Embed Size (px)
Citation preview

Infections in Organ Infections in Organ TransplantationTransplantation
Dr.Mahmud Javed HasanDr.Mahmud Javed Hasan
Nephrology Dept.Nephrology Dept.
MMCHMMCH

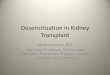
The Timeline of The Timeline of Posttransplant InfectionsPosttransplant Infections
HSV, herpes simplex virus; CMV, cytomegalovirus; HBV, hepatitis B virus; HCV, hepatitis C virus; PCP, Pneumocystis carinii pneumonia; TOXO, toxoplasmosis;EBV, Epstein-Barr virus.
Common Variables in Immune Suppression
Rejection, antirejection therapy, new agents
Neutropenia, lymphopenia
Viral coinfection (CMV, HCV, EBV)
Transplantation 4 Weeks 6-12 Months Long-term
Nosocomial Technical
From Commonto ZEBRAS
HSV, CMV, HBV, HCV, LISTERIA, PCP, TOXO
Period of most intensiveimmune suppression
Donor-derived infection
Opportunistic, Relapsed, Residual
Nosocomial infection

Use of the Timeline of Use of the Timeline of Posttransplant InfectionsPosttransplant Infections
Differential diagnosis by time posttransplantationDifferential diagnosis by time posttransplantation Excess epidemiologic hazardExcess epidemiologic hazard
Nosocomial infections:Nosocomial infections: AspergillusAspergillus, MRSA, VRE, , MRSA, VRE, clustered in time and space, by hospital, physician, clustered in time and space, by hospital, physician, clinical unitclinical unit
Community-acquired:Community-acquired: influenza and respiratory viruses, influenza and respiratory viruses, HistoplasmaHistoplasma, , CryptococcusCryptococcus
Individual:Individual: gardening, travel, work related, children gardening, travel, work related, children Excessive immune suppression in a programExcessive immune suppression in a program
Too many infections, too severe, or at the wrong Too many infections, too severe, or at the wrong time on timeline in entire cohort of patientstime on timeline in entire cohort of patients
MRSA, methicillin-resistant Staphylococcus aureus; VRE, vancomycin-resistant enterococci.

Timetable of Infection After Timetable of Infection After Transplantation: Transplantation:
First Month Following TransplantationFirst Month Following Transplantation Infection carried by donor cells or graftInfection carried by donor cells or graft Present (in recipient) prior to transplantationPresent (in recipient) prior to transplantation Technical complicationsTechnical complications
Obstructed stents, organ damage in procurementObstructed stents, organ damage in procurement Hemorrhage, hematoma, leaks, ischemiaHemorrhage, hematoma, leaks, ischemia
Postoperative complications in complex Postoperative complications in complex patientspatients Aspiration, pulmonary embolusAspiration, pulmonary embolus Lines, drains, cathetersLines, drains, catheters Clostridium difficile Clostridium difficile colitiscolitis

HBV, hepatitis B virus; HCV, hepatitis C virus; HIV, human immunodeficiency virus.Johnston L et al. Clin Infect Dis. 1999;29:819-823.
Early Posttransplant Early Posttransplant InfectionsInfections
Possible infections from the allograft include:Possible infections from the allograft include: TuberculosisTuberculosis Known pathogens (screened): HBV, HCV, HIVKnown pathogens (screened): HBV, HCV, HIV Uncommon pathogens: West Nile virus, Chagas’ disease, Uncommon pathogens: West Nile virus, Chagas’ disease,
Toxoplasma gondiiToxoplasma gondii, rabies, lymphocytic choriomeningitis , rabies, lymphocytic choriomeningitis virusvirus
Common “sticky” bacteria (may be nosocomial colonizers Common “sticky” bacteria (may be nosocomial colonizers of donor): of donor): PneumococcusPneumococcus, , StaphylococcusStaphylococcus, , StreptococcusStreptococcus, , PseudomonasPseudomonas, , SalmonellaSalmonella, , AspergillusAspergillus, , CandidaCandida

Vancomycin-Resistant Vancomycin-Resistant Enterococci Enterococci
in Transplantationin Transplantation Among highest risk Among highest risk
kidney transplant recipients,kidney transplant recipients, in neutropenic patients, and in neutropenic patients, and other critically ill patients (LVADs, dialysis, ventilators)other critically ill patients (LVADs, dialysis, ventilators)
Common bacterial pathogen after liver transplantationCommon bacterial pathogen after liver transplantation ““Predictor” of morbidity and mortality that reflects Predictor” of morbidity and mortality that reflects
overall “illness” of patientoverall “illness” of patient Up to 50% of all Up to 50% of all Enterococcus faeciumEnterococcus faecium in United States in United States
LVADs, left ventricular assist devices.

Conditions Predisposing to Early Conditions Predisposing to Early and Nosocomial Infectionand Nosocomial Infection
Exogenous immune suppressionExogenous immune suppression
Intubation (>3 days)Intubation (>3 days)
Catheters (urinary, venous, balloon pumps, dialysis, other Catheters (urinary, venous, balloon pumps, dialysis, other mucosal injuries)mucosal injuries)
Ascites, peritoneal dialysisAscites, peritoneal dialysis
Constipation, endoscopy, Constipation, endoscopy, Clostridium difficileClostridium difficile colitis colitis
Broad-spectrum antimicrobial agentsBroad-spectrum antimicrobial agents
Deep vein thrombosis, atelectasis, decubitus ulcersDeep vein thrombosis, atelectasis, decubitus ulcers
Metabolic (malnutrition/uremia/hyperglycemia)Metabolic (malnutrition/uremia/hyperglycemia)
Latent infections (viral and parasitic) Latent infections (viral and parasitic)
Colonization (bacterial and fungal)Colonization (bacterial and fungal)

Timetable of Infection After Transplantation: Timetable of Infection After Transplantation: 2 to 6 Months Following Transplantation 2 to 6 Months Following Transplantation
Classic “opportunistic infections”Classic “opportunistic infections” Pneumocystis cariniiPneumocystis carinii Toxoplasma gondiiToxoplasma gondii
Endemic pathogensEndemic pathogens Trypanosoma cruziTrypanosoma cruzi, , Strongyloides stercoralisStrongyloides stercoralis, ,
LeishmaniaLeishmania species species Geographic/endemic fungi: Geographic/endemic fungi: HistoplasmaHistoplasma, ,
CoccidioidesCoccidioides TuberculosisTuberculosis
Reactivation of latent viral infections: Reactivation of latent viral infections: CMV, EBV, HSV, VZV, HBV, HCVCMV, EBV, HSV, VZV, HBV, HCV
CMV, cytomegalovirus; EBV, Epstein-Barr virus; HSV, herpes simplex virus; CMV, cytomegalovirus; EBV, Epstein-Barr virus; HSV, herpes simplex virus; VZV, varicella-zosterVZV, varicella-zostervirus; HBV, hepatitis B virus; HCV, hepatitis C virus.virus; HBV, hepatitis B virus; HCV, hepatitis C virus.

Timetable of Infection After Transplantation: Timetable of Infection After Transplantation: >6 to 12 Months Following Transplantation >6 to 12 Months Following Transplantation
Timetable of Infection After Transplantation: Timetable of Infection After Transplantation: >6 to 12 Months Following Transplantation >6 to 12 Months Following Transplantation
Most patients are doing well—gradual Most patients are doing well—gradual decrease in immune suppressiondecrease in immune suppression
Infections are those of the communityInfections are those of the community Community-acquired pneumoniaCommunity-acquired pneumonia Influenza, RSV, Influenza, RSV, ChlamydiaChlamydia, , MycoplasmaMycoplasma Urinary tract infectionsUrinary tract infections
RSV, respiratory syncytial virus.RSV, respiratory syncytial virus.

Timetable of Infection After Transplantation: Timetable of Infection After Transplantation: >6 to 12 Months Following Transplantation >6 to 12 Months Following Transplantation
A subset with:A subset with: Chronic viral infectionChronic viral infection
CMV (now uncommon)CMV (now uncommon) HCV (very common) HCV (very common) HBV (some viral resistance and relapse)HBV (some viral resistance and relapse) EBV (PTLD)EBV (PTLD) Papillomavirus (warts, anogenital and squamous cell Papillomavirus (warts, anogenital and squamous cell
cancers)cancers) BK virus nephropathyBK virus nephropathy
Recurrent bacterial infections (lungs)Recurrent bacterial infections (lungs)
Chronic anastamotic issues Chronic anastamotic issues
Recurrent Recurrent Clostridium difficile Clostridium difficile colitiscolitis
CMV, cytomegalovirus; HCV, hepatitis C virus; HBV, hepatitis B virus; EBV, Epstein-Barr virus; PTLD, posttransplant lymphoproliferative disorder.

Timetable of Infection After Timetable of Infection After Transplantation: Transplantation:
>6 to 12 Months Following >6 to 12 Months Following Transplantation Transplantation
Chronic “ne’er do wells” with poor allograft function Chronic “ne’er do wells” with poor allograft function and higher levels of immune suppression in an and higher levels of immune suppression in an attempt to preserve graft function attempt to preserve graft function
At highest risk for recurrent opportunistic infections At highest risk for recurrent opportunistic infections including including Nocardia asteroides, CryptococcusNocardia asteroides, Cryptococcus, and , and fungal infectionsfungal infections
Benefit from extended prophylaxis Benefit from extended prophylaxis

InfectionInfection
TypesTypes BacterialBacterial FungalFungal ViralViral ParasiticParasitic
27

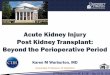
Copyright ©2008 American Society of Nephrology
Weikert, B. C. et al. Clin J Am Soc Nephrol 2008;3:S76-S86
Figure 1. Time of presentation of common viral illnesses post-transplant

InfectionInfection
ProphylaxisProphylaxis Time table of occurrenceTime table of occurrence Evaluation of feverEvaluation of fever
28

29

Classification of Classification of InfectionsInfections
Donor-derivedDonor-derived
Recipient-derivedRecipient-derived
NosocomialNosocomial
Community-acquiredCommunity-acquired

Donor-derived InfectionDonor-derived Infection Most are latentMost are latent
CMV, TB, T.cruziCMV, TB, T.cruzi
Rarely can be acuteRarely can be acute Bacteremia/viremia at time of procurementBacteremia/viremia at time of procurement West Nile, rabies, HIV, hepatitis, LCVWest Nile, rabies, HIV, hepatitis, LCV
The majority of these are sub-clinical in The majority of these are sub-clinical in healthy patients, but can be catastrophic when healthy patients, but can be catastrophic when transplanted into an immunosuppresed patienttransplanted into an immunosuppresed patient
At present, routine evaluations of donors for At present, routine evaluations of donors for infectious diseases relies upon serologic infectious diseases relies upon serologic antibody testing, and thus sensitivity is not antibody testing, and thus sensitivity is not 100% for those that may not have had time to 100% for those that may not have had time to seroconvert seroconvert

Donor-derivedDonor-derived Transplantation of organs from deceased donors Transplantation of organs from deceased donors
with viral syndromes is controversialwith viral syndromes is controversial
Livers with known Chagas or Hep B infection may Livers with known Chagas or Hep B infection may be used as there are effective treatments for these be used as there are effective treatments for these infectionsinfections
Hep C infected organs are sometimes transplanted Hep C infected organs are sometimes transplanted into Hep C(+) donorsinto Hep C(+) donors

Fishman J. N Engl J Med 2007;357:2601-2614

Recipient-derived Recipient-derived InfectionsInfections
Infections that can be treated or controlled Infections that can be treated or controlled do not necessarily preclude transplantationdo not necessarily preclude transplantation
Most commonly screened for:Most commonly screened for: TBTB syphilissyphilis Viral: CMV, EBV, VZV, HSV, HIV, HBV, HCVViral: CMV, EBV, VZV, HSV, HIV, HBV, HCV
Other things to think ofOther things to think of T.cruzi, strongyloides, cryptococcusT.cruzi, strongyloides, cryptococcus Endemic fungi: histoplasma, coccidioides, Endemic fungi: histoplasma, coccidioides,
paracoccidioides, aspergillus, blastomycosis paracoccidioides, aspergillus, blastomycosis

Fishman J. N Engl J Med 2007;357:2601-2614

ImmunizationsImmunizations Pt’s should be current on the following vaccinesPt’s should be current on the following vaccines
MMRMMR HBVHBV InfluenzaInfluenza Strep pneumoniaeStrep pneumoniae TetanusTetanus DiphtheriaDiphtheria PertussisPertussis PolioPolio VZV – if never infectedVZV – if never infected
Consideration should be given to boosters for any of the Consideration should be given to boosters for any of the above prior to transplantation as live vaccines are above prior to transplantation as live vaccines are generally contraindicated post-transplant, and generally contraindicated post-transplant, and immunologic memory will become impairedimmunologic memory will become impaired

Nosocomial InfectionsNosocomial Infections MRSAMRSA VREVRE fluconazole-resistant Candida speciesfluconazole-resistant Candida species
associated with surgical site and indwelling cathetersassociated with surgical site and indwelling catheters C.diffC.diff Resistant gram-negative bacilliResistant gram-negative bacilli Aspergillus Aspergillus

Community InfectionsCommunity Infections
AspergillusAspergillus NocardiaNocardia Cryptococcus neoformans (birds)Cryptococcus neoformans (birds) Respiratory virusesRespiratory viruses
Secondary bacterial superinfectionSecondary bacterial superinfection

Monitoring Monitoring ImmunosuppressionImmunosuppression
There are no specific tests currently There are no specific tests currently available to determine the overall available to determine the overall susceptibility of patients to infection…susceptibility of patients to infection…
……but they are on the horizonbut they are on the horizon
Currently, the known determinants Currently, the known determinants contributing to the overall risk of infection contributing to the overall risk of infection are the dose, duration, and sequence of are the dose, duration, and sequence of immunosuppressive therapiesimmunosuppressive therapies

Fishman J. N Engl J Med 2007;357:2601-2614
Changing Timeline of Infection after Organ Transplantation

Early post-transplant Early post-transplant period (30d)period (30d)
Opportunistic infections are rare in the first month Opportunistic infections are rare in the first month post-transplantpost-transplant
>1 month of medical therapy is required to >1 month of medical therapy is required to effectively deplete cell-mediated therapyeffectively deplete cell-mediated therapy
One exception is large, prolonged doses of One exception is large, prolonged doses of corticosteroidscorticosteroids
Infections are generally donor-derived or associated Infections are generally donor-derived or associated with complications from the surgery itselfwith complications from the surgery itself


Intermediate period (1-Intermediate period (1-6mos)6mos)
Viral infections and allograft rejection account for Viral infections and allograft rejection account for the majority of febrile episodesthe majority of febrile episodes
Adherence to Bactrim and antiviral prophylaxis Adherence to Bactrim and antiviral prophylaxis renders infections such as PCP, UTI’s, listeria, renders infections such as PCP, UTI’s, listeria, toxoplasmosis, and herpes very unlikelytoxoplasmosis, and herpes very unlikely
Fungi, cryptococcus, T.cruzi, strongyloides can Fungi, cryptococcus, T.cruzi, strongyloides can surfacesurface
Other: polyoma virus (BK and JC), recurrent HCVOther: polyoma virus (BK and JC), recurrent HCV


Late post-transplant period Late post-transplant period (>6mos)(>6mos)
Risk wanes as immunosuppressive therapy is taperedRisk wanes as immunosuppressive therapy is tapered
Risk profile however, is “reset” with each episode of Risk profile however, is “reset” with each episode of acute rejectionacute rejection
Chronic viral infections can cause allograft injuryChronic viral infections can cause allograft injury HCV HCV cirrhosis cirrhosis BOOP in lungsBOOP in lungs CMV CMV coronary vasculopathy coronary vasculopathy PTLDPTLD Skin/anogenital cancersSkin/anogenital cancers
Fungi/molds, virusesn and “typical” bugs still remain Fungi/molds, virusesn and “typical” bugs still remain on radaron radar


Viral Infection after Renal Viral Infection after Renal Transplantation: Transplantation: Surveillance and Surveillance and
ManagementManagement

CMV and Solid Organ TransplantationCMV and Solid Organ Transplantation
• CMV is still among the most important CMV is still among the most important infectious complications after transplantinfectious complications after transplant
• In the absence of prophylaxis, CMV In the absence of prophylaxis, CMV reactivation can occur in over 75% of solid reactivation can occur in over 75% of solid organ transplant recipients depending on organ transplant recipients depending on other risk factorsother risk factors(1)(1)
• Once CMV infection is established, then its Once CMV infection is established, then its replication is highly dynamic with rapid replication is highly dynamic with rapid increases in viral loadincreases in viral load
CMV infection may lead to tissue invasive CMV infection may lead to tissue invasive diseasedisease
34
1. Fishman JA, Rubin RH. Infection in organ-transplant recipients. N Engl J Med. 1998;338:1741.

CMV Infection and Renal CMV Infection and Renal TransplantationTransplantation
Dr. Md. Shahidul Islam (Selim)Dr. Md. Shahidul Islam (Selim)MD, FACPMD, FACP
Department of NephrologyDepartment of NephrologyBSMMU, DhakaBSMMU, Dhaka..

IntroductionIntroduction CMV infection is a major cause of CMV infection is a major cause of
morbidity and mortality after solid organ morbidity and mortality after solid organ Tx.Tx.
It is widely distributed in general It is widely distributed in general population ranging from 30-70%population ranging from 30-70%
It usually develops during the first few It usually develops during the first few months of Tx. when patient on months of Tx. when patient on immunosuppressed. immunosuppressed.
It has also been implicated as a cause of It has also been implicated as a cause of acute and chronic allograft injury.acute and chronic allograft injury.
CMV may play a crucial role in chronic CMV may play a crucial role in chronic graft vasculopathy resulting CAN, graft vasculopathy resulting CAN, bronchiolitis and accelerated CAD.bronchiolitis and accelerated CAD.

CMV Infection: Risk Categories in CMV Infection: Risk Categories in Solid Organ Transplant RecipientsSolid Organ Transplant Recipients
Risk CategoryRisk Category Donor (D) or Recipient (R)Donor (D) or Recipient (R)Seropositivity (+/-)Seropositivity (+/-)
High High D+/R-D+/R-
Intermediate*Intermediate* D+/R+, D-/R+D+/R+, D-/R+
LowLow D-/R-D-/R-
37
* D+/R+ generally at higher risk than D-/R+
Fishman JA, Emery V, Freeman R, et al. Cytomegalovirus in transplantation – challenging the status quo. Clinical Transplantation. 2007;21:149-158.

CMV PathogenesisCMV Pathogenesis
• Viral factorsViral factors– replication dynamicsreplication dynamics– immune evasionimmune evasion– viral heterogeneityviral heterogeneity– viral co-infectionsviral co-infections
• Host factorsHost factors– CD4+, CD8+ T-cellCD4+, CD8+ T-cell– NK cell, B-cell NK cell, B-cell – exogenous exogenous
immunosuppression immunosuppression – D/R immune statusD/R immune status
38

INFLAMMATION(CYTOKINES, NF-B)
LATENTLATENT CMV INFECTIONCMV INFECTION
ANTILYMPHOCYTEANTILYMPHOCYTEANTIBODIESANTIBODIES
OTHER OTHER HERPES VIRUSESHERPES VIRUSES
SEPSIS/SEPSIS/SURGERYSURGERYREJECTIONREJECTION
39

CMV INFECTIONCMV INFECTION CMV DISEASECMV DISEASE
IncreasingIncreasingviral loadviral load
40
Co-Infection
Factors contributingto risk for infection:• Viral factors• Immunosuppression• Co-infection

CMV InfectionCMV Infection
Latent CMV infection
Active CMV infection(viral replication)
Direct effects
Indirect effects
41

Direct Effects of CMV InfectionDirect Effects of CMV Infection
CMV Viral SyndromeCMV Viral Syndrome• Fever, malaise, myalgiasFever, malaise, myalgias• Leukopenia, Leukopenia,
thrombocytopenia, and thrombocytopenia, and other laboratory other laboratory abnormalitiesabnormalities
Tissue Invasive Tissue Invasive DiseaseDisease
• HepatitisHepatitis• PneumonitisPneumonitis• ColitisColitis• CarditisCarditis• Nephritis Nephritis • PancreatitisPancreatitis• RetinitisRetinitis
Direct Effects
42

Indirect Effects of CMV InfectionIndirect Effects of CMV Infection
Altered host immune Altered host immune responseresponse
• Graft rejection; graft dysfunctionGraft rejection; graft dysfunction
• Opportunistic infections: Bacterial fungal Opportunistic infections: Bacterial fungal superinfectionsuperinfection
• Decreased graft and patient survivalDecreased graft and patient survival
• Herpesvirus interactions: EBV/PTLDHerpesvirus interactions: EBV/PTLD
Indirect Effects
43

CMV HepatitisCMV Hepatitis
44

Anti-CMV TherapyAnti-CMV Therapy
ValganciclovirValganciclovir:: (Valcyte®) a prodrug form of ganciclovir (Valcyte®) a prodrug form of ganciclovir with improved oral bioavailabilitywith improved oral bioavailability
FoscarnetFoscarnet: : (Foscavir(Foscavir) is an inhibitor CMV DNA polymerase ) is an inhibitor CMV DNA polymerase (UL54)(UL54)‒ Useful for ganciclovir resistant CMVUseful for ganciclovir resistant CMV
‒ Major limitation is nephrotoxicityMajor limitation is nephrotoxicity
CidofovirCidofovir: : (Vistide(Vistide) inhibits viral DNA polymerase) inhibits viral DNA polymerase‒ May be useful for ganciclovir resistant CMV but not well studied in May be useful for ganciclovir resistant CMV but not well studied in
organ transplant recipients organ transplant recipients
MaribavirMaribavir: : is an investigational agent that prevents viral is an investigational agent that prevents viral encapsidation and nuclear egress encapsidation and nuclear egress
GanciclovirGanciclovir: : (Cytovene® and Cymevene®) is a synthetic (Cytovene® and Cymevene®) is a synthetic analogue of analogue of 2-deoxyguanosine, that competitively inhibits the incorporation 2-deoxyguanosine, that competitively inhibits the incorporation of dGTP by viral DNA polymerase–intravenous or oralof dGTP by viral DNA polymerase–intravenous or oral
45

GanciclovirGanciclovir Adverse effectsAdverse effects: :
– Hematologic: neutropenia, anemia, thrombocytopeniaHematologic: neutropenia, anemia, thrombocytopenia– Gastrointestinal: nausea, vomiting, diarrhea, abdominal pain, Gastrointestinal: nausea, vomiting, diarrhea, abdominal pain,
flatulence, anorexia flatulence, anorexia – Neurologic: headache, confusion, hallucination, seizuresNeurologic: headache, confusion, hallucination, seizures– Other: pain and phlebitis at injection site (due to high pH), Other: pain and phlebitis at injection site (due to high pH),
sweating, rash, itch, increased serum creatinine and blood urea sweating, rash, itch, increased serum creatinine and blood urea concentrationsconcentrations
ToxicityToxicity: : – Human carcinogen, teratogen, and mutagenHuman carcinogen, teratogen, and mutagen– Inhibits spermatogenesisInhibits spermatogenesis
PharmacokineticsPharmacokinetics::– Oral ganciclovir: poor absorption – (~ 5% fasting and ~ 8% with Oral ganciclovir: poor absorption – (~ 5% fasting and ~ 8% with
food)food)– 90% of plasma ganciclovir is eliminated unchanged in the urine with 90% of plasma ganciclovir is eliminated unchanged in the urine with
a half-life of 2-6 hrs, depending on renal function (elimination takes a half-life of 2-6 hrs, depending on renal function (elimination takes over 24 hours in end-stage renal disease)over 24 hours in end-stage renal disease)
46

ValganciclovirValganciclovir
Adverse effectsAdverse effects: : – Similar to ganciclovirSimilar to ganciclovir
– Myelosuppression is one of the main side effects that may limit Myelosuppression is one of the main side effects that may limit prolonged use of valganciclovirprolonged use of valganciclovir
PharmacokineticsPharmacokinetics::– Oral bioavailability ~ 60%Oral bioavailability ~ 60%
• Fatty foods significantly increase the bioavailabilityFatty foods significantly increase the bioavailability
– Eliminated as ganciclovir in the urine, with a half-life of about Eliminated as ganciclovir in the urine, with a half-life of about 4 hours4 hours
47

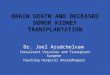
CMV PreventionCMV Prevention
• Pre-emptive Pre-emptive – Guided by laboratory monitoring for evidence of Guided by laboratory monitoring for evidence of
early viral replication; treatment is started when early viral replication; treatment is started when CMV viral load or antigenemia reaches a certain CMV viral load or antigenemia reaches a certain thresholdthreshold
• Universal prophylaxisUniversal prophylaxis– Therapy from the time of transplant to all patientsTherapy from the time of transplant to all patients
or a subgroup of patients at risk for CMV diseaseor a subgroup of patients at risk for CMV disease
48

++ ++ ++ ++ ++ ____ ++ ++ __
00 44 88 12weeks
Initiate pre-emptive therapy to prevent CMV disease
CMV disease
TESTTEST
Pre-emptive TherapyPre-emptive Therapy
____
49

Pre-emptive TherapyPre-emptive Therapy
• AdvantagesAdvantages::– Minimizes drug exposure Minimizes drug exposure
– This may potentially decrease toxicity and costsThis may potentially decrease toxicity and costs
– Theoretically lower risk of resistanceTheoretically lower risk of resistance
– Less late-onset disease: may allow development of Less late-onset disease: may allow development of cell-mediated immune responsecell-mediated immune response
• DisadvantagesDisadvantages::– Logistically more difficult to coordinateLogistically more difficult to coordinate
– May be unsuccessful in preventing progression to active May be unsuccessful in preventing progression to active disease in high-risk patients due to rapid doubling timedisease in high-risk patients due to rapid doubling time
– May not eliminate the indirect effects of CMVMay not eliminate the indirect effects of CMV
50

Late Onset CMV Disease DefinitionLate Onset CMV Disease Definition
• CMV disease occurring > 3 months post CMV disease occurring > 3 months post transplanttransplant
• May be primary infection (D+/R-) or May be primary infection (D+/R-) or recurrence (R+)recurrence (R+)
• In epidemiology studies associated with In epidemiology studies associated with significant morbidity (including graft significant morbidity (including graft dysfunction) and occasional mortality dysfunction) and occasional mortality (indirect effects)(indirect effects)(1)(1)
• Incidence 3%-17%; In IMPACT study Incidence 3%-17%; In IMPACT study 37% with 3 months of prophylaxis in 37% with 3 months of prophylaxis in D+/R-D+/R-
51 Limaye, AP, et al. Transplantation. 2004;78(9):1390-1396.

CMV Prophylaxis: Late-Onset DiseaseCMV Prophylaxis: Late-Onset Disease
Prophylaxis period
Patie
nts
With
No
CMV
Dis
ease
(%)
0
10
20
30
40
50
60
70
80
90
100
Time (days)0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150 160 170 180 190 200
364 D+/R- SOT patients
Ganciclovir (oral)
Valganciclovir
Paya, et al. Am J Transplant. 2004;4:611-620.52

Late Onset CMV Disease in High-Late Onset CMV Disease in High-Risk GroupsRisk Groups
• CMV D+/R- individualsCMV D+/R- individuals(1)(1)
• CMV R+ on potent CMV R+ on potent immunosuppression; anti-lymphocyte immunosuppression; anti-lymphocyte therapytherapy
• Therapy of acute rejectionTherapy of acute rejection• Lung transplant highest risk; kidney, Lung transplant highest risk; kidney,
liver lower riskliver lower risk
1. Limaye AP, et al. Transplantation. 2004;78:1390-1396.53

Importance of CMV InfectionImportance of CMV Infection
Infectious disease syndrome (fever, Infectious disease syndrome (fever, pneumonia, hepatitis, retinitis. pneumonia, hepatitis, retinitis.
Increased additional opportunistic Increased additional opportunistic infections.infections.
Acute and chronic graft injury.Acute and chronic graft injury. Tx. recipients are high-risk of CMV Tx. recipients are high-risk of CMV
disease.disease. Ganciclovir is the antiviral Ganciclovir is the antiviral
chemotherapy use in both therapeutic chemotherapy use in both therapeutic and prophylaxis against CMV.and prophylaxis against CMV.

Risk factors of CMV diseaseRisk factors of CMV disease Risk of CMV disease is height in Risk of CMV disease is height in
D+ve/R-ve solid organ Tx. recipient D+ve/R-ve solid organ Tx. recipient who are lack of cellular and humoral who are lack of cellular and humoral immunity. immunity.
Other risk factors one recipient over Other risk factors one recipient over all state of immunosuppression (drugs, all state of immunosuppression (drugs, dose, duration) & various host factors dose, duration) & various host factors (age, comorbidity, neutropenia)(age, comorbidity, neutropenia)
Induction therapy.Induction therapy. Lowest risk of CMV disease in R-ve /D -Lowest risk of CMV disease in R-ve /D -
ve setting.ve setting.

Laboratory diagnosisLaboratory diagnosis Serologic assays (CMV IgA & IgM) Serologic assays (CMV IgA & IgM)
are useful for delineating risk at are useful for delineating risk at the time of Tx.the time of Tx.
New era for CMV diagnosis by the New era for CMV diagnosis by the PP65 antigenemia assay. This test PP65 antigenemia assay. This test is heigher sensitive and specific.is heigher sensitive and specific.
CMV PCR assays.CMV PCR assays. Molicular diagnostic test by CMV- Molicular diagnostic test by CMV-
DNA or RNA.DNA or RNA.

Clinical Presentation of CMV Clinical Presentation of CMV DiseaseDisease
Asymptomatic / Prolong irregular Asymptomatic / Prolong irregular fever.fever.
Multi organ involvement features Multi organ involvement features like RTI, Hepatobiliary and CNS like RTI, Hepatobiliary and CNS are importantare important. .

PreventionPrevention
Two strategies are commonly used for CMV Two strategies are commonly used for CMV prevention:prevention:
Universal prophylaxisUniversal prophylaxis Preemptive therapy.Preemptive therapy. In universal prophylaxis involves antiviral In universal prophylaxis involves antiviral
therapy to all at risk patients beginning at therapy to all at risk patients beginning at or immediate post Tx. for a defined time or immediate post Tx. for a defined time period.period.
In preemptive therapy, patients are In preemptive therapy, patients are monitored at regular intervals for early monitored at regular intervals for early evidence of CMV replications by laboratory evidence of CMV replications by laboratory assess and initiate antiviral therapy.assess and initiate antiviral therapy.

Universal prophylaxisUniversal prophylaxisAcyclovir, ganciclovir, valacyclovir, valgancilovir and Acyclovir, ganciclovir, valacyclovir, valgancilovir and
immune- globulin. immune- globulin.
Acyclovir: Acyclovir: Possesses comparatively poor vitro activity Possesses comparatively poor vitro activity against CMV at clinically achievable levels.against CMV at clinically achievable levels.
Ganciclovir:Ganciclovir: Both I/V & oral preparations are available.Both I/V & oral preparations are available. 5-10 mg/kg/d in two divided dose for 4-6 weeks for 5-10 mg/kg/d in two divided dose for 4-6 weeks for
treatment and 2-4 weeks for prophylaxis in normal treatment and 2-4 weeks for prophylaxis in normal renal function.renal function.
Use in D+ & R-ve patients immediate after Tx.Use in D+ & R-ve patients immediate after Tx. Oral ganciclovir achieve significantly lower serum Oral ganciclovir achieve significantly lower serum
level in compared with I/V ganciclovir (dose 1000 mg level in compared with I/V ganciclovir (dose 1000 mg tds for 3 m.)tds for 3 m.)
Valacyclovir:Valacyclovir: (1) Oral 8 gm per day for 3 months(1) Oral 8 gm per day for 3 months
(2) Less effective than gancyclovir.(2) Less effective than gancyclovir.

Polyvalint I/V ImmunoglobulinPolyvalint I/V Immunoglobulin
The efficacy of I/V Ig in solid organ Tx. The efficacy of I/V Ig in solid organ Tx. has been investigated.has been investigated.

Guidelines for CMV prevention Guidelines for CMV prevention in SOT recipients.in SOT recipients.
Organ/group:Organ/group: Recommendations:Recommendations:
* * Kidney, liver, pancreas,Kidney, liver, pancreas, * Oral ganciclovir* Oral ganciclovir
heart. D+ve/R-ve. heart. D+ve/R-ve. for 3 months/IV for 3 months/IV ganciclovir 1-3 M. ganciclovir 1-3 M.
*Kidney, liver , pancreas,*Kidney, liver , pancreas, * As above.* As above.
heart. R+ve.heart. R+ve.
Start prophylaxis within 10 days post Tx. And Start prophylaxis within 10 days post Tx. And continue for 3 months.continue for 3 months.

BK virus-associated BK virus-associated nephropathynephropathy

BK virus-associated BK virus-associated nephropathynephropathy
Double-stranded DNA polyoma virusDouble-stranded DNA polyoma virus JC JC → PML→ PML SV40 → renal disease in immunodeficient SV40 → renal disease in immunodeficient
monkeysmonkeys 1971: BK virus first isolated from a kidney 1971: BK virus first isolated from a kidney
transplant recipient with ureteral stricturetransplant recipient with ureteral stricture 11stst reported case of nephropathy in 1993 reported case of nephropathy in 1993
(Pitt), graft failure in 3 months*(Pitt), graft failure in 3 months* Affects ~8% of renal transplant recipientsAffects ~8% of renal transplant recipients 30-60% of affected allografts fail of 30-60% of affected allografts fail of
BKVAN within 1 yearBKVAN within 1 year
* Purighalla R, et al. Am J Kid Dis 1995.

EpidemiologyEpidemiology Estimated that 80-90% of adult population Estimated that 80-90% of adult population
has been exposed to BK virus has been exposed to BK virus Probably multiple routes of transmission, Probably multiple routes of transmission,
but respiratory secretions predominatebut respiratory secretions predominate Primary infection may be asymptomatic, Primary infection may be asymptomatic,
mild URI, cystitis…mild URI, cystitis… Enters latent phase, in urogenital tract, Enters latent phase, in urogenital tract,
lymphoid tissue, brainlymphoid tissue, brain

PathogenesisPathogenesis
BK replication (viruria) occurs during BK replication (viruria) occurs during states of immune suppressionstates of immune suppression PregnancyPregnancy MalignancyMalignancy HIVHIV DiabetesDiabetes TransplantationTransplantation
Viremia (13-20%) & nephropathy (5-8%) Viremia (13-20%) & nephropathy (5-8%) are unique to the post-kidney transplant are unique to the post-kidney transplant settingsetting

Clinical manifestationsClinical manifestations
Risk factors:Risk factors: Older, male, White, diabetic recipientOlder, male, White, diabetic recipient More HLA mm, ACR, DGFMore HLA mm, ACR, DGF Net state of immune suppressionNet state of immune suppression
Asymptomatic allograft dysfunctionAsymptomatic allograft dysfunction Suspect BK when rejection does not Suspect BK when rejection does not
resolve with usual therapyresolve with usual therapy

DiagnosisDiagnosis
Viruria precedes viremia and Viruria precedes viremia and nephropathynephropathy Urine cytologyUrine cytology Urine PCRUrine PCR
Viremia Viremia More specific for nephropathyMore specific for nephropathy
Screening protocols increasingly usedScreening protocols increasingly used Renal biopsy is gold standardRenal biopsy is gold standard

www.kidneypathology.com
BK nephritisBK nephritis
Variable degree of Variable degree of interstitial interstitial inflammation, inflammation, fibrosis, atrophyfibrosis, atrophy
Nuclear inclusionsNuclear inclusions Similar in Similar in
appearance to appearance to cellular rejectioncellular rejection
ImmunohistochemisImmunohistochemistry usefultry useful

TreatmentTreatment
Reduce immune suppressionReduce immune suppression Stop antiproliferativeStop antiproliferative Stop steroidsStop steroids Cut CNI and antiproliferative doses by Cut CNI and antiproliferative doses by
50%50% Noteworthy that all other treatments Noteworthy that all other treatments
for BKVAN include reducing IS…for BKVAN include reducing IS… CidofovirCidofovir LeflunomideLeflunomide

Herpes Simplex Virus and Herpes Simplex Virus and Varicella Zoster Virus Varicella Zoster Virus

Herpes simplex (HSV) and Varicella Herpes simplex (HSV) and Varicella zoster (VZV) are both alpha herpes zoster (VZV) are both alpha herpes viruses with a double stranded DNA viruses with a double stranded DNA core.core.
Seroprevalence for HSV-1 in the Seroprevalence for HSV-1 in the adult population is as high as 60 adult population is as high as 60 percent, while VZV rates can be as percent, while VZV rates can be as high as 90 percent high as 90 percent

Infection in the renal transplant Infection in the renal transplant patient is usually caused by patient is usually caused by reactivation of latent virus.reactivation of latent virus.
HSV infection usually presents with HSV infection usually presents with oral or genital lesions, but in some oral or genital lesions, but in some instances can cause instances can cause esophagitis,hepatitis, encephalitis or esophagitis,hepatitis, encephalitis or pneumonitis pneumonitis

ZV reactivation usually presents as ZV reactivation usually presents as dermatomal zoster, but can dermatomal zoster, but can disseminate, causing similar visceral disseminate, causing similar visceral complications. complications.
In the absence of prophylaxis, HSV and VZV In the absence of prophylaxis, HSV and VZV may be seen early with HSV observed even in may be seen early with HSV observed even in the first post transplant month and VZV as the first post transplant month and VZV as early as 1 to 6 mo post transplant early as 1 to 6 mo post transplant
The incidence of HSV in renal The incidence of HSV in renal transplant recipients is estimated to be transplant recipients is estimated to be approximately 53% and VZV 4 to 12% approximately 53% and VZV 4 to 12%

Diagnosis Diagnosis Direct fluorescence antibody for HSV and VZV from Direct fluorescence antibody for HSV and VZV from
vesicular lesions or vesicular lesions or PCR from CSF or visceral tissue samples. PCR from CSF or visceral tissue samples.
Due to high seroprevalence in the adult Due to high seroprevalence in the adult population, serologies are rarely helpful in the population, serologies are rarely helpful in the setting of active infection.setting of active infection.
Treatment Treatment Disseminated infections involves intravenous acyclovir, Disseminated infections involves intravenous acyclovir, Less severe infection ; oral acyclovir, valacyclovir, or Less severe infection ; oral acyclovir, valacyclovir, or
famciclovir famciclovir Acyclovir resistance has been rarely reported in some Acyclovir resistance has been rarely reported in some
strains; foscarnet, cidofovir, and topical trifluridine may be strains; foscarnet, cidofovir, and topical trifluridine may be considered for treatment ofresistant virus, although careful considered for treatment ofresistant virus, although careful monitoring of renal function is required monitoring of renal function is required

Epstein Barr Virus Epstein Barr Virus

Epstein Barr Virus (EBV) is a gamma herpes Epstein Barr Virus (EBV) is a gamma herpes virus with a double stranded DNA core; virus with a double stranded DNA core; similar to other herpesviruses,similar to other herpesviruses,
EBV remains latent in lymphocytes following EBV remains latent in lymphocytes following primary infection. primary infection.
EBV can cause replication and clonal EBV can cause replication and clonal expansion of the B cells that serve as its expansion of the B cells that serve as its primary reservoir and other cell lines as well. primary reservoir and other cell lines as well.
However, a competent immune system, However, a competent immune system, specifically T cell response, prevents these specifically T cell response, prevents these cells from propagating. cells from propagating.
When T cell function is impaired, as is the When T cell function is impaired, as is the case in renal transplant patients, this case in renal transplant patients, this surveillance system can fail and post surveillance system can fail and post transplant lymphoproliferative transplant lymphoproliferative disorder (PTLD)disorder (PTLD) can develop can develop

Risk of development of PTLD,Risk of development of PTLD, with higher incidence rates observed in with higher incidence rates observed in
patients receiving cytolytic therapies,patients receiving cytolytic therapies, including antithymocyte globulin andincluding antithymocyte globulin and OKT3 OKT3
PTLD most commonly occurs in the first year post transplant

Serologies for EBVSerologies for EBV Serologies for EBV of both donor and recipient should be Serologies for EBV of both donor and recipient should be
obtained before transplant. obtained before transplant. Allograft recipients who are EBV negative before Allograft recipients who are EBV negative before
transplant and receive an organ from a seropositive transplant and receive an organ from a seropositive donor are at greatest risk for PTLD; donor are at greatest risk for PTLD;
consequently it is most commonly seen in pediatric and consequently it is most commonly seen in pediatric and young adult populations.young adult populations.
Currently there is no single standard strategy to prevent Currently there is no single standard strategy to prevent PTLD. PTLD.
In some centers, high-risk individuals are screened In some centers, high-risk individuals are screened regularly for the presence of EBV viremia and regularly for the presence of EBV viremia and immunosuppression decreased when viremia is observed.immunosuppression decreased when viremia is observed.
Effective prevention of CMV may also prevent Effective prevention of CMV may also prevent EBVinfections, primarily by limiting the impact of CMV on EBVinfections, primarily by limiting the impact of CMV on immune regulationimmune regulation
A recent trial demonstrated that CMV Ig did not prevent A recent trial demonstrated that CMV Ig did not prevent the onset of PTLD in high risk recipients the onset of PTLD in high risk recipients

Definitive diagnosis of PTLD requires Definitive diagnosis of PTLD requires histopathologic confirmation, histopathologic confirmation,
preferably of tissue obtained by excisional biopsy.preferably of tissue obtained by excisional biopsy. In the case of CNS PTLD, analysis of CSF for EBV In the case of CNS PTLD, analysis of CSF for EBV
PCR and cytology should be performed. PCR and cytology should be performed. Although viremia may be noted at the time of PTLD, Although viremia may be noted at the time of PTLD,
its detection cannot be used to confirm or refute the its detection cannot be used to confirm or refute the diagnosis. diagnosis.
Staging is performed by histologic type Staging is performed by histologic type (monoclonal (monoclonal versusversus polyclonal, T cell polyclonal, T cell versusversus B cell) B cell) and location (allograft, other organ, metastasis).and location (allograft, other organ, metastasis).
Often the Ann Arbor classification, used for other Often the Ann Arbor classification, used for other non-Hodgkin lymphomas, is utilized non-Hodgkin lymphomas, is utilized

Human Herpesvirus-6, Human Herpesvirus-6, Human Herpesvirus-7, and Human Herpesvirus-7, and
Human Herpesvirus-8 Human Herpesvirus-8

Human Herpes Virus 8 (HHV8) is a Human Herpes Virus 8 (HHV8) is a gamma herpes virus that has been gamma herpes virus that has been associated with Kaposi's Sarcoma, associated with Kaposi's Sarcoma, primary effusive lymphoma, and primary effusive lymphoma, and Multicentric Castleman's Disease Multicentric Castleman's Disease (lymphoproliferative disorder) (lymphoproliferative disorder)

Hepatitis B and C Hepatitis B and C

Patients with chronic renal failure, Patients with chronic renal failure, notably those receiving hemodialysis, notably those receiving hemodialysis, may be at increased risk for Hepatitis B. may be at increased risk for Hepatitis B.
Consequently all nonimmune patients Consequently all nonimmune patients with chronic renal failure should with chronic renal failure should be vaccinated with Hepatitis B vaccine be vaccinated with Hepatitis B vaccine and immunity verified with Hepatitis B and immunity verified with Hepatitis B surface antibody screening following surface antibody screening following completion of the vaccination series completion of the vaccination series

West Nile Virus West Nile Virus West Nile Virus is a flavivurus that causes a West Nile Virus is a flavivurus that causes a
febrile illness, associated with encephalitis, and febrile illness, associated with encephalitis, and can be fatal can be fatal
To prevent infection, seasonal screening should To prevent infection, seasonal screening should be considered for donors before transplant by be considered for donors before transplant by serologic and/or nucleic acid testing. serologic and/or nucleic acid testing.
Additionally all transplant recipients should be Additionally all transplant recipients should be counseled in preventive measures counseled in preventive measures regarding mosquito bites, including the use of regarding mosquito bites, including the use of protective clothing and DEET containing insect protective clothing and DEET containing insect repellants. repellants.
Treatment for West Nile intransplant recipients Treatment for West Nile intransplant recipients has not been standardized but should include a has not been standardized but should include a reduction in immunosuppression along with reduction in immunosuppression along with supportive care supportive care

Fungal infections Fungal infections in solid organ in solid organ
transplantation transplantation recipients recipients

Incidence of major invasive fungal Incidence of major invasive fungal infection(IFI) among Kidney infection(IFI) among Kidney recipient patient:recipient patient:
1.1. Aspergillus:0-26%Aspergillus:0-26%
2.2. Candida:76-95%Candida:76-95%
3.3. Cryptococcus:0-39%Cryptococcus:0-39%
4.4. Other fungi:0-39%Other fungi:0-39%
Hand book of renal transplant:( Gabriel)

Incidence of fungal infections in renal Incidence of fungal infections in renal transplant recipient s is less than other transplant recipient s is less than other SOT but mortality high :SOT but mortality high : Pathogen city of organismPathogen city of organism Site of infectionSite of infection Impaired host inflammatory responseImpaired host inflammatory response Limited diagnostic toolsLimited diagnostic tools Potential for rapid clinical progression Potential for rapid clinical progression Failure to recognize a “high risk” patientsFailure to recognize a “high risk” patients Co morbid disease (renal failure and DM)Co morbid disease (renal failure and DM)
Hand book of renal transplant:( Gabriel)

Risk factor for colonization with Risk factor for colonization with yeast and molds after KT:yeast and molds after KT: Corticosteroid therapyCorticosteroid therapy Broad spectrum antibioticBroad spectrum antibiotic Domiciliary exposureDomiciliary exposure Presence of urinary catheter Presence of urinary catheter Endotracheal tubeEndotracheal tube
Hand book of renal transplant:( Gabriel)

Fungal growth on:Fungal growth on:
SkinSkin Mucosal surfacesMucosal surfaces Within gastrointestinal tractWithin gastrointestinal tract
Hand book of renal transplant:( Gabriel)

Common fungalCommon fungal
Common Common Candida spp.Candida spp. Aspergilous sppAspergilous spp C. neoformansC. neoformans
Hand book of renal transplant:( Gabriel)

Geographical mycosis:Geographical mycosis:
Geographical mycosis:Geographical mycosis: HistoplasmaHistoplasma CoccidioidesCoccidioides BlastomycesBlastomycesOccur under clinical circumstances:Occur under clinical circumstances:1.1. Immunomodulating viral infImmunomodulating viral inf2.2. ReactivationReactivation3.3. Ch. Graft dysfunctionCh. Graft dysfunction4.4. During treatment of post transplant During treatment of post transplant
malignanciesmalignanciesHand book of renal transplant:( Gabriel)

Renal transplantationRenal transplantation
CandidaCandida species: 95% species: 95% GI tractGI tract Disseminated infection: <5%Disseminated infection: <5% Risk factors:Risk factors:
DiabetesDiabetes Prolonged pretransplant dialysisProlonged pretransplant dialysis RejectionRejection Tacrolimus suppressionTacrolimus suppression
Invasive aspergillosis infrequentInvasive aspergillosis infrequent
Hand book of renal transplant:( Gabriel)

Candida Candida
Occurs most Occurs most commonly during the commonly during the 11stst month following month following transplant associated transplant associated with;with; Technical Technical
complexitiescomplexities Complication KT Complication KT
surgerysurgery Early rejectionEarly rejection Enhanced Enhanced
immunosuppressionimmunosuppression
Sources:Sources: Endogenous: Endogenous:
Source of Source of colonizationcolonization
Exogenous: lack of Exogenous: lack of hand washing of hand washing of health workershealth workers
Hand book of renal transplant:( Gabriel)

Most common Most common species:species: C. albicansC. albicans
Others:Others: C. GlabrataC. Glabrata C tropicalisC tropicalis C. kruseiC. krusei
Hand book of renal transplant:( Gabriel)

Candidal colonizationCandidal colonization
Pulmonary tree
BowelVagina
Esophageal / GI

Candida: Infection Candida: Infection sitessites
C. parapsilosisC. parapsilosisC. parapsilosisC. parapsilosis C. tropicalisC. tropicalisC. tropicalisC. tropicalis
C. albicansC. albicansC. albicansC. albicans
C. kruseiC. kruseiC. kruseiC. krusei
C. glabrataC. glabrataC. glabrataC. glabrata

SPECTRUM OF INVASIVE SPECTRUM OF INVASIVE CANDIDA INFECTIONSCANDIDA INFECTIONS
SPECTRUM OF INVASIVE SPECTRUM OF INVASIVE CANDIDA INFECTIONSCANDIDA INFECTIONS
candidemiacandidemia
organ infectionorgan infection
acute acute CandidaCandida septicemia septicemia
prompt prompt empiric coverempiric cover
candidemia candidemia
eliminate risk factoreliminate risk factor specific coverspecific cover
acuteacute disseminateddisseminated candidiasis candidiasis
prompt empiric cover
‘ ‘hepato-hepato- splenic’splenic’
candidiasis candidiasis
specific coverspecific cover beware of toxicitybeware of toxicity

GI tractGI tract
MODEL FOR INVASIVE CANDIDIASISMODEL FOR INVASIVE CANDIDIASISMODEL FOR INVASIVE CANDIDIASISMODEL FOR INVASIVE CANDIDIASIS
antibioticsinsult
injury selection
translocationtranslocation
infectioninfection CandidaCandida species species
Normal Normal commensal commensal floraflora
DiseaseDisease
Central venous catheterCentral venous catheter

Candida: From colonisation to Candida: From colonisation to infectious disease in a infectious disease in a neutropenic patientneutropenic patient
COLONISATIONCOLONISATION
MUCOSAL MUCOSAL INVASIONINVASIONMUCOSAL MUCOSAL INVASIONINVASION
DISSEMINATIONDISSEMINATIONDISSEMINATIONDISSEMINATION
ORGAN ORGAN INFECTIONINFECTIONORGAN ORGAN INFECTIONINFECTION
11 22 33

Renal candidosisRenal candidosis

PROGNOSTIC FACTORS IN CANDIDEMIAPROGNOSTIC FACTORS IN CANDIDEMIA NUCCI & ANAISSIE Clin Infect Dis 2002; 34:591-9NUCCI & ANAISSIE Clin Infect Dis 2002; 34:591-9
PROGNOSTIC FACTORS IN CANDIDEMIAPROGNOSTIC FACTORS IN CANDIDEMIA NUCCI & ANAISSIE Clin Infect Dis 2002; 34:591-9NUCCI & ANAISSIE Clin Infect Dis 2002; 34:591-9
Associated with death:Associated with death:-more severe clinical symptoms-more severe clinical symptoms-persisting neutropenia-persisting neutropenia-organ involvement-organ involvement--high agehigh age
Beter survival if:Beter survival if:**catheter is removedcatheter is removed*neutropenic patients given antifungals*neutropenic patients given antifungals

AspergillosisAspergillosis

DEVELOPMENT OF ASPERGILLOSISDEVELOPMENT OF ASPERGILLOSISDEVELOPMENT OF ASPERGILLOSISDEVELOPMENT OF ASPERGILLOSIS
11 22 33
INHALATIONINHALATION INFECTIONINFECTIONCOLONIZATIONCOLONIZATION DisseminationDissemination

Invasive aspergillosisInvasive aspergillosis
Liver recipients: 1-4.5%Liver recipients: 1-4.5% Kidney recipients: 0.5-2.2%Kidney recipients: 0.5-2.2% Lung or lung-heart recipients: 18%Lung or lung-heart recipients: 18%

Renal aspergillosisRenal aspergillosis

Invasive aspergillosis in Invasive aspergillosis in solid-organ transplantationsolid-organ transplantation
Type Type DonorDonor Time of IA after TxTime of IA after Tx RenalRenal CadevarCadevar 21st day21st day RenalRenal CadevarCadevar 23rd day23rd day RenalRenal LiveLive 26th day26th day
Ergin et al. Transplant International 2003; 16: 280-286Ergin et al. Transplant International 2003; 16: 280-286

Invasive aspergillosis in Invasive aspergillosis in solid-organ transplantation: solid-organ transplantation:
risk factorsrisk factors Pulse steroidPulse steroid OKT3OKT3 Antibiotic useAntibiotic use Organ failureOrgan failure RetransplantationRetransplantation ThrombocytopeniaThrombocytopenia CONSTRUCTIONCONSTRUCTION
Ergin et al. Transplant International 2003; 16: 280-286Ergin et al. Transplant International 2003; 16: 280-286

Invasive aspergillosis in Invasive aspergillosis in solid-organ transplantation: solid-organ transplantation:
diagnosisdiagnosis Radiology: chest X-ray and CT: no halo signRadiology: chest X-ray and CT: no halo sign MicrobiologyMicrobiology
Respiratory secretions: BAL/biopsyRespiratory secretions: BAL/biopsy Direct microscopyDirect microscopy cultureculture
Serological surveillanceSerological surveillance ELISA for galactomannanELISA for galactomannan
PCRPCR
Ergin et al. Transplant International 2003; 16: 280-286Ergin et al. Transplant International 2003; 16: 280-286

Invasive aspergillosis in Invasive aspergillosis in solid-organ transplantation: solid-organ transplantation:
TreatmentTreatment Conventional amphoterin B: 20-83% Conventional amphoterin B: 20-83% responseresponse
?iv itraconazole: limited data?iv itraconazole: limited data Lipid formulations of ampho BLipid formulations of ampho B 5 mg/kg/day liposomal ampho B5 mg/kg/day liposomal ampho B Surgical interventionSurgical intervention ProphylaxisProphylaxisErgin et al. Transplant International 2003; 16: 280-Ergin et al. Transplant International 2003; 16: 280-
286286

Zygomycosis in SOTZygomycosis in SOT
Median 2 months post-transplantMedian 2 months post-transplant Most cases occur within 6 months Most cases occur within 6 months
of transplantof transplant Rhinocerebral formRhinocerebral form 76% diabetes and corticosteroids76% diabetes and corticosteroids 56% mortality56% mortality

Where do filamentous fungi Where do filamentous fungi come from?come from?
Mycological surveillanceMycological surveillance
PatientPatient Home/work environmentHome/work environment Hospital: air, waterHospital: air, water

Aspergillus is in the air!Aspergillus is in the air!

Nosocomial aspergillosisNosocomial aspergillosis

Aspergillus is in tea!Aspergillus is in tea!

DustDust

Air samplingAir sampling

Air sampling culture platesAir sampling culture plates

Patient’s house: home sweet Patient’s house: home sweet homehome

Who diagnoses fungal Who diagnoses fungal infections?infections?
Infectious Disease PhysicianInfectious Disease Physician
ClinicianClinician MicrobiologistMicrobiologist
Pharmaceutical IndustryPharmaceutical Industry
PathologistPathologist

Diagnosis: The site of Diagnosis: The site of infectioninfection
SkinSkinOral cavityOral cavityAlimentary tractAlimentary tractAirwaysAirwaysLungsLungsLiver/spleenLiver/spleenCNSCNSDisseminatedDisseminated

Impact of diagnostic Impact of diagnostic markers on treatment markers on treatment
decisionsdecisions HRCTHRCT Aspergillus galactomannanAspergillus galactomannan GlucanGlucan MannanMannan DNA/RNA: PCRDNA/RNA: PCR

Clinical hasteClinical haste
answeranswer
MicrobiologyMicrobiology

ProphylaxisProphylaxis
AmBisomeAmBisome ItraconazoleItraconazole

Prevention of fungal Prevention of fungal infection in infection in
transplantationtransplantation Issues:Issues:
Candida remains major complication in intra-Candida remains major complication in intra-abdominal solid organ transplantion where bowel is abdominal solid organ transplantion where bowel is surgically manipulated.surgically manipulated.
Aspergillus main fungal complication in lung Aspergillus main fungal complication in lung transplant recipientstransplant recipients
Intra-abdominal: fluconazole: 100-400 mg/day 1-3 Intra-abdominal: fluconazole: 100-400 mg/day 1-3 months post liver Txmonths post liver Tx
Lung Tx: Lung Tx: inhaled liposomal ampho Binhaled liposomal ampho B ItraconazoleItraconazole Avoidance of exposureAvoidance of exposure

Successful managementSuccessful management
Prompt recognition of infectionPrompt recognition of infection Adjustment of level of Adjustment of level of
immunosuppressionimmunosuppression Antifungal therapy and surgeryAntifungal therapy and surgery

TreatmentTreatment Conventional amphotericin BConventional amphotericin B
1-1.5 mg/kg/day1-1.5 mg/kg/day Nephrotoxicity big issueNephrotoxicity big issue
30%30% 18% require haemodialysis18% require haemodialysis
Liposomal amphotericin BLiposomal amphotericin B Much reduced nephrotoxicityMuch reduced nephrotoxicity Superior efficacySuperior efficacy
Itraconazole: iv formulation: little dataItraconazole: iv formulation: little data Voriconazole/caspofungin: little data.Voriconazole/caspofungin: little data.
Singh 2003 Infect Dis Clin N Am 17; 113-134.Singh 2003 Infect Dis Clin N Am 17; 113-134.

Strategies for Strategies for dealing with dealing with
systemic systemic fungal fungal
infectious infectious diseasedisease

00
3636
3737
3838
3939
4040
4411
Tem
per
atu
re (
°C)
Tem
per
atu
re (
°C)
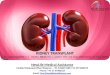
Optimal antifungal Optimal antifungal management?management?
CultureCultureCultureCulture + TissueTissueTissueTissue +GalactomannanGalactomannanGalactomannanGalactomannan+
PCRPCRPCRPCR +
Treatment
Disease likelihood
-7-7 00 77 1414 2121 2828 3535 4242 4949 5656 6363-14-14
0.10.1
11
1010
Days after transplantDays after transplant
Gra
nu
locy
tes
(lo
gG
ran
ulo
cyte
s (l
og
1010x
10x1099 /
L)
/L)
EmpiricalEmpirical
PossiblePossible
ProphylaxisProphylaxis
RemoteRemote
SpecificSpecific
ProvenProven
Pre-emptivePre-emptive
Probable diseaseProbable disease

-7-7 00 77 1414 2121 2828 3535 4242 4949 5656 6363-14-14
0.10.1
11
1010
Days after transplantDays after transplant
Gra
nu
locy
tes
(lo
gG
ran
ulo
cyte
s (l
og
1010x
10x1099 /
L)
/L) 00
55
1010
1515
Gal
acto
man
nan
G
alac
tom
ann
an
rati
ora
tio
3636
3737
3838
3939
4040
4141
Tem
per
atu
re (
°C)
Tem
per
atu
re (
°C)
Todays choices: IPATodays choices: IPA
GalactomannanGalactomannanGalactomannanGalactomannan +
Itraconazole
AmBisomeCaspofunginVoriconazole
Antibacterial therapy

Largest experience with Largest experience with AmBisomeAmBisome
More than 10 years experience in 383 patients. More than 10 years experience in 383 patients. Two double blind placebo controlled randomized Two double blind placebo controlled randomized
trials with AmBisome as prophylaxistrials with AmBisome as prophylaxis Allogeneic & autologous BMT Allogeneic & autologous BMT Liver transplant recipients Liver transplant recipients
Three retrospective analyses of treatment with Three retrospective analyses of treatment with respect to safety and efficacyrespect to safety and efficacy Allogeneic BMT recipients (5 years) (79 patients)Allogeneic BMT recipients (5 years) (79 patients) Solid organ transplant recipients (10years) (196 patients)Solid organ transplant recipients (10years) (196 patients) Child recipients of transplant (7 years) (61 patients)Child recipients of transplant (7 years) (61 patients)
Tollemar and colleagues, Huddinge Hospital, StockholmTollemar and colleagues, Huddinge Hospital, Stockholm

AmBisome AmBisome treatmenttreatment
Solid organ transplant Solid organ transplant recipients,recipients,
10 year data10 year data
J. TollemarJ. Tollemar
Huddinge Hospital, Huddinge Hospital, StockholmStockholm
www.fungalforum.comwww.fungalforum.com

SOT patientsSOT patients Patients treated between Jan 1989 - March 1999Patients treated between Jan 1989 - March 1999 196 solid organ transplant recipients 196 solid organ transplant recipients 220 episodes of AmBisome treatment220 episodes of AmBisome treatment
56 for a verified infections56 for a verified infections 79 for a suspected infections79 for a suspected infections 85 as prophylaxis85 as prophylaxis
106 males106 males 90 females90 females Median age was 42 years, range 1 - 72Median age was 42 years, range 1 - 72
J. Tollemar, Huddinge Hospital, StockholmJ. Tollemar, Huddinge Hospital, Stockholmwww.fungalforum.comwww.fungalforum.com

SOT patientsSOT patients
123 liver (LTX) transplant recipients123 liver (LTX) transplant recipients 3 liver and bone marrow transplant recipients3 liver and bone marrow transplant recipients 5 liver and kidney transplant recipients5 liver and kidney transplant recipients 42 kidney (KTX) transplant recipients42 kidney (KTX) transplant recipients 21 kidney & pancreas (KPTX) transplant 21 kidney & pancreas (KPTX) transplant
recipientsrecipients 1 kidney and insulin islet transplantation 1 kidney and insulin islet transplantation
recipientrecipient 1 pancreas (P) transplant recipients1 pancreas (P) transplant recipients
J. Tollemar, Huddinge Hospital, StockholmJ. Tollemar, Huddinge Hospital, Stockholmwww.fungalforum.comwww.fungalforum.com

AmBisome treatment data in SOTAmBisome treatment data in SOT
Fungal InfectionFungal Infection
AmBisome treatmentAmBisome treatment VerifiedVerified SuspectedSuspected ProphylacticProphylactic
Duration (days),Duration (days),
mean ± SD (median)mean ± SD (median) 23±17(18)23±17(18) 18±15 (14)18±15 (14) 16±19 (7)16±19 (7)
rangerange 4-814-81 1-801-80 1-831-83
Max. dose (mg), Max. dose (mg),
mean ± SD (median)mean ± SD (median) 2.0±1 (1.8)2.0±1 (1.8) 1.7±0.9 (1.4)1.7±0.9 (1.4) 1.4±0.8 (1.0 )1.4±0.8 (1.0 )
rangerange 0.7-5.50.7-5.5 0.7-50.7-5 0.6-60.6-6
Total dose (g), Total dose (g),
mean ± SD (median)mean ± SD (median) 1.7±1.7 (0.95)1.7±1.7 (0.95) 1.4±1.3 (1.1)1.4±1.3 (1.1) 0.6±0.5 (0.4)0.6±0.5 (0.4)
rangerange 0.05-8.10.05-8.1 0.06-80.06-8 0.03-2.40.03-2.4J. Tollemar, Huddinge Hospital, StockholmJ. Tollemar, Huddinge Hospital, Stockholm
www.fungalforum.comwww.fungalforum.com

Adverse events in SOTAdverse events in SOT 335 adverse events were reported335 adverse events were reported 9 (3%) were regarded as caused by AmBisome treatment9 (3%) were regarded as caused by AmBisome treatment
6 Lumbago 6 Lumbago 2 Lumbago combined with chills2 Lumbago combined with chills 1 Lumbago with dyspnea1 Lumbago with dyspnea
No anaphylactic reaction was reportedNo anaphylactic reaction was reported 224 (67%) of the adverse events were regarded as 224 (67%) of the adverse events were regarded as
probably related to AmBisomeprobably related to AmBisome 112 (33%) of the adverse events were regarded as not 112 (33%) of the adverse events were regarded as not
related to AmBisomerelated to AmBisomeJ. Tollemar, Huddinge Hospital, StockholmJ. Tollemar, Huddinge Hospital, Stockholm
www.fungalforum.comwww.fungalforum.com

Efficacy: Suspected FI in Efficacy: Suspected FI in SOTSOT
75 patients recieved 79 episodes of treatment for 75 patients recieved 79 episodes of treatment for suspected FIsuspected FI
57 patients survived with clearance of symptoms and 57 patients survived with clearance of symptoms and 10 died with no FI at autopsy10 died with no FI at autopsy
7 patients died, no autopsy was performed7 patients died, no autopsy was performed 1 patient died with FI at autopsy (1 patient died with FI at autopsy (Aspergillus. fumAspergillus. fum)) Efficacy was shown in 67 out of 75 patients, Efficacy was shown in 67 out of 75 patients, 89 %89 %
J. Tollemar, Huddinge Hospital, StockholmJ. Tollemar, Huddinge Hospital, Stockholmwww.fungalforum.comwww.fungalforum.com

Conclusion: solid organ Conclusion: solid organ transplantationtransplantation
10 years experience of Ambisome treatment 10 years experience of Ambisome treatment in solid organ transplant recipients at one in solid organ transplant recipients at one single center has revealed:single center has revealed:
AmBisome treatment was safe AmBisome treatment was safe AmBisome treatment was efficacious as seen as AmBisome treatment was efficacious as seen as
survival or mycotic clearance in 92% of survival or mycotic clearance in 92% of proven proven fungal fungal infections in SOT patients infections in SOT patients
Efficacy in Efficacy in suspected FI suspected FI was 89 % clinical cureswas 89 % clinical cures
J. Tollemar, Huddinge Hospital, StockholmJ. Tollemar, Huddinge Hospital, Stockholmwww.fungalforum.comwww.fungalforum.com

Liposomal amphotericin B is safe Liposomal amphotericin B is safe and effective in the treatment of and effective in the treatment of
invasive mycosis in organ invasive mycosis in organ transplant patientstransplant patients 140 patients SOT140 patients SOT
12 (8%) IFI: 11 Candida; 1 Aspergillus12 (8%) IFI: 11 Candida; 1 Aspergillus Liver (3)Liver (3) Pancreas and kidney (4)Pancreas and kidney (4) Kidney (5)Kidney (5)
Liposomal ampho B: 1-5 mg/kg/dayLiposomal ampho B: 1-5 mg/kg/day Duration: 1-21 daysDuration: 1-21 days 10 patients completed 10 patients completed
1 death1 death 1 rejection1 rejection 8 infection cleared8 infection cleared
Merhav et al. 2001, Transplantation Proceedings 33: 2937-2938Merhav et al. 2001, Transplantation Proceedings 33: 2937-2938

susceptib
le
Empiricalor
positve GMtest
AmBisome
Fluconazole
AmBisome
glucan synthesis inhibitor (IV) ornew azole orally
no response
risk of aspergillosis
CULTURE
RESULT
Future Strategy Against Future Strategy Against Probable Probable
Invasive Fungal InfectionInvasive Fungal Infection??

Thank for your attention