Embed Size (px)
Citation preview
JOT
JOURNALOF ORTHOPAEDIC
TRAUMA
www.jorthotrauma.com
OFFICIAL JOURNAL OF
Orthopaedic Trauma Association
Belgian Orthopaedic Trauma Association
Canadian Orthopaedic Trauma Society
Foundation for Orthopedic Trauma
International Society for Fracture Repair
The Japanese Society for Fracture Repair
Special Case Report Series
CASE REPORTS

Evaluation and Management of an Unstable IntertrochantericFracture of the Femur: A Case Report
Harish Kempegowda, MS, Akhil Tawari, MS, Michael Suk, MD, JD, MPH, FACS,and Daniel S. Horwitz, MD
Unstable intertrochanteric fracture of the femur is one of the mostcommonly encountered orthopaedic injuries in the United States.A 63-year-old female sustained a highly unstable intertrochantericfracture of the femur (OTA 31-A 3.3) and she was treated witha long cephalomedullary nail. Four months later, a solid unionoccurred at the fracture site with minimal limb length discrepancyand the patient regained her pre-operative functional status. Thiscase report highlights the important points which must beconsidered in the treatment of an unstable intertrochantericfracture with emphasis on preoperative evaluation, intraoperativemanagement and post-operative protocol for a good outcome.
Key Words: unstable intertrochanteric fractures, cephalomedul-lary nail
INTRODUCTIONUnstable intertrochanteric (IT) fractures are relatively common
injuries among the geriatric population.1,2 As per the most com-monly used Evans classification, loss of posteromedial integrity, ITfractures with subtrochanteric extension, and the reverse obliquepattern are considered unstable.2,3 The complications after internal
fixation include hardware failure, nonunion, malunion, limb lengthdiscrepancy, and diminished abductor lever strength.4 The increasein the incidence of complications has led to an extension of thedefinition of instability to include lateral wall blow out, greatertrochanteric fracture, and osteoporosis.4,5 The preoperative identi-fication of an unstable pattern is of utmost importance in reducingcomplications.
Many fixationmethods have been described to treat IT fractures,of which the sliding hip screw and intramedullary devices (IMDs)have stood the test of time. Biomechanical and clinical studiesshow a clear advantage of IMDs over sliding hip screws in fixationof unstable fracture patterns.6,7 The evolution of nailing systemsbegan with the first-generation gamma nail (Stryker, Mahwah, NJ)in the 1980s and has progressed to current fourth-generationnails.8,9
CLINICAL SCENARIOA 63-year-old woman presented to the emergency department
with 10/10 pain in her left hip subsequent to fall at home. She hada known diagnosis of osteoporosis for which she was on regularcalcium, vitaminD supplements, and once yearly bisphosphonates.She was nonhypertensive, nonsmoker, and denied any othersignificant past medical or surgical illnesses. A focused clinicalexamination revealed a left lower extremity in extreme externalrotation, shortening, and generalized hip pain.
DIAGNOSTIC ASSESSMENTPlain radiographs anteroposterior (AP) view and cross-table
lateral view of the left hip, traction-internal rotation view, anda computed tomography scan (CT) scan with 3D reconstructionwere obtained. These revealed a loss of posteromedial continuity,subtrochanteric extension, greater trochanteric comminution, anda fracture line extending up to the femoral neck, making this injuryhighly unstable (Figs. 1A–E).
Accepted for publication June 2, 2015.
From the Department of Orthopaedic Surgery, Geisinger Medical Center,Danville, PA.
D. S. Horwitz is a consultant and receives royalties from Biomet. Theremaining authors report no conflict of interest.
Reprints: Daniel S. Horwitz, MD, Department of Orthopaedic Surgery,Geisinger Medical Center, 100 N Academy Avenue, Danville, PA 17822-2130 (e-mail: [email protected]).
The views and opinions expressed in this case report are those of theauthors and do not necessarily reflect the views of the editors of Journalof Orthopaedic Trauma or Biomet.
J Orthop Trauma � 2015 www.jorthotrauma.com e1
Copyright � 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.

TREATMENTConsidering the highly unstable nature of the fracture, the
authors chose to proceed with long intramedullary nailing. Closedreduction was attempted with longitudinal traction followed byinternal rotation but was unable to correct posterior sag andmedialization of the femoral neck. Based on this, the decisionwas made to perform an open reduction.10 The posterior sag wascorrected using a posteriorly placed Cobb elevator, and the medi-alization of the femoral neck was corrected using a bone hook.The reduction thus obtained was maintained by a coaxial clamp(Fig. 2A). The intraoperative fluoroscopic images revealed anacceptable alignment of the femoral head and neck with the shaftwithout any varus or medialization of the femoral neck. An incisionwas made proximal to the tip of the greater trochanter, and an entrywire was placed 1 mm medial to the tip of greater trochanter to
avoid damage to abductors and to promote valgus reduction.11 Theentry wire position was confirmed on AP and true lateral fluoro-scopic views and advanced into the medullary canal. Afteradvancement of the wire, the position was confirmed on AP andtrue lateral fluoroscopic views. The entry reamer was then used togain access to themedullary canal, and the entry wire was removed.The reduction was maintained with the reduction forceps through-out the procedure, and a ball-tipped guide wire was introduced intothe proximal femoral canal and advanced down the distal femur. Itsposition was confirmed distally on AP and lateral views. The fem-oral canal was sequentially reamed up to 11mm, and a 93 360mmnail was then placed over the guide wire and seated distally byhand. At this point, central–central position of a compression screwguide wire in the femoral head was obtained, screw length wasdetermined, a step drill was used over the guide wire, and an
FIGURE 1. AP (A), lateral (B), traction-internal rotation (C), radiographicimages and CT scan with 3D recon-struction (D and E) of the left hip showan IT fracture femur with the commi-nution of greater trochanter, sub-trochanteric extension, and a separateanteromedial and posteromedial frag-ment.
FIGURE 2. Note the correction of medialization ofthe femoral neck after the placement of a bone hook,and the reduction was held with a coaxial clamp (A).The ball-spiked pusher was placed laterally to impactthe fracture (B).
Kempegowda et al
e2 www.jorthotrauma.com Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Copyright � 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
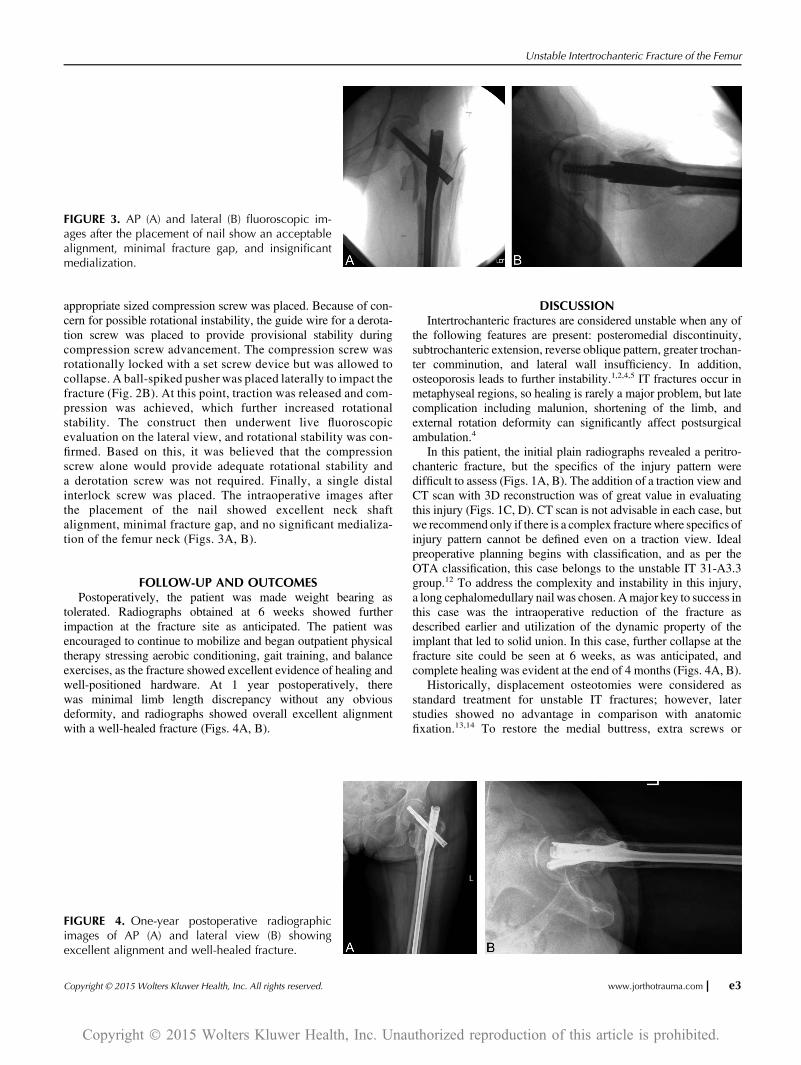
appropriate sized compression screw was placed. Because of con-cern for possible rotational instability, the guide wire for a derota-tion screw was placed to provide provisional stability duringcompression screw advancement. The compression screw wasrotationally locked with a set screw device but was allowed tocollapse. A ball-spiked pusher was placed laterally to impact thefracture (Fig. 2B). At this point, traction was released and com-pression was achieved, which further increased rotationalstability. The construct then underwent live fluoroscopicevaluation on the lateral view, and rotational stability was con-firmed. Based on this, it was believed that the compressionscrew alone would provide adequate rotational stability anda derotation screw was not required. Finally, a single distalinterlock screw was placed. The intraoperative images afterthe placement of the nail showed excellent neck shaftalignment, minimal fracture gap, and no significant medializa-tion of the femur neck (Figs. 3A, B).
FOLLOW-UP AND OUTCOMESPostoperatively, the patient was made weight bearing as
tolerated. Radiographs obtained at 6 weeks showed furtherimpaction at the fracture site as anticipated. The patient wasencouraged to continue to mobilize and began outpatient physicaltherapy stressing aerobic conditioning, gait training, and balanceexercises, as the fracture showed excellent evidence of healing andwell-positioned hardware. At 1 year postoperatively, therewas minimal limb length discrepancy without any obviousdeformity, and radiographs showed overall excellent alignmentwith a well-healed fracture (Figs. 4A, B).
DISCUSSIONIntertrochanteric fractures are considered unstable when any of
the following features are present: posteromedial discontinuity,subtrochanteric extension, reverse oblique pattern, greater trochan-ter comminution, and lateral wall insufficiency. In addition,osteoporosis leads to further instability.1,2,4,5 IT fractures occur inmetaphyseal regions, so healing is rarely a major problem, but latecomplication including malunion, shortening of the limb, andexternal rotation deformity can significantly affect postsurgicalambulation.4
In this patient, the initial plain radiographs revealed a peritro-chanteric fracture, but the specifics of the injury pattern weredifficult to assess (Figs. 1A, B). The addition of a traction view andCT scan with 3D reconstruction was of great value in evaluatingthis injury (Figs. 1C, D). CT scan is not advisable in each case, butwe recommend only if there is a complex fracturewhere specifics ofinjury pattern cannot be defined even on a traction view. Idealpreoperative planning begins with classification, and as per theOTA classification, this case belongs to the unstable IT 31-A3.3group.12 To address the complexity and instability in this injury,a long cephalomedullary nail was chosen. Amajor key to success inthis case was the intraoperative reduction of the fracture asdescribed earlier and utilization of the dynamic property of theimplant that led to solid union. In this case, further collapse at thefracture site could be seen at 6 weeks, as was anticipated, andcomplete healing was evident at the end of 4 months (Figs. 4A, B).
Historically, displacement osteotomies were considered asstandard treatment for unstable IT fractures; however, laterstudies showed no advantage in comparison with anatomicfixation.13,14 To restore the medial buttress, extra screws or
FIGURE 3. AP (A) and lateral (B) fluoroscopic im-ages after the placement of nail show an acceptablealignment, minimal fracture gap, and insignificantmedialization.
FIGURE 4. One-year postoperative radiographicimages of AP (A) and lateral view (B) showingexcellent alignment and well-healed fracture.
Unstable Intertrochanteric Fracture of the Femur
Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved. www.jorthotrauma.com e3
Copyright � 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.

cerclage wire would be necessary if a sliding screw was theimplant of choice, but this is associated with significant soft tissuestripping and only a 17% increase in the fixation strength.15 Thegreater trochanter constitutes the lever arm of the abductor mech-anism, so near anatomic fixation is necessary for normal hip func-tion. In this case, although the greater trochanter appeared to becomminuted, it was believed that the abductor mechanism wasintact. If components of the greater trochanter are widely dis-placed, we would advise open reduction and suture fixation offragments to whatever implant is chosen.
The cost-effective analysis, biomechanical studies, and clin-ical outcomes suggest that IMDs are better devices for unstableIT fractures.16 The earlier generation nails were associated withmultiple problems including shaft fracture at the end of nail,screw cutout, and femoral neck fracture after hardware removal.8
The newer generation nails are associated with significantlyfewer complications; however, some issues such as femoral neckfracture after implant removal continue to exist.9 The advantageof an IMD also includes earlier mobilization and less limb short-ening, both of which may enhance the patient’s general well-being.17
In conclusion, preoperative identification of the unstablefracture pattern with proper radiologic investigations, selection ofthe most suitable implant based on fracture pattern, achieving andmaintaining reduction during nail placement, and early postoper-ative mobilization will maximizes the patient’s recovery in anunstable IT fracture.
REFERENCES1. Koval KJ, Zuckerman JD. Intertrochanteric fractures. In: Bucholz RW,Heckman JD, eds. Fractures in Adults. 5th ed Philadelphia, PA: LippincottWilliams and Wilkins; 2001:1635–1663.
2. Evans EM. The treatment of trochanteric fractures of the femur. J BoneJoint Surg Br. 1949;31B:190–203.
3. Jensen JS. Classification of trochanteric fractures. Acta Orthop Scand.1980;51:803–810.
4. Im GI, Shin YW, Song YJ. Potentially unstable intertrochanteric fractures.J Orthop Trauma. 2005;19:5–9.
5. Kim WY, Han CH, Park JI, et al. Failure of intertrochanteric fracturefixation with a dynamic hip screw in relation to pre-operative fracturestability and osteoporosis. Int Orthopaedics. 2001;25:360–362.
6. Curtis MJ, Jinnah RH, Wilson V, et al. Proximal femoral fractures: a bio-mechanical study to compare intramedullary and extramedullary fixation.Injury. 1994;25:99–104.
7. Al-yassari G, Langstaff RJ, Jones JW, et al. The AO/ASIF proximalfemoral nail (PFN) for the treatment of unstable trochanteric femoral frac-ture. Injury. 2002;33:395–399.
8. Albareda J, Laderiga A, Palanca D, et al. Complications and technicalproblems with the gamma nail. Int Orthop. 1996;20:47–50.
9. Yaozeng X, Dechun G, Huilin Y, et al. Comparative study trochantericfracture treated with the proximal femoral nail anti-rotation and the thirdgeneration gamma nail. Injury. 2010;41:1234–1238.
10. Afsari A, Liporace F, Lindvall E, et al. Clamp-assisted reduction of high sub-trochanteric fractures of the femur. J Bone Joint Surg Am. 2009;91:1913–1918.
11. Ostrum RF, Marcantonio A, Marburger R. A critical analysis of the eccen-tric starting point for trochanteric intramedullary femoral nailing. J OrthopTrauma. 2005;19:681–686.
12. Marsh JL, Slongo TF, Agel J, et al. Fracture and dislocation classificationcompendium—2007: Orthopaedic Trauma Association classification, databaseand outcomes committee. J Orthop Trauma. 2007;21(10 suppl l):S1–S133.
13. Dimon JH, Hughston JC. Unstable intertrochanteric fractures of the hip. JBone Joint Surg Am. 1967;49:440–450.
14. Desjardins AL, Roy A, Paimont G, et al. Unstable intertrochanteric frac-ture of the femur: a prospective randomized study comparing anatomicalreduction and medial displacement osteotomy. J Bone Joint Surg Br. 1993;75:445–447.
15. Apel DM, Patwardhan A, Pinzur MS, et al. Axial loading studies ofunstable intertrochanteric fractures of the femur. Clin Orthop Relat Res.1989;246:156–164.
16. Swart E, Makhni EC, Macaulay W, et al. Cost-effectiveness analysis offixation options for intertrochanteric hip fractures. J Bone Joint Surg Am.2014;96:1612–1620.
17. Gadegone WM, Salphale YS. “Proximal femoral nail—an analysis of 100cases of proximal femoral fractures with an average follow up of 1 year”.Int Orthop. 2007;31:403–408.
Read the rest of the JOT Case Reports online on www.jorthotrauma.com. It’s theGrandRounds series from the Journalof Orthopaedic Trauma, the official journal of the OrthopaedicTrauma Association.
Kempegowda et al
e4 www.jorthotrauma.com Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Copyright � 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.





























