Embed Size (px)
Citation preview

QUESTIONS DIALYSIS FACILITY MANAGEMENT MIGHT ASK ABOUT KIDNEY TRANSPLANT 1.
2.
• •
• •
• • • • •
Do patients have the information they need to make a decision?
Each dialysis facility should have a written policy specifying when treatment options, including transplant, are discussed with patients and who is responsible for presenting this discussion. The Social Worker or Head Nurse may be the individual designated to discuss hemodialysis, peritoneal dialysis and transplant with a patient. Even if information has been distributed to the patient previously, he/she might need a second opportunity to decide whether transplant is an option for them. Patients are frequently overwhelmed by decisions when dialysis treatment is initiated, or may feel too ill to think about having a kidney transplant. The use of educational tools, such as audio-visual materials and brochures, provide patients and family members an opportunity to review options and ask questions. Many facilities use the Long Term Care Plan (required for all ESRD patients) and an admission assessment tool to document discussions of treatment options, including transplant. Physicians can use the annual review of the Long Term Care Plan to re-consider transplant eligibility. This encourages input from the patient about quality of life and satisfaction with current treatment modality.
Which patients are candidates for transplant referral?
Each transplant center sets minimum criteria specifying which patients are medically eligible for transplant. It is important that physicians know each center’s criteria. Patients should carefully discuss any current medical conditions with their nephrologist before referral to a transplant center to determine whether they are healthy enough to receive a kidney transplant. Remember that each center will approach “unsuitable” conditions differently, for instance if you are overweight, the transplant center might ask you to sign a contract stating you will lose weight so that you can be eligible for a transplant.
Suitable Patients Are Usually: Psychologically stable Understand risks, hazards & benefits of transplant Free of uncorrectable medical conditions Less than 70 years of age (varies per Transplant program)
Unsuitable Patient: Untreatable psychopathology Alcohol or drug abuse Morbid obesity Advanced cardiac or vascular disease Recent (or incurable) cancer
Consultation with the transplant center is encouraged before determining unsuitability.
MARC, 2002 1

Age may not exclude patients from receiving a kidney transplant. In some instances, 75-year-old patients are transplanted in Network 5. Older dialysis patients should not be discouraged from pursuing transplant if their general health is good. In addition, patients should have access to information about transplant, even if their physical condition is considered marginal. Transplant center intake coordinators are trained to screen patients to determine whether they meet transplant eligibility criteria and the transplant surgeon makes the final decision as to whether the patient is an eligible candidate. If the patient is refused transplant due to a medical condition, that information is frequently accepted more easily from the transplant center staff. The patient may also be given the option to have elective surgical procedures, such as coronary artery bypass graft or bladder surgery, in order to be eligible for transplant.
3. Is transplant discussed with all medically eligible patients?
Network 5 conducts the Transplant Status Survey every two years. This survey requires that each dialysis facility classify adult patients, (18-65 years of age) into five status groups.
STATUS 1: Patient on transplant waiting list OR scheduled for living donor transplant STATUS 2: Patient referred for transplant evaluation with status pending STATUS 3: Patient refuses transplant option STATUS 4: Patient medically unsuitable for transplant STATUS 5: Patient’s transplant candidacy not yet established
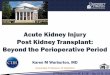
NW 5 TRANSPLANT REFERRAL PATTERNS Year End 1990-2000, Dialysis Patients 18-65 Years of Age
0
10
20
30
40
% Waiting % Referred % Refusing % Med Unsuit % Not Estab
1992 1994 1996 2000
1990 1998
When reviewing the results of the 2000 survey noted in the graph above, certain “facility” effects were identified.
24 dialysis units reported that less that 10% of their patients had been referred for transplant evaluation
•
• •
41 dialysis units reported that more than 40% of their patients refuse transplant as an option 35 dialysis units reported that 60% of their patients were medically unsuitable to receive transplant
Biased attitudes in the dialysis units may be affecting transplant discussions with some income, gender, and racial groups. For these reasons, each facility is asked to develop written policies that specifically define that transplant information is presented to ALL medically eligible patients.
MARC, 2002 2

QUESTIONS PATIENTS MIGHT ASK ABOUT KIDNEY TRANSPLANT
1. How much will a transplant cost? Will my insurance pay for my transplant?
What will my medications cost?
It is impossible to provide a complete list of transplant costs for each Network 5 transplant center. Patients need to be aware that transplant centers have financial counselors available to discuss and explore transplant costs so the patient knows exactly what costs are covered. The counselor will also ask the patient to provide complete financial information, which will be kept confidential. It has been estimated that first year cost of a kidney transplant is $116,100. Medicare covers all reasonable expenses with the exception of the Part A deductible and the Part B 20% co-insurance. Patients are encouraged to have a primary and secondary insurance policy in place before initiating transplant work-up (dialysis facility social workers may be able to assist patients in obtaining secondary or “Medigap” hospital insurance policies). Remember that you must think about the 20% cost of surgery and immunosuppressive medications if you elect to have only Medicare coverage, and those costs add up quickly. If the patient has a private primary insurance carrier, transplant benefits should be verified prior to evaluation, including information on deductibles and co-payment requirements. The transplant center financial counselor or social worker will assist the patient in obtaining this information. Patients are encouraged to ask about “pre-approval” for transplant and “approved transplant centers.” The patient should be certain that each monthly insurance premium is paid so that there is no lapse in insurance coverage. It is necessary for every transplant recipient to take several different medicines to keep you body from rejecting or damaging the new kidney. Currently, Medicare covers immunosuppressive medications for three years after kidney transplant for End Stage Renal Disease Patients (ESRD) patients. Congress has extended this coverage for the life of the transplanted kidney if the patient is eligible for Medicare due to age, or receives Social Security Disability Income (SSDI). The annual cost of immunosuppressive medications is estimated to be approximately $20,000. Some pharmaceutical grant programs exist for a small number of indigent patients. The transplant center may be able to help patients explore these options. These “immunosuppressive” medications also change the way your body responds to infection. Please be certain that you ask questions about these medications and their use when you see the transplant center staff.
2. Will receiving a transplant make my life better?
Transplant patients state that receiving a new kidney allows them to return to a more normal life, feel better, and be more active. They enjoy freedom from dialysis, and have fewer dietary restrictions. Statistically, patients who receive kidney transplants have a longer life expectancy than dialysis patients. The following tables display United States Renal Data System (USRDS) survival probability rates from the 2001 Annual Data Report (Reference Tables 1.22 and G.3). More USRDS data can be viewed on the Internet at http://www.usrds.org/reference.htm. Survival data are displayed for patients who received cadaveric transplants, living donor transplants, and new (incident) dialysis patients during the periods shown below. Age comparisons were aligned as closely as possible, based on USRDS’ selected age cohorts.
1 year cohort, 1998, • • 5 year cohort data, 1994, and • 10 year cohort data, 1989.
MARC, 2002 3

USRDS PATIENT Survival Unadjusted Probability Rates
USRDS GRAFT Survival Unadjusted Probability Rates
Following 1st Cadaveric Transplant Following 1st Cadaveric Transplant Patient Age 1 Yr 5 Yr 10 Yr Patient Age 1 Yr 5 Yr 10 Yr 18-29 Yrs Old 98.2% 91.6% 76.4% 18-29 Yrs Old 90.8% 53.7% 38.0% 30-44 Yrs Old 97.1% 85.0% 64.5% 30-44 Yrs Old 91.7% 61.4% 37.5% 45-54 Yrs Old 94.9% 79.9% 52.3% 45-54 Yrs Old 88.4% 59.2% 34.2%
USRDS PATIENT Survival Unadjusted Probability Rates
USRDS GRAFT Survival Unadjusted Probability Rates
Following 1st Living Donor Transplant Following 1st Living Donor Transplant Patient Age 1 Yr 5 Yr 10 Yr Patient Age 1 Yr 5 Yr 10 Yr 18-29 Yrs Old 99.7% 95.8% 86.5% 18-29 Yrs Old 94.7% 53.7% 70.5% 30-44 Yrs Old 98.8% 91.2% 78.7% 30-44 Yrs Old 95.1% 61.4% 74.5% 45-54 Yrs Old 97.4% 86.5% 65.5% 45-54 Yrs Old 94.1% 59.2% 70.8% USRDS Patient Survival
Unadjusted Probability Rates
Incident (NEW) Dialysis Patients Patient Age 1 Yr 5 Yr 10 Yr 20-29 Yrs Old 94.8% 73.0% 41.1% 30-39 Yrs Old 90.9% 58.7% 30.9% 40-49 Yrs Old 88.9% 51.0% 19.2%
3.
4.
5.
Can I catch a serious disease like AIDS if I get a kidney transplant?
The transplant center and Organ Procurement Organization (OPO) will conduct multiple tests to prevent disease transmission from the donor during transplantation. All donors, both cadaveric and living, are tested for infectious diseases including HIV, Hepatitis B and C, and Cytomegalovirus (CMV). Additional tests are conducted to determine the status of other diseases, which could present a problem for the immunosuppressed patient after transplant.
How can I be sure I will get the right kidney for me?
Laboratory tests will be done to insure that the donor and recipient are medically compatible. These include blood type (A, B, O grouping), genetic testing of body cells for HLA typing (Human Leukocyte Antigen), and monthly Panel Reactive Antibody (PRA). The recipient’s blood is tested each month to help the physician evaluate any changes until a transplant occurs. The patient should be certain that the dialysis unit or physician’s office draws these monthly blood samples, and sends them to the transplant center. When an organ is available, it is offered to patients who are the best match for that particular organ. A final compatibility test is done prior to the transplant using the monthly serum sample. If the laboratory does not have a current sample, you may not be selected. If the crossmatch is acceptable, then the transplant can take place if the size of the donor organ, the storage time, and the recipient’s health on that date are acceptable.
How long will I have to wait for a transplant?
MARC, 2002 4

When a patient is listed for cadaveric transplant, they could receive a kidney the day they are placed on the waiting list, or they might wait several years before receiving a kidney. Time spent waiting for a cadaveric transplant varies by transplant center. In the thirteen Network 5 transplant centers, the median time that patients waited for a transplant between January 1996 and June 2001 was 39.1 months. Median is defined as the middle number in a range; as used here it means that half of the patients waited less than 39 months and half waited longer than 39 months for their transplant. The shortest median wait was 9.6 months and the longest median wait was 70.3 months. The number of months spent on the wait list at every United States transplant center can be viewed on the Internet at http://www.ustransplant.org/national.html. The number of donor organs available, the number of patients listed for transplant, and the results of the monthly PRA testing all affect wait time. When there is a living donor, surgery can be scheduled at a time convenient to the donor and recipient as soon as medical evaluation and testing are complete. Generally, the time waiting is much shorter with a living donor.
6.
7.
8.
9.
•
•
What are the risks involved if I have surgery?
Any major surgery and general anesthesia can pose some risks to the patient. An extensive medical evaluation is done to determine whether a patient is an acceptable candidate for surgery and for transplant.
Will I have a lot of pain? How long will I be in the hospital?
Most patients recover from kidney transplant surgery rapidly, and are ready to leave the hospital in a few days, depending on the transplant center. While surgery is always associated with pain, there are varieties of intravenous and oral medications that provide excellent pain control. Fear of pain should not be a reason to decide against a kidney transplant!
Will I lose my disability benefits?
Some transplant patients are eligible for Supplemental Security Income (SSI) assistance and medication grants. If the patient is currently receiving disability benefits, the Social Security Office can advise them on how frequently their file will be reviewed after transplant. If their medical condition improves, and they are able to work, their benefits may stop. Individuals are allowed to work for nine “trial” months before their final status is determined. The financial counselor at the transplant center can provide complete information about how the disability program works.
Can a member of my family, or a friend, give me a kidney?
Yes, family members, distant relatives, spouses, or friends can donate a kidney to you. You can receive a living related transplant (a kidney donated by a family member) or a living unrelated transplant (a kidney donated by someone who is not a blood relative). Transplant centers look at many variables when evaluating a possible living donor. Living donors must be healthy, free of kidney disease, and have normal blood pressure. The best matches come from full siblings (brothers or sisters), but transplants from the poorest matched living donor are more successful than the best matched cadaver (non-living) donor. The transplant center will educate both the donor and the recipient about what to expect during this process. Examples of areas evaluated by transplant centers and OPOs are listed below.
Blood Group; A, B, O compatibility – determine the blood type of the donor and the recipient and make decisions about whether the donor can be used Cross match - mix samples of donor’s and recipient’s blood together on a slide and view under a microscope to determine whether recipient’s cells try to destroy the donor’s cells
MARC, 2002 5

Donor and Recipient - Preliminary medical assessment – extensive review of donor’s and recipient’s existing and previous medical conditions to determine whether transplant surgery is possible
•
•
•
Age, renal function, and anatomy acceptable? - Evaluate function, size and structure of the donor kidney to determine whether transplant is possible Psychosocial assessment – assessment of mental and emotional stability of the prospective donor to determine their ability to donate an organ
If all of the above assessments are found to be positive then Transplant surgery can take place.
10. What kind of outcomes can I expect after a transplant?
The transplant center can provide outcome data on the performance of their program. Data on patient survival, graft (the kidney) survival, infection rates, and complication rates are public record and are available to the patient. To view survival data on the Internet go to The Scientific Registry of Transplant Recipients (SRTR) at http://ustransplant.org/. QUESTIONS DIALYSIS FACILITY STAFF MEMBERS MIGHT ASK ABOUT KIDNEY TRANSPLANT
1.
2.
Does the patient’s family understand what the patient wants and needs?
When a patient considers transplant, specifically living donor transplant, he/she may have to deal with many emotions, for example:
• “Will someone in my family want to do this?” • “How will it affect their (the donor’s) health?” • “I DON’T WANT a member of my family to donate a kidney!”
While the use of written and audio-visual materials can answer questions and concerns voiced by patients and families, they may also need to discuss their thoughts and feelings with a facility health professional knowledgeable about transplantation. When one individual in the facility is designated as the primary source of transplant information, patients and families get consistent information. Patients should be offered the opportunity to meet with this staff member.
How are cadaveric donors chosen? What is brain death?
Hospital personnel frequently identify potential organ donors. Organ donor candidates generally have irreversible brain damage and are ventilator dependent, but have normally functioning organ systems. National laws mandate that hospital medical personnel follow “routine referral ” procedures to notify Organ Procurement Organizations (OPOs) of all imminent deaths. The OPO will discuss organ donation with the family of all patients who are donor candidates. An individual patient is declared brain dead when neurological testing shows no brain activity, and/or no recovery of brain function is possible. Brain death criteria includes the following:
• Unresponsive to any stimuli • No spontaneous movement • No spontaneous respiration • No cough to tracheal stimulation • Absence of brain stem reflexes
MARC, 2002 6

These patients might be victims of massive head trauma, such as auto accidents or gun shot wounds, but might include a patient who suffered a massive cerebral vascular accident (stroke). A physician who is not involved in the transplant process must determine brain death, and in some states, two physicians must agree on the diagnosis of brain death. Using an extensive questionnaire, OPOs review the medical history and age of these individuals, and determine whether they can be considered organ donors.
3. Who can sign a Uniform Donor Card? Can the donor or that person’s family change their mind?
Any adult may sign a Uniform Donor Card or indicate on their driver’s license that they wish to be an organ donor. The donor can withdraw his/her permission to become an organ donor at any time. If the next of kin refuses, organ donation may not take place, depending on state laws. If you want to become an organ donor when you die, you should tell family members and your primary doctor about your decision. Information on “Share Your Life, Share Your Decision” and other donor information can be viewed on the Internet at The Coalition of Donation at http://www.shareyourlife.org/, and The Washington Regional Transplant Consortium http://www.beadonor.org/.
4.
5.
6.
Is the donor screened for infectious diseases?
All donors, both cadaveric and living, are tested for infectious diseases and viruses including HIV, Hepatitis B and C, and CMV.
What are tissue typing, PRA, and crossmatching?
Tissue typing and crossmatching refer to the laboratory tests performed on donor and recipient blood samples to determine whether the two are compatible. Tissue typing determines Human Leukocyte Antigens (HLA), a form of genetic testing. The recipient’s serum is also tested for Panel Reactive Antibodies (PRA), which show whether recipients have antibodies that would cause rejection problems following transplant. The PRA test is repeated monthly after the patient is listed for a transplant; the patient should be certain samples are submitted to the transplant center by the dialysis unit or the physician’s office. When the recipient has a high PRA it is more difficult to find a compatible donor, however new medical advances are improving the outlook for these patients. The crossmatch is the final test to determine whether the donor and recipient are compatible. Recipient serum is tested against donor cells to determine whether there are antibodies that will kill donor cells. A negative crossmatch means there is no reaction, and the transplant can occur. A positive reaction means the recipient would reject the donor organ. Antibody reduction techniques such as plasmapheresis are sometimes employed in an effort to reverse positive crossmatches. If successful, then transplants between previously incompatible donors and recipients can proceed successfully.
How soon must the donated kidney be transplanted?
The sooner the better! A cadaveric kidney must be used within 48 to 72 hours (most Network 5 transplant centers transplant organs within 24 hours); longer storage times are associated with poorer initial kidney function and poorer long-term success rates. The storage time varies due to the distance between the donor and recipient centers, how long it took to find a compatible recipient, recipient preparation for surgery and the availability of operating rooms and surgeons. The most common method of kidney storage includes flushing the kidney with cold preservation solution, packing in a sterile container, and storing on ice to keep it cold. Kidneys can also be placed on a machine to pump preservation fluid through the kidney. This may extend the safe preservation period. When there is a living donor, the transplant operation takes place immediately after the donor kidney is recovered. The kidney frequently works immediately because there
MARC, 2002 7

is little or no storage or transport time (cold ischemic time) involved. This is one reason living donor transplants are more successful than non-living (cadaveric) donor transplants.
7.
8.
Who pays for the removal of donated organs?
Medicare Parts A and B cover all reasonable costs of donor evaluation and organ recovery performed in a Medicare approved hospital. If the recipient has private insurance coverage, it is important to determine what items are covered. In general, most private insurers pay all reasonable donor costs, but require that you go to a designated transplant center (perhaps one in another state), and require “pre transplant approval” before the surgery takes place.
Will the recipient ever know who donated the organ?
In 1997, a task force of major transplant organizations developed guidelines to answer this difficult question. Guidelines established the right of the recipient and the donor family to state their wishes about exchanging information. At the time of donation and when organs are received, patients and family members should be offered an opportunity to state whether they wish to give or receive information, or whether they wish to communicate with the donor family/recipient.
9. Do transplant patients have rejection symptoms?
1.
Yes, some patients will experience rejection episodes; these episodes frequently cause no symptoms that the patient can recognize and do not occur as often as they did a decade ago. The best way for a patient to avoid rejection is to take all immunosuppressive medications as prescribed, avoid taking unauthorized medications of any type, and have frequent follow-up visits with the transplant center to monitor laboratory tests that evaluate renal function, blood counts, and immunosuppressive medication levels. In order to avoid rejection, patients should promptly report any fever, signs of infection, soreness of the transplant site, or any change in urine output to the transplant center. These may be signs of serious infection or rejection. Rejection episodes, when detected promptly and properly treated, do not always result in immediate loss of the transplanted organ; however acute rejection episodes may lead to chronic rejection, where the kidney is lost over a period of months to years later. Some patients can receive a repeat kidney transplant if the previous transplant has failed, or is failing, but first transplants are generally more successful. Patients who receive living donor organs may have less rejection and may require less immunosuppressive medication. QUESTIONS ASKED ABOUT LIVING DONOR KIDNEY TRANSPLANT
Who can donate a kidney?
Anyone in good general health and over the age of eighteen (over 21 for some centers) can be an organ donor. Prospective living donors should not be obese, should be free of hypertension (high blood pressure), cancer, chronic infection, kidney disease, or heart disease. Extensive medical testing will be done by the transplant center or OPO to determine the medical eligibility of the donor. The transplant center may also request psychological evaluations to assure that the donor understands everything about donating an organ. (SEE Page 6-7 for discussion of testing prior to kidney transplant.) The donor should not be forced to donate an organ, or feel they have a right to control the recipient’s future life. They should understand the time required for evaluation, costs not covered, such as travel to the testing site, and time that will be lost from work at the time of donation. Some employers now offer paid time off to organ donors to recognize the commitment made by these individuals.
MARC, 2002 8

2.
3.
4.
1.
Will the donor have an opportunity to change his/her mind?
The donor may change their mind at any time and withdraw from consideration. Transplant centers are aware of their commitment to protect the confidentiality of the donor. If a donor changes his/her mind, it is discussed with the transplant staff, and the center may simply state that the person no longer qualifies as a donor. This prevents resentment by family members who might not understand the donor’s feelings.
What donor costs will be covered by insurance?
Medicare Part A and B will cover all reasonable cost of kidney donation when organ recovery is performed in a Medicare approved hospital. This includes the medical evaluation, donation surgery, and follow-up care for one year. Costs not covered are travel to the transplant center for evaluation, time lost from work during evaluation and donation surgery, and the cost of childcare during recuperation.
What are the health risks for the donor? How long will the donor be in the hospital?
Research studies show that kidney donation does not increase the donor’s chances of developing future health problems, including kidney failure. The death rate due to living kidney donation is extremely low. There have been three deaths in 10,000 living donor procedures (0. 03%). The living donor can lead a normal life with one kidney.
Innovations, such as Laparoscopic Donor Nephrectomy reduce post-operative pain and shorten recovery time after donation, allowing discharge within in a few days after donating a kidney, in most instances. This procedure uses multiple small incisions and microscopic surgical instruments to remove the donor kidney. The donor’s hospital stay and recovery time are shorter when compared to the traditional “open” surgery.
5. When can the donor resume normal activities?
After laparoscopic nephrectomy, the patient should not lift anything heavier than 25 pounds for approximately two weeks. Most patients can return to work within two weeks after surgery, depending on the type of work involved, and assuming recovery was un-complicated. When the traditional “open” procedure is done, the recuperation period is expected to be at least 4-6 weeks, before resuming full activity. QUESTIONS PHYSICIANS MIGHT ASK ABOUT KIDNEY TRANSPLANT
Where can I find transplant center-specific outcome data?
The United Network for Organ Sharing (UNOS) maintains a computer database of patients waiting for cadaveric transplant and records transplants done in the United States. The University Renal Research and Education Association (URREA), maintains The Scientific Registry of Transplant Recipients (SRTR), and compiles an annual Report of Center Specific Graft and Patient Survival Rates. You can visit UNOS on the Internet at http://www.unos.org/ and view patient and graft survival data at http://www.ustransplant.org/; summary transplant data is available on the Network 5 web page at http://www.esrdnet5.org/. By viewing information on these websites, you can compare transplant center performance.
2. What steps have been initiated to make more transplantable organs available?
The medical community is aware that too many patients die while waiting for a transplant. ESRD patients have a unique life sustaining system, hemodialysis or peritoneal dialysis, while waiting for a transplant. However, since life expectancy is negatively affected by the long waiting time to transplant, transplant
MARC, 2002 9

professionals have focused on increasing living donor transplants for patients who are suitable transplant candidates. Some other methods of increasing the supply of organs for transplant include:
Living Donor Exchange Registries: •
•
•
UNOS has given four OPOs permission to establish “exchange” living donor protocols. When a living donor and a recipient (such as a spouse or sibling) are incompatible, the donor and recipient are placed on a registry to identify another incompatible local donor and recipient pair with whom a “swap” could be arranged. Another option is for the incompatible living donor to donate a kidney to a patient on the cadaveric wait list. In return, their partner would gain added priority on the waiting list for a cadaveric kidney transplant. (See transplant centers *** that participate in exchange programs identified in the Transplant Center Website Address Table on page 12.) Non-Heart Beating Donors (NHBD’s): Organs for transplantation are typically recovered from donors who are brain dead and have beating hearts. Organ recovery from Non-Heart Beating Donors is now routine and successful as reported by Dr. Markus Weber, et al. in the July 2002 Net England Journal of Medicine article entitled Kidney Transplantation from Donors without a Heartbeat. Typically, these patients do not meet brain death criteria, but require ventilator support due to illness or injury. The physician and family have decided to discontinue life-support systems. Some families may then elect organ donation when approached by the OPO. Key factors in successful organ recovery from the NHBD include: cardiac arrest within 60 minutes of removing ventilator support, OPO support, and Operating Room and surgical teams on standby. When everyone is ready, the patient is transported to the operating room and removed from the ventilator. After cardiac arrest occurs, organ recovery takes place. For many families, being able to make this donation allows them to gain some solace from their tragedy. Transplant of Expanded Criteria Donor Kidneys: Research has shown that transplantation of kidneys from the ECD can be accomplished safely, although the relative risk for graft loss after a few years is increased. The ECD kidneys come from donors who may also have some impairment of kidney function, high blood pressure, and/or have suffered a cerebral vascular accident (CVA) i.e., stroke, as further explained by the UNOS Expanded Criteria Donor Kidney Policy.
Donor Age Categories Donor Condition
50-59 yrs > 60 yrs
CVA + HTN + CREATININE > 1.5 X X CVA + HTN X X CVA + Creatinine >1.5 X X HTN + Creatinine >1.5 X X CVA X HTN X Creatinine > 1.5 X None of the above X
X = Expanded Criteria Donor
Expanded Criteria Donor Kidneys are defined by donor characteristics that are associated with a 70% greater risk of kidney graft failure when compared to a reference group of non-hypertensive donors age 10-39, who did not have a CVA, and whose Creatinine was < 1.5 mg/dl. Waitlisted patients must be fully informed about the increased risk of graft failure and give informed consent before accepting
MARC, 2002 10

these ECD kidneys. Nonetheless, the ECD represents an important additional resource of transplantable kidneys for the appropriate recipient.
Plasmapheresis And Immunosuppressants Prior To Transplant To Reduce PRA Levels: •
•
Two Network 5 transplant centers are publishing results of pilot programs that use plasmapheresis and drug therapy (immunosuppression) to reduce the kidney recipients PRA level prior to cadaveric or living donor transplant. The majority of patients in these programs have stopped producing antibodies against their transplanted organ. The long-term goal of these pilot and research programs is to develop a treatment that will allow the transplantation of “NO MATCH” organs and reduce the immunosuppressant medications currently required after transplant.
Outreach Programs For African Americans To Reduce Transplant Waiting Times: African Americans were previously shown to have reduced access to kidney transplant, lower rates of kidney (graft) survival and higher rates of acute rejection. One Network 5 transplant center’s comprehensive program of patient education, efforts to increase living donations, and improve graft survival, has resulted in cutting the center kidney transplant waiting time for African Americans in half (681 days compared to the national average of 1335 days waiting). The outreach program also resulted in the reduction of non–African American patients average waiting time for a kidney transplant from 734 days to 391 days.
Please visit the Network 5 transplant center’ websites using the hyperlinks listed below to learn more about each program. (Note *** - Transplant Centers that participate in paired exchange programs.)
Transplant Centers Web site Address
DISTRICT OF COLUMBIA Children’s National Medical Center *** http://www.cnmc.org/
Georgetown University Med. Center *** http://www.georgetownuniversityhospital.org/
Howard University Hospital http://www.huhosp.org/transplant/
Washington Hospital Center *** http://www.whcenter.org/
MARYLAND
Johns Hopkins Hospital *** http://www.med.jhu.edu/transplant/
University of Maryland http://www.umm.edu/transplant/
VIRGINIA
Fairfax Hospital INOVA *** http://www.inova.org/transplant
Henrico Doctors Hospital http://www.henricodoctorshospital.com/ and http://www.virginiatransplantcenter.com/
Medical College of Virginia http://www.vcuhealth.org/transplant/
Sentara Norfolk General Hospital http://www.sentara.com/transplant/
University of Virginia Hospital http://www.hsc.virginia.edu/medcntr/specialty/transplant-center/
WEST VIRGINIA
Charleston Area Medical Center ***
http://www.camcare.com/
West Virginia University *** http://www.health.wvu.edu/
MARC, 2002 11

3. What is the status of organ allocation for kidney transplants?
The kidney allocation system is being revised presently to improve equity and shorten the preservation time, while still finding the most suitable recipient for a given kidney. When kidneys become available, the local Organ Procurement Organization enters information about the donor in the UNOS computer containing the names and demographic information on all waitlisted patients. The computer generates a list of patients that match the donor laboratory profile. If a perfectly matched recipient is identified, the kidney is offered to that individual regardless of their location in the United States. In the absence of a perfectly matched recipient, the kidney is offered to the most compatible potential recipient listed locally, then regionally, and then nationally until a recipient is identified. When a physician is notified that his patient is a possible recipient, he/she considers the patient’s status, and whether that patient is suitable for that particular donor kidney. Physicians consider the donor medical profile, the organ condition and size, the potential recipient’s recent medical status, and recipient availability for transplant. It is important that dialysis facilities and physicians maintain communication with the transplant team about changes in the potential recipient’s condition, such as infections or recent surgery that would prevent a transplant. This information can save invaluable time when organs are offered. When necessary, physicians can place wait-listed patients on inactive status until health problems are resolved, without any loss of waiting time.
4. Can I be comfortable advising my patient to consider living donor and living unrelated donor kidney transplant?
Yes, by all means! Physicians should consider living donor kidney transplant before the patient needs dialysis whenever possible! National transplant statistics indicate that patients who receive kidney transplants not only enjoy better quality of life, but frequently have longer life expectancy than dialysis patients of the same age, gender, race, etc. ESRD patients state that quality of life is important to them, and that quality is greatly improved by receiving a kidney transplant. The risk of death following living donor transplant is extremely low and the probability of good graft function exceeds 95% in most transplant centers.
5. Who will follow the recipient after kidney transplant?
Which physician provides post transplant follow-up care varies by transplant center, and by the interest/experience of the community nephrologist. Some centers return the care and follow-up to the referring nephrologist shortly after transplant, while other centers provide follow-up services to the patient indefinitely. The best option for the patient is to have both the nephrologist and transplant physicians involved as a team.
MARC, 2002 12

INFORMATION SOURCES:
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
American Nephrology Nurses Association, Core Curriculum for Nephrology Nursing, Third Edition, 1994-1995.
Humar A, et al, Living Unrelated Donors In Kidney Transplants: Better Long-Term Results Than With Non-HLA-Identical Living Related Donors? Transplantation, 69 (9): 1942-1945, 2000 May 15.
Matas AJ, et al, Immumologic And Nonimmunologic Factors: Different Risks For Cadaver And Living Donor Transplantation. Transplantation. 69 (1): 54-58, 2000 January 15.
Members of the Live Organ Donor Consensus Group, Consensus Statement on the Live Organ Donor, Journal of the American Medical Association, December 13,2000-Vol 284, No. 22
Missouri Kidney Program, University of Missouri-Columbia, Giving Your Kidney.
National Kidney Foundation of the National Capital Area, Donating Your Kidney…What’s It All About? 1995.
The National Kidney Foundation, Inc., The Organ Donor Program, O8-37, PUBLIC EDUCATION, Organ Donation Series.
The National Kidney Foundation, Inc., People Like Us, Transplantation – Choosing a Treatment That’s Right for You, A Family Focus Program.
Ojo AO, et al, Survival in Recipients of Marginal Cadaveric Donor Kidneys Compared with Other Recipients and Wail-Listed Transplant Candidates, Journal of the American Society of Nephrology 12:589-597, 2001.
Ramos, E., Aoun, S., Harmon, W. E. (2002). Expanding the Donor Pool: Effect on Graft Outcome. Journal of the American Society of Nephrology 13: 2590-2599
Transplant Recipients International Organization, Inc., Donor-Family/Recipient Communication, 1997 Conference Report.
United States Department of Health and Human Services, Health Resources and Services Administration, United Network of Organ Sharing (UNOS), 1998 Annual Report, The U.S. Scientific Registry of Transplant Recipients and The Organ Procurement and Transplantation Network.
United States Department of Health and Human Services, Health Resources and Services Administration, United Network of Organ Sharing (UNOS), Update, June 1999.
United States Department of Health and Human Services, Health Resources and Services Administration, United Network of Organ Sharing (UNOS), Update, October 2002.
United States Department of Health and Human Services, Health Resources and Services Administration, United Network of Organ Sharing (UNOS), What Every Patient Needs to Know.
United States Department of Health and Human Services, Public Health Service, National Institutes of Health, United States Renal Data System (USRDS), 2001 Annual Data Report.
United States Department of Health and Human Services, Health Resources and Services Administration (HRSA), University Renal Research and Education Association (URREA), The Scientific Registry of Transplant Recipients (SRTR), Transplant Statistics: National Reports 2001, Table 6.
University of Maryland Medical Center, The Maryland Institute for Transplantation, Laparoscopic Kidney Donation – Questions and Answers.
Weber M, et al. Kidney Transplantation from Donors without a Heartbeat. New England Journal of Medicine 2002;347:248-255.
MARC, 2002 13

MARC, 2002 14
1.
RESOURCES AVAILABLE TO PATIENTS AND STAFF:
American Association of Kidney Patients 100 S. Ashley Drive, Suite 280 Tampa, Florida 33602 800/ 749-2257 Web site: www.aakp.org
2.
American Kidney Fund 6110 Executive Boulevard, Suite 1010 Rockville, MD 20852 800/638-8299 Web site: www.akfinc.org
3. National Kidney Foundation 30 East 33 Street New York, NY 12186 800/622-9010 Web site: http://www.kidney.org/
4. Transplant Recipients International Organization 1000 16th Street, NW, Suite 602 Washington, D.C. 20036 800/TRIO-386 (800/874-6386) 202/293-0980 Web site: http://www.trioweb.org/
5. UNOS (United Network for Organ Sharing) 1100 Boulders Parkway, Suite 500 P.O. Box 13770 Richmond, Virginia 23225 804/330-8561 888 TX INFO-1 (1/888/894-6361) Web site: www.unos.org
6. The Transplant Patient Partnering Program View the Web site @ www.tppp.net, select Kidney. Bringing together the expertise of transplant doctors and coordinators with the insights of transplant recipients, the TPPP hopes to provide you with a realistic understanding of the transplant experience.
7. University Renal Research and Education Association (URREA) A not-for-profit organization founded in Ann Arbor Michigan by Philip J. Held, PhD, established for the purpose of collecting information and conducting worldwide epidemiologic, clinical, and economic studies of kidney and related diseases. General transplant-related information as well as Organ Procurement Organization (OPO) and transplant center-specific statistics can be found at www.ustransplant.org. Contact at: (734) 665-4108 (telephone), (734) 665-2103 (fax), [email protected] (email)
8. Dept. of Health and Human Services, Organ Donation Website
http://www.organdonor.gov/