Embed Size (px)
Citation preview

Kambia Planning Visit Report
31st May 2009 – 11th June 2009
Work shop participants 8th June 2009, Kambia Hospital

Kambia Planning Visit Report. 31/5/09 - 11/6/09 2
Summary This is the report of a visit from the UK to Kambia conducted from the 31st May 2009 – 11th June 2009 by Dr Richard Kerr-Wilson, Dr David Holmes and Ms Sarah Williams. The visit aimed to address recommendations in the evaluation by Dr Rahmat Hassan Mohammad of the work of the partnership between Gloucestershire Hospitals NHS Foundation Trust, Kambia District Hospital, The Kambia Appeal and the Peripheral Health Units of Barmoi and Maselleh. The information in this report is intended for use in planning future interventions. The visit included meetings with Mr Moses Kabba the Kambia appeal / link representative in Sierra Leone, senior hospital staff including Dr David Sesay the hospital medical superintendent, district health staff including Dr I.J. Kargbo Labour the district medical officer, community leaders and representatives, traditional birth attendants, ordinary men and women living in Kambia town and Ms Chemi Fujii the JICA project expert working with the DHMT in Kambia. Meetings were also held with government officials in Freetown. On the 8th of June a prioritisation and planning workshop was held in Kambia. During this meeting potential future activities were prioritised, a table of which appears on pp 44. Plans were made for the following highly prioritised activities.
• Making hospital maternal and newborn services more affordable. • Formal training of State enrolled community health nurses. • Training of hospital volunteers/formal upgrade training to nurse aides. • CPD in neonatal resuscitation, vacuum extraction, adult resuscitation,
anaesthetic training, theatre/scrub nursing and obstetric emergency training.
• Strengthening the TBA system and links between TBAs and health facilities.
• Health promotion so that sick children under the age of five are referred to health facilities before it becomes too late.
• Improving the availability of safe drinking water / refresher training of blue flag volunteers.
• Maternity waiting home to be established and assessed at the hospital along with maternity bus and emergency transportation system.
Outcomes regarding operational issues of the partnership were made including:
• The formation of the “Kambia Health Development Committee” in Kambia with members from the Hospital and DHMT. The Committee will meet monthly and communicate with the GHNHSFT Committee in the UK.
• A plan for improvements to visits from the UK to Kambia and visa versa. • Agreements aimed at improving transparency of decision making and
financing issues.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 3
Contents
SUMMARY ............................................................................................................2
CONTENTS ...........................................................................................................3
ACRONYMS USED IN REPORT ..........................................................................6
INTRODUCTION ...................................................................................................7 Activity recommendations ..................................................................................7 Operational recommendations ...........................................................................8
ACTIVITIES OF VISIT ...........................................................................................8
Time table for meetings and discussions held during the visit. .....................9
IMPORTANT BACKGROUND INFORMATION..................................................10
Sierra Leonean Reproductive and Child Health Directorate. ........................10
The Structure of the Health system in Kambia District (Management and Facilities.) ...........................................................................................................11
Central government, the district council and the council health committee. ....11 The District Health Management Team and JICA............................................11 Kambia District Referral Hospital .....................................................................12 The Peripheral Health Units (PHUs) ................................................................12 Funding of Health Services ..............................................................................13
INFORMATION ON PRESENT ACTIVITIES OF THE PARTNERSHIP AND FUTURE PLANS. ................................................................................................15
Funding for Caesarean sections ......................................................................15
User Fees............................................................................................................16 Plan ..................................................................................................................17
Staffing................................................................................................................18 Hospital staffing................................................................................................18 CHO training.....................................................................................................18 Laboratory Staff Training..................................................................................20 Training of State Enrolled Community Health Nurses including plan...............20 Formal training of Environmental Health Officers.(EHOs) ...............................20 Formal upgrade training of hospital volunteers to nurse aides including plan. 20 Continuing Professional Development including plan ......................................21

Kambia Planning Visit Report. 31/5/09 - 11/6/09 4
TBA training and strengthening links between TBAs and Health Facilities..............................................................................................................................22
Plan ..................................................................................................................23
Health Promotion: Care seeking behaviours for children under five and pregnant / labouring women.............................................................................24
Plan ..................................................................................................................24
Water and Sanitation .........................................................................................25 Hospital water supply .......................................................................................25 PHU water supply ............................................................................................25 Sanitation .........................................................................................................26 Blue flag volunteers..........................................................................................26 Plan ..................................................................................................................27
Health transportation system, bicycles, motorbike ambulances, maternity bus and maternity waiting home. .....................................................................27
Bicycles. ...........................................................................................................27 Motorbike ambulances .....................................................................................28 The Maternity Bus ............................................................................................29 Maternity waiting home. ...................................................................................29 Plan ..................................................................................................................30
Hospital Garage .................................................................................................30
Surgical and theatre support. ...........................................................................31 Plan ..................................................................................................................31
Surgical camps ..................................................................................................31
PHU Infrastructure.............................................................................................32 Baramoi PHU building......................................................................................32 Solar fridges .....................................................................................................33 Generator for Maselleh PHU............................................................................33
INFORMATION AND PLANS REGARDING OPERATIONAL ISSUES OF THE PARTNERSHIP ...................................................................................................34
Communications and decision making between all partners. ......................34
Visits from the UK to Kambia and from Kambia to the UK............................35
Transparency of decision making and funding / financing issues. ..............35
APPENDIX...........................................................................................................37

Kambia Planning Visit Report. 31/5/09 - 11/6/09 5
Nationwide needs assessment for emergency obstetric and newborn care servises in Sierra Leone: Executive Summary...............................................38 Three month reproductive ad child health directorate plan………………….39
Kambia DHMT members ...................................................................................42
Bar chart showing admissions, discharges and deaths from 19/1/09-25/5/09 at Kambia Hospital. …………………………………………………………………42
Participants of the Kambia Health Partnership Prioritising and Planning Workshop. Monday 8th June 2009 ...................................................................43
Workshop Activity Prioritisation Table............................................................44
PLANNING: Making hospital, maternal and newborn care health services more affordable..................................................................................................47
PLANNING: Formal training of SECHNs..........................................................49
PLANNING: Training of hospital volunteers / formal upgrade training to nurse aides. ........................................................................................................50
PLANNING: CPD in neonatal resuscitation, vacuum extraction, adult resuscitation, anaesthetic training, theatre/scrub nursing, and obstetric emergency training............................................................................................52
PLANNING: Strengthening the TBA system and links between TBAs and heath facilities. ...................................................................................................54
PLANNING: Health promotion so that sick children under the age of five are referred to health facilities before it becomes too late. .................................56
PLANNING: Improving the availability of safe drinking water / refresher training of blue flag volunteers. .......................................................................58
PLANNING: Maternity waiting home to be established and assessed at the hospital along with maternity bus and emergency transportation system. 60
PLANNING: Obtaining Theatre kits and instruments / theatre and surgical training................................................................................................................62

Kambia Planning Visit Report. 31/5/09 - 11/6/09 6
Acronyms used in Report AIDS Acquired Immune Deficiency Syndrome ANC Antenatal Care ARI Acute Respiratory infection. BEmONC Basic Emergency Obstetric and Newborn Care BSc Batchelor of Science CEmONC Comprehensive Emergency Obstetric and Newborn Care CHC Community Health Centre CHO Community Health Officer CHP Community Health Post CPD Continuing Professional Development DHMT District Health Management Team DMO District Medical Officer EHO Environmental Health Officer EmONC Emergency Obstetric and Newborn Care EPI Expanded Programme on Immunisation GHNHSFT Gloucestershire Hospitals NHS Foundation Trust GMC General Medical Council (UK) HIV Human Immunodeficiency Virus HMC Hospital Management Committee HMIS Health Management Information Systems JICA Japan International Cooperation Agency KA Kambia Appeal M&E Monitoring and Evaluation MCH Maternal Child Health MCH aide Maternal Child Health Aide MCHP Maternal Child Health Post NHS National Health Service (UK) ORS Oral Rehydration Salts PHU Peripheral Health Unit SECHN State Enrolled Community Health Nurse STI Sexually Transmitted Infection TB Tuberculosis TBA Traditional Birth Attendant THET Tropical Health and Education Trust TOR Terms of Reference TOT Training of Trainer UK United Kingdom UNICEF United Nations Children’s Fund USS Ultra Sound Scan VIP Ventilated Improved Pit (Latrine) VVF Vesico Vaginal Fistula WASCE West African School Certificate Examination Wat/San Water and Sanitation

Kambia Planning Visit Report. 31/5/09 - 11/6/09 7
Introduction The information contained in this report is intended to be used in planning future interventions for the partnership between the Kambia District Hospital, Gloucestershire Hospitals NHS Foundation Trust, the Kambia Appeal and Kambia DHMT. The report will firstly give the reasons behind the visit then outline the activities of the visit. Information obtained during the visit and plans made will then be presented under topic headings. The information is divided into three main sections; these are:
• Important background information. • Information on present activities of the partnership and future plans. • Information and plans regarding operational issues of the partnership.
The link between Kambia District hospital and Cheltenham General hospital began in 1992, and since then the partnership has evolved. In Kambia it now incorporates not only Kambia hospital but also the Peripheral Health Units (PHU) of Barmoi and Maselleh. In the UK the link institution is now Gloucestershire Hospitals NHS Foundation Trust (GHNHSFT), which is primarily involved with training activities, and the Kambia Appeal, which is a registered UK charity and deals with funding and operational issues. Over time the programme has grown and activities taken on new directions. With this growth has come a need to become more strategic and less ad hoc. To this end an external evaluation, supported by THET, was conducted in late 2008 by Dr Rahmat Hassan Mohammad. The present report documents the planning visit made to address the findings and recommendations of the evaluation. The following recommendations of the evaluation (see chapter 6 in the THET report) that will be addressed in this report are:
Activity recommendations
• Training of health workers, including follow up, Continuing professional development (CPD) and TBA training.
• Support and extend maternity services at Kambia District Hospital. • Expanded emergency Obstetric service at Kambia District Hospital. • Resolve Problems that lead to delays in funding for caesarean sections. • Remuneration and financing of services. • Improved water supply at Kambia District Hospital • Support and extend community level Maternity services (at the two PHUs) • Strengthening and expanding the Motorcycle Ambulance system.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 8
• Planning of surgeries, Including local demand, availability of facilities, and an emphasis on capacity building.
• Child health.
Operational recommendations
• Develop a demand driven planning process that involves all partners. • Greater ownership by hospitals. • Further strengthen information sharing with the local community. • Strengthen systems for record keeping, monitoring and evaluation. • Planning and management of link visits from the UK.
Activities of Visit A small team from the UK consisting of Dr Richard Kerr-Wilson chairman of the Kambia appeal, Dr David Holmes of the link committee and Sarah Williams, a health development facilitator, visited Sierra Leone from the 31st May 2009 to the 11th June 2009. During the visit they worked closely with Mr. Moses Kabba the Kambia appeal / link representative in Sierra Leone. Meetings were held with various stakeholders primarily made up of service providers from the DHMT, the hospital and the PHUs. In order to get community impressions of the health service and especially barriers to accessing care, focus group discussions were held with separate groups of men and women in Kambia town. Information on policies was also sought at national level from the ministry of health. On Monday the 8th a prioritising and planning workshop was held which included representatives form the Kambia appeal, the link, the hospital, the DHMT, the district council, the paramount chief and the community. A list of participants can be found in the appendix. During the workshop, existing and potential activities for the partnership were discussed and prioritised into three groups. Those that “Must be done”, those that “Should be done” and those that “Could be done”. Plans were then made in smaller groups for the “Must be done” activities. After this operational issues were discussed and some points agreed on. After the visit this report was written by Sarah Williams and sent out to stakeholders for feedback twice before being finalised. On the following page is the timetable for the meetings and discussions held during the visit:

Kambia Planning Visit Report. 31/5/09 - 11/6/09 9
Timetable for meetings and discussions held during the visit. Sunday 31/5
• Meeting at airport with Drs Janaki and Per Brolin, UK doctors leaving Sierra Leone who had been working in Kambia for 5 months.
Monday 1/6
• Kambia based link management team: Moses Kabba and volunteers Ibrahim Kamara and Khalil Kamara.
• Dr David Sesay, Kambia hospital medical superintendent.
Tuesday 2/6
• Ms Chiemi Fujii. JICA project expert working with DHMT • Dr I.J.Kargbo Labour, District Medical Officer
Wednesday 3/6
• District Health Management Team • Dr David Sesay and Dr I.J.Kargbo Labour
Thursday 4/6
• Senior Hospital staff: Dr D Sesay, CHO Mohamed Kamara, Sister Frances Pearce (hospital matron) the Laboratory technician and the Pharmacist.
Friday 5/6
• Deputy paramount chief. • Focus group discussions with 18 women in Kambia town. • Focus group discussions with 10 men in Kambia town. • Kambia appeal scholarship CHO students: Ms Elizabeth
Conteh, Mr Al Hassan Sumah, Mr Al Hassan Koroma, Mr Mohammed A.L. Kamara, Mr Joseph Kalokoh, Ms Terena Thollay.
Saturday 6/6:
• Barmoi PHU staff and committee, PHU chief Edward Sesay, MCH aides Elizabeth and Salim Kabia, Section Chief, Town head, Deputy paramount chief, Town chief, motorbike ambulance drivers, 9 TBAs
• Maselleh PHU staff and committee, MCH aide Ms Isatu Bangura (in charge) community leaders and six TBAs
Sunday 7/6 • Preparation for workshop. Monday 8/6 • Prioritising and planning workshop. Tuesday 9/6 • Dr Foday Dafae, Director, National TB and Leprosy
control programme. • Mr Ibrahim Fofana , Assistant to national NGO Liaison
Officer Wednesday 10/6
• Dr Duramani Conteh, Director of hospital and laboratory services.
• Dr Bundu Ibrahim, regional head of surgery for the North. • Dr Samuel A.S Kargbo, Director National Reproductive
and Child Health Programme

Kambia Planning Visit Report. 31/5/09 - 11/6/09 10
Important background information.
Sierra Leonean Reproductive and Child Health Directorate. The national Reproductive and Child Health Directorate has launched a new reproductive and child health strategy. It follows on from a nation wide assessment conducted in 2008 of emergency obstetric and neonatal care (EmONC). A copy of the executive summary of the needs assessment can be found in the appendix on pp 38. The main findings of the assessment were
• Only 14 hospitals in Sierra Leone offer comprehensive EmONC, which include the provision of 24hour facilities for blood transfusion and caesarean section; other than these hospitals nowhere offers basic EmONC (which includes midwifery supervision with ability to perform instrumental vaginal delivery and manual removal of placenta). In Kambia the only place where a full package of EmONC services were available was the district hospital; none of the PHUs were able to provide BEmONC.
• The percentage of births in health facilities was 10% • There is a lack of appropriate human resources. Especially in the areas of
operative deliveries, blood transfusion and care of premature and low birth weight babies.
• Traditional birth attendants attend the majority of births. • There is low utilisation of health facilities by labouring women possibly due
to lack of skilled attendants (most institutional deliveries are by MCH aides) and fees charged.
• There are poor links between health facilities of different levels and difficulties in referring patients due to communication and transportation difficulties.
• There is a lack of basic utilities, water, electricity and transportation. There are two programmes of particular relevance to this partnership; one is the creation of five BEmONC centres at CHC’s in Kambia district. The other is a three month programme, which if successful will be extended, an outline of this programme can be found in the appendix (pp 39), the main activities are:
• Incentives to be paid to Maternity ward, theatre staff, laboratory staff and ambulance drivers.
• Radio jingles on EmONC, ANC and delivery by skilled attendant. • Maternal and under fives weekly mortality audits. • Incentives and fuel for transportation for outreach activities. • Training for PHU and hospital on integrated maternal, child and neonatal
survival interventions. • Training on PHU and hospital staff in EmONC. • Transportation of vaccines and supplied monthly to PHUs. • Support to monthly supervision by DHMT
Kambia Planning Visit Report. 31/5/09 - 11/6/09 11
• Training of health staff on data collection tools. As the partnership aims to complement and strengthen the existing work of the health facilities in Kambia, and not unnecessarily duplicate activities, it is necessary to remain aware of the activities of the Reproductive and Child Health Directorate as these can significantly affect the need for and effectiveness of partnership programmes.
The Structure of the Health system in Kambia District (Management and Facilities.) The Kambia appeal and the link work within the Kambia district health system so a clear understanding of how this system works is essential. The following is a summary of information obtained on the health system from the meetings held during the visit.
Central government, the district council and the council health committee. Decentralisation of certain powers and funds from central government to district councils is a recent event in Sierra Leone. At central government level the Ministry of Health and Sanitation provides policies, guidelines and funds to the district council. The District council contains a council health committee. The head of the council health committee in Kambia is Mr Mohamed Jalloh. The council health committee coordinates with the District Health Management Team.
The District Health Management Team and JICA The district health management team coordinates all the health activities in the district, including training, supportive supervision, campaigns and data collection. It is headed by Dr I.J Kargbo Labour the District Medical Officer. Mr Moses Kabba of the Kambia link is also on the DHMT. A full list of DHMT Members can be found in the appendix. The Japan International Cooperation Agency (JICA) has been working with the DHMT for two and a half years. Their representative in Kambia is Ms Chiemi Fujii. JICA work with the DHMT on management capacity development, strengthening of the health management information system (HMIS) and of the district health planning system and coordination of DHMT with the district council, the PHU committees and other stakeholders. Ms Chiemi Fujii reassured us that there is no duplication of the work of the Kambia appeal / link and JICA. The work of JICA in strengthening the DHMT will help the DHMT with data gathering which is good for the Kambia appeal / link as better quality data means improved ability to assess the affect of link activities.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 12
Kambia District Referral Hospital This is the only referral hospital in Kambia District for secondary care; it is located in Magbema Chiefdom. Dr David Sesay is the Medical Superintendent of the hospital and its only doctor. Data from Drs Janaki and Per Brolin show that in a four-month period from January to May the hospital admitted approximately 441 patients. A bar chart in the appendix gives a further breakdown of hospital admissions, discharges and deaths during this period. Hospitals in Sierra Leone should have a hospital board with the intended members established by an act of parliament in 2003. Members are meant to be the District medical officer, the matron, the paramount chief, the chairman of the council health committee, the district pharmacist, civil society members and a lawyer from the attorney generals office in Freetown. However this board does not meet very often.
The Peripheral Health Units (PHUs) There are 57 PHUs in Kambia district. Each PHU should have a PHU Committee who help with the running of the PHU and is representative of the community served by the PHU. However most PHUs do not have working committees. Nationwide PHUs must produce quarterly reports. JICA has given TOT training to the DHMT for these reports, the training has not yet cascaded to the MCH aides at the health posts. There are three levels of PHU and these are determined by the staff they have. The top level is a Community health Centre (CHC) that must have a Community health officer (CHO); they should also have a laboratory technician and a nurse; every chiefdom (seven in Kambia district) is meant to have a CHC but this is not always the case. A Community Health Post (CHP) must have a state enrolled nurse (SECHN) and MCH aide. A Maternal child health post is staffed by an MCH aide alone.
Kambia Planning Visit Report. 31/5/09 - 11/6/09 13
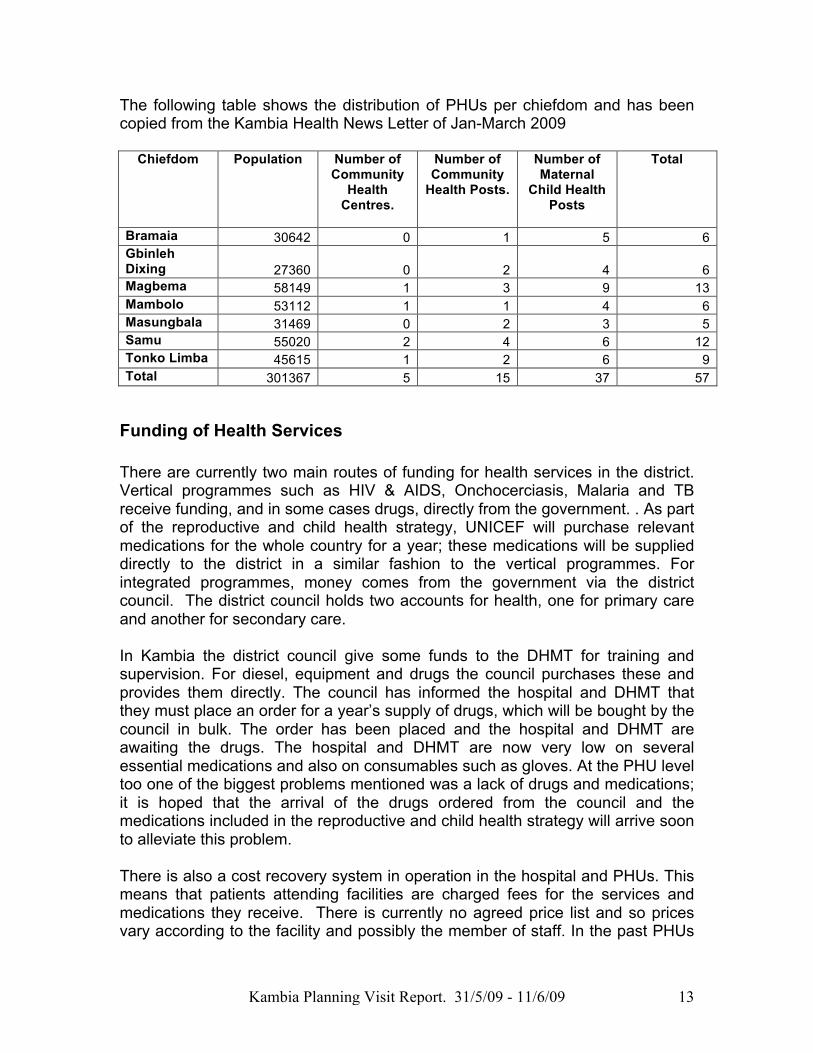
The following table shows the distribution of PHUs per chiefdom and has been copied from the Kambia Health News Letter of Jan-March 2009
Chiefdom Population Number of Community
Health Centres.
Number of Community
Health Posts.
Number of Maternal
Child Health Posts
Total
Bramaia 30642 0 1 5 6 Gbinleh Dixing 27360 0 2 4 6 Magbema 58149 1 3 9 13 Mambolo 53112 1 1 4 6 Masungbala 31469 0 2 3 5 Samu 55020 2 4 6 12 Tonko Limba 45615 1 2 6 9 Total 301367 5 15 37 57
Funding of Health Services There are currently two main routes of funding for health services in the district. Vertical programmes such as HIV & AIDS, Onchocerciasis, Malaria and TB receive funding, and in some cases drugs, directly from the government. . As part of the reproductive and child health strategy, UNICEF will purchase relevant medications for the whole country for a year; these medications will be supplied directly to the district in a similar fashion to the vertical programmes. For integrated programmes, money comes from the government via the district council. The district council holds two accounts for health, one for primary care and another for secondary care. In Kambia the district council give some funds to the DHMT for training and supervision. For diesel, equipment and drugs the council purchases these and provides them directly. The council has informed the hospital and DHMT that they must place an order for a year’s supply of drugs, which will be bought by the council in bulk. The order has been placed and the hospital and DHMT are awaiting the drugs. The hospital and DHMT are now very low on several essential medications and also on consumables such as gloves. At the PHU level too one of the biggest problems mentioned was a lack of drugs and medications; it is hoped that the arrival of the drugs ordered from the council and the medications included in the reproductive and child health strategy will arrive soon to alleviate this problem. There is also a cost recovery system in operation in the hospital and PHUs. This means that patients attending facilities are charged fees for the services and medications they receive. There is currently no agreed price list and so prices vary according to the facility and possibly the member of staff. In the past PHUs

Kambia Planning Visit Report. 31/5/09 - 11/6/09 14
kept 50% of the fees they received and gave 50% to the district council, this has now changed and officially the PHU share of the fee is 25% the rest goes to the council. There are two factors related to funding of special relevance to the Kambia appeal / link which will be discussed in the activity planning section which follows. These are the cost of services as a barrier to care and the specific cost of caesarean sections.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 15
Information on present activities of the partnership and future plans.
This section looks at activity related information.
Funding for Caesarean sections From October 2007 until the end of April 2009, the Kambia Appeal has covered the cost of caesarean section at the hospital and were paying 230 000 le per section. This was so that the cost did not prevent women who needed a caesarean from receiving one. The table below gives an idea of the obstetric activity at the hospital in the last four months and of particular relevance the numbers of Caesarean sections performed relative to the number of births. The data for the table has come from Drs Janaki and Per Brolin.
The evaluation highlighted the problem of delays in funding for caesarean sections; delays may be due to the reporting system from the hospital to the Kambia appeal in Sierra Leone and then on to the KA in the UK. It was also suggested that there might be delays on the financial side in the UK due to the passage of information to relevant people in the UK. Drs Janaki and Per Brolin stated and Dr Sesay confirmed that the number of caesareans performed was not affected by the funding issue (in May 11-12 were

Kambia Planning Visit Report. 31/5/09 - 11/6/09 16
performed) but that it was causing a problem. As money is not coming from the KA for sections women are being charged for the operation. However if they don’t pay the caesarean section is still carried out. The fee for a caesarean at the hospital has also increased and now costs 350 000 le. The fee can be divided in to four parts one for administration, one for fuel, one for drugs and another for the operation. Payment by the KA appeal for caesareans was discussed in meetings with the senior hospital staff and the DHMT. The need for the KA to fund caesareans may only be temporary and depends upon agreements over service fees for the whole district and money to support reproductive and child health care as part of the pilot three-month reproductive and child health strategy programme. However if the KA continues to fund caesareans the following was agreed:
• Reliable information on sections performed including patient names, place of residence, clinical indications and outcome will be provided to the KA on a monthly basis along with the minutes of the Kambia committee meeting.
• If the KA funds sections they will cover the cost of caesarean for all women at the hospital who need one regardless of where they are from (questions on funding of a caesarean performed on a woman from another district had caused problems in the past).
• The hospital is happy to receive payment in retrospect as long as it knows when the money will come.
User Fees. User fees are an issue of concern and affect access to services, users are currently charged fees under the cost recovery system. Whilst there seems to be a general acceptance that fees will be charged, information from male and female focus group discussions indicate that the fees are too high and act as a deterrent from seeking health care. Of the 18 women from Kambia town who participated in the female focus group discussions they all said that cost of care was the biggest barrier to accessing antenatal and labour services at the hospital. One woman, who was approximately six months pregnant, said that whilst she wanted to, she had never been for ANC, as it was too expensive and that she would not be able to go for her entire pregnancy. The table below shows what women stated the current costs to be and what they would consider to be acceptable/ affordable costs. They also stated that there should be an exemption scheme for really poor women and that care at a PHU was cheaper than care at the hospital.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 17
Hospital Service Current cost as stated by women’s focus group.
Acceptable cost as stated by women’s focus group
Child health card 5 000 le ANC card 5 000 le Single ANC visit (inclusive of TT and iron supplements)
10 000 le 5000 le
Birth of baby girl 40 000 le Birth of baby boy 50 000 le
15 000 – 20 000 le
£1 is approximately 5 000 Le
Two women also stated that they had heard stories about women unable to pay giving birth in hospital and being held, unable to leave until someone had come and paid for their release. Whether or not this is true the women in the focus group were scared of giving birth in hospital in case this happened to them. When asked how they felt about the cost of giving birth to a boy being more expensive than a girl one group of women laughed and told me it was because boys were harder to give birth to and this meant more work for the hospital staff. More worryingly this could be a reflection of values attached to gender in the communities. Especially when viewed along with the Brolin's observation, that if a hospital patient is an adult man families seem more ready to pay the user fee than if the patient is a woman or a child. Similar sentiments were echoed by senior hospital staff who stated that if a male patient dies there is more likely to be an investigation and the hospital is more likely to be blamed (even in some cases on the radio) than if a female or child patient dies. As with the cost of caesarean sections the new reproductive and child health strategy may have a positive impact on user fees. The subject of making maternal and newborn health services more affordable was discussed in the workshop. Some participants seemed genuinely shocked that women stated they were paying for ANC and child health services.
Plan During the workshop a plan was formulated with the whole group to tackle this issue. (The full plan can be found in the appendix, pp 47) In summary it includes:
• Meetings with stakeholders to agree on a standardised list of prices. • Community sensitisation about the value of ANC and skilled attendance at
birth through meetings and radio broadcasts. • Clear display of standard prices at health facilities. • Monitoring and supervision to ensure the standardised prices are the ones
charged.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 18
Staffing
Hospital staffing. The hospital currently has five trained professional staff, among them Dr Sesay the Medical superintendent, CHO Mohamed, and Sister Francess Pearce the Matron. There is currently no midwife working at the hospital. So whilst the hospital has many workers around 68 staff, 39 of which are volunteers, it has very few trained staff. Another five trained staff including a doctor have been assigned to the hospital, and although they receive their salary, they are not yet present in Kambia. Matron has said that if the assigned nursing staff do not attend the hospital within the next month she will write a letter to stop their pay. Of the 39 hospital volunteers the majority are not paid at all, however their health care and health care for their families is provided free. Most volunteers have a basic general education, they receive no training once they commence work in the hospital and learn from observing only. Sometimes there are difficulties with volunteers’ form filling and writing in patient notes. In the meetings, training of these volunteers in basic nursing skills was frequently mentioned as a need and CHO Mohamed has written a draft curriculum for them. At Maselleh PHU, Isatu, the MCH aide is the only member of staff. The PHU is large and the community leaders said there is “too much work for one nurse” they would very much like some more staff for the PHU.
CHO training To help with the shortage of trained staff the Kambia appeal has provided scholarships for twelve CHO students who are currently at different stages of their training. After qualification the students will be bonded to work in Kambia for three years. In several meetings the sponsor ship for the CHO students was recognised as a strong point of the programme as the students seem enthusiastic and on qualification they can do many of the activities of a doctor but are more likely to stay in the area. Six of the 12 CHO students attended the meeting on the 5th of June. They explained about the training and how they are finding the financial situation difficult. CHO training is three years long and is based in Bo. They receive theoretical and practical training from national and international tutors. The course is 60% practical and it includes experience of working in hospital and rural PHUs, performing caesarean sections, appendectomies, hernia repairs and minor surgery and teaching skills. Difficulties faced by students include lack of books and the fact that they must purchase pamphlets from tutors. There are about 9-10 pamphlets and the cheapest of these is 10 000 le. At the end of every semester they must work in a rural PHU for three weeks, they do not have

Kambia Planning Visit Report. 31/5/09 - 11/6/09 19
transport to get to the PHU, they are not always expected and when they arrive they do not know anyone and have no where to stay. They have requested a small raise in their scholarship to cover specific costs. The following table is an itemisation of the additional money they are requesting which was drafted by themselves and Moses Kabba at the end of the meeting. Items needed by CHO students in training: Estimate of additional cost per student.
Items Year one (Le)
Year two (Le)
Year three (Le)
Total
Pamphlets 250,000 200,000 200,000 Transportation for practical 100,000 100,000 100,000 Feeding 300,000 300,000 300,000 Dissertation writing ------------- -------------- 400,000 Blood pressure machine Emergency kit Autoscope Total 650,000 600,000 1,000,000 2,250,000
£1 is approximately 5 000 Le Three of the students qualify this year and among them is Mr Joseph Kalokoh, the other two could not be present. He explained that in the third year they must conduct a piece of research in the field and write this up as a dissertation. He is doing his dissertation on cholera prevalence in Kambia. The dissertation costs them additional money. There is the potential that future student dissertations could be used to help evaluate programme activities. There are currently changes being made to CHO training in Sierra Leone wit an additional year being added to the course to turn it into a BSc. There is not much information currently available about this but it is thought the additional year will be optional. Before the end of the year Moses Kabba will visit Njala University to get more information. It is the DHMT who will decide where in Kambia the students will work upon qualification. The Kambia appeal / link would like to suggest that each Chiefdom could have a CHO to work in the CHC and that to increase continuous learning, CHOs could rotate to the hospital and back to the CHC. Joseph said that it is important for the CHOs to work in the communities after they have been trained and that communities must know that the Kambia appeal sponsored them. He also said that because they are all from Kambia they are likely to stay in the district. Once the CHOs have completed their training there are no current plans to sponsor more, however a similar model of sponsorship / scholarship could be used in the training of different cadres of health worker

Kambia Planning Visit Report. 31/5/09 - 11/6/09 20
Laboratory Staff Training Mr Francis Pieh is finishing a laboratory course in Freetown sponsored by the Kambia appeal. He will be returning to the hospital. It was not mentioned in any of the meetings in Kambia but in Freetown Dr Conteh said there is a growing need for support to hospital laboratories. It was decided that Moses Kabba would ask the hospital laboratory in Kambia if they needed support and what kind of support; this could then be discussed further with partners.
Training of State Enrolled Community Health Nurses including plan. Scholarships for SECHN nurses, similar to the scholarships of the CHOs, were recommended by Dr Labour, and in the workshop this was classed as a “Must” activity. Reasons for this were that it would increase the quality of care in the district, and nurses are even more likely to stay in Kambia than CHOs. During the workshop a plan for the training of SECHNs was made (see appendix pp49) In summary the plan is for:
• Coordination by DHMT/DMO and district council. • Selection of candidates to be awarded scholarships with a bond to work in
Kambia after qualification. • To train 30 SECHNs on the two and a half year course over three intakes.
Formal training of Environmental Health Officers (EHOs). During the planning workshop the training of environmental health officers was raised and prioritised as a “should do” activity. The training is to the same level as that of CHOs and focuses on environmental health. It was suggested to train 7 EHOs, one for every chiefdom in Kambia. For information on water and sanitation issues please see the relevant section of the report (pp25).
Formal upgrade training of hospital volunteers to nurse aides including plan. As previously discussed there are 39 hospital volunteers who have received no training but provide the majority of nursing care to patients. The senior hospital staff believe this training to be very important. They stated that any training that is done should be done through the Sierra Leonean nursing board so that the certificate they receive at the end will be recognised. During the workshop a plan for the training of hospital volunteers was formulated (see appendix, pp50, for plan) in summary it involves:

Kambia Planning Visit Report. 31/5/09 - 11/6/09 21
• Identifying trainers, facilitators and venue. • Preparation of curriculum. • Provision of training materials. • Conduction and evaluation of training. • Supportive supervision of trainees. • Outcomes of training would be monitored by pre and post questionnaires
of patients cared for by nursing aids and completed supervision checklists.
Continuing Professional Development including plan CPD in the areas of neonatal resuscitation, vacuum extraction, adult resuscitation, anaesthetic training, theatre /scrub nursing and obstetric emergency care were all considered as “Must” activities in the workshop Additional to this Dr Sesay, who could not be present at the workshop, requested training in use of the ultrasound scanner. It is known that the present ultrasound scanner in Kambia does not work well and produces grainy pictures so if training in use of ultrasound were to be carried out a new USS machine would also be necessary. Basic ultrasound facilities at the hospital would be beneficial to patients as it could be used to confirm foetal position, multiple births and placental position; it could also be used to facilitate external cephalic version of breech babies. In addition to obstetric uses it could also be used for renal scans. Training could be conducted in the UK or in Kambia by a link member once the USS had been purchased. It was agreed that if a scanner was purchased and training conducted two members of staff from Kambia hospital should be trained and the scanner should be kept in a safe place. Reporting on the use of the scanner would also be needed to monitor the activity. A plan was produced during the workshop, which can be found in the appendix, in summary consists of:
• Identifying the nursing and medical staff to be trained in each area. • Identifying trainers from Kambia and the UK. • Formulation and use of pre and post training questionnaires. • Provision of training materials. • Implementation of training. • Among outcomes to be measured would be incidence of wound infection,
length of hospital stay, neonatal mortality rates and numbers of caesarean section and vontouse births.
Kambia Planning Visit Report. 31/5/09 - 11/6/09 22
TBA training and strengthening links between TBAs and Health Facilities. TBA training is not frowned upon in Sierra Leone and official government policy is to train them and encourage them to work in collaboration with the government health system. Dr SAS Kargbo said that when a TBA brings a woman to give birth at a PHU or hospital they are meant to get 50% of the money paid by the woman to the health facility. Both Dr Labour and Dr Sesay are in favour of working with TBAS. During the workshop, participants prioritised strengthening of the TBA system and links with the health facilities as a Must activity. Dr Labour informed us that there are 800 TBAs working in Kambia district and they attend 3000 births. He also said that women prefer TBAs as they are friendly and known to them. The PHUs and MCH aides are perceived as being less friendly and expensive. The TBAs of the Kambia appeal / link PHUs of Maselleh and Barmoi encourage women to give birth in the PHU with their assistance. In Barmoi we met with several TBAs who all said that women want to give birth in the PHU but sometimes distance prevents them and they give birth with the TBA at home, at other times their labours are so fast that there is not enough time to get to the PHU. The TBAs appeared to have a good relationship with Elizabeth and Salim Kabia, the MCH aides. Financially the TBAs said it was difficult for them as they are taken from their daily routine to deliver women and so they lose money, especially when they deliver babies at the PHU and are given only token money. To compensate for this they would like some sort of incentive and raised the idea of an income generation scheme to be run through the TBA association. They would like a cassava grater so that they can grow, process and then sell it. The cost of the machine is around 2,000,500 Le and they already have the land they need for growing the cassava. They also requested refresher training, TBA “top up” kits and uniforms for the TBAs without uniforms. There was also discussion of TBA kits being kept at the PHU to encourage them to bring women there to deliver, however there was no decision made on this.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 23
The picture above shows TBAs both in brown and white check uniforms and their own clothes standing with MCH aides Elizabeth and Salim Kabia at Barmoi PHU. In Maselleh we met with six TBAs. One TBA said that now they usually work from home. In their training they were told to work in the clinic and were “promised assistance” if they brought women to the PHU. However she said that the clinic has no equipment for them to use and they get no money when they bring women to the PHU. The other TBAs agreed with this and we were told by the MCH aide that the money women pay for birth only covers the drugs used and no more. These TBAs also requested refresher training, TBA kits and an income generation scheme. The scheme they suggested was for growing groundnuts. If they were given seeds they could grow the nuts and repay the seeds the following year, they could then sell the groundnuts locally. TBAs said they have enough land and just need the seeds. The seeds must be planted in April so it is now too late for this year but could be done next year. The TBAs stated that the details and seed numbers have already been provided to the KA appeal / link.
Plan A plan to strengthen the TBA system and links between TBAs and health facilities was formulated in the workshop (see appendix pp54) in it involves:
• TBA refresher training. summary • Provision of TBA kits and uniforms.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 24
• Strengthening of TBA associations. • Income generation activities for TBAs. • Community sensitisation to the importance of giving birth at a health
facility. • Agreement on user fee for delivery at PHU. • The primary outcome will be the number of births at PHUs.
Health Promotion: Care seeking behaviours for children under five and pregnant / labouring women. Two subjects where health education is needed became apparent during the visit. These were community recognition of danger signs in sick children and the importance of taking these children to the health facility before it is too late, and the benefits of antenatal care, knowledge of danger signs of pregnancy and birthing at a health facility. During the focus group discussions with men and women it was found that after the major barriers of cost and transportation to accessing care for pregnant and labouring women other barriers included fear and lack of knowledge. Whilst three of the women in focus group discussions said they gave birth at a health facility as they felt safer another three said they would not attend as they were scared of injections, another woman said she had heard hospital staff using “bad words” to labouring women and another that she would not go to the hospital, if she went to the hospital and laboured for a long time (3 hours or more) staff would perform a caesarean section that she would not need. Health education on the importance of tetanus toxoid immunisation and the benefits of labouring at a health facility may help with these problems. In both the men and women’s focus groups the majority of participants were unaware of the danger signs of pregnancy and were anxious to learn. It is very important that health education is given to men as well as women as in the men’s focus group it was said that it is husbands who decide on place of delivery. The senior hospital staff stated that the most common cause of children under five attending the hospital was malaria followed by typhoid and ARI. Staff said they are happy with their ability to treat children with these conditions. The biggest problem is that the children are brought to health facilities too late when their illness has already become serious. Delays include recognition of illness and a preference for treating with traditional herbs rather than seeking professional care. Health promotion to get sick children to the health facility earlier was deemed as a must activity during the workshop.
Plan Because there wasn’t enough time to complete the planning for this activity during the workshop, the planning was done quickly by Mr Deen and Sarah at

Kambia Planning Visit Report. 31/5/09 - 11/6/09 25
the end of the workshop (see appendix pp56). In summary it involves:
• Community sensitisation through meetings and radio about the danger signs of sickness in children and the importance of seeking professional care quickly.
• Formation of mothers clubs at PHUs. • Strengthening of PHU outreach services, including provision of bicycles to
enable staff to reach communities. • Bylaws about taking sick children to the PHU.
Water and Sanitation
Hospital water supply The hospital does not have a functioning water and sanitation system in place and this is obviously a hygiene concern. The hospital has a well, which contains enough water for most of the year but runs dry in March and April just before the start of the rainy season. To prevent this it needs to be dug deeper and the hospital have a plan in place to do this. The well is chlorinated on a regular basis. Roof rainwater collection containers can also be seen at the hospital. With regards to drinking water, a water purification unit was donated as a sample to the Kambia appeal / link and is currently used at the Kambia Appeal base. The hospital has previously been interested in obtaining these to provide drinking water to patients. Because this unit is run on electricity, it would be difficult to maintain if it breaks and would also need to be imported. Although it was suggested that bio filters would be more appropriate, Mr Abdul Deen the WAT/SAN coordinator said that filters do not tend to be used in Kambia but solar disinfection (where by water is placed in transparent plastic containers and exposed to sunlight) is. The use of solar disinfection of water by the hospital for drinking purposes could be investigated.
PHU water supply Both Barmoi and Maselleh PHU have working wells that are chlorinated on a regular basis. In Barmoi the well runs dry just before the rainy season. Barmoi PHU also utilise rainwater collection. Both PHUs said that villages in their catchment area do not all have access to safe drinking water. Isatu the MCH aide at Maselleh said that only two of the 19 villages covered by the PHU have access to safe drinking water, the others use unsafe sources such as rivers and streams. For the area covered by Barmoi PHU there are at least two wells that need repairing with covers and pumps.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 26
The picture above shows people collecting water from the pump well at Maselleh PHU.
Sanitation Sanitation was only discussed briefly and not raised as an area for which the district require help from the Kambia appeal/link. Both PHUs supported by the appeal have ventilated improved pit latrines although the new ones in Barmoi appear not to be used. Mr Deen said that communities in the district have been trained in how to make their own latrines but not every one did so.
Blue flag volunteers Previously Kambia was known as the “Gateway for Cholera”. This gate way has now been closed and the DHMT believe Blue Flag volunteers have contributed to this. Blue flag volunteers are trained to recognise, treat and advise on prevention of diarrhoea, cholera and other waterborne illnesses in their communities and are identified by a blue flag flying from the roof of their residences. They provide oral rehydration salts (ORS) and give advice on use of sugar/ salt solution. The blue flag volunteers in Kambia district have been around for about three years and are monitored by the DHMT. It has been about three years since initial training and some volunteers have left their communities. The need for active blue flag volunteers to receive refresher training and for replacement volunteers to be trained was highlighted by the DHMT. The refresher training programme is the same as initial training programme.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 27
Plan During the workshop a plan was made for improving the availability of safe drinking water and refresher training of blue flag volunteers (see appendix pp58) in summary it involves:
• Determining the number of volunteers to be trained • Emphasising that it is an ongoing programme so volunteers in each area
need to be trained / refreshed every three years. • Determining PHU water sources and maintenance of pumps. • Where possible providing safe water sources to PHUs that lack them. • Identifying areas suitable for rainwater harvesting. • Training pump caretakers. • Identifying funding sources. • The main outcome indicator will be incidence of diarrhoea in intervention
areas.
Health transportation system, bicycles, motorbike ambulances, maternity bus and maternity waiting home. In one of the male focus group discussions a man explained how his sister had died in labour with her second baby. She was living in Mambolo and could not get to the hospital as it was too far away. The TBAs at Barmoi also explained that for some women the PHUs are also too far away. Plans to tackle the transportation problems that women face when giving birth and that all community members face in an emergency are vital. The reproductive and child health strategy has some money available for transportation. However there is still a gap that the Kambia appeal /link could fill. The KA has set up an emergency transportation system designed for women in labour but which can be used for other emergencies at the PHU’s of Barmoi and Maselleh,. It consists of bicycles distributed to the communities served by the two health centres, if there is an emergency someone from the village cycles to the PHU and informs the motorbike ambulance driver who goes to pick up the patient and take them to either the PHU or the hospital.
Bicycles. Some bicycles had already been taken to Barmoi PHU and on our visit we took the rest. The community representatives were not clear about the purpose of the bicycles so it was explained to them and they agreed. At Maselleh, Ms Isatu Bangura the MCH aide distributed the bicycles to village heads during our visit. Because the bicycles have only just been distributed there is no feedback on their use.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 28
The provision of bicycles for use by PHU staff on outreach was suggested at several meetings by Ms Fujii, Dr Labour, and the DHMT. The Paramount Chief’s office was also in favour of this idea. Outreach activities include ANC, family planning, immunisation, STI treatment and health education on breastfeeding and wat/san issues.
Motorbike ambulances In Maselleh the ambulances are working very well, the community recognise their value as demonstrated by their contribution of 500 le a month per household for fuel and maintenance of the bikes. The MCH aide in Maselleh drives a bike herself. The bikes are already described as “life saving” and have been used to transport a patient with severe upper limb burns and another who had been bitten by a snake. Both were felt by the community to have had their lives saved by the Motorbike Ambulances. In Barmoi the system is not working so well: previously some villages had been contributing to the running costs but some had not. When the villages who were contributing found out that others were not but still had the service available to them they stopped too. Currently all three bikes are in store at the PHU and so a plan needs to be made with the community on how to get the scheme up and running. Evidence on use of the bikes also needs to be gathered and Mr Edward Sesay, the head of Barmoi PHU, said they would start to do this. In Barmoi the drivers would like some refresher training; two have been trained per bike and the MCH aides would also like to learn to use the bikes. They have difficulty with outreach as many villages are a long way away, so they requested one of the three bikes to be available for them to use on outreach. It was agreed this would be an acceptable use for one of the bikes. Drivers of ambulances at both PHUs requested waterproofs and mobile phones for use when the bikes break down or get stuck when transporting patients to and from the PHU or hospital. Moses Kabba has been given a mobile phone for this purpose already. The emergency transport system is to be evaluated by two medical students from the UK later this year. If proved of value, there was a request that the motorbike service should be expanded to all the CHCs.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 29
Above is a photo of the emergency transport system, bicycles and motorbike ambulance, of Maselleh PHU. With Isatu Bangura the MCH aide, village heads and a pregnant lady.
The Maternity Bus A Land Rover for transporting women near the end of their pregnancy from the PHUs to the hospital has been purchased by the Kambia appeal and the process of its importation to Sierra Leone is underway. However before it is used the following needs to be clarified.
• Who will own the vehicle? • Where will it be stored when not in use? • Will communities / PHUs be willing to contribute to its running costs? • What will be the route and how often will it go to different PHUs? • Will an MCH aide accompany the driver in case people need care on the
journey to the hospital?
Maternity waiting home. Mr Moses Kabba stated that there is interest in the setting up of a maternity

Kambia Planning Visit Report. 31/5/09 - 11/6/09 30
waiting house and that beds are currently being made on the Kambia Appeal base for use in the PHUs and the waiting house. The new BEmONC centres are relevant to the waiting homes, as instead of setting up just one home at the hospital the BEmONC centres could also provide a waiting home close to the villages. During the workshop the group all agreed that it would be better to set up one waiting home at the hospital as a pilot; if this worked well the idea could be expanded in the future to include BEmONC centres.
Plan During the workshop a plan for the maternity waiting home, emergency transport system and maternity bus was produced. The full plan can be found in the appendix (pp60). The emergency transport system will be led primarily by the Kambia appeal and the maternity bus and waiting home by the DHMT and Kambia appeal. In summary it includes:
• Sensitisation and education meetings on the use of the emergency transport system, the bus and waiting home.
• Acquiring / repairing accommodation. • Provision of vehicle / driver and running costs. • A protocol for use of the bus. • Monitoring use of present motorbike ambulance service to assess and see
if it should be expanded to other CHCs. • Provision of bicycles.
Major risk factors to this plan are high community expectations and reluctance to accept services.
Hospital Garage This is a potential programme idea that both Dr Sesay and Dr Labour are strongly in favour of. Currently the hospital and DHMT spend a lot of money on maintenance of their vehicles by private mechanics. The district council spoke about getting their own mechanic for the works department but this has not happened. The hospital has enough space to accommodate a garage and the mechanic could also help with maintenance of the hospital generator. It was suggested that the two doctors write a joint letter to the council requesting a garage. The Kambia appeal could be involved with helping to train the mechanic.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 31
Surgical and theatre support. In addition to the training of theatre staff as mentioned in the CPD section of this report, theatre instruments were also requested by the hospital. It was emphasised that these would need to be cared for properly and if provided there use and maintenance would need to be monitored. The senior hospital staff also requested that the second theatre be opened and equipped as it is very difficult to get patients from the obstetric department to the current theatre, and if the theatre were moved it would be difficult to get patients from the other wards to theatre.
Plan Whilst support to theatres was seen as a must activity by the workshop participants there was not enough time to make a plan during the workshop. A plan for provision of instruments and surgical support was made at a latter date, it did not involve hospital staff but was based on information gained during the meeting with senior hospital staff (for plan see appendix pp62). In summary it involves:
• Laparotomy kit and theatre drapes to be provided and checked by the Kambia appeal with a member of hospital staff assigned to be responsible for them.
• Theatre consumables to be provided by hospital procurement. • Assessment of the numbers and training needs of staff participating in
surgical activity and immediate post surgical care. • Training of CHOs to strengthen their surgical skills. • Training in theatre nursing and anaesthesia skills.
Surgical camps At the meeting for senior hospital staff surgical camps were discussed and it was emphasised that any such activity should include training as well as service provision. The example of a recent hernia repair camp was given. Hernia repair camps would be welcome in the future using appropriate techniques and with an emphasis on training. Vesico vaginal fistula repair camps were also discussed. VVF patients have previously been referred to the fistula hospital in Freetown, but with the opening of a fistula unit in Bo, where the CHOs have contacts, most are now being referred there. If there is felt to be a need for VVF repair services at the hospital, the fistula hospital in Freetown could be approached to see if they would be

Kambia Planning Visit Report. 31/5/09 - 11/6/09 32
willing to train hospital staff. Simple repairs could be carried out In Kambia, given the appropriate training. Cataract camps were also discussed as a possibility for the future and would need to be discussed with ophthalmologic colleagues in the UK and Sight savers in Sierra Leone. No plans were made during the visit with regard to surgical camps.
PHU Infrastructure
Barmoi PHU building The building of Barmoi PHU was renovated with help from the Kambia appeal two years ago. The new VIP latrines are locked and not being used, the incinerator has not been used as evidenced by its lack of ash and smoke staining of its chimney. Mr Edward Sesay, in charge of the PHU, said that the incinerator had not been used as someone told him it needed tiling; now he knows it can be used without tiles he will use it.
The above is a photo of the unused incinerator at Barmoi PHU.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 33
An additional building was requested for use by one of the MCH aides as currently not all staff can live on site. The PHU also requested a concrete fence to be put up around the facility, this request was refused at the meeting as not being a priority.
Solar fridges The solar fridge at Barmoi does not work well. The MCH aides check it regularly and as evidenced by the temperature chart on the fridge it is not cold enough. To be kept cold vaccines must be kept in the freezer section. When the weather is very sunny the fridge starts working and the MCH aides say they must quickly take the vaccines from the freezer compartment and put them in the fridge section. They are obviously paying close attention to the vaccines as despite the difficulties keeping them cold they are still viable and suitable for use (as indicated by the vaccine vial monitor) The DHMT says that many PHUs are having difficulties with their solar fridges as they break regularly and often need repairing. In the prioritising exercise of the workshop repairing / replacing these fridges was classed as a “must” activity.
Generator for Maselleh PHU Maselleh PHU does not have a generator and this causes problems when patients arrive at night as it means they have no light. Currently the PHU is borrowing a small generator from Moses Kabba. They would like a small generator and said that if one were provided they could cover fuel and maintenance costs from patient fees. No plans were made with regard to PHU infrastructure during the visit.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 34
Information and plans regarding operational issues of the partnership
This section covers the operational issues that affect the partnership and is broken down in to three sections. Communication between all partners, visits from the UK to Kambia and from Kambia to the UK and transparency of decision making and funding / financing issues.
Communications and decision making between all partners. There were many discussions about communication during the visit and it was found there were communication issues to be resolved between all partners. For Dr Sesay as the medical superintendent of the hospital and its only doctor he currently makes all the decisions about the hospital and finds this a difficult responsibility for one person alone. It also means he is blamed for unpopular decisions. This was discussed in a private meeting with him and the formation of a Hospital management committee was suggested. Dr Sesay felt this to be a good idea. Potential committee members could be Dr Sesay, CHO Mohamed Kamara, Sister Francess Pearce (hospital matron) and another senior hospital member of staff, such as the dispenser/pharmacist. This idea was then discussed at the DHMT meeting and no objections were raised. Regarding communication between Kambia and the UK, the DHMT and the hospital communicate to Moses Kabba who communicates to the UK link and Kambia appeal. This was felt to be time consuming and frustrating by some. To help resolve this it was agreed that the “Kambia Health Development Committee” would be set up with four members of staff from the hospital including Dr Sesay or CHO Mohamed, Matron, the senior laboratory technician and the pharmacist, Four members of staff from the DHMT including Dr Labour, one of the district health sisters and Mr Deen. It would also include Mr Moses Kabba as secretary and Ms Fujii from JICA. The committee would meet monthly on the first Wednesday of every month, minutes from the meeting would be ready by the Friday. Minutes would be shared with all committee members and sent to the GHNHSFT committee, who would then share them with partners in the UK. A similar committee in the UK already exists. Minutes from monthly meetings in the UK would also be shared with the Kambia Health Development Committee. It was also agreed that improved e-mail access in Kambia should be utilised to help with communications. Mr Moses Kabba can be contacted directly, although the present satellite-based system is costly, and DHMT can be contacted via e-

Kambia Planning Visit Report. 31/5/09 - 11/6/09 35
mail through JICA. A possible cheaper alternative is to access the internet via the mobile phone system. Once the JICA resource centre is up and running e-mail access for partners based on the hospital grounds will be greatly improved.
Visits from the UK to Kambia and from Kambia to the UK Visits of partners in both directions are important for planning, learning, monitoring and evaluation purposes as well as carrying out programme activities. Whilst Kambia hospital senior staff said they were happy to have people from the UK work at the hospital there was a need for better planning so that relevant people are aware of the reasons for their presence. It was also agreed that visits in both directions would be more effective if pre-departure briefings are given and orientation is provided on arrival. With regards to accommodation when visitors travel from Kambia to Cheltenham they are provided with accommodation and so this is not a problem. When visitors come from Cheltenham to Kambia they currently stay at the Kambia Appeal base. The base is a contentious issue as it is expensive and is seen as indicating to some that the Kambia appeal / link has more money than it actually does. If the base is let go there will be a need to find other suitable accommodation for UK visitors. During the workshop the following points about visits were agreed.
• There must be clear objectives and a TOR for every visit. • Pre-departure briefing and orientation on arrival should be provided. • UK health professionals who will work in Sierra Leone must register by
sending their papers (copies of GMC and professional insurance documents) to Moses Kabba along with a brief background about themselves and their skills. Mr Kabba would then write a covering letter, forward papers to appropriate people within the Ministry and share information with the Kambia health development committee.
Transparency of decision making and funding / financing issues. The formation of the Kambia Health Development committee should help with this. During the workshop the following was also agreed.
• Partners in Kambia should be aware that the main resource of the Kambia appeal and link is people and skills. Therefore expectations must be realistic.
• Financial reports from Kambia and the UK should be shared at partnership meetings. Estimates for funds should be followed by financial reports.
• Planning should involve stages of assessment i.e. funding for needs

Kambia Planning Visit Report. 31/5/09 - 11/6/09 36
assessment should come before other funding for activities. • Monitoring of all activities should be carried out. • Reports should go to donors when programmes are completed. • If contractors are hired they should be supervised by the DHMT,
community members, ward level councillors and committee members.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 37
Appendix


Kambia Planning Visit Report. 31/5/09 - 11/6/09 39

Kambia Planning Visit Report. 31/5/09 - 11/6/09 40

Kambia Planning Visit Report. 31/5/09 - 11/6/09 41

Kambia DHMT members Dr I.J Kargbo Labour District Medical Officer Dr David Sesay Medical Superintendent Sister Gladys Yavana District Health Sister I Sister Hawa Kallon District Health Sister II Mr A.B.Y. Bangura Health Superintendent Sister Francess Pearce Matron Sister Hawa Fofana MCH Aide Training Coordinator Mr M.C Massaquoi District Operation Officer/ EPI Mr Alusine Sesay Monitoring and Evaluation Officer Mr Hassa M Kanu DSMO/Assistant. M&E focal person Mr Abdul T Deen WATSAN Coordinator Mr Kalie H Kamara District Storekeeper / Logistic Officer Mr Alieu B Sheriff District Pharmacist Technician Mrs Beatrice Nabiey District Finance Officer Mr Amara Brima NMCP Focal Person Mr Alusine Kamara HIV/AIDs Councillor Mr Ishmael Rogers NOCP Focal Person / Chairman PHUs Association Mr I A T Kamara Public Relation Officer Mr Anthony Sesay Births and Deaths Registrar Mr Sheku Samba NLTCP Field Supervisor Mr Moses Kabba Kambia Appeal / Link representative.
Bar chart showing admissions, discharges and deaths from 19/1/09-25/5/09 at Kambia Hospital.

Kambia Planning Visit Report. 31/5/09 - 11/6/09 43
Participants of the Kambia Health Partnership Prioritising and Planning Workshop. Monday 8th June 2009 Name Position Richard Kerr – Wilson
Kambia Appeal Representative
David Holmes Kambia –GHNHSFT Link Moses Kabba Kambia Appeal – SL Office Mohamed Kamara Government Hospital Kambia CHO Hawa Kallon DHMT Kambia, District Health sister Gladys A Sisay DHMT Kambia, District Health Sister Francess Pearce Matron Kambia Hospital Haja Fatama D Bangura Zonal Supervisor Education Office Nabien Yaya Yillah Councillor Kambia D C Foday Tarawally Social Worker. Ministry of social
welfare. Abdul T Deen Wat/San Coordinator, DHMT, Kambia Hawa Fofonah Training coordinator Kambia Chiemi Fujii JICA project expert Ibrahim AS Kamara (AKA FT) Kambia Appeal Paramount chief M.S Sesay Chiefdom Administration Khalil A I Kamara Kambia Appeal volunteer Sarah Williams Facilitator

Kambia Planning Visit Report. 31/5/09 - 11/6/09 44
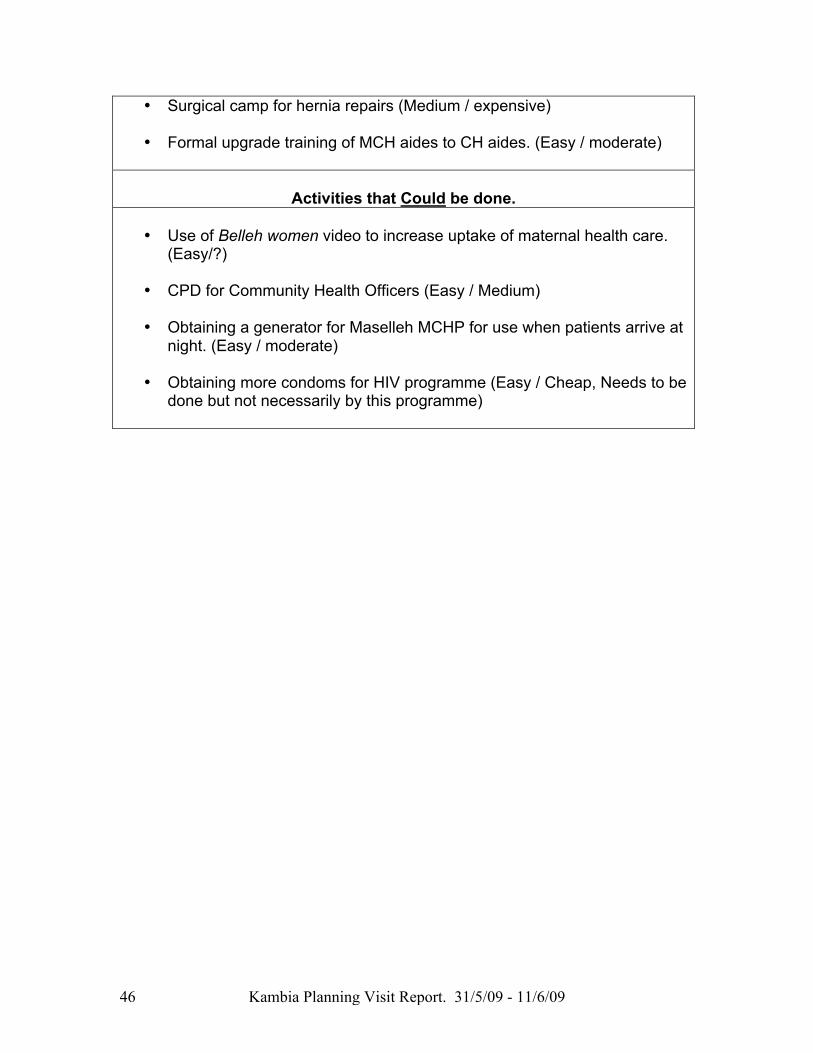
Workshop Activity Prioritisation Table This table shows whether workshop participants thought activities discussed during the visit were activities that must be done, should be done or could be done. In brackets is whether the activity was deemed as easy or difficult to do followed by its expense or inexpensive.
Activities that Must be done.
• CPD Neonatal resuscitation. (easy/expensive if training supplied from
GHNHST)
• Training of midwives in Vacuum extraction. (easy/expensive if training supplied from GHNHST
• CPD adult resuscitation. (easy/expensive if training supplied from
GHNHST
• CPD anaesthetic training (easy / moderate - expensive)
• CPD training for theatre / scrub nurses (Easy / expensive)
• CPD obstetric emergency training (Easy / expensive)
• Refresher training for blue flag volunteers. (Easy / moderate - expensive)
• The maternity bus for transferring obstetric and other patients from CHCs to the hospital. (Difficult /expensive)
• Pilot maternity waiting home to be established and assessed at the
hospital with the option of expanding the idea to CHCs in the future. (Difficult / moderate- expensive)
• The emergency transport system motorbike ambulances and bicycles.
(Difficult / moderate - expensive)
• Training of hospital volunteers (Easy / moderate if training is supplied locally)
• Formal upgrade training of hospital volunteers to nurse aides (easy /
expensive)
• Formal training of SECHNs (easy/ expensive)

Kambia Planning Visit Report. 31/5/09 - 11/6/09 45
• Strengthening the TBA system and links between TBAs and health facilities (easy/ expensive)
• Improving the availability of safe drinking water (difficult / expensive)
• Health promotion so that sick children under the age of five are referred
to health facilities before it becomes too late. (Easy / medium)
• CPD Caesarean section training (Medium / medium)
• Maintenance / rehabilitation/ replacement of solar fridges in some PHUs (Difficult /expensive)
• Obtaining theatre kits / instruments (Easy / expensive)
• Obtaining basic equipment for PHUs (Medium / expensive)
• Gap in services of chiefdom who will not receive the BEmONC package
(difficult / expensive)
• Making hospital, maternal and newborn care health services more affordable.
• Health promotion so that sick children under the age of five are referred
to health facilities before it becomes too late.
Activities that Should be done. • • CPD Training in use of ultrasound scanner for obstetrics and provision of
scanner. (Difficult / expensive)
• Formal training of more MCH aides (Easy / Expensive currently happening)
• Two way communication between PHU and hospital regarding referred
patients (Easy / Cheap)
• Establishment of a garage on the hospital grounds to maintain and repair hospital and district health vehicle and generators. (Difficult / Expensive)
• Formal training of Environmental Health Officers. (Easy / Expensive)
• Provision of bicycles to PHUs for use on outreach (Easy/ moderately
expensive)
Kambia Planning Visit Report. 31/5/09 - 11/6/09 46
• Surgical camp for hernia repairs (Medium / expensive)
• Formal upgrade training of MCH aides to CH aides. (Easy / moderate)
Activities that Could be done.
• Use of Belleh women video to increase uptake of maternal health care. (Easy/?)
• CPD for Community Health Officers (Easy / Medium)
• Obtaining a generator for Maselleh MCHP for use when patients arrive at
night. (Easy / moderate)
• Obtaining more condoms for HIV programme (Easy / Cheap, Needs to be done but not necessarily by this programme)





























