibialcondyles and the amount of laxity are compared to theuninjured side.
KNEE 383
Figure 20.5 Lachman test for the anterior cruciate ligament of theknee.
Figure 20.6 Pivot shift test for the anterior cruciate ligament of theknee.
F07154-20.qxd 3/9/02 1:28 PM Page 383

Another useful test is the posterior sag test (Veltri &Warren 1993). For this test, the patient is positionedsupine while the examiner passively flexes the hips andknees to 90°. To maintain the 90–90 position, the examinereither cradles the distal tibia or places the patient’s foot on a chair of appropriate height. If the tibial tubercleon the injured side is less prominent than the tibialtubercle on the uninvolved side, the test is consideredpositive. The ‘sag’, or posterior displacement, of the tibia during this test is a consequence of gravitationalpull.
The third test commonly used to assess PCL integrity isthe quadriceps active test (Veltri & Warren 1993). Thepatient is positioned supine with the knee flexed toapproximately 90°. The examiner stabilizes the patient’sfoot on the examining table and instructs the patient totry to extend the knee. This will result in an isometriccontraction of the quadriceps. If there is PCL compro-mise, the posteriorly subluxed tibia will be drawnanteriorly by the quadriceps, causing the tibial tubercle tobecome more prominent.
Arcuate complex
The arcuate complex is the primary restraint to externalrotation of the tibia (Gollehon et al 1987). The arcuatecomplex is tested by the prone external rotation test withthe knee at 30° of flexion (Veltri & Warren 1993). The testis performed with the patient prone (Fig. 20.8). Bothknees are flexed to 30° by the examiner and the feet areexternally rotated, causing tibial external rotation.External rotation of the foot relative to the thigh iscompared between the injured and uninjured legs. Anincrease in the amount of external rotation by 10° or morecompared to the uninjured side is considered a positivetest (Veltri & Warren 1993).
MENISCAL TESTS
Meniscal tears are difficult to diagnose by physicalexamination. McMurray’s test is commonly used todiagnose meniscal tears and is performed by fully flexingthe patient’s injured knee, then grasping the foot androtating the tibia on the femur while the knee remainsflexed (Corea et al 1994). Although McMurray’s test iscommonly used, the sensitivity of the test is only 59%(Corea et al 1994). Clinicians should have a high index ofsuspicion for a meniscal tear when symptoms of joint linetenderness, clicking in the knee, and knee locking arepresent (Anderson & Lipscomb 1986, Shakespeare &Rigby 1983).
EFFUSION
Assessing knee effusion allows the clinician to monitorthe patient’s recovery after injury and the patient’sresponse to treatment progression. Girth measurementsdo not adequately quantify effusion, particularly if theeffusion is small. Instead, the stroke test can give moremeaningful information about the presence and amountof effusion (McGee 1992). The stroke test is performedwith the patient supine and the knee relaxed in fullextension. The test starts with the examiner performingseveral strokes upward from the medial joint linetowards the suprapatellar pouch in an attempt to moveeffusion from the medial aspect of the knee. Theexaminer then strokes downward on the lateral side ofthe knee from the suprapatellar pouch towards the lateraljoint line, observing the medial aspect of the knee in aneffort to appreciate a fluid wave emanating from thesuprapatellar pouch (McGee 1992). At our facility, we use
384 REGIONAL SPORT AND EXERCISE INJURY MANAGEMENT
Figure 20.7 Posterior drawer test for the posterior cruciate ligamentof the knee.
Figure 20.8 Prone external rotation test for the arcuate complex.
F07154-20.qxd 3/9/02 1:28 PM Page 384

four different grades to describe the amount of effusion.If no wave is produced with the downward stroke, thereis no effusion present. If the downward stroke producesa small wave on the medial side of the knee, the effusionis given a ‘trace’ grade; a larger bulge is given a ‘1+’grade. If the effusion returns to the medial side of theknee without a downward stroke, the effusion is given a‘2+’ grade. The inability to move the effusion out of themedial aspect of the knee equates to a ‘3+’ grade.
SPECIAL TOPICS RELATED TO KNEEEVALUATION
Arthrometer testing
Arthrometer testing is most often used to quantify kneejoint laxity when ACL injury is suspected. Many differentknee arthrometers have been developed, however, resultsobtained with these different systems are not necessarilygeneralizable to each other (Anderson et al 1992). The KT1000 arthrometer (Medmetrics, San Diego, CA, USA) is acommonly used arthometer. Results using KT 1000 witha manual maximum pull have shown a 3 mm differencebetween sides to be greater than 90% sensitive for anACL rupture (Liu et al 1995, Rangger et al 1993).
Quadriceps strength testing
Quadriceps weakness is a common sequela after a kneeinjury, therefore measurement of quadriceps strength isimportant to ensure full resolution of this impairmentprior to return to sport. Biomechanical studies have
demonstrated that a quadriceps strength deficit iscorrelated with altered gait (Snyder-Mackler et al 1995).
A variety of methods can be used to test quadricepsstrength. The two most common methods used in theclinical setting are manual muscle testing and isokinetictesting. Manual muscle testing is one of the easiest toemploy; however, results are less accurate when a patientis able to generate high force or when the strength dif-ference between limbs is minimal. Isokinetic testingoffers the benefit of objective measurement through aforce transducer, but there is controversy about which isthe most clinically significant testing speed. Faster speedsbetter approximate speed of joint motion duringfunction; however, they underestimate strength deficits(Gapeyeva et al 2000, Keays et al 2000).
Neither manual muscle testing nor isokinetic testingmeasure the patient’s effort or offer a method forquadriceps inhibition (inability to fully activate thequadriceps voluntarily). Quadriceps can be inhibitedafter knee injury (Snyder-Mackler et al 1994). The burst-superimposition method of testing quadriceps strength isnot used as commonly in the clinical setting as in researchstudies, but this method offers the ability to measureinhibition (Snyder-Mackler et al 1994). For this type oftesting, an electrical stimulus is administered (super-imposed) while the patient produces a maximal voluntaryisometric contraction. If the patient has fully activated thequadriceps, there will be no force augmentation when theelectrical stimulus is delivered. If the burst-super-imposition method of testing is not available to theclinician, targets should be set and verbal encouragementgiven during testing to improve quality of effort.
KNEE 385
Tota
l dis
tanc
e
Tota
l dis
tanc
e
A 6 meters B 6 meters C 6 meters
Tota
l dis
tanc
e
D 6 meters
Figure 20.9 Hop tests for the knee. A: Single hop for distance.B: Timed hop. C: Triple hop for distance. D: Cross-over hop for distance.
F07154-20.qxd 3/9/02 1:28 PM Page 385

Hop testing
Hop testing is a commonly used clinical test of function.Many clinics use one or all of the hop tests described byNoyes et al (1991), which include: the single hop test,triple hop test, cross-over triple hop test and timed hoptest (Fig. 20.9). Testing in an uninjured populationshowed that 92–93% had a symmetry index (side-to-sidecomparison) of at least 85% for the single hop and timedhop tests (Barber et al 1990); thus a score less than 85% onthe hop tests can be indicative of disability. Hop testinghas been shown to have good reliability, particularlywhen patients are given more than one practice trial(Bolgla & Keskula 1997).
Self-report questionnaires
Self-report questionnaires can assist the clinician inmeasuring disability and monitoring changes in functionalstatus during the course of treatment. The knee-specific(e.g. Lysholm Scale [Lysholm & Gillquist 1982], CincinnatiKnee Rating Scale [Noyes et al 1989]) and general healthstatus questionnaires (e.g. SF-36 [Ware & Shelbourne1992]), both provide important, but very differentinformation. Knee-specific questionnaires give insightinto disability caused by the knee injury, whereas generalhealth status questionnaires reveal mental and emotionalstates that may impact on rehabilitation. Cliniciansshould select knee-specific questionnaires that includequestions related to high-level activities; otherwise, anathlete may reach the highest score even when somedisability remains. Furthermore, clinicians should checkthe literature to make sure the selected questionnaire hashigh reliability and is able to measure changes infunctional status.
REHABILITATION OF COMMON SPORTS-RELATED INJURIES
GENERAL REHABILITATION GUIDELINES
Rehabilitation guidelines are structured to direct theclinician in returning athletes to preinjury activity levelsas quickly and safely as possible. Guidelines should bebased upon current scientific evidence and have criteriafor progression in rehabilitation. Criterion-based proto-cols eliminate subjective progression through rehabilita-tion by dictating the milestones that must be reached inorder to progress to the next phase. The rate of pro-gression can differ between athletes and is dependent onthe individual rate of healing and the demands of theathlete’s activity level. Also, clinicians should prescribetherapeutic interventions within each phase that are
tailored to the patient’s needs. Prescribing therapeuticinterventions in a ‘cookbook’ fashion for each particulardiagnosis is committing a disservice to the patient.
PHASES OF REHABILITATION
Three phases of rehabilitation will be discussed: the acutephase, advanced phase, and return-to-play phase (Box 20.1). It should be noted that many variations onrehabilitation programs for knee injuries are possible andthat only some of these approaches are presented in thechapter.
Acute phase
In the acute phase of rehabilitation, strategies are focusedon controlling the effects of inflammation (pain, effusion,
386 REGIONAL SPORT AND EXERCISE INJURY MANAGEMENT
Box 20.1 Phases of rehabilitation
Acute phase
GoalsDecrease painIncrease range of movementRetard muscle atrophyUnassisted ambulation
Common interventionsCryotherapyNMESPatellar mobilizationSoft tissue mobilization at incision site (if surgical intervention)Isometric exercise (quadriceps sets)Range of motion exercisesGait trainingCardiovascular exercise (stationary bike, swimming)
Advanced phase
Criteria to enterFull range of motion and effusion controlled (below 2+)
GoalIncrease muscle strength and endurance
Common interventionsIsotonic (both open and closed chain) and isokinetic exerciseNMESProprioception exerciseFlexibility exerciseRunning programCardiovascular exercise (stationary bike, StairMaster, ellipticalmachine)
Return-to-play phase
Criteria to enterQuadriceps strength ≥80% of the uninjured side
GoalPrepare athlete for a return to competition
Common interventionsIsotonic (both open and closed chain) and isokinetic exerciseAgility trainingSport-specific exercise
F07154-20.qxd 3/9/02 1:28 PM Page 386

loss of motion, and muscle atrophy). The goal of the acutephase is to restore full range of motion, reduce effusion,retard muscle atrophy, and ambulate without an assistivedevice (Box 20.1). Ice, compression, and elevation of theinjured limb can assist in counteracting the effects ofinflammation. Relative rest is usually indicated to allowfor healing to occur without the detrimental effects ofstrict immobilization, such as arthrofibrosis anddeconditioning.
In the acute stage, ambulation with an assistive deviceis indicated if the athlete is unable to walk without alimp. A knee brace that limits tibiofemoral motion isoften used in conjunction with an assistive device tosafely allow increased weightbearing. Use of an assistivedevice is maintained until the athlete can walk without alimp, joint effusion has been controlled, and when thequadriceps have recovered sufficiently to provideprotection of healing tissues (typically 60% of theuninvolved side).
Range of motion deficits should also be resolved in thisportion of rehabilitation. Most often, regaining kneeextension is more difficult, so priority should be placedon achieving extension. The clinician should evaluate thenumerous possible sources contributing to a restrictedrange of motion including: decreased patella mobility,poor quadriceps recruitment, decreased quadricepsstrength, decreased accessory motion of the tibiofemoraljoint, and muscle guarding and tightness. Interventionsshould be chosen that address the specific cause ofrestricted range. A combination of low-load sustainedstretching, joint mobilizations of the patella and tibio-femoral joints, and modalities to control pain andresultant muscle spasm are commonly performedfollowing most injuries and surgeries.
Rapid and significant quadriceps femoris weakness isa common concern following injuries to the tibiofemoraljoint (Morrissey 1989, Nyland 1999, Snyder-Mackler et al1994). Efforts to retard atrophy and facilitate volitionalquadriceps activation form the basis of early progressivestrengthening programs (Snyder-Mackler et al 1991).Successful early quadriceps strengthening will facilitateefforts to gain full knee extension, restore normal patellarmobility, and correct antalgic gait patterns. Reciprocally,early emphasis on obtaining full knee extension duringweightbearing will assist in efforts to regain kneeextensor strength.
If the athlete is experiencing difficulty producing astrong quadriceps contraction, neuromuscular electricalstimulation (NMES) is indicated (see Ch. 13). Parametersfor NMES of athletes include: frequency of 50–75 Hz,wavelength of 200–400 µs, ramp time of 2 s, 10 s of ontime, 50 s of off time, and ten contractions during asession, 2–3 sessions a week. The success of NMESdepends upon achieving adequate levels of electrical
stimulation to provide stimulus to promote strengthgains. Patients are counseled to try and relax while theelectrically elicited isometric contractions are increased inan effort to achieve 50% of the injured leg’s maximalvolitional isometric contraction. Intensity levels that arebelow 50% of maximal voluntary isometric contraction(MVIC) have limited capacity to assist in strength gainbeyond volitional exercise alone. Use of this highintensity NMES is maintained until the involved limbachieves strength equal to 80% of the uninvolved side.
Advanced phase
The advanced phase of rehabilitation is initiated whenrange of motion is full and effusion controlled (belowgrade 2+) (Box 20.1). The goal of this phase is to increasemuscle strength and endurance. Higher intensityresistance training can be initiated and should includeexercises for all muscles of lower extremity. If theintensity of therapeutic exercise creates an increase ineffusion, intensity levels are reduced to the previouslevel. Progression to higher activity is dictated by thepresence of soreness after exercise (Box 20.2).
Rehabilitation exercises are commonly categorized asopen or closed chain exercises. Open chain exercises arethose in which the distal end is free to move (e.g. kneeextension), and closed chain exercises are those in whichthe distal end is fixed (e.g. squat). Optimal strengtheningrequires a combination of both open and closed chainexercises (Fitzgerald 1997, Mikkelson et al 2000,Morrissey et al 2000). When athletes perform closedchain exercises, clinicians should be cognizant of thetendency to compensate for weak muscles in the kineticchain. Reliance of the ankle plantar flexors and the hipextensors is a common substitution with closed chainexercises following knee injury.
Often, exercises designed to improve dynamic stabilityare added in this phase. Although there is no literature tosupport the inclusion of such exercises, there is atheoretical framework for including such exercises basedon basic science and applied research. Balance exercisesusing unstable surfaces and perturbation devices areincluded.
KNEE 387
Box 20.2 Exercise progression guidelines based on soreness
• If no soreness is present from previous exercise, progressexercise by modifying one variable.
• If soreness is present from previous exercise, but recedeswith warm-up, stay at same level.
• If soreness is present from previous exercise, but does notrecede with warm-up, decrease exercise to the level prior toprogression. Consider taking the day off if soreness is stillpresent with the reduced level of exercise. When exercise isresumed, it should be at the reduced level.
F07154-20.qxd 3/9/02 1:28 PM Page 387

Progression of aerobic condition often includes arunning program that is usually initiated in this phase ofrehabilitation. To start running, the athlete’s injured sidequadriceps strength must be restored to at least 80% ofthe uninvolved side, and sufficient healing of the injuredstructure must have occurred (e.g. ACL reconstructionapproximately 8 weeks, grade I MCL injury at 1–2weeks). Soft tissue healing is usually sufficient at 4–6weeks. Running progression starts on a treadmill andwill move to running on a track. Track workouts areinitiated with running the straight-a-ways and walkingcorners. The intensity is gradually increased until theathlete can run the full length of the track. Road runningand finally off-road running represent the least controlledtraining situations and are instituted as a final stage inrunning progression. Jogging duration may start with as much as 2 miles and may be progressed on a weeklybasis if there is no pain or swelling (Box 20.2).Completing a full running progression can take as long as2–3 month.
Return-to-play phase
The goal of the return-to-play phase is to prepare theathlete to return to the demands of competition (Box20.1). The athlete is allowed to enter this phase whenintense resistance training and a running program do notincrease effusion. Therapeutic exercise interventionsshould follow the SAID (Specific Adaptations to ImposedDemands) principle. This concept is based in the notionthat the body will adapt to accommodate to the stress andstrains applied to it. Therefore, exercises should attemptto mimick the demands of activities required for theathlete to successfully return to sport.
The return-to-play phase is characterized by agilitytraining and sport-specific exercise. Less complex agilitydrills (e.g. shuffle, shuttle run) should be used initially,moving to more complex agility drills (e.g. figure of 8,braiding). The volume of agility activities should begraded by frequency, duration, and intensity. Only onevariable should be modified at one time, otherwise it isdifficult to determine what was the factor that caused anadverse response (increased pain or effusion) to thetreatment. Sport-specific activities are introduced andprogressed in the same manner. Practice drills are started,leading to competition level activities.
Athletes are cleared to return to sport when they haveprogressed through all phases of rehabilitation withoutsymptoms and have met the criteria of return-to-playtesting. Return-to-play testing involves quadricepsstrength testing, hop testing and self-report question-naires. Athletes must score 90% on all tests beforereturning to competition (Manal & Snyder-Mackler1996).
ANTERIOR CRUCIATE LIGAMENT
Mechanism of injury
The ACL is injured when the tibia translates too faranteriorly relative to the femur. The majority of ACLinjuries (around 70%) occur by non-contact mechanisms;the remaining injuries involve contact (Boden et al 2000).Non-contact injuries typically involve a sharp decelera-tion with the knee close to extension, with or without achange in direction, or landing from a jump (Boden et al2000). Injury to the ACL can also occur when the knee ishyperextended, or when contact results in valguscollapse of the knee (Boden et al 2000).
Non-operative treatment
Most athletes with an ACL tear experience kneeinstability during sports that involve cutting or jumping(Shelton et al 1997). Non-operative treatment hasprimarily been reserved for those willing to reduce theiractivity level; however, non-operative treatment can be ashort-term option for athletes if certain conditions aremet. A screening examination has been developed toassess an athlete’s potential for dynamically stabilizingthe injured knee, to determine if an athlete is a goodcandidate for non-operative treatment. The screeningexamination is composed of a variety of clinical tests andis administered when there is no knee effusion present,full knee range of motion has been restored, and thepatient experiences no pain with unilateral hopping. Inorder to qualify for non-operative treatment, the athletemust: (1) have no more than one episode of giving way(i.e. buckling) since the initial injury, (2) score at least 80%on the timed hop test, (3) score at least 80% on the KneeOutcome Survey-Activities of Daily Living Scale (Irrganget al 1998), and (4) score at least 60% on the Global RatingScale (Fitzgerald et al 2000a). If the athlete meets thecriteria of the screening examination, then non-operativetreatment can be offered as a viable option, otherwisesurgical intervention is recommended. Non-operativetreatment should only be considered when there is noconcomitant ligamentous injury greater than grade I, norepairable meniscal tear, and no full-thickness articularcartilage defect.
Athletes who pass the criteria of the screeningexamination are enrolled in a ten session rehabilitationprogram that includes lower extremity strengtheningexercises, agility training, and perturbation training(Fitzgerald et al 2000b). In a randomized controlled trial,perturbation training augmented rehabilitation wascompared to a program consisting of only strengtheningexercises and agility training, and was found to result ingreater success in returning to sport without episodes ofgiving way (Fitzgerald et al 2000b). Perturbation training
388 REGIONAL SPORT AND EXERCISE INJURY MANAGEMENT
F07154-20.qxd 3/9/02 1:28 PM Page 388

involves the application of controlled forces to the lower extremity through support surface movement.Rockerboard, rollerboard, and rollerboard with astationary platform are used to apply the perturbationsduring this type of training (Figs 20.10–20.12). The force,direction and predictability of the perturbations areprogressed throughout the ten sessions. Athletes wear afunctional brace during agility training and when theyreturn to sport activity. This protocol is given as a short-
term option for athletes who wish to complete theircompetitive season; operative intervention is recom-mended when the competitive season is finished.
Operative treatment
Operative treatment should be considered for any athletewho wishes to return to sports that require cutting,jumping, and lateral movement. Athletes may benefitfrom preoperative rehabilitation to decrease inflamma-tion and improve knee motion. Surgery less than 1 monthfrom injury was found to be one of the factors related toa loss of motion following surgery (Harner et al 1992).
ACL reconstructions are performed with a variety ofgrafts. Typical autogenous graft choices include themiddle third of the patellar tendon or doubledsemitendinosis-gracilis tendons. Allograft choices includefresh frozen Achilles or patellar tendon.
Advances in surgical fixation allow for full weight-bearing and the ability to obtain full knee extension in theimmediate postoperative phase without concern for graftfailure. Considerable research has been conducted todetermine which exercises may impose harmful strain tothe ACL graft, thus contributing to graft stretching. Somestudies suggest that performing knee extension in arange from 0–40° may impose high strain on the ACL;however, other studies show that the amount of strainmay be comparable to that during weightbearing(Beynnon et al 1997, Escamilla et al 1998, Lutz et al 1993).Clinicians should, therefore, prescribe knee extensionexercises in a terminal range judiciously. It is important toremember that absence of strain can also be detrimental,
KNEE 389
Figure 20.10 Perturbation training for non-operative ACLrehabilitation (rockerboard technique).
Figure 20.11 Perturbation training for non-operative ACLrehabilitation (rollerboard technique).
Figure 20.12 Perturbation training for non-operative ACLrehabilitation (rollerboard with stationary platform technique).
F07154-20.qxd 3/9/02 1:28 PM Page 389

since strain is essential for graft remodeling. Unfortun-ately, the optimal strain level has not yet beendetermined.
Postoperative treatment
Immediately after surgery, patients may experiencedifficulty producing a quadriceps contraction, particu-larly if an autogenous patellar tendon graft was used. Aninability to produce a quadriceps contraction, coupledwith donor site healing, can lead to a restriction ofsuperior patellar mobility. Superior patellar mobilizationis therefore essential for these patients. Patients should bepositioned at 60° of knee flexion for NMES. By the secondweek after surgery, 90° of active knee flexion should beachieved, and by 6–8 weeks after surgery, the patientshould achieve full active range of motion (Manal &Snyder-Mackler 1996).
In the advanced phase of rehabilitation (6–12 weekspostoperatively), strengthening exercises should beprogressed. Approximately 8 weeks after surgery, arunning program can be initiated if the patient’s involvedside quadriceps strength is 80% of the uninvolved side(Manal & Snyder-Mackler 1996).
In the return-to-play phase (12–20 weeks post-operatively), athletes are allowed to gradually increasethe complexity and intensity of activities. Athletes areallowed to return to sport approximately 4–6 monthsafter surgery, provided they have met all clinical mile-stones and progressed through all phases of rehabilita-tion. The athlete should demonstrate quadriceps strengthand hop testing scores that are 90% of the uninjured sidebefore being cleared to return to sport (Manal & Snyder-Mackler 1996). A functional brace is typically prescribedfor a return to sport and is worn until the patient feelsconfident in the stability of the knee.
MEDIAL COLLATERAL LIGAMENT
Mechanism of injury
The majority of isolated MCL injuries involve lateralimpact to the lower thigh or upper leg (Indelicato 1995).Injury to the MCL can also occur in combination with anACL injury, and possibly a POL injury, when the knee issubjected to a large valgus force with external rotation(Indelicato 1995).
Non-operative treatment
Non-operative treatment is recommended for most MCLinjuries because the MCL has a rich blood supply andassociated high healing potential. Non-operativelymanaged, incomplete (grade I and II) MCL injuriestypically result in an unrestricted return to activity
(Derscheid & Garrick 1981, Holden et al 1983). Isolated,complete MCL ruptures can also have good outcomes,although the recovery time will be longer and greaterresidual laxity will remain (Indelicato et al 1990, Jones etal 1986).
The duration of the acute phase may be as brief as afew days for a grade I MCL sprain and as long as 4 weeksfor grade III MCL injuries. In the acute phase ofrehabilitation, valgus stress to the knee is avoided toallow initial healing of the MCL. Patients may complainof pain when the knee nears full extension because theMCL is in a lengthened position in extension. For grade IIand III MCL sprains, an immobilizer or brace thatprohibits knee extension past 30° may be used to reducepain and to decrease strain of the MCL. Often, an immo-bilizer is worn initially, then the athlete is progressed to abrace which restricts range of motion. Total duration ofmotion restriction is 1–4 weeks, dependent on theseverity of the sprain (Holden et al 1983, Indelicato 1983).Patients who are limited from full knee extension shouldbe encouraged to perform range of motion exercises in apain-free range, gradually working on increasing rangeof motion.
In the advanced phase of rehabilitation, valgus stressto the knee can gradually be introduced. Either side-stepping over cones or hip adduction exercises can beused to introduce valgus stress at the knee. Resistance forhip adduction exercises should initially be placedproximally on the tibia and move distally as the patient isable to tolerate and control a longer lever arm. If thepatient was limited from full knee extension in the acutephase, resistance in a terminal range should be pro-gressed gradually.
In the return-to-play phase, agility drills should beinitiated in the sagittal plane and progressed to thefrontal plane. Agility drills in the frontal plane, such asshuffles, braiding or side jumping, all increase valgusstress across the knee and should be progressed withcaution. Functional braces may be worn when the athletereturns to sport, but long-term use is discouraged(Indelicato 1995).
Operative treatment
Operative treatment is usually reserved for complete(grade III) ruptures of the MCL, or complete MCLruptures in combination with other ligamentous rup-tures. The operative procedure is usually primary repair.
Postoperative treatment
Postoperative treatment after MCL repair follows aprotocol similar to non-operative treatment of grade IIIMCL injuries, with the exception that attention must be
390 REGIONAL SPORT AND EXERCISE INJURY MANAGEMENT
F07154-20.qxd 3/9/02 1:28 PM Page 390

paid to incision site mobility. An immobilizer is typicallyworn for 2 weeks, and crutches are used for ambulation.Patient comfort and ability to meet clinical milestonesdictate progression to the next phase (Indelicato 1995).
MENISCI
Mechanism of injury
Meniscal tears can occur in isolation or in combinationwith a ligamentous injury. One mechanism for anisolated meniscal injury is pivoting, in which the femurrotates on the meniscus while the meniscus is com-pressed. Another mechanism for meniscal injury is risingfrom a squat. This results because weight is transferred tothe posterior horns with increasing knee flexion, then asthe athlete begins the ascent phase of the squat, themenisci are pushed forward while the posterior hornremains trapped.
Non-operative treatment
Non-operative treatment may be recommended for anisolated meniscal tear that is stable and non-sympto-matic. Rehabilitation is directed at resolving kneeimpairments, and progression is based on symptoms.
Operative treatment
Repair of the meniscus is always preferred to excision ordebridement; however, healing potential dictates whatprocedure is performed. The meniscal rim is vascularizedand has been termed the ‘red zone’; whereas the centralportion of the meniscus is devoid of vascularity and hasbeen termed the ‘white zone’ (DeHaven & Arnoczky1994). A tear in the white zone has poor healing potentialand is usually treated with debridement. Tears that occurin the red zone or the transition to the white zone(red–white zone) have greater healing potential and maybe treated with a repair, if deemed appropriate by thephysician.
Postoperative treatment
Postoperative rehabilitation depends on whether themeniscal tear was debrided or repaired. If the tear wastreated with debridement, progression is entirely basedon symptoms. There is little tissue morbidity associatedwith meniscal debridement resulting in a fairly rapidprogression in rehabilitation. The clinician should beaware that removal of the meniscus has been associatedwith increased risk of osteoarthritic changes, therefore,attention should be paid to quadriceps strength deficits,since improving quadriceps strength can provide poten-tial chondroprotective benefits (Slemenda et al 1998).
Protocols reported for postoperative meniscal repairrehabilitation vary in the initiation of weightbearing andmotion exercises. Some protocols allow motion from 0° to90° immediately after surgery (Cooper et al 1991); othersrecommend keeping the knee in full extension for 2weeks, then beginning a range of motion progression(DeHaven & Arnoczky 1994). Weightbearing to toleranceafter surgery has not been associated with any detri-mental effects to the repair (Shelbourne et al 1996);although an immobilizer that keeps the knee in fullextension may be used for the first couple of weeks toprotect the repair site. Patients are advised to avoid deepsquatting for the first 4 weeks to allow healing of therepair site if it is in the posterior part of the meniscus.Patient tolerance and ability to meet clinical milestonesdictate progression through the phases of rehabilitation.
REHABILITATION OF LESS COMMONINJURIES
POSTERIOR CRUCIATE LIGAMENT ANDPOSTEROLATERAL CORNER INJURIES
Mechanism of injury
Compared to the ACL and MCL, the PCL is lesscommonly injured; however, there is suspicion that manyinjuries go unreported or are misdiagnosed. PCL injuriesduring sports usually occur as a result of a posteriorlydirected blow to the proximal tibia. Often this occurswhen the athlete falls onto a flexed knee with the footplantar-flexed. This injury is common in ice hockeyplayers or figure skaters who slip and fall on the ice. ThePCL can also be compromised in a knee hyperextensioninjury.
Injuries to the PCL classically create long-term impair-ments and functional limitations due to secondarypathology of degenerative arthritic changes in thetibiofemoral and patellofemoral joints (Harner & Höher1998, Keller et al 1993). Some authors have gone so far asto state that degenerative changes in the tibiofemoraljoint following PCL injury ‘are inevitable’ (Cross &Powell 1984). Concomitant quadriceps weakness foundafter PCL tears often compounds the disability of theseconditions.
The posterolateral corner is described as the LCL, thepopliteus complex, the arcuate ligament complex,fabellofibular ligament, biceps tendon, and the postero-lateral capsular structures (Covey 2001). Injury to theseligamentous and muscular components that surroundthe posterior aspect of the lateral femoral condyle rarelyoccurs in isolation; rather, it is usually a concomitantinjury with the PCL. The posterolateral corner is typically
KNEE 391
F07154-20.qxd 3/9/02 1:28 PM Page 391

injured with a posteriorly direct force to the anteromedialtibia with the knee in hyperextension (Baker et al 1985,Covey 2001). Injury to the posterolateral corner can oftenbe missed in an examination of knee ligamentoussupport, especially with a concomitant PCL injury(Harner & Höher 1998, Noyes & Barber-Westin 1996).Those patients with combined PCL and posterolateralcorner injuries have a greater predisposition todegenerative changes than isolated PCL injured patients(Baker et al 1985, Torg et al 1989). Also, the addition of aposterolateral corner to a PCL injury is unlikely to besatisfactorily stabilized with sole reconstruction of thePCL (Harner et al 2000).
Non-operative treatment
Non-operative treatment is usually recommended after agrade I or II injury to the PCL. This corresponds with anisolated PCL injury with posterior translation of less than10 mm (Veltri & Warren 1993). Multiple directional laxityas a result of concomitant ACL, MCL, or posterolateralcorner injury usually undergoes operative reconstruction(Harner & Höher 1998, Harner et al 2000).
Restoring quadriceps strength is the cornerstone ofconservative rehabilitation following PCL injury (Torg etal 1989, Wilk 1994). Early efforts to improve quadricepsstrength must be tempered by the potentially detrimentalposterior stresses that are generated by some types ofstrengthening exercises. Several studies have investi-gated the potential posterior translation with open andclosed chain knee extension exercises. Open chain kneeextension exercises from 0–60° produce anterior shearforces at the tibiofemoral joint while open chain kneeextensions beyond 60° can create posterior tibial trans-lations (Jurist & Otis 1985, Kaufman et al 1991, Lutz et al1993). Studies that have investigated closed chainexercise also report high posterior displacement forceswhich seem to increase with increased flexion (Lutz et al1993, Stuart et al 1996). Caution should be taken in usingopen chain knee flexion exercises in rehabilitationprograms following PCL injury, due to the undesiredposterior forces associated with these types ofstrengthening.
During the first 2 weeks following injury, the athletetypically wears a knee brace that limits motion to nearfull extension. Range of motion exercises from 0–60° areperformed 3–4 times a day along with isometric andshort arc (0–30°) open chain quadriceps exercises. Use of isometric NMES usually starts at 30° of flexion (Axe etal 2001).
After 2 weeks, biking may be used for range of motionefforts (Wilk 1994). The open chain knee extension exer-cise range is progressed to 0–60° with progressive resist-ance. General strengthening of the calf musculature can
be initiated at this time. Range of motion is typicallyprogressed until the patient achieves 0–110° by theirfourth week.
At the start of the fourth week, the patient should haverestored gait without a limp. Limited range, closed chainstrengthening exercises can be initiated if they are purelysagittal plane exercises of no deeper than 45° of flexion(Wilk 1994). The main emphasis of strengthening shouldcontinue to be open chain knee extension in limitedrange. Anterior knee pain is common in this patientpopulation and modifications to open chain exercises toavoid painful strengthening should be employed. Fullrange of motion should be achieved by 4–6 weeks afterinjury. By approximately 8 weeks after injury, rehabili-tation may progress to the return-to-play phase withclose monitoring of patellofemoral joint pain andchanges in posterior laxity.
Posterolateral corner instability in combination withPCL injury usually slows the speed of progression innon-operative and operative rehabilitation. There are anumber of operative techniques to correct this instability,but currently there is no ‘gold standard’ for operativemeasures (Covey 2001). Attempts to improve thedynamic stability of the knee using techniques com-parable to non-operative rehabilitation following ACLinjury appear to be the best non-operative treatmentoption to correct for knee instability that lacks a viablesurgical correction. A combination of perturbationtraining and completion of a functional progressionrepresent the non-operative treatment of posterolateralcorner injuries.
Operative treatment
Reconstruction as operative management of posteriorlaxity is typically indicated if the patient has functionalinstability or pain, early degenerative changes in thetibiofemoral joint, or combined ligamentous injuries(Harner et al 2000). Typical autograft material forreconstruction consists of bone–patellar tendon–bone,semitendinous and gracilis, and quadriceps tendon–bone(Axe et al 2001). Most allografts use Achilles tendon,bone–patellar tendon–bone, or allograft (Bullis & Paulos1994). A surgical repair may be performed if a bonefragment has avulsed with the PCL. Relatively little isknown concerning fixation strength and graft incorpora-tion following PCL operative treatment.
Postoperative treatment
Rehabilitation following surgery is governed by therelatively poor strength of the fixation of the recon-structed ligament. Increased posterior laxity is a morefrequent complication than arthrofibrosis and subse-
392 REGIONAL SPORT AND EXERCISE INJURY MANAGEMENT
F07154-20.qxd 3/9/02 1:28 PM Page 392

quent loss of flexion range of motion. Therefore, earlyrehabilitative efforts are focused on controlling inflam-matory processes, and preventing arthrofibrosis andatrophy without excessively stressing the newlyreconstructed graft.
Physical therapy following surgery is very similar toconservative treatment for a grade III PCL tear butinvolves a longer protective phase to insure that posteriorlaxity does not develop. Again, open chain knee flexionexercises are avoided as they will likely cause deleteriousposterior stress on the newly reconstructed ligament.Patients are usually braced in full extension for at least 2weeks and as long as 4 weeks. One to two weeks aftersurgery, preservation of knee extensor musculature isinitiated, as this will be crucial for eliminating posteriortibial translation to provide graft protection in laterstages of therapy. Knee extension stretches typically areperformed in the prone position to minimize possibleposterior translation due to gravitational forces on thetibia. Early knee flexion stretches are also performed inthe prone position, with careful instructions to the patientto avoid active knee flexion during stretches. A manualanterior displacement of the tibia on the femur should bemaintained during passive flexion stretching for the first4 weeks. A knee range of motion of 0–60° is the milestonefor 2 weeks after surgery. Quadriceps control shouldimprove to the point that, at 2 weeks, the patient is ableto maintain full knee extension without a lag againstgravity.
At 3–4 weeks, the athlete can start to be weaned fromthe brace and gait training should be initiated if there isdemonstration of adequate quadriceps control (Wilk1994). Open chain knee extensions can be performedfrom 0–60° of flexion. Closed chain exercises can beincorporated at this point as the patient moves throughthe advanced rehabilitation stage. Progression into thereturn-to-play phase will start at approximately 3 monthsafter surgery if the corresponding criteria is met.
Reconstruction for posterior laxity with a combinedposterolateral corner injury requires an even greaterprotection period. Combined posterolateral corner laxityhas been identified as a potential cause of graft failure inPCL reconstruction (Harner et al 2000). There are no clearguidelines to perform a reconstruction or repair of thisrotational laxity, even when it is recognized (Harner et al2000). The athlete must be counseled regarding adiminished likelihood of a rapid return to sport with aninjury involving combined posterior and posterolateralinstability. Clinical milestones should be delayed by 2weeks compared to isolated PCL injury, and return tocutting and rotational activities will be implemented in amore gradual fashion.
Combined PCL and posterolateral corner reconstruc-tions involve the greatest amount of restrictions
following surgery due to the severity of the injury andthe reconstruction (Wilk 1994). Crutches are typicallydiscontinued after about 2 weeks but a knee immobilizeris used to lock the knee in full extension for 6 weeks withno motion allowed during this period. At about 6 weeks,strengthening moves beyond isometric quadricepsactivities to active and active assisted motions and isprogressed as for PCL reconstruction. Typically, full rangeof motion is achieved at about 8 weeks postoperatively(Wilk 1994). Return to strenuous activities varies from 18to 21 weeks following surgery.
TIBIAL PLATEAU FRACTURE
Mechanism of injury
A significant varus, valgus or compressive force at theknee can cause a fracture of the tibial plateau. Tibialplateau fractures commonly occur in loaded, twistinginjuries or direct blows to the knee causing a directcompressive force through a femoral condyle into thetibial plateau. Due to the natural valgus angulation of theknee, lateral tibial plateau fractures are more commonthan medial fractures (Kennedy & Bailey 1968). Tibialplateau fractures are categorized as medial, lateral orbicondylar; non-displaced or displaced; and depressed ornon-depressed.
Non-operative treatment
If a tibial plateau fracture is treated non-operatively, thereis no attempt to restore the anatomical position of thejoint surface through surgical reduction. The knee iscommonly placed in a cast-brace, with or withouttraction. Many researchers believe that traction will allowspontaneous reduction via ‘ligamentotaxis’; early motionwill further contribute to reduction by ‘molding’displaced bone fragments (Apley 1979). Allowing at least2 weeks of immobilization before beginning motionexercises has resulted in greater gains in knee flexionrange of motion (Gausewitz & Hohl 1986). Weightbearingcan be initiated within the first 7–14 days for all types oftibial plateau fractures, except fractures that are bothdisplaced and depressed, and has positive effects on kneerange of motion and avoidance of valgus deformity(Segal et al 1993).
Rehabilitation is dictated first and foremost by theneed for physiological healing of the fracture. Weight-bearing exercises like squatting are avoided for the first4–6 weeks in order to allow the fracture sufficient time toheal. Quadriceps strength and knee extension should bea focus of treatment in the acute phase; however, giventhe fact that tibial plateau fractures are placed in a cast-brace, regaining knee flexion will also become a priority
KNEE 393
F07154-20.qxd 3/9/02 1:28 PM Page 393

once the cast-brace is removed. Patients are allowed toprogress to strenuous weightbearing exercise, such asdeep squatting, in the advanced phase, once callusformation is seen on X-ray. Progression in the return-to-play phase is dictated by patient symptoms.
Operative treatment
Operative management of tibial plateau fractures beginswith the decision of whether or not the patient needsinternal fixation of the fracture. Open reduction withinternal fixation (ORIF) is currently the surgical choice,where most tibial plateau fractures are displaced ordisplay more than 4 mm of tibial plateau depression(Lachiewicz & Funcik 1990, Segal et al 1993). Bonegrafting into the fracture site or into the depressed tibialplateau is a common adjunct to surgery. Lachiewicz &Funcik (1990) found that the absence of a bone graft withORIF was associated with less than excellent resultspostoperatively. Surgical reduction can also help to pre-vent arthritic changes to the tibiofemoral joint surfaces byrestoring joint congruency and correcting for damagingvarus/valgus joint instability.
Postoperative treatment
Postoperatively, tibial plateau fractures are treated simi-larly to non-displaced, non-surgical fractures. Weight-bearing, in a cast-brace, is best initiated within 7–14 daysfor the best range of motion and valgus deformity results(Segal et al 1993). In surgically treated displacedfractures, early motion before 2 weeks postinjury hasallowed for the most knee flexion range of motion at 6month follow-ups (Gausewitz 1986). Like non-operativetreatment of tibial plateau fractures, rehabilitation mustallow for physiological healing of the reduced jointsurface. Weightbearing exercises should be avoided forthe first 4–6 weeks. Progression in the advanced andreturn-to-play phases of rehabilitation is similar to thenon-operative treatment protocol.
ARTHRITIS AND THE ATHLETE
More people are remaining active for longer periods oftheir life. Decisions regarding treatment of an athleteshould be based on their desired activity level and nottheir biological age. The eventual consequence of sportsinjuries such as meniscal tears, maintaining high bodymass index, ligamentous sprains, and articular surfacedamage, play a substantial role in developing secondaryjoint disease (Felson et al 2000, Gelber et al 1999, 2000,Kujala et al 1994, Lundberg & Messner 1997, Messner etal 2001). An important factor to remember in treating
athletes with these injuries is that there is no cure forosteoarthritis. Once cartilage damage has occurred, itcannot be perfectly repaired with more hyaline cartilage(Buckwalter 1998). Thus, to slow continued deteriorationis a goal of rehabilitative interventions.
Non-operative treatment for osteoarthritis
Counseling is one of the most important aspects in thecourse of treatment for osteoarthritis. Efforts to reduceweight should be strongly encouraged as obesity is arecognized risk factor in the development ofosteoarthritis (Felson et al 1997, Stürmer et al 2000). Lossof body weight can have a pronounced affect on stressesat the knee as the loss of a 1 lb of body weight cancorrelate to a loss of 3 lbs of force at the knee (Schipplein& Andriacchi 1991).
Joint-sparing activities should be used as a mainstay toprovide minimal risk to the knee joint while stillproviding adequate stimulus to maintain strength andconditioning. Non-impact aerobic exercises take the placeof running type activities. Examples include, but are notlimited to, cross-country skiing, swimming, bicycling,roller-blading, elliptical running simulators, walking, andwater aerobics. Avoidance of aerobic exercise should notbe counseled, as increased weight associated withinactivity would be likely to have a detrimental affect on the knee. If the athlete insists on the need to continueimpact activities, instruction on improved footwearchoices, and encouraging exercise on a more forgivingsurface, will help to attenuate stresses on the arthriticknee.
Quadriceps strength can play an important role inpreserving activity level and potentially decreasing therisk for progressive osteoarthritis (O’Reilly et al 1998,Slemenda et al 1998). Several studies that have investi-gated strengthening protocols for knee osteoarthritishave reported modest strength gains, but significantreduction in pain and increased function (Fisher et al1991, Fisher et al 1997, Hurley & Newham 1993, Hurley& Scott 1998). In general, strengthening programs shouldinclude an emphasis on open chain exercise to avoid theadditional compressive force present during weighted,closed chain strengthening exercise. Efforts should betaken to prescribe exercises that do not cause pain duringtheir execution and do not stimulate an inflammatoryresponse. A process of trial and error is used to prescribethe best exercises for each patient.
In patients that have unicompartmental arthritis,additional mechanical interventions can be attempted toreduce load to the affected compartment. Medialinvolvement is the most common site of unicompartmentjoint degeneration. An unloading brace or a lateral heelwedge can potentially decrease the external valgus
394 REGIONAL SPORT AND EXERCISE INJURY MANAGEMENT
F07154-20.qxd 3/9/02 1:28 PM Page 394

moment at the knee and decrease pain in patients withthis form of the disease (Hewett et al 1998, Keating et al1993, Pollo 1998, Tohyama et al 1991).
Typically, pain management for osteoarthritis can beachieved through the simple use of analgesics such asacetiminophen (Bradley et al 2001, Brandt 2000). Non-steroidal anti-iflammatory drugs (NSAIDs) can be usedas well, but have higher risk for gastrointestinal, renal, orhepatic side-effects from long-term use. For arthriticknees that present with continual effusion, NSAIDs maybe more effective in controlling symptoms than anal-gesics. Joint aspiration and intra-articular corticosteroidinjections may also provide pain relief for patients whohave effused joints (Creamer 1997, Fadale & Wiggins1994, Livesley et al 1991). In the knee that is painfulwithout the presence of an effusion, injections ofhyaluronic acid have been shown to have pain-reducingproperties that are similar to NSAIDs. This relief can lastfor months after treatment (Altman & Moskowitz 1998,Brandt et al 2001). This treatment usually consists of 3–5injections given over 15 days and presents a relativelyhigh financial risk for the patient due to the high cost ofthis form of management.
Recent studies have also supported the use of some‘neutracuticals’ in managing symptoms and potentiallyprotecting remaining articular cartilage in knee osteo-arthritis. In particular, the oral supplements, chondroitinsulphate and glucosamine, have some efficacy indecreasing symptoms of pain in patients with mild osteo-arthritis, with few to no known side-effects (Bourgeois etal 1998, Lippiello et al 2000, Mazieres et al 2001, Muller-Fassbender et al 1994, Reginster et al 2001). Thesesupplements have been hypothesized to provide somechondroprotective effects and can have an impact on painwith osteoarthritis of the knee.
Operative treatment
Several operative treatments are available to reduce thesigns and symptoms of an arthritic knee. Procedures assimple as arthroscopic lavage have been proven toprovide relief, albeit temporary, from the pain associatedwith osteoarthritis (Kalunian et al 2000, Livesley et al1991). Little soft tissue injury is involved in theseprocedures and the majority of rehabilitation is centeredaround resolving impairments of pain, loss of range ofmotion, and weakness.
Chondral lesions, either chronic degenerative injuriesor traumatic blows such as involved in an ACL tear, havelimited potential for repair or reconstruction. Operativeprocedures involve evoking a vascular response from theunderlying subchondral bone and bone marrow to ‘scar’the lesion with fibrocartilage (Buckwalter 1998, Buckwalter& Lohmander 1994). The repaired cartilage has inferior
mechanical properties when compared to hyalinecartilage for joint preservation (Walker 1998). This isachieved through the use of surgical burr (i.e. abrasionchondroplasty, or some form of microfracture whereholes are poked through the cartilage defect) (Friedmanet al 1984). If a full thickness lesion is present, an OATS(Osteochondral Autograft Transfer System) procedure isperformed using a chondral graft to transplant into anarea of chondral defect (Bobic 1996, Matsusue et al 1993).Severe chondral lesions can also be addressed withautologous chondrocyte transplantation. Autologouschondrocyte transplantation is where donor chondro-cytes are cultured in a laboratory and then reintroducedinto the chondral defect under a protective, autologousperiosteal flap. This procedure may allow the defect to fillwith hyaline-like cartilage (Brittberg et al 1994, Gilloglyet al 1998).
Postoperative treatment
Rehabilitation following chondroplasty procedures isfocused on limiting early weightbearing to allow forfibrocartilage to mature at the site of microfracture orabrasion. Patients are typically restricted to no greaterthan touch down weightbearing for 4–6 weeks followingthese procedures (Irrgang & Pezzullo 1998, Suh et al1997). Isometric exercises and NMES at joint angles thatdo not engage the repaired tissue are used to improvemuscle function during this period of limited weight-bearing (Irrgang & Pezzullo 1998). Stretching efforts areencouraged as immobilization has a detrimental effect onchondrocytes, cartilage thickness, and proteoglycanconcentration (Behrens et al 1989, Palmoski & Brandt1982).
Weightbearing is slowly progressed from this point.Closed chain exercise is used sparingly with a slow pro-gression. Use of an unloading brace and/or heel wedge(s)for 3 months after surgery, with assistive devices duringactivity, assists in potential unweighting of the repairedchondral defect. Chances for joint effusion are highfollowing these procedures and if patients demonstrateincreased effusion, then they step back in activity level.This may mean they go back to the use of crutches toassist in efforts to the control inflammation.
Slowly advancing impact to return to play can easily beachieved through the use of aerobics in the pool. Walkingin progressively shallow water and instituting aqua-jogging can assist in facilitating conditioning whileproviding progressive stress to assist in remodeling thehealing cartilage surface. Returning to impact activitiessuch as jogging will be instituted as late as 8 months afterthe repair (Gillogly et al 1998). Most patients whoundergo chondroplasty procedures should be counseledin joint-sparing lifestyle changes.
KNEE 395
F07154-20.qxd 3/9/02 1:28 PM Page 395

SUMMARY
A thorough knowledge of knee anatomy and bio-mechanics is needed for proper diagnosis and rehabilita-tion of the injured athlete. Without this knowledge,healing tissue may be overly stressed, impeding anexpedient return to activity. It is also important forclinicians working with athletes to know the demands ofthe athlete’s sport, so that they can properly prepare theathlete for the stresses that will be encountered.
Non-operative rehabilitation and rehabilitation fol-lowing surgery both follow criterion-based protocols,which outline clinical milestones that must be met inorder to progress to the next phase of rehabilitation. Painand effusion dictate progression within a rehabilitativephase. Athletes must progress through all phases ofrehabilitation in order to ensure that they are adequatelyprepared to return to sport; however, exercises withineach phase should be tailored to the athlete’s needs andcertain exercises may be excluded, based on surgicalconsiderations.
396 REGIONAL SPORT AND EXERCISE INJURY MANAGEMENT
REFERENCES
Altman R D, Moskowitz R 1998 Intraarticular sodium hyaluronate(Hyalgan) in the treatment of patients with osteoarthritis of theknee: a randomized clinical trial. Hyalgan Study Group25(11):2203–2212
Anderson A F, Lipscomb A B 1986 Clinical diagnosis of meniscal tears.Description of a new manipulative test. American Journal of SportsMedicine 14(4):291–293
Anderson A F, Snyder R B, Federspiel C F et al 1992 Instrumentedevaluation of knee laxity: a comparison of five athrometers.American Journal of Sports Medicine 20(2):135–140
Apley A G 1979 Fractures of the tibial plateau. Orthopaedic Clinics ofNorth America 10:61–74
Arnoczky S P, Warren R F 1982 Microvasculature of the humanmeniscus. American Journal of Sports Medicine 10(2):90–95
Axe M J, Swigart K H, Snyder-Mackler L 2001 Surgical options andprocedure-modified rehabilitation for PCL injury. Athletic TherapyToday 6:16–22
Baker C L Jr, Norwood L A, Hughston J C 1985 Acute combinedposterior cruciate and posterolateral instability of the knee.American Journal of Sports Medicine 12:204–208
Barber S D, Noyes F R, Mangine R E et al 1990 Quantitativeassessment of functional limitations in normal and anterior cruciateligament-deficient knees. Clinical Orthopaedics and RelatedResearch Jun(255):204–214
Behrens F, Kraft E L, Oegema T R Jr 1989 Biochemical changes inarticular cartilage after joint immobilization by casting or externalfixation. Journal of Orthopaedic Research 7(3):335–343
Beynnon B D, Johnson R J, Fleming B C et al 1997 The strain behaviorof the anterior cruciate ligament during squatting and activeflexion-extension. A comparison of an open and a closed kineticchain exercise. American Journal of Sports Medicine 25(6):823–829
Bobic V 1996 Arthroscopic osteochondral autograft transplantation inanterior cruciate ligament reconstruction: a preliminary clinicalstudy. Knee Surgery, Sports Traumatology, Arthroscopy 3(4):262–264
Boden B P, Dean G S, Feagin J A Jr et al 2000 Mechanisms of anteriorcruciate ligament injury. Orthopedics 23(6):573–578
Bolgla L A, Keskula D R 1997 Reliability of lower extremity functionalperformance tests. Journal of Orthopaedic and Sports PhysicalTherapy 26(3):138–142
Bourgeois P, Chales G, Dehais J et al 1998 Efficacy and tolerability ofchondroitin sulfate 1200 mg/day vs chondroitin sulfate 3 × 400mg/day vs placebo. Osteoarthritis and Cartilage 6(suppl A):25–30
Bradley J D, Katz B P, Brandt K D 2001 Severity of knee pain does notpredict a better response to an anti-inflammatory dose of ibuprofenthan to analgesic in patients with osteoarthritis. Journal ofRheumatology 28:1073–1076
Brandt K D 2000 The role of analgesics in the management ofosteoarthritis pain. American Journal of Therapeutics 7:75–90
Brandt K D, Block J A, Michalski J P et al 2001 Efficacy and safety ofintraarticular sodium hyaluronate in knee osteoarthritis. ClinicalOrthopaedics and Related Research 385:130–143
Brittberg M, Lindahl A, Nilsson A et al 1994 Treatment of deepcartilage defects in the knee with autologous chondrocytetransplantation. New England Journal of Medicine 331(14):889–895
Buckwalter J A 1998 Articular cartilage: injuries and potential forhealing. Journal of Orthopaedic and Sports Physical Therapy28(4):192–202
Buckwalter J, Lohmander S 1994 Current concepts review: operativetreatment of osteoarthrosis. Journal of Bone and Joint Surgery (Am)76-A(9):1405–1418
Bullis D W, Paulos L E 1994 Reconstruction of the posterior cruciateligament with allograft. Clinics in Sports Medicine 13(3):581–597
Butler D L, Noyes F R, Grood E S 1980 Ligamentous restraints toanterior-posterior drawer in the human knee. A biomechanicalstudy. Journal of Bone and Joint Surgery (Am) 62-A(2):259–270
Clark C R, Ogden J A 1983 Development of the menisci of the humanknee joint. Morphological changes and their potential role inchildhood meniscal injury. Journal of Bone and Joint Surgery (Am)65-A(4):538–547
Cooper D E, Arnoczky S P, Warren R F 1991 Meniscal repair. Clinics inSports Medicine 10(3):529–548
Corea J R, Moussa M, Al Othman A 1994 McMurray’s test tested. KneeSurgery, Sports Traumatology, Arthroscopy 2:70–72
Covey D C 2001 Current concepts review injuries of the posterolateralcorner of the knee. Journal of Bone and Joint Surgery (Am) 83-A(1):106–118
Creamer P 1997 Intra-articular corticosteroid injections inosteoarthritis: do they work and if so, how? Annals of RheumaticDiseases 56(11):634–636
Cross M J, Powell J F 1984 Long-term followup of posterior cruciateligament rupture: A study of 116 cases. American Journal of SportsMedicine 12(4):292–297
DeHaven K E, Arnoczky S P 1994 Meniscus repair: basic science,indications for repair and open repair. Instructional Course Lectures43:65–76
Derscheid G L, Garrick J G 1981 Medial collateral ligament injuries infootball: nonoperative management of grade I and grade II sprains.American Journal of Sports Medicine 9:365–368
Donaldson W F, Warren R F, Wickiewicz T 1985 A comparison of acute anterior cruciate ligament examinations. Initial versus
examination under anesthesia. American Journal of Sports Medicine13(1):5–9
Escamilla R F, Fleisig G S, Zheng N et al 1998 Biomechanics of theknee during closed kinetic chain and open kinetic chain exercise.Medicine and Science in Sports and Exercise 30(4):556–569
Fadale P D, Wiggins M E 1994 Corticosteroid Injections: their use andabuse. Journal of the American Academy of Orthopaedic Surgeons2(3):133–140
Felson D T, Zhang Y, Hannan M T et al 1997 Risk factors for incidentradiographic knee osteoarthritis in the elderly. Arthritis andRheumatism 40(4):728–733
Felson D T, Lawrence R C, Dieppe P A et al 2000 Osteoarthritis: new
F07154-20.qxd 3/9/02 1:28 PM Page 396

insights. Part 1: the disease and its risk factors. Annals of InternalMedicine 133(8):635–646
Fisher N D, Pendergast D R, Gresham G E et al 1991 Musclerehabilitation: its effect on muscular and functional performance ofpatients with knee osteoarthritis. Archives of Physical Medicine andRehabilitation 72:367–374
Fisher N M, White S C, Yack H J et al 1997 Muscle function and gait inpatients with knee osteoarthritis before and after musclerehabilitation. Disability and Rehabilitation 19(2):47–55
Fitzgerald G K 1997 Open versus closed kinetic chain exercises: issuesin rehabilitation after anterior cruciate ligament reconstructivesurgery. Journal of Orthopaedic and Sports Physical Therapy77(12):1747–1754
Fitzgerald G K, Axe M J, Snyder-Mackler L 2000a A decision-makingscheme for returning patients to high-level activity withnonoperative treatment after anterior cruciate ligament rupture.Knee Surgery, Sports Traumatology, Arthroscopy 8(2):76–82
Fitzgerald G K, Axe M J, Snyder-Mackler 2000b The efficacy ofperturbation training in nonoperative anterior cruciate ligamentrehabilitation programs for physically active individuals. PhysicalTherapy 80(2):128–140
Friedman M, Berasi C, Fox J et al 1984 Preliminary results withabrasion arthroplasty in the osteoarthritic knee. ClinicalOrthopaedics and Related Research 82:200–205
Fu F H, Baratz M 1994 Meniscal injuries. In: DeLee J C, Drez DOrthopaedic sports injuries. WB Saunders, Philadelphia
Fukubayashi T, Torzilli P A, Sherman M F et al 1982 An in vitrobiomechanical evaluation of anterior-posterior motion of the knee.Tibial displacement, rotation, and torque. Journal of Bone and JointSurgery (Am) 64A(2):258–264
Galway H R, Beaupre A, MacIntosh D L 1972 Pivot shift: a clinical signof symptomatic anterior cruciate deficiency. Journal of Bone andJoint Surgery (Br) 54-B:763–764
Gapeyeva H, Paasuke M, Ereline J et al 2000 Isokinetic torque deficitof the knee extensor muscles after arthroscopic partial menisectomy.Knee Surgery, Sports Traumatology, Arthroscopy 8(5):301–304
Gausewitz S, Hohl M 1986 The significance of early motion in thetreatment of tibial plateau fractures. Clinical Orthopaedics202:135–138
Gelber A C, Hochberg M C, Mead L A et al 1999 Body mass index inyoung men and the risk of subsequent knee and hip osteoarthritis.American Journal of Medicine 107:542–548
Gelber A C, Hochberg M C, Mead L A et al 2000 Joint injury in youngadults and risk for subsequent knee and hip osteoarthritis. Annalsof Internal Medicine 133:321–328
Gillogly S D, Voight M, Blackburn T 1998 Treatment of articularcartilage defects of the knee with autologous chondrocyteimplantation. Journal of Orthopaedic and Sports Physical Therapy28(4):241–251
Girgis F G, Marshall J L, Monajem A R S 1975 The cruciate ligamentsof the knee: anatomical, functional and experimental analysis.Clinical Orthopedics 106:216–231
Gollehon D L, Torzilli P A, Warren R F 1987 The role of theposterolateral and cruciate ligaments in the stability of the humanknee. A biomechanical study. Journal of Bone and Joint Surgery(Am) 69A(2):233–242
Grood E S, Noyes F R, Butler D L et al 1981 Ligamentous and capsularrestraints preventing straight medial and lateral laxity in intacthuman cadaver knees. Journal of Bone and Joint Surgery (Am)63A(8):1257–1269
Harner C D, Höher J 1998 Evaluation and treatment of posteriorcruciate ligament injuries. American Journal of Sports Medicine26(3):471–82
Harner C D, Irrgang J J, Paul J et al 1992 Loss of motion after anteriorcruciate ligament reconstruction. American Journal of SportsMedicine 20(5):499–506
Harner C D, Vogrin T M, Höher J et al 2000 Biomechanical analysis ofa posterior cruciate ligament reconstruction. Deficiency of theposterolateral structures as a cause of graft failure. American Journalof Sports Medicine 28(1):32–39
Heller L, Langman J 1964 The menisco-femoral ligaments of thehuman knee. Journal of Bone and Joint Surgery (Br) 46-B:307–313
Hewett T E, Noyes F R, Barber-Westin S D et al 1998 Decrease in kneejoint pain and increase in function in patients with medialcompartment arthrosis: a prospective analysis of valgus bracing.Orthopedics 21(2):131–138
Holden D L, Eggert A W, Butler J E 1983 The nonoperative treatmentof Grade I and II medial collateral ligament injuries to the knee.American Journal of Sports Medicine 11(5):340–343
Hughston J C, Andrews J R 1976 Classification of knee ligamentinstabilities. Part I. The medial compartment and cruciate ligaments.Journal of Bone and Joint Surgery (Am) 58A:159–172
Hurley M V, Newham D J 1993 The influence of arthrogenous muscleinhibition on quadriceps rehabilitation of patients with early,unilateral osteoarthritic knees. British Journal of Rheumatology32:127–131
Hurley M V, Scott D L 1998 Improvements in quadriceps sensorimotorfunction and disability of patients with knee osteoarthritis followinga clinically practicable exercise regime. British Journal ofRheumatology 37:1181–1187
Indelicato P A 1983 Nonoperative treatment of complete tears of themedial collateral ligament of the knee. Journal of Bone and JointSurgery (Am) 65A:323–329
Indelicato P A 1995 Isolated medial collateral ligament injuries in theknee. Journal of the American Academy of Orthopaedic Surgeons3(1):9–14
Indelicato P A, Hermansdorfer J, Huegel M 1990 Nonoperativemanagement of complete tears of the medial collateral ligament ofthe knee in intercollegiate football players. Clinical Orthopaedicsand Related Research Jul (256):174–177
Inoue M, McGurk-Burleson E, Hollis J M et al 1987 Treatment of themedial collateral ligament injury: the importance of anterior cruciateligament on the valgus-varus knee laxity. American Journal ofSports Medicine 15(1):15–21
Irrgang J J, Pezzullo D P 1998 Rehabilitation following surgicalprocedures to address articular cartilage lesions in the knee. Journalof Orthopaedic and Sports Physical Therapy 28(4):232–240
Irrgang J J, Snyder-Mackler L, Wainner R S et al 1998 Development ofa patient-reported measure of function of the knee. Journal of Boneand Joint Surgery (Am) 80A(8):1132–1145
Jones R E, Henley M B, Francis P 1986 Nonoperative management ofisolated Grade III collateral ligament injury tears in high schoolfootball players. Clinical Orthopaedics 213:137–140
Jurist K A, Otis J C 1985 Anteroposterior tibifemoral displacementsduring isometric extension efforts. The roles of external load andknee flexion angle. American Journal of Sports Medicine.13(4):254–258
Kalunian K C, Moreland L W, Klashman D J et al 2000 Visually-guidedirrigation in patients with early knee osteoarthritis: a multicenterrandomized, controlled trial. Osteoarthritis and Cartilage 8:412–418
Kaufman K R, An K N, Litchy W J et al 1991 Dynamic joint forcesduring knee isokinetic exercise. American Journal of SportsMedicine 19(3):305–316
Keating E M, Faris P M, Ritter M A et al 1993 Use of lateral heel andsole wedges in the treatment of medial osteoarthritis of the knee.Orthopaedic Review 22(8):921–924
Keays S L, Bullock-Saxton J, Keays A C 2000 Strength and functionbefore and after anterior cruciate ligament reconstruction. ClinicalOrthopaedics and Related Research Apr (373):174–183
Keller P M, Shelbourne K D, McCarroll J R et al 1993 Nonoperativelytreated isolated posterior cruciate ligament injuries. AmericanJournal of Sports Medicine 21(1):132–136
Kennedy J C, Bailey W H 1968 Experimental tibial plateau fractures:studies of mechanism and a classification. Journal of Bone and JointSurgery (Am) 50A:1522
Kujala U M, Kaprio J, Sarno S 1994 Osteoarthritis of weight bearingjoints of lower limbs in former elite male athletes. British MedicalJournal 308:231–234
Lachiewicz P F, Funcik T 1990 Factors influencing the results of openreduction and internal fixation of tibial plateau fractures. ClinicalOrthopaedics 259:210–215
Lippiello L, Woodward J, Karpman R et al 2000 In vivochondroprotection and metabolic synergy of glucosamine and
KNEE 397
F07154-20.qxd 3/9/02 1:28 PM Page 397

chondroitin sulfate. Clinical Orthopaedics and Related Research381:229–240
Liu S H, Osti L, Henry M et al 1995 The diagnosis of acute completetears of the anterior cruciate ligament. Comparison of MRI,arthrometry and clinical examination. Journal of Bone and JointSurgery (Br) 77-B(4):586–588
Livesley P J, Doherty M, Needoff M et al 1991 Arthroscopic lavage ofosteoarthritic knees. Journal of Bone Joint Surgery (Br) 73-B(6):922–926
Lundberg M, Messner K 1997 Ten-year prognosis of isolated andcombined medial collateral ligament ruptures: a matchedcomparison in 40 patients using clinical and radiographicevaluations. American Journal of Sports Medicine 25(1):2–6
Lutz G E, Palmitier R A, An K N et al 1993 Comparison of tibiofemoraljoint forces during open-kinetic-chain and closed-kinetic-chainexercises. Journal of Bone and Joint Surgery (Am) 75-A(5):732–739
Lysholm J, Gillquist J 1982 Evaluation of knee ligament surgery resultswith special emphasis on use of a scoring scale. American Journal ofSports Medicine 10(3):150–154
McGee D J 1992 Orthopedic physical assessment, 2nd edn. WBSaunders, Philadelphia
Manal T J, Snyder-Mackler L 1996 Practice guidelines for anteriorcruciate ligament rehabilitation: a criterion-based rehabilitationprogression. Operative Techniques in Orthopaedics 6(3):190–196
Markolf K L, Gorek J F, Kabo J M et al 1990 Direct measurement ofresultant forces in the anterior cruciate ligament. An in vitro studyperformed with a new experimental technique. Journal of Bone andJoint Surgery (Am) 72-A(4):557–567
Matsusue Y, Yamamuro T, Hama H 1993 Arthroscopic multipleosteochondral transplantation to the chondral defect in the kneeassociated with anterior cruciate ligament disruption. Arthroscopy9(3):318–321
Mazieres B, Combe B, Van A P et al 2001 Chondroitin sulphate inosteoarthritis of the knee: a prospective, double blind, placebocontrolled multicenter clinical study. Journal of Rheumatology28:173–181
Messner K, Fahlgren A, Persliden J et al 2001 Radiographic joint spacenarrowing and histologic changes in a rabbit menisectomy model ofearly knee osteoarthrosis. American Journal of Sports Medicine29(2):151–160
Mikkelsen C, Werner S, Eriksson E 2000 Closed kinetic chain alonecompared to combined open and closed kinetic chain exercises forquadriceps strengthening after anterior cruciate ligamentreconstruction with respect to return to sports: a prospectivematched follow-up study. Knee Surgery, Sports Traumatology,Arthroscopy 8(6):337–342
Morrissey M C 1989 Reflex inhibition of thigh muscles in knee injury.Causes and treatment. Sports Medicine 7(4):263–276
Morrissey M C, Hudson Z L, Drechsler W I et al 2000 Effects of openversus closed kinetic chain training on knee laxity in the earlyperiod after anterior cruciate ligament reconstruction. Knee Surgery,Sports Traumatology, Arthroscopy 8(6):343–348
Muller-Fassbender H, Bach G L, Haase W et al 1994 Glucosaminesulfate compared to ibuprofen in osteoarthritis of the knee.Osteoarthritis and Cartilage 2(1):61–69
Noyes F R, Barber S D, Mooar L A 1989 A rationale for assessingsports activity levels and limitations in knee disorders. ClinicalOrthopaedics and Related Research Sep(246):238–249
Noyes F R, Barber S D, Mangine R E 1991 Abnormal lower limbsymmetry determined by function hop tests after anterior cruciateligament rupture. American Journal of Sports Medicine19(5):513–518
Noyes F R, Barber-Westin S D 1996 Surgical restoration to treat chronicdeficiency of the posterolateral complex and cruciate ligaments ofthe knee joint. American Journal of Sports Medicine 24(4):415–426
Nyland J 1999 Rehabilitation complications following knee surgery.Clinics in Sports Medicine 18(4):905–925
O’Reilly S C, Jones A, Muir K R et al 1998 Quadriceps weakness inknee osteoarthritis: the effect on pain and disability. Annals ofRheumatic Diseases 57(10):588–594
Palmoski M, Brandt K 1982 Immobilisation of the knee preventsosteoarthritis after anterior cruciate ligament resection. Arthritis andRheumatism 25:1201–1208
Pollo F E 1998 Bracing and heel wedging for unicompartmentalosteoarthritis of the knee. American Journal of Knee Surgery11(1):47–50
Rangger C, Daniel D M, Stone M L et al 1993 Diagnosis of an ACLdisruption with KT-1000 arthrometer measurements. Knee Surgery,Sports Traumatology, Arthroscopy 1(1):60–66
Reginster J Y, Deroisy R, Rovati L C et al 2001 Long-term effects ofglucosamine sulphate on osteoarthritis progression: a randomised,placebo-controlled clinical trial. Lancet 357(9252):247–248
Schipplein O D, Andriacchi T P 1991 Interaction between active andpassive knee stabilizers during level walking. Journal ofOrthopaedic Research 9(1):113–119
Segal D, Mallik A R, Wetzler M J et al 1993 Early weight bearing oflateral tibial plateau fractures. Clinical Orthopaedics 294:232–237
Shakespeare D T, Rigby H S 1983 The bucket-handle tear of themeniscus. A clinical and arthrographic study. Journal of Bone andJoint Surgery (Br) 65-B:383–387
Shelbourne K D, Patel D V, Adsit W S et al 1996 Rehabilitation aftermeniscal repair. Clinics in Sports Medicine 15(3):595–612
Shelton W R , Barrett G R, Dukes A 1997 Early season anterior cruciateligament tears. A treatment dilemma. America Journal of SportsMedicine 25(5):656–658
Slemenda C, Heilman D K, Brandt K D et al 1998 Reduced quadricepsstrength relative to body weight. A risk factor for knee osteoarthritisin women? Arthritis and Rheumatism 41(11):1951–1959
Snyder-Mackler L, Ladin Z, Schepsis A A et al 1991 Electricalstimulation of the thigh muscles after reconstruction of the anteriorcruciate ligament. Effects of electrically elicited contractions of thequadriceps femoris and hamstring muscles on gait and on strengthof the thigh muscles. Journal of Bone and Joint Surgery (Am) 73-A(7):1025–1036
Snyder-Mackler L, De Luca P F, Williams P R et al 1994 Reflexinhibition of the quadriceps femoris muscle after injury orreconstruction of the anterior cruciate ligament. Journal of Bone andJoint Surgery (Am) 76-A(4):555–560
Snyder-Mackler L, Delitto A, Bailey S L et al 1995 Strength of thequadriceps femoris muscle and functional recovery afterreconstruction of the anterior cruciate ligament. A prospective,randomized clinical trial of electrical stimulation. Journal of Boneand Joint Surgery (Am) 77-A(8):1166–1173
Stuart M J, Meglan D A, Lutz G E et al 1996 Comparison ofintersegmental tibiofemoral joint forces and muscle activity duringvarious closed kinetic chain exercises. American Journal of SportsMedicine 24(6):792–799
Stürmer T, Klaus-Peter G, Brenner H 2000 Obesity, overweight andpatterns of osteoarthritis: the Ulm Osteoarthritis Study. Journal ofClinical Epidemiology 53:307–313
Suh J, Åroen A, Muzzonigro T et al 1997 Injury and repair of articularcartilage: related scientific issues. Operative Techniques inOrthopaedics 7(4):270–278
Tohyama H, Yasuda K, Kaneda K 1991 Treatment of osteoarthritis of the knee with heel wedges. International Orthopaedics15(1):31–33
Torg J S, Barton T M, Pavlov H et al 1989 Natural history of theposterior cruciate deficient knee. Clinical Orthopaedics and RelatedResearch 246:208–216
Veltri D M, Warren R F 1993 Isolated and combined posterior cruciateligament injuries. Journal of the American Academy of OrthopaedicSurgeons 1(2):67–75
Walker J M 1998 Pathomechanics and classification of cartilage lesions,facilitation of repair. Journal of Orthopaedics and Sports PhysicalTherapy 28(4):216–231
Ware J E Jr, Shelbourne C D 1992 The MOS 36-item short-form healthsurvey (SF-36). I. Conceptual framework and item selection. MedicalCare 30(6):473–483
Wilk K E 1994 Rehabilitation of isolated and combined posteriorcruciate ligament injuries. Clinics in Sports Medicine 13(3):649–677
398 REGIONAL SPORT AND EXERCISE INJURY MANAGEMENT
F07154-20.qxd 3/9/02 1:28 PM Page 398


















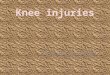










![Pathomechanics of the knee - Bowen University · The Knee joint [Revision] •Knee is the largest joint in the body •Involved in approximately 50% of musculoskeletal injuries…](https://img.dokumen.tips/doc/110x75/60864d9eeab92d257773be93/pathomechanics-of-the-knee-bowen-university-the-knee-joint-revision-aknee.jpg)