Embed Size (px)
Citation preview
King’s College Hospital Board of Directors PUBLIC AGENDA
Time of meeting 15:00 Date of meeting Tuesday 20 December 2011 Venue Dulwich Committee Room, King’s College Hospital Members: Prof. Sir George Alberti (GA) Chair Robert Foster (RF) Non-Executive Director Prof. Alan McGregor (AM) Non-Executive Director Graham Meek Non-Executive Director Marc Meryon (MM1) Non-Executive Director Christopher Stooke Non-Executive Director Tim Smart (TS) Chief Executive Angela Huxham (AH) Director of Workforce Development Dr. Michael Marrinan (MM) Medical Director Roland Sinker (RS) Director of Operations Simon Taylor (ST) Chief Financial Officer Dr. Geraldine Walters (GW) Director of Nursing & Midwifery Jane Walters (JW) - Non-voting Director Director of Corporate Affairs Jacob West (JW1) - Non-voting Director Director of Strategy
In attendance: Tamara Cowan (TC) Assistant Board Secretary (minutes) Sally Lingard (SL) Associate Director of Communications Judith Seddon (JS) Associate Director of Governance
Apologies Maxine James (MJ) Non-Executive Director
Circulation to Board of Directors Circulation List
Enclosure Lead Time
1. 1.1. Apologies G Alberti 15:00
1.2. Declarations of interest – to receive
1.3. Chair’s action
1.3.1. Chair Approval of Q3 Submission G Alberti
1.4. Minutes of previous meeting – 29/11/2011 Enc 1.4 G Alberti
1.5. Matters Arising/Action Tracking Enc 1.5 G Alberti
2. FOR REPORT/DISCUSSION
2.1. KHP Update Verbal J Moxham 15:10
2.2. Chair’s and Non-Executive Directors’ Report Enc 2.2 G Alberti 15:30
2.3. Chief Executive’s Report Enc 2.3 T Smart 15:35
2.4. Finance Report – Month 8 To follow S Taylor 15:45
2.5. Performance Report – Month 8 To follow R Sinker 16:00
2.6. Winter Resilience To follow R Sinker 16:15
2.7. Quality & Safety Focus:
2.7.1. Patient Experience Report Enc 2.7.1 J Walters 16:30
2.7.2. Eliminating Mixed Sex Accommodation Enc 2.7.2 G Walters 16:40
2.8. Outline of Key Matters arising from Council of Governors meeting on 01 December 2011
Enc 2.8 G Alberti 16.50
3. FOR INFORMATION
3.1. Declarations of Directors’ Interests Enc 3.1
4. ANY OTHER BUSINESS 16.55
5. DATE OF NEXT MEETING
Tuesday, 31 January 2012 at 14:30 in the Dulwich Committee Room
Enc 1.4
1
King’s College Hospital NHS Foundation Trust Board of Directors Minutes of the meeting of the Board of Directors held at 15.00 hrs on Tuesday, 29 November 2011 in the Dulwich Committee Room, King’s College Hospital.
Members: Michael Parker CBE (MP) Chair Prof. Sir George Alberti (GA) Non-Executive Directors Robert Foster (RF) Non-Executive Directors Maxine James (MJ) Non-Executive Directors Marc Meryon (MM1) Non-Executive Directors Prof. Alan McGregor (AM) Non-Executive Directors Tim Smart (TS) Chief Executive Angela Huxham (AH) Director of Workforce Development Dr. Michael Marrinan (MM) Medical Director Roland Sinker (RS) Director of Operations Simon Taylor (ST) Chief Financial Officer Dr. Geraldine Walters (GW) Director of Nursing & Midwifery Jane Walters (JW) - Non-voting Director Director of Corporate Affairs Jacob West (JW1) - Non-voting Director Director of Strategy In attendance: Prof. Robert Lechler (RL) Executive Director, KHP (Item 2.7) Frances O’Callaghan Director of Performance and Delivery (Item 2.7) Sally Lingard (SL) Associate Director of Communications Deputy Director, Integrated Care Pilot Maggie Kemmner Jim Lusby (JL Director, Integrated Care Pilot Tamara Cowan Assistant Board Secretary (minutes) Hedi Argent Governor Christine Klaassen Shadow Governor Ann Mullins Governor Barbara Pattinson Shadow Governor Michelle Pearce Governor Nanda Ratnavel Shadow Governor Mariangela Giombini King’s College Hospital Robert Lee King’s College London
Enc 1.4
2
Item
Subject Action
011/167 Apologies MM1 and JW1. The Chair welcomed all public attendees.
011/168 Declarations of Interest There were no declarations of interests raised.
011/169 Chair’s Action
Research Operational Capability Statement
MP circulated the King’s Research Operational Capability Statement. The Statement is the standardised form that each Trust must complete and post on their website, to show prospective investigators the various research interests and services that each Trust offers. This would enable researchers to identify which sites will be suitable for multi-centre studies. He advised he had signed-off the Statement and it would be available on the website, shortly.
011/170 Minutes from the meeting held on 25 October 2011 • Under 011/158, page 5, correct E&D is to read E&D’s; and • Under 011/161, page 8, remove the fourth bullet point, ‘This also
extends…’.
011/171 Matters Arising/ Action Tracker The action tracker was noted.
FOR REPORT/ DISCUSSION
011/172 Chairman and Non-Executive Directors’ (NEDs) Report The report of Chairman and NED activity for the period was noted.
Enc 1.4
3
Item
Subject Action
011/173 Chief Executive’s Report The Board noted the Chief Executive Report. TS noted that the Trust is moving into a new dawn with the impending departure of MP who had played a pivotal role in strengthening the Board and leading the Trust to its current position as a leading teaching hospital. GA will take over the role of Chair on 01 December coinciding with the start date of the new Governors as the Trust also says farewell to the departing Governors who have served the Trust well. TS advised that operationally the Trust was doing reasonably well. However, as a result of higher activity levels and not delivering 100% of the CIP plans the Trust was currently off its financial plan. Therefore in the coming weeks some difficult decisions will need to made but not at the cost of quality of patient care which will be safeguarded at all times.
011/174 Finance Report – Month 7 The Board noted and discussed the financial performance for the period. ST advised that for the first time this year the Trust had a deficit. This was the result of the Trust over performing, seeing more patients and the external economic environment. To improve the situation it is estimated that the Trust would have to reduce the current spend by £1m per month for the remainder of the financial year. Patient Safety remains paramount and would not be compromised under any circumstances but the Trust needed to make some difficult decisions about investment and discretionary expenditure. An interim action plan has been agreed which includes a review of divisional expenditure, agency spend and CIP targets, and proactive chasing of outstanding PCT payments. Given the resultant pressures on the capital programme the planned re - development of maternity is likely to be re-phased. Any failure to reduce the deficit position would place the Trust’s current Monitor risk rating of 3 at risk, which would have implications for the Trust’s regulatory position.
Enc 1.4
4
Item
Subject Action
011/174 Performance Report – Month 7 The Board noted the performance report for month 7. The Chair advised that the Finance and Performance Committee conducted an extensive review and discussion around the performance report earlier. The key issues arising from the report were:
• The Trust met all referral to treatment, cancer and the five ED indicator targets in the period;
• Healthcare acquired infection remains an area for concern:
o MRSA is ahead of trajectory; and o The C.diff target had been exceeded for Q3 but the
trajectory was improving. • How are we doing (HRWD) results below target; and • Change to a new national measure for mortality tracking.
011/1175 Patient Experience Report – Month 7 The Board noted the patient experience report for month 7.
• Two questions added to the HRWD survey this month on hand hygiene and care at night;
Key discussion points:
• The volunteer programme is underway and 200 new volunteers
have been recruited so far. Volunteers will be able spend time speaking to patients and help with the softer side of in patient care; and
• The Trust continues to work to improve the way it involves and
communicate with patients including, amongst other initiatives: o the Garnet patient experience training which 1000
members of staff have received; o ‘In Your Shoes’ events; and o Ward 20:20.
Enc 1.4
5
Item
Subject Action
011/176 Integrated Care Pilot The Board received and discussed the report on the Integrated Care Pilot (ICP). The Board commended the initiative noting that ICP would put people at the centre of their own care and would reduce the number of avoidable admissions to hospital. This would result in significant cost savings for the Trusts. The final decision would be sought from the KHP Board in the new year in the hope of implementing the pathway from April 2012. A significant challenge for ICP is getting the correct IT system in place to enable the joined-up working that is required for the success of the initiative. However a portal-based IT solution has already been identified address this issue before the roll out. In addition, an integrated management board would be established and strong clinical input would form the basis of the service.
011/177 KHP Update The Board received and noted the update on KHP activities from Prof. Robert Lechler and Frances O’Callaghan. The Clinical Academic Groups (CAGs) continued to make good progress. CAGs were focusing on cohesion of their leadership teams and strategic development. The CAGs that had been most successful are those with strong leadership and a focus on partnership working and co-operation. CAG 2 (Orthopaedics, Trauma, Emergency ENT and Plastics) had been approved for Modules 1 & 2 of the CAG accreditation programme. There are still challenges with getting some other CAGs through the full accreditation modules. Work is also under way to get GPs involved in CAGs in light of the forthcoming changes under the Health and Social Care Bill. It was agreed that: 1. NEDs would be sent information about Accreditation
Modules 1 & 2.
TC
Enc 1.4
6
Item
Subject Action
011/178 AOB
AH provided an update on the planned industrial action noting that a possible 100-150 trust staff had indicated they would strike. Some staff in Radiology, Imaging and Ophthalmology would also work to rule.
Day of Action
Although disruption was not expected to be widespread, there would be a limited number of cancellations of outpatient clinics, and patients affected had been notified.
011/179 Date of Next Meeting: Tuesday 20 December 2011, 3.00 pm - Dulwich Room.
Enc 1.5
CONFIDENTIAL
Enc_C1.5 – BoD Action Tracker – 20 December 2011 1
BOARD OF DIRECTORS PUBLIC SESSION
ACTION TRACKER UPDATE
20 December 2011 Date/Agenda Item Action By whom By when Status
NOT DUE
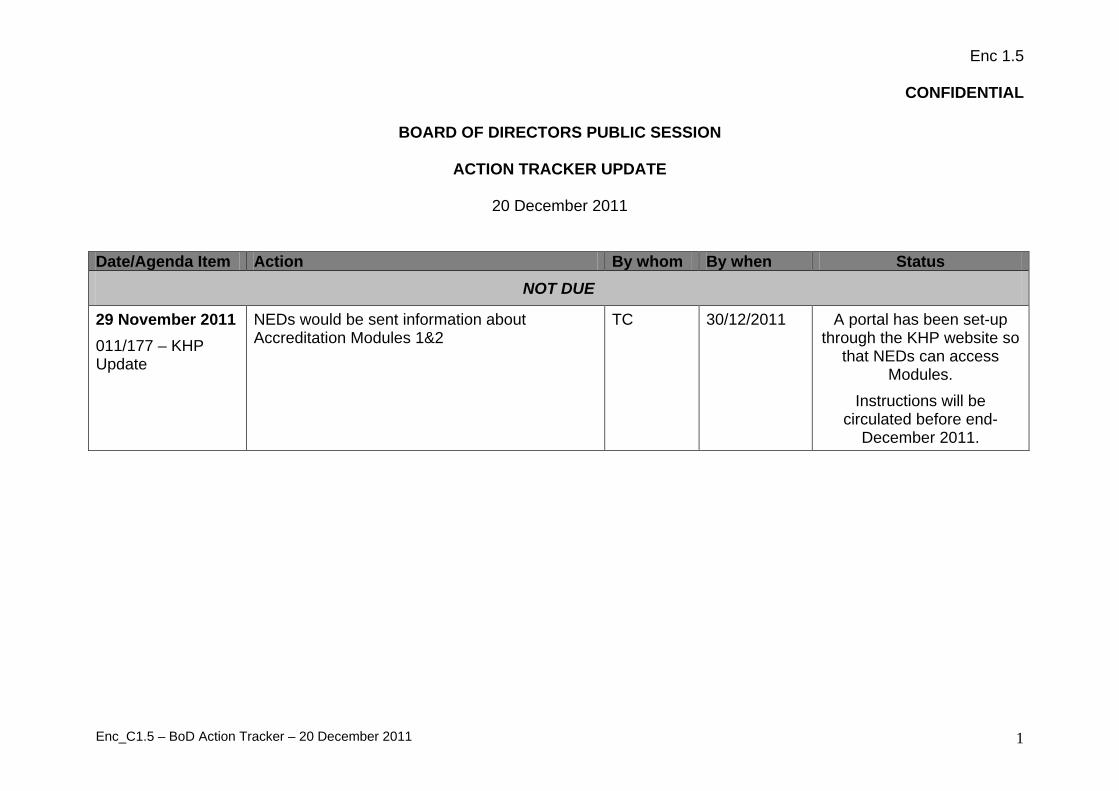
29 November 2011 011/177 – KHP Update
NEDs would be sent information about Accreditation Modules 1&2
TC 30/12/2011 A portal has been set-up through the KHP website so
that NEDs can access Modules.
Instructions will be circulated before end-
December 2011.

Enc 2.2
Report to:
King’s College Hospital Board of Directors
Date of meeting:
20th
By:
December 2011
Professor Sir George Alberti, Chairman
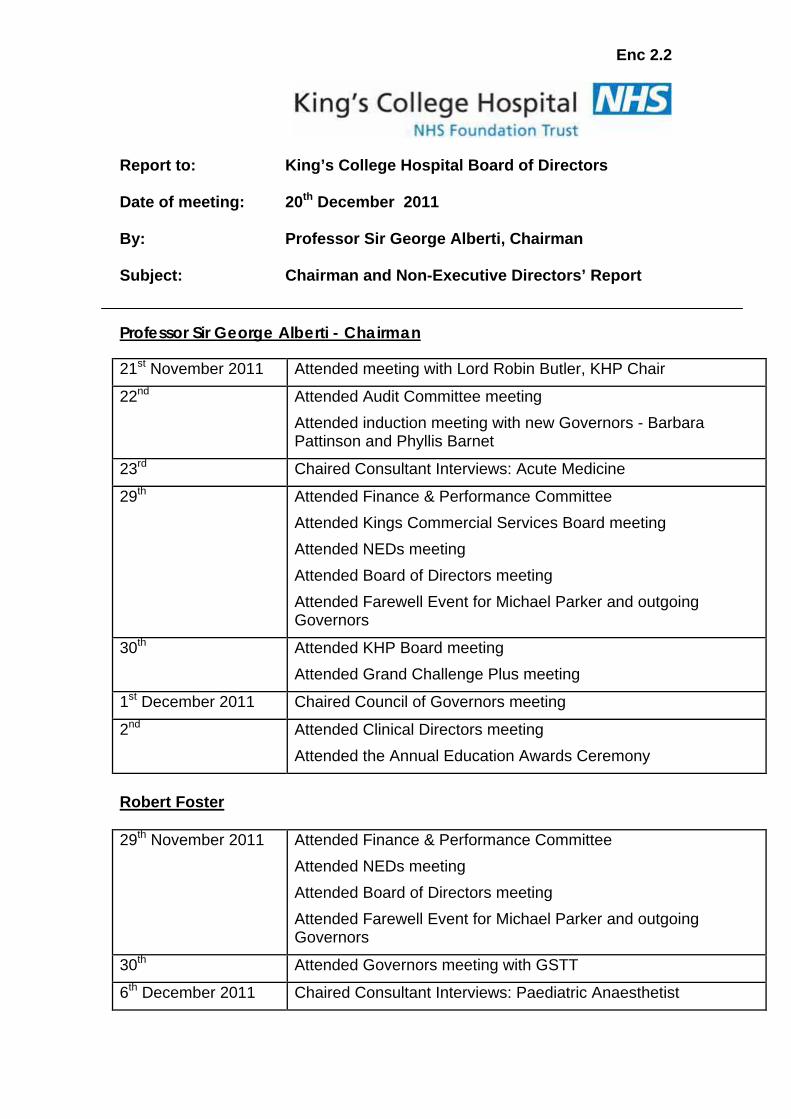
Subject: Chairman and Non-Executive Directors’ Report
Professor Sir George Alberti - Chairman 21st Attended meeting with Lord Robin Butler, KHP Chair November 2011
22nd Attended Audit Committee meeting Attended induction meeting with new Governors - Barbara Pattinson and Phyllis Barnet
23 Chaired Consultant Interviews: Acute Medicine rd
29 Attended Finance & Performance Committee th Attended Kings Commercial Services Board meeting Attended NEDs meeting Attended Board of Directors meeting Attended Farewell Event for Michael Parker and outgoing Governors
30 Attended KHP Board meeting th Attended Grand Challenge Plus meeting
1st Chaired Council of Governors meeting December 2011
2nd Attended Clinical Directors meeting Attended the Annual Education Awards Ceremony
Robert Foster 29th Attended Finance & Performance Committee November 2011
Attended NEDs meeting Attended Board of Directors meeting Attended Farewell Event for Michael Parker and outgoing Governors
30 Attended Governors meeting with GSTT th
6th Chaired Consultant Interviews: Paediatric Anaesthetist December 2011
Enc 2.2
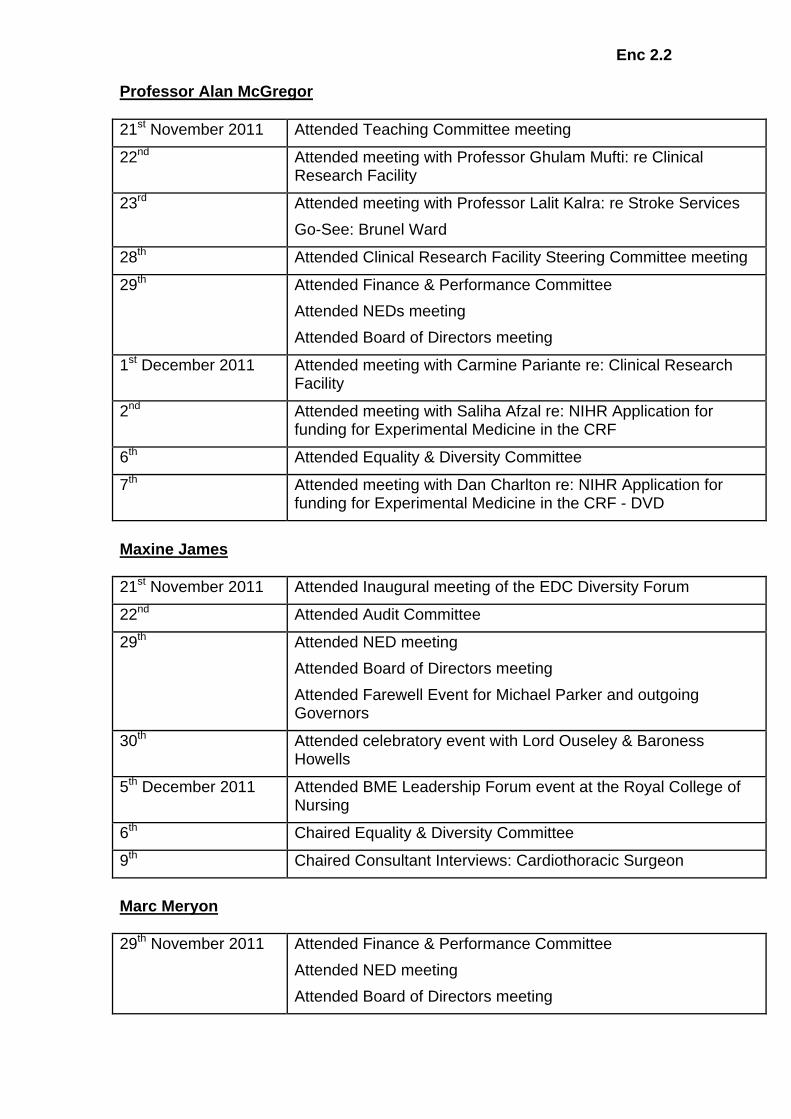
Professor Alan McGregor 21st Attended Teaching Committee meeting November 2011
22 Attended meeting with Professor Ghulam Mufti: re Clinical Research Facility
nd
23 Attended meeting with Professor Lalit Kalra: re Stroke Services rd Go-See: Brunel Ward
28 Attended Clinical Research Facility Steering Committee meeting th
29 Attended Finance & Performance Committee th Attended NEDs meeting Attended Board of Directors meeting
1st Attended meeting with Carmine Pariante re: Clinical Research Facility
December 2011
2 Attended meeting with Saliha Afzal re: NIHR Application for funding for Experimental Medicine in the CRF
nd
6 Attended Equality & Diversity Committee th
7 Attended meeting with Dan Charlton re: NIHR Application for funding for Experimental Medicine in the CRF - DVD
th
Maxine James 21st Attended Inaugural meeting of the EDC Diversity Forum November 2011
22 Attended Audit Committee nd
29 Attended NED meeting th Attended Board of Directors meeting Attended Farewell Event for Michael Parker and outgoing Governors
30 Attended celebratory event with Lord Ouseley & Baroness Howells
th
5th Attended BME Leadership Forum event at the Royal College of Nursing
December 2011
6th Chaired Equality & Diversity Committee
9 Chaired Consultant Interviews: Cardiothoracic Surgeon th
Marc Meryon 29th Attended Finance & Performance Committee November 2011
Attended NED meeting Attended Board of Directors meeting
Enc 2.2
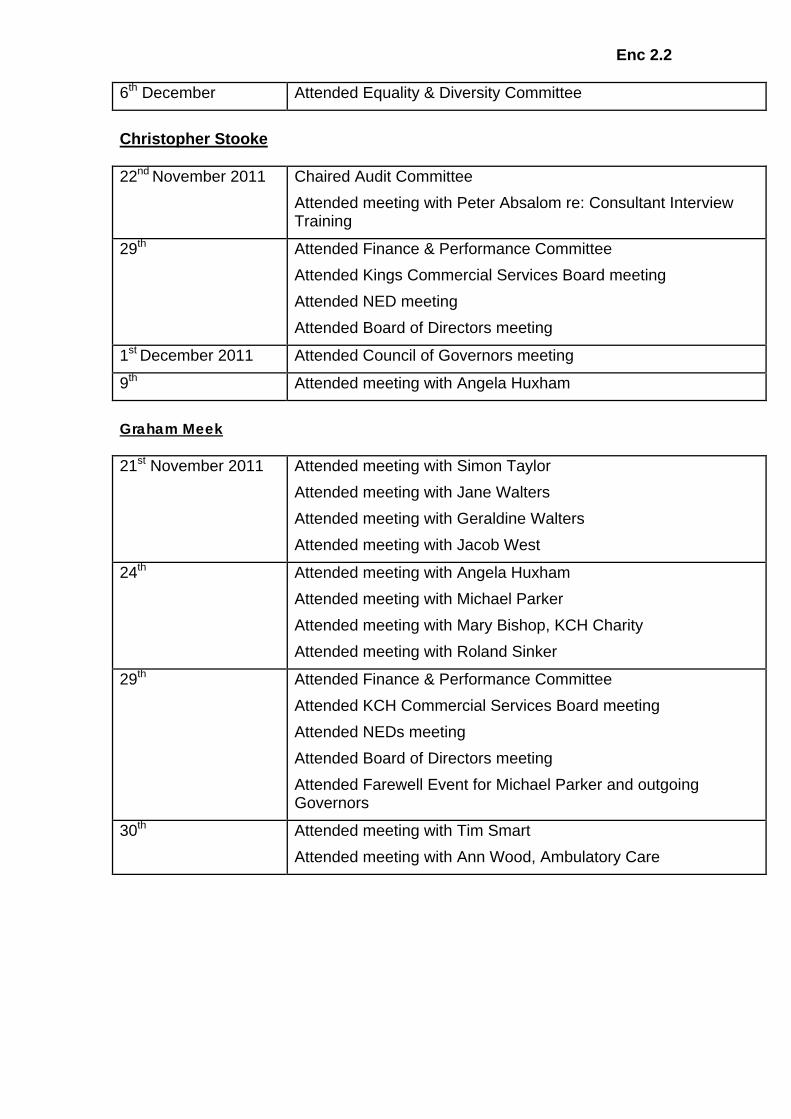
6th Attended Equality & Diversity Committee December
Christopher Stooke 22nd Chaired Audit Committee November 2011
Attended meeting with Peter Absalom re: Consultant Interview Training
29 Attended Finance & Performance Committee th Attended Kings Commercial Services Board meeting Attended NED meeting Attended Board of Directors meeting
1st Attended Council of Governors meeting December 2011
9 Attended meeting with Angela Huxham th
Graham Meek 21st Attended meeting with Simon Taylor November 2011
Attended meeting with Jane Walters Attended meeting with Geraldine Walters Attended meeting with Jacob West
24 Attended meeting with Angela Huxham th Attended meeting with Michael Parker Attended meeting with Mary Bishop, KCH Charity Attended meeting with Roland Sinker
29 Attended Finance & Performance Committee th Attended KCH Commercial Services Board meeting Attended NEDs meeting Attended Board of Directors meeting Attended Farewell Event for Michael Parker and outgoing Governors
30 Attended meeting with Tim Smart th Attended meeting with Ann Wood, Ambulatory Care

Enc 2.3
CEO Update December 2011 Page 1
Report to: Board of Directors Date of meeting: 20 December 2011 By: Tim Smart, Chief Executive Subject: Chief Executive’s Board Report 1. Executive Summary The festive period is almost upon us and I hope that all of you are making plans to rest and recharge at some point over Christmas and New Year. Many of you will be working, to keep our services going and our patients safe, and I thank you for that. However and whenever you celebrate the festive season, I wish you the very best. We are finding it hard to balance the high levels of activity with the need to achieve our budget for be year. Our CIP requires an acceleration of our efficiency programme to do that, at the same time as maintaining patient safety. Many of our peer organisations are struggling. There is a tough quarter coming up, financially and operationally, and we must be prepared to make difficult decisions; to question our expenditure and find ways of being more efficient whilst ‘always aiming higher’. It is very much this particular King’s Value that lies behind the review of King’s Health Partners and the feasibility study currently underway to help us decide the future direction of KHP and King’s. But I urge you not to be bowed by gloomy predictions or uncertainty. I have confidence in the team we have here at King’s. Recently this has been recognised more widely with awards for our Diabetes team, The Haven and for the Trust as a whole, which received a ‘Family Friendly’ award in recognition of our efforts to provide flexible working conditions, advice and cover for those with family commitments. The inaugural meeting of the Council of Governors reminded me of the positive contribution that can be made by Governors of different backgrounds and experience. 2012 will be a significant year for King’s, for the NHS and for London. I look forward to working together with Governors, a new Chairman and new Non-executive Directors, bringing fresh insight and energy as we anticipate the New Year and all the challenges it holds. 2. Finance – month 8 An update will be given at the Board of Directors meeting.
Enc 2.3
CEO Update December 2011 Page 2
3. Performance – month 8 Pressure has begun to intensify, as anticipated during winter months, but the Trust has continued to achieve against all of the referral to treatment and cancer wait access standards in month 8. The emergency 4 hour wait target for the 95th
percentile has also been maintained this month. The next few months will undoubtedly be challenging and we will need to manage this carefully.
We have not had an MRSA post 48 hour bacteraemia in month, keeping our year to date total at 3 against our quota of 6 for the year. However, C-difficile remains a significant concern. The number of cases is above trajectory with 71 reported in the first eight months of the year compared to our quota of 52. The independent review of antibiotic usage within the Trust was completed on 22
November. We are awaiting feedback from this review to inform improvements that we can make in this area.
4. Services for Older Patients On the 15 December I will be attending the launch of the transformed Marjory Warren Ward here at King’s. This celebration to mark the official opening is the culmination of two years work and the combined efforts of ward staff, specialists and the Facilities team to re-design the space in order to create a safe and stimulating environment specifically for patients with dementia. The Sensory Project has been supported by the King’s Fund, Friends of King’s and Dulwich Picture Gallery. Also in the month of December, the Older Person Assessment Unit will be transferred from Dulwich Community Hospital to the Denmark Hill site, additionally strengthening the services that we offer to older patients. 5. Strategy/ KHP Update
The Integrated Care Pilot team are preparing a bid to the GSTT Charity for funding to support full implementation of the pilot, with the first phase being to implement a new model of care for frail older people in Lambeth and Southwark. At the same time, a six month review of the Transformation Programme is being undertaken. At King’s, the Strategy and Operations teams are working together to develop an overarching capacity plan for the Trust. And more widely, the Strategy team are supporting children’s services across a number of commissioner led paediatric service reviews, including paediatric epilepsy surgery & paediatric neurosurgery (both National Specialist Commissioner led), and paediatric trauma and paediatric tertiary services (NHS London led).
Strategy
Discussions about a new provider cancer network (London Cancer Alliance) continue. Proposals will be presented to the Board early in the New Year.
Cancer
The strategy teams of the KHP partners are developing options regarding new external partnerships in the context of the government's desire to create "Academic Health Science Networks" across the country. The Goldsbrough feasibility study of
KHP
Enc 2.3
CEO Update December 2011 Page 3
KHP organisational form is currently underway, following on from the McKee review and will be a topic of discussion at the Joint KHP Governors meeting on 14 December, and Board meetings in January and beyond. 6. Capital, Estates & Facilities
Capital and Estates Projects
• Estate Condition Survey - The site condition survey has now been completed across all KCH estates. Data is being reviewed and report will be delivered to the Board early in 2012.
• Davidson Ward will be undergoing some essential maintenance work during December, including a full deep clean. The ward will be closed for approximately 3 weeks.
• Carbon Reduction Commitment (CRC) – King’s has performed well in the
Environment Agency’s energy efficiency scheme, appearing in the top 6% in all sectors. Out of 159 NHS organizations involved in the CRC King’s was ranked 9
th.
The current contract ends on the 30 March 2012 and will be extended for a period of 12 months. This is to allow for in depth planning, taking into account traffic restrictions and congestion, which are anticipated around the period of the London 2012 Olympics.
Patient Transport Services
7. Media & Events (16 November - 8 December 2011) Press and broadcast coverage 15 – 17 November – Extensive national and international broadcast and press coverage about Professor Anil Dhawan’s pioneering liver procedure performed at King’s. Professor Dhawan injected a nine month old baby with donor cells as a substitute for his ailing liver, enabling it to recover. 15 November – The Daily Mail reported on a new operation being trialled at King’s for the first time by neurosurgeon Mr Irfan Malik. The surgery is for patients with a range of back injuries, including slipped discs. The surgery is minimally invasive, and patients can leave the hospital on the same day they are operated on. 21 November – The Daily Mail published a letter from King’s counter-fraud manager Terry Smith following an article published the previous week saying that King’s – and other hospitals – turned a ‘blind eye’ to fraud within the NHS. In the letter, we made clear that we take cases of fraud very seriously, with many cases resulting in custodial sentences for those found guilty. We also explained that we work hard to develop a culture of counter-fraud at King’s.
Enc 2.3
CEO Update December 2011 Page 4
21 November – The Daily Telegraph reported on ground-breaking surgery carried out at King’s by maxilla-facial surgeon Mr Shaun Matthews. After a year of research, the surgery involved breaking patient Sandra Pearce’s jaw, and inserting a computer fashioned bespoke joint. This has enabled the patient to chew properly for the first time in twenty years. 30 November – The Nursing Standard published a three page article about the transformation of the Marjory Warren ward. The focus was on the efforts of King’s Dementia Nurse Specialist Emma Ouldred and her team, and the work that has been carried out over the last two years to convert the ward into a multi-sensory environment for dementia patients. 2 December – Dr Kosh Agarwal was interviewed on the BBC Radio London Breakfast Show about the effects of drinking on young people. The interview was part of the BBC Inside Out current affairs programme in which King’s is taking part, due to be broadcast on BBC One in the New Year. Events 2 December – A new recruitment section on King’s website was launched this month. The new site provides concise, easy to use information about current job vacancies at King’s and how to apply. It also provides information about the geography of the local area, as well as childcare, accommodation and cycle to work schemes. Coming up - On December 15, the new Marjory Warren ward will officially open, with representatives from King’s, the King’s Fund, Friends of King’s, as well as staff, patients and their relatives in attendance. 8. Consultant Appointments Specialty New/
Existing Appointee(s) Start Date
Paediatric Anaesthesia x 4 posts
2 x N 2 x E
Andrew Blevin Sanjay Saikia Mariangela Giombini Meera Kurup
Start dates in 2012 to be confirmed
Acute Medicine N Akash Saxena Start date in 2012 to be confirmed
9. Chief Executive’s Brief The CEO’s Brief for December is attached.
CHIEF EXECUTIVE’S
BRIEF December 2011 Issue 65
An update from the Chief Executive to all staff at King’s College Hospital
As yet, it hasn’t felt very seasonal, but by the time you read this, I hope it is. Christmas and the Festive Season is a time
of celebration for many of us, and it is a time for recharging and being with families and friends for all. If you are working
over this period; thank you. You make an enormous difference to those who need our services over Christmas.
As I write this, we have just heard the Chancellor in his Autumn statement limiting future public sector pay increases to
one percent, following on from a two year pay freeze. At the same time much of the public sector—including some of
our own staff— are on strike in protest against the proposed changes to public sector pensions. There can be no clearer
indication of the financial challenges that face us all in the short term. As the winter has started, and our need to be
more efficient has grown, it is clear that we will struggle to meet targets and budgets this year. We must not fail though,
and we must keep focusing on the basics of cost control, quality and patient safety. We have developed an accelerated
plan which my executive director colleagues will be cascading, but everyone must contribute. There is no room for any
discretionary expenditure. The preservation of jobs is far more important than attending a conference, for example.
We are all expecting an interesting time in the next few weeks as we consider the findings of the feasibility study that
has been commissioned into organisational options for KHP. Progress is being made in a number of areas, but the
Partners’ Board knows that there is a lot of frustration that organisational inefficiency is getting in the way of achieving
our potential. We will consult widely on the findings of the feasibility review in the New Year.
This will provide an interesting set of challenges for our new Chairman, our new Non-executive Directors, and our new
Council of Governors, all of whom I welcome with open arms and in anticipation of an exciting time ahead of us. This is
an opportunity to build on the achievements of the past and to have a brand new start. We are a world-leading
Academic Health Sciences Centre. We need to deliver better care to our local population, and we will play our part in the
reform of the local healthcare system. We think things are tough at King’s, but we are thought to be stronger and more
able than most to succeed. This is because of the excellence and diligence of so many of our staff.
There has been a lot of media coverage about some of our “stars” in recent weeks – the cardiac team, the trauma teams,
the liver team. The BBC piece about Professor Dhawan and his team’s treatment of a young boy from East London
echoed around the world as a living example of what translational research really is about. The groundbreaking
treatment that young boy received meant he did not have to have a liver transplant or to take anti-rejection drugs for
the rest of his life. The liver he would have received has benefited another patient.
Our new Resus department has opened in A+E. the largest in the country, it is a real achievement by the team that
during all the refurbishment we have met all our targets. And of course by now you may have heard the news that we
have agreed to the filming of two new series of ’24 Hours in A+E’; another testament to how highly we are viewed by the
world outside.
So against a backdrop of difficult performance and financial issues, which will take up most of the Board’s time, I hope
you still feel optimistic about the hospital. I know that for many colleagues times are tough, but the reason we work in
the NHS is because we want to make a contribution to those who need help more than we do. Let me finish by again
wishing everyone a Merry Christmas and Happy New Year, which I hope you will be able to celebrate in whichever way
you choose.
Tim Smart
Chief Executive
An update from the Chief Executive to all staff at King’s College Hospital
24 Hours in A&E
Channel 4 is returning to King’s in the New Year to make a
further two series of 24 Hours in A&E.
The public and critical response to series 1 was positive.
More importantly, it provided us with a unique opportunity
to educate the public about the services we provide, and
the commitment and dedication of our staff.
As previously, safeguards will be put in place to protect the
privacy and dignity of our patients, as well as staff taking
part in the series. Further information will be circulated on
Kingsweb and via clinical teams in the coming weeks.
We are keen to feature as many hospital services as
possible in the series, although there will always need to be
a strong A&E link. If you want to discuss your potential
involvement in the series, or require further information,
please contact Chris Rolfe in communications on x 3006.
Compulsory defibrillator training for all clinical staff
As you should already know, the defibrillators currently
used at King’s are being replaced by the new Zoll
defibrillators. The Resuscitation Training Department will
be providing defibrillation training for the new ZOLL
defibrillators from Monday 28 November for two weeks.
Each day, there will be a 'drop-in' centre from 8am until
5pm, on the hour, every hour.
The training is compulsory for all clinical staff – the new
defibrillators will be deployed at the end of the two week
training. Dates and locations for the training can be found
on Kingsweb (link)
Olympic and Paralympic Games - volunteering and
attendance
King’s staff expecting to volunteer at the Olympic or
Paralympic games should give their managers as much
notice as possible of any leave requirements. Staff must
notify their managers if they have applied to be a volunteer,
and confirm if/when they have been accepted. Staff must
then apply for leave promptly once the volunteer training
dates and the volunteer duty dates are known.
Staff wishing to take leave in the period 27 July – 9
September 2012 should submit requests to their line
manager as soon as possible, but not later than 1 May 2012.
To ensure that as many staff as possible can take leave
over this period, requests should be restricted to a
maximum of 2 weeks (either taken as blocks or in days)
during the period 27 July – 9 September 2012. If for any
reason more than two weeks leave is requested this will
need to be approved by the Divisional Manager/Corporate
Head. All leave requests will be granted at their manager’s
discretion.
Further information about King’s preparation for London
2012 will be publicised on Kingsweb in the coming weeks.
Staff survey deadline approaching
Were you one of the 850 people selected to complete the
staff attitude survey this year? If you received the survey in
October, and haven't completed it yet, you will be getting
another copy in the internal mail this week.
The survey asks for your views about your job and working
for this Trust. The overall aim is to gather information that
will help us to improve the working lives of staff and so
provide better care for patients.
If you were one of those selected, please let us know your
views on working at King's by completing and returning this
confidential survey. All staff who participate will be entered
into a free prize draw to win Marks and Spencer's gift
vouchers, 1st
prize £100 and a runner up prize of £50. The
deadline for completing and returning surveys is 16th
December 2011. Results will be out early in 2012.
For further information please contact Jane Matty HR
Manager via [email protected] or see the National Staff
Survey Q&As page on Kwiki.
King’s has won a number of awards recently.
Our diabetes team won gold in the ‘Community Initiative of
the Year’ award at this year’s Quality in Care (QIC) awards.
The award was for our ‘3 Dimensions of Care for
Diabetes’ (3DFD) initiative, which is designed to increase
the effectiveness of medical treatment by addressing the
psychological and social needs of people with diabetes. The
initiative also won silver in the ‘Best integrated care
initiative’ category.
The Haven Sexual Assault Referral Centre at King’s was
successful at the British Arrows Craft Awards for its film
‘Where is your line?’ launched last year. The interactive film
– which looks at people’s attitudes towards sex and consent
– won in the following categories: Best Overall Production,
Best Director, Best Actress, Best Editing. The film was a joint
effort by the London Havens, the Metropolitan Police, and
production company Youth Club.
Trust Christmas party
On Tuesday, December 13, the Trust will be holding its
annual Christmas drinks in the Board room. The event starts
at 5pm and is open to all members of staff – drinks and
mince pies will be served.
Date of last MRSA bacteraemia: 10 September 2011
Clinical area: Davidson ward
Cause: Poor management of Hickman line insertion/
ongoing management.

Finance Report
Month 8 (November) 2011/12
Board of Directors Meeting 20th December 2011
Enc. 2.4

Page 2
Month 8 Executive Financial Summary Income and Expenditure – At month 8 (November), the Trust’s position is a deficit of £1,048k, against a surplus plan of £1.75m.
This is a negative variance from plan of £2.798m.
The Trust’s budget is phased to build up a surplus target towards quarter 3 in order to cover the remaining dividend payment (£4.2m) and potential asset impairments (£2.7m) in quarter 4. The asset impairment will be based on the completed capital projects for the upgraded Waddington and Private Patients Wards.
The Monitor Rating for month 8 is 3 in line with the Annual Plan target rating. The underlying performance (EBITDA margin) of 3 is
due to the deficit position and this is driving the reduced liquidity financial ratio of 2. Payment for Emergency Re-admission monies and Project Diamond monies will improve the cash-flow ; but expenditure reduction is required to improve the ratings.
Annual Budget YTD Budget YTD ActualMonth 8 YTD
VarianceMonth 7 YTD
VarianceMovement in
Month£'000 £'000 £'000 £'000 £'000 £'000
Income 598,070 397,109 407,890 10,781 8,965 1,816Pay (341,852) (228,098) (232,718) (4,620) (4,189) (431)Non-Pay (236,600) (156,638) (164,482) (7,844) (6,423) (1,421)Capital Charges (17,711) (10,424) (11,431) (1,007) (885) (122)Recharges (107) (199) (307) (108) 478 (586)
Total 1,800 1,750 (1,048) (2,798) (2,054) (744) Operating Financial Performance - A detailed forecast analysis looking at a mid-case case scenario would result in a £3m
deficit for the Trust, including asset impairments of £2.7m (Net operating deficit £0.3m). A number of key actions have been developed as part of a short term recovery plan to deliver this position; ranging from beds and main theatre/day surgery efficiencies; and strict financial controls to ensure only essential expenditure is incurred over last quarter.
Scenario Forecast Worst Case Mid Case Best Case
Total projected Deficit (£’000) (4,671) (2,956) (1,153)
Less Impairment (£’000) 2,700 2,700 2,700
EBITDA (Deficit)/Surplus (£’000) (1,971) (256) 1,547
Page 3
Month 8 Executive Financial Summary
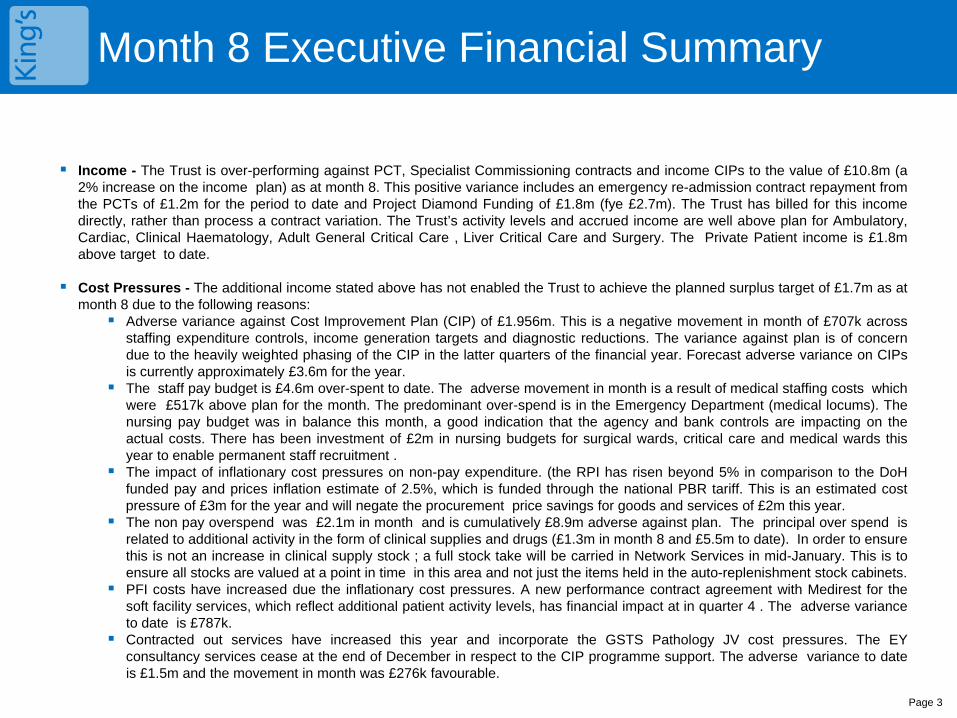
Income - The Trust is over-performing against PCT, Specialist Commissioning contracts and income CIPs to the value of £10.8m (a 2% increase on the income plan) as at month 8. This positive variance includes an emergency re-admission contract repayment from the PCTs of £1.2m for the period to date and Project Diamond Funding of £1.8m (fye £2.7m). The Trust has billed for this income directly, rather than process a contract variation. The Trust’s activity levels and accrued income are well above plan for Ambulatory, Cardiac, Clinical Haematology, Adult General Critical Care , Liver Critical Care and Surgery. The Private Patient income is £1.8m above target to date.
Cost Pressures - The additional income stated above has not enabled the Trust to achieve the planned surplus target of £1.7m as at month 8 due to the following reasons: Adverse variance against Cost Improvement Plan (CIP) of £1.956m. This is a negative movement in month of £707k across
staffing expenditure controls, income generation targets and diagnostic reductions. The variance against plan is of concern due to the heavily weighted phasing of the CIP in the latter quarters of the financial year. Forecast adverse variance on CIPs is currently approximately £3.6m for the year.
The staff pay budget is £4.6m over-spent to date. The adverse movement in month is a result of medical staffing costs which were £517k above plan for the month. The predominant over-spend is in the Emergency Department (medical locums). The nursing pay budget was in balance this month, a good indication that the agency and bank controls are impacting on the actual costs. There has been investment of £2m in nursing budgets for surgical wards, critical care and medical wards this year to enable permanent staff recruitment .
The impact of inflationary cost pressures on non-pay expenditure. (the RPI has risen beyond 5% in comparison to the DoH funded pay and prices inflation estimate of 2.5%, which is funded through the national PBR tariff. This is an estimated cost pressure of £3m for the year and will negate the procurement price savings for goods and services of £2m this year.
The non pay overspend was £2.1m in month and is cumulatively £8.9m adverse against plan. The principal over spend is related to additional activity in the form of clinical supplies and drugs (£1.3m in month 8 and £5.5m to date). In order to ensure this is not an increase in clinical supply stock ; a full stock take will be carried in Network Services in mid-January. This is to ensure all stocks are valued at a point in time in this area and not just the items held in the auto-replenishment stock cabinets.
PFI costs have increased due the inflationary cost pressures. A new performance contract agreement with Medirest for the soft facility services, which reflect additional patient activity levels, has financial impact at in quarter 4 . The adverse variance to date is £787k.
Contracted out services have increased this year and incorporate the GSTS Pathology JV cost pressures. The EY consultancy services cease at the end of December in respect to the CIP programme support. The adverse variance to date is £1.5m and the movement in month was £276k favourable.
Page 4
Month 8 Executive Financial Summary
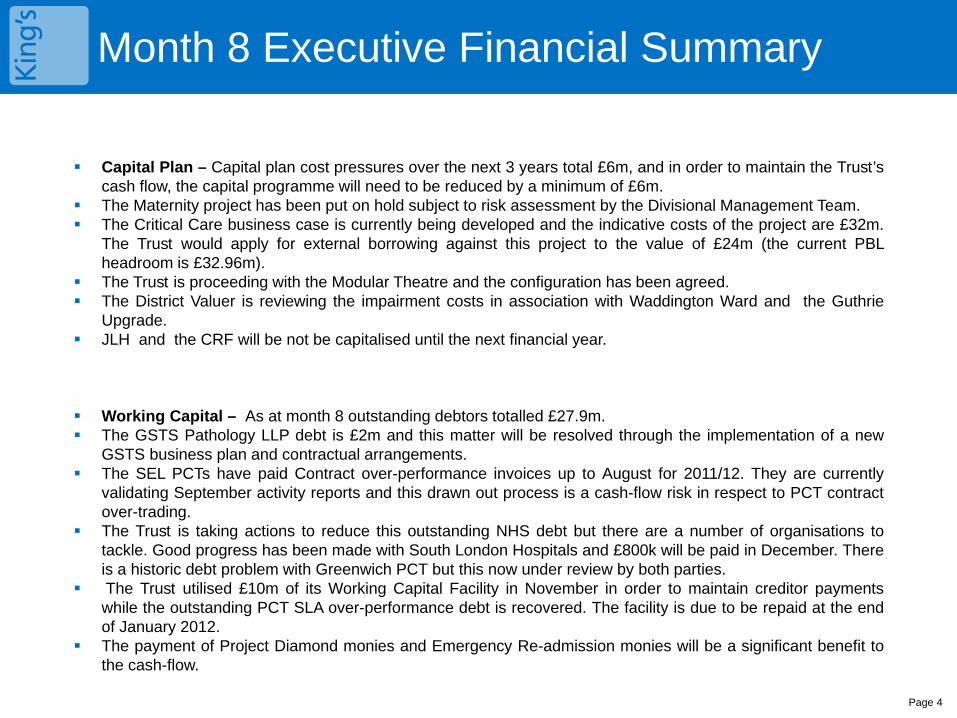
Capital Plan – Capital plan cost pressures over the next 3 years total £6m, and in order to maintain the Trust’s
cash flow, the capital programme will need to be reduced by a minimum of £6m. The Maternity project has been put on hold subject to risk assessment by the Divisional Management Team. The Critical Care business case is currently being developed and the indicative costs of the project are £32m.
The Trust would apply for external borrowing against this project to the value of £24m (the current PBL headroom is £32.96m).
The Trust is proceeding with the Modular Theatre and the configuration has been agreed. The District Valuer is reviewing the impairment costs in association with Waddington Ward and the Guthrie
Upgrade. JLH and the CRF will be not be capitalised until the next financial year.
Working Capital – As at month 8 outstanding debtors totalled £27.9m. The GSTS Pathology LLP debt is £2m and this matter will be resolved through the implementation of a new
GSTS business plan and contractual arrangements. The SEL PCTs have paid Contract over-performance invoices up to August for 2011/12. They are currently
validating September activity reports and this drawn out process is a cash-flow risk in respect to PCT contract over-trading.
The Trust is taking actions to reduce this outstanding NHS debt but there are a number of organisations to tackle. Good progress has been made with South London Hospitals and £800k will be paid in December. There is a historic debt problem with Greenwich PCT but this now under review by both parties.
The Trust utilised £10m of its Working Capital Facility in November in order to maintain creditor payments while the outstanding PCT SLA over-performance debt is recovered. The facility is due to be repaid at the end of January 2012.
The payment of Project Diamond monies and Emergency Re-admission monies will be a significant benefit to the cash-flow.
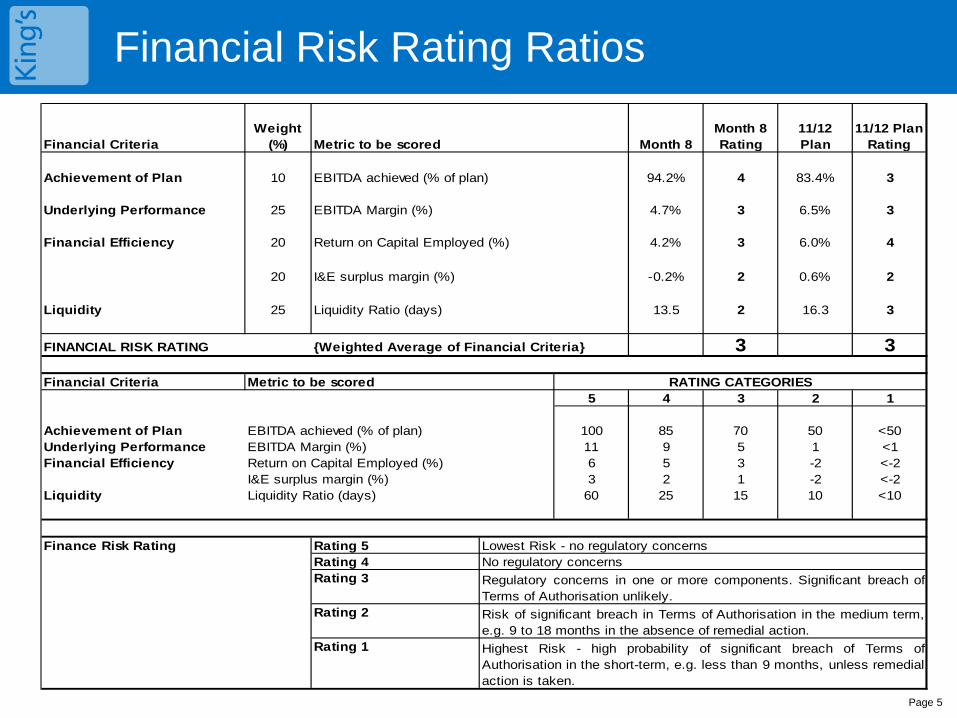
Financial Risk Rating Ratios
Page 5
Financial CriteriaWeight
(%) Metric to be scored Month 8Month 8 Rating
11/12 Plan
11/12 Plan Rating
Achievement of Plan 10 EBITDA achieved (% of plan) 94.2% 4 83.4% 3
Underlying Performance 25 EBITDA Margin (%) 4.7% 3 6.5% 3
Financial Efficiency 20 Return on Capital Employed (%) 4.2% 3 6.0% 4
20 I&E surplus margin (%) -0.2% 2 0.6% 2
Liquidity 25 Liquidity Ratio (days) 13.5 2 16.3 3
FINANCIAL RISK RATING {Weighted Average of Financial Criteria} 3 3
Financial Criteria Metric to be scored5 4 3 2 1
Achievement of Plan EBITDA achieved (% of plan) 100 85 70 50 <50Underlying Performance EBITDA Margin (%) 11 9 5 1 <1Financial Efficiency Return on Capital Employed (%) 6 5 3 -2 <-2
I&E surplus margin (%) 3 2 1 -2 <-2Liquidity Liquidity Ratio (days) 60 25 15 10 <10
Finance Risk Rating Rating 5Rating 4Rating 3
Rating 2
Rating 1
Risk of significant breach in Terms of Authorisation in the medium term,e.g. 9 to 18 months in the absence of remedial action.Highest Risk - high probability of significant breach of Terms ofAuthorisation in the short-term, e.g. less than 9 months, unless remedialaction is taken.
RATING CATEGORIES
Regulatory concerns in one or more components. Significant breach ofTerms of Authorisation unlikely.
No regulatory concernsLowest Risk - no regulatory concerns
Financial Forecast for 2011/12
Page 6
Basis for deriving Financial Forecast Actual expenditure has been examined by each individual budget line by finance
managers in conjunction with Divisional leads and Heads of Department. Projected figures for Months 9-12 have been compared to current budget spend.
M8 Year to date actuals were used as a starting point.
Months 9-12 – assumed an average of months 3-7 to extrapolate forward.
Finance managers have then adjusted the straight line forecast based on:
CIPs which are yet to impact, taking a risk adjusted view as to how much will be achieved.
Non-recurring spend (one-offs) in previous months which skew the average Known cost pressures – such as winter pressures beds, PFI etc. Income is generally straight-line projected unless there is known to be
additional income arriving. Position has all major risks covered and is prudent. The Division’s will now be expected to meet these mid-case targets at
minimum.
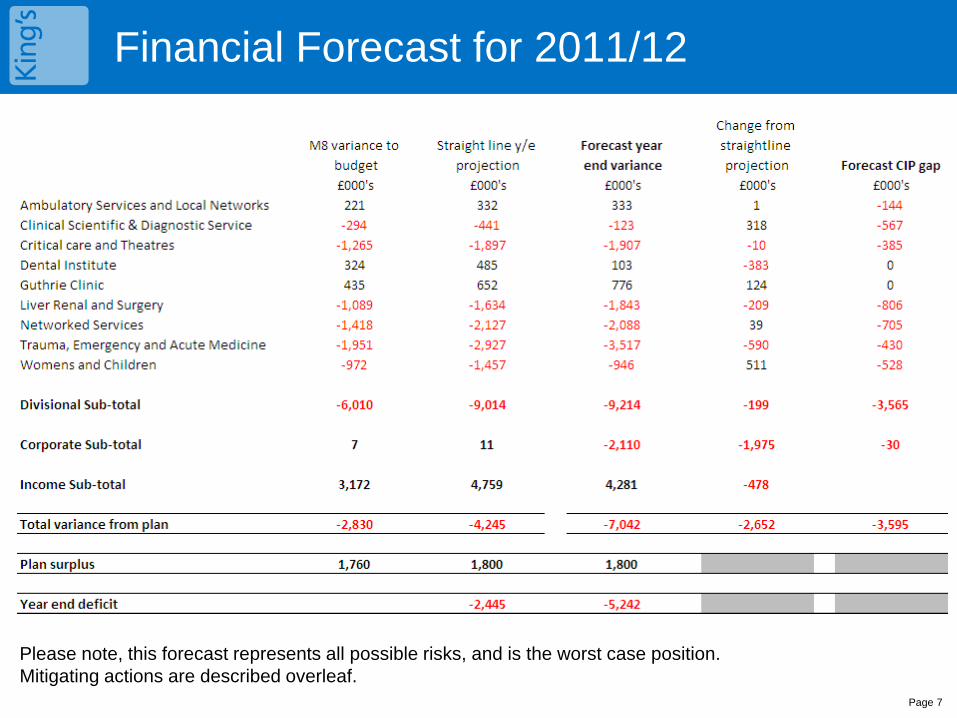
Page 7
Please note, this forecast represents all possible risks, and is the worst case position. Mitigating actions are described overleaf.
Financial Forecast for 2011/12
Financial Forecast for 2011/12
Reasons for variation from straightline M8 financial forecast • CSDS £318k favourable movement – additional income from Blood products re- bate. • Dental institute £383k adverse – contingencies for claw-backs on underperformance on training monies (Dental Care Professionals).
• Liver Renal and surgery £209k adverse – additional emergency activity through winter pressures.
• TEAM - £590k adverse – additional winter pressure beds to be opened. This will be a cost pressure as there will be no additional income to cover this work. The PCT contracts for emergency work are capped at a 2008/9 baseline level.
• Women’s and Children’s - £511k favourable – this is due to the ability to charge for additional NICU spells which will improve income over the final quarter.
• Corporate - £1.975m adverse – additional PFI costs, External Consultancy costs, KHP costs; Provision for bad debts and Research and Education investment commitments.
Financial Forecast for 2011/12
Page 9
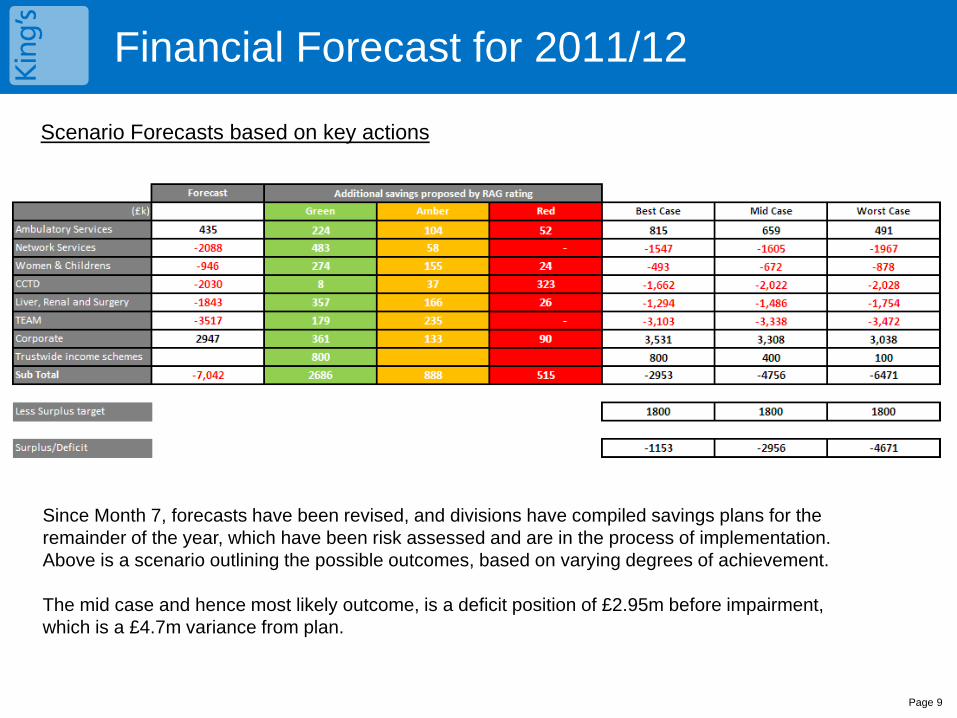
Scenario Forecasts based on key actions
Since Month 7, forecasts have been revised, and divisions have compiled savings plans for the remainder of the year, which have been risk assessed and are in the process of implementation. Above is a scenario outlining the possible outcomes, based on varying degrees of achievement. The mid case and hence most likely outcome, is a deficit position of £2.95m before impairment, which is a £4.7m variance from plan.
Financial Forecast for 2011/12
Key Divisional savings plans • Ambulatory – Additional Dental activity in line with demand, Staff vacancy slippages, reductions in radiology and pathology recharges.
•Networked – Additional Cardiac and BMT income, backdated staff recharges against R&D income streams.
•W&C – Various additional income schemes such as NICU.
•CCTDS – Reduction in drugs spend across the Trust and a reduction in temporary staffing spend.
•LRS – Additional income schemes, reduction in medical staffing temporary spend.
•TEAM – Reduction in temporary staffing spend. Medical Locum reduction as CDU is transferred back to ED. Short –term Consultant contracts to reduce locum demand. •Trustwide income schemes – these are additional PP activity, Day surgery increased usage, Bariatric waiting list initiatives. Implementation timing is the key risk.
Page 11
Key Trustwide Income and Expenditure Variances
Income for the year to date is £10.8m above target, a favourable movement of £1.8m from month 8. Networked services income over-performance is £1.4m and Private Patients is £1.8m. Corporate income is favourable due to the unplanned income from Project Diamond and The Emergency Re-Admission monies.
Pay overall is £4.6m overspent, an adverse movement of £417k. This is driven by overspends on nursing staff of
£3.2m, shown in Critical Care (£1.49m), Liver Renal and Surgery (£223k), TEAM (£183k) and Women's & Children's (£1.053m). Staff recruitment delays in Critical Care services have driven high agency costs along with the increased patient volume and acuity. Since Month 7, recruitment has been successful so agency spend has fallen, and this is expected to continue. Similarly in Child Health, increased NICU and PICU activity is driving increased Bank and Agency staff costs. The other overspend and movement is in Medical staffing (£2.29m) – with £1.2m overspent in TEAM due to Agency Locums to cover vacancies in ED and CDU.
Non-Pay is £8.9m overspent year to date, an adverse movement of £2.1m as follows; Clinical supplies (£3.6m), overspends are seen across most clinical areas, and relate to both increased
activity, and unmet CIP’s. Price inflation above Treasury estimates is having an adverse impact in this area. Drugs (£1.86m), this is predominantly driven by increased expenditure in Haematology relating to Eculizumab,
for which income is recovered as an off-tariff drug. Non-clinical supplies (£1.86m), which relates to Advertising, Utility Costs including the Carbon Reduction
Commitment and Patient Transport services. The PFI contract (£787k) is due to contract variation costs for cleaning new areas and increased patient
numbers. The revised Medirest performance agreement will continue to impact in quarter 3 and 4. Miscellaneous cost moved favourably by £276k in month. Capital Charges (Depreciation) are lower than planned due to slippage on the capital programme and these
are off setting the loss of planned proceeds due to the postponement of the sale of Jennie Lee House.
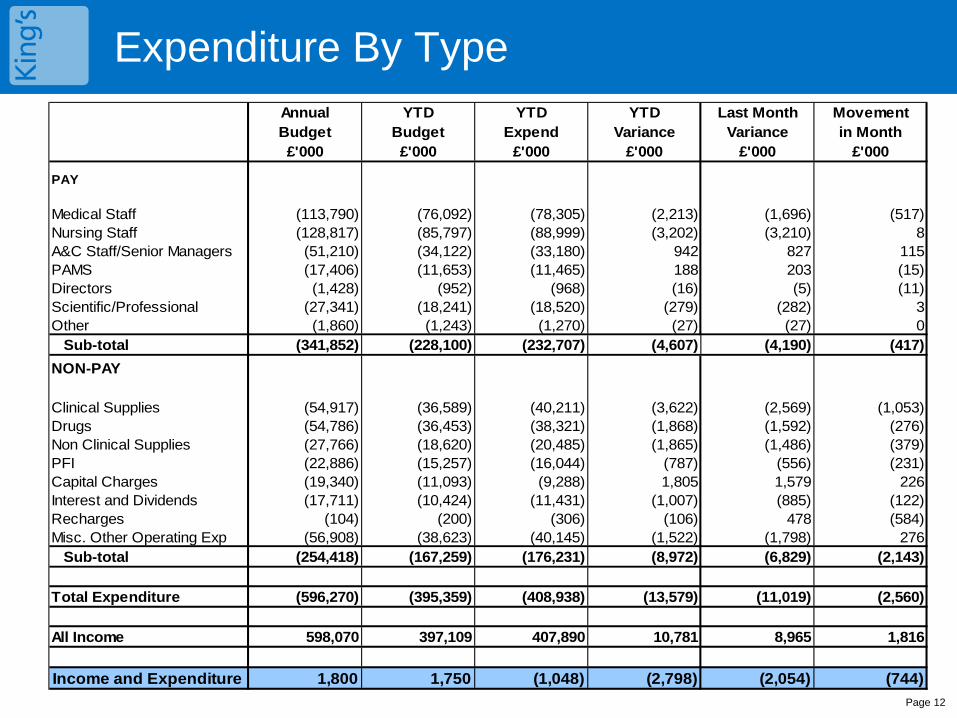
Expenditure By Type
Page 12
Annual YTD YTD YTD Last Month MovementBudget Budget Expend Variance Variance in Month£'000 £'000 £'000 £'000 £'000 £'000
PAY
Medical Staff (113,790) (76,092) (78,305) (2,213) (1,696) (517)Nursing Staff (128,817) (85,797) (88,999) (3,202) (3,210) 8A&C Staff/Senior Managers (51,210) (34,122) (33,180) 942 827 115PAMS (17,406) (11,653) (11,465) 188 203 (15)Directors (1,428) (952) (968) (16) (5) (11)Scientific/Professional (27,341) (18,241) (18,520) (279) (282) 3Other (1,860) (1,243) (1,270) (27) (27) 0
Sub-total (341,852) (228,100) (232,707) (4,607) (4,190) (417)NON-PAY
Clinical Supplies (54,917) (36,589) (40,211) (3,622) (2,569) (1,053)Drugs (54,786) (36,453) (38,321) (1,868) (1,592) (276)Non Clinical Supplies (27,766) (18,620) (20,485) (1,865) (1,486) (379)PFI (22,886) (15,257) (16,044) (787) (556) (231)Capital Charges (19,340) (11,093) (9,288) 1,805 1,579 226Interest and Dividends (17,711) (10,424) (11,431) (1,007) (885) (122)Recharges (104) (200) (306) (106) 478 (584)Misc. Other Operating Exp (56,908) (38,623) (40,145) (1,522) (1,798) 276
Sub-total (254,418) (167,259) (176,231) (8,972) (6,829) (2,143)
Total Expenditure (596,270) (395,359) (408,938) (13,579) (11,019) (2,560)
All Income 598,070 397,109 407,890 10,781 8,965 1,816
Income and Expenditure 1,800 1,750 (1,048) (2,798) (2,054) (744)
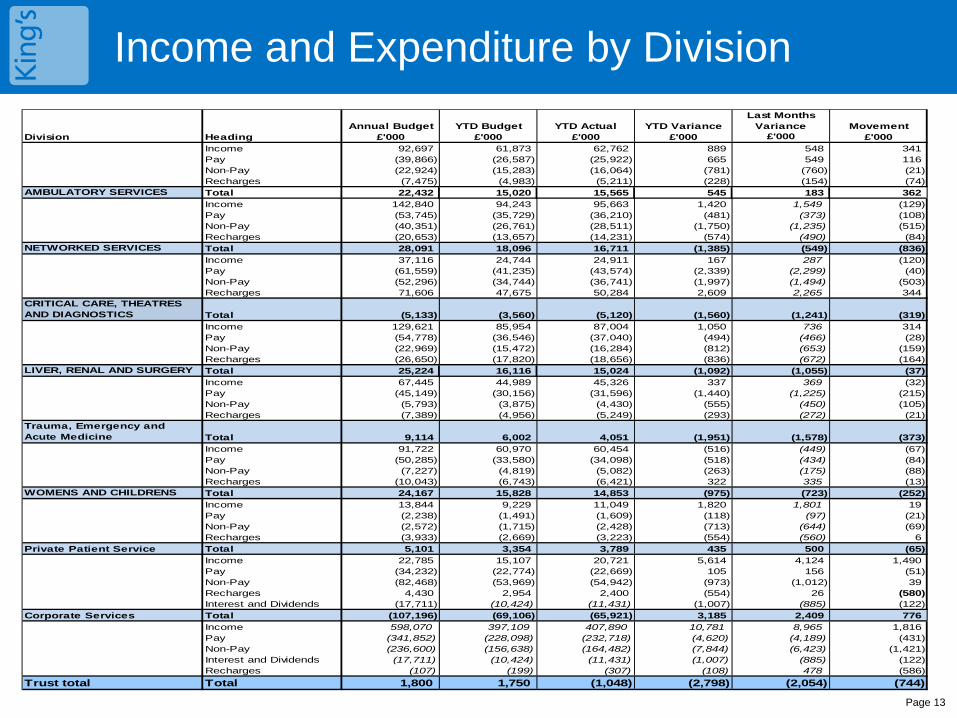
Income and Expenditure by Division
Page 13
Annual Budget YTD Budget YTD Actual YTD VarianceLast Months
Variance MovementDivision Heading £'000 £'000 £'000 £'000 £'000 £'000
Income 92,697 61,873 62,762 889 548 341Pay (39,866) (26,587) (25,922) 665 549 116Non-Pay (22,924) (15,283) (16,064) (781) (760) (21)Recharges (7,475) (4,983) (5,211) (228) (154) (74)
AMBULATORY SERVICES Total 22,432 15,020 15,565 545 183 362Income 142,840 94,243 95,663 1,420 1,549 (129)Pay (53,745) (35,729) (36,210) (481) (373) (108)Non-Pay (40,351) (26,761) (28,511) (1,750) (1,235) (515)Recharges (20,653) (13,657) (14,231) (574) (490) (84)
NETWORKED SERVICES Total 28,091 18,096 16,711 (1,385) (549) (836)Income 37,116 24,744 24,911 167 287 (120)Pay (61,559) (41,235) (43,574) (2,339) (2,299) (40)Non-Pay (52,296) (34,744) (36,741) (1,997) (1,494) (503)Recharges 71,606 47,675 50,284 2,609 2,265 344
CRITICAL CARE, THEATRES AND DIAGNOSTICS Total (5,133) (3,560) (5,120) (1,560) (1,241) (319)
Income 129,621 85,954 87,004 1,050 736 314Pay (54,778) (36,546) (37,040) (494) (466) (28)Non-Pay (22,969) (15,472) (16,284) (812) (653) (159)Recharges (26,650) (17,820) (18,656) (836) (672) (164)
LIVER, RENAL AND SURGERY Total 25,224 16,116 15,024 (1,092) (1,055) (37)Income 67,445 44,989 45,326 337 369 (32)Pay (45,149) (30,156) (31,596) (1,440) (1,225) (215)Non-Pay (5,793) (3,875) (4,430) (555) (450) (105)Recharges (7,389) (4,956) (5,249) (293) (272) (21)
Trauma, Emergency and Acute Medicine Total 9,114 6,002 4,051 (1,951) (1,578) (373)
Income 91,722 60,970 60,454 (516) (449) (67)Pay (50,285) (33,580) (34,098) (518) (434) (84)Non-Pay (7,227) (4,819) (5,082) (263) (175) (88)Recharges (10,043) (6,743) (6,421) 322 335 (13)
WOMENS AND CHILDRENS Total 24,167 15,828 14,853 (975) (723) (252)Income 13,844 9,229 11,049 1,820 1,801 19Pay (2,238) (1,491) (1,609) (118) (97) (21)Non-Pay (2,572) (1,715) (2,428) (713) (644) (69)Recharges (3,933) (2,669) (3,223) (554) (560) 6
Private Patient Service Total 5,101 3,354 3,789 435 500 (65)Income 22,785 15,107 20,721 5,614 4,124 1,490Pay (34,232) (22,774) (22,669) 105 156 (51)Non-Pay (82,468) (53,969) (54,942) (973) (1,012) 39Recharges 4,430 2,954 2,400 (554) 26 (580)Interest and Dividends (17,711) (10,424) (11,431) (1,007) (885) (122)
Corporate Services Total (107,196) (69,106) (65,921) 3,185 2,409 776Income 598,070 397,109 407,890 10,781 8,965 1,816Pay (341,852) (228,098) (232,718) (4,620) (4,189) (431)Non-Pay (236,600) (156,638) (164,482) (7,844) (6,423) (1,421)Interest and Dividends (17,711) (10,424) (11,431) (1,007) (885) (122)Recharges (107) (199) (307) (108) 478 (586)
Trust total Total 1,800 1,750 (1,048) (2,798) (2,054) (744)
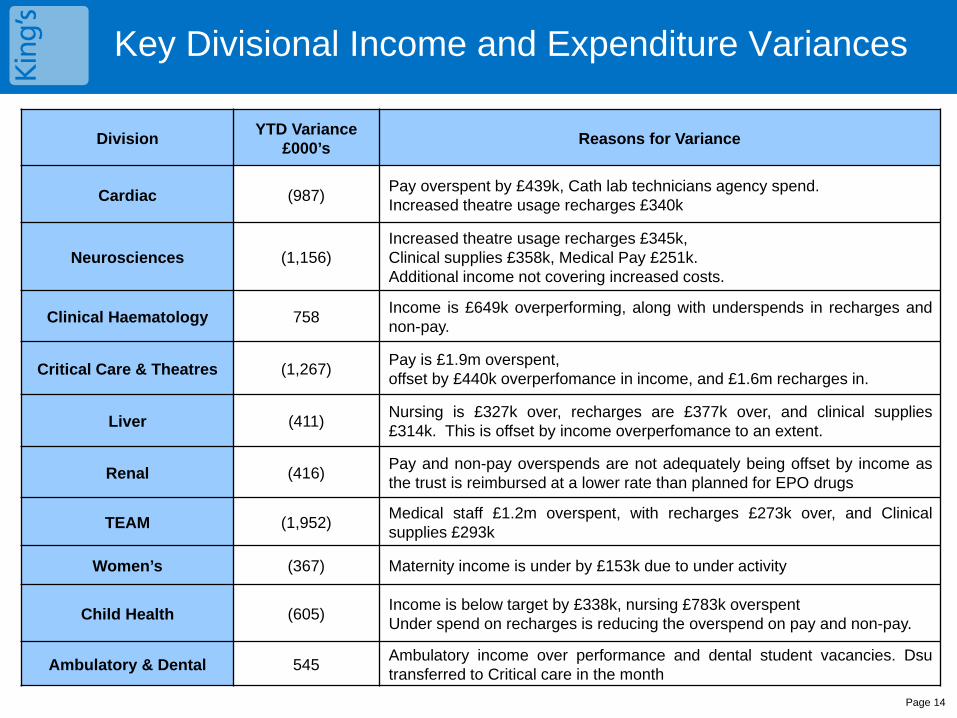
Key Divisional Income and Expenditure Variances
Page 14
Division YTD Variance £000’s Reasons for Variance
Cardiac (987) Pay overspent by £439k, Cath lab technicians agency spend. Increased theatre usage recharges £340k
Neurosciences (1,156) Increased theatre usage recharges £345k, Clinical supplies £358k, Medical Pay £251k. Additional income not covering increased costs.
Clinical Haematology 758 Income is £649k overperforming, along with underspends in recharges and non-pay.
Critical Care & Theatres (1,267) Pay is £1.9m overspent, offset by £440k overperfomance in income, and £1.6m recharges in.
Liver (411) Nursing is £327k over, recharges are £377k over, and clinical supplies £314k. This is offset by income overperfomance to an extent.
Renal (416) Pay and non-pay overspends are not adequately being offset by income as the trust is reimbursed at a lower rate than planned for EPO drugs
TEAM (1,952) Medical staff £1.2m overspent, with recharges £273k over, and Clinical supplies £293k
Women’s (367) Maternity income is under by £153k due to under activity
Child Health (605) Income is below target by £338k, nursing £783k overspent Under spend on recharges is reducing the overspend on pay and non-pay.
Ambulatory & Dental 545 Ambulatory income over performance and dental student vacancies. Dsu transferred to Critical care in the month
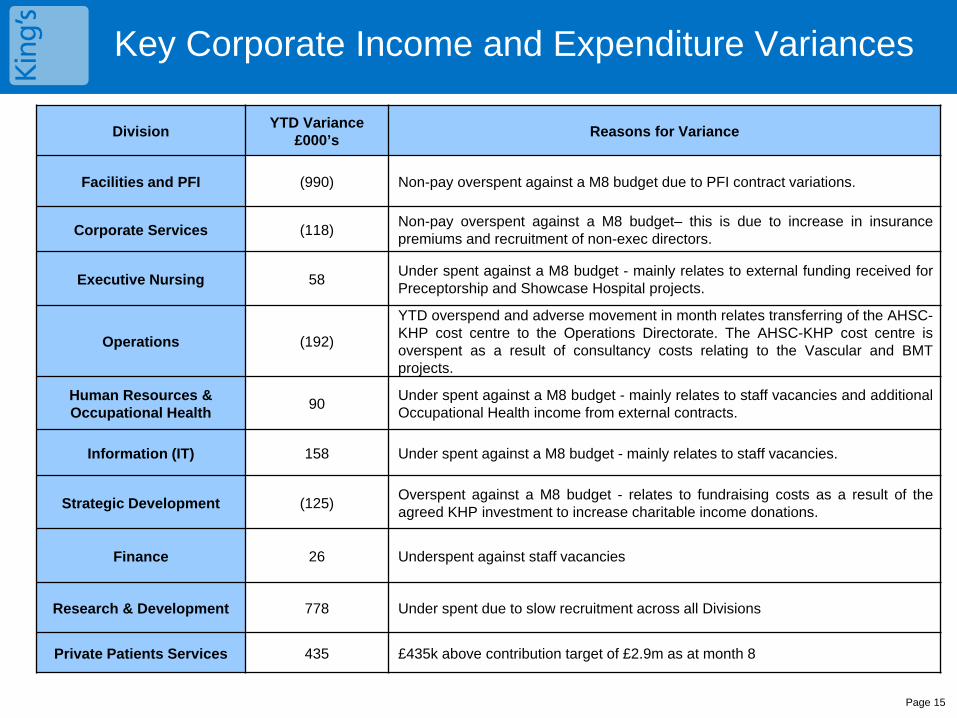
Key Corporate Income and Expenditure Variances
Page 15
Division YTD Variance £000’s Reasons for Variance
Facilities and PFI (990) Non-pay overspent against a M8 budget due to PFI contract variations.
Corporate Services (118) Non-pay overspent against a M8 budget– this is due to increase in insurance premiums and recruitment of non-exec directors.
Executive Nursing 58 Under spent against a M8 budget - mainly relates to external funding received for Preceptorship and Showcase Hospital projects.
Operations (192)
YTD overspend and adverse movement in month relates transferring of the AHSC-KHP cost centre to the Operations Directorate. The AHSC-KHP cost centre is overspent as a result of consultancy costs relating to the Vascular and BMT projects.
Human Resources & Occupational Health 90 Under spent against a M8 budget - mainly relates to staff vacancies and additional
Occupational Health income from external contracts.
Information (IT) 158 Under spent against a M8 budget - mainly relates to staff vacancies.
Strategic Development (125) Overspent against a M8 budget - relates to fundraising costs as a result of the agreed KHP investment to increase charitable income donations.
Finance 26 Underspent against staff vacancies
Research & Development 778 Under spent due to slow recruitment across all Divisions
Private Patients Services 435 £435k above contribution target of £2.9m as at month 8
Page 16
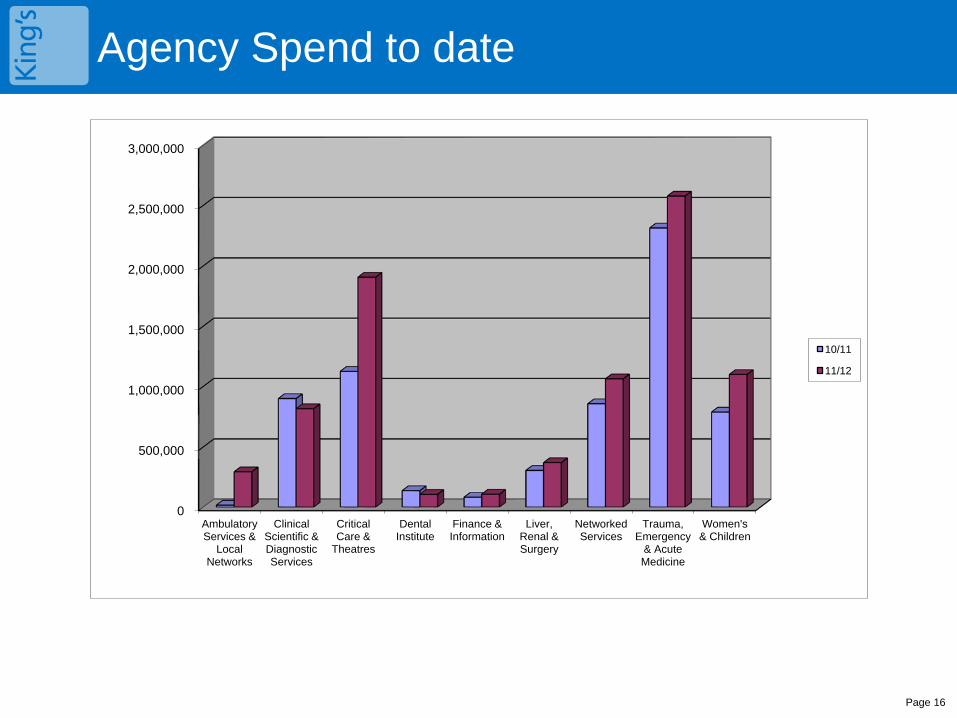
Agency Spend to date
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
Ambulatory Services &
Local Networks
Clinical Scientific & Diagnostic Services
Critical Care &
Theatres
Dental Institute
Finance & Information
Liver, Renal & Surgery
Networked Services
Trauma, Emergency
& Acute Medicine
Women's & Children
10/11
11/12
Page 17
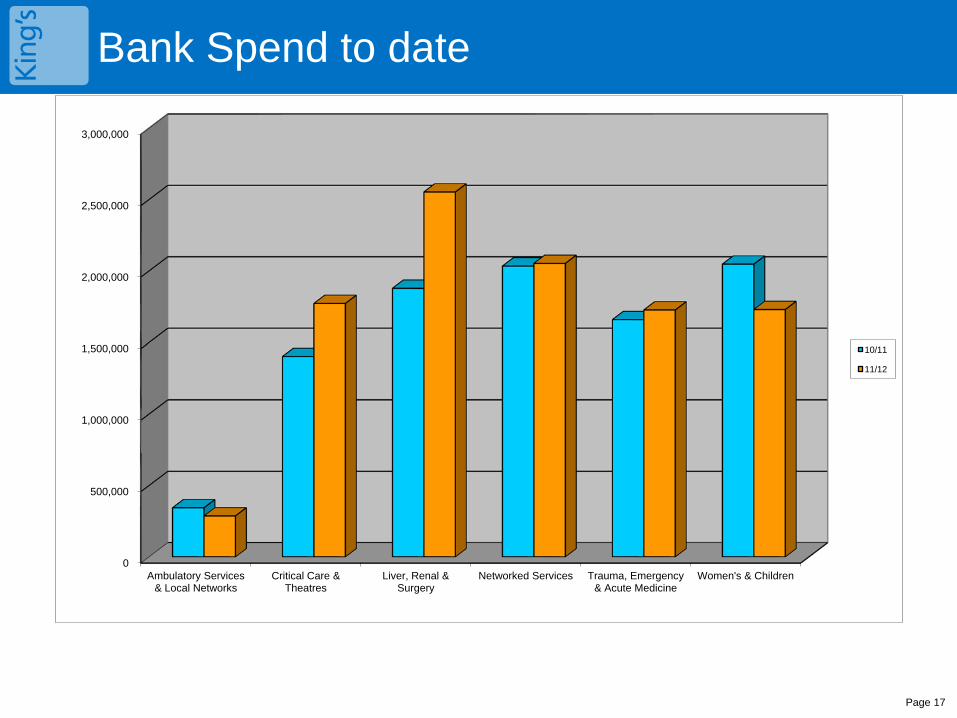
Bank Spend to date
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
Ambulatory Services & Local Networks
Critical Care & Theatres
Liver, Renal & Surgery
Networked Services Trauma, Emergency & Acute Medicine
Women's & Children
10/11
11/12
Page 18
CIP update – Actuals to Date
At Month 8, CIPs totalling £18m have been achieved against a plan of £19.9m, a 90% success rate. The overall achievement is 2% below the month 7 achievement. The trends continue with under achievement against Bank and Agency reductions, Diagnostic demand management, and additional income targets (primarily income related to bed and theatre efficiencies).
Divisional plans are 94% achieved, with underachievement now in all areas, the highest being in Networked services and CCTD. No further substitutions are proposed, with savings plans now being monitored through the financial forecast process.
Divisional schemes: 94% These are largely similar to previous months, although in absolute terms, savings are underacheived by £784k.
Networked services are off target due in the main to Neurosurgical income being off track. Womens and childrens adverse variance is due to Child health income.
Devolved schemes: 78%
These are for Procurement, Pharmacy, Beds and Theatres trustwide schemes which have been devolved. The main driver for this under achievement is because Bank and agency spend has not reduced in line with plan. Beds & theatres income is currently underachieved, particularly in Neuro and General Surgery.
Trustwide schemes: 86%
Year to date, underachievement of workforce control and medical productivity are shown. Some further beds and theatres schemes are scheduled to be devolved (approx £140k), however the remaining schemes yet to be devolved will now be deferred into 12/13 financial year. These have been covered by reserves.
Deferred schemes:
£7m has been deferred to 12/13 although additional beds and theatres and outpatient CIPs should impact in quarter 4 for 11/12. A contingency reserve was established to cover this deferment along with unplanned income.
Page 19
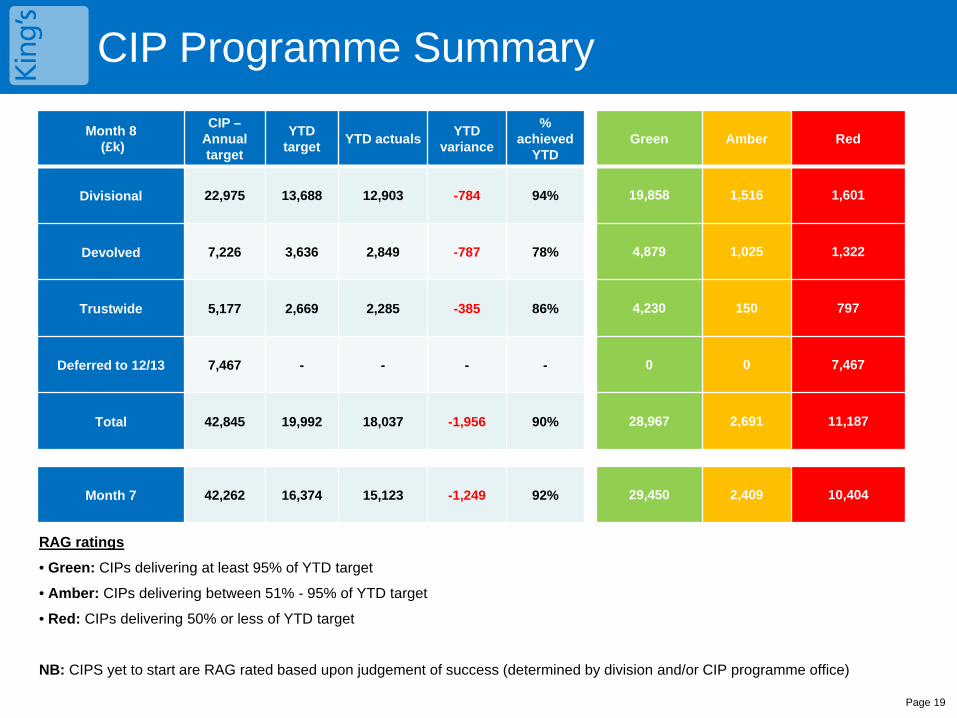
CIP Programme Summary
RAG ratings
• Green: CIPs delivering at least 95% of YTD target
• Amber: CIPs delivering between 51% - 95% of YTD target
• Red: CIPs delivering 50% or less of YTD target
NB: CIPS yet to start are RAG rated based upon judgement of success (determined by division and/or CIP programme office)
Month 8 (£k)
CIP – Annual target
YTD target YTD actuals YTD
variance
% achieved
YTD Green Amber Red
Divisional 22,975 13,688 12,903 -784 94% 19,858 1,516 1,601
Devolved 7,226 3,636 2,849 -787 78% 4,879 1,025 1,322
Trustwide 5,177 2,669 2,285 -385 86% 4,230 150 797
Deferred to 12/13 7,467 - - - - 0 0 7,467
Total 42,845 19,992 18,037 -1,956 90% 28,967 2,691 11,187
Month 5
Month 7 42,262 16,374 15,123 -1,249 92% 29,450 2,409 10,404
Page 20
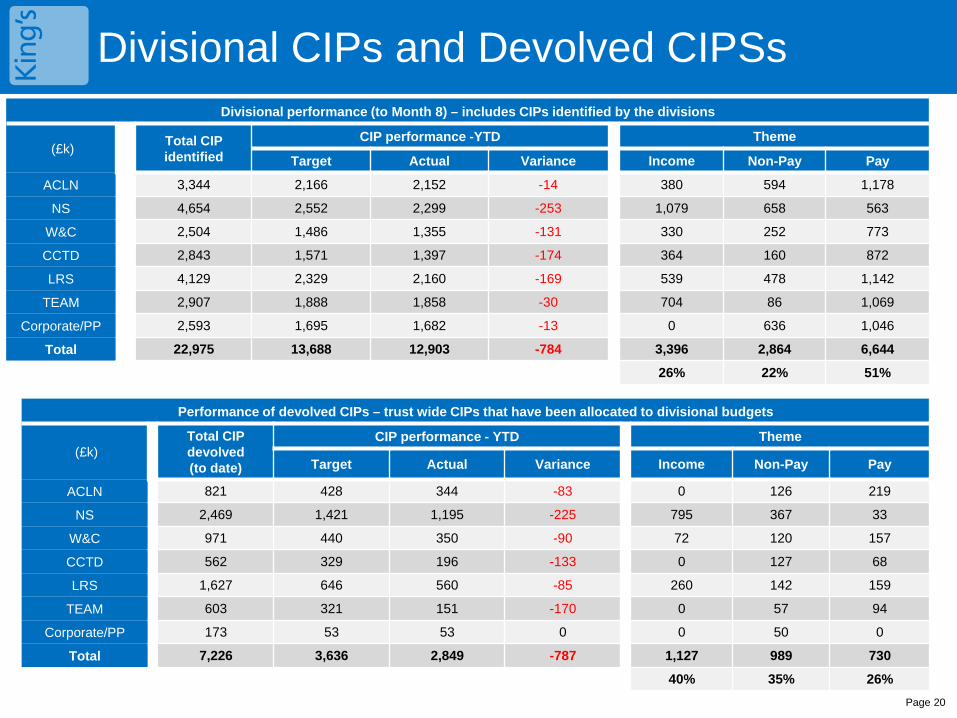
Divisional CIPs and Devolved CIPSs Divisional performance (to Month 8) – includes CIPs identified by the divisions
(£k) Total CIP identified
CIP performance -YTD Theme
Target Actual Variance Income Non-Pay Pay
ACLN 3,344 2,166 2,152 -14 380 594 1,178
NS 4,654 2,552 2,299 -253 1,079 658 563
W&C 2,504 1,486 1,355 -131 330 252 773
CCTD 2,843 1,571 1,397 -174 364 160 872
LRS 4,129 2,329 2,160 -169 539 478 1,142
TEAM 2,907 1,888 1,858 -30 704 86 1,069
Corporate/PP 2,593 1,695 1,682 -13 0 636 1,046
Total 22,975 13,688 12,903 -784 3,396 2,864 6,644
26% 22% 51%
Performance of devolved CIPs – trust wide CIPs that have been allocated to divisional budgets
(£k) Total CIP devolved (to date)
CIP performance - YTD Theme
Target Actual Variance Income Non-Pay Pay
ACLN 821 428 344 -83 0 126 219
NS 2,469 1,421 1,195 -225 795 367 33
W&C 971 440 350 -90 72 120 157
CCTD 562 329 196 -133 0 127 68
LRS 1,627 646 560 -85 260 142 159
TEAM 603 321 151 -170 0 57 94
Corporate/PP 173 53 53 0 0 50 0
Total 7,226 3,636 2,849 -787 1,127 989 730
40% 35% 26%
Page 21
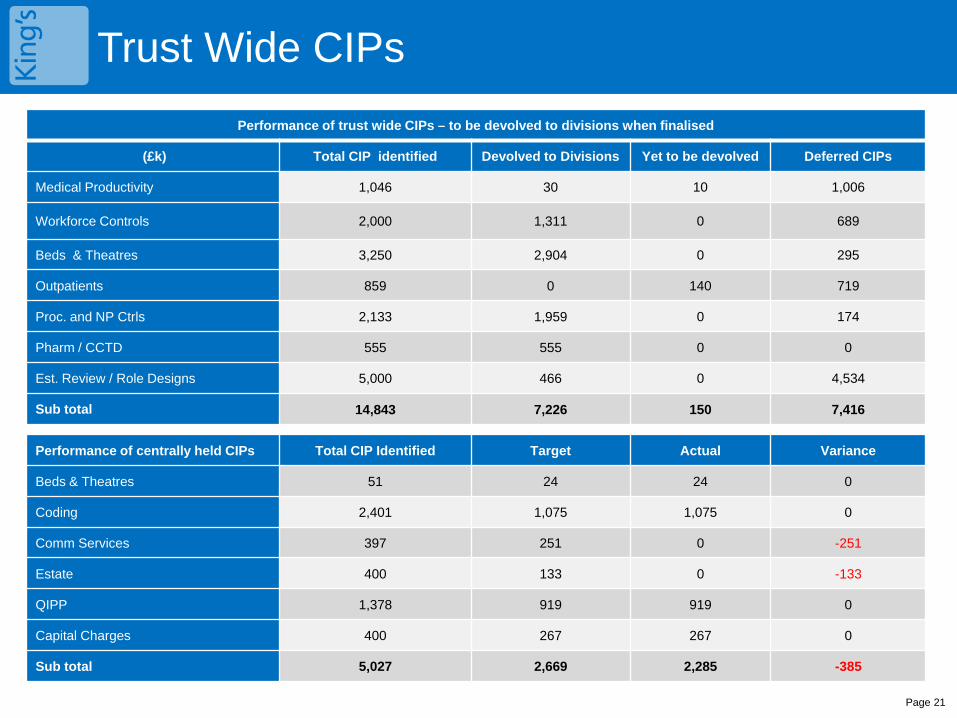
Trust Wide CIPs Performance of trust wide CIPs – to be devolved to divisions when finalised
(£k) Total CIP identified Devolved to Divisions Yet to be devolved Deferred CIPs
Medical Productivity 1,046 30 10 1,006
Workforce Controls 2,000 1,311 0 689
Beds & Theatres 3,250 2,904 0 295
Outpatients 859 0 140 719
Proc. and NP Ctrls 2,133 1,959 0 174
Pharm / CCTD 555 555 0 0
Est. Review / Role Designs 5,000 466 0 4,534
Sub total 14,843 7,226 150 7,416
Performance of centrally held CIPs Total CIP Identified Target Actual Variance
Beds & Theatres 51 24 24 0
Coding 2,401 1,075 1,075 0
Comm Services 397 251 0 -251
Estate 400 133 0 -133
QIPP 1,378 919 919 0
Capital Charges 400 267 267 0
Sub total 5,027 2,669 2,285 -385
Page 22
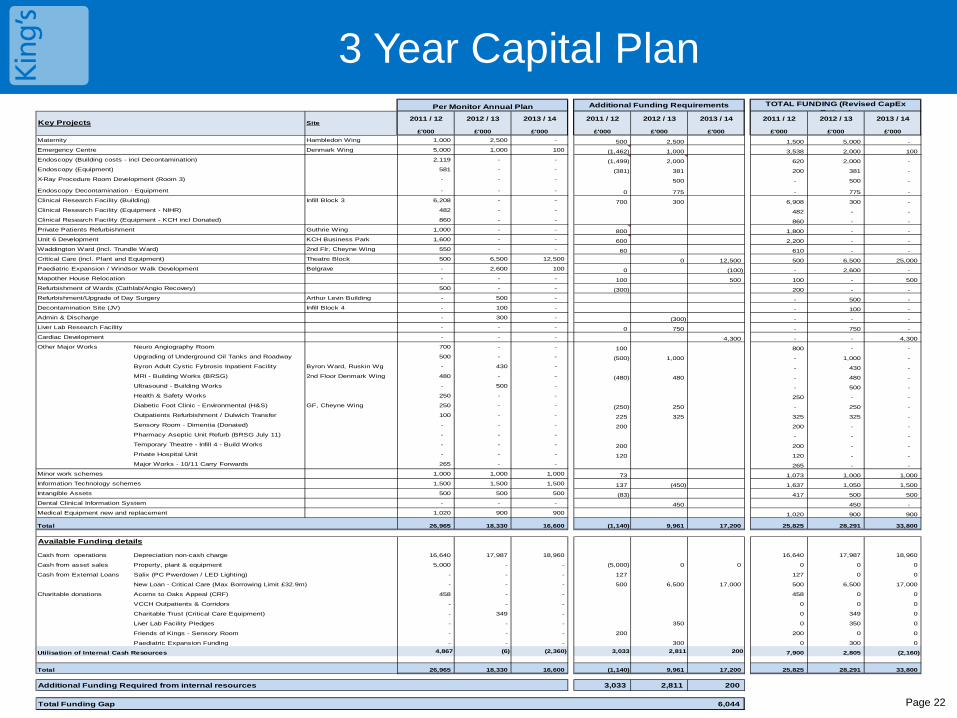
3 Year Capital Plan Key Projects Site
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000Maternity Hambledon Wing 1,000 2,500 - 500 2,500 1,500 5,000 - Emergency Centre Denmark Wing 5,000 1,000 100 (1,462) 1,000 3,538 2,000 100 Endoscopy (Building costs - incl Decontamination) 2,119 - - (1,499) 2,000 620 2,000 - Endoscopy (Equipment) 581 - - (381) 381 200 381 - X-Ray Procedure Room Development (Room 3) - - - 500 - 500 -
Endoscopy Decontamination - Equipment - - - 0 775 - 775 - Clinical Research Facility (Building) Infill Block 3 6,208 - - 700 300 6,908 300 - Clinical Research Facility (Equipment - NIHR) 482 - - 482 - - Clinical Research Facility (Equipment - KCH incl Donated) 860 - - 860 - - Private Patients Refurbishment Guthrie Wing 1,000 - - 800 1,800 - - Unit 6 Development KCH Business Park 1,600 - - 600 2,200 - - Waddington Ward (incl. Trundle Ward) 2nd Flr, Cheyne Wing 550 - - 60 610 - - Critical Care (incl. Plant and Equipment) Theatre Block 500 6,500 12,500 0 12,500 500 6,500 25,000 Paediatric Expansion / Windsor Walk Development Belgrave - 2,600 100 0 (100) - 2,600 - Mapother House Relocation - - - 100 500 100 - 500 Refurbishment of Wards (Cathlab/Angio Recovery) 500 - - (300) 200 - - Refurbishment/Upgrade of Day Surgery Arthur Levin Building - 500 - - 500 - Decontamination Site (JV) Infill Block 4 - 100 - - 100 - Admin & Discharge - 300 - (300) - - - Liver Lab Research Facility - - - 0 750 - 750 - Cardiac Development - - - 4,300 - - 4,300 Other Major Works Neuro Angiography Room 700 - - 100 800 - -
Upgrading of Underground Oil Tanks and Roadway 500 - - (500) 1,000 - 1,000 - Byron Adult Cystic Fybrosis Inpatient Facility Byron Ward, Ruskin Wg - 430 - - 430 - MRI - Building Works (BRSG) 2nd Floor Denmark Wing 480 - - (480) 480 - 480 - Ultrasound - Building Works - 500 - - 500 - Health & Safety Works 250 - - 250 - - Diabetic Foot Clinic - Environmental (H&S) GF, Cheyne Wing 250 - - (250) 250 - 250 - Outpatients Refurbishment / Dulwich Transfer 100 - - 225 325 325 325 - Sensory Room - Dimentia (Donated) - - - 200 200 - - Pharmacy Aseptic Unit Refurb (BRSG July 11) - - - - - - Temporary Theatre - Infill 4 - Build Works - - - 200 200 - - Private Hospital Unit - - - 120 120 - - Major Works - 10/11 Carry Forwards 265 - - 265 - -
Minor work schemes 1,000 1,000 1,000 73 1,073 1,000 1,000 Information Technology schemes 1,500 1,500 1,500 137 (450) 1,637 1,050 1,500 Intangible Assets 500 500 500 (83) 417 500 500 Dental Clinical Information System - - - 450 450 - Medical Equipment new and replacement 1,020 900 900 1,020 900 900
Total 26,965 18,330 16,600 (1,140) 9,961 17,200 25,825 28,291 33,800
Available Funding details
Cash from operations Depreciation non-cash charge 16,640 17,987 18,960 16,640 17,987 18,960
Cash from asset sales Property, plant & equipment 5,000 - - (5,000) 0 0 0 0 0
Cash from External Loans Salix (PC Pwerdown / LED Lighting) - - - 127 127 0 0
New Loan - Critical Care (Max Borrowing Limit £32.9m) - - - 500 6,500 17,000 500 6,500 17,000
Charitable donations Acorns to Oaks Appeal (CRF) 458 - - 458 0 0
VCCH Outpatients & Corridors - - - 0 0 0
Charitable Trust (Critical Care Equipment) - 349 - 0 349 0
Liver Lab Facility Pledges - - - 350 0 350 0
Friends of Kings - Sensory Room - - - 200 200 0 0
Paediatric Expansion Funding - - - 300 0 300 0
Utilisation of Internal Cash Resources 4,867 (6) (2,360) 3,033 2,811 200 7,900 2,805 (2,160)
Total 26,965 18,330 16,600 (1,140) 9,961 17,200 25,825 28,291 33,800
Additional Funding Required from internal resources 3,033 2,811 200
Total Funding Gap 6,044
2011 / 12
Per Monitor Annual Plan Additional Funding Requirements TOTAL FUNDING (Revised CapEx R t )
2011 / 12 2012 / 13 2013 / 142011 / 12 2012 / 13 2013 / 14 2013 / 142012 / 13
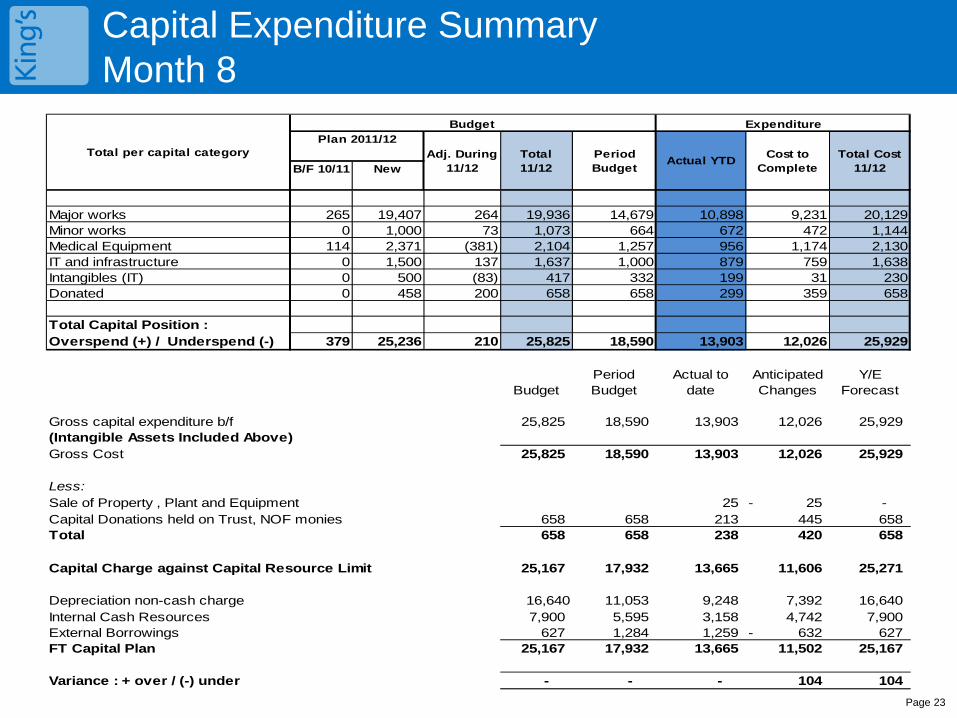
Capital Expenditure Summary Month 8
Page 23
Budget
B/F 10/11 New
Major works 265 19,407 264 19,936 14,679 10,898 9,231 20,129Minor works 0 1,000 73 1,073 664 672 472 1,144Medical Equipment 114 2,371 (381) 2,104 1,257 956 1,174 2,130IT and infrastructure 0 1,500 137 1,637 1,000 879 759 1,638Intangibles (IT) 0 500 (83) 417 332 199 31 230Donated 0 458 200 658 658 299 359 658
Total Capital Position :Overspend (+) / Underspend (-) 379 25,236 210 25,825 18,590 13,903 12,026 25,929
BudgetPeriod Budget
Actual to date
Anticipated Changes
Y/E Forecast
Gross capital expenditure b/f 25,825 18,590 13,903 12,026 25,929 (Intangible Assets Included Above)Gross Cost 25,825 18,590 13,903 12,026 25,929
Less:Sale of Property , Plant and Equipment 25 25- - Capital Donations held on Trust, NOF monies 658 658 213 445 658 Total 658 658 238 420 658
Capital Charge against Capital Resource Limit 25,167 17,932 13,665 11,606 25,271
Depreciation non-cash charge 16,640 11,053 9,248 7,392 16,640 Internal Cash Resources 7,900 5,595 3,158 4,742 7,900 External Borrowings 627 1,284 1,259 632- 627 FT Capital Plan 25,167 17,932 13,665 11,502 25,167
Variance : + over / (-) under - - - 104 104
Total per capital category
ExpenditurePlan 2011/12
Adj. During 11/12
Total 11/12
Period Budget Actual YTD Cost to
CompleteTotal Cost
11/12
Page 24
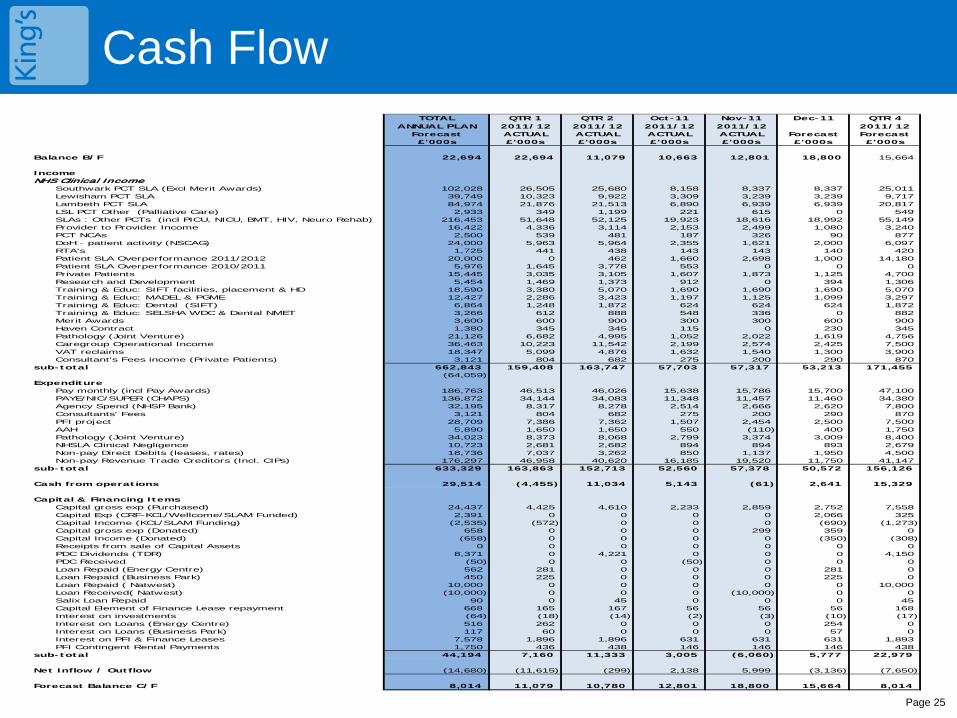
Cash Flow Summary
The Cash balance at the end of Month 8 was £18.800m against a forecast cash balance of £16.993m Due to the additional debt collecting procedures implemented there has been an increase in debt recovery from
other Trusts and PCT’s. Material cash payments are due in month 9 from this work. Trusts and PCT’s – Provider to Provider Income, NCA’s and SLA’s - £1.304m greater than forecast has been
received to date. The income has been re-phased to 31st March 2012 SLA’s Overperformance - £2.698m greater than forecast has been received to date. The income has been re-
phased to 31st March 2012 The Trust needs to recover the funding for Project Diamond (£2.7m) and the PCT Emergency Re-admission
funds (1.2m).
2011 PCT SLA over/under-performance As at the end of Month 8 the Trust has invoiced £2.467m relating to Q1 and £2.501m relating to July 2011 PCT
SLA over-performance. Of this, £3.409m has been received to date. PCT SLA over-performance invoices for August 2011(£3.159m) and September 2011 (£3.135m) were raised in
November, all of which remain outstanding. PCT SLA underperformance credit notes totalling £2.126m have been raised to September 2011.
Working Capital Facility
The Trust’s current Working Capital Facility (WCF) of £35m has was finalised at the Trust’s October Board meeting. The updated agreement will allow the Trust to benefit from reduced renewal costs and lower interest rates and non-utilisation fees.
The Trust has drawdown £10m against the working capital facility in November, this will be repaid back on the 27th January 2012. Interest on this utilisation will be £42k.
Prudential Borrowing Limit
The Trust is currently utilising £91.122m (73.4%) of its 2011/2012 Prudential Borrowing Limit (Long-term borrowing) of £124.1m leaving headroom of £32.978m. The Trust is looking into the possibility of obtaining external financing to fund the Critical Care capital project over the next 3 years.
Cash Flow
Page 25
TOTAL QTR 1 QTR 2 Oct-11 Nov-11 Dec-11 QTR 4ANNUAL PLAN 2011/12 2011/12 2011/12 2011/12 2011/12
Forecast ACTUAL ACTUAL ACTUAL ACTUAL Forecast Forecast£'000s £'000s £'000s £'000s £'000s £'000s £'000s
Balance B/F 22,694 22,694 11,079 10,663 12,801 18,800 15,664
IncomeNHS Clinical Income
Southwark PCT SLA (Excl Merit Awards) 102,028 26,505 25,680 8,158 8,337 8,337 25,011Lewisham PCT SLA 39,749 10,323 9,922 3,309 3,239 3,239 9,717Lambeth PCT SLA 84,974 21,876 21,513 6,890 6,939 6,939 20,817LSL PCT Other (Palliative Care) 2,933 349 1,199 221 615 0 549SLAs : Other PCTs (incl PICU, NICU, BMT, HIV, Neuro Rehab) 216,453 51,648 52,125 19,923 18,616 18,992 55,149Provider to Provider Income 16,422 4,336 3,114 2,153 2,499 1,080 3,240PCT NCAs 2,500 539 481 187 326 90 877DoH - patient activity (NSCAG) 24,000 5,963 5,964 2,355 1,621 2,000 6,097RTA's 1,725 441 438 143 143 140 420Patient SLA Overperformance 2011/2012 20,000 0 462 1,660 2,698 1,000 14,180Patient SLA Overperformance 2010/2011 5,976 1,645 3,778 553 0 0 0Private Patients 15,445 3,035 3,105 1,607 1,873 1,125 4,700Research and Development 5,454 1,469 1,373 912 0 394 1,306Training & Educ: SIFT facilities, placement & HD 18,590 3,380 5,070 1,690 1,690 1,690 5,070Training & Educ: MADEL & PGME 12,427 2,286 3,423 1,197 1,125 1,099 3,297Training & Educ: Dental (SIFT) 6,864 1,248 1,872 624 624 624 1,872Training & Educ: SELSHA WDC & Dental NMET 3,266 612 888 548 336 0 882Merit Awards 3,600 600 900 300 300 600 900Haven Contract 1,380 345 345 115 0 230 345Pathology (Joint Venture) 21,126 6,682 4,995 1,052 2,022 1,619 4,756Caregroup Operational Income 36,463 10,223 11,542 2,199 2,574 2,425 7,500VAT reclaims 18,347 5,099 4,876 1,632 1,540 1,300 3,900Consultant's Fees income (Private Patients) 3,121 804 682 275 200 290 870
sub-total 662,843 159,408 163,747 57,703 57,317 53,213 171,455(64,059)
ExpenditurePay monthly (incl Pay Awards) 186,763 46,513 46,026 15,638 15,786 15,700 47,100PAYE/NIC/SUPER (CHAPS) 136,872 34,144 34,083 11,348 11,457 11,460 34,380Agency Spend (NHSP Bank) 32,195 8,317 8,278 2,514 2,666 2,620 7,800Consultants' Fees 3,121 804 682 275 200 290 870PFI project 28,709 7,386 7,362 1,507 2,454 2,500 7,500AAH 5,890 1,650 1,650 550 (110) 400 1,750Pathology (Joint Venture) 34,023 8,373 8,068 2,799 3,374 3,009 8,400NHSLA Clinical Negligence 10,723 2,681 2,682 894 894 893 2,679Non-pay Direct Debits (leases, rates) 18,736 7,037 3,262 850 1,137 1,950 4,500Non-pay Revenue Trade Creditors (Incl. CIPs) 176,297 46,958 40,620 16,185 19,520 11,750 41,147
sub-total 633,329 163,863 152,713 52,560 57,378 50,572 156,126
Cash from operations 29,514 (4,455) 11,034 5,143 (61) 2,641 15,329
Capital & Financing ItemsCapital gross exp (Purchased) 24,437 4,425 4,610 2,233 2,859 2,752 7,558Capital Exp (CRF-KCL/Wellcome/SLAM Funded) 2,391 0 0 0 0 2,066 325Capital Income (KCL/SLAM Funding) (2,535) (572) 0 0 0 (690) (1,273)Capital gross exp (Donated) 658 0 0 0 299 359 0Capital Income (Donated) (658) 0 0 0 0 (350) (308)Receipts from sale of Capital Assets 0 0 0 0 0 0 0PDC Dividends (TDR) 8,371 0 4,221 0 0 0 4,150PDC Received (50) 0 0 (50) 0 0 0Loan Repaid (Energy Centre) 562 281 0 0 0 281 0Loan Repaid (Business Park) 450 225 0 0 0 225 0Loan Repaid ( Natwest) 10,000 0 0 0 0 0 10,000Loan Received( Natwest) (10,000) 0 0 0 (10,000) 0 0Salix Loan Repaid 90 0 45 0 0 0 45Capital Element of Finance Lease repayment 668 165 167 56 56 56 168Interest on investments (64) (18) (14) (2) (3) (10) (17)Interest on Loans (Energy Centre) 516 262 0 0 0 254 0Interest on Loans (Business Park) 117 60 0 0 0 57 0Interest on PFI & Finance Leases 7,578 1,896 1,896 631 631 631 1,893PFI Contingent Rental Payments 1,750 436 438 146 146 146 438
sub-total 44,194 7,160 11,333 3,005 (6,060) 5,777 22,979
Net Inflow / Outflow (14,680) (11,615) (299) 2,138 5,999 (3,136) (7,650)
Forecast Balance C/F 8,014 11,079 10,780 12,801 18,800 15,664 8,014
Cash Flow Key Outstanding Debts
Page 26
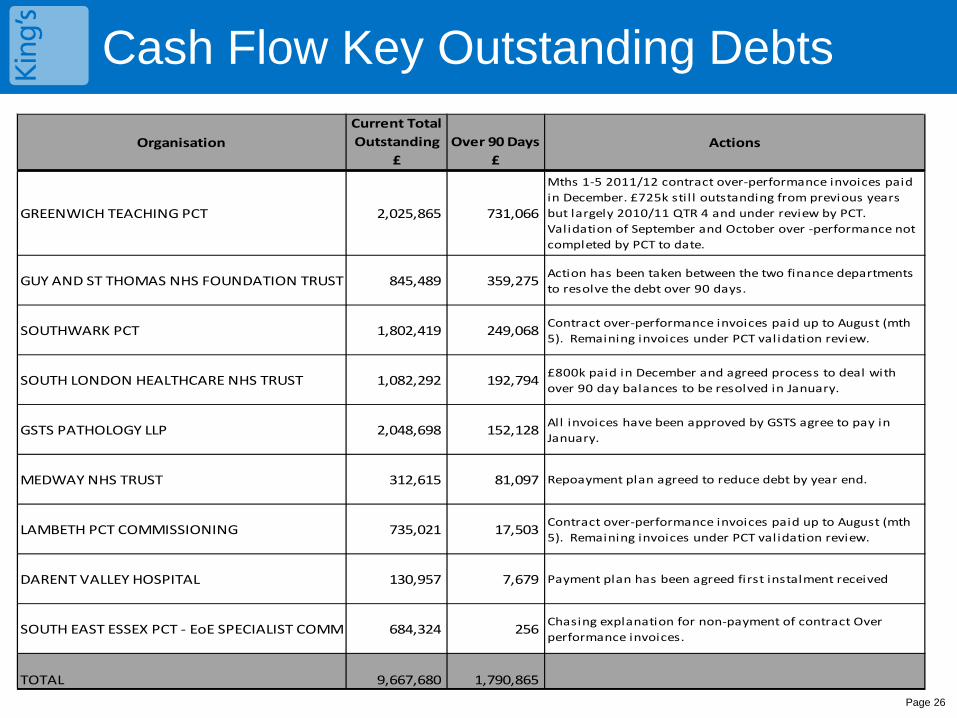
Cash Flow Key Outstanding Debts
OrganisationCurrent Total Outstanding
£Over 90 Days
£Actions
GREENWICH TEACHING PCT 2,025,865 731,066
Mths 1-5 2011/12 contract over-performance invoices paid in December. £725k sti l l outstanding from previous years but largely 2010/11 QTR 4 and under review by PCT. Validation of September and October over -performance not completed by PCT to date.
GUY AND ST THOMAS NHS FOUNDATION TRUST 845,489 359,275Action has been taken between the two finance departments to resolve the debt over 90 days.
SOUTHWARK PCT 1,802,419 249,068Contract over-performance invoices paid up to August (mth 5). Remaining invoices under PCT validation review.
SOUTH LONDON HEALTHCARE NHS TRUST 1,082,292 192,794£800k paid in December and agreed process to deal with over 90 day balances to be resolved in January.
GSTS PATHOLOGY LLP 2,048,698 152,128All invoices have been approved by GSTS agree to pay in January.
MEDWAY NHS TRUST 312,615 81,097 Repoayment plan agreed to reduce debt by year end.
LAMBETH PCT COMMISSIONING 735,021 17,503Contract over-performance invoices paid up to August (mth 5). Remaining invoices under PCT validation review.
DARENT VALLEY HOSPITAL 130,957 7,679 Payment plan has been agreed first instalment received
SOUTH EAST ESSEX PCT - EoE SPECIALIST COMM 684,324 256Chasing explanation for non-payment of contract Over performance invoices.
TOTAL 9,667,680 1,790,865
Analysis of Cash Borrowings
Page 27
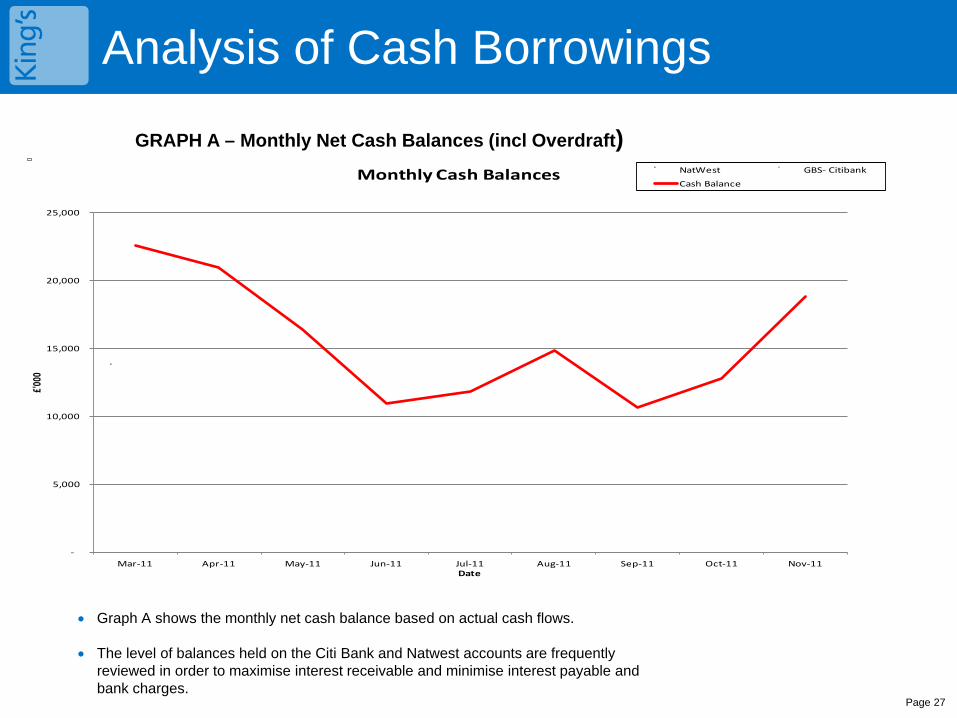
GRAPH A – Monthly Net Cash Balances (incl Overdraft)
-
5,000
10,000
15,000
20,000
25,000
Mar-11 Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11
£'00
0
Date
Monthly Cash Balances NatWest GBS- Citibank
Cash Balance
• Graph A shows the monthly net cash balance based on actual cash flows.
• The level of balances held on the Citi Bank and Natwest accounts are frequently reviewed in order to maximise interest receivable and minimise interest payable and bank charges.
Analysis of Cash Balances Borrowings
Page 28
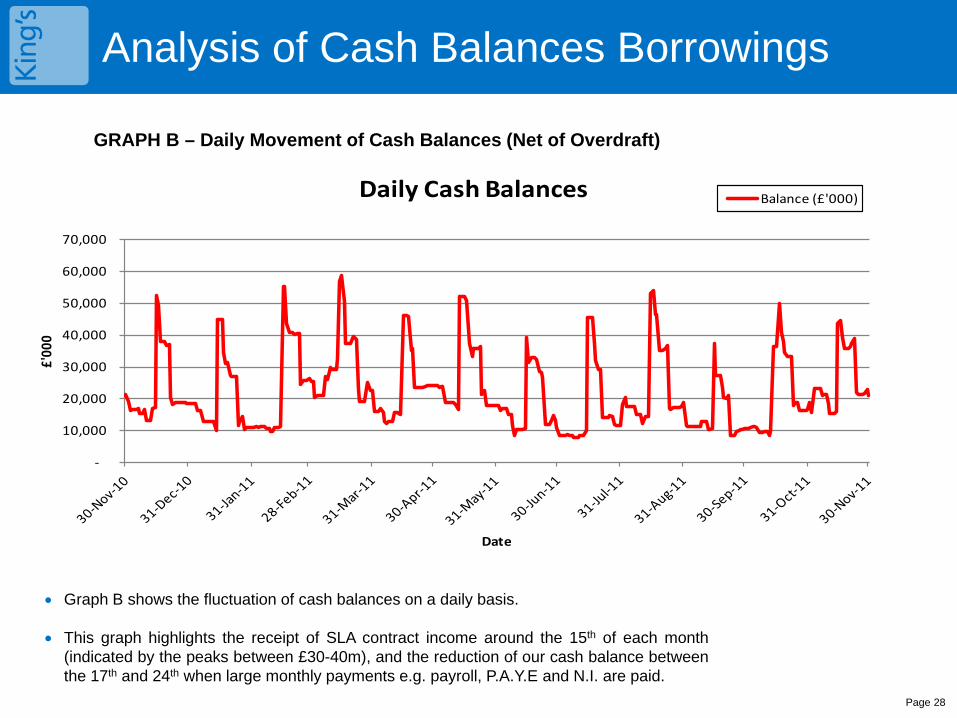
GRAPH B – Daily Movement of Cash Balances (Net of Overdraft)
-
10,000
20,000
30,000
40,000
50,000
60,000
70,000
£'00
0
Date
Daily Cash Balances Balance (£'000)
• Graph B shows the fluctuation of cash balances on a daily basis.
• This graph highlights the receipt of SLA contract income around the 15th of each month (indicated by the peaks between £30-40m), and the reduction of our cash balance between the 17th and 24th when large monthly payments e.g. payroll, P.A.Y.E and N.I. are paid.
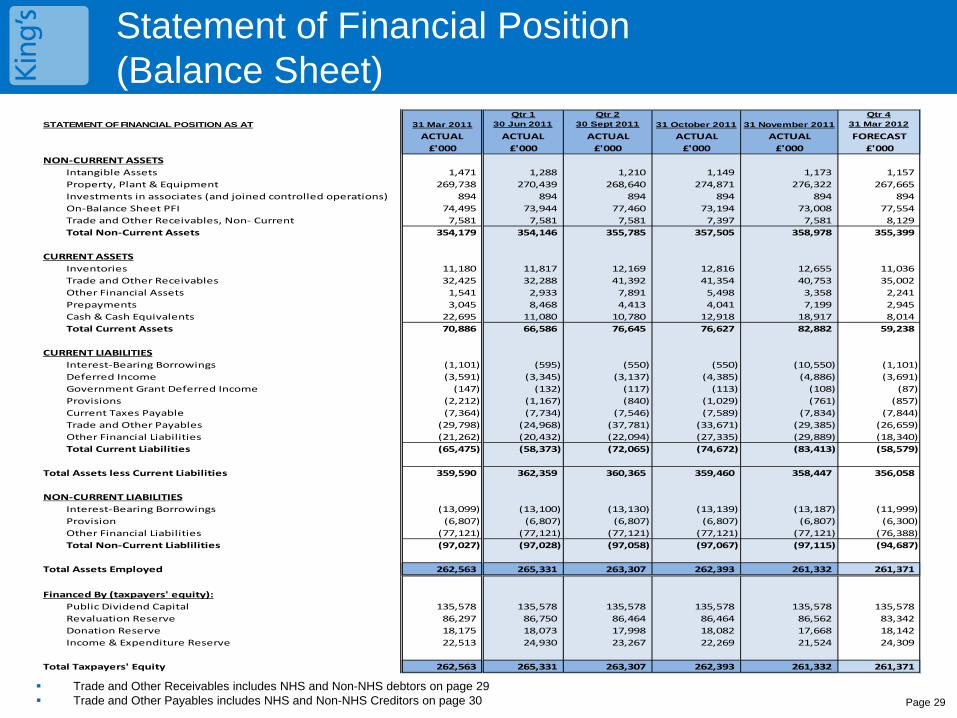
Statement of Financial Position (Balance Sheet)
Page 29 Trade and Other Receivables includes NHS and Non-NHS debtors on page 29 Trade and Other Payables includes NHS and Non-NHS Creditors on page 30
STATEMENT OF FINANCIAL POSITION AS AT 31 Mar 2011Qtr 1
30 Jun 2011Qtr 2
30 Sept 2011 31 October 2011 31 November 2011Qtr 4
31 Mar 2012
ACTUAL ACTUAL ACTUAL ACTUAL ACTUAL FORECAST£'000 £'000 £'000 £'000 £'000 £'000
NON-CURRENT ASSETSIntangible Assets 1,471 1,288 1,210 1,149 1,173 1,157Property, Plant & Equipment 269,738 270,439 268,640 274,871 276,322 267,665Investments in associates (and joined controlled operations) 894 894 894 894 894 894On-Balance Sheet PFI 74,495 73,944 77,460 73,194 73,008 77,554Trade and Other Receivables, Non- Current 7,581 7,581 7,581 7,397 7,581 8,129Total Non-Current Assets 354,179 354,146 355,785 357,505 358,978 355,399
CURRENT ASSETSInventories 11,180 11,817 12,169 12,816 12,655 11,036Trade and Other Receivables 32,425 32,288 41,392 41,354 40,753 35,002Other Financial Assets 1,541 2,933 7,891 5,498 3,358 2,241Prepayments 3,045 8,468 4,413 4,041 7,199 2,945Cash & Cash Equivalents 22,695 11,080 10,780 12,918 18,917 8,014Total Current Assets 70,886 66,586 76,645 76,627 82,882 59,238
CURRENT LIABILITIESInterest-Bearing Borrowings (1,101) (595) (550) (550) (10,550) (1,101)Deferred Income (3,591) (3,345) (3,137) (4,385) (4,886) (3,691)Government Grant Deferred Income (147) (132) (117) (113) (108) (87)Provisions (2,212) (1,167) (840) (1,029) (761) (857)Current Taxes Payable (7,364) (7,734) (7,546) (7,589) (7,834) (7,844)Trade and Other Payables (29,798) (24,968) (37,781) (33,671) (29,385) (26,659)Other Financial Liabilities (21,262) (20,432) (22,094) (27,335) (29,889) (18,340)Total Current Liabilities (65,475) (58,373) (72,065) (74,672) (83,413) (58,579)
Total Assets less Current Liabilities 359,590 362,359 360,365 359,460 358,447 356,058
NON-CURRENT LIABILITIESInterest-Bearing Borrowings (13,099) (13,100) (13,130) (13,139) (13,187) (11,999)Provision (6,807) (6,807) (6,807) (6,807) (6,807) (6,300)Other Financial Liabilities (77,121) (77,121) (77,121) (77,121) (77,121) (76,388)Total Non-Current Liablilities (97,027) (97,028) (97,058) (97,067) (97,115) (94,687)
Total Assets Employed 262,563 265,331 263,307 262,393 261,332 261,371
Financed By (taxpayers' equity):Public Dividend Capital 135,578 135,578 135,578 135,578 135,578 135,578Revaluation Reserve 86,297 86,750 86,464 86,464 86,562 83,342Donation Reserve 18,175 18,073 17,998 18,082 17,668 18,142Income & Expenditure Reserve 22,513 24,930 23,267 22,269 21,524 24,309
Total Taxpayers' Equity 262,563 265,331 263,307 262,393 261,332 261,371
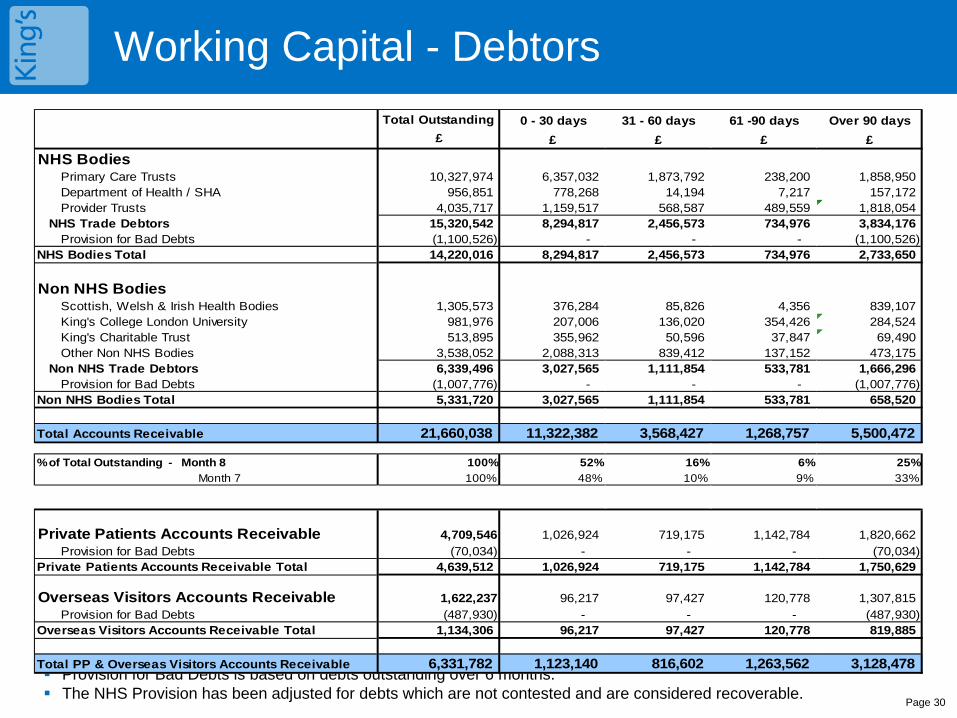
Working Capital - Debtors
Page 30
Provision for Bad Debts is based on debts outstanding over 6 months. The NHS Provision has been adjusted for debts which are not contested and are considered recoverable.
Total Outstanding 0 - 30 days 31 - 60 days 61 -90 days Over 90 days£ £ £ £ £
NHS BodiesPrimary Care Trusts 10,327,974 6,357,032 1,873,792 238,200 1,858,950 Department of Health / SHA 956,851 778,268 14,194 7,217 157,172 Provider Trusts 4,035,717 1,159,517 568,587 489,559 1,818,054
NHS Trade Debtors 15,320,542 8,294,817 2,456,573 734,976 3,834,176 Provision for Bad Debts (1,100,526) - - - (1,100,526)
NHS Bodies Total 14,220,016 8,294,817 2,456,573 734,976 2,733,650
Non NHS BodiesScottish, Welsh & Irish Health Bodies 1,305,573 376,284 85,826 4,356 839,107 King's College London University 981,976 207,006 136,020 354,426 284,524 King's Charitable Trust 513,895 355,962 50,596 37,847 69,490 Other Non NHS Bodies 3,538,052 2,088,313 839,412 137,152 473,175
Non NHS Trade Debtors 6,339,496 3,027,565 1,111,854 533,781 1,666,296 Provision for Bad Debts (1,007,776) - - - (1,007,776)
Non NHS Bodies Total 5,331,720 3,027,565 1,111,854 533,781 658,520
Total Accounts Receivable 21,660,038 11,322,382 3,568,427 1,268,757 5,500,472
% of Total Outstanding - Month 8 100% 52% 16% 6% 25% Month 7 100% 48% 10% 9% 33%
Private Patients Accounts Receivable 4,709,546 1,026,924 719,175 1,142,784 1,820,662 Provision for Bad Debts (70,034) - - - (70,034)
Private Patients Accounts Receivable Total 4,639,512 1,026,924 719,175 1,142,784 1,750,629
Overseas Visitors Accounts Receivable 1,622,237 96,217 97,427 120,778 1,307,815 Provision for Bad Debts (487,930) - - - (487,930)
Overseas Visitors Accounts Receivable Total 1,134,306 96,217 97,427 120,778 819,885
Total PP & Overseas Visitors Accounts Receivable 6,331,782 1,123,140 816,602 1,263,562 3,128,478
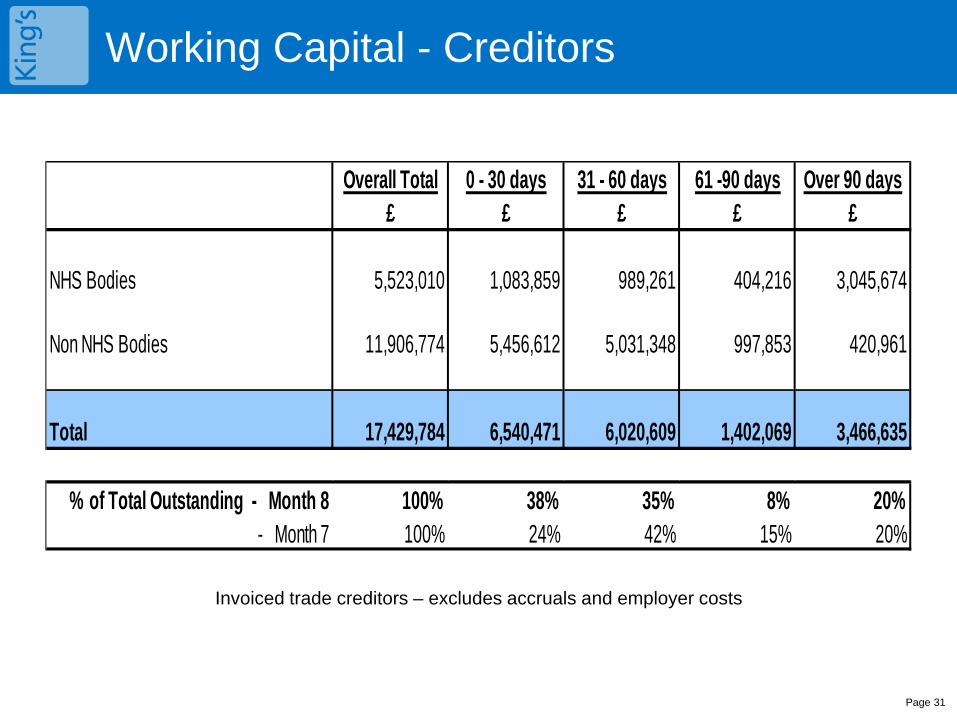
Working Capital - Creditors
Invoiced trade creditors – excludes accruals and employer costs
Page 31
Overall Total 0 - 30 days 31 - 60 days 61 -90 days Over 90 days£ £ £ £ £
NHS Bodies 5,523,010 1,083,859 989,261 404,216 3,045,674
Non NHS Bodies 11,906,774 5,456,612 5,031,348 997,853 420,961
Total 17,429,784 6,540,471 6,020,609 1,402,069 3,466,635
% of Total Outstanding - Month 8 100% 38% 35% 8% 20%- Month 7 100% 24% 42% 15% 20%
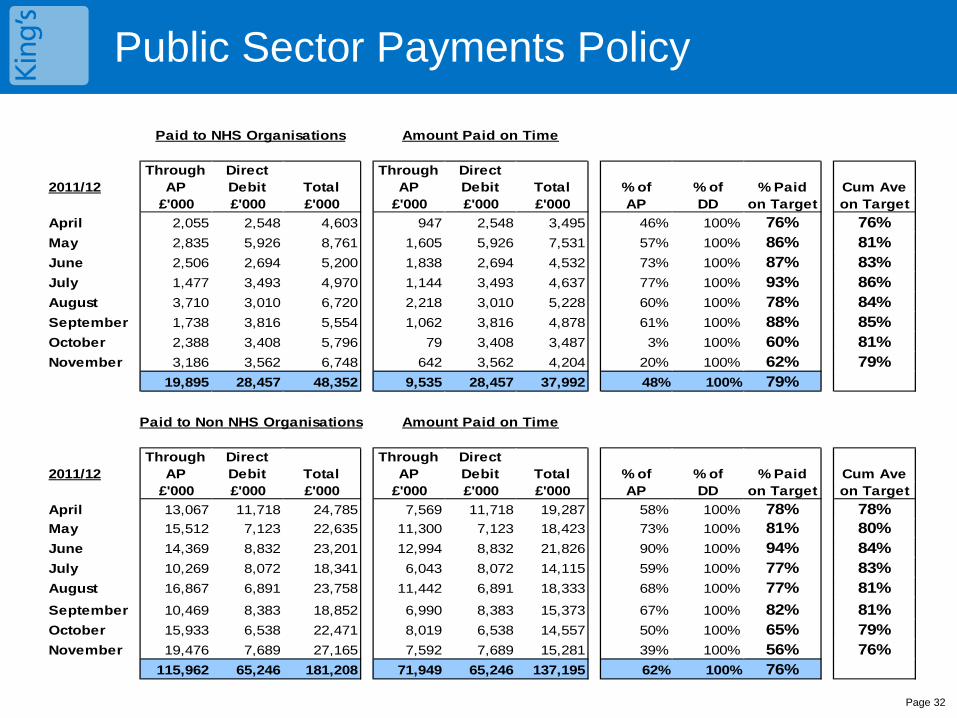
Public Sector Payments Policy
Page 32
Public Sector Payments Policy
Paid to NHS Organisations Amount Paid on Time
2011/12Through
APDirect Debit Total
Through AP
Direct Debit Total % of % of % Paid Cum Ave
£'000 £'000 £'000 £'000 £'000 £'000 AP DD on Target on TargetApril 2,055 2,548 4,603 947 2,548 3,495 46% 100% 76% 76%May 2,835 5,926 8,761 1,605 5,926 7,531 57% 100% 86% 81%June 2,506 2,694 5,200 1,838 2,694 4,532 73% 100% 87% 83%July 1,477 3,493 4,970 1,144 3,493 4,637 77% 100% 93% 86%August 3,710 3,010 6,720 2,218 3,010 5,228 60% 100% 78% 84%September 1,738 3,816 5,554 1,062 3,816 4,878 61% 100% 88% 85%October 2,388 3,408 5,796 79 3,408 3,487 3% 100% 60% 81%November 3,186 3,562 6,748 642 3,562 4,204 20% 100% 62% 79%
19,895 28,457 48,352 9,535 28,457 37,992 48% 100% 79%
Paid to Non NHS Organisations Amount Paid on Time
2011/12Through
APDirect Debit Total
Through AP
Direct Debit Total % of % of % Paid Cum Ave
£'000 £'000 £'000 £'000 £'000 £'000 AP DD on Target on TargetApril 13,067 11,718 24,785 7,569 11,718 19,287 58% 100% 78% 78%May 15,512 7,123 22,635 11,300 7,123 18,423 73% 100% 81% 80%June 14,369 8,832 23,201 12,994 8,832 21,826 90% 100% 94% 84%July 10,269 8,072 18,341 6,043 8,072 14,115 59% 100% 77% 83%August 16,867 6,891 23,758 11,442 6,891 18,333 68% 100% 77% 81%September 10,469 8,383 18,852 6,990 8,383 15,373 67% 100% 82% 81%October 15,933 6,538 22,471 8,019 6,538 14,557 50% 100% 65% 79%November 19,476 7,689 27,165 7,592 7,689 15,281 39% 100% 56% 76%
115,962 65,246 181,208 71,949 65,246 137,195 62% 100% 76%

Glossary
Page 33
CIP – Cost Improvement Plan SLA – Service Level Agreement PDC – Public Dividend Capital PSPP – Public Sector Payment Policy Working Capital Facility - represents a sum of money reserved by the relevant bank for potential use by the Foundation Trust Asset - An asset is a resource controlled by the enterprise as a result of past events and from which future economic benefits are expected to flow to the enterprise Liability - an entity's present obligation arising from a past event, the settlement of which will result in an outflow of economic benefits from the entity Equity - the residual interest in the entity's assets after deducting its liabilities EBITDA – Earnings before Interest, Taxation, Depreciation and Amortisation EBITDA Achieved (% of Plan) – measures the achievement of earnings against plan EBITDA Margin (%) – Measures Earnings as a percentage of total income indicating underlying performance Return on Assets excluding Dividends – Net surplus before Dividends as a percentage of average assets indicating financial efficiency I & E Surplus margin net of dividends – Net surplus as a percentage of total income indicating financial efficiency Liquidity Ratio (days) - The liquidity ratio (days) indicates the number of days that net liquid assets can cover operating expenses without further cash coming from cash sales of fixed or long-term assets.
1
Performance Report Month 8 Board of Directors Meeting 20 December 2011
Roland Sinker
Executive Director of Operations
Enc 2.5
2
Contents
•Executive Summary
•Trust Performance Summary
•Divisional Performance Summary
•Regulatory/Contractual Performance • Monitor Q3 interim position
• Care Quality Commission (CQC) – Quality Risk Profile Update
• CQUIN 2011/12 and Quality Accounts Update
•Specific Performance Reports • Infection Control Update-13 Operating Framework
• Summary Winter Action Plan for Weekly Meetings
• Leading Indicators Report
• 2012-13 Operating Framework Update
• Dr Foster Good Hospital Guide 2010-11 Update
3
Executive Summary (1/3)
Trust Wide Month 8 Performance
• Good Performance:
Referral time to treatment (RTT) targets for admitted and non-admitted pathways, and Cancer Waiting Time targets were achieved in November, despite increasing emergency pressure. The 95% threshold for Total Time spent in ED was achieved at 96.4% this month. All 5 ED Clinical Quality indicators were achieved at Trust level, apart from the 60 minute time to treatment indicator within the A&E department.
• Concerns going forward:
Finance position: At month 8 (November), the Trust’s position is a deficit of £1,048k, against a surplus plan of £1.75m. This is a negative variance from plan of £2.798m. Further detail is picked up later in the Finance report to this committee.
Health Care Acquired Infection (HCAI): 6 C-difficile cases were attributed to the Trust during November, 3 less than the previous month. Although 4 fewer cases have been reported compared to the same time last year, the Trust is only 4 cases away from reaching its 2011/12 trajectory of 75 cases. No new MRSA bacteraemias were reported again this month, so the Trust continues to remain ahead of its trajectory of 4 cases to November. Hand hygiene audits which provide a leading indicator for managing infection control demonstrate that 2 divisions are now achieving the 95% internal targets.
Access Targets and Winter Planning: Whilst ED indicators have been achieved to November, Total Time spent in A&E has fallen below the 95% target to just over 94% in the first two weeks of December. The current waiting list shows we have a challenging number of longer waiters in the following specialties: General Surgery (Bariatrics), Urology, Trauma & Orthopaedics, Neurosurgery and Gynaecology. They will be further challenged with the need to deliver 90% patients admitted within 18 weeks from April 2012 by specialty-level delivery requirements laid out in the recently published Operating Framework for 2012-13.
4
Executive Summary (2/3)
• Actions:
Finance position: Weekly Tuesday reviews continue and targeted reviews with Clinical Directors, Heads of Nursing and Divisional Managers are being organised as needed.
HCAI: An Independent/Expert review of Antibiotic usage took place on 22 November as planned. Following the report from this independent review, the Director of Nursing and Midwifery will write to Monitor. Further details are provided in the Infection Control update at the end of this report.
Access Targets and Winter Planning: Plans for managing winter pressures have been developed in two areas:
1)A Winter Resilience Plan is in place and being reported to the Board this month.
2)TEAM division have developed a revised action plan for managing current pressures, and actions reviewed at weekly emergency performance meeting. A summary is provided at the end of this report.
RTT validation to target 18-23 week waiting time patients is being carried out,, to enable early identification of RTT pressures in delivering the specialty-level standards proposed from April 2012 in the Operating Framework.
Regulatory
• Monitor Q3 position
The Trust is rating itself a score of 3.0 in the Monitor Compliance Framework for its interim Q3 position based on performance to November. This does give the Trust a Governance risk rating of Red, due to C-difficile cases being off-trajectory for 3 consecutive quarters. The downward quarterly trend in reported cases may allow Monitor to downgrade our rating to ‘Amber Red’.
•Care Quality Commission CQC Quality Risk Profile (QRP):
The CQC has just published a December QRP update for the Trust, with no major causes for concern. There has been 1 positive and 1 adverse movement in risk estimates, otherwise outcomes have remained the same apart from Outcome 13 (Staffing) which moved to low neutral from an “insufficient data” rating.
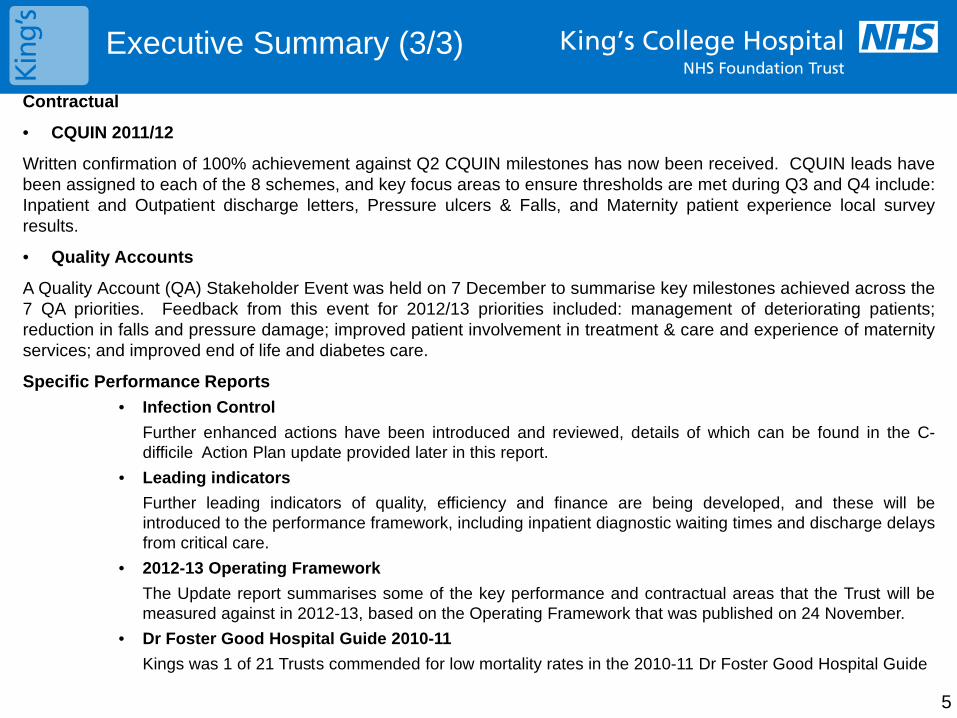
5
Executive Summary (3/3)
Contractual
• CQUIN 2011/12
Written confirmation of 100% achievement against Q2 CQUIN milestones has now been received. CQUIN leads have been assigned to each of the 8 schemes, and key focus areas to ensure thresholds are met during Q3 and Q4 include: Inpatient and Outpatient discharge letters, Pressure ulcers & Falls, and Maternity patient experience local survey results.
• Quality Accounts
A Quality Account (QA) Stakeholder Event was held on 7 December to summarise key milestones achieved across the 7 QA priorities. Feedback from this event for 2012/13 priorities included: management of deteriorating patients; reduction in falls and pressure damage; improved patient involvement in treatment & care and experience of maternity services; and improved end of life and diabetes care.
Specific Performance Reports • Infection Control Further enhanced actions have been introduced and reviewed, details of which can be found in the C-
difficile Action Plan update provided later in this report. • Leading indicators Further leading indicators of quality, efficiency and finance are being developed, and these will be
introduced to the performance framework, including inpatient diagnostic waiting times and discharge delays from critical care.
• 2012-13 Operating Framework The Update report summarises some of the key performance and contractual areas that the Trust will be
measured against in 2012-13, based on the Operating Framework that was published on 24 November. • Dr Foster Good Hospital Guide 2010-11 Kings was 1 of 21 Trusts commended for low mortality rates in the 2010-11 Dr Foster Good Hospital Guide
6
Contents
•Executive Summary
•Trust Performance Summary
•Divisional Performance Summary
•Regulatory/Contractual Performance • Monitor Q3 interim position
• Care Quality Commission (CQC) – Quality Risk Profile Update
• CQUIN 2011/12 and Quality Accounts Update
•Specific Performance Reports • Infection Control Update-13 Operating Framework
• Summary Winter Action Plan for Weekly Meetings
• Leading Indicators Report
• 2012-13 Operating Framework Update
• Dr Foster Good Hospital Guide 2010-11 Update
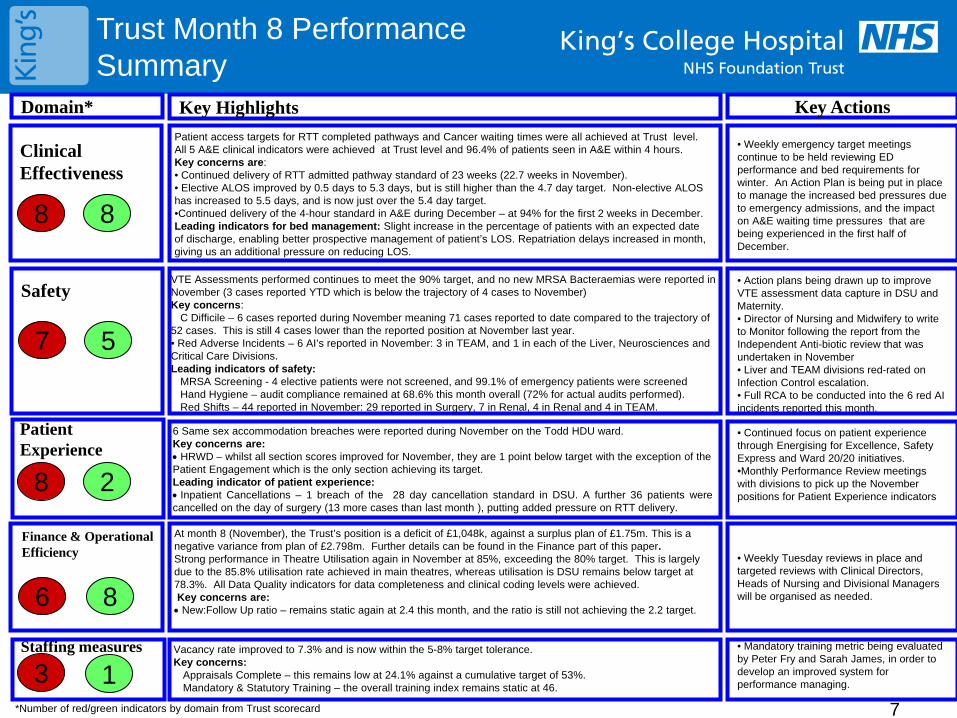
Trust Month 8 Performance Summary
Domain* Key Highlights Key Actions
• Weekly Tuesday reviews in place and targeted reviews with Clinical Directors, Heads of Nursing and Divisional Managers will be organised as needed.
8 8
Clinical Effectiveness
7
Safety
8 2
Patient Experience
6
Finance & Operational Efficiency
3 1 Staffing measures
5
8
Vacancy rate improved to 7.3% and is now within the 5-8% target tolerance. Key concerns:
Appraisals Complete – this remains low at 24.1% against a cumulative target of 53%. Mandatory & Statutory Training – the overall training index remains static at 46.
*Number of red/green indicators by domain from Trust scorecard
• Mandatory training metric being evaluated by Peter Fry and Sarah James, in order to develop an improved system for performance managing.
7
Patient access targets for RTT completed pathways and Cancer waiting times were all achieved at Trust level. All 5 A&E clinical indicators were achieved at Trust level and 96.4% of patients seen in A&E within 4 hours. Key concerns are: • Continued delivery of RTT admitted pathway standard of 23 weeks (22.7 weeks in November). • Elective ALOS improved by 0.5 days to 5.3 days, but is still higher than the 4.7 day target. Non-elective ALOS has increased to 5.5 days, and is now just over the 5.4 day target. •Continued delivery of the 4-hour standard in A&E during December – at 94% for the first 2 weeks in December. Leading indicators for bed management: Slight increase in the percentage of patients with an expected date of discharge, enabling better prospective management of patient’s LOS. Repatriation delays increased in month, giving us an additional pressure on reducing LOS.
VTE Assessments performed continues to meet the 90% target, and no new MRSA Bacteraemias were reported in November (3 cases reported YTD which is below the trajectory of 4 cases to November) Key concerns:
C Difficile – 6 cases reported during November meaning 71 cases reported to date compared to the trajectory of 52 cases. This is still 4 cases lower than the reported position at November last year. • Red Adverse Incidents – 6 AI’s reported in November: 3 in TEAM, and 1 in each of the Liver, Neurosciences and Critical Care Divisions. Leading indicators of safety:
MRSA Screening - 4 elective patients were not screened, and 99.1% of emergency patients were screened Hand Hygiene – audit compliance remained at 68.6% this month overall (72% for actual audits performed). Red Shifts – 44 reported in November: 29 reported in Surgery, 7 in Renal, 4 in Renal and 4 in TEAM.
6 Same sex accommodation breaches were reported during November on the Todd HDU ward. Key concerns are: • HRWD – whilst all section scores improved for November, they are 1 point below target with the exception of the Patient Engagement which is the only section achieving its target. Leading indicator of patient experience: • Inpatient Cancellations – 1 breach of the 28 day cancellation standard in DSU. A further 36 patients were cancelled on the day of surgery (13 more cases than last month ), putting added pressure on RTT delivery.
At month 8 (November), the Trust’s position is a deficit of £1,048k, against a surplus plan of £1.75m. This is a negative variance from plan of £2.798m. Further details can be found in the Finance part of this paper. Strong performance in Theatre Utilisation again in November at 85%, exceeding the 80% target. This is largely due to the 85.8% utilisation rate achieved in main theatres, whereas utilisation is DSU remains below target at 78.3%. All Data Quality indicators for data completeness and clinical coding levels were achieved. Key concerns are: • New:Follow Up ratio – remains static again at 2.4 this month, and the ratio is still not achieving the 2.2 target.
• Weekly emergency target meetings continue to be held reviewing ED performance and bed requirements for winter. An Action Plan is being put in place to manage the increased bed pressures due to emergency admissions, and the impact on A&E waiting time pressures that are being experienced in the first half of December.
• Action plans being drawn up to improve VTE assessment data capture in DSU and Maternity. • Director of Nursing and Midwifery to write to Monitor following the report from the Independent Anti-biotic review that was undertaken in November • Liver and TEAM divisions red-rated on Infection Control escalation. • Full RCA to be conducted into the 6 red AI incidents reported this month.
• Continued focus on patient experience through Energising for Excellence, Safety Express and Ward 20/20 initiatives. •Monthly Performance Review meetings with divisions to pick up the November positions for Patient Experience indicators
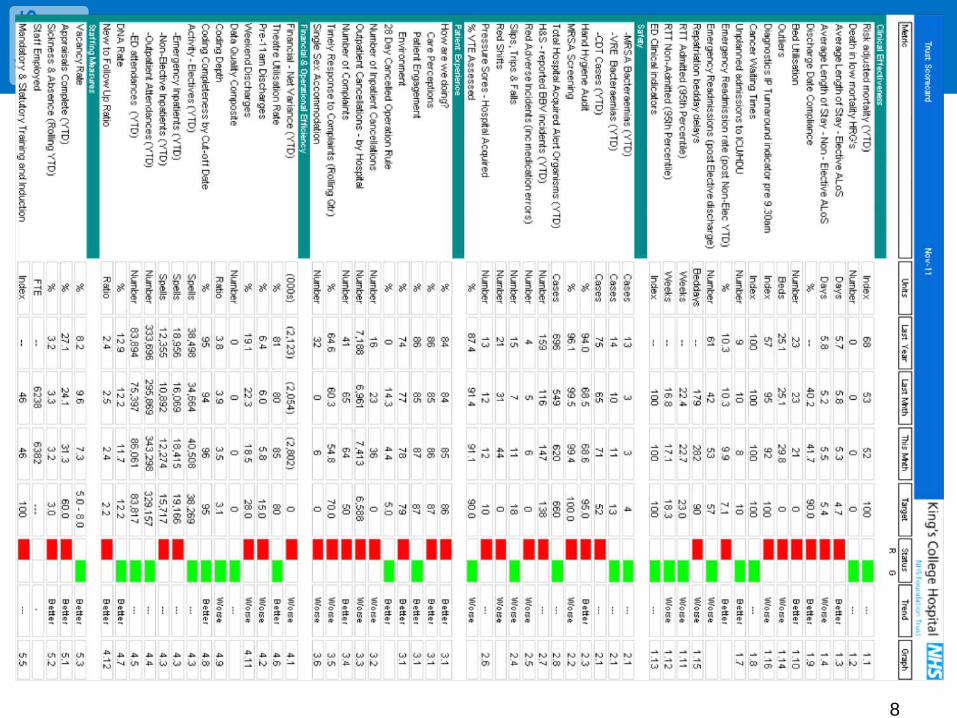
8
2011-12 M2 Trust Performance
9
Contents
•Executive Summary
•Trust Performance Summary
•Divisional Performance Summary
•Regulatory/Contractual Performance • Monitor Q3 interim position
• Care Quality Commission (CQC) – Quality Risk Profile Update
• CQUIN 2011/12 and Quality Accounts Update
•Specific Performance Reports • Infection Control Update-13 Operating Framework
• Summary Winter Action Plan for Weekly Meetings
• Leading Indicators Report
• 2012-13 Operating Framework Update
• Dr Foster Good Hospital Guide 2010-11 Update
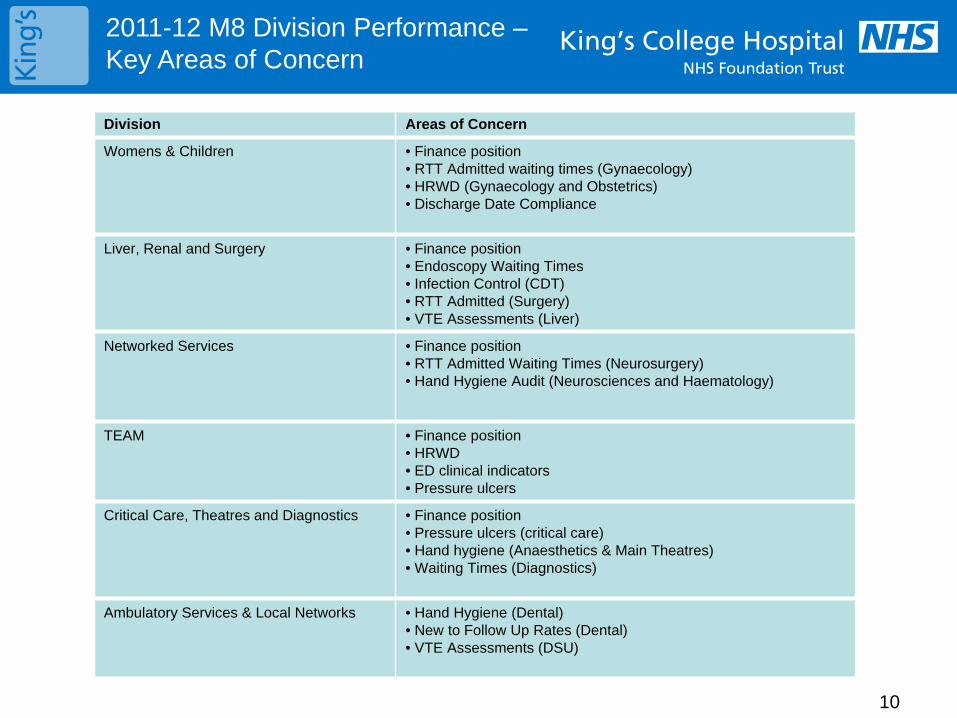
10
Division Areas of Concern
Womens & Children • Finance position • RTT Admitted waiting times (Gynaecology) • HRWD (Gynaecology and Obstetrics) • Discharge Date Compliance
Liver, Renal and Surgery
• Finance position • Endoscopy Waiting Times • Infection Control (CDT) • RTT Admitted (Surgery) • VTE Assessments (Liver)
Networked Services • Finance position • RTT Admitted Waiting Times (Neurosurgery) • Hand Hygiene Audit (Neurosciences and Haematology)
TEAM
• Finance position • HRWD • ED clinical indicators • Pressure ulcers
Critical Care, Theatres and Diagnostics
• Finance position • Pressure ulcers (critical care) • Hand hygiene (Anaesthetics & Main Theatres) • Waiting Times (Diagnostics)
Ambulatory Services & Local Networks
• Hand Hygiene (Dental) • New to Follow Up Rates (Dental) • VTE Assessments (DSU)
2011-12 M8 Division Performance – Key Areas of Concern
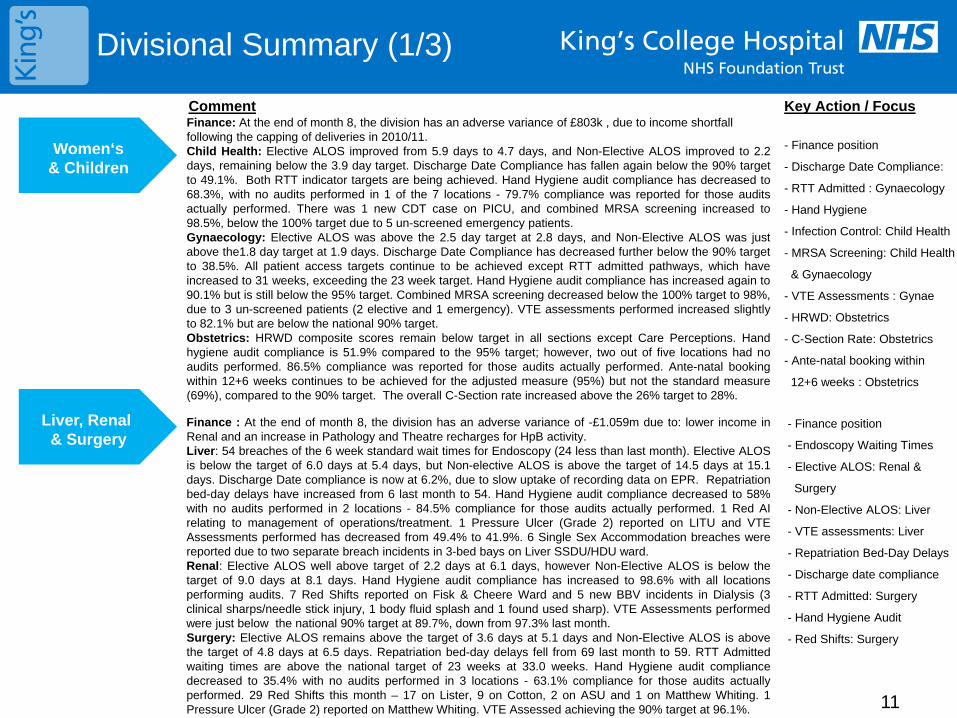
Divisional Summary (1/3)
Women‘s
& Children
Liver, Renal
& Surgery Finance : At the end of month 8, the division has an adverse variance of -£1.059m due to: lower income in Renal and an increase in Pathology and Theatre recharges for HpB activity. Liver: 54 breaches of the 6 week standard wait times for Endoscopy (24 less than last month). Elective ALOS is below the target of 6.0 days at 5.4 days, but Non-elective ALOS is above the target of 14.5 days at 15.1 days. Discharge Date compliance is now at 6.2%, due to slow uptake of recording data on EPR. Repatriation bed-day delays have increased from 6 last month to 54. Hand Hygiene audit compliance decreased to 58% with no audits performed in 2 locations - 84.5% compliance for those audits actually performed. 1 Red AI relating to management of operations/treatment. 1 Pressure Ulcer (Grade 2) reported on LITU and VTE Assessments performed has decreased from 49.4% to 41.9%. 6 Single Sex Accommodation breaches were reported due to two separate breach incidents in 3-bed bays on Liver SSDU/HDU ward. Renal: Elective ALOS well above target of 2.2 days at 6.1 days, however Non-Elective ALOS is below the target of 9.0 days at 8.1 days. Hand Hygiene audit compliance has increased to 98.6% with all locations performing audits. 7 Red Shifts reported on Fisk & Cheere Ward and 5 new BBV incidents in Dialysis (3 clinical sharps/needle stick injury, 1 body fluid splash and 1 found used sharp). VTE Assessments performed were just below the national 90% target at 89.7%, down from 97.3% last month. Surgery: Elective ALOS remains above the target of 3.6 days at 5.1 days and Non-Elective ALOS is above the target of 4.8 days at 6.5 days. Repatriation bed-day delays fell from 69 last month to 59. RTT Admitted waiting times are above the national target of 23 weeks at 33.0 weeks. Hand Hygiene audit compliance decreased to 35.4% with no audits performed in 3 locations - 63.1% compliance for those audits actually performed. 29 Red Shifts this month – 17 on Lister, 9 on Cotton, 2 on ASU and 1 on Matthew Whiting. 1 Pressure Ulcer (Grade 2) reported on Matthew Whiting. VTE Assessed achieving the 90% target at 96.1%.
Key Action / Focus Comment
- Finance position
- Endoscopy Waiting Times
- Elective ALOS: Renal &
Surgery
- Non-Elective ALOS: Liver
- VTE assessments: Liver
- Repatriation Bed-Day Delays
- Discharge date compliance
- RTT Admitted: Surgery
- Hand Hygiene Audit
- Red Shifts: Surgery
Finance: At the end of month 8, the division has an adverse variance of £803k , due to income shortfall following the capping of deliveries in 2010/11. Child Health: Elective ALOS improved from 5.9 days to 4.7 days, and Non-Elective ALOS improved to 2.2 days, remaining below the 3.9 day target. Discharge Date Compliance has fallen again below the 90% target to 49.1%. Both RTT indicator targets are being achieved. Hand Hygiene audit compliance has decreased to 68.3%, with no audits performed in 1 of the 7 locations - 79.7% compliance was reported for those audits actually performed. There was 1 new CDT case on PICU, and combined MRSA screening increased to 98.5%, below the 100% target due to 5 un-screened emergency patients. Gynaecology: Elective ALOS was above the 2.5 day target at 2.8 days, and Non-Elective ALOS was just above the1.8 day target at 1.9 days. Discharge Date Compliance has decreased further below the 90% target to 38.5%. All patient access targets continue to be achieved except RTT admitted pathways, which have increased to 31 weeks, exceeding the 23 week target. Hand Hygiene audit compliance has increased again to 90.1% but is still below the 95% target. Combined MRSA screening decreased below the 100% target to 98%, due to 3 un-screened patients (2 elective and 1 emergency). VTE assessments performed increased slightly to 82.1% but are below the national 90% target. Obstetrics: HRWD composite scores remain below target in all sections except Care Perceptions. Hand hygiene audit compliance is 51.9% compared to the 95% target; however, two out of five locations had no audits performed. 86.5% compliance was reported for those audits actually performed. Ante-natal booking within 12+6 weeks continues to be achieved for the adjusted measure (95%) but not the standard measure (69%), compared to the 90% target. The overall C-Section rate increased above the 26% target to 28%.
- Finance position
- Discharge Date Compliance:
- RTT Admitted : Gynaecology
- Hand Hygiene
- Infection Control: Child Health
- MRSA Screening: Child Health
& Gynaecology
- VTE Assessments : Gynae
- HRWD: Obstetrics
- C-Section Rate: Obstetrics
- Ante-natal booking within
12+6 weeks : Obstetrics
11
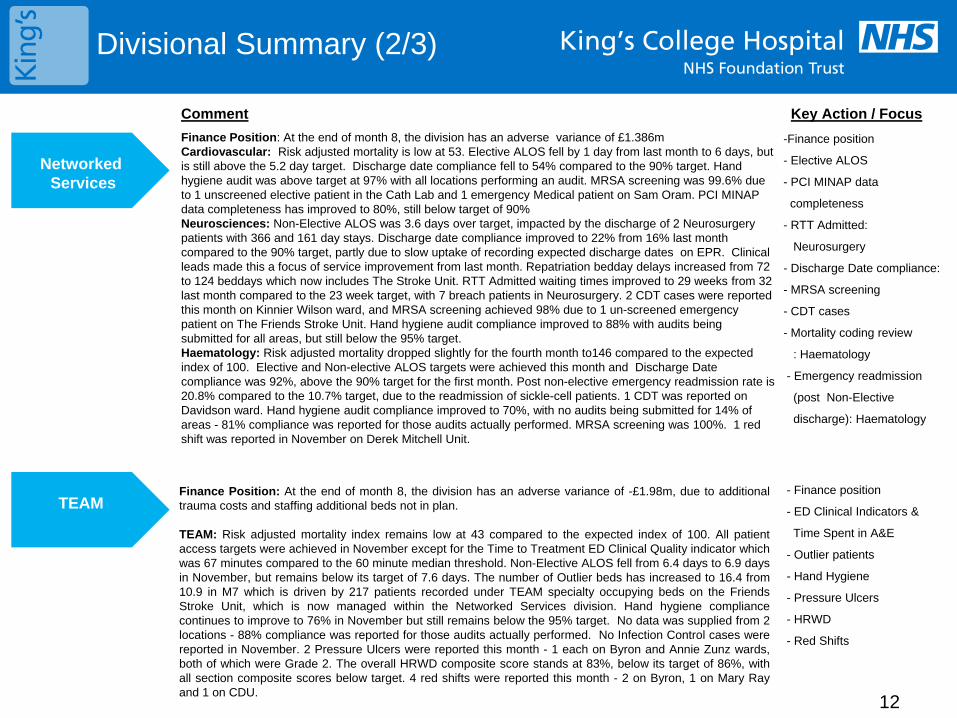
Divisional Summary (2/3)
Networked Services
TEAM
Finance Position: At the end of month 8, the division has an adverse variance of £1.386m Cardiovascular: Risk adjusted mortality is low at 53. Elective ALOS fell by 1 day from last month to 6 days, but is still above the 5.2 day target. Discharge date compliance fell to 54% compared to the 90% target. Hand hygiene audit was above target at 97% with all locations performing an audit. MRSA screening was 99.6% due to 1 unscreened elective patient in the Cath Lab and 1 emergency Medical patient on Sam Oram. PCI MINAP data completeness has improved to 80%, still below target of 90% Neurosciences: Non-Elective ALOS was 3.6 days over target, impacted by the discharge of 2 Neurosurgery patients with 366 and 161 day stays. Discharge date compliance improved to 22% from 16% last month compared to the 90% target, partly due to slow uptake of recording expected discharge dates on EPR. Clinical leads made this a focus of service improvement from last month. Repatriation bedday delays increased from 72 to 124 beddays which now includes The Stroke Unit. RTT Admitted waiting times improved to 29 weeks from 32 last month compared to the 23 week target, with 7 breach patients in Neurosurgery. 2 CDT cases were reported this month on Kinnier Wilson ward, and MRSA screening achieved 98% due to 1 un-screened emergency patient on The Friends Stroke Unit. Hand hygiene audit compliance improved to 88% with audits being submitted for all areas, but still below the 95% target. Haematology: Risk adjusted mortality dropped slightly for the fourth month to146 compared to the expected index of 100. Elective and Non-elective ALOS targets were achieved this month and Discharge Date compliance was 92%, above the 90% target for the first month. Post non-elective emergency readmission rate is 20.8% compared to the 10.7% target, due to the readmission of sickle-cell patients. 1 CDT was reported on Davidson ward. Hand hygiene audit compliance improved to 70%, with no audits being submitted for 14% of areas - 81% compliance was reported for those audits actually performed. MRSA screening was 100%. 1 red shift was reported in November on Derek Mitchell Unit.
12
Comment Key Action / Focus
Finance Position: At the end of month 8, the division has an adverse variance of -£1.98m, due to additional trauma costs and staffing additional beds not in plan. TEAM: Risk adjusted mortality index remains low at 43 compared to the expected index of 100. All patient access targets were achieved in November except for the Time to Treatment ED Clinical Quality indicator which was 67 minutes compared to the 60 minute median threshold. Non-Elective ALOS fell from 6.4 days to 6.9 days in November, but remains below its target of 7.6 days. The number of Outlier beds has increased to 16.4 from 10.9 in M7 which is driven by 217 patients recorded under TEAM specialty occupying beds on the Friends Stroke Unit, which is now managed within the Networked Services division. Hand hygiene compliance continues to improve to 76% in November but still remains below the 95% target. No data was supplied from 2 locations - 88% compliance was reported for those audits actually performed. No Infection Control cases were reported in November. 2 Pressure Ulcers were reported this month - 1 each on Byron and Annie Zunz wards, both of which were Grade 2. The overall HRWD composite score stands at 83%, below its target of 86%, with all section composite scores below target. 4 red shifts were reported this month - 2 on Byron, 1 on Mary Ray and 1 on CDU.
- Finance position
- ED Clinical Indicators &
Time Spent in A&E
- Outlier patients
- Hand Hygiene
- Pressure Ulcers
- HRWD
- Red Shifts
-Finance position
- Elective ALOS
- PCI MINAP data
completeness
- RTT Admitted:
Neurosurgery
- Discharge Date compliance:
- MRSA screening
- CDT cases
- Mortality coding review
: Haematology
- Emergency readmission
(post Non-Elective
discharge): Haematology
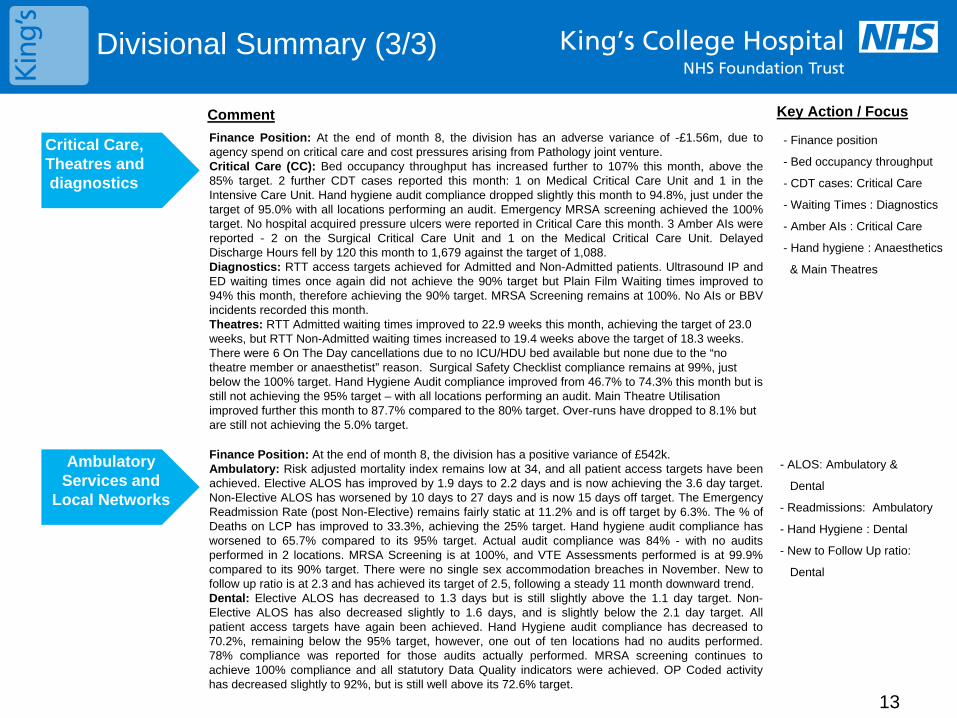
Divisional Summary (3/3)
Critical Care, Theatres and diagnostics
Ambulatory Services and
Local Networks
Finance Position: At the end of month 8, the division has an adverse variance of -£1.56m, due to agency spend on critical care and cost pressures arising from Pathology joint venture. Critical Care (CC): Bed occupancy throughput has increased further to 107% this month, above the 85% target. 2 further CDT cases reported this month: 1 on Medical Critical Care Unit and 1 in the Intensive Care Unit. Hand hygiene audit compliance dropped slightly this month to 94.8%, just under the target of 95.0% with all locations performing an audit. Emergency MRSA screening achieved the 100% target. No hospital acquired pressure ulcers were reported in Critical Care this month. 3 Amber AIs were reported - 2 on the Surgical Critical Care Unit and 1 on the Medical Critical Care Unit. Delayed Discharge Hours fell by 120 this month to 1,679 against the target of 1,088. Diagnostics: RTT access targets achieved for Admitted and Non-Admitted patients. Ultrasound IP and ED waiting times once again did not achieve the 90% target but Plain Film Waiting times improved to 94% this month, therefore achieving the 90% target. MRSA Screening remains at 100%. No AIs or BBV incidents recorded this month. Theatres: RTT Admitted waiting times improved to 22.9 weeks this month, achieving the target of 23.0 weeks, but RTT Non-Admitted waiting times increased to 19.4 weeks above the target of 18.3 weeks. There were 6 On The Day cancellations due to no ICU/HDU bed available but none due to the “no theatre member or anaesthetist” reason. Surgical Safety Checklist compliance remains at 99%, just below the 100% target. Hand Hygiene Audit compliance improved from 46.7% to 74.3% this month but is still not achieving the 95% target – with all locations performing an audit. Main Theatre Utilisation improved further this month to 87.7% compared to the 80% target. Over-runs have dropped to 8.1% but are still not achieving the 5.0% target.
Finance Position: At the end of month 8, the division has a positive variance of £542k. Ambulatory: Risk adjusted mortality index remains low at 34, and all patient access targets have been achieved. Elective ALOS has improved by 1.9 days to 2.2 days and is now achieving the 3.6 day target. Non-Elective ALOS has worsened by 10 days to 27 days and is now 15 days off target. The Emergency Readmission Rate (post Non-Elective) remains fairly static at 11.2% and is off target by 6.3%. The % of Deaths on LCP has improved to 33.3%, achieving the 25% target. Hand hygiene audit compliance has worsened to 65.7% compared to its 95% target. Actual audit compliance was 84% - with no audits performed in 2 locations. MRSA Screening is at 100%, and VTE Assessments performed is at 99.9% compared to its 90% target. There were no single sex accommodation breaches in November. New to follow up ratio is at 2.3 and has achieved its target of 2.5, following a steady 11 month downward trend. Dental: Elective ALOS has decreased to 1.3 days but is still slightly above the 1.1 day target. Non-Elective ALOS has also decreased slightly to 1.6 days, and is slightly below the 2.1 day target. All patient access targets have again been achieved. Hand Hygiene audit compliance has decreased to 70.2%, remaining below the 95% target, however, one out of ten locations had no audits performed. 78% compliance was reported for those audits actually performed. MRSA screening continues to achieve 100% compliance and all statutory Data Quality indicators were achieved. OP Coded activity has decreased slightly to 92%, but is still well above its 72.6% target.
13
- Finance position
- Bed occupancy throughput
- CDT cases: Critical Care
- Waiting Times : Diagnostics
- Amber AIs : Critical Care
- Hand hygiene : Anaesthetics
& Main Theatres
Comment Key Action / Focus
- ALOS: Ambulatory &
Dental
- Readmissions: Ambulatory
- Hand Hygiene : Dental
- New to Follow Up ratio:
Dental

2011-12 M8 Trust & Division Heatmap (1/2)
14
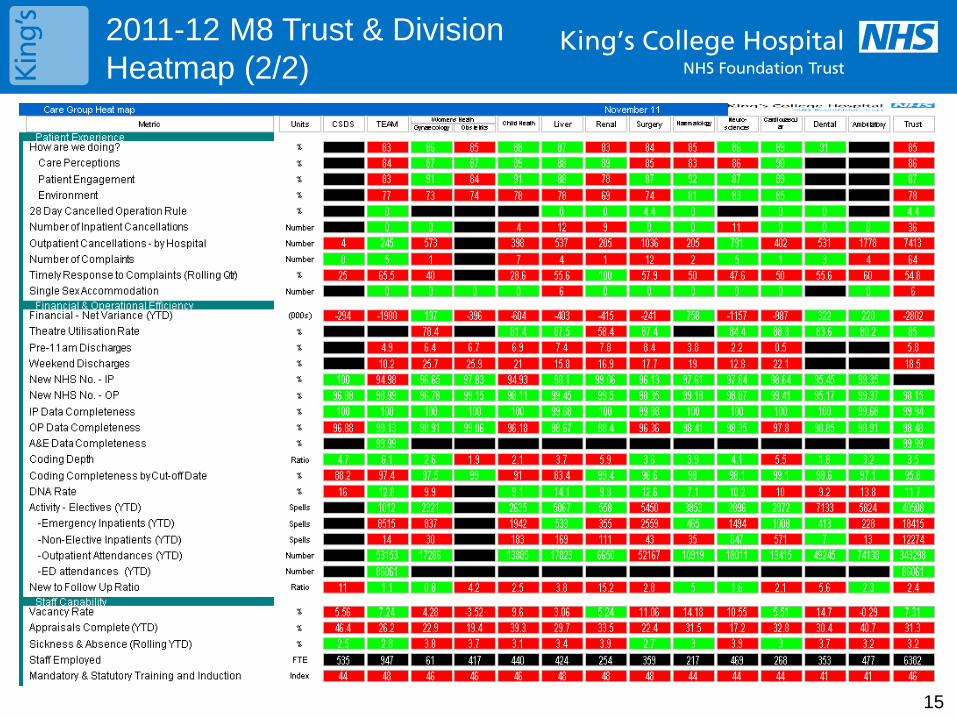
2011-12 M8 Trust & Division Heatmap (2/2)
15
16
Contents
•Executive Summary
•Trust Performance Summary
•Divisional Performance Summary
•Regulatory/Contractual Performance • Monitor Q3 interim position
• Care Quality Commission (CQC) – Quality Risk Profile Update
• CQUIN 2011/12 and Quality Accounts Update
•Specific Performance Reports • Infection Control Update-13 Operating Framework
• Summary Winter Action Plan for Weekly Meetings
• Leading Indicators Report
• 2012-13 Operating Framework Update
• Dr Foster Good Hospital Guide 2010-11 Update
Regulatory/Contractual Performance 2011/12 (1/2)
17
Regulatory
• Monitor Governance Rating Q3:
The Trust is rating itself a score of 3.0 in the Monitor Compliance Framework for the interim Q3 position based on November reported performance, giving the Trust a governance risk rating of Red, due to C-difficile cases being off-trajectory for 3 consecutive quarters.
The Trust reported an additional 6 c-difficile cases in November, and therefore has 71 cases attributed to the Trust YTD. This does mean that the Trust has already exceeded its Q3 trajectory of 58 cases. The Trust is showing a downward trend Q1 = 32 cases, Q2 = 24 cases, Q3 to date 15 cases. This downward trend will allow Monitor to make a possible decision to down grade our rating to Amber-red. No new MRSA bacteraemias were reported this month, so the Trust continues to remain ahead of its trajectory.
All Referral to Treatment and Cancer waiting time targets have been achieved in November. The 95% threshold for Total Time spent in ED within 4 hours was just achieved, with November’s performance at 96.4%.
Actions: Director of Nursing and Midwifery to write to Monitor following the report from the Independent Anti-biotic review that was undertaken in November and the improved C-difficile performance.
• Care Quality Commission (CQC) Quality Risk Profile:
The December QRP risk profile has just been published by the CQC. Positive risk movements were observed for Outcome 10 (Safety and Suitability of Premises) from high neutral to low neutral. There was 1 adverse movement in risk estimates:
“Outcome 5: Meeting Nutritional needs” – moved adversely from high green to low neutral. The indicator ratings remain unchanged, and the slight movement appears to be related to CQC statistical modelling.
All other outcomes remain the same with the exception of “Outcome 13: Staffing” – which is now reported as low neutral having moved from a rating of “insufficient data”.
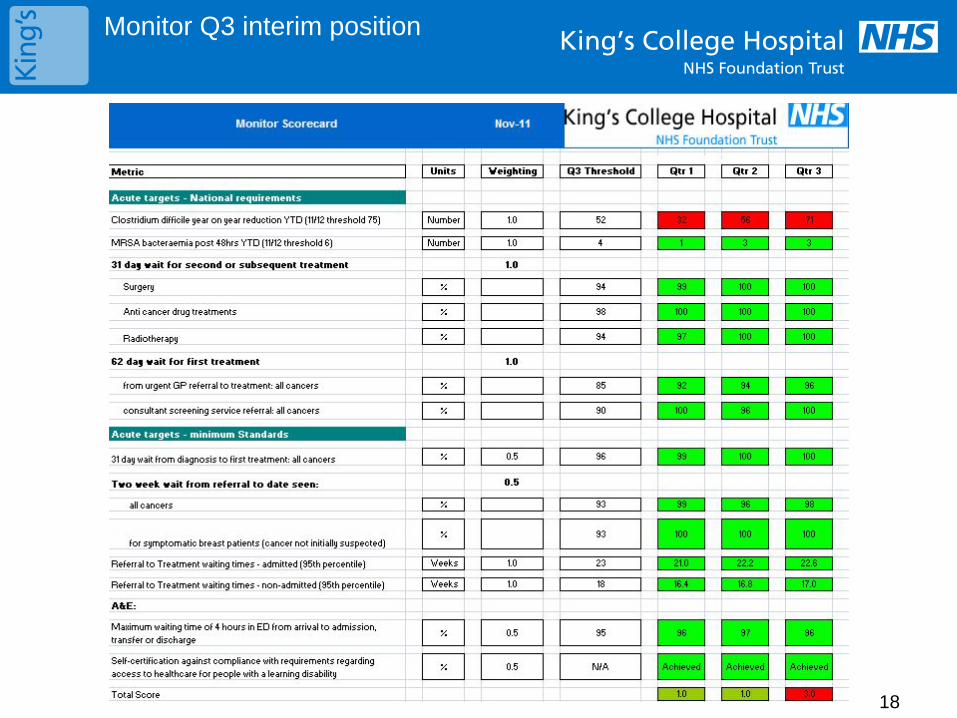
Monitor Q3 interim position
18
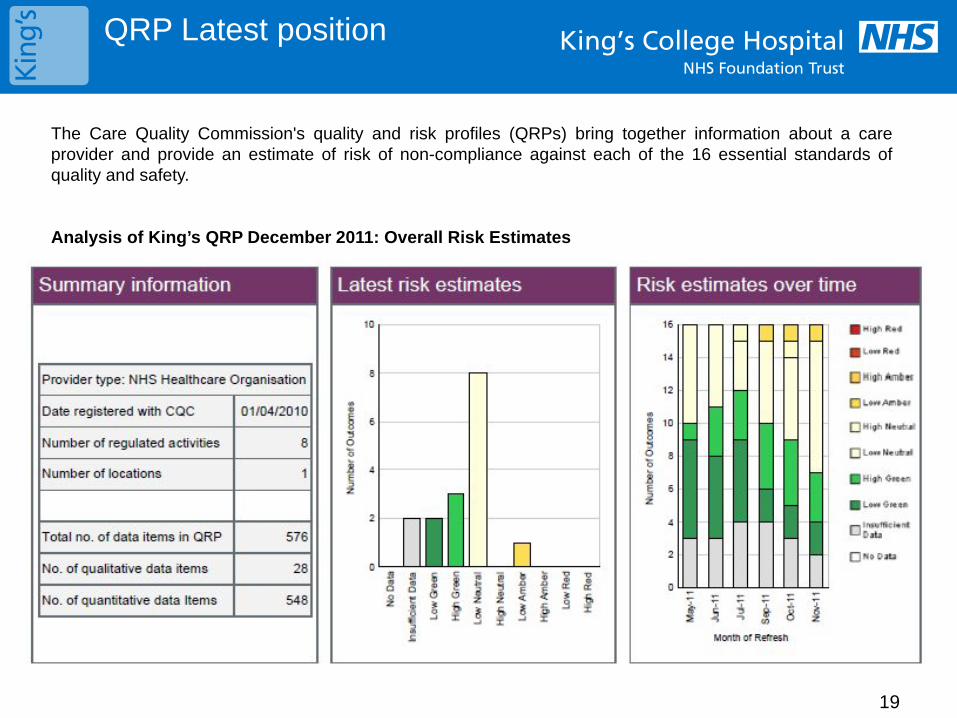
QRP Latest position
19
The Care Quality Commission's quality and risk profiles (QRPs) bring together information about a care provider and provide an estimate of risk of non-compliance against each of the 16 essential standards of quality and safety.
Analysis of King’s QRP December 2011: Overall Risk Estimates

Regulatory/Contractual Performance 2011/12 (2/2)
20
Regulatory
• CQUIN
Written confirmation of 100% achievement against Q2 CQUIN milestones has been received. Formal confirmation pending final agreement of Q3 and Q4 targets.
An additional £1.87m and £2.05m is attributed to Q3 and Q4 performance. CQUIN leads assigned to each of the 8 schemes and key focus areas for the rest of the year is to ensure thresholds are met for:
Inpatient Discharge Summaries and Outpatient Discharge (Q3 - £191k, Q4 - £191k)
Pressure Ulcers and Falls (Q3 - £300k, Q4 - £260k)
Maternity Patient Experience local survey results (Q3 - £200k, Q4 - £200k).
Actions: Final agreement from commissioners to be reached in December and regular progress meeting scheduled with internal CQUIN leads until the end of Q4.
• Quality Accounts
On 7 December, the Trust hosted a Quality Account Stakeholder event to summarise key milestones achieved across the seven Quality Accounts Priorities so far in 11/12. Attendees were given an opportunity to prioritise outcomes for 12/13. Feedback included:
Safety: to improve the identification and escalation of acutely ill patients, and reduce harm from falls and pressure damage.
Patient Experience: to improve the way that we involve patients in their care and treatment and experience of maternity services
Patient Outcomes: to improve end of life and diabetes care
Actions: Liaise with local commissioners, OSC and internal committees to develop objectives and performance metrics ahead of the next stakeholder event in January 2012.
21
Contents
•Executive Summary
•Trust Performance Summary
•Divisional Performance Summary
•Regulatory/Contractual Performance • Monitor Q3 interim position
• Care Quality Commission (CQC) – Quality Risk Profile Update
• CQUIN 2011/12 and Quality Accounts Update
•Specific Performance Reports • Infection Control Update-13 Operating Framework
• Summary Winter Action Plan for Weekly Meetings
• Leading Indicators Report
• 2012-13 Operating Framework Update
• Dr Foster Good Hospital Guide 2010-11 Update
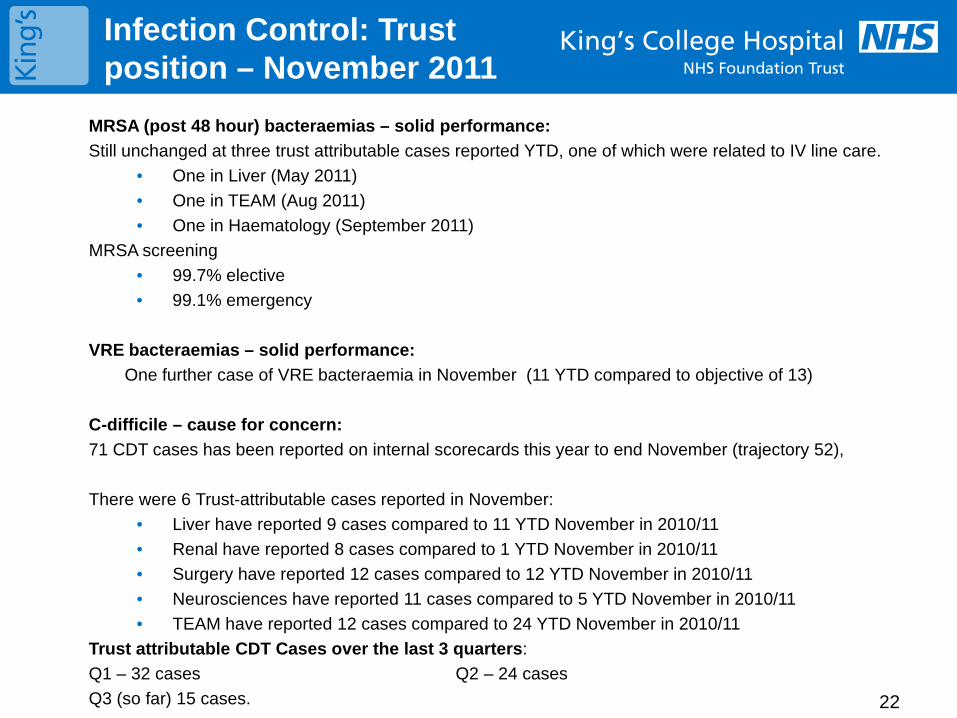
Infection Control: Trust position – November 2011
22
MRSA (post 48 hour) bacteraemias – solid performance: Still unchanged at three trust attributable cases reported YTD, one of which were related to IV line care.
• One in Liver (May 2011) • One in TEAM (Aug 2011) • One in Haematology (September 2011)
MRSA screening • 99.7% elective • 99.1% emergency
VRE bacteraemias – solid performance:
One further case of VRE bacteraemia in November (11 YTD compared to objective of 13)
C-difficile – cause for concern: 71 CDT cases has been reported on internal scorecards this year to end November (trajectory 52), There were 6 Trust-attributable cases reported in November:
• Liver have reported 9 cases compared to 11 YTD November in 2010/11 • Renal have reported 8 cases compared to 1 YTD November in 2010/11 • Surgery have reported 12 cases compared to 12 YTD November in 2010/11 • Neurosciences have reported 11 cases compared to 5 YTD November in 2010/11 • TEAM have reported 12 cases compared to 24 YTD November in 2010/11
Trust attributable CDT Cases over the last 3 quarters: Q1 – 32 cases Q2 – 24 cases Q3 (so far) 15 cases.
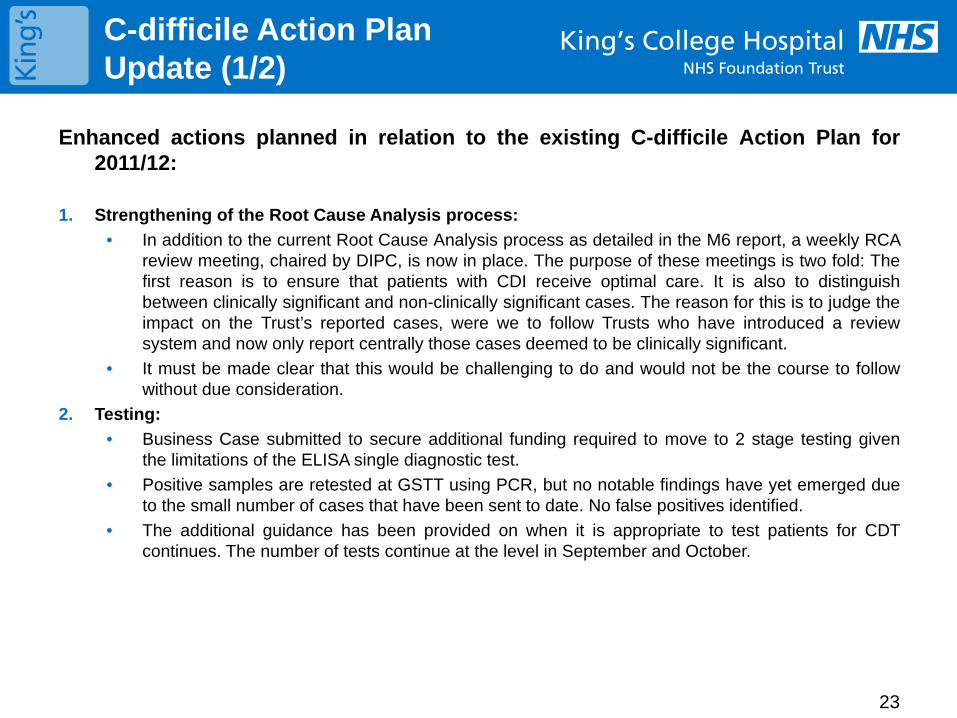
C-difficile Action Plan Update (1/2)
23
Enhanced actions planned in relation to the existing C-difficile Action Plan for 2011/12:
1. Strengthening of the Root Cause Analysis process: • In addition to the current Root Cause Analysis process as detailed in the M6 report, a weekly RCA
review meeting, chaired by DIPC, is now in place. The purpose of these meetings is two fold: The first reason is to ensure that patients with CDI receive optimal care. It is also to distinguish between clinically significant and non-clinically significant cases. The reason for this is to judge the impact on the Trust’s reported cases, were we to follow Trusts who have introduced a review system and now only report centrally those cases deemed to be clinically significant.
• It must be made clear that this would be challenging to do and would not be the course to follow without due consideration.
2. Testing: • Business Case submitted to secure additional funding required to move to 2 stage testing given
the limitations of the ELISA single diagnostic test. • Positive samples are retested at GSTT using PCR, but no notable findings have yet emerged due
to the small number of cases that have been sent to date. No false positives identified. • The additional guidance has been provided on when it is appropriate to test patients for CDT
continues. The number of tests continue at the level in September and October.
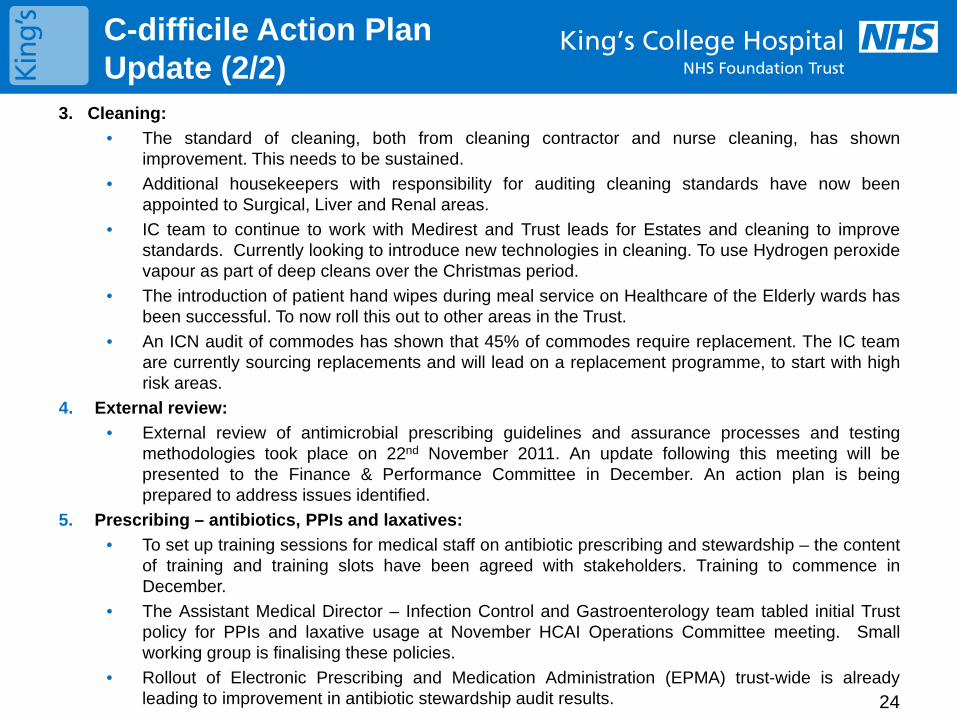
C-difficile Action Plan Update (2/2)
24
3. Cleaning: • The standard of cleaning, both from cleaning contractor and nurse cleaning, has shown
improvement. This needs to be sustained. • Additional housekeepers with responsibility for auditing cleaning standards have now been
appointed to Surgical, Liver and Renal areas. • IC team to continue to work with Medirest and Trust leads for Estates and cleaning to improve
standards. Currently looking to introduce new technologies in cleaning. To use Hydrogen peroxide vapour as part of deep cleans over the Christmas period.
• The introduction of patient hand wipes during meal service on Healthcare of the Elderly wards has been successful. To now roll this out to other areas in the Trust.
• An ICN audit of commodes has shown that 45% of commodes require replacement. The IC team are currently sourcing replacements and will lead on a replacement programme, to start with high risk areas.
4. External review: • External review of antimicrobial prescribing guidelines and assurance processes and testing
methodologies took place on 22nd November 2011. An update following this meeting will be presented to the Finance & Performance Committee in December. An action plan is being prepared to address issues identified.
5. Prescribing – antibiotics, PPIs and laxatives: • To set up training sessions for medical staff on antibiotic prescribing and stewardship – the content
of training and training slots have been agreed with stakeholders. Training to commence in December.
• The Assistant Medical Director – Infection Control and Gastroenterology team tabled initial Trust policy for PPIs and laxative usage at November HCAI Operations Committee meeting. Small working group is finalising these policies.
• Rollout of Electronic Prescribing and Medication Administration (EPMA) trust-wide is already leading to improvement in antibiotic stewardship audit results.
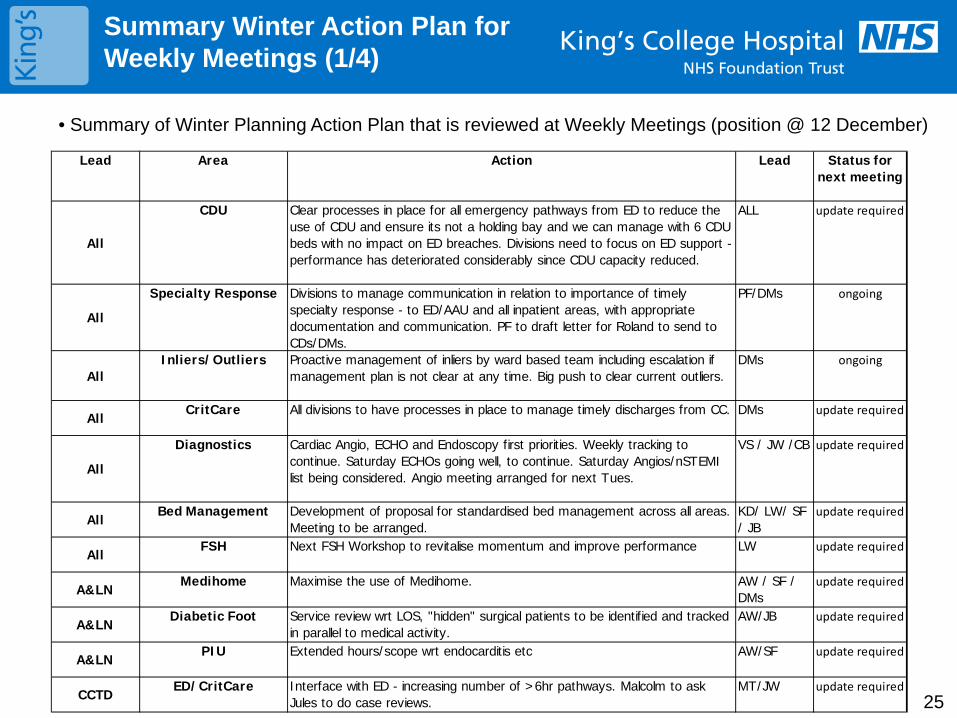
25
Summary Winter Action Plan for Weekly Meetings (1/4)
Lead Area Action Lead Status for next meeting
All
CDU Clear processes in place for all emergency pathways from ED to reduce the use of CDU and ensure its not a holding bay and we can manage with 6 CDU beds with no impact on ED breaches. Divisions need to focus on ED support - performance has deteriorated considerably since CDU capacity reduced.
ALL update required
All
Specialty Response Divisions to manage communication in relation to importance of timely specialty response - to ED/AAU and all inpatient areas, with appropriate documentation and communication. PF to draft letter for Roland to send to CDs/DMs.
PF/DMs ongoing
AllInliers/Outliers Proactive management of inliers by ward based team including escalation if
management plan is not clear at any time. Big push to clear current outliers.DMs ongoing
AllCritCare All divisions to have processes in place to manage timely discharges from CC. DMs update required
All
Diagnostics Cardiac Angio, ECHO and Endoscopy first priorities. Weekly tracking to continue. Saturday ECHOs going well, to continue. Saturday Angios/nSTEMI list being considered. Angio meeting arranged for next Tues.
VS / JW /CB update required
AllBed Management Development of proposal for standardised bed management across all areas.
Meeting to be arranged.KD/ LW/ SF / JB
update required
AllFSH Next FSH Workshop to revitalise momentum and improve performance LW update required
A&LNMedihome Maximise the use of Medihome. AW / SF /
DMsupdate required
A&LNDiabetic Foot Service review wrt LOS, "hidden" surgical patients to be identified and tracked
in parallel to medical activity.AW/JB update required
A&LNPIU Extended hours/scope wrt endocarditis etc AW/SF update required
CCTDED/CritCare Interface with ED - increasing number of >6hr pathways. Malcolm to ask
Jules to do case reviews.MT/JW update required
• Summary of Winter Planning Action Plan that is reviewed at Weekly Meetings (position @ 12 December)
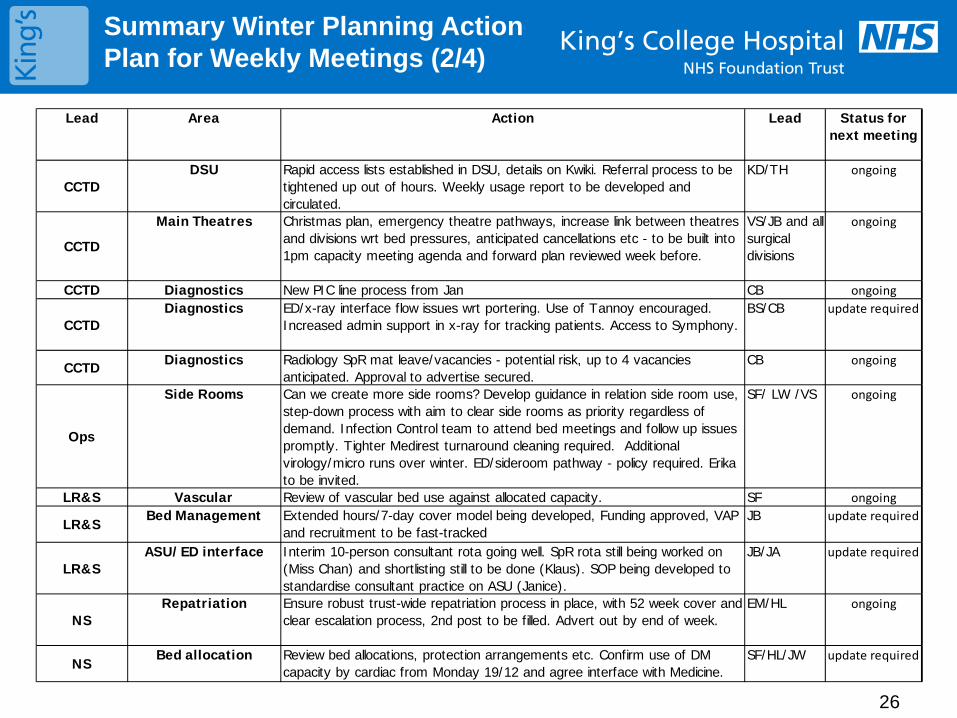
26
Summary Winter Planning Action Plan for Weekly Meetings (2/4)
Lead Area Action Lead Status for next meeting
CCTDDSU Rapid access lists established in DSU, details on Kwiki. Referral process to be
tightened up out of hours. Weekly usage report to be developed and circulated.
KD/TH ongoing
CCTD
Main Theatres Christmas plan, emergency theatre pathways, increase link between theatres and divisions wrt bed pressures, anticipated cancellations etc - to be built into 1pm capacity meeting agenda and forward plan reviewed week before.
VS/JB and all surgical divisions
ongoing
CCTD Diagnostics New PIC line process from Jan CB ongoing
CCTDDiagnostics ED/x-ray interface flow issues wrt portering. Use of Tannoy encouraged.
Increased admin support in x-ray for tracking patients. Access to Symphony.BS/CB update required
CCTD Diagnostics Radiology SpR mat leave/vacancies - potential risk, up to 4 vacancies anticipated. Approval to advertise secured.
CB ongoing
Ops
Side Rooms Can we create more side rooms? Develop guidance in relation side room use, step-down process with aim to clear side rooms as priority regardless of demand. Infection Control team to attend bed meetings and follow up issues promptly. Tighter Medirest turnaround cleaning required. Additional virology/micro runs over winter. ED/sideroom pathway - policy required. Erika to be invited.
SF/ LW /VS ongoing
LR&S Vascular Review of vascular bed use against allocated capacity. SF ongoing
LR&SBed Management Extended hours/7-day cover model being developed, Funding approved, VAP
and recruitment to be fast-trackedJB update required
LR&SASU/ED interface Interim 10-person consultant rota going well. SpR rota still being worked on
(Miss Chan) and shortlisting still to be done (Klaus). SOP being developed to standardise consultant practice on ASU (Janice).
JB/JA update required
NSRepatriation Ensure robust trust-wide repatriation process in place, with 52 week cover and
clear escalation process, 2nd post to be filled. Advert out by end of week.EM/HL ongoing
NSBed allocation Review bed allocations, protection arrangements etc. Confirm use of DM
capacity by cardiac from Monday 19/12 and agree interface with Medicine.SF/HL/JW update required
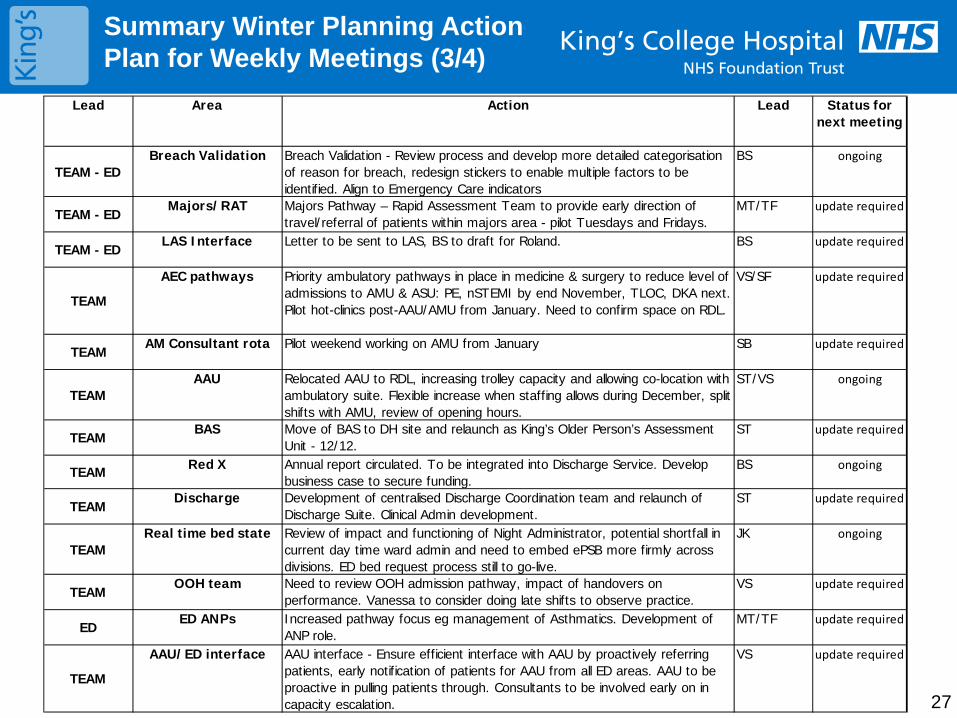
27
Summary Winter Planning Action Plan for Weekly Meetings (3/4)
Lead Area Action Lead Status for next meeting
TEAM - EDBreach Validation Breach Validation - Review process and develop more detailed categorisation
of reason for breach, redesign stickers to enable multiple factors to be identified. Align to Emergency Care indicators
BS ongoing
TEAM - EDMajors/RAT Majors Pathway – Rapid Assessment Team to provide early direction of
travel/referral of patients within majors area - pilot Tuesdays and Fridays.MT/TF update required
TEAM - EDLAS Interface Letter to be sent to LAS, BS to draft for Roland. BS update required
TEAM
AEC pathways Priority ambulatory pathways in place in medicine & surgery to reduce level of admissions to AMU & ASU: PE, nSTEMI by end November, TLOC, DKA next. Pilot hot-clinics post-AAU/AMU from January. Need to confirm space on RDL.
VS/SF update required
TEAMAM Consultant rota Pilot weekend working on AMU from January SB update required
TEAMAAU Relocated AAU to RDL, increasing trolley capacity and allowing co-location with
ambulatory suite. Flexible increase when staffing allows during December, split shifts with AMU, review of opening hours.
ST/VS ongoing
TEAMBAS Move of BAS to DH site and relaunch as King’s Older Person’s Assessment
Unit - 12/12.ST update required
TEAM Red X Annual report circulated. To be integrated into Discharge Service. Develop business case to secure funding.
BS ongoing
TEAMDischarge Development of centralised Discharge Coordination team and relaunch of
Discharge Suite. Clinical Admin development.ST update required
TEAMReal time bed state Review of impact and functioning of Night Administrator, potential shortfall in
current day time ward admin and need to embed ePSB more firmly across divisions. ED bed request process still to go-live.
JK ongoing
TEAMOOH team Need to review OOH admission pathway, impact of handovers on
performance. Vanessa to consider doing late shifts to observe practice. VS update required
EDED ANPs Increased pathway focus eg management of Asthmatics. Development of
ANP role. MT/TF update required
TEAM
AAU/ED interface AAU interface - Ensure efficient interface with AAU by proactively referring patients, early notification of patients for AAU from all ED areas. AAU to be proactive in pulling patients through. Consultants to be involved early on in capacity escalation.
VS update required
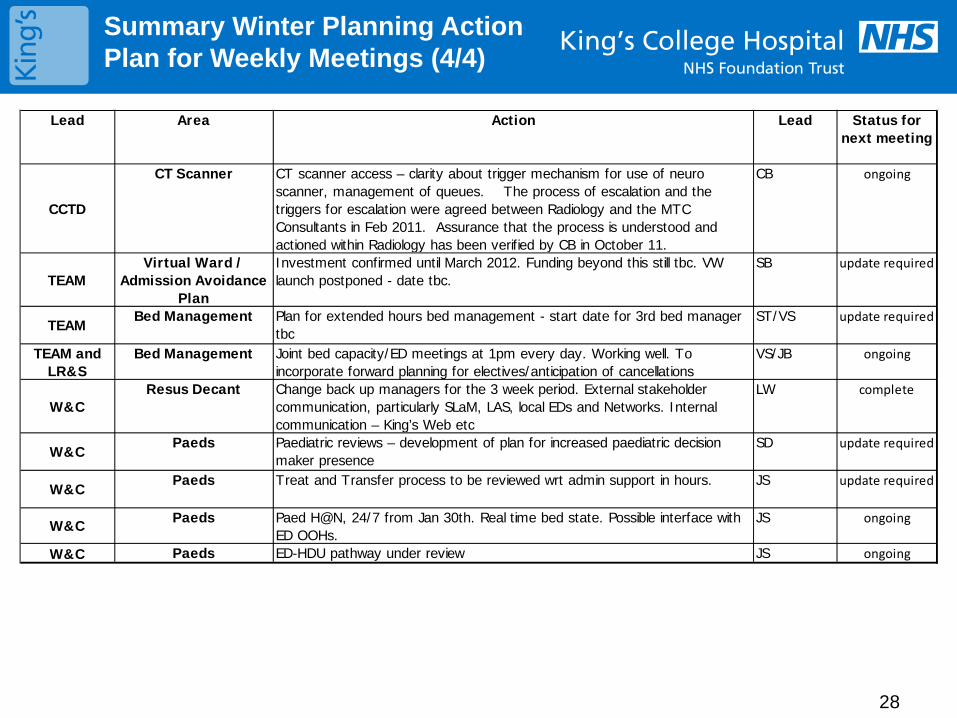
28
Summary Winter Planning Action Plan for Weekly Meetings (4/4)
Lead Area Action Lead Status for next meeting
CCTD
CT Scanner CT scanner access – clarity about trigger mechanism for use of neuro scanner, management of queues. The process of escalation and the triggers for escalation were agreed between Radiology and the MTC Consultants in Feb 2011. Assurance that the process is understood and actioned within Radiology has been verified by CB in October 11.
CB ongoing
TEAMVirtual Ward /
Admission Avoidance Plan
Investment confirmed until March 2012. Funding beyond this still tbc. VW launch postponed - date tbc.
SB update required
TEAMBed Management Plan for extended hours bed management - start date for 3rd bed manager
tbcST/VS update required
TEAM and LR&S
Bed Management Joint bed capacity/ED meetings at 1pm every day. Working well. To incorporate forward planning for electives/anticipation of cancellations
VS/JB ongoing
W&CResus Decant Change back up managers for the 3 week period. External stakeholder
communication, particularly SLaM, LAS, local EDs and Networks. Internal communication – King’s Web etc
LW complete
W&CPaeds Paediatric reviews – development of plan for increased paediatric decision
maker presence SD update required
W&CPaeds Treat and Transfer process to be reviewed wrt admin support in hours. JS update required
W&C Paeds Paed H@N, 24/7 from Jan 30th. Real time bed state. Possible interface with ED OOHs.
JS ongoing
W&C Paeds ED-HDU pathway under review JS ongoing
29
Leading and lagging /output Key Performance Indicators
• We have consistently tracked a number of lagging/output KPI’s, predominately as part of the regulatory agenda
• We have introduced leading indicators into scorecards, for example Estimated Date of Discharge, VTE Assessment as part of the regulatory agenda but also as strategic priorities
• We are developing more leading indicators of quality, efficiency and finance and these will be introduced to the performance framework e.g. Inpatient diagnostic wait times, delays in discharge for critical care etc.
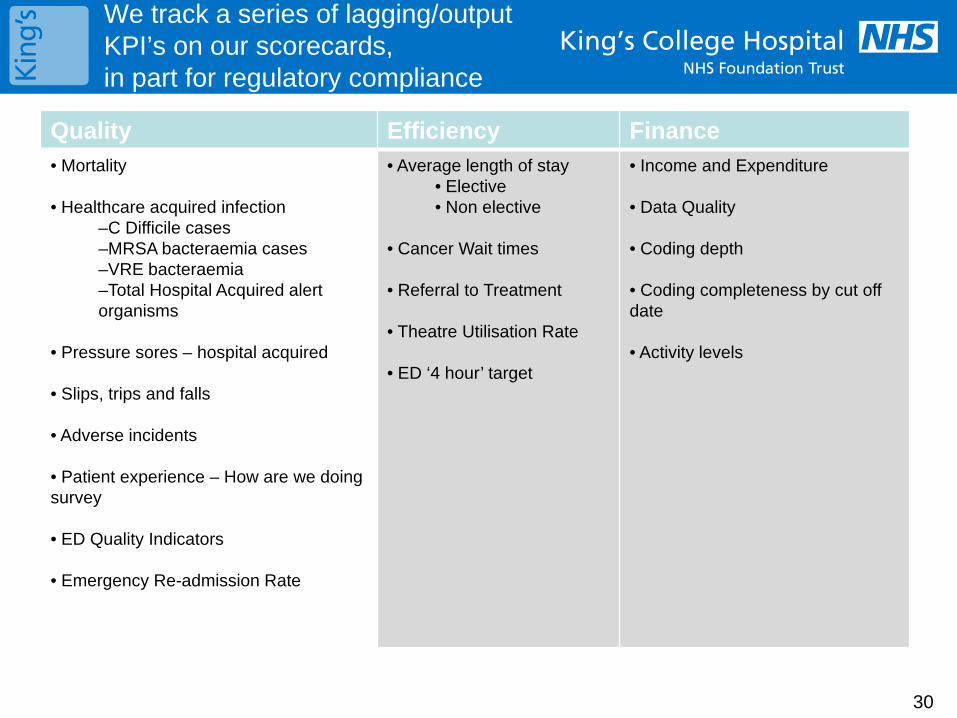
30
We track a series of lagging/output KPI’s on our scorecards, in part for regulatory compliance
Quality Efficiency Finance • Mortality
• Healthcare acquired infection –C Difficile cases –MRSA bacteraemia cases –VRE bacteraemia –Total Hospital Acquired alert organisms
• Pressure sores – hospital acquired
• Slips, trips and falls
• Adverse incidents
• Patient experience – How are we doing survey
• ED Quality Indicators
• Emergency Re-admission Rate
• Average length of stay • Elective • Non elective
• Cancer Wait times
• Referral to Treatment
• Theatre Utilisation Rate
• ED ‘4 hour’ target
• Income and Expenditure • Data Quality
• Coding depth
• Coding completeness by cut off date
• Activity levels
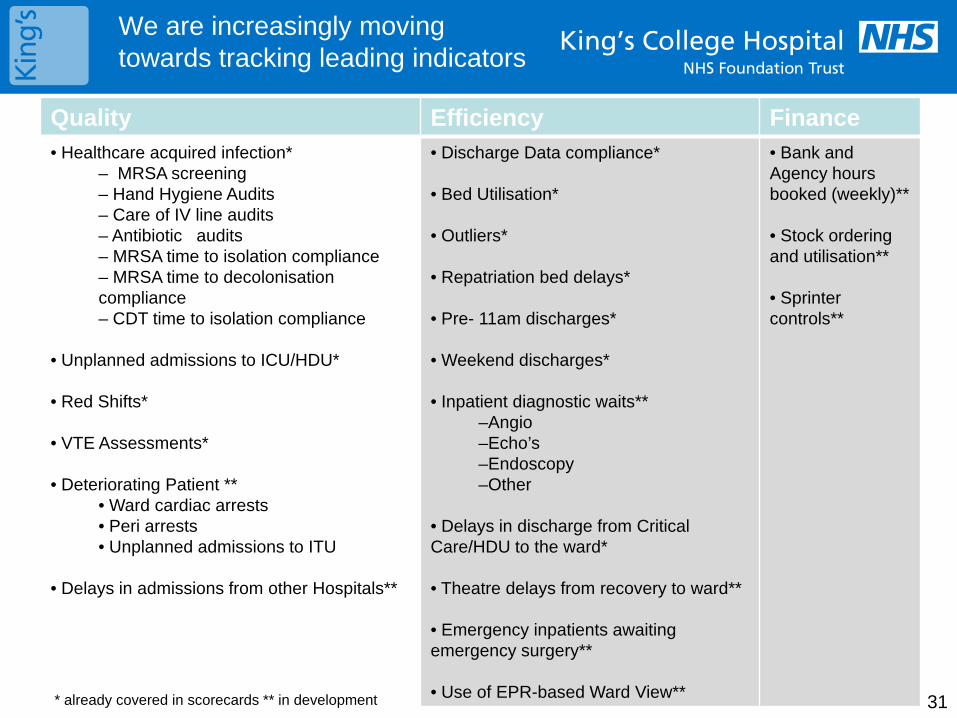
Quality Efficiency Finance • Healthcare acquired infection*
– MRSA screening – Hand Hygiene Audits – Care of IV line audits – Antibiotic audits – MRSA time to isolation compliance – MRSA time to decolonisation compliance – CDT time to isolation compliance
• Unplanned admissions to ICU/HDU*
• Red Shifts*
• VTE Assessments*
• Deteriorating Patient ** • Ward cardiac arrests • Peri arrests • Unplanned admissions to ITU
• Delays in admissions from other Hospitals**
• Discharge Data compliance*
• Bed Utilisation*
• Outliers*
• Repatriation bed delays*
• Pre- 11am discharges*
• Weekend discharges*
• Inpatient diagnostic waits** –Angio –Echo’s –Endoscopy –Other
• Delays in discharge from Critical Care/HDU to the ward*
• Theatre delays from recovery to ward**
• Emergency inpatients awaiting emergency surgery**
• Use of EPR-based Ward View**
• Bank and Agency hours booked (weekly)**
• Stock ordering and utilisation**
• Sprinter controls**
We are increasingly moving towards tracking leading indicators
* already covered in scorecards ** in development 31
2012-13 Operating Framework
Key Performance Highlights (1/3)
32
Context The Operating Framework was published on 24 November 2011 and outlines the business and planning arrangements for the NHS, and describes the national priorities for 2012/13. This report summarises some of the key performance and contractual areas against which the Trust will be measured next year.
Summary Hospital Mortality Indicator (SHMI)
• Published quarterly for a rolling 12-months on NHS Information Centre and NHS Choices website
• All Trusts to scrutinise and understand their data and performance, and take appropriate action.
Cancer
• All four of the 31 day standards and all 3 three of the 62 day standards to continue to be required.
Emergency readmissions
• Commissioners need not reimburse providers for admissions within 30 days of discharge following an elective admission
• Locally agreed thresholds to be put in place for other readmissions
• Kings is one of 5 Trusts taking part in a study and review of emergency readmissions in associated with the FT Network and Department of Health
Accident & Emergency
• A&E clinical indicators to remain in place for 2012-13, and this information to be published to the general public to access
• National performance to be assessed based on the operational standard of 95% of patients seen within 4 hours
2012-13 Operating Framework
Key Performance Highlights (2/3)
33
Access to services
• 18 week RTT standards for 90% admitted and 95% non-admitted completed waits to be achieved at specialty and Trust level – and monitored monthly. Specialties giving our biggest challenge include:
General Surgery
Urology
Trauma & Orthopaedics
Ophthalmology
Neurosurgery
Gynaecology
• 92% of patients on an incomplete pathway should be waiting no more than 18 weeks (Oct-11 = 96.7%)
• Less than 1% of patients should wait longer than 6 weeks for a diagnostic test (Nov-11 position = 1.6%)
• All planned waiting list for all specialties and diagnostic services to be reviewed by the end of December 2011, to ensure that it is clinically appropriate for the patient to wait for the specified time.
Eliminating Mixed Sex accommodation
• Breaches will continue to attract contract sanctions through the NHS Contract
Healthcare associated infections (HCAIs)
• Commissioners and providers to agree plans for reducing MRSA and C-diff infections in line with national objectives
2012-13 Operating Framework
Key Performance Highlights (3/3)
34
Information Strategy
• There will be punitive contract sanctions for any organisation not compliant with NHS number usage requirements by 31 March 2013.
Finance & Business Rules
• The tariff price adjuster will be a reduction of at least 1.5%, and this will also be applied to non-tariff services
• CQUIN will be increased from 1.5% to 2.5% of actual outturn value
2 national goals on VTE and responsiveness to personal needs to patients will continue to be in place
3rd national goal on improving diagnosis of dementia in hospitals
4th national goal to incentivise use of the NHS Safety Thermometer (pressure ulcers, urine infection in patients with catheters and falls)
Next Steps
• To include an internal SHMI mortality indicator on internal performance scorecards, as soon as the indicator is available to be reported on via CHKS, our benchmarking performance data provider.
• Feedback key findings from the FT Networked-initiated review of emergency readmission pathways, with a view to informing the Payment by Results guidance for excluding valid readmission pathways from contractual non-payment mechanisms in 2012-13.
• Divisions to review all patients on the Planned waiting list to ensure that it is clinically appropriate for the patient to be waiting for the specified period, as opposed to waiting on the active waiting list by end-December 2011. The Trust is required to feedback to commissioners to confirm that this review has taken place.
• Delivery plans required to ensure 90% admitted 18-week compliance achieved prior to April 2012.
Dr Foster Good Hospital Guide
2010-11 Key Highlights (1/2)
35
• The Dr Foster Good Hospital Guide for 2010-11 was published on 28 November 2011.
• This is the tenth publication of the guide which is published for consumption by patients, clinicians, NHS managers and NHS organisations
• Information is drawn from national data submissions and a survey questionnaire that is completed by Trusts ahead of publication
• Trusts are assessed across a number of key themes including:
Mortality
Broken hip repair
Stroke and Vascular services
Orthopaedics
Urology
Cardiac
Key Outcomes: Mortality Indicators
• Kings was listed as one of 21 Trusts with low reported mortality rates across a number of indicators including the Hospital Standardised Mortality Ratio (HSMR), but was also specifically mentioned for its low number of deaths in low-risk conditions.
• The Trust’s performance against the “Deaths after Surgery” indicator was higher than expected (index=100) at 106.08 which is being investigated further for outlying areas.
Dr Foster Good Hospital Guide
2010-11 Key Highlights (2/2)
36
Palliative Care Coding
• King’s was also listed as one of 10 Trust’s, including Guys & St Thomas’ Trust who have over a quarter of their in-hospital deaths recorded as palliative care.
• The Palliative Care Team have audited coding data and are satisfied that the clinical coding is of high quality, and reflects the busy, high profile palliative care service that is provided at the Trust.
• There has been a drive to improve the coding palliative care which is an additional factor in showing Kings as a potential outlier.
Hip & Knee Average Length of Stay (ALOS)
• Hip and Knee replacement ALOS indicators were red-rated at over 179 and 173 respectively, compared to the expected index value of 100.
• Kings was also one of 10 Trusts highlighted for not following at least 4 of the 7 steps within the rapid recovery pathway.
• Enhanced recovery processes are being implemented during 2011/12 for hip and knee replacement procedures, which is also a CQUIN scheme for this year. Based on an assessment on our current position, we would have shown reported compliance with the pathway steps
Next Steps • Deaths after surgery and Hip & Knee ALOS indicator performance are being investigated further based on locally-recorded data, in conjunction with the Clinical Effectiveness Team
• An update on any key issues identified will be presented to the Patient Outcomes Committee meeting in January 2012

Enc 2.6
Winter Resilience Plan Report to Board 20 December 2011 Page 1
Report to: Board of Directors
Date of meeting: 20th
December 2011
Subject: Winter Resilience Plan
Author(s): Liz Wells Head of Clinical Site Management and Emergency Planning Sue Field – Head of Capacity
Presented by: Roland Sinker
Sponsor: Roland Sinker
History:
Status: For information
1. Background/Purpose Winter resilience planning is required by the Department of Health and coordinated locally by NHS London. The Trust’s plan has been developed in liaison with local PCTs, acute trusts and other partners. The Trust’s strategic intention is to maintain business as usual for as long as possible while meeting the needs of patients in the face of growing demand/reduced levels of staffing. The Winter Resilience Plan (the Plan) sets out procedures for managing patient and Trust services during the winter and addresses particular scenarios such as extreme weather conditions and increased levels of attendance that occur during cold and/or icy conditions. The Plan includes assuring supplies and adequate internal services. It incorporates all relevant hospital areas and links into other agencies in the local health economy. The key objectives of the Plan are laid out in Appendix 1 2. Key implications for the Board The Plan enables the Trust to demonstrate Compliance with legislation as a Category 1 responder and healthcare provider. It aims to minimise the effects of winter issues, maintaining performance in terms of service provision and quality, and key performance indicators such as emergency care targets, 23 weeks and cancer pathways. Should the Trust not meet these aims there may be a reduction in the quality of care provided by the Trust, a financial loss due to loss or cancellation of services and also failure to meet key performance targets with a knock on effect on Monitor compliance and the CQC Quality and Risk Profile and hence on the Trust’s reputation. In addition, compliance and performance failures may trigger penalties and hence further costs to the Trust. 3. Preparation of the plan The plan for dealing with emergency admissions during the winter of 2011/2012 is based on our experience of the past few years, where demand for emergency treatment and admissions has risen steadily. Activity over the summer of 2011 is comparable to that experienced across the winters of 2008 and 2009, particularly the high levels of demand
Enc 2.6
Winter Resilience Plan Report to Board 20 December 2011 Page 2
experienced at weekends and Mondays. The high level of demand for emergency treatment and admission remains a significant risk and expense. It is further influenced by the valuable advice obtained from the Emergency Care Intensive Support Team (ECIST) visits to South East London over the past year and the work of the Emergency Care Network (ECN). Kings College Hospital (KCH) has introduced a significant number of changes to the emergency patient pathway over the past year through the Transformation programme and we are confident that we have a robust plan in place for the coming winter. However there is much that remains to be done in the wider health community to deliver the system wide improvements which will reduce demand and improve discharge in the medium to long term. Consequently this plan has been prepared on the assumption that we will have to cope with a significant increase in demand over the next few months and that the system wide reforms will not significantly change the demand for emergency care at KCH nor will they improve the external discharge processes in time to help with the coming winter. The winter capacity plan is key to the delivery of winter resilience (Appendix 3). The plan provides divisional requirements to deliver capacity against the expected increased emergency activity whilst minimising the disruption of elective/cancer activity, to support all of the Trusts access targets. Additional costs are factored in to the plan, but will be covered by income for sustaining elective activity through the winter months. Leading indicators have also been derived to enable us to track performance against this plan. The winter capacity plan is reviewed at a weekly emergency performance meeting, chaired by Peter Fry/Sue Bowler. The weekly meeting supports the already established monthly emergency care board and is attended by multi-disciplinary teams from all divisions. Any plans that are not on trajectory to deliver will be escalated to the Director of Operations, where remedial actions will be discussed and introduced. 4. Scope of Plan The Plan will apply without exception to all individuals within the Trust who are involved in providing inpatient services to patients. Key personnel who have responsibility in the Plan are listed at Appendix 2. The Plan covers the six key work streams: 1. Winter Capacity Action Plan ( Appendix 3) 2. Annual leave planning – all departments with the aim to increase elective activity and decrease
bank and agency staffing costs. 3. Emergency Care plans – e.g. additional resuscitation bays, Meet and Greet initiative, weekly
emergency care meeting 4. Access for patients – changes in bed configuration and use e.g. Acute Assessment Unit, Acute
Medical and Surgical wards 5. Current year plans in progress – Transformation projects 6. Pandemic/seasonal flu and staff vaccination plans 7. Infection control in the use of isolation and cohorting in the event of an outbreak Finally, the plan addresses the identified risks laid out below: 1. Excess bed Pressures; 2. Pandemic Flu; 3. Diagnostic delays and Support Services delays; 4. Transport delays; 5. Social services delays;
Enc 2.6
Winter Resilience Plan Report to Board 20 December 2011 Page 3
6. Delayed discharge; 7. Single sex requirement breaches; and 8. Mental health assessment delays. Please see Appendix 4 for more detail.
Recommendations
The board is asked to note the plan.
Winter Resilience Plan Report to Board 20 December 2011 Page 4
Appendix 1 Key Objectives of the Winter Resilience Plan 1. To ensure quality of care is not compromised over the winter period, by eliminating
avoidable trolley waits and waits in the ED department. 2. To ensure KCH has plans in place to cope with the predicted level of emergency
admissions over the winter months, which are predominately during the first 3 weeks in January.
3. To support front line staff in light of predicted emergencies. 4. To ensure that all staff and services are prepared and understand their roles and
responsibilities. 5. To have clear escalation plans and processes to deal with peaks in demand. 6. Ensure an efficient discharge process is in place at all times to prevent bed blocking. 7. Ensure KCH meets the 5 clinical quality indicators in light of predicted rising attendances
over the winter months 8. Minimise the disruption to Elective activity 9. Ensure KCH can meet the current performance targets over the winter period e.g. 23
weeks, cancer waits. Appendix 2 Key personnel • Director of Operations. • Divisional Managers. • Clinical Site Management Team. • Assistant Director of Performance and Contracts • Bed Managers/Patient flow co-ordinators • Medical Staff • Nursing Staff • ED Staff • Discharge Co-ordinators • Hospital Discharge Team (Lambeth and Southwark) • Heads of Nursing • Facilities – housekeeping, porters and linen.
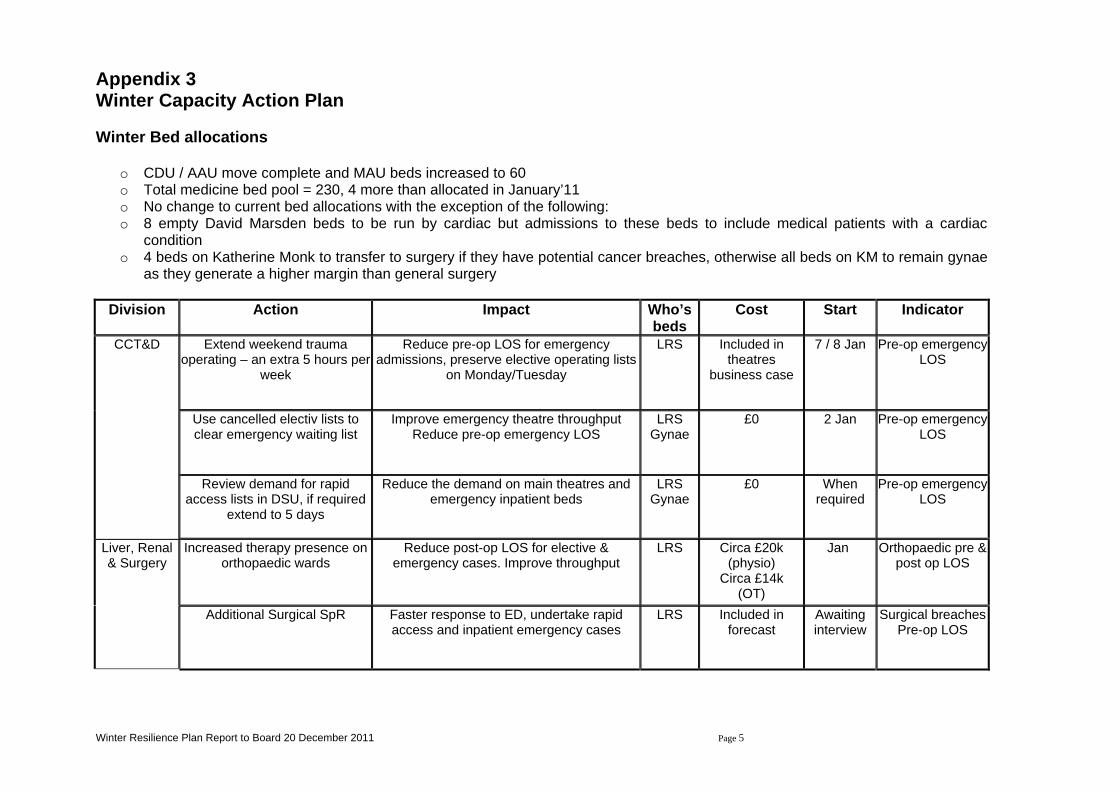
Winter Resilience Plan Report to Board 20 December 2011 Page 5
Appendix 3 Winter Capacity Action Plan Winter Bed allocations
o CDU / AAU move complete and MAU beds increased to 60 o Total medicine bed pool = 230, 4 more than allocated in January’11 o No change to current bed allocations with the exception of the following: o 8 empty David Marsden beds to be run by cardiac but admissions to these beds to include medical patients with a cardiac
condition o 4 beds on Katherine Monk to transfer to surgery if they have potential cancer breaches, otherwise all beds on KM to remain gynae
as they generate a higher margin than general surgery
Division Action Impact Who’s beds
Cost Start Indicator
CCT&D Extend weekend trauma operating – an extra 5 hours per
week
Reduce pre-op LOS for emergency admissions, preserve elective operating lists
on Monday/Tuesday
LRS Included in theatres
business case
7 / 8 Jan Pre-op emergency LOS
Use cancelled electiv lists to clear emergency waiting list
Improve emergency theatre throughput Reduce pre-op emergency LOS
LRS Gynae
£0 2 Jan Pre-op emergency LOS
Review demand for rapid access lists in DSU, if required
extend to 5 days
Reduce the demand on main theatres and emergency inpatient beds
LRS Gynae
£0 When required
Pre-op emergency LOS
Liver, Renal & Surgery
Increased therapy presence on orthopaedic wards
Reduce post-op LOS for elective & emergency cases. Improve throughput
LRS Circa £20k (physio)
Circa £14k (OT)
Jan Orthopaedic pre & post op LOS
Additional Surgical SpR Faster response to ED, undertake rapid access and inpatient emergency cases
LRS Included in forecast
Awaiting interview
Surgical breaches Pre-op LOS
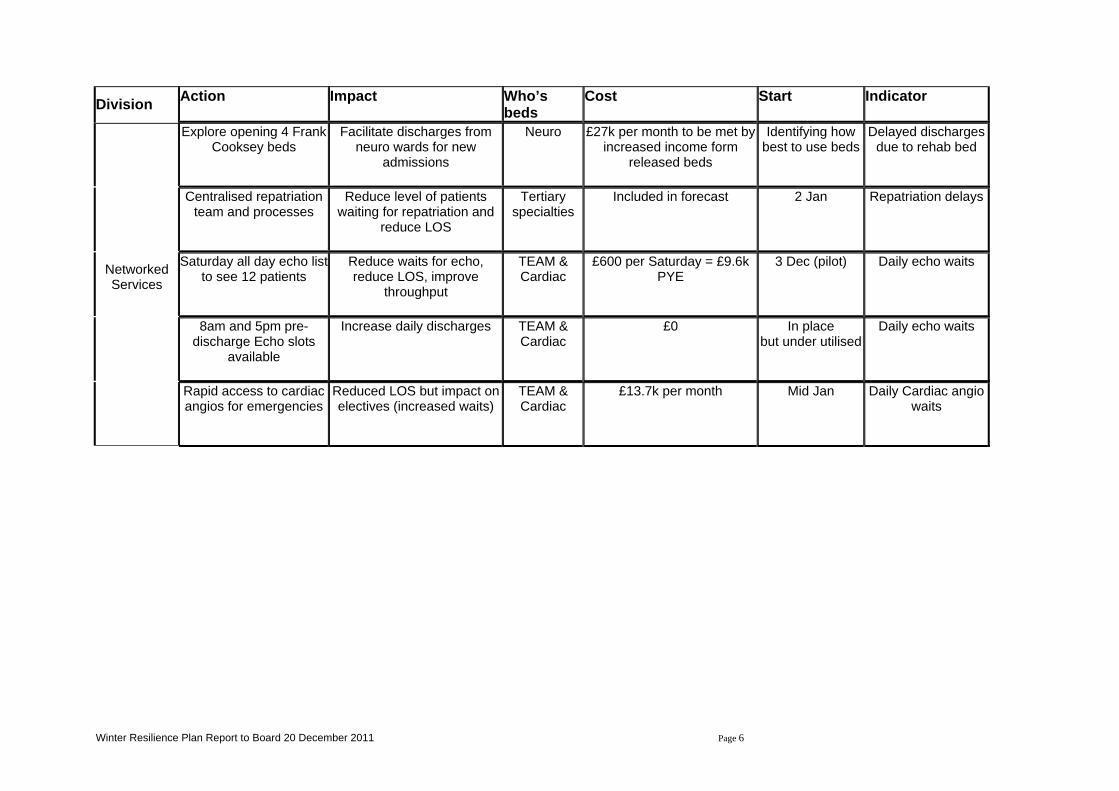
Winter Resilience Plan Report to Board 20 December 2011 Page 6
Division Action Impact Who’s beds
Cost Start Indicator
Networked Services
Explore opening 4 Frank Cooksey beds
Facilitate discharges from neuro wards for new
admissions
Neuro £27k per month to be met by increased income form
released beds
Identifying how best to use beds
Delayed discharges due to rehab bed
Centralised repatriation team and processes
Reduce level of patients waiting for repatriation and
reduce LOS
Tertiary specialties
Included in forecast 2 Jan Repatriation delays
Saturday all day echo list to see 12 patients
Reduce waits for echo, reduce LOS, improve
throughput
TEAM & Cardiac
£600 per Saturday = £9.6k PYE
3 Dec (pilot) Daily echo waits
8am and 5pm pre-discharge Echo slots
available
Increase daily discharges TEAM & Cardiac
£0 In place but under utilised
Daily echo waits
Rapid access to cardiac angios for emergencies
Reduced LOS but impact on electives (increased waits)
TEAM & Cardiac
£13.7k per month Mid Jan Daily Cardiac angio waits
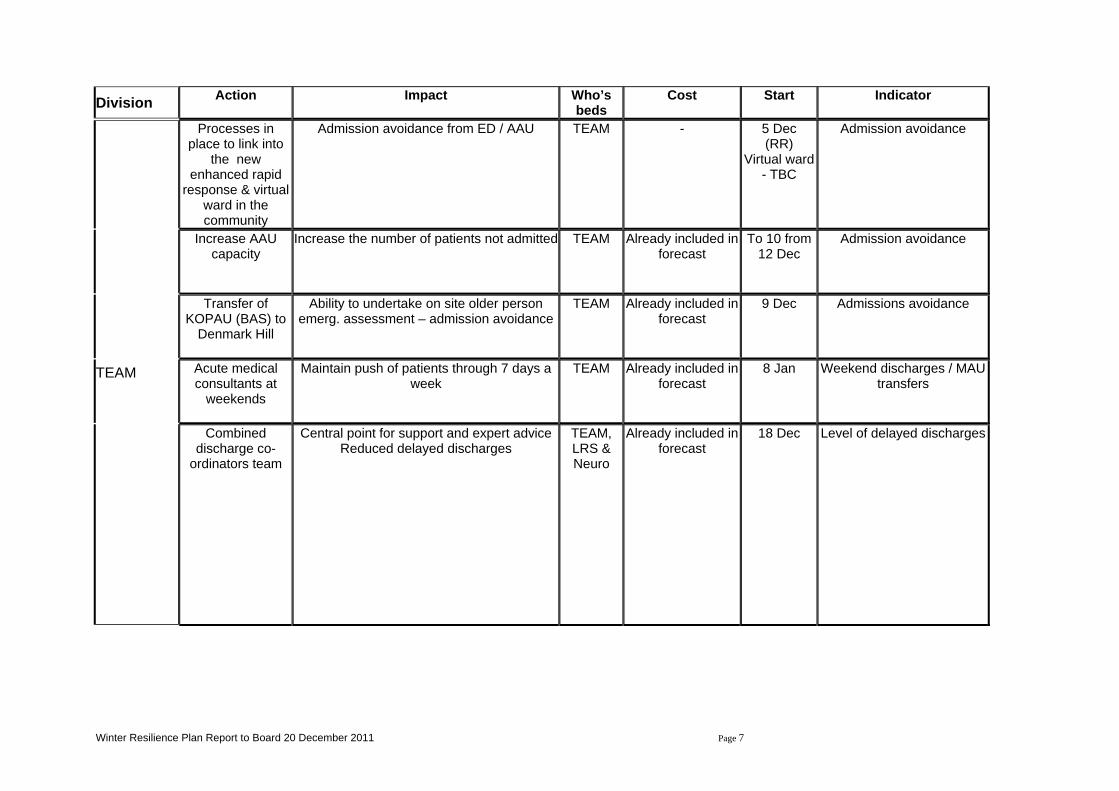
Winter Resilience Plan Report to Board 20 December 2011 Page 7
Division Action Impact Who’s
beds Cost Start Indicator
TEAM
Processes in place to link into
the new enhanced rapid
response & virtual ward in the community
Admission avoidance from ED / AAU TEAM - 5 Dec (RR)
Virtual ward - TBC
Admission avoidance
Increase AAU capacity
Increase the number of patients not admitted TEAM Already included in forecast
To 10 from 12 Dec
Admission avoidance
Transfer of KOPAU (BAS) to
Denmark Hill
Ability to undertake on site older person emerg. assessment – admission avoidance
TEAM Already included in forecast
9 Dec Admissions avoidance
Acute medical consultants at
weekends
Maintain push of patients through 7 days a week
TEAM Already included in forecast
8 Jan Weekend discharges / MAU transfers
Combined discharge co-
ordinators team
Central point for support and expert advice Reduced delayed discharges
TEAM, LRS & Neuro
Already included in forecast
18 Dec Level of delayed discharges
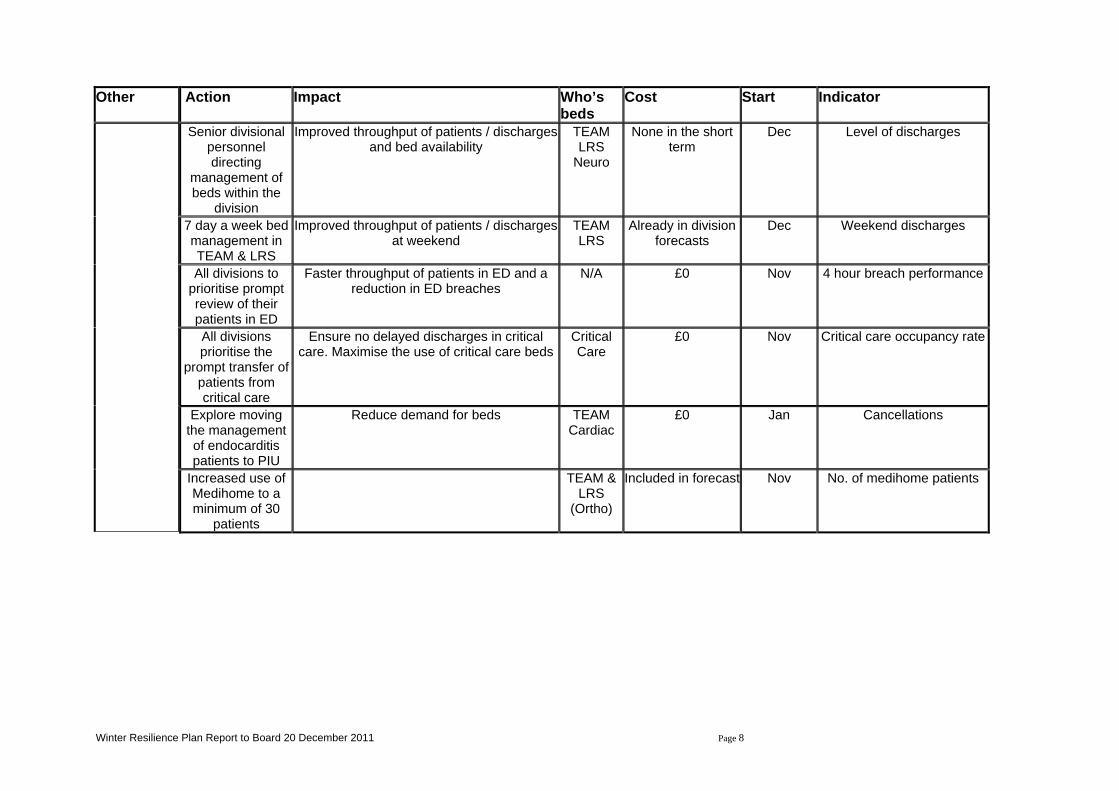
Winter Resilience Plan Report to Board 20 December 2011 Page 8
Other Action Impact Who’s
beds Cost Start Indicator
Senior divisional personnel directing
management of beds within the
division
Improved throughput of patients / discharges and bed availability
TEAM LRS
Neuro
None in the short term
Dec Level of discharges
7 day a week bed management in TEAM & LRS
Improved throughput of patients / discharges at weekend
TEAM LRS
Already in division forecasts
Dec Weekend discharges
All divisions to prioritise prompt review of their patients in ED
Faster throughput of patients in ED and a reduction in ED breaches
N/A £0 Nov 4 hour breach performance
All divisions prioritise the
prompt transfer of patients from critical care
Ensure no delayed discharges in critical care. Maximise the use of critical care beds
Critical Care
£0 Nov Critical care occupancy rate
Explore moving the management of endocarditis patients to PIU
Reduce demand for beds TEAM Cardiac
£0 Jan Cancellations
Increased use of Medihome to a minimum of 30
patients
TEAM & LRS
(Ortho)
Included in forecast Nov No. of medihome patients
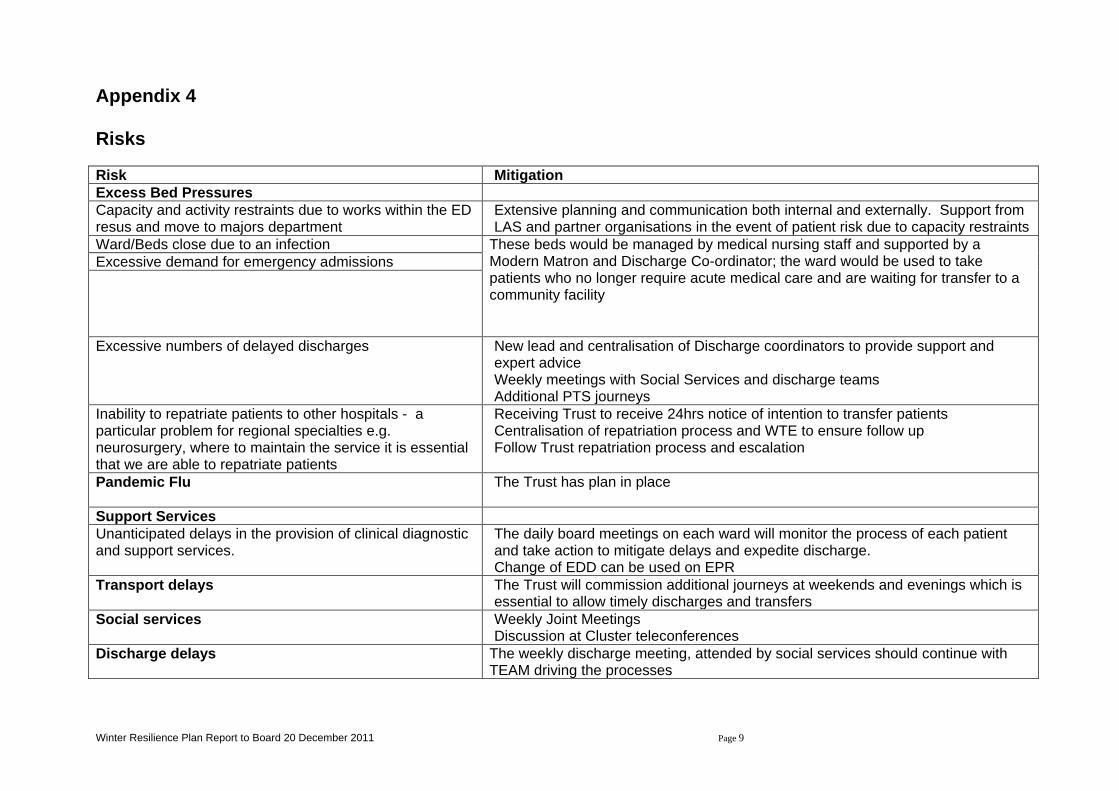
Winter Resilience Plan Report to Board 20 December 2011 Page 9
Appendix 4 Risks Risk Mitigation Excess Bed Pressures Capacity and activity restraints due to works within the ED resus and move to majors department
Extensive planning and communication both internal and externally. Support from LAS and partner organisations in the event of patient risk due to capacity restraints
Ward/Beds close due to an infection These beds would be managed by medical nursing staff and supported by a Modern Matron and Discharge Co-ordinator; the ward would be used to take patients who no longer require acute medical care and are waiting for transfer to a community facility
Excessive demand for emergency admissions
Excessive numbers of delayed discharges New lead and centralisation of Discharge coordinators to provide support and expert advice Weekly meetings with Social Services and discharge teams Additional PTS journeys
Inability to repatriate patients to other hospitals - a particular problem for regional specialties e.g. neurosurgery, where to maintain the service it is essential that we are able to repatriate patients
Receiving Trust to receive 24hrs notice of intention to transfer patients Centralisation of repatriation process and WTE to ensure follow up Follow Trust repatriation process and escalation
Pandemic Flu The Trust has plan in place
Support Services Unanticipated delays in the provision of clinical diagnostic and support services.
The daily board meetings on each ward will monitor the process of each patient and take action to mitigate delays and expedite discharge. Change of EDD can be used on EPR
Transport delays The Trust will commission additional journeys at weekends and evenings which is essential to allow timely discharges and transfers
Social services Weekly Joint Meetings Discussion at Cluster teleconferences
Discharge delays The weekly discharge meeting, attended by social services should continue with TEAM driving the processes
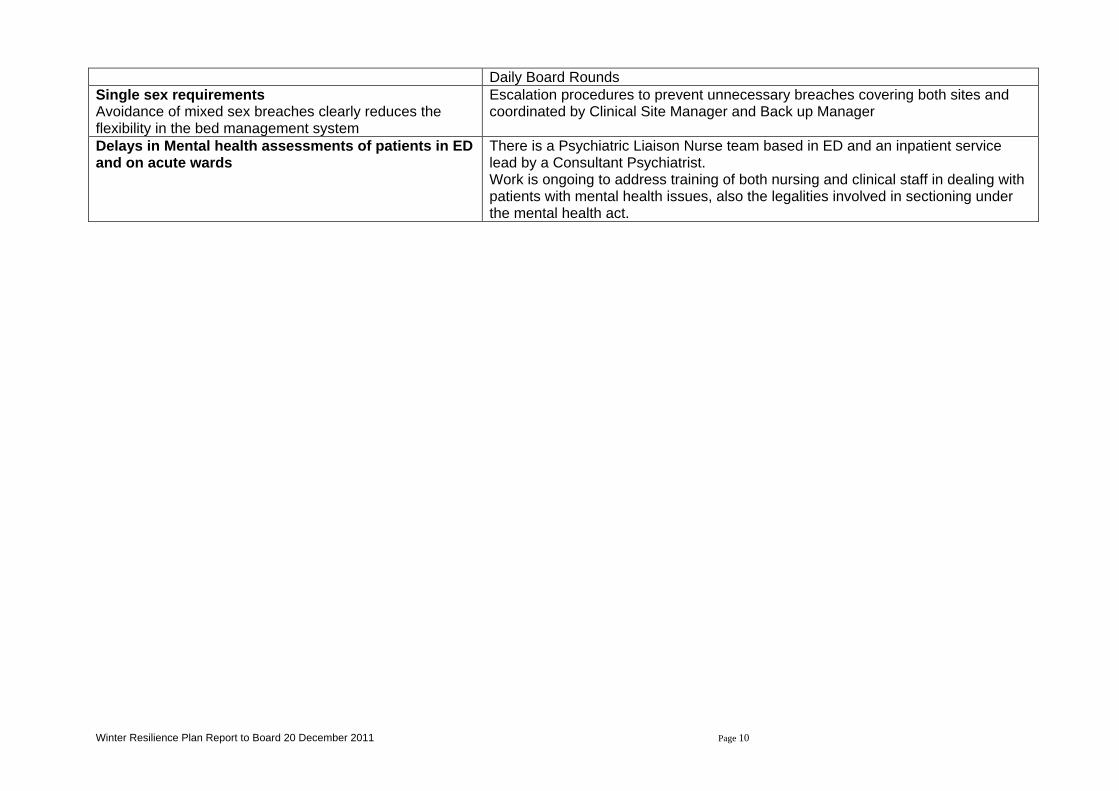
Winter Resilience Plan Report to Board 20 December 2011 Page 10
Daily Board Rounds Single sex requirements Avoidance of mixed sex breaches clearly reduces the flexibility in the bed management system
Escalation procedures to prevent unnecessary breaches covering both sites and coordinated by Clinical Site Manager and Back up Manager
Delays in Mental health assessments of patients in ED and on acute wards
There is a Psychiatric Liaison Nurse team based in ED and an inpatient service lead by a Consultant Psychiatrist. Work is ongoing to address training of both nursing and clinical staff in dealing with patients with mental health issues, also the legalities involved in sectioning under the mental health act.
1
Jane Walters, Director of Corporate Affairs Board of Directors, December 2011
King’s Patient Experience Report
November 2011
Enc. 2.7.1
2
Patient Experience Report
• Integrated monthly patient experience data to inform service improvement launched in December 2008
• Includes a scorecard format monthly overview of: – Complaints – PALS – How are we doing inpatients, maternity and day surgery – Commissioning for Quality and Innovation (CQUIN) patient experience
scores
– Eliminating Mixed Sex Accommodation patient experience • Reports data at Trust, Division, ward and specialty level for
inpatients and outpatients • Near real-time reporting ten working days after the end of
the month • Supports King’s Quality Strategy, CQUIN and EMSA
monitoring
3
Complaints and PALS
• Complaints fell slightly this month to 64 but the trend since July is up • PALS activity also dropped • Complaint response times fell to 55% within target for the last rolling quarter, the lowest
score since April
How are we doing?
• Day Surgery: Satisfaction remains high at 92 overall • Maternity: overall score for Maternity improved three points to 85 • Inpatients:
• Overall score rose one point to 85, one point below the benchmark • Environment rose to 78, one point below target • Improved cleaning scores were maintained this month and, after a dip in October, food gained four
points to exceed the benchmark • Patient Engagement recovered to meet the benchmark of 87 with only ‘involving patients in
decisions about their care and treatment’ remaining in the red for the third month in a row • Care Perceptions gained one point to bring the overall score back to amber. Although 12 out of
17 indicators are green or amber, there are still key areas in the red including,noise at night from staff, discharge delays and information given to patients on discharge
• Scores for the two new questions on hand washing and care at night remained on amber
Key results for October 2011
4
• This month Divisional performance improved with Cardiac, Child Health Liver, Neurosciences and Women’s hitting the benchmark, with Haematology and Private Patients achieving an amber rating
• Cardiac received its highest rating this year with an overall score of 89 • The response rate was a disappointing 44%, 6 points below target. Only Liver,
TEAM and Haematology achieved 50% or more with response rates for Neurosciences (31%), Renal (17%) and Women’s (32%) being particularly low
• The ratio of positive comments rose to 66%
CQUIN • Mixed performance continues, with only “Privacy when discussing treatment”
hitting the benchmark.
Single Sex Accommodation (EMSA) • Both EMSA question scores improved and hit the benchmark
Key results for September 2011
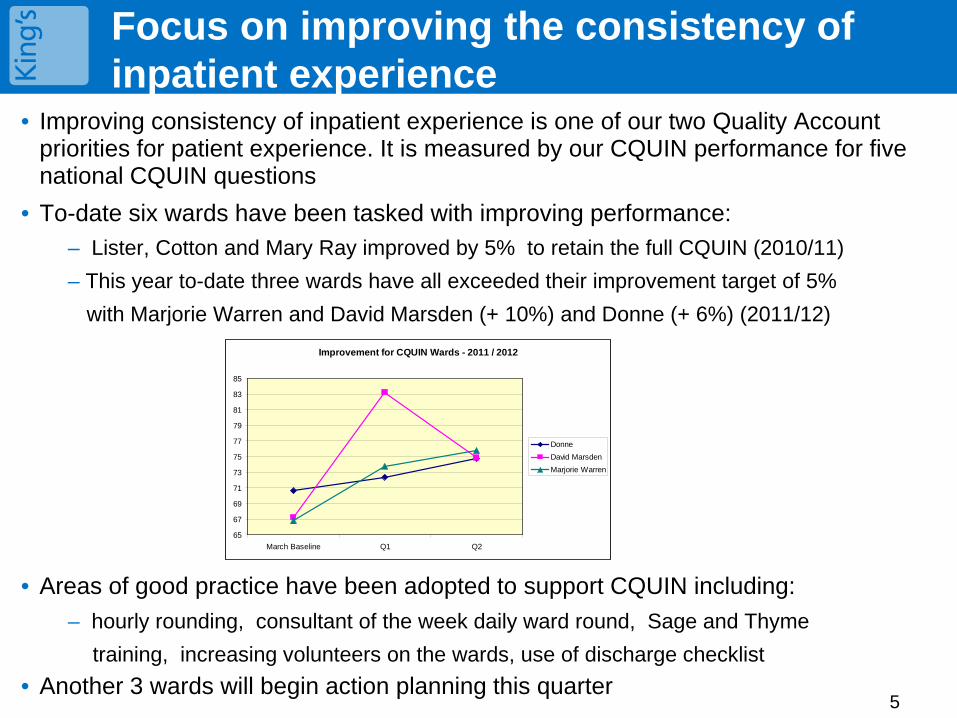
5
• Improving consistency of inpatient experience is one of our two Quality Account priorities for patient experience. It is measured by our CQUIN performance for five national CQUIN questions
• To-date six wards have been tasked with improving performance: – Lister, Cotton and Mary Ray improved by 5% to retain the full CQUIN (2010/11) – This year to-date three wards have all exceeded their improvement target of 5% with Marjorie Warren and David Marsden (+ 10%) and Donne (+ 6%) (2011/12)
• Areas of good practice have been adopted to support CQUIN including: – hourly rounding, consultant of the week daily ward round, Sage and Thyme training, increasing volunteers on the wards, use of discharge checklist
• Another 3 wards will begin action planning this quarter
Focus on improving the consistency of inpatient experience
Improvement for CQUIN Wards - 2011 / 2012
65
67
69
71
73
75
77
79
81
83
85
March Baseline Q1 Q2
DonneDavid MarsdenMarjorie Warren
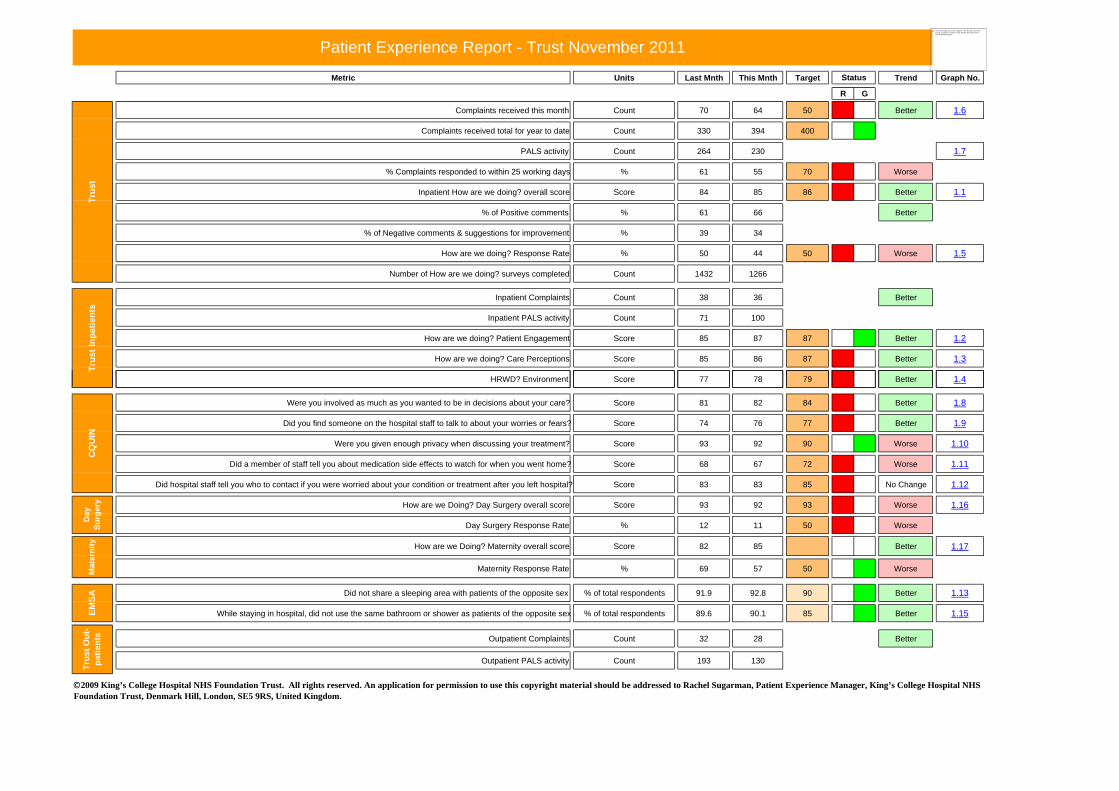
Metric Units Last Mnth This Mnth Target Trend Graph No.
R G
Complaints received this month Count 70 64 50 Better 1.6
Complaints received total for year to date Count 330 394 400
PALS activity Count 264 230 1.7
% Complaints responded to within 25 working days % 61 55 70 Worse
Inpatient How are we doing? overall score Score 84 85 86 Better 1.1
% of Positive comments % 61 66 Better
% of Negative comments & suggestions for improvement % 39 34
How are we doing? Response Rate % 50 44 50 Worse 1.5
Number of How are we doing? surveys completed Count 1432 1266
Inpatient Complaints Count 38 36 Better
Inpatient PALS activity Count 71 100
How are we doing? Patient Engagement Score 85 87 87 Better 1.2
How are we doing? Care Perceptions Score 85 86 87 Better 1.3
HRWD? Environment Score 77 78 79 Better 1.4
Patient Experience Report - Trust November 2011
Status
Trus
tTr
ust I
npat
ient
s
The linked image cannot be displayed. The file may have been moved, renamed, or deleted. Verify that the link points to the correct file and location.
Were you involved as much as you wanted to be in decisions about your care? Score 81 82 84 Better 1.8
Did you find someone on the hospital staff to talk to about your worries or fears? Score 74 76 77 Better 1.9
Were you given enough privacy when discussing your treatment? Score 93 92 90 Worse 1.10
Did a member of staff tell you about medication side effects to watch for when you went home? Score 68 67 72 Worse 1.11
Did hospital staff tell you who to contact if you were worried about your condition or treatment after you left hospital? Score 83 83 85 No Change 1.12
How are we Doing? Day Surgery overall score Score 93 92 93 Worse 1.16
Day Surgery Response Rate % 12 11 50 Worse
P
How are we Doing? Maternity overall score Score 82 85 Better 1.17
Maternity Response Rate % 69 57 50 Worse
P
Did not share a sleeping area with patients of the opposite sex % of total respondents 91.9 92.8 90 Better 1.13
While staying in hospital, did not use the same bathroom or shower as patients of the opposite sex % of total respondents 89.6 90.1 85 Better 1.15
Outpatient Complaints Count 32 28 Better
Outpatient PALS activity Count 193 130
CQ
UIN
Day
Su
rger
yM
ater
nity
2009 King’s College Hospital NHS Foundation Trust. All rights reserved. An application for permission to use this copyright material should be addressed to Rachel Sugarman, Patient Experience Manager, King’s College Hospital NHS Foundation Trust, Denmark Hill, London, SE5 9RS, United Kingdom.
EMSA
Trus
t Out
-pa
tient
s
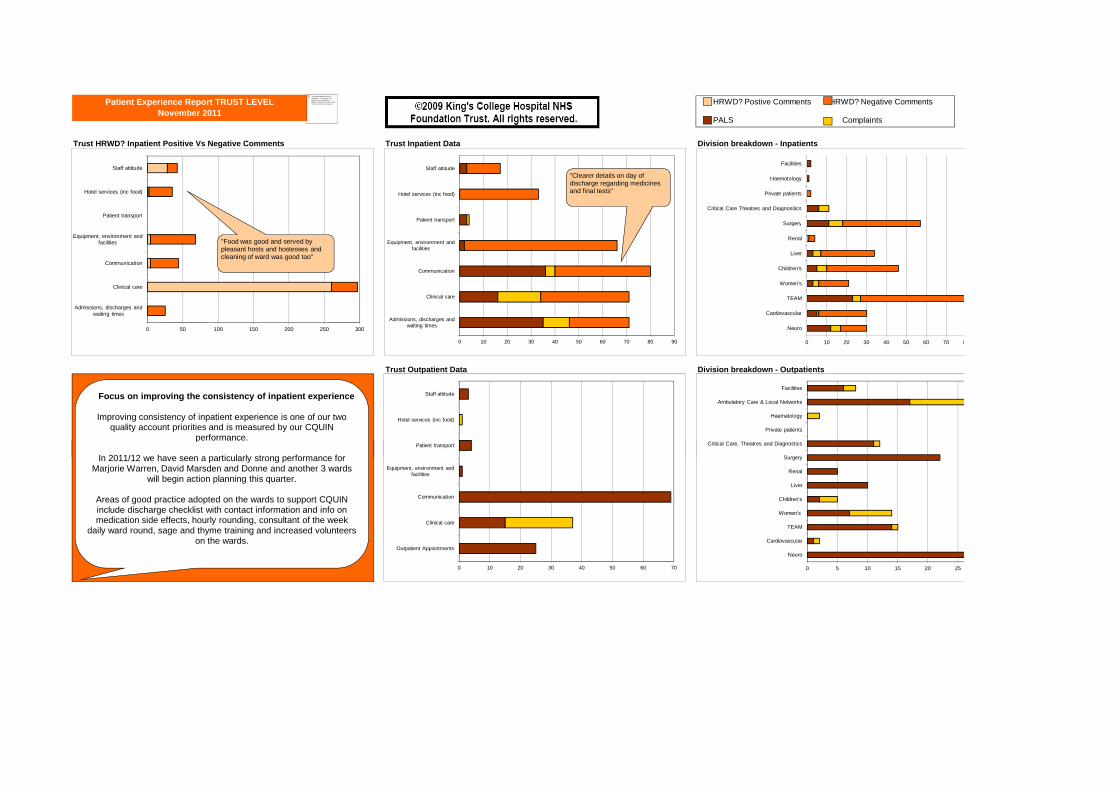
Trust HRWD? Inpatient Positive Vs Negative Comments Trust Inpatient Data Division breakdown - Inpatients
Trust Outpatient Data Division breakdown - Outpatients
Patient Experience Report TRUST LEVEL November 2011
0 10 20 30 40 50 60 70 80 90
Admissions, discharges and waiting times
Clinical care
Communication
Equipment, environment and facilities
Patient transport
Hotel services (inc food)
Staff attitude
Patient transport
Hotel services (inc food)
Staff attitude
0 10 20 30 40 50 60 70 8
Neuro
Cardiovascular
TEAM
Women's
Children's
Liver
Renal
Surgery
Critical Care Theatres and Diagnositics
Private patients
Haemotology
Facilities
Surgery
Critical Care, Theatres and Diagnostics
Private patients
Haematology
Ambulatory Care & Local Networks
Facilities
0 50 100 150 200 250 300
Admissions, discharges and waiting times
Clinical care
Communication
Equipment, environment and facilities
Patient transport
Hotel services (inc food)
Staff attitude
"Food was good and served by pleasant hosts and hostesses and cleaning of ward was good too"
"Clearer details on day of discharge regarding medicines and final tests"
HRWD? Postive Comments HRWD? Negative Comments
PALS Complaints
The linked image cannot be displayed. The file may have been moved, renamed, or deleted. Verify that the link points to the correct file and location.
Focus on improving the consistency of inpatient experience
Improving consistency of inpatient experience is one of our two quality account priorities and is measured by our CQUIN
performance.
In 2011/12 we have seen a particularly strong performance for
0 10 20 30 40 50 60 70
Outpatient Appointments
Clinical care
Communication
Equipment, environment and facilities
Patient transport
0 5 10 15 20 25
Neuro
Cardiovascular
TEAM
Women's
Children's
Liver
Renal
Surgery
Critical Care, Theatres and Diagnosticsperformance.
In 2011/12 we have seen a particularly strong performance for Marjorie Warren, David Marsden and Donne and another 3 wards
will begin action planning this quarter.
Areas of good practice adopted on the wards to support CQUIN include discharge checklist with contact information and info on medication side effects, hourly rounding, consultant of the week
daily ward round, sage and thyme training and increased volunteers on the wards.

83
84
85
86
87
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
How are we doing? Trust Overall
HRWD? Score Benchmark
1.1
84
85
86
87
88
89
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
How are we doing? Patient Engagement
HRWD? Score Benchmark
1.2
84
85
86
87
88
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
How are we doing? Care Perceptions
HRWD? Score Benchmark
1.3
7071727374757677787980
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
How are we doing? Environment
HRWD? Score Benchmark
1.4
Dec
-
Jan-
Feb-
Mar
-
Apr
-
May
-
Jun-
Jul-
Aug
-
Sep
-
Oct
-
Nov
-HRWD? Score Benchmark
Dec
-
Jan-
Feb-
Mar
-
Apr
-
May
-
Jun-
Jul-
Aug
-
Sep
-
Oct
-
Nov
-
HRWD? Score Benchmark
363840424446485052545658
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
How are we doing? Response Rates
Response Rate Benchmark
1.5
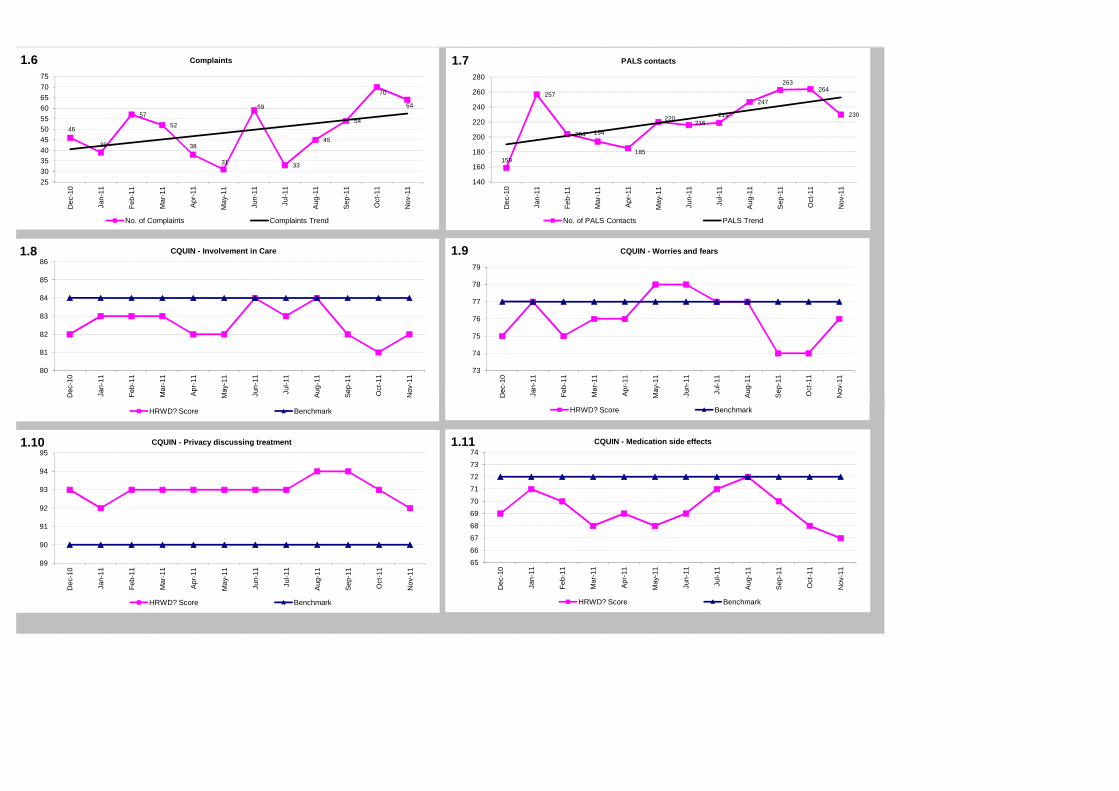
46
39
57
52
38
31
59
33
45
54
70
64
2530354045505560657075
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
Complaints
No. of Complaints Complaints Trend
1.6
159
257
204 194
185
220216
219
247
263264
230
140
160
180
200
220
240
260
280
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
PALS contacts
No. of PALS Contacts PALS Trend
1.7
80
81
82
83
84
85
86
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
CQUIN - Involvement in Care
HRWD? Score Benchmark
1.8
73
74
75
76
77
78
79
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
CQUIN - Worries and fears
HRWD? Score Benchmark
1.9
De Ja Fe Ma
Ap
Ma Ju J Au
Se O No
HRWD? Score Benchmark
De Ja Fe Ma
Ap
Ma Ju J Au
Se O No
HRWD? Score Benchmark
89
90
91
92
93
94
95
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
CQUIN - Privacy discussing treatment
HRWD? Score Benchmark
1.10
65
66
6768
69
70
7172
73
74
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
CQUIN - Medication side effects
HRWD? Score Benchmark
1.11
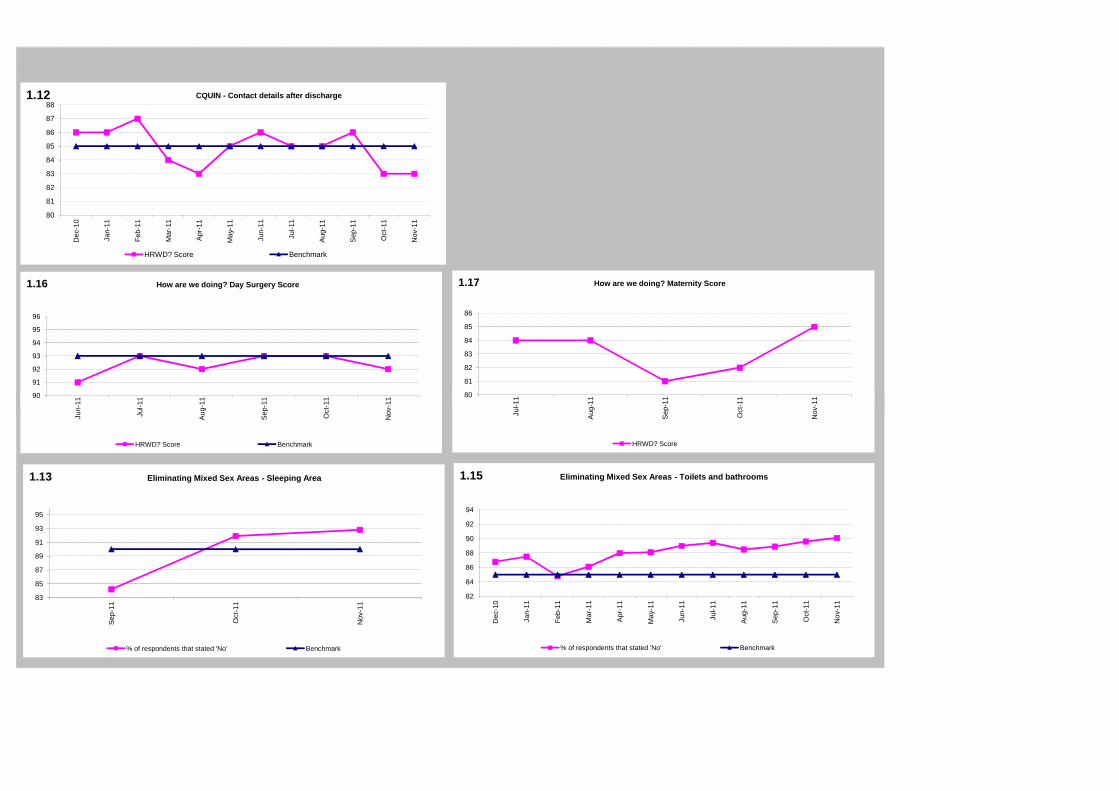
80
81
82
83
84
85
86
87
88
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
CQUIN - Contact details after discharge
HRWD? Score Benchmark
1.12
90
91
92
93
94
95
96
un-1
1
Jul-1
1
ug-1
1
ep-1
1
Oct
-11
ov-1
1
How are we doing? Day Surgery Score1.16
80
81
82
83
84
85
86
Jul-1
1
ug-1
1
ep-1
1
Oct
-11
ov-1
1
How are we doing? Maternity Score1.17
83
85
87
89
91
93
95
Sep
-11
Oct
-11
Nov
-11
Eliminating Mixed Sex Areas - Sleeping Area
% of respondents that stated 'No' Benchmark
1.13
82
84
86
88
90
92
94
Dec
-10
Jan-
11
Feb-
11
Mar
-11
Apr
-11
May
-11
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
Eliminating Mixed Sex Areas - Toilets and bathrooms
% of respondents that stated 'No' Benchmark
1.15
90
Jun-
11
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
HRWD? Score Benchmark
80
Jul-1
1
Aug
-11
Sep
-11
Oct
-11
Nov
-11
HRWD? Score
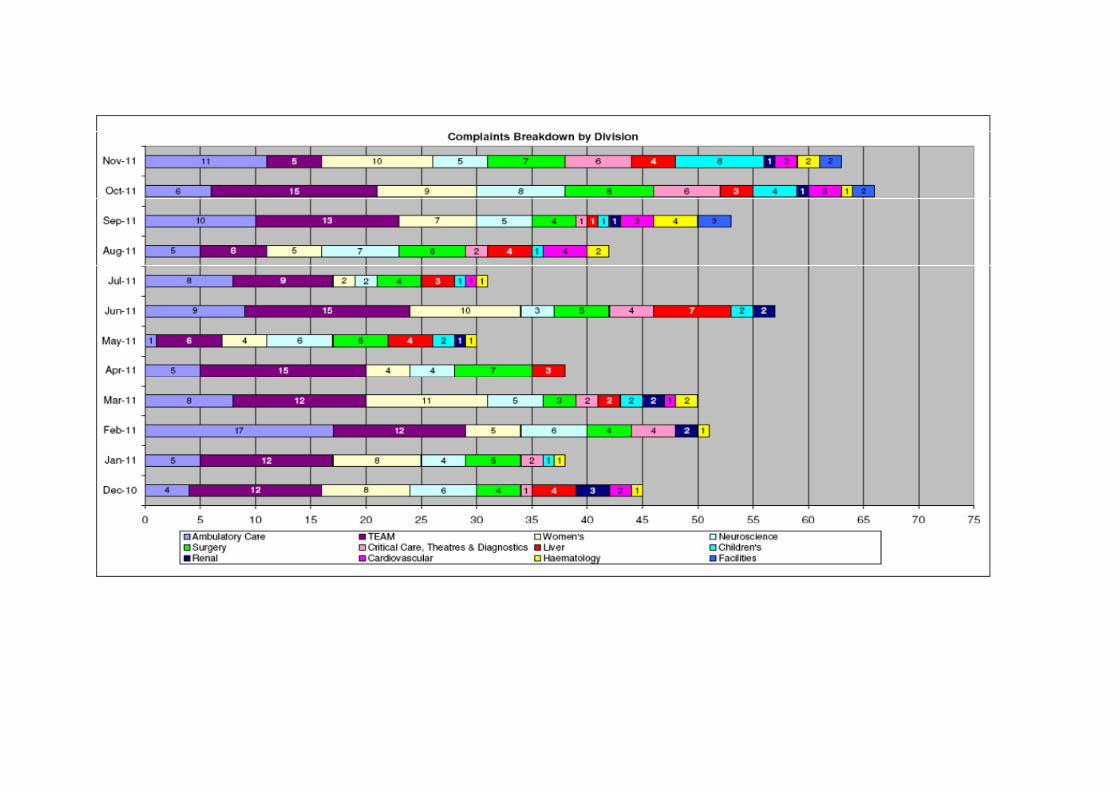
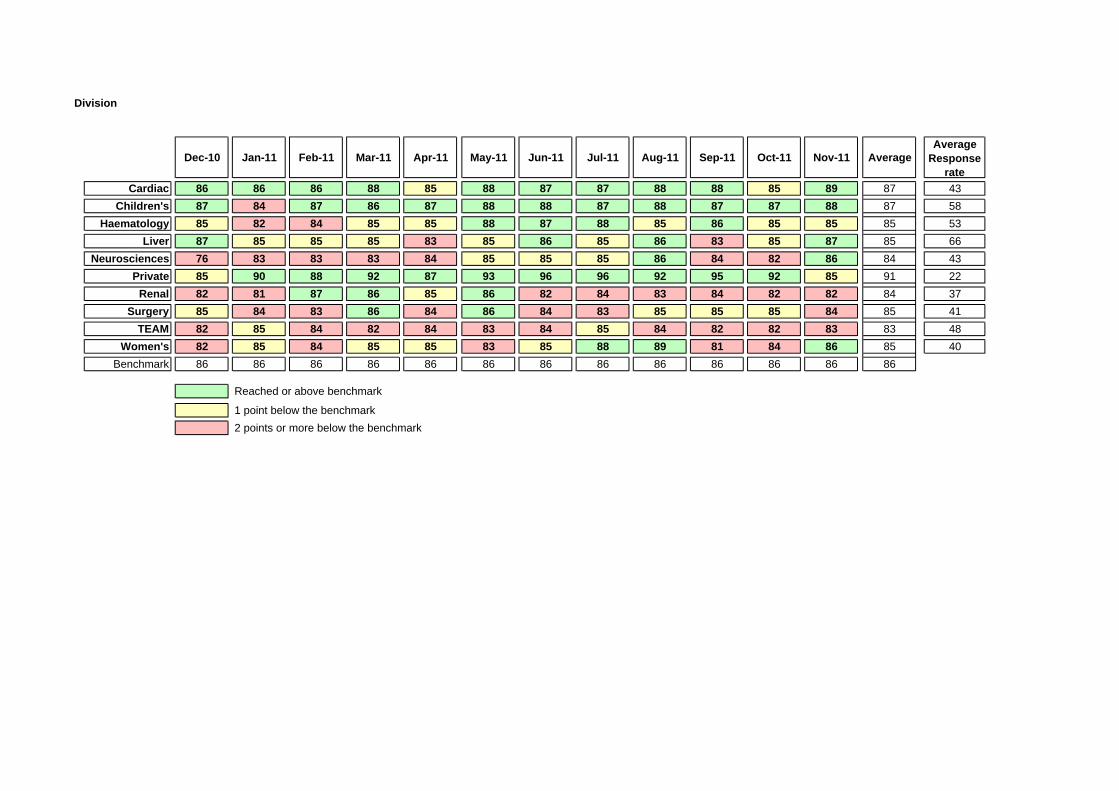
Division
Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 AverageAverage
Response rate
Cardiac 86 86 86 88 85 88 87 87 88 88 85 89 87 43Children's 87 84 87 86 87 88 88 87 88 87 87 88 87 58
Haematology 85 82 84 85 85 88 87 88 85 86 85 85 85 53Liver 87 85 85 85 83 85 86 85 86 83 85 87 85 66
Neurosciences 76 83 83 83 84 85 85 85 86 84 82 86 84 43Private 85 90 88 92 87 93 96 96 92 95 92 85 91 22
Renal 82 81 87 86 85 86 82 84 83 84 82 82 84 37Surgery 85 84 83 86 84 86 84 83 85 85 85 84 85 41
TEAM 82 85 84 82 84 83 84 85 84 82 82 83 83 48Women's 82 85 84 85 85 83 85 88 89 81 84 86 85 40
Benchmark 86 86 86 86 86 86 86 86 86 86 86 86 86
Reached or above benchmark
1 point below the benchmark2 points or more below the benchmark


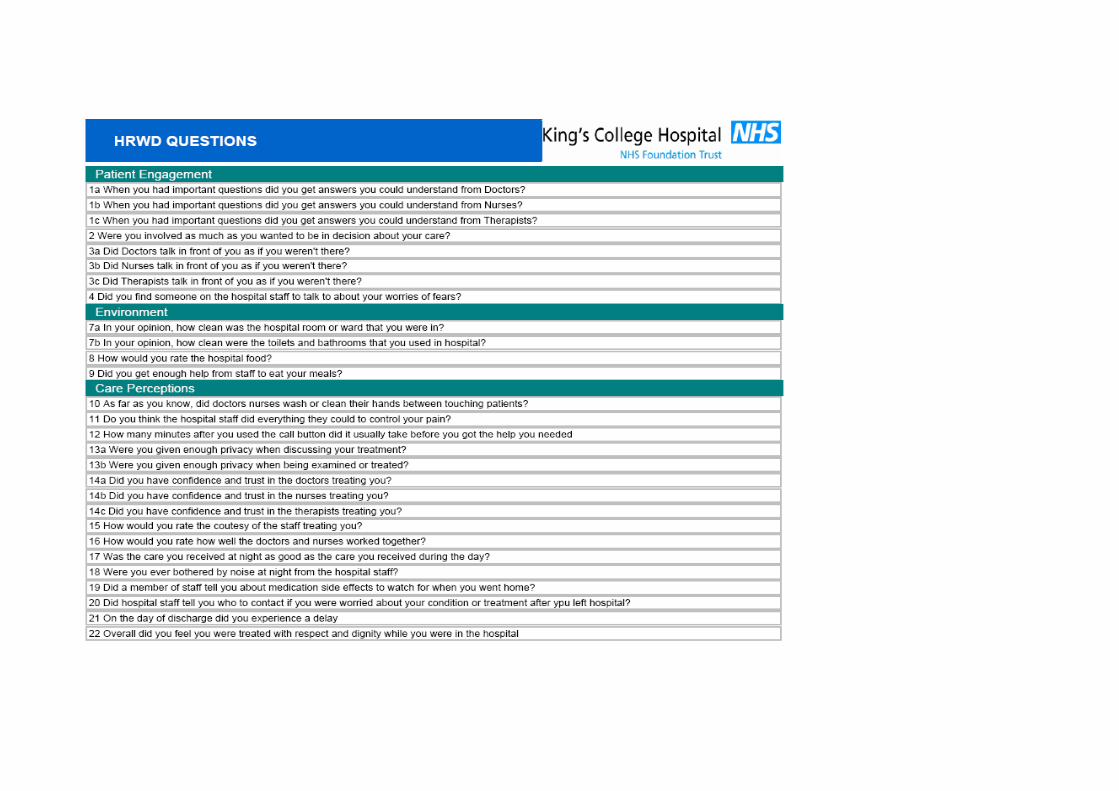
Enc 2.7.2
1
Report to: Board of Directors
Date of meeting: 20 December 2011
Subject: Eliminating Mixed Sex Accommodation (EMSA)
Author(s): Nicky Jonas, Design for Dignity Project Manager
Paula Townsend, Deputy Director of Nursing
Presented by: Geraldine Walters, Executive Director of Nursing & Midwifery
Sponsor: Geraldine Walters, Executive Director of Nursing & Midwifery
History: Previously considered by KE
Status: Information
1. Background/Purpose
This report provides an overview of the continued actions undertaken and highlights the improvements made by the Trust to achieve Same-Sex Accommodation (SSA) compliance.
2. Action required
The Trust Executive Committee is asked to note the contents of this report.
3. Key implications
Legal:
EMSA compliance forms part of the Care Quality Commission registration
Financial:
Non-compliance will incur financial penalties. The cost of undertaking the remaining changes to the Estate has been included in the 2011/12 capital programme
Assurance:
Detailed quarterly reports are made to the Board of Directors to highlight progress with the delivery plan
Clinical:
Significant quality issues that have arisen are summarised. The priority to admit patients and treat them promptly still remains.
Equality & Diversity:
This report has been subject to an equality impact assessment. Actions addressed in this paper are not believed to disadvantage any groups of patients or staff. Addressing the areas of non-compliance will ensure that all patients are treated in SSA
Performance:
Daily monitoring via the SSA database takes place and performance is monitored by NHS SE London bi-monthly. All
Enc 2.7.2
2
breaches are also reported on UNIFY
Strategy:
Risks highlighted in this report are recorded on the Trusts Risk Register and are monitored via the quarterly report to the Governance Committee.
Workforce:
All relevant staff have been made aware of the requirement to place patients in SSA
Estates:
Changes to some clinical areas have been identified and are being progressed. There is a process to ensure that all future developments are SSA compliant
Reputation:
Failure to be single sex complaint impacts adversely on the trust’s reputation
Enc 2.7.2
3
ELIMINATING MIXED SEX ACCOMMODATION (EMSA)
REPORT TO THE TRUST EXECUTIVE COMMITTEE. DECEMBER 2011
1. Current position Since the last report, the Trust has continued to make improvements in the provision of single sex accommodation and as a consequence has seen a steady reduction in breaches over the preceding months. Between June and October 2011 the trust was free from MSA breaches, but disappointingly in November 2011 reported breaches on 2 occasions due to a lack of capacity for step down care. As breaches are reducing, patient feedback through the HRWD survey has seen a corresponding sustained improvement in providing separate toilet and washrooms, and a recent improvement in single sex sleeping accommodation. Specific improvements over the last 6 months include All children over the age of 10 years who are admitted to a ward are asked their
preference for single gender and similar age accommodation which is recorded in their notes.
Alteration of theatre lists in day surgery to alternative times with more single sex and adult or child lists.
The purchase and use of portable screens in endoscopy and angiography. Completion of building alterations in Waddington and Clinical Decision Units in ED. Trust approval of business plan to redevelop Endoscopy to commence in July 2012 Updating of the Kwiki page and screen saver
NHS SE London re-visited in June 2011 and again reported favourably regarding our progress with EMSA. Their main area of concern was Endoscopy and they noted the planned improvement programme. A further visit is arranged for Jan/Feb 2012. The Trust’s improvement plans can be found in appendices 1and 2 2. Performance The Trust monitors single sex compliance through 2.1. Daily breach reporting (see tables over) Ward staff record breaches which are scrutinised daily by the DDNS and BIU with corrective action taken as indicated. This database is also used to report to Unify and produce a monthly report for the PCT and progress is reviewed at the quality bi-monthly meeting with NHS SE London. Over the last year the Trust has reduced the incidence of breaches which are becoming the exception rather the norm. In Q1 we had 13 breaches on 2 occasions; in Q2 there were no breaches, however in Q3 we reported 6 breaches on 2 occasions. The trust is fined £250 per breach.
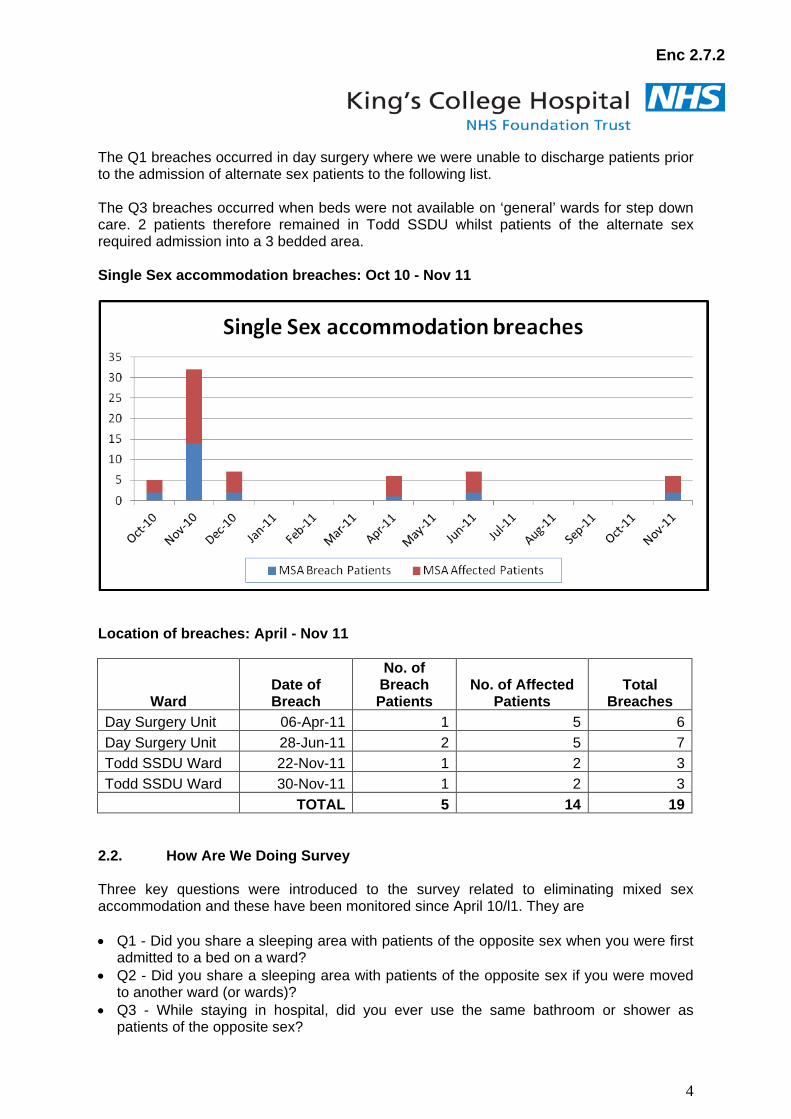
Enc 2.7.2
4
The Q1 breaches occurred in day surgery where we were unable to discharge patients prior to the admission of alternate sex patients to the following list. The Q3 breaches occurred when beds were not available on ‘general’ wards for step down care. 2 patients therefore remained in Todd SSDU whilst patients of the alternate sex required admission into a 3 bedded area. Single Sex accommodation breaches: Oct 10 - Nov 11
Location of breaches: April - Nov 11
Ward Date of Breach
No. of Breach Patients
No. of Affected Patients
Total Breaches
Day Surgery Unit 06-Apr-11 1 5 6 Day Surgery Unit 28-Jun-11 2 5 7 Todd SSDU Ward 22-Nov-11 1 2 3 Todd SSDU Ward 30-Nov-11 1 2 3 TOTAL 5 14 19
2.2. How Are We Doing Survey Three key questions were introduced to the survey related to eliminating mixed sex accommodation and these have been monitored since April 10/l1. They are • Q1 - Did you share a sleeping area with patients of the opposite sex when you were first
admitted to a bed on a ward? • Q2 - Did you share a sleeping area with patients of the opposite sex if you were moved
to another ward (or wards)? • Q3 - While staying in hospital, did you ever use the same bathroom or shower as
patients of the opposite sex?
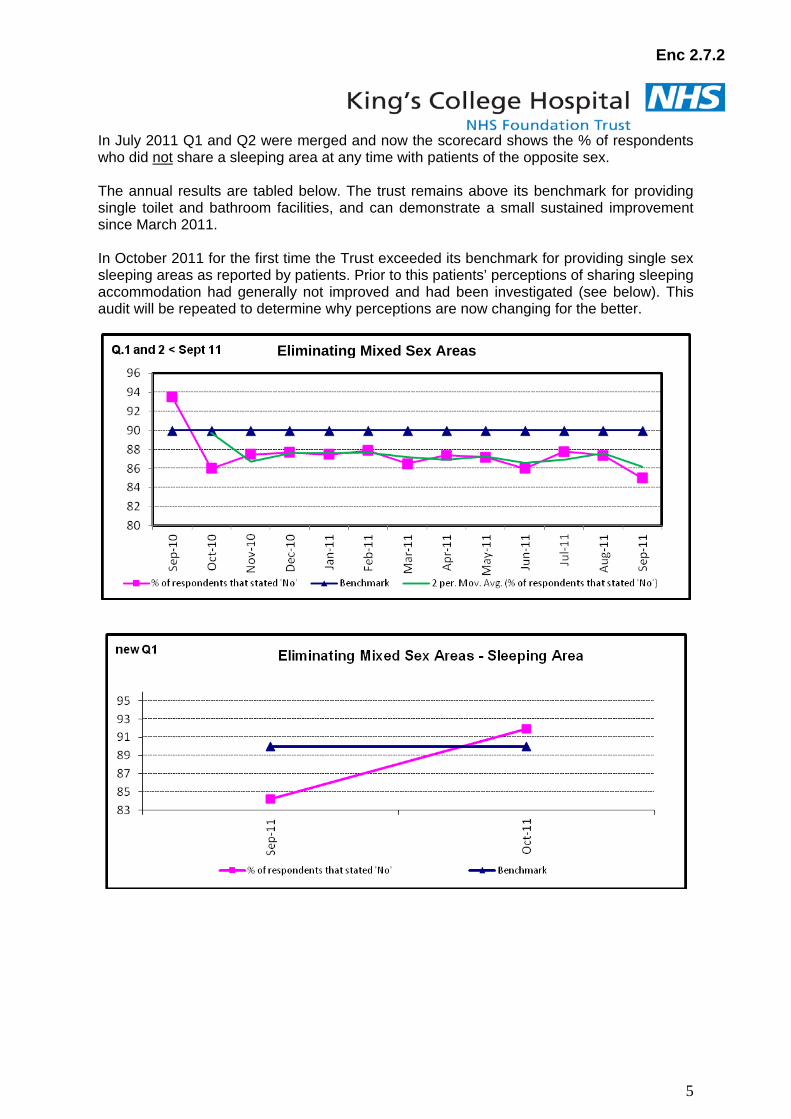
Enc 2.7.2
5
In July 2011 Q1 and Q2 were merged and now the scorecard shows the % of respondents who did not
share a sleeping area at any time with patients of the opposite sex.
The annual results are tabled below. The trust remains above its benchmark for providing single toilet and bathroom facilities, and can demonstrate a small sustained improvement since March 2011. In October 2011 for the first time the Trust exceeded its benchmark for providing single sex sleeping areas as reported by patients. Prior to this patients’ perceptions of sharing sleeping accommodation had generally not improved and had been investigated (see below). This audit will be repeated to determine why perceptions are now changing for the better.
Eliminating Mixed Sex Areas
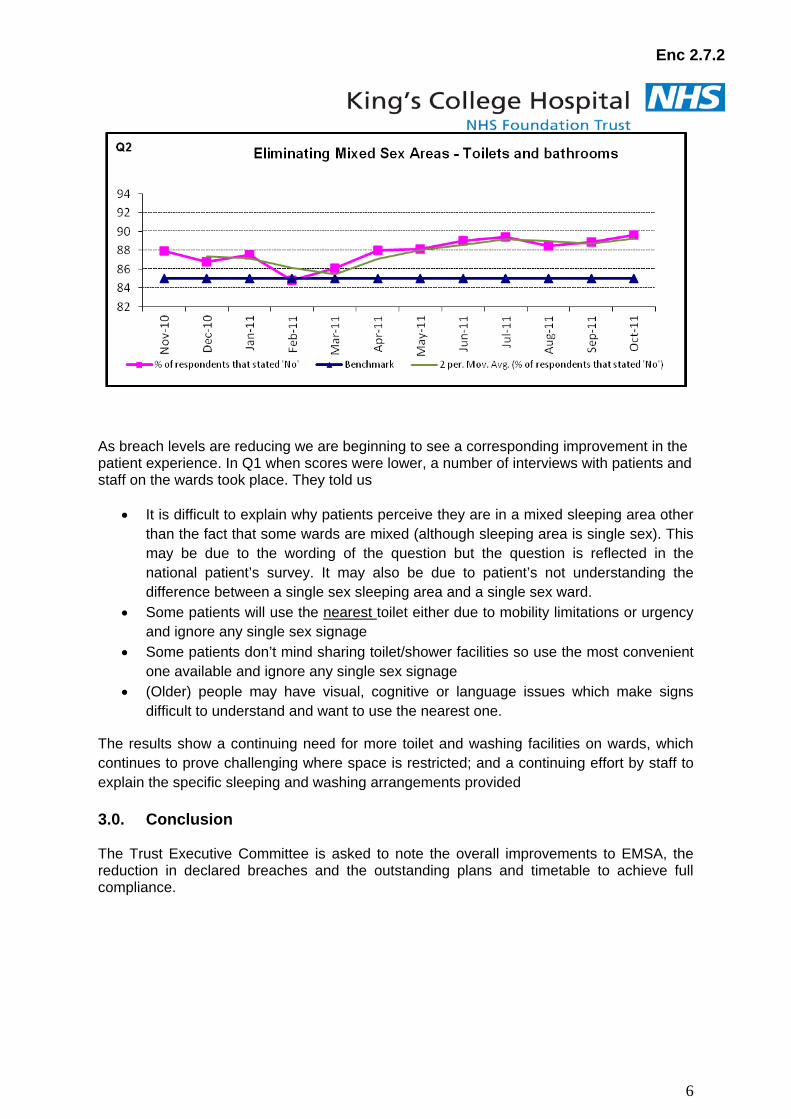
Enc 2.7.2
6
As breach levels are reducing we are beginning to see a corresponding improvement in the patient experience. In Q1 when scores were lower, a number of interviews with patients and staff on the wards took place. They told us
• It is difficult to explain why patients perceive they are in a mixed sleeping area other than the fact that some wards are mixed (although sleeping area is single sex). This may be due to the wording of the question but the question is reflected in the national patient’s survey. It may also be due to patient’s not understanding the difference between a single sex sleeping area and a single sex ward.
• Some patients will use the nearest
• Some patients don’t mind sharing toilet/shower facilities so use the most convenient one available and ignore any single sex signage
toilet either due to mobility limitations or urgency and ignore any single sex signage
• (Older) people may have visual, cognitive or language issues which make signs difficult to understand and want to use the nearest one.
The results show a continuing need for more toilet and washing facilities on wards, which continues to prove challenging where space is restricted; and a continuing effort by staff to explain the specific sleeping and washing arrangements provided 3.0. Conclusion The Trust Executive Committee is asked to note the overall improvements to EMSA, the reduction in declared breaches and the outstanding plans and timetable to achieve full compliance.
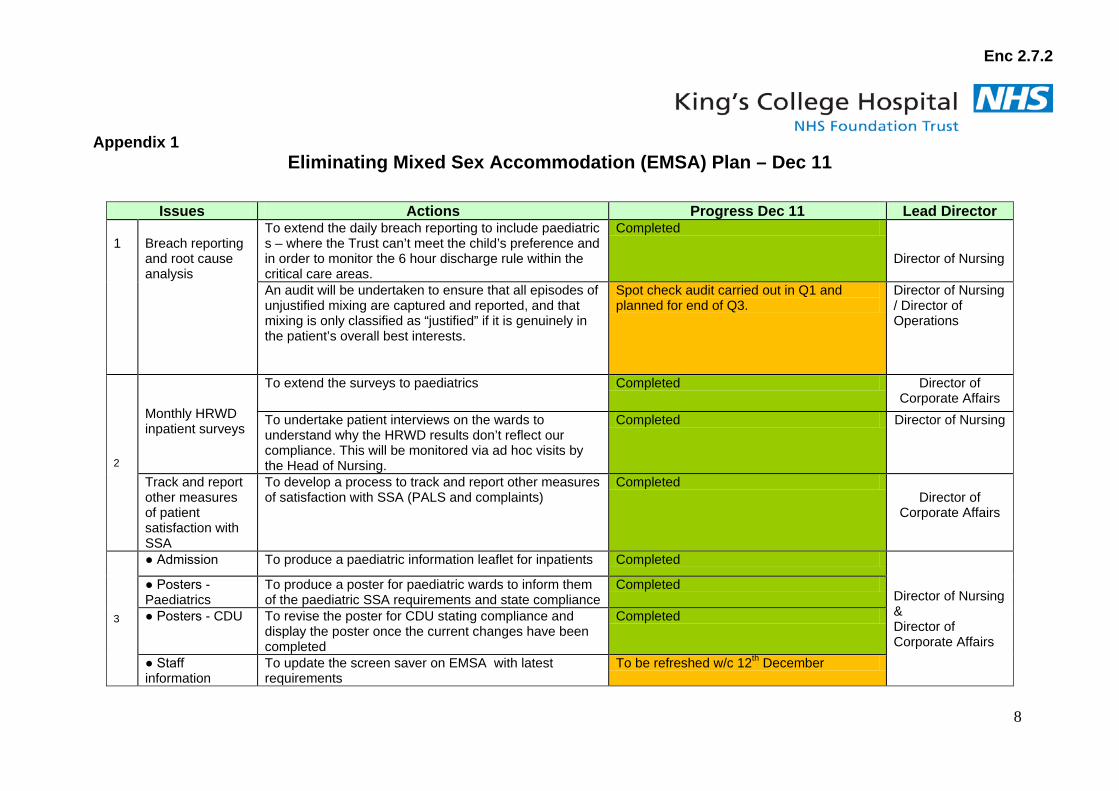
Enc 2.7.2
8
Appendix 1 Eliminating Mixed Sex Accommodation (EMSA) Plan – Dec 11
Issues Actions Progress Dec 11 Lead Director 1
Breach reporting and root cause analysis
To extend the daily breach reporting to include paediatric s – where the Trust can’t meet the child’s preference and in order to monitor the 6 hour discharge rule within the critical care areas.
Completed
Director of Nursing
An audit will be undertaken to ensure that all episodes of unjustified mixing are captured and reported, and that mixing is only classified as “justified” if it is genuinely in the patient’s overall best interests.
Spot check audit carried out in Q1 and planned for end of Q3.
Director of Nursing / Director of Operations
2
Monthly HRWD inpatient surveys
To extend the surveys to paediatrics Completed Director of Corporate Affairs
To undertake patient interviews on the wards to understand why the HRWD results don’t reflect our compliance. This will be monitored via ad hoc visits by the Head of Nursing.
Completed Director of Nursing
Track and report other measures of patient satisfaction with SSA
To develop a process to track and report other measures of satisfaction with SSA (PALS and complaints)
Completed Director of
Corporate Affairs
3
● Admission To produce a paediatric information leaflet for inpatients Completed
Director of Nursing & Director of Corporate Affairs
● Posters - Paediatrics
To produce a poster for paediatric wards to inform them of the paediatric SSA requirements and state compliance
Completed
● Posters - CDU To revise the poster for CDU stating compliance and display the poster once the current changes have been completed
Completed
● Staff information
To update the screen saver on EMSA with latest requirements
To be refreshed w/c 12th December
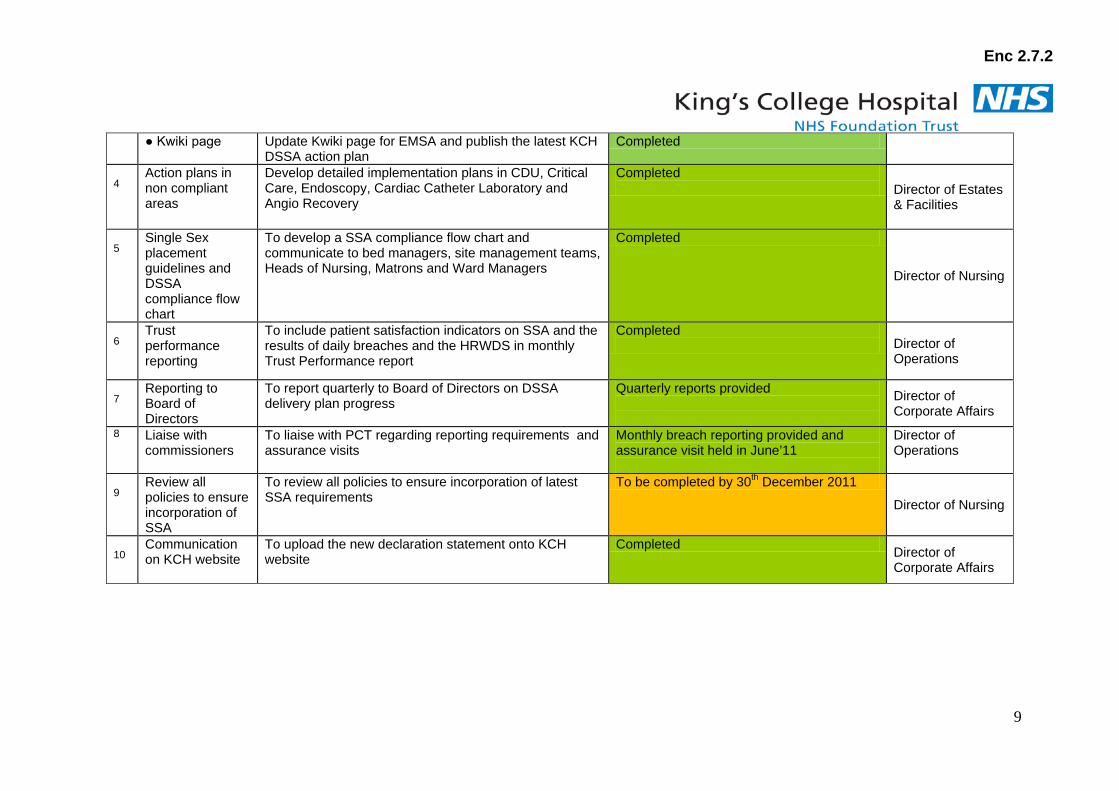
Enc 2.7.2
9
● Kwiki page Update Kwiki page for EMSA and publish the latest KCH DSSA action plan
Completed
4
Action plans in non compliant areas
Develop detailed implementation plans in CDU, Critical Care, Endoscopy, Cardiac Catheter Laboratory and Angio Recovery
Completed Director of Estates
& Facilities
5
Single Sex placement guidelines and DSSA compliance flow chart
To develop a SSA compliance flow chart and communicate to bed managers, site management teams, Heads of Nursing, Matrons and Ward Managers
Completed
Director of Nursing
6
Trust performance reporting
To include patient satisfaction indicators on SSA and the results of daily breaches and the HRWDS in monthly Trust Performance report
Completed Director of
Operations
7
Reporting to Board of Directors
To report quarterly to Board of Directors on DSSA delivery plan progress
Quarterly reports provided
Director of Corporate Affairs
8 Liaise with commissioners
To liaise with PCT regarding reporting requirements and assurance visits
Monthly breach reporting provided and assurance visit held in June’11
Director of Operations
9
Review all policies to ensure incorporation of SSA
To review all policies to ensure incorporation of latest SSA requirements
To be completed by 30th
Director of Nursing
December 2011
10
Communication on KCH website
To upload the new declaration statement onto KCH website
Completed Director of Corporate Affairs
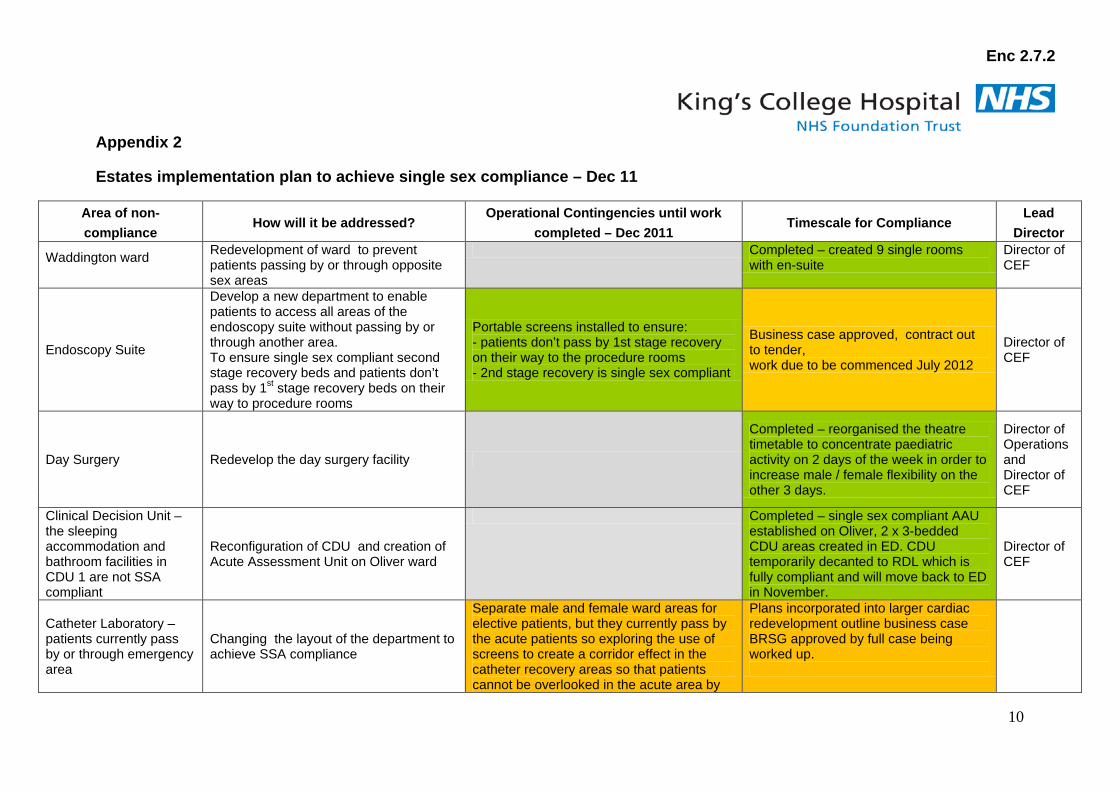
Enc 2.7.2
10
Appendix 2
Estates implementation plan to achieve single sex compliance – Dec 11
Area of non-compliance
How will it be addressed? Operational Contingencies until work
completed – Dec 2011 Timescale for Compliance
Lead Director
Waddington ward
Redevelopment of ward to prevent patients passing by or through opposite sex areas
Completed – created 9 single rooms with en-suite
Director of CEF
Endoscopy Suite
Develop a new department to enable patients to access all areas of the endoscopy suite without passing by or through another area. To ensure single sex compliant second stage recovery beds and patients don’t pass by 1st stage recovery beds on their way to procedure rooms
Portable screens installed to ensure: - patients don’t pass by 1st stage recovery on their way to the procedure rooms - 2nd stage recovery is single sex compliant
Business case approved, contract out to tender, work due to be commenced July 2012
Director of CEF
Day Surgery Redevelop the day surgery facility
Completed – reorganised the theatre timetable to concentrate paediatric activity on 2 days of the week in order to increase male / female flexibility on the other 3 days.
Director of Operations and Director of CEF
Clinical Decision Unit – the sleeping accommodation and bathroom facilities in CDU 1 are not SSA compliant
Reconfiguration of CDU and creation of Acute Assessment Unit on Oliver ward
Completed – single sex compliant AAU established on Oliver, 2 x 3-bedded CDU areas created in ED. CDU temporarily decanted to RDL which is fully compliant and will move back to ED in November.
Director of CEF
Catheter Laboratory – patients currently pass by or through emergency area
Changing the layout of the department to achieve SSA compliance
Separate male and female ward areas for elective patients, but they currently pass by the acute patients so exploring the use of screens to create a corridor effect in the catheter recovery areas so that patients cannot be overlooked in the acute area by
Plans incorporated into larger cardiac redevelopment outline business case BRSG approved by full case being worked up.
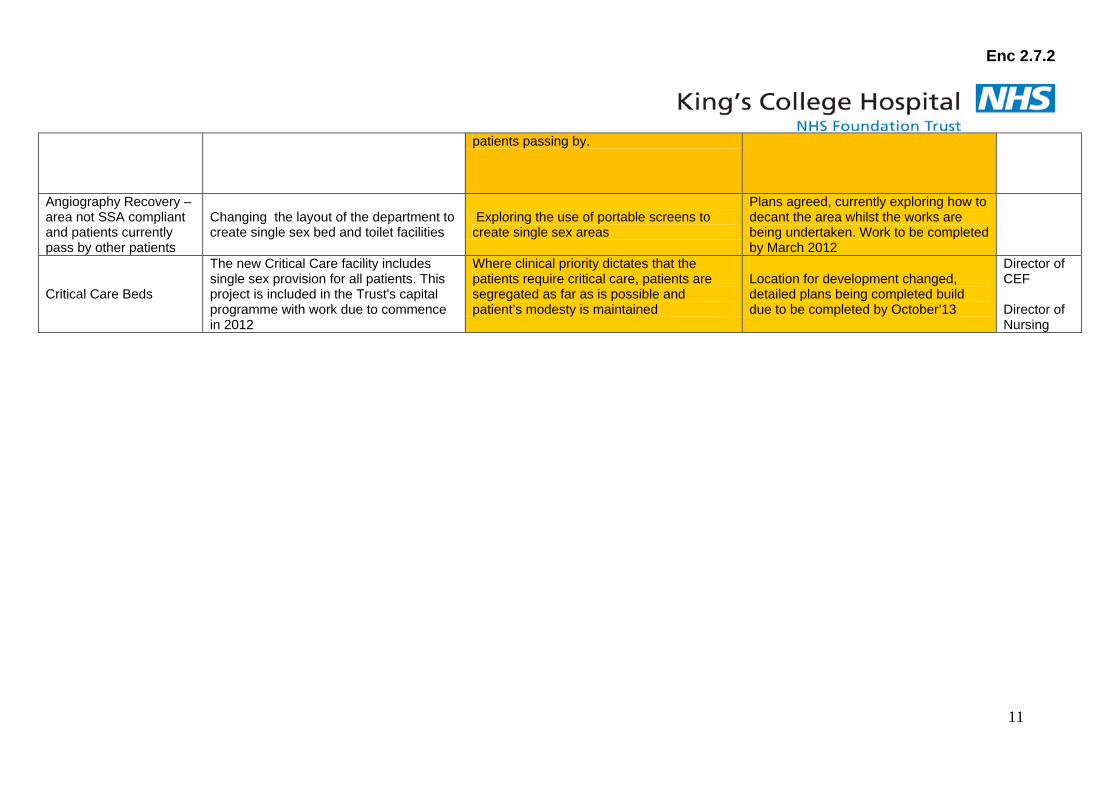
Enc 2.7.2
11
patients passing by.
Angiography Recovery – area not SSA compliant and patients currently pass by other patients
Changing the layout of the department to create single sex bed and toilet facilities
Exploring the use of portable screens to create single sex areas
Plans agreed, currently exploring how to decant the area whilst the works are being undertaken. Work to be completed by March 2012
Critical Care Beds
The new Critical Care facility includes single sex provision for all patients. This project is included in the Trust's capital programme with work due to commence in 2012
Where clinical priority dictates that the patients require critical care, patients are segregated as far as is possible and patient’s modesty is maintained
Location for development changed, detailed plans being completed build due to be completed by October’13
Director of CEF Director of Nursing
Enc 2.8
1
Report to: Board of Directors Date of meeting: 20 December 2011 By: George Alberti, Chair Subject: Outline of Key Matters arising from Council of Governors 1. Summary The new Council of Governors met on 01 December 2011. The meeting was well attended and it was encouraging and appreciated to see so many of the executive team members at the meeting. The meeting focus on forward planning, induction and future engagement and training needs. The Council also received two comprehensive presentations on Ward 20:20 and the Health & Social Care Bill. 2. Matters for Decision 2.2 Name of the Board/Council of Governors Governors agreed to a proposal to change the name of the Board of Governors to Council of Governors. This change reflects both the change of name mooted in the Health and Social Care Bill and also is felt to avoid potential confusion between the respective roles and responsibilities of the Board of Directors and Council of Governors. 2.3 Council Committees The Council agreed to continue the following four committees with the agreed changes to their remit:
1) Strategy Committee - No change to the remit but the Council would like more regular information on KHP. The first meeting of the new Strategy Committee would discuss the KHP proposals on 19 January 2012.
2) Membership and Community Engagement Committee – The remit of this
Committee is to be expanded to encompass consideration of wider community issues and outreach.
3) Patient Safety and Experience Committee – No Change
Enc 2.8
2
4) Transport and Environment Committee – The remit of the Committee is to be expanded to encompass other areas of the local environment such as planning issues, car parking and general environmental issues which affect the hospital, its patients and the local community at large.
Dates of the Committee meetings are attached for information - Appendix 1. It was emphasised that any Governor can attend any of the sub–committees. 2.4 Lead Governor The Council agreed to defer consideration of the role and process for appointing a Lead Governor until the New Year, to enable Council members to get to know one another first. 2.5 Governor Engagement Governors have asked for more engagement opportunities with executives and non-executives and also to network with each other. Provisional dates have been identified for a Joint Council of Governors/Board of Directors Meeting in the Spring and an annual Governor Development Day:
• 20 March 2012 – Joint Meeting of Council of Governors/Board of Directors
• 18 October 2012 – Annual Governor Development Day Work continues to identify other opportunities to facilitate networking opportunities. 2.6 Directors’ Surgeries Governors indicated that they would like to continue with the previous tradition of holding’ Directors Surgeries’, to be held three times a year, on topics chosen by Governors. The initial areas of interest highlighted at the meeting were finance and healthcare acquired infections. Governors will be invited to suggest topics for discussion, and dates for 2012 will be notified. 2.7 Other areas of interest and actions Governors want to receive regular newsletters/information sheets on KHP Developments. Once the Health and Social Care Act is enacted, the Governors would like to receive a detailed guide on the implications for the Trust and Governors. The Chair encouraged Governors to contact him if they had any issues that they wished to raise. 3. Recommendation The Board is asked to note this report and offer any comments.
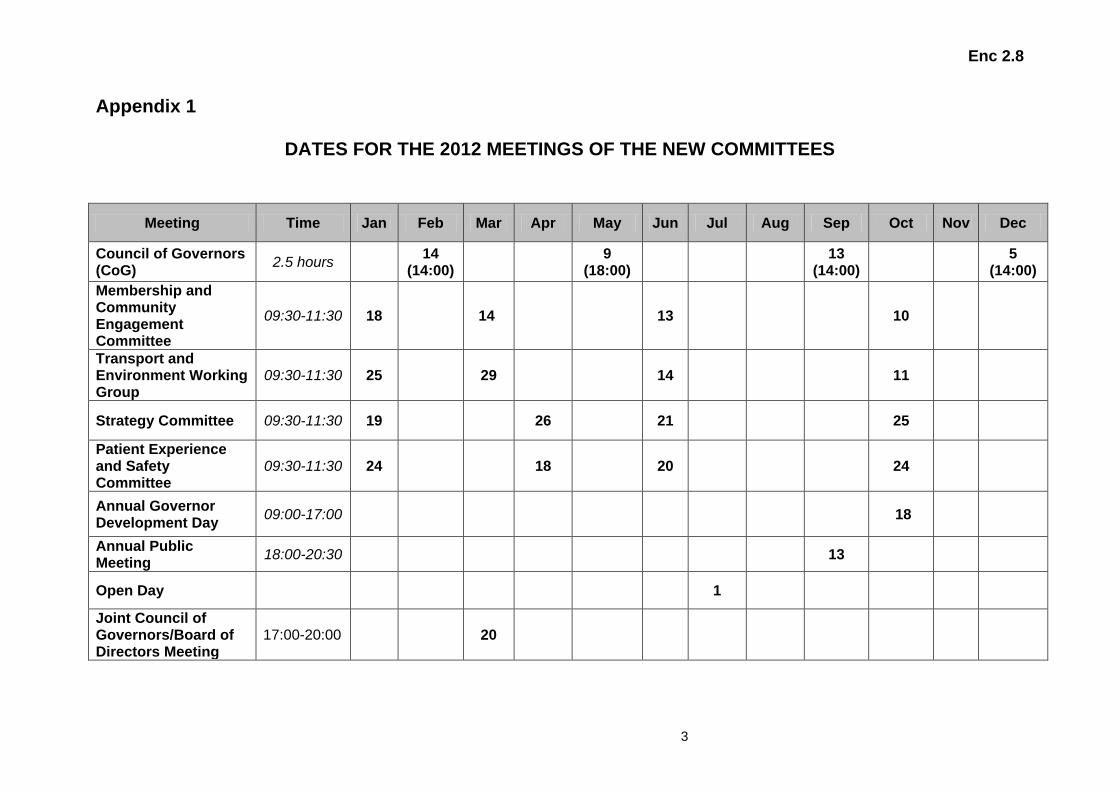
Enc 2.8
3
Appendix 1
DATES FOR THE 2012 MEETINGS OF THE NEW COMMITTEES
Meeting Time Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Council of Governors (CoG) 2.5 hours 14
(14:00) 9 (18:00) 13
(14:00) 5 (14:00)
Membership and Community Engagement Committee
09:30-11:30 18 14 13 10
Transport and Environment Working Group
09:30-11:30 25 29 14 11
Strategy Committee 09:30-11:30 19 26 21 25
Patient Experience and Safety Committee
09:30-11:30 24 18 20 24
Annual Governor Development Day 09:00-17:00 18
Annual Public Meeting 18:00-20:30 13
Open Day 1
Joint Council of Governors/Board of Directors Meeting
17:00-20:00 20

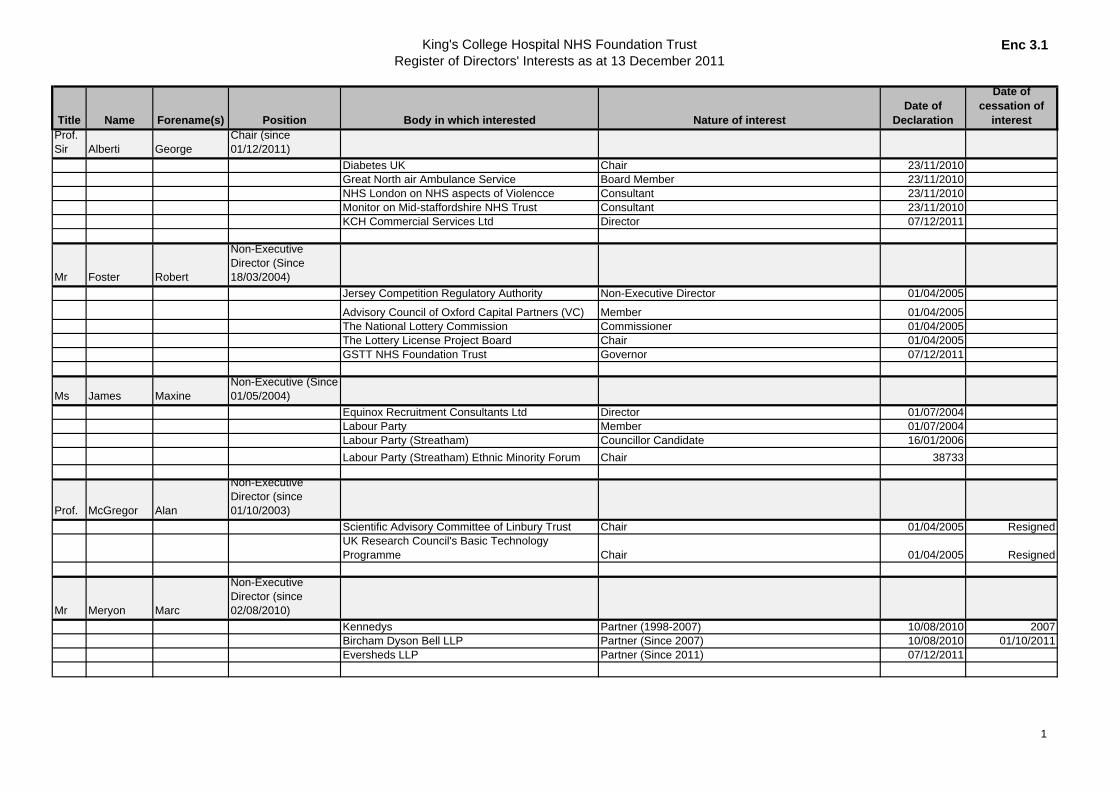
King's College Hospital NHS Foundation TrustRegister of Directors' Interests as at 13 December 2011
Enc 3.1
Title Name Forename(s) Position Body in which interested Nature of interestDate of
Declaration
Date of cessation of
interestProf. Sir Alberti George
Chair (since 01/12/2011)
Diabetes UK Chair 23/11/2010Great North air Ambulance Service Board Member 23/11/2010NHS London on NHS aspects of Violencce Consultant 23/11/2010Monitor on Mid-staffordshire NHS Trust Consultant 23/11/2010KCH Commercial Services Ltd Director 07/12/2011
Mr Foster Robert
Non-Executive Director (Since 18/03/2004)
Jersey Competition Regulatory Authority Non-Executive Director 01/04/2005
Advisory Council of Oxford Capital Partners (VC) Member 01/04/2005The National Lottery Commission Commissioner 01/04/2005The Lottery License Project Board Chair 01/04/2005GSTT NHS Foundation Trust Governor 07/12/2011
Ms James MaxineNon-Executive (Since 01/05/2004)
Equinox Recruitment Consultants Ltd Director 01/07/2004Labour Party Member 01/07/2004Labour Party (Streatham) Councillor Candidate 16/01/2006Labour Party (Streatham) Ethnic Minority Forum Chair 38733
Prof. McGregor Alan
Non-Executive Director (since 01/10/2003)
Scientific Advisory Committee of Linbury Trust Chair 01/04/2005 ResignedUK Research Council's Basic Technology Programme Chair 01/04/2005 Resigned
Mr Meryon Marc
Non-Executive Director (since 02/08/2010)
Kennedys Partner (1998-2007) 10/08/2010 2007Bircham Dyson Bell LLP Partner (Since 2007) 10/08/2010 01/10/2011Eversheds LLP Partner (Since 2011) 07/12/2011
1
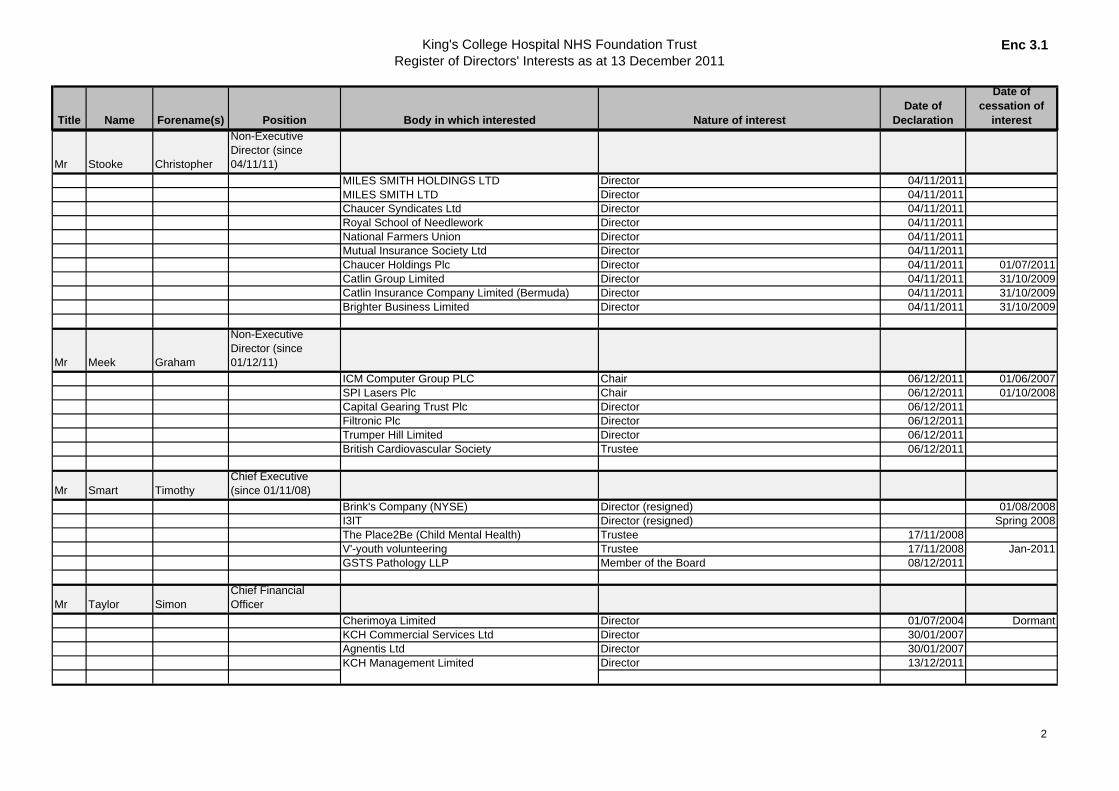
King's College Hospital NHS Foundation TrustRegister of Directors' Interests as at 13 December 2011
Enc 3.1
Title Name Forename(s) Position Body in which interested Nature of interestDate of
Declaration
Date of cessation of
interest
Mr Stooke Christopher
Non-Executive Director (since 04/11/11)
MILES SMITH HOLDINGS LTD Director 04/11/2011MILES SMITH LTD Director 04/11/2011Chaucer Syndicates Ltd Director 04/11/2011Royal School of Needlework Director 04/11/2011National Farmers Union Director 04/11/2011Mutual Insurance Society Ltd Director 04/11/2011Chaucer Holdings Plc Director 04/11/2011 01/07/2011Catlin Group Limited Director 04/11/2011 31/10/2009Catlin Insurance Company Limited (Bermuda) Director 04/11/2011 31/10/2009Brighter Business Limited Director 04/11/2011 31/10/2009
Mr Meek Graham
Non-Executive Director (since 01/12/11)
ICM Computer Group PLC Chair 06/12/2011 01/06/2007SPI Lasers Plc Chair 06/12/2011 01/10/2008Capital Gearing Trust Plc Director 06/12/2011Filtronic Plc Director 06/12/2011Trumper Hill Limited Director 06/12/2011British Cardiovascular Society Trustee 06/12/2011
Mr Smart TimothyChief Executive (since 01/11/08)
Brink's Company (NYSE) Director (resigned) 01/08/2008I3IT Director (resigned) Spring 2008The Place2Be (Child Mental Health) Trustee 17/11/2008V'-youth volunteering Trustee 17/11/2008 Jan-2011GSTS Pathology LLP Member of the Board 08/12/2011
Mr Taylor SimonChief Financial Officer
Cherimoya Limited Director 01/07/2004 DormantKCH Commercial Services Ltd Director 30/01/2007Agnentis Ltd Director 30/01/2007KCH Management Limited Director 13/12/2011
2
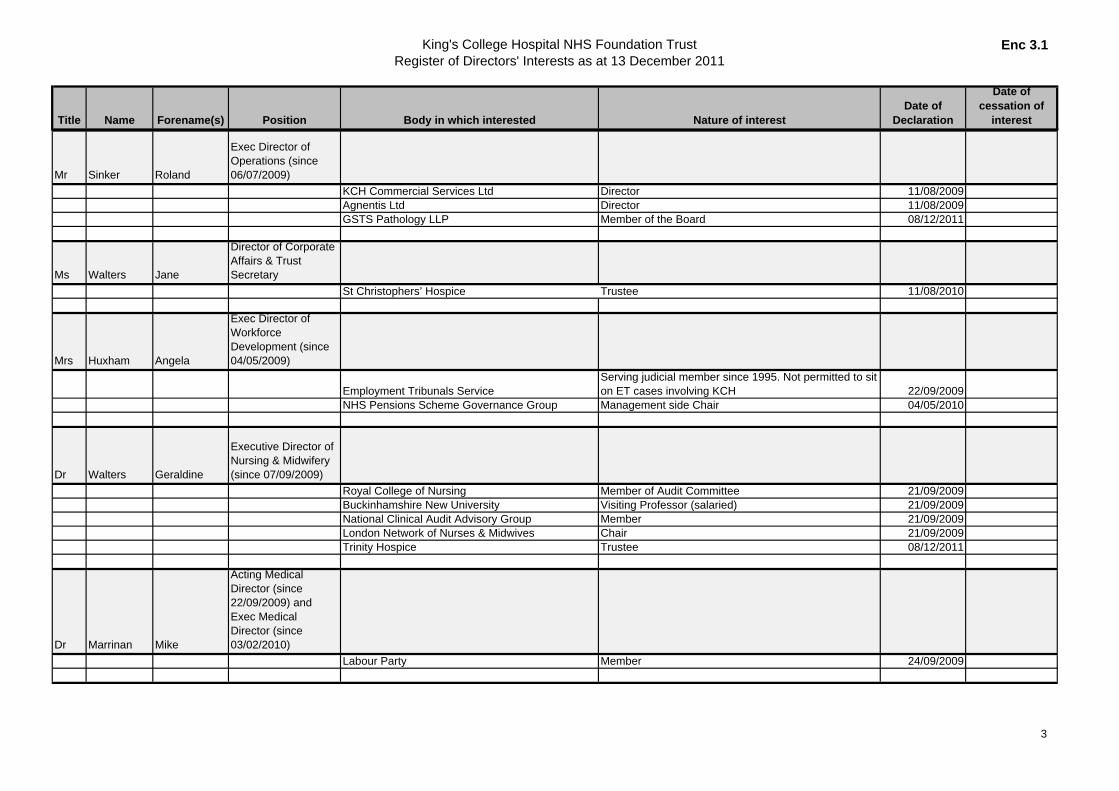
King's College Hospital NHS Foundation TrustRegister of Directors' Interests as at 13 December 2011
Enc 3.1
Title Name Forename(s) Position Body in which interested Nature of interestDate of
Declaration
Date of cessation of
interest
Mr Sinker Roland
Exec Director of Operations (since 06/07/2009)
KCH Commercial Services Ltd Director 11/08/2009Agnentis Ltd Director 11/08/2009GSTS Pathology LLP Member of the Board 08/12/2011
Ms Walters Jane
Director of Corporate Affairs & Trust Secretary
St Christophers’ Hospice Trustee 11/08/2010
Mrs Huxham Angela
Exec Director of Workforce Development (since 04/05/2009)
Employment Tribunals ServiceServing judicial member since 1995. Not permitted to sit on ET cases involving KCH 22/09/2009
NHS Pensions Scheme Governance Group Management side Chair 04/05/2010
Dr Walters Geraldine
Executive Director of Nursing & Midwifery (since 07/09/2009)
Royal College of Nursing Member of Audit Committee 21/09/2009Buckinhamshire New University Visiting Professor (salaried) 21/09/2009National Clinical Audit Advisory Group Member 21/09/2009London Network of Nurses & Midwives Chair 21/09/2009Trinity Hospice Trustee 08/12/2011
Dr Marrinan Mike
Acting Medical Director (since 22/09/2009) and Exec Medical Director (since 03/02/2010)
Labour Party Member 24/09/2009
3
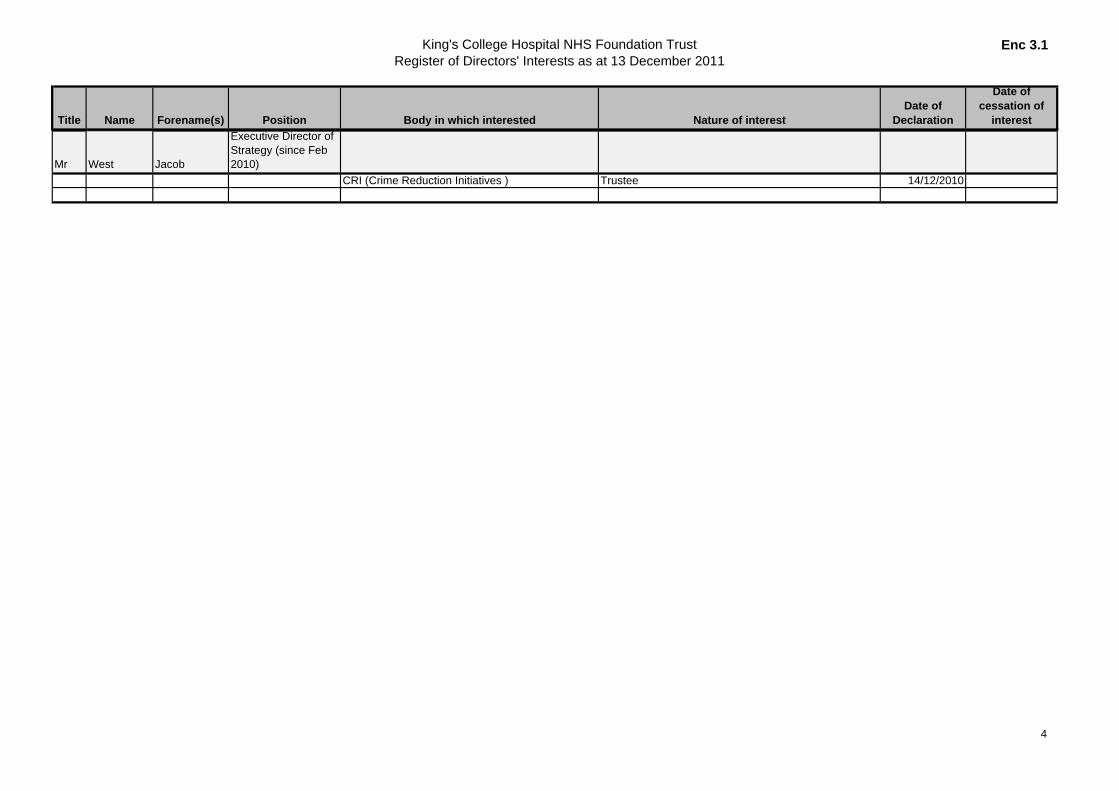
King's College Hospital NHS Foundation TrustRegister of Directors' Interests as at 13 December 2011
Enc 3.1
Title Name Forename(s) Position Body in which interested Nature of interestDate of
Declaration
Date of cessation of
interest
Mr West Jacob
Executive Director of Strategy (since Feb 2010)
CRI (Crime Reduction Initiatives ) Trustee 14/12/2010
4