Embed Size (px)
Citation preview

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 1/27
JURNAL READING
UPDATED MANAGEMENT STRATEGIES FOR MASTOIDITIS AND
MASTOID ABSCESS
OLEH :
Maulan Saputra, S.Ked (J 500 080 112)
Ayu Rahimah, S.Ked (J500 080 093)
Ayu Wulan Sari, S.Ked (J 500 080 070)
PEMBIMBING :
dr. Made Jeren, Sp.THT
KEPANITERAAN KLINIK ILMU PENYAKIT THT
RSUD DR. HARJONO PONOROGO
FAKULTAS KEDOKTERAN
UNIVERSITAS MUHAMMADIYAH SURAKARTA
2012

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 2/27
1
UPDATED MANAGEMENT STRATEGIES FOR MASTOIDITIS
AND MASTOID ABSCESS
M. Abdel Raouf, B. Ashour *, A. Abdel Gawad
Ear, Nose and Throat Dept., Cairo University Hospital, Cairo, Egypt
Received 16 February 2012; accepted 19 March 2012
Available online 17 April 2012
Egyptian Journal of Ear, Nose, Throat and Allied Sciences (2012) 13, 43 – 48
ABSTRACT
Abstract Mastoiditis remains a problem in Egypt. Despite the widespread use
of antibiotics for otitis media, many patients still present with complications.
Treatment options for mastoiditis vary from simple incision and drainage of the
tympanic membrane to radical mastoidectomy.
There seems to be no unanimous agreement on the best management strategy
for this problem. In this study, we will review various management protocols for
mastoiditis and mastoid abscess. Along with our experience with 12 cases of
mastoiditis and mastoid abscess, we will propose our own management guidelines
summarized in an easily accessible flowchart.
1. INTRODUCTION
Some level of mastoid involvement is expected in any inflammation of themiddle ear. Acute mastoiditis may spread through the periosteum and induce
periostitis, which may cause bone destruction (acute coalescence mastoiditis). The
infection may progress through adjacent bones or through emissary veins beyond the

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 3/27
2
mastoid air cells and may present as a subperiosteal abscess or an intracranial
complication.1
Acute mastoiditis involves the formation of pus and only occurs in cellular
mastoids. Chronic mastoiditis is a slow penetration of acellular bone by granulations
accompanied by hyperaemic decalcification of bone. In most cases otitis media is
concurrent either acute or chronic.2
Some patients may present with a postauricular fistula which may be
spontaneous or iatrogenic. It may persist to become a chronic fistula. With the advent
of broad spectrum antibiotics, the clinical course of middle ear disease has been
altered. One result has been the occasional suppression of the presenting signs and
symptoms of mastoiditis. The course may be so insidious that the first awareness of
mastoiditis may be following the presentation of an intracranial complication such as
meningitis, lateral sinus thrombosis, or brain abscess.3
According to Dudkiewicz dkk., the incidence of acute mastoiditis in patients
with acute otitis media (AOM) has dropped from 50% at the turn of the 20th century
to 6% in 1955 and to 0.4% in 1959, by 1993, only 0.24% of patients with acute otitis
media (AOM) developed acute mastoiditis.1
Petersen dkk. reported a decline in the incidence of acute mastoiditis from
20% in 1938 to 2.5% in 1945. Acute mastoiditis has become rare, approaching 0%. It
is, however, uncertain whether this is directly associated with the antibiotics or if an
altered nature of the disease/microorganisms and/or the state of health is involved.4
There is evidence that the incidence of acute mastoiditis hasrecently been
rising again; this phenomenon could be due to the increasing antibiotic resistance of
microorganisms like Streptococcus to penicillin.5
Streptococcus pneumoniae, Streptococcus pyogenes, Staphylococcus aureus
and Haemophilus influenzae are the most common organisms recovered in acute
mastoiditis. Pseudomonas aeruginosa, Enterobacteriaceae and S. aureus are the
predominant isolates that have been recovered from chronically inflamed mastoids.
The role of P. aeruginosa in many of these cases is questionable because it colonizes

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 4/27
3
the external ear canal and can contaminate specimens obtained through the non-sterile
ear canal. Some reports described the recovery of anaerobes, including Bacteroides
species, from cases of chronic mastoiditis in children.6
2. MATERIALS AND METHODS
This study was conducted on patients who presented with mastoiditis or
mastoid abscess to the ENT Department at Cairo University Hospital between June
2007 and June 2009. One patient presented with a mastoid abscess and postauricular
fistula but was lost to follow up.
This study included 12 patients, 8 males and 4 females. The age ranged
between 2 and 23 years with a mean age of 11.5 years.
All the patients were subjected to the following assessment protocol:
1. Full otologic examination.
2. Culture and sensitivity obtained for patients who did not receive previous antibiotic
therapy.
3. CT scan, in cases of a suspected complication, MRI was performed.
4. Neurosurgical consultation when needed to exclude any intracranial complications.
Patients were treated with either medical or surgical treatment or both
according to their presentation.
2.1. Medical treatment
Patients were hospitalized and given empiric parenteral antibiotics. Antibiotics were
modified according to the results of culture and sensitivity.
2.2. Surgical treatment
- Minimally invasive procedures: Incision and drainage of the mastoid abscess
and Myringotomy.
- Definitive surgery: cortical, radical or modified radical mastoidectomy was
performed according to pathology, patient presentation and age. The Patients
were followed up after 1, 3 and 6 months.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 5/27
4
3. RESULTS
Patients were classified according to their presentation into the following groups:
1. Cases with mastoid abscess: There were nine cases; these cases were
classified according to aetiopathology into the following groups.
a. Acute otitis media: There were three cases. Two of them were below 5
years of age. These patients presented with antritis (Fig. 1) since the
mastoid process is not fully pneumatized at this age, they were treated
with medical treatment in addition to incision and drainage of the abscess.
The third case received medical treatment followed by cortical
mastoidectomy.
b. Cholesteatoma: There were five cases, two of them presented with a
complication (one with sigmoid sinus thrombosis and the other with an
extradural abscess). All cases were treated with open mastoidectomy in
addition to the treatment of the complication in the two complicated cases.
c. Safe chronic suppurative otitis media: We saw one case which was treated
with medical treatment in addition to incision and drainage of the abscess.
Later on after acute inflammation had subsided, tympanoplasty with
cortical mastoidectomy was performed.
2. Cases with mastoiditis: There were three cases; they were classified according
to aetiopathology into the following groups.
a. Acute otitis media: There were two cases. One of them was complicated
with facial nerve paralysis and was treated with cortical mastoidectomy
and myringotomy in addition to medical treatment. The other non
complicated case was given medical treatment alone.
b.
Safe chronic suppurative otitis media: One case was seen and treated with
medical treatment and later on after infection subsided, tympanoplasty
with cortical mastoidectomy was done.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 6/27
5
CT scans were performed for all cases, MRI was performed in complicated
cases only. All patients showed marked improvement after the treatment regimens
previously described. No detectable recurrence of mastoiditis or mastoid abscess or
any complication was recorded during follow-up.
Mastoiditis and mastoid abscess have become a rare clinical occurrence. The
small number of cases included in our study precludes statistical analysis (Charts 1 –
3).
4. DISCUSSION
Egypt is a developing nation and many of its citizens still do not have access
to adequate healthcare. Although the incidence of mastoiditis and mastoid abscess has
declined in most developed nations, we still continue to see many cases.
In this study, all cases with mastoid abscess required some sort of surgical
intervention, either by incision and drainage or by definitive surgery (cortical orradical mastoidectomy).
Incision and drainage is considered sufficient below 2 years of age because
the mastoid is not fully pneumatized below the age of 5 (antritis only). Also,
definitive surgery may be postponed until infection subsides in cases with safe

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 7/27
6
chronic suppurative otitis media to allow better healing. This is similar to conclusions
previously reported by Tarantino dkk.,5 who stressed the need for surgical drainage
of a subperiosteal abscess in order to prevent the spread of suppuration to vital areas.
Reported mastoidectomy rates in clinical studies have shown large variations,
ranging from 12% to 98%. The large variability suggests that the decision for or
against mastoidectomy is not only a question of preferred conservative treatment or
immediate surgical intervention, but to a large extent based on subjective surgical
criteria.7
Mastoidectomy is an effective treatment for acute mastoiditis associated with
one of the following: subperiosteal abscess or exteriorization, cholesteatoma,
intracranial complications and otorrhea persisting for more than 2 weeks despite
adequate antibiotic treatment or in children <15 kg of weight.8
In this study, one of the three patients presenting with mastoiditis was treated
medically, the other two cases required surgical treatment because one of them was
complicated and the other presented with safe chronic suppurative otitis media. This
is similar to the study conducted by Tarantino dkk.,5 who stated that the criteria for
conservation are absence of toxic appearance or signs complications; absence of
postauricular fluctuation and absence of CT signs of mastoid bone cell destruction.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 8/27
7
5. CONCLUSION
After reviewing the literature and from our experience in recent years, we
concluded that the management of mastoiditis and mastoid abscess requires clear
guidelines. We propose the following guidelines in order to standardize the
management strategy both in the diagnostic and in the treatment phases.
5.1. Diagnosis guidelines
1. Full otologic examination should be performed to identify the signs of mastoiditis
which are otalgia, fever, proptosis of the auricle, erythema, and disappearance of
the retroauricular sulcus. The posterosuperior wall may sag in the external auditory
canal. There may or may not be otorrhea, but its absence does not exclude
mastoiditis and the tympanic membrane is usually inflamed and thickened and
may also be perforated with mucopurulent otorrhea.
2. Culture and sensitivity should be obtained for patients who have not received
previous antibiotic therapy. Specimens are collected during tympanocentesis or
surgery, and should be promptly sent to the microbiology laboratory on
appropriate media. The samples should not be taken from the external auditory
canal to avoid contamination.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 9/27
8
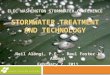
3. CT scan (Fig. 2) is considered the imaging modality of choice for patients with
acute mastoiditis. CT images should be obtained in every patient with acute
mastoiditis. If a complication is detected, MRI should follow. CT should be
repeated if improvement is inadequate or incomplete and to detect any
complications that may arise during hospitalization.
4. The diagnosis should be made with cooperation between the clinical pathology
department, the radiodiagnosis team and if required, neurosurgical consultation to
exclude any intracranial complication.
Figure 2 Coronal CT scan showing a mastoid abscess with bone destruction.
5.2. Treatment guidelines
1. Medical treatment:
a. Indications:
Absence of toxic appearance or signs of intracranial involvement that
point towards complicated mastoiditis.
Absence of postauricular fluctuation. Absence of CT signs of mastoid bone cell destruction.
Safe type of suppurative otitis media and absence of cholesteatoma.
b. Methods:

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 10/27
9
Administration of parenteral antibiotic therapy: Culture and
sensitivity should be obtained prior to therapy and antibiotics should be
modified according to the organisms recovered and their susceptibility.
Gram-stain preparation of the specimen can provide initial guidance for
the empirical choice of antimicrobial therapy.
The empiric antibiotics given were 3rd generation cephalosporin
(e.g. cefotaxime) and metronidazole. The antibiotics were given
intravenously 1gm/12 h for adults and half the dose was given for
children.
2. Surgical treatment:
a. Indications:
Intracranial complications.
Evidence of postauricular fluctuation and subperiosteal abscess.
Diagnosis of acute coalescent mastoiditis.
Failure of medical therapy programme despite adequate antibiotic
treatment for 48 – 72 h.
Otorrhoea persisting for more than 2 weeks despite adequate antibiotictreatment.
Cholesteatoma.
b. Methods:
1. Minimally invasive procedures:
a. Incision and drainage of the mastoid abscess: Incision and drainage
(I&D) should be performed as soon as fluctuation appears. The
incision should be in line with any future surgical incisions. Hilton’s
method is used to open all the abscess loculi and to achieve complete
drainage of the pus. A pack of gauze soaked with Betadine can be
placed in the abscess cavity and changed daily with wound nursing.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 11/27
10
b. Myringotomy: with or without tympanostomy tube placement. It
should be considered as an established treatment in every case of
mastoiditis with an intact tympanic membrane or inadequate
drainage.
2. Definitive surgery:
If cholesteatoma is present, an open mastoidectomy should be
performed.
If cholesteatoma is not found, cortical mastoidectomy is the best
choice.
A postauricular fistula (Fig. 3) should be followed through the mastoid and
totally excised, the skin edges should be freshened, undermined and carefully sutured
in 2 layers. The timing of surgery depends mainly on the patient’s condition and his
response to the medical treatment. If the patient is deteriorating, surgery should be
carried out promptly to save the patient’s life.
However, if the patient’s response to medical treatment is good, as evidenced
by clinical improvement and a follow-up CT scan, the surgery may be postponed for
one week to avoid perichondritis.
Figure 3 Postauricular fistula.
5.3. Guidelines of management of mastoid abscess according to aetiopathology
1. Acute coalescent mastoiditis without abscess formation.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 12/27
11
Treatment is mainly medical in the form of intravenous antibiotics
according to culture and sensitivity.
Myringotomy is needed in cases with insufficient drainage e.g. intact
drum or small high perforation.
Treatment of the cause e.g. acute suppurative otitis media
2. Acute coalescent mastoiditis presenting with a complication e.g. facial nerve
paralysis or intracranial complications e.g. lateral sinus thrombophlebitis.
Treatment is mainly surgical under cover of broad spectrum intravenous
antibiotics.
Treatment of the cause.
Intracranial complications such as brain abscess or meningitis should be
co-managed with the neurosurgery department with priority going to the
neurosurgery. When the patient is neurologically stable, management of
the ear disease can be addressed.
3. Acute mastoiditis with postauricular abscess.
Treatment is surgical in the form of cortical mastoidectomy after medical
preparation with intravenous antibiotics.
In unfavourable circumstances, the abscess may be incised and drained
followed a few days later by mastoidectomy.
Treatment of the cause.
4. Acute mastoiditis complicating safe type of chronic suppurative otitis media.
Medical treatment similar to acute suppurative otitis media.
Treatment of the cause after the abscess has resolved e.g. tympanoplasty
with cortical mastoidectomy.5. Acute mastoiditis on top of unsafe type of chronic suppurative otitis media
(cholesteatoma).
Treatment is surgical in the form of open mastoidectomy under cover of
intravenous broad spectrum antibiotic.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 13/27
12

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 14/27
13

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 15/27
14
STRATEGI PENATALAKSANAAN TERKINI pada
MASTOIDITIS dan ABSES MASTOID
ABSTRAK
Mastoiditis merupakan masalah tetap di Mesir. Kendati penggunaan beberapa
antibiotik secara luas untuk otitis media, banyak pasien yang masih mengalami
komplikasi. Pilihan pengobatan untuk mastoiditis ada berbagai macam dari insisi
ringan dan drainase membran tympani sampai radikal mastoidektomi.
Hal tersebut nampaknya menjadi persetujuan yang belum disepakati pada
strategi penatalaksanaan terbaik untuk masalah ini.
Pada penelitian ini, kami akan meninjau berbagai protokol penatalaksanaan
untuk mastoiditis dan abses mastoid. Sejalan dengan penilitian kami pada 12 kasus
mastoiditis dan abses mastoid, kami akan mengajukan pedoman penatalaksanaan
kami yang diringkas dalam diagram/grafik yang dapat di akses dengan mudah.
1. PENDAHULUAN
Ada beberapa tingkat keterlibatan mastoid dalam terjadinya inflamasi telinga
bagian tengah (middle ear ). Mastoiditis akut bisa menyebar melalui periosteum dan
menginduksi periostitis yang bisa menyebabkan destruksi tulang (mastoiditis
koalesen akut). Infeksi dapat berkembang melalui tulang-tulang yang berdekatan atau
melalui pembuluh emisari (emissary veins) di luar sel-sel udara mastoid dan bisa
hadir sebagai abses subperiosteal atau komplikasi intrakranial.
Mastoiditis akut melibatkan pus dan hanya terjadi dalam mastoid selular.
Mastoiditis kronis merupakan penetrasi lambat dari tulang aselular dengan granulasi
yang disertai dengan dekalsifikasi hiperemik tulang. Dalam sebagian besar kasus,
otitis media akut atau kronis sering terjadi bersamaan.
Beberapa pasien bisa datang dengan fistula postaurikular yang bersifat
spontan atau iatrogenik. Fistula ini dapat bertahan lama menjadi fistula kronis.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 16/27
15
Dengan penemuan berbagai macam antibiotik, jalur klinis penyakit telinga
bagian tengah (middle ear disease) telah berubah. Salah satu akibatnya adalah supresi
yang terkadang terjadi pada tanda-tanda yang hadir pada simptom mastoiditis. Jalur
ini boleh jadi tersembunyi dan berbahaya sehingga kesadaran pertama mengenai
mastoiditis akan muncul setelah hadirnya komplikasi intrakranial seperti meningitis,
trombosis sinus lateral, atau abses otak.
Menurut Dudkiewicz dkk., insidensi mastoiditis akut pada pasien dengan
acute otitis media (AOM) menurun dari dari 50% pada peralihan abad 20 sampai 6%
pada tahun 1955 dan sampai 0,4% pada tahun 1959, pada tahun 1993, hanya 0,24%
dari pasien AOM mengembangkan mastoiditis akut.
Petersen dkk. melaporkan penurunan insidensi mastoiditis akut dari 20% pada
tahun 1938 sampai 2,5% pada tahun 1945. Mastoiditis akut telah jarang, dan
mendekati 0%. Namun, tidak jelas apakah hal ini berhubungan secara langsung
dengan antibiotika atau tidak, atau apakah sifat yang berubah dari penyakit atau
mikroorganisme dan/atau keadaan kesehatan terlibat atau tidak.
Terdapat bukti bahwa insidensi mastoiditis akut baru-baru ini meningkat lagi;
fenomena ini dapat diakibatkan oleh peningkatan resistensi antibiotik dari
mikroorganisme seperti Streptococcus terhadap penicillin.
Streptococcus pneumoniae, Streptococcus pyogenes, Staphylococcus aureus
dan Haemophilus influenzae adalah organisme yang paling umum yang ditemukan
dalam mastoiditis akut. Pseudomonas aeruginosa, Enterobacteriaceae dan S. aureus
adalah isolat yang dominan yang telah dipulihkan dari mastoid yang terinflamasi
secara kronis. Peran P. aeruginosa dalam banyak dari kasus ini dapat dipertanyakan
karena organisme mengkolonisasi kanal telinga di bagian luar dan dapat
mengkontaminasi spesimen yang diperoleh melalui kanal telinga yang tidak steril.
Beberapa laporan telah mendeskripsikan penemuan anaerob, seperti spesies
Bacteroide, dari kasus mastoiditis kronis pada anak-anak.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 17/27
16
2. BAHAN DAN METODE
Penelitian ini dilakukan pada pasien yang datang dengan abses mastoiditisatau mastoid ke ENT Department di Cairo University Hospital antara bulan Juni 2007
sampai Juni 2009. Salah satu pasien datang dengan abses mastoid dan fistula
postaurikular, tetapi hilang dari tindakan lanjutan.
Penelitian ini menginklusi 12 pasien, 8 pria dan 4 wanita. Usianya berkisar
antara 2 sampai 23 tahun dengan usia rata-rata 11,5 tahun.
Semua pasien harus mengikuti protokol penilaian berikut:
1. Pemeriksaan otologis penuh.
2. Kultur dan sensitivitas yang diperoleh untuk pasien yang tidak menerima terapi
antibiotik sebelumnya.
3. CT scan, bila dicurigai terjadi komplikasi, MRI dilakukan.
4. Konsultasi bedah syaraf bila diperlukan untuk mengeksklusi komplikasi
intrakranial apa pun.
Pasien diperlakukan dengan perlakuan medis atau bedah atau keduanya sesuai
dengan kehadiran mereka.
2.1. Terapi medis
Pasien diopname dan diberi antibiotik parenteral empiris. Antibiotik
dimodifikasi sesuai dengan hasil kultur dan sensitivitas.
2.2. Terapi bedah
- Prosedur invasif minimal: Irisan dan pengeluaran abses mastoid dan
Miringotomi.
- Bedah definitif: Mastoidektomi kortikal, radikal atau radikal modifikasi
dilakukan sesuai dengan patologi, presentasi pasien, dan usia.
Pasien difollow up sampai setelah 1, 3 dan 6 bulan.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 18/27
17
3. HASIL
Pasien diklasifikasikan menurut presentasi pasien ke dalam berikut kelompok :
1) Kasus dengan abses mastoid: Ada sembilan kasus, kasus ini diklasifikasikan
menurut etiopatologi ke dalam kelompok.
a. Otitis media akut : Ada tiga kasus, dua dari kasus berusia di bawah 5
tahun. Pasien-pasien ini dengan antritis (Gambar 1) karena proses mastoid
tidak sepenuhnya membentuk rongga kecil berisi udara pada usia ini,
pasien diobati dengan pengobatan medis selain insisi dan drainase abses.
Kasus ketiga mendapat perawatan medis disertai dengan mastoidektomi
kortikal.
b. Cholesteatoma : Ada lima kasus, dua dari kasus dengan komplikasi (satu
dengan trombosis sinus sigmoid dan lainnya dengan abses ekstradural).
Semua kasus diobati dengan mastoidektomi terbuka selain pengobatan
komplikasi dalam dua kasus yang rumit.
c.
Otitis media supuratif kronis yang aman : terdapat satu kasus yang diobati
dengan pengobatan medis selain insisi dan drainase abses. Kemudian
setelah peradangan akut mereda, dilakukan timpanoplasti dengan kortikal
mastoidektomi.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 19/27
18
2) Kasus dengan mastoiditis: Ada tiga kasus, kasus ini diklasifikasikan menurut
etiopatologi ke dalam kelompok.
a. Otitis media akut : Ada dua kasus. Satu kasus merupakan kasus yang
rumit dengan kelumpuhan saraf wajah, pada kasus ini dilakukan kortikal
mastoidektomi dan miringotomi di samping pengobatan medis. Kasus
lainnya yang tidak rumit hanya diberikan pengobatan non medis.
b. Otitis media supuratif kronis aman: Salah satu kasus dilihat dan diobati
dengan pengobatan medis dan kemudian setelah infeksi mereda,
dilakukan timpanoplasti dengan kortikal mastoidektomi.
CT scan dilakukan pada semua kasus, MRI hanya dilakukan dalam kasus-
kasus yang rumit saja.
Semua pasien yang menunjukkan perbaikan ditandai setelah rejimen
perawatan yang telah dijelaskan sebelumnya. Pasien Ttdak kambuh terdeteksi dari
mastoiditis atau abses mastoid atau komplikasi apapun yang tercatat selama masa
follow-up.
Mastoiditis dan abses mastoid telah menjadi kejadian klinis yang langka.
Sejumlah kecil kasus yang termasuk dalam penelitian menghalangi analisis statistik
(Grafik 1-3).

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 20/27
19
4. DISKUSI
Mesir merupakan negara berkembang dan banyak warganya yang masih
tidak memiliki akses pelayanan kesehatan yang memadai. Meskipun kejadian
dari mastoiditis dan abses mastoid menurun di sebagian besar negara
berkembang, tapi terlihat masih banyak kasus yang terjadi.
Dalam studi ini, semua kasus dengan abses mastoid memerlukan
beberapa macam intervensi bedah, baik dengan insisi dan drainase atau dengan
operasi definitif (kortikal atau radikal mastoidektomi).
Insisi dan drainase dianggap cukup dilakukan pada usia dibawah 2 tahun
karena mastoid tidak sepenuhnya membentuk rongga kecil berisi udara dibawah
usia 5 tahun (antritis saja). Selain itu, operasi definitif dapat ditunda sampai
infeksi reda pada kasus dengan otitis media supuratif kronis yang aman untuk

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 21/27
20
memungkinkan penyembuhan yang lebih baik. Ini sesuai dengan kesimpulan
sebelumnya yang dilaporkan oleh Tarantino dkk.,5
yang menekankan perlunya
drainase bedah dari abses subperiosteal untuk mencegah penyebaran supurasi ke
daerah yang vital.
Dalam studi klinis tingkat mastoidektomi dilaporkan menunjukkan
variasi yang besar, berkisar antara 12% sampai 98%. Besar variabilitas
menunjukkan bahwa keputusan untuk atau tidak melakukan mastoidektomi tidak
hanya soal pengobatan konservatif atau intervensi bedah segera, tetapi sebagian
besar berdasarkan pada kriteria bedah subjektif.7
Mastoidektomi merupakan pengobatan yang efektif untuk mastoiditis
akut terkait dengan salah satu, yaitu : abses subperiosteal atau eksteriorisasi,
cholesteatoma, komplikasi intrakranial dan otorrhea yang bertahan selama lebih
dari 2 minggu meskipun dengan pengobatan antibiotik yang adekuat atau pada
anak-anak <15 kg BB.8
Dalam penelitian ini, satu dari tiga pasien dengan mastoiditis dirawat
medis, dua kasus lainnya memerlukan pengobatan bedah karena salah satu kasus
merupkan kasus yang rumit dan kasus lain dengan otitis media supuratif kronis
yang aman. Hal ini sesuai dengan penelitian yang dilakukan oleh Tarantino dkk.,
5 yang menyatakan bahwa kriteria untuk konservasi adalah tidak adanya
gambaran toksik atau tanda-tanda komplikasi, tidak adanya fluktuasi
postaurikular dan tidak adanya tanda-tanda CT dari dekstruksi sel tulang
mastoid.
5. KESIMPULAN
Setelah mengkaji literatur dan dari pengalaman kami dalam beberapa tahun
terakhir, kami menyimpulkan bahwa penatalaksanaan mastoiditis dan abses mastoid
membutuhkan pedoman yang jelas. Kami mengusulkan pedoman berikut dalam

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 22/27
21
rangka standarisasi strategi penatalaksanaan baik dalam diagnostik maupun dalam
tahap pengobatan.
5.1. Pedoman diagnosis
1. Pemeriksaan otologic secara menyeluruh harus dilakukan untuk mengenali
tanda-tanda mastoiditis seperti otalgia, demam, proptosis dari auricula,
eritema, dan hilangnya sulkus retroauricular. Dinding posterosuperior
mungkin mengendur di saluran pendengaran eksternal. Otorrhea mungkin ada
tapi mungkin juga tidak, namun ketiadaannya tidak menyingkirkan
mastoiditis dan membran timpani biasanya meradang dan menebal dan
mungkin juga berlubang dengan otorrhea mukopurulen.
2. Kultur dan sensitivitas harus diperoleh untuk pasien yang belum menerima
terapi antibiotik sebelumnya. Spesimen dikumpulkan selama t ympanocentesis
atau operasi, dan harus segera dikirim ke laboratorium mikrobiologi pada
media yang tepat. Sampel tidak boleh diambil dari saluran pendengaran
eksternal untuk menghindari kontaminasi.
3. CT scan dianggap sebagai modalitas pencitraan pilihan untuk pasien dengan
mastoiditis akut. CT Scan harus didapatkan dari setiap pasien dengan
mastoiditis akut. Jika komplikasi terdeteksi, maka harus dilakukan MRI. CT
Scan harus diulang jika perbaikan tidak adekuat atau tidak lengkap dan untuk
mendeteksi adanya komplikasi yang mungkin timbul selama rawat inap.
4. Diagnosis harus dilakukan melalui kerjasama antara departemen patologi
klinik, tim Radiodiagnosis dan jika diperlukan, konsultasi bedah saraf untuk
menghindari komplikasi intrakranial.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 23/27
22
Gambar 2. Coronal CT scan menunjukkan abses mastoid dengan kerusakan
tulang
5.2. Pedoman Pengobatan
1. Terapi Medis:
a. Indikasi :
- Tidak ada tanda keracunan atau tanda keterlibatan intrakranial yang
menunjuk ke arah mastoiditis rumit- Tidak adanya fluktuasi postauricular
- Tidak adanya tanda-tanda CT kerusakan sel tulang mastoid
- Otitis media supuratif yang aman dan tidak adanya cholesteatoma
b. Metode:
Tata cara terapi antibiotik parenteral: kultur dan sensitivitas harus
diperoleh sebelum terapi dan antibiotik harus disesuaikan dengan
kerentanan dan pemulihan suatu organism. Persiapan pewarnaan Gram
untuk spesimen dapat memberikan pedoman awal untuk pilihan empiris
terapi antimikroba.
Antibiotik empiris yang diberikan adalah sefalosporin generasi ke-3
(misalnya sefotaksim) dan metronidazol. Antibiotik diberikan secara

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 24/27
23
intravena 1gm/12 jam untuk orang dewasa dan setengah dosis diberikan
untuk anak-anak.
2. Terapi Bedah:
a. Indikasi:
- Komplikasi intracranial
- Bukti fluktuasi postauricular dan abses subperiosteal
- Diagnosis mastoiditis coalescent akut.
- Kegagalan program terapi medis meskipun pengobatan antibiotik yang
memadai selama 48-72 jam.
- Otore bertahan selama lebih dari 2 minggu meskipun pengobatan
antibiotik yang memadai.
- Cholesteatoma
b. Metode:
1. Minimal Prosedur Invasif :
a. Insisi dan drainase abses mastoid: Insisi dan drainase (I & D) harus
dilakukan segera setelah fluktuasi muncul. Sayatan harus samadengan sayatan bedah yang akan datang. Metode Hilton digunakan
untuk membuka semua loculi abses dan untuk mencapai drainase
lengkap dari nanah. Satu pak kasa basah dengan Betadine dapat
ditempatkan di rongga abses dan diganti setiap hari dengan
perawatan luka.
b. Myringotomy: dengan atau tanpa penempatan tabung tympanostomy.
Ini harus dipertimbangkan sebagai pengobatan di setiap kasus
mastoiditis dengan membran timpani utuh atau drainase yang tidak
memadai.
2. Bedah :

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 25/27
24
- Jika terdapat cholesteatoma, mastoidectomy terbuka harus
dilakukan.
- Jika tidak terdapat cholesteatoma, mastoidectomy kortikal adalah
pilihan terbaik.
Sebuah fistula postauricular (Gambar 3) harus difollow-up melalui
mastoid dan dieksisi total, tepi kulit harus dibersihkan, diinsisi dan dijahit secara
hati-hati dalam 2 lapisan. Waktu operasi terutama tergantung pada kondisi pasien
dan respon kepada perawatan medis. Jika pasien memburuk, operasi harus segera
dilakukan untuk menyelamatkan hidup pasien.
Namun, jika respon pasien terhadap perawatan medis baik, sebagaimana
dibuktikan oleh perbaikan klinis dan tindak lanjut CT scan, operasi dapat ditunda
selama satu minggu untuk menghindari perichondritis.
Gambar 3. Sebuah fistula postauricular
5.3. Pedoman penatalaksanaanabses mastoid menurut aetiopathology
1. Mastoiditis coalescent akut tanpa pembentukan abses
-
Pengobatan terutama medis dalam bentuk antibiotik intravena sesuaidengan kultur dan sensitivitas.
- myringotomy diperlukan dalam kasus-kasus dengan drainase cukup
misalnya membrane timpani utuh atau perforasi.
- Mengobati penyebab misalnya akut otitis media supuratif

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 26/27
25
2. Mastoiditis coalescent akut dengan komplikasi misalnya saraf wajah
kelumpuhan atau komplikasi intrakranial misalnya lateralis sinus
thrombophlebitis.
- Terapi bedah dengan terapi antibiotik intravena spektrum luas.
- Mengobati penyebabnya.
- komplikasi intrakranial seperti abses otak atau meningitis harus dikelola
bersama dengan departemen bedah saraf dengan prioritas bedah saraf.
Ketika pasien neurologis stabil, penatalaksanaanpenyakit telinga dapat
diatasi.
3.
Mastoiditis akut dengan abses postaurikuler
- Terapi bedah dalam bentuk mastoidectomy kortikal setelah persiapan
medis dengan antibiotik intravena.
- Dalam keadaan yang tidak menguntungkan, abses dapat digores dan
dikeringkan berapa hari kemudian dapat dilakukan mastoidectomy.
- Mengobati penyebabnya.
4. Mastoiditis akut komplikasi otitis media supuratif kronis yang aman
- Pengobatan seperti dengan akut otitis media supuratif.
- Mengobati penyebabnya setelah abses teratasi misalnya tympanoplasty
dengan mastoidectomy kortikal.
5. Mastoiditis akut dari kronis otitis media supuratif yang tidak aman
(cholesteatoma).
- Terapi bedah dalam bentuk mastoidectomy terbuka dengan terapi
antibiotik intravena spektrum luas.

8/13/2019 Jurnal Tht Ay Maul Yuu
http://slidepdf.com/reader/full/jurnal-tht-ay-maul-yuu 27/27
DAFTAR PUSTAKA
[1]. Dudkiewicz M, Livni G, Kornreich L, Nageris B, Ulanovski D, Raveh E. Acute
mastoiditis and osteomyelitis of the temporal bone. Int J Pediatr
Otorhinolaryngol. 2005;69:1399 – 1405.
[2]. Mawson SR. In: Mawson SR, ed. Complications of suppurative otitis media in
diseases of the ear. Edward Arnold (Publishers) LTD;1967:329 – 349 [Chapter
XIII].
[3]. Holt GR, Gates GA. Masked mastoiditis. Laryngoscope. 1983;93:1034 – 1037.
[4]. Petersen CG, Ovesen T, Pedersen CB. Acute mastoidectomy in a Danish county
from 1977 to 1996 with focus on the bacteriology. Int J Pediatr Otorhinolaryngol.
1998;45:21 – 29.
[5]. Tarantino V, D’Agostino R, Taborelli G, Melagrana A, Porcu A, Stura M. Acute
Mastoiditis: a 10 year retrospective study. Int J Pediatr Otorhinolaryngol.
2002;66:143 – 148.
[6]. Brook I. The role of anaerobic bacteria in acute and chronic mastoiditis.
Anaerobe. 2005;11:252 – 257.
[7]. Khafif A, Halperin D, Hochman I, dkk. Acute mastoiditis: a 10-year review. Am
J Otolaryngol. 1998;19:170 – 173.
[8]. De S, Makura ZG, Clarke RW. Paediatric acute mastoiditis: the Alder Hey
experience. J Laryngol Otol. 2002;116:440 – 442.