Embed Size (px)
Citation preview

8/12/2019 Jurnal Ogi
http://slidepdf.com/reader/full/jurnal-ogi 1/6
Scandinavian Journal of Surgery 100: 147–152, 2011
A CLINICAL STUDY ON THE RESECTION OF BREAST
FIBROADENOMA USING TWO TYPES OF INCISION
X.-F. Liu1 , J.-X. Zhang2 , Q. Zhou1 , F. Chen1 , Z.-M. Shao2 , C. Lu1
1 Department of Breast, Nanjing Maternity and Child Health Hospital of Nanjing Medical University,Nanjing, China
2 Department of Breast Surgery, Cancer Hospital/Cancer Institute, Department of Oncology,Fudan University, Shanghai, China
ABSTRACT
Background and Aims: Breast fibroadenoma (FA) is traditionally managed by FA excisionthrough an overlying incision (FETOI). FA excision through a periareolar incision (FETPI)has been developed, paying special attention to incision location to preserve cosmesis.The purpose of this article is to discuss the FETPI technique.
Methods: The clinical data of 76 patients who underwent FETPI (98 FAs, group A) and82 patients who underwent FETOI (122 FAs, group B) were retrospectively analyzed inthis non-randomized study. Early postoperative complications, nipple sensation loss, andcosmetic results were compared between the two groups. The techniques, indications,and special considerations of the FETPI technique were described and identified.
Results: The FETPI technique was associated with more early postoperative complica-tions (7/76 vs. 2/82, p = 0.067) and more nipple sensation losses (15/76 vs. 7/82, p = 0.042)
than those of the FETOI technique. Cosmetic assessment at 6 months demonstrated sta-tistically more excellent/good results in group A than in group B (62/76 vs. 50/82,p = 0.004).
Conclusion: The FETPI technique yields superior cosmetic results with minor postop-erative complications.
Key words: Areola; incision; breast; fibroadenoma; excision; periareolar incision; overlying incision; non-randomized study; surgical techniques; surgical indications
Correspondence:Zhi-Ming Shao, M.D.Department of Breast SurgeryCancer Hospital/Cancer InstituteDepartment of Oncology, Fudan University270 Dong’an RoadShanghai 200032People’s Republic of ChinaEmail: [email protected]
nazol, since the most prevalent theory on the etiologyof FAs attributes them to excessive estrogen influenceor response. Unfortunately, FAs fail to respond tothese antiestrogen medications (1).
In the era of modern radiology and nonsurgicaltissue biopsies, conservative treatment of FA is oftenconsidered safe and acceptable after adequate tripletesting (clinical examination, radiology, and biopsy)(2, 3, 4, 5, 6). Patients who choose conservative man-agement need to be informed of the limitation oftriple testing and must be assessed promptly if thereis symptomatic or clinical change (4).
The authors have noted that, in clinical practice,approximately 1/3 of FAs that have undergone long-term periodic monitoring ultimately cause anxietyand discomfort for patients and difficulty for physi-cians. These masses will be excised, and only surgicalresection is curative.
INTRODUCTION
Fibroadenomas (FAs) are benign solid tumors com-posed of stromal and epithelial elements. After carci-
noma, FA is the second most common tumor in the breast and is the most common tumor in womenyounger than 30 years. Conservative therapy has been attempted medically with progesterone and da-

8/12/2019 Jurnal Ogi
http://slidepdf.com/reader/full/jurnal-ogi 2/6
148 X.-F. Liu, J.-X. Zhang, Q. Zhou, F. Chen, Z.-M. Shao, C. Lu
The criteria for surgical treatment in this study in-cluded the following:
1. Patients older than 35 years of age (7).2. Mean change in tumor dimension for a 6-month
interval is greater than 20% for all ages (8).3. Patients with FAs that are symptomatic (surgery in
this case is a traditional option, and patients prefer
it).4. Patients younger than 20 years who have a likeli-hood of juvenile FAs (9).
5. Patients with psychological/nervous disordercaused by long-term regular follow-up or who areunavailable for regular follow-up.
Surgical removal is curative, and the most obviousapproach to surgical excision is through an incisionoverlying the mass. That is why breast FA has beentraditionally managed by FETOI, which often resultsin marked scarring. Patients feel uncomfortable aboutthe unsightly scar, especially adolescent patients whoare sensitive about their body appearance.
The FETPI technique offers the advantage of an
incision in an aesthetically acceptable area. The scarcan be camouflaged by the dark color of the areolarskin and the roughness of the areolar glands (10). Theperiareolar scar is esthetically superior to the overly-ing scar (11).
However, FETPI is not possible if the lesion is faraway from the areolar border or if the areola is smalland the lesion is not underneath the areola. In addi-tion, if a lesion is 2–5 cm away from the areolar bor-der, a subcutaneous tunnel, which may cause skininjury, is necessary to expose the lesion in the FETPItechnique. Therefore, FETPI should be selectively andcarefully performed. Unfortunately, few publicationshave dealt in detail with the technical considerations
necessary for successful execution of the FETPI pro-cedure.
In this paper, some important aspects of the FETPIprocedure – indications, contraindications, surgicaltechnique, procedural limitations, benefits, complica-tions, and surgical outcomes – are analyzed by com-paring FETPI and FETOI through a review of pa-tients’ medical records.
METHODS
STUDY DESIGN
Informed consent was obtained from the patients, and ap-
proval was obtained from the designated review board ofthe institution involved.
This study was performed with a retrospective, compara-tive, historical design. Before the study, for the purpose ofselecting suitable patients, the authors had already deter-mined the well-defined criteria of indications and contrain-dications for the FETPI technique based on their previousclinical experience.
The FETPI technique was indicated for patients with thefollowing characteristics: an areola diameter greater than3.5 ~ 5.0 centimeters (cm), a distance from the outer marginof the mass to the nearest areola’s edge ≤ 5.0 cm, the largestdiameter of clinically diagnosed palpable FAs ≤ 3.0 cm, andage ≤ 35 years. The contraindications of FETPI included thefollowing: the largest diameter of the mass > 5.0 cm and a
small areola, distance from the outer margin of the mass tothe nearest areola’s edge > 6.0 cm, suspicion of malignancy,nonpalpable lesions, and age > 35 years.
From June 2008 to February 2009, 260 consecutive femalepatients underwent FA excision at Nanjing Maternity andChild Health Hospital of Nanjing Medical University andat Shanghai Cancer Hospital of Fudan University. Amongthem, 92 patients with 106 breast FAs were excluded fromanalysis for the following reasons: age > 35 years, suspicionof malignancy, inframammary incision, impalpable tumors,or tumors greater than 5 cm.
The study included a total of 158 patients with a meanage of 27.4 years (range, 12–35 years) and a median follow-up period of 12 months (8 to 16 months). Fifty-one patientshad multiple tumors, including 36 patients with bilaterallesions, and 6 patients were young adolescents (youngerthan 20 years and older than 12 years). Histopathologicexamination was consistent with FA in each tumor, andaverage tumor diameter was 2.5 cm.
Among these 158 patients, 76 patients (with 98 FAs) ful-filling the FETPI indications were entered into group A.Patients who underwent FETOI (n = 82, 122 FAs, group B) by the surgeon teams in the same period included 22 pa-tients suitable for FETPI who chose FETOI after informed
consent.
EXCISIONAL PROCEDURES OF THE FETPI TECHNIQUE
The incision marking was outlined preoperatively, with thepatient in a supine position and arms abducted 90 degreeson arm boards. The procedure generally was performedunder a local anesthetic or intravenous anesthesia.
A circumareolar skin incision was made on the mark-ing at the areolar border after the anesthesia had been ad-ministered. The subcutaneous tissue was dissected off byelectrocautery, pulling the edges of the incision upwardwith skin hooks. Dissection was continued in the plane between subcutaneous fat and breast tissue, and downwardtoward the mass. The position of the mass was determinedagain by palpation. A radial incision within breast tissuewas made outward and downward to the palpable massto an appropriate depth. After mass exposure, the skin flapwas raised, and the thin tissue around the FA was graspedwith forceps to facilitate exposure of the mass. A thin exci-sion of the tumor with a 2–3 mm circumferential margin ofmacroscopically normal tissue was necessary. After the FAwas removed, meticulous hemostasis was needed beforeclosure. Breast tissue approximation was not considerednecessary but was preferred if such closure would not re-sult in deformity. The dermis of the skin was approximatedusing interrupted 4-0 absorbable sutures (Ethicon Vicryl) todecrease skin tension. A running subcuticular stitch with4-0 absorbable sutures was used without burying the start-ing and finishing knots in order to take stitches out in anappropriate time to avoid skin irritation.
A soft cotton pressure dressing was then placed inside,and the outside was bandaged postoperatively. Compres-sion with a sandbag for 6 hours was preferred in the case ofsubcutaneous tunnel or when the operative site was locatedin front of the chest. Both methods played a critical role inhemostasis.
EXCISIONAL PROCEDURES OF THE FETOI TECHNIQUE
The main difference between the FETOI and FETPI proce-dures was the incision location. Most commonly, a curveincision was located on the lesion in FETOI. Dissection wascontinued down through the subcutaneous tissue at theedges of the mass by electrocautery after the skin overlyingthe mass was dissected.
8/12/2019 Jurnal Ogi
http://slidepdf.com/reader/full/jurnal-ogi 3/6
149 A clinical study on the resection of breast fibroadenoma using two types of incision
THE EVALUATION CRITERIA
The scar clinical grading scale was determined using 3 pa-rameters: scar width, area of pigment loss in the scar, andheight of scar swelling. These parameters were quantifiedusing a score from 1 to 4 (1 = minimal; 2 = discreet; 3 = mod-erate; and 4 = marked; Table 1). The significance of the scarwas assessed on a scale from grade 1 (best scar) to grade 4(poor scar), according to the sum of the scores of the threeparameters at 6 months after treatment (3 or 4 = grade 1;
5, 6 or 7 = grade 2; 8, 9 or 10 = grade 3; and 11 or12 = grade 4).Patients rated their subjective feelings about cosmetic
outcomes themselves. They were asked to assess the scaron a scale of 1 to 4 (1 = excellent; 2 = good; 3 = fair; and4 = poor) at 6 months after treatment.
The nipple sensation loss was investigated after a6-month follow-up period. The patients told the doctorswhether their nipple sensation was lost or not. Nipple sen-sation was rated as 1 (good) or 2 (sensation loss).
STATISTICAL ANALYSIS
The areola diameter, tumor diameter, distance between theareola border and the mass, bleeding volume, and opera-tion time in the two groups were expressed as the mean ±standard error of the mean (SEM, see Table 2). Differences between the 2 groups were compared by Student’s t-test.Early complications, nipple sensation loss, and cosmeticresults in the 2 groups were compared using the chi-squaretest, and p < 0.05 was considered to be significant. All thestatistics analysis was performed in SAS® ZealAnyDay Ver-sion 1.7 (Copyright 1997–98 HaiLi, Zeal SoftStudio).
RESULTS
SURGICAL COMPLICATIONS
There was no surgical mortality. All patients toleratedthe procedure well without acute complications, andno major complications were noted. The early com-plications (pain on the first postoperative night, skinflap bruises, hematoma formation) of group A werenot significantly higher than that of group B (7/76,
TABLE 1
Scored by assessment (from 1 to 4) of three scar parameters, namely, scar width, area of pigment loss in the scar, and height of scar swelling.
Score* Scar width Area of pigment loss in scar Height of scar swelling
1 ≤ 1 mm ≤ 20 mm2 ≤ 1 mm2 > 1 mm and ≤ 2 mm > 20 mm2 and ≤ 40 mm2 > 1 mm and ≤ 2 mm3 > 2 mm and ≤ 3 mm > 40 mm2 and ≤ 80 mm2 > 2 mm and ≤ 3 mm4 > 3 mm > 80 mm2 > 3 mm
* These parameters were quantified using the following scale: 1 = minimal, 2 = discreet, 3 = moderate, and 4 = marked.
TABLE 2
Difference between group A and group B in areola diameter, tumorsizes, distance between the areolar border and the mass (DBABM),
operation time, bleeding volume, scar length, early complications, andnipple sensation loss.
Group A Group B p-value
Areola’s diameter 4.4 ± 0.5cm 4.2 ± 0.4cm 0.004Tumor diameter 2.4 ± 0.5cm 2.9 ± 0.4cm 0.000DBABM 2.6 ± 0.9cm 4.0 ± 0.8cm 0.000Operation time 44 ± 5 minutes 42 ± 4 minutes 0.003Bleeding volume 34 ± 5ml 24 ± 6ml 0.000Scar length 4.8 ± 0.6cm 4.6 ± 0.6cm 0.034The early complications* 7 2 0.067Nipple sensation loss 15 7 0.042
* Early complications included (comparing group A to group B):hematoma formation (4 vs. 2), pain on the first postoperativenight (1 vs. 0), and skin flap bruises (2 vs. 0).
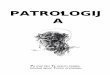
Fig. 1. One patient had a fibroadenoma in the left breast. The fi- broadenoma is circled with ink, and the skin-areola junction isdrawn with ink.
Fig. 2. A line is drawn along the skin-areola junction, the outeredge of the lesion is located 5 cm away from the areolar border.
8/12/2019 Jurnal Ogi
http://slidepdf.com/reader/full/jurnal-ogi 4/6
150 X.-F. Liu, J.-X. Zhang, Q. Zhou, F. Chen, Z.-M. Shao, C. Lu
2/82; p = 0.067). Four patients in group A presentedhematoma in the subcutaneous tunnel area, whichresolved between 1 and 6 months after surgery. Twopatients in group B developed a small postoperativehematoma, which resolved within 3 months of obser-vation. No patients in either group developed masti-tis or incisional complications.
OPERATION TIME, BLEEDING VOLUME, AND NIPPLESENSATION
The operation time of group A was longer than thatof group B (44 ± 5 minutes vs. 42 ± 4 minutes, p =
0.003). The bleeding volume of group A was greaterthan that of group B (34 ± 5ml vs. 24 ± 6 ml, p = 0.000).A significantly higher proportion of female patientslacked normal nipple-areola sensation in group Athan group B (15/76 vs. 7/82, p = 0.042, Table 2).
TABLE 3
Number (percentage) of patients with various scar grades. Scars were graded from 1(best scar) to 4 (poor scar)
Grade 1* Grade 2 Grade 3 Grade 4 Total
Group A 12 (15.8%) 34 (44.7%) 26 (34.2%) 4 (5.3%) 76
Group B 20 (24.4%) 29 (35.4%) 23 (28.0%) 10 (12.2%) 82Sum 37 (23.98) 53 (62.0%) 25 (15.8%) 14 (8.9%) 158
* Scars were graded according to the total scores of the 3 parameters (scar width, area of pigment loss in scar, and height of scar swelling)at 6 months after treatment. (3 or 4 = grade 1; 5, 6 or 7 = grade 2; 8, 9 or 10 = grade 3; and 11 or 12 = grade 4).
TABLE 4
Patients rated their subjective feelings of cosmetic outcomes using the scale of excellent, good, fair, or poor at 6 months after treatment
Excellent Good Fair Poor Total
Group A 18 (23.7%) 44 (57.9%) 10 (13.2%) 4 (5.3%) 076Group B 14 (17.1%) 36 (43.9%) 10 (12.2%) 22 (26.8%) 082Total 32 (20.3%) 75 (47.5%) 20 (12.7%) 31 (19.6%) 158
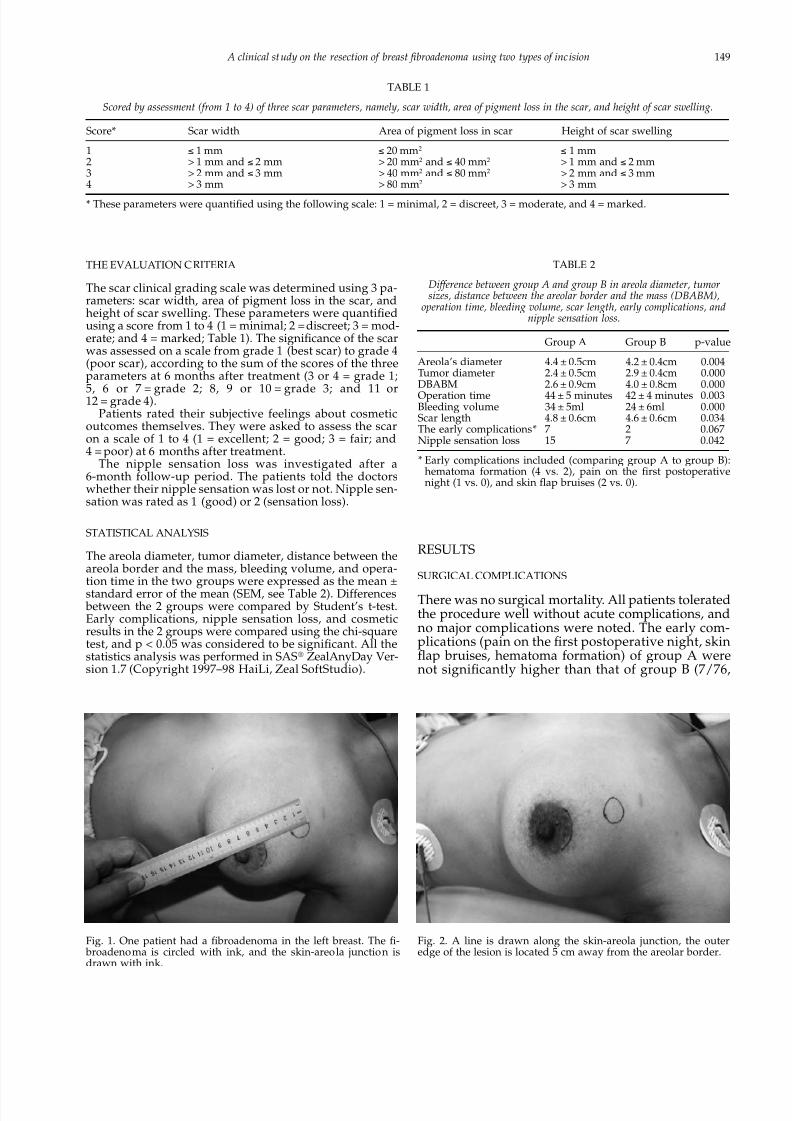
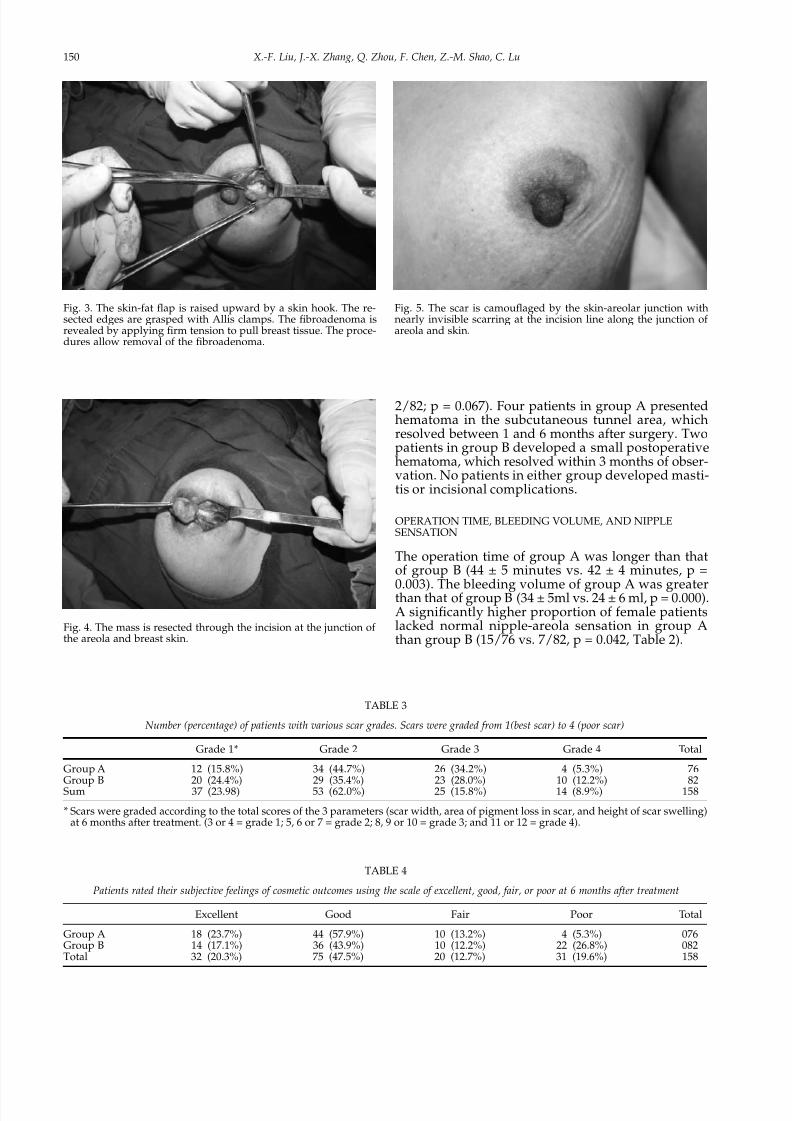
Fig. 3. The skin-fat flap is raised upward by a skin hook. The re-sected edges are grasped with Allis clamps. The fibroadenoma isrevealed by applying firm tension to pull breast tissue. The proce-dures allow removal of the fibroadenoma.
Fig. 5. The scar is camouflaged by the skin-areolar junction withnearly invisible scarring at the incision line along the junction ofareola and skin.
Fig. 4. The mass is resected through the incision at the junction ofthe areola and breast skin.

8/12/2019 Jurnal Ogi
http://slidepdf.com/reader/full/jurnal-ogi 5/6
151 A clinical study on the resection of breast fibroadenoma using two types of incision
AESTHETIC OUTCOME
No scars were surgically revised in either group. Themean scar length was 4.8 ± 0.6 cm in group A and3.7 ± 0.6 cm in group B (p = 0.034), 5.3% of patients ingroup A had marked scarring (grade 4), comparedwith 12.2% in group B (p = 0.126, Table 3). A signifi-cantly higher proportion of female patients com-
plained of poor scarring in group B than in group A(4/76 vs. 22/82, p = 0.001, Table 4).The cosmetic results were positive (excellent, good,
and fair) in 72 (94.7%) of the 76 patients in group A,in contrast to 60 (73.2%, p = 0.001) out of 82 in groupB. Sixty-two of the 76 (81.6%) patients in group A and50 of the 82 (61.0%) patients in group B judged theircosmetic results to be excellent or good during the6-month follow-up period (p = 0.004).
DISCUSSION
HISTORY AND ADVANTAGE OF THE PERIAREOLARINCISION
The periareolar incision was introduced first by Du-fourmentel in 1928. Subsequently, the incision waswidely used in gynecomastia (12, 13) and in breastaugmentation (14, 15) for a long time because of itscosmetic advantage. Some surgeons considered theperiareolar incision as the gateway to the breast (11).Cosmetic results were satisfactory for pediatric pa-tients with palpable breast FAs who had undergoneoperation through a circumareolar incision (16). Atpresent, the majority of surgical textbooks suggest ahemi-circumareolar or periareolar incision if possi- ble.
DISADVANTAGES OF FETPI
In the FEPTI group, the operation time was longer(by 2 min), and the volume of intraoperative bloodloss was larger (by 10 ml) when compared with theFETOI group. Although statistically significant, bothdifferences, the longer duration and the excess bloodloss, are meaningless in clinical practice. Refinementof surgical techniques (such as exposure, hemostasis,and closure) is required for surgeons.
Dissection parallel to the skin in the vascular plane between subcutaneous fat and breast tissue will min-imize bleeding. Meticulous hemostasis should be
achieved before closure to minimize hemorrhage andto prevent the formation of hematomas. A commonreason for skin flap bruises is excessive traction dur-ing surgery, and these may resolve without treatment.A consistently dark spot may be a sign of dysfunctionof venous drainage or arterial supply; therefore, re-lieving the compression is necessary. A thick flap thatincludes skin and all subcutaneous fat is a good op-tion to prevent skin flap necrosis and skin flap bruises.
The majority of these complications occurred earlyin the learning curve. Most of the complications wereminor and preventable. They did not interfere withthe esthetic outcome.
NIPPLE SENSATION LOSS
The only factor found to influence the sensitivity ofthe nipple in the study was the lateral location of theincision. There are other findings that support thesame point (17). Schlenz et al. found that the nippleand areola were always innervated by the lateral andanterior cutaneous branches of the 3rd, 4th, and 5th
intercostal nerves (18). These cutaneous branchestook superficial courses within the subcutaneous fatand reached the nipple from the lateral side, termi-nating at the medial areolar border. These findingssuggest that the nerves innervating the nipple andareola are best protected if skin incisions at the lateralareolar border are avoided (18).
DISRUPTION OF LACTATION
The FETPI technique involves extensive underminingand may interrupt milk ducts. It is not possible toassess problems in lactation in the context of the pres-ent study. However, in order to avoid damage to lac-
tiferous ducts due to extensive undermining whenusing FETPI, the dissection plane between subcutane-ous fat and breast tissue should be identified andfollowed by pulling the edges of the incision up-ward.
PATIENT SELECTION FOR FETPI
The formulated criteria are generally practicable inthe light of the present study, with no need to changethem thus far. However, in certain cases the criteriamaybe inapplicable. For example, if a patient with asuperficially located mass greater than 5 cm in diam-eter (which violates the indications of FETPI) also
had a large areola, FETPI would be technical feasi- ble.
THE LIMITATIONS OF THE STUDY
This was not a randomized study. Tumor locationswere more peripheral among the FETOI patients,which may bias the results. Thus, a prospective, ran-domized study appears to be warranted.
CONCLUSION
To summarize, the results show that if criteria for
patient selection are carefully respected, the FETPIprocedure can provide both oncological safety andcosmesis. A circumareolar incision should be per-formed when feasible.
ACKNOWLEDGEMENTS
This work was supported by a grant from NanjingHealth Bureau Clinic Research Foundation [ProjectNo.YKK09080].

8/12/2019 Jurnal Ogi
http://slidepdf.com/reader/full/jurnal-ogi 6/6
152 X.-F. Liu, J.-X. Zhang, Q. Zhou, F. Chen, Z.-M. Shao, C. Lu
REFERENCES
01. Greenblatt RB, Nezhat C, Ben-Nun I: The treatment of benign breast disease with danazol. Fertil Steril 1980; 34(3): 242–245
02. Ranieri E, Barberi S, Caprio G, et al: Diagnosis and treatmentof fibroadenoma of the breast: 20 years’ experience. Chir Ital2006;58(3):295–297
03. Ron G, Yehuda S, Ofer K: Management of breast fibroade-nomas. J Gen Intern Med 1998;13(9):640–645
04. Houssami N, Cheung MN, Dixon JM, et al: Fibroadenoma ofthe breast. Med J Aust 2001;174(4):185–18805. Alle KM, Moss J, Venegas RJ, et al: Conservative management
of fibroadenoma of the breast. Br J Surg 1996;83(7):992–99306. Dixon JM, Dobie V, Lamb J, et al: Assessment of the accept-
ability of conservative management of fibroadenoma of the breast. Br J Surg 1996;83(2):264–265
07. Kuijper A, Mommers EC, van der Wall E, et al: Histopathologyof fibroadenoma of the breast. Am J Clin Pathol 2001;115(5):736–742
08. Gordon PB, Gagnon FA, Lanzkowsky L: Solid breast massesdiagnosed as fibroadenoma at fine-needle aspiration biopsy:acceptable rates of growth at long-term follow-up. Radiology2003;229(1):233–238
09. Farrow JH: Fibroadenoma of the breast. CA Cancer J Clin 1961;11(5):182–190
10. Song RY: Augmentation mammoplasty and an improved meth-od of silastic gel breast prosthesis implantation through anareolar incision. Zhonghua Zheng Xing Shao Shang Wai Ke ZaZhi 1990; 6(1):72–74
11. Shrotria S: The peri-areolar incision--gateway to the breast! Eur J Surg Oncol 2001;27(6):601–603
12. Saad MN, Kay S: The circumareolar incision: a useful incisionfor gynaecomastia. Ann R Coll Surg Engl 1984;66(2):121–122
13. Pitanguy I: Transareolar incision for gynecomastia. Plast Re-constr Surg 1966;38(5):414–419
14. Becker H: The intra-areolar incision for breast augmentation.Ann Plast Surg 1999;42(1):103–106
15. Jones FR, Tauras AP: A periareolar incision for augmentationmammaplasty. Plast Reconstr Surg 1973;51(6):641–644
16. Tiryaki T, Senel E, Hucumenoglu S, et al: Breast fibroadenomain female adolescents. Saudi Med J 2007;28(1):137–138
17. Benediktsson KP, Perbeck L, Geigant E, et al: Touch sensibilityin the breast after subcutaneous mastectomy and immediatereconstruction with a prosthesis. Br J Plast Surg 1997;50(6):443–449
18. Schlenz I, Kuzbari R, Gruber H, et al: The sensitivity of thenipple-areola complex: an anatomic study. Plast Reconstr Surg2000;105(3):905–909
Received: June 22, 2010Accepted: December 8, 2010