Embed Size (px)
Citation preview

iiMJD 2009 June Vol 22
JURNAL DERMATOLOGI MALAYSIA
VOLUME 22 | JUNE 2009 | ISSN: 1511-5356
Contents
PAEDIATRIC DERMATOLOGY
Review Article1 Recognising cutaneous signs and
treatment in paediatric connective tissue diseases Tang SP, MRCP (Paeds) UK
DERMATO-ONCOLOGY
Original Article7 Pattern of cutaneous malignancies in a
tertiary hospital in SarawakYap FBB, MRCP, Pubalan M, MRCP
AUTOIMMUNE DISORDERS
Original Article11 Henoch - Schönlein Purpura:
Relationship between cutaneous clinical manifestations with severity outcomes:A 5-year retrospective study Tarita T, M Med, Lee CE, MBBS, Rohna R, MRCP
Case Report19 Acute cardiac failure in a young atopic
patientPan JY, MRCP, Yong WH, FAMS (Rheumatology), Audrey TWH, FAMS (Dermatology)
Case Reports25 Mucous membrane pemphigoid
Lee CK,MRCP, Zuraiza MZ, MBBS,Rokiah I, MRCP
GRANULOMATOUS DISEASES
Original Article29 Risk factors for type 1 leprosy reaction in
a tertiary skin clinic in Sarawak Yap FBB, MRCP, Pubalan M, MRCP
Case Report33 A lady with complicated erythema
nodosum leprosumYap FBB, MRCP, Pubalan M, MRCP
Short Communication35 Post vaccination lupus vulgaris
Masliza Hanuni, MD, Ong CL, MRCP, Zamri MD, Nor Azura, MD
GENERAL DERMATOLOGY
Original Article38 An outbreak of Rove Beetle dermatitis in
Penang Hospital: A report of 37 casesTan WC MRCP, Chan LC, MMed
Short Communication43 Twin psoriasis
Zaigham M, MD
Self Assessment44 Clinical Diagnostic Skill Testing
Rohna R, MRCP
DERMATOSURGERY
Surgical Tips46 Surgical lines
Gangaraam H, FRCP
Malaysian Journal of Dermatology
iii MJD 2009 June Vol 22
THERAPEUTICS
Original Article47 Efficacy and safety of tacrolimus
ointment in patients with moderate to severe atopic dermatitis - Malaysian experienceNg TG, M Adv Derm, Mardziah A, M Med, Roshidah BB, MRCP, Heng A, MRCP,Najeeb A, MRCP, Lo Kang SC, M Adv. Derm, Pubalan M, MRCP, Loh LC, MRCP, Suraiya HH, FRCP
Original Article55 A 5-yr retrospective study on the outcome
of patients with acne vulgaris treated with oral isotretinoin in Ipoh Hospital Tang JJ, MRCP, Chan LC, MMed, Heng A, MRCP
Short Communication60 Penicillin-treated plaque psoriasis:
Report of 2 cases from TaiwanAng XX, Wong SM, MRCP
NURSING
Quiz62 Dermatology Care Plan Quiz for nurses
Rohna R, MRCP
Short Communication63 Nursing challenges in a teenager with
pemphigus vulgaris and toxic epidermal necrolysis Hazfaneza AH, MBBS, Kasmahwati T, SRN, Noradiah J, SRN, Norhasmie R, SRN
ANNOUNCEMENT
Administrative Update24 Pain as a vital sign
Mary SC, FRCS (Anaes)
67 Guidelines to diagnosis of occupational dermatoses and its compensationMohammed AAM, LFOMRCP, Zainul AMH, M SC (OM)
Continuous Professional Development18 Malaysian Dermatology Congress
18 Regional Congress of Dermatology(Asian - Australasian)
28 Satellite Meeting 2009
ANSWERS TO QUIZES
68 Answers to Clinical Diagnostic Skill Test
70 Answers to Dermatology Care Plan Quiz
Keywords Juvenile systemic lupus erythematosus,juvenile dermatomyositis treatment
IntroductionPaediatric rheumatology is an emerging field inpaediatrics which deals with both inflammatory andnon inflammatory conditions of the connectivetissue and joints in children. In paediatricrheumatology, the skin remains one of the mostimportant organs which can be involved especiallywith respect to the group of inflammatoryconnective tissue diseases. In children with thesediseases, the cutaneous signs are often importantdiagnostic clues of the underlying disease.
However, due to the rarity of these conditions andthe relative inexperience by many, these cutaneoussigns can sometimes be mistakenly diagnosed. Thisnot only leads to a delay in diagnosis but alsoinstitution of appropriate therapy and a detrimentallong term outcome. In this review, the focus will beon cutaneous signs in the two main paediatricconnective tissue disorders and its currentmanagement.
Juvenile Systemic Lupus Erythematosus (JSLE)Juvenile systemic lupus erythematosus (JSLE) orchildhood lupus is a chronic multisystemautoimmune disease that accounts for 15-20% of alllupus patients. In the paediatric population,cutaneous manifestations remain one of thecommon organ systems to be involved and arepresent in an estimated 50-80% of children at initialpresentation1. In a Malaysian study of 38 childrenwith JSLE, 89% had cutaneous symptoms and signsat initial presentation of which only 55% had malarrash, 45% mucosal ulceration and 42% alopecia2.
1MJD 2009 June Vol 22
Malaysian Journal of Dermatology
PAEDIATRIC DERMATOLOGY - Review Article
Recognising cutaneous signs and the management in
paediatric connective tissue diseases
Tang SP, MRCP(Paeds) UK
Cutaneous involvement in JSLE can be either dueto lupus specific interface dermatitis or nonspecific manifestations of lupus like(photosensitivity, vasculitis, erythema or Raynaud’sphenomenon). Lupus specific cutaneous diseasecan be further divided into acute cutaneous lupus,subacute cutaneous lupus (SCLE) and chroniccutaneous (discoid) lupus (CCLE). As a result ofthis, the presentation of skin disease in lupus can bevery varied. Whilst lupus specific skin lesions serveprimarily as an important diagnostic clue to theunderlying disease, the presence non specific lupuslesions has been associated with more active SLEand hence may warrant more intensive therapy anddisease monitoring3.
The malar rash or ‘butterfly’ rash which is thetypical rash of SLE unfortunately only occurs inabout 50-70% of childhood lupus. One needs toremember that although it is pathognomonic ofSLE, it is not a diagnostic rash and can be presentin other conditions like juvenile dermatomyositis.Subacute cutaneous lesions are rare in children andoften begin as papules that evolve to annular lesionswith raised edges which can then crust, becomehyperpigmented and atrophied. Discoid skin lesionsare also relatively rare in children and characterizedby sharply demarcated papulosquamous lesionswhich are often photosensitive and heal withatrophy and scarring. It is important to note thatdiscoid lesions in children tend to have a higherchance of being associated or transitioning tosystemic lupus erythematosus as compared toadults, and hence a careful search for systemicsymptoms is warranted once a diagnosis of discoidLE is made4. Children with lupus can also presentwith various non specific rashes like maculopapularrashes, petechiae, purpura or urticaria. The fingersand nails need to be checked carefully looking fornailfold infarcts and periungual erythema.Periungual erythema which is the result of nail foldcapillary dilatation and tortuosity is not a findingwhich is specific to lupus and can be found in otherconnective tissue diseases like juveniledermatomyositis
CorrespondenceDr Tang Swee PingDepartment of PaediatricsSelayang Hospital, Selangor, MalaysiaEmail : [email protected]
2 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
dermatomyositis, juvenile scleroderma andundifferentiated connective tissue disease. In lupus,nailfold capillary abnormalities appear to be relatedto disease activity as well as the presence of variousdifferent autoantibodies like anti-cardiolipin,anti-Sm and also the presence and higher titres ofanti-dsDNA antibodies5. Livedo reticularis is alsosometimes seen in children and one needs toinvestigate for associated presence ofantiphospholipid antibodies6. Diffuse alopecia iscommon in active lupus while scarring alopecia isnot common in children. Rare presentations includevesicobullous lesions, nodules, lupus profundus andchilblain lupus. Oral mucosal lesions are alsocommon and there can either be palate erythema orclassically a shallow, ragged painless ulcer on thehard palate. On some occasions, there can also benasal septum ulceration.
As in adult patients, skin disease can sometimes beone of the most refractory clinical manifestations ofJSLE. The standard therapy consists of sunprotection, topical corticosteroids andantimalarials. In addition, children are advised toavoid direct sun exposure, wear lightweight tightlywoven clothing and use broad-spectrum, waterresistant sunscreens. Sun avoidance in particular isdifficult for children and ensuring compliance is achallenge as this often limits their physicalactivities or play especially at school or withfriends. In addition, children generally do not likeapplying sunscreens for reasons of stickiness, smellor colour especially in those who have pigmentedskin. Skin lesions of acute LE often resolve withtreatment of the systemic disease in particular theaddition of oral steroids but management of morepersistent skin lesions remain a challenge. Someadditional suggested treatments includemethotrexate, intravenous immunoglobulin,mycophenolate mofetil and more recently anti-CD20 monoclonal antibody rituximab.
Low dose methotrexate given in weekly dosages hasbeen reported in various uncontrolled case series tobe of benefit for adults with active cutaneous and/orarticular disease7,8,9. However the efficacy ofmethotrexate for skin disease in the paediatricpopulation is not so clear with two studies yieldingconflicting results. Abud- Mendoza et al treated 10children with various manifestations including 7with cutaneous symptoms and found in this group,positive response in 80% (5 excellent, 3 good) withonly 1 patient having a poor response10. However
Ravielli et al in his cohort of 11 paediatric onsetlupus of which majority had nephritis, found noresponse for the cutaneous symptoms (3 malar rashand 2 skin vasculitis) and also that methotrexate didnot show any major corticosteroid sparingpotential11.
Mycophenolate mofetil (MMF), animmunosuppressive agent initially used fortransplantation has proven to be beneficial in lupusnephritis in both adults and children. However theevidence for refractory skin disease has beenconflicting. Several adult case reports and caseseries have shown good response to MMF and thisincluded patients with refractory discoid lupus,SCLE, lupus profundus, lupus pernio, lupustumidus and chilblain lupus12, 13, 14, 15. However inanother adult case series of 7 patients who hadpreviously failed to respond to a median of 4 drugs,response to MMF was poor with only one patientshowing a partial response and another showing aninitial response but flared subsequently even whilston MMF16. Currently, most available MMF data inchildren relates to its efficacy as either an inductionor maintenance agent for lupus nephritis but there issuggestion that MMF may be of benefit especiallyin non-renal lupus although there are no specificreports on the response of refractory cutaneousdisease in children17,18,19.
Rituximab, a chimeric monoclonal anti-CD20 IgG1antibody has shown promising results in paediatricpatients with severe or refractory SLE mainlyinvolving lupus nephritis, severe vasculitis orcytopenias20, 21. There is inadequate experience of itsuse in isolated skin disease. There is a recent casereport of successful use of rituximabf22 or refractorylupus skin disease in an adult. An 11 year oldpaediatric patient with recurrent skin flares withsystemic manifestations has also been successfullytreated with rituximab and remained in remission 9months after initiating therapy23.
Oral thalidomide has also been reported to be a veryuseful agent in inducing remission for refractorylupus skin lesions in adults but its use is limited bypotential teratogenicity as well as peripheralneuropathy24,25,26. Although the response may begood, the effect of thalidomide appears not to besustained and a relapse rate of as high as 67% wasreported upon cessation of the drug in one study26.In children, data on thalidomide is scarce and iscurrently reserved only for those with severeautoimmune
3MJD 2009 June Vol 22
Malaysian Journal of Dermatology
autoimmune pathologies. A major difficultyconcerning the use of thalidomide in children is themonitoring for peripheral neuropathy. Theperipheral neuropathy unlike in adults, has beenshown to be dose-dependent especially cumulativedosages; age dependent and also occurs at asignificantly high frequency of 53.8%, and thus hasto be used with much caution27. Children may not beable to verbalise symptoms of clinical neuropathyand it is difficult to perform nerve conduction testin small children frequently. There is promise ofsafer thalidomide analogues on the horizon whichmay then make this an appropriate choice in thefuture.
Topical pimecrolimus 1% cream, an ascomycinmacrolactam which inhibits calcineurin and has noatrophogenic potential has been reported to be safeand efficacious in small cases series in adults but noavailable data in children28,29.
In our experience managing childhood lupus, mostcutaneous lesions respond to topicalcorticosteroids, antimalarials and sometimesrequire low dose prednisolone. However secondline agents like methotrexate and azathioprine donot seem to have beneficial effects in improvingrefractory skin lesions. Intravenousimmunoglobulin has been tried in 3 patients withrefractory cutaneous symptoms but we did not seeany improvement. Mycophenolate mofetil has beenused successfully in two patients with chronicdiscoid lupus with skin vasculitis - one who hadpreviously failed oral prednisolone and monthlyintravenous pulse methylprednisolone,antimalarials, azathioprine, intravenousimmunoglobulin and 6 months of intravenouscycophosphamide. The other had failedantimalarials, azathioprine and six months ofmonthly intravenous immunoglobulin. Theimprovement in the skin rash was seen as early as 2months after initiation of MMF therapy. Currently,Rituximab has been reserved for children with moresevere major organ involvement of lupus.
Juvenile DermatomyositisJuvenile Dermatomyositis (JDM) is a rare diseasebut remains the commonest of all the idiopathicinflammatory myopathies of childhood. Itcharacteristically affects the proximal musclesresulting in weakness and also the skin withpathognomonic rashes. However, the cutaneousdisease does not always parallel the muscle disease
in terms of onset, activity or response to therapy.Although both these organ systems can be affectedsimultaneously at presentation, at times themanifestation of one organ system may precede theother and often the skin rashes may be undiagnosedfor months before the clinical muscle weakness setsin. In an unpublished study of 20 Malaysianchildren with JDM, the initial presentation in 50%of the patients was cutaneous alone with only 20%presenting simultaneously with skin rashes andmuscle disease. In this cohort, facial rash was thecommonest presentation present in 90% of thepatients whilst Gottron papules was reported in75% of patients. The mean delay between onset ofskin disease to diagnosis was 15 months indicatinga significant delay in diagnosis30.
Juvenile dermatomyositis has typical skin rashwhich include the heliotrope rash and Gottronpapules. Heliotrope rash is a purplishdiscolouration of the upper eyelids whilst Gottronpapules are erythematous scaly lesions often foundover the metacarpophalangeal and proximalinterphalangeal joints as well as over the elbowsand knees. In our experience, the Gottron papulesmay sometimes just be non-discrete erythema andoften in our population especially those withpigmented skin, the rash can appears as non-erythematous hyperpigmented lesions. Lesions overthe elbows are more common than over the kneesand Gottron papules are also seen on occasions overthe distal interphalangeal joints although it isusually associated with lesions elsewhere. Childrenwith JDM can also present with a malar rash whichis often well demarcated although the area ofinvolvement can be quite small and sometimes bemissed. In some children, an extensiveerythematous rash can also occur over the wholebody whilst others can present with vasculitic orulcerative skin lesions and these often signify amore aggressive disease and a poor prognosis.Periungual erythema due to nailfold capillary loopdilatations is common and can affect both fingerand toe tips. In some instances in acute JDM, therecan also be periorbital oedema or diffuse oedema ofthe whole face whether erythematous or not. This issometimes mistaken as an allergic reaction tovarious drugs administered. Photosensitivity is alsoa feature in these patients and sun exposure canprecipitate a flare. Calcinosis and lipodystrophy areconsidered complications of inadequately orprolonged untreated disease.

4 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
Smith et al in a study of 60 newly diagnosed,previously untreated children with JDM found thatthe cutaneous manifestations were associated withend row capillary loss which indicated avasculopathy. As such, they proposed that thecutaneous manifestations of JDM are associatedwith vascular disease and hence warrant aggressivetherapy31. The presence of a persistent rash and theduration of untreated disease have also beenassociated with one of the dreaded complications ofJDM which is calcifications32. As such, cutaneouslesions of JDM need to be diagnosed accurately andgiven prompt and perhaps systemic therapy.
As in JSLE, the standard therapy for skin lesions inJDM include sun protection, topical cortiosteroidsand sometimes antimalarials. More resistant skinlesions sometimes require the addition of low doseoral corticosteroids. The use of topicalimmunosuppressive agents has largely beendisappointing. In an unblinded observational studyof 5 adults with dermatomyositis and 1 child withJDM, topical tacrolimus was reported to be a usefuladjunct in patients for refractory cutaneouslesions33. However this beneficial effect was notobserved in another study whereby none of the 5patients treated with topical tacrolimus showed anyimprovement34. Oral tacrolimus on the other hand,has been reported to be of benefit for severecutaneous manifestations in a total of 9 children in2 different case series but its role in controllingmuscle disease is conflicting in these 2 studies35,36.
Intravenous immunoglobulin has been proveneffective as an adjunctive treatment for myositis insevere JDM with improvement in disease activity aswell as permitting steroid reduction37,38. In addition,Lang et al also reported 5 children who not onlyshowed improvement in their muscle strength butalso their skin rash39. Two adult patients treated withintravenous immunoglobulin for their skin diseasein dermatomyositis have also been reported to showresponse - one complete and one partial40.
Riley et al reviewed the efficacy of intravenouspulse Cyclophosphamide in 12 patients with severerefractory JDM and of these 8 had ulcerative skinlesions. Two patients died of underlying pulmonaryinsufficiency early in the disease, but the remaining10 showed improvement after 6 months oftreatment in both muscular and extra-musculardisease including skin scores. Although all theulcerative skin disease was successfully treated,
other skin disease was also one of the mainpersistent features41.
Other drugs which have been tried include thefollowing. Infliximab has also recently beenreported to be of benefit for 5 children withrefractory JDM but the positive effect was mainlynoted for muscle disease, contractures andcalcinosis whilst skin disease was less wellcontrolled42. As in JSLE, Rituximab, a chimericmonoclonal anti - CD20 IgG1 antibody has alsobeen reported to be potentially useful for JDM in anobservational study of 4 children of which 3 showedclinical benefit regardless of status of myositisspecific antibodies43.
In our experience, monthly intravenousimmunoglobulin (IVIg) at 1g/kg/day for 2 days hasbeen used in six children with severe JDM withmoderate success. One patient with only severecutaneous disease who had failed prior therapy withoral and topical corticosteroids, antimalarials,methotrexate and topical tacrolimus showed adramatic response and went into completeremission only after 2 doses of IVIg and hasremained in remission since then. Four otherchildren showed improvement in both theircutaneous and muscle disease whilst one child didnot show any response despite having had aprolonged 12 month course of intravenousimmunoglobulin. We postulate that the poorresponse in this child is due to long term damagefrom uncontrolled inflammation which isirreversible.
ConclusionThe prognosis of common paediatric connectivetissue diseases like juvenile systemic lupuserythematosus and juvenile dermatomyositis hasimproved tremendously over the recent decadeswith better understanding of the disease as well asmore aggressive therapy. However, the treatment forcutaneous manifestations in these diseases haslargely remained the same and resistant skinmanifestations continue to be a therapeuticchallenge. The emergence and ongoing research ofnew drugs including biologic therapy have offeredpromise in these situations but more research has tobe conducted before they can be widely appliedespecially in children.

5MJD 2009 June Vol 22
Malaysian Journal of Dermatology
References
1. Wananukul S, Watana D, et al, Cutaneousmanifestations of childhood lupus erythematosus.Pediatr Dermatol 1998; 15(5): 342-6
2. Hii KC, Tang SP. Clinical and laboratory features ofjuvenile systemic lupus erythematosus at initialpresentation. (unpublished) - personal communication
3. Zecevic RD, Vojvodic D, et al. Skin lesions - anindicator of disease activity in systemic lupuserythematosus. Lupus 2001; 10(5): 364-7
4. Fenniche S, Triki S, Benmously R et al. Lupuserythematosus in children: a report of six cases.Dermatol Online J 2005; 11(2): 11
5. Riccieri V, Spadaro A et al. Nailfold capillaroscopychanges in systemic lupus erythematosus : correlationswith disease activity and autoantibody profile. Lupus2005; 14(7): 521-5
6. Weinstein C, Miller MH, et al. Livedo reticularisassociated with increased titres of anticardiolipinantibodies in systemic lupus erythematosus. ArchDermatol 1987; 123(5) 596-600
7. Sato E I. Methotrexate therapy in systemic lupuserythematosus. Lupus 2001; 10(3) 162-4
8. Asherson RA, Schatten S, Hughes GRV. Methotrexatein systemic lupus erythematosus. J Rheumatol 1997;24: 610-611
9. Wise CM, Vuyyuru S, Roberts WN. Methotrexate innonrenal lupus and undifferentiated connective tissuedisease - a review of 36 patients. J Rheumatol 1996;23(6) : 1005-10
10. Abud-Mendoza C, Sturbaum AK, Vasquez-Compean Eet al. Methotrexate therapy in childhood systemic lupuserythematosus. J Rheumatol 1993;20:731-733
11. Ravelli A, Ballardini G, Viola S et al. Methotrexatetherapy in refractory pediatric onset systemic lupuserythematosus. J Rheumatol 1998; 25(3): 572-5
12. Goyal S, Nousari HC. Treatment of resistant discoidlupus erythematosus of the palsm and soles withmycophenolate mofetil. J Am Acad Dermatol2001;45:142-4
13. Boehm I, Bieber T. Chilblain lupus erythematosus :successful treatment with mycophenolate mofetil.Arch Dermatol 2001; 137: 235-6
14. Schanz S, Ulmer A, Rassner G et al, Successfultreatment of subacute lupus erythematosus withmycophenolate mofetil. Br J Dermatol 2002; 147:174-8
15. Hanjani NM, Nousari CH. Mycophenolate mofetil forthe treatment of cutaneous lupus erythematosus withsmoldering systemic involvement. Arch Dermatol2002; 138:1616-18
16. Pisoni CN, Obermoser G, Cuadrado MJ et al, Skinmanifestations of systemic lupus erythematosusrefractory to multiple treatment modalities: poorresults with mycophenolate mofetil. Cin ExpRheumatol 2005; 23: 393-6
17. Lau KK, Ault BH, Jones DP et al. Induction therapyfor pediatric focal proliferative lupus nephritis:cyclophosphamide versus mycophenolate mofetil. JPediatr Health Care 2008; 22(5): 282-8
18. Fujinaya S, Ohtomo Y, Hara S et al. Maintenancetherapy with mycophenolate mofetil for children withsevere lupus nephritis after low-dose intravenouscyclophosphamide regimen. Pediatr Nephrol. 2008;23(10):1877-82
19. Falcini F, Capannini S, Martini G et al. Mycophenolatemofetil for the treatment of juvenile onset SLE: amulticenter study. Lupus 2009;18 (2): 139-43
20. Nwobi O, Abitbol CL, Chandar J et al, Rituximabtherapy for juvenile onset systemic lupuserythematosus. Pediatr Nephrol 2008; 23: 413-9
21. Willems M, Haddad E, Niaudet P et al, FrenchPaediatric - Onset SLE study group. Rituximab therapyfor childhood onset systemic lupus erythematosus. JPediatr 2006; 148:623-7
22. Uthman I, Taher A et al. Successful treatment ofrefractory skin manifestations of systemic lupuserythematosus with rituximab: report of a case.Dermatology 2008; 216(3): 257-9
23. Menon S. Hari P, Bagga A. Beneficial effects ofrituximab therapy for systemic lupus erythematosus.Indian J Pediatr 2007; 74(1): 79-82
24. Sato E I, Assis LS et al, Long term thalidomide use inrefractory cutaneous lesions of systemic lupuserythematosus. Rev Assoc Med Bras 1998; 44(4):289-93
25. Coelho A, Souto MI, Cardoso CR et al. Long termthalidomide use in refractory cutaneous lesions oflupus erythematosus; a 65 series of Brazilian patients.Lupus 2005; 14(6) ; 434-9
26. Cuadrado MJ, Karim Y, Sanna G et al Thalidomide forthe treatment of resistant cutaneous lupus: efficacyand safety of different therapeutic regimes. Am J Med2005; 118(3); 246-50
27. Priolo T, Lamda LD, Giribaldi G et al. Childhoodthalidomide neuropahty: a clinical andneurophysiologic study. Pediatr Neurol 2008; 38:196-9
28. Tlacuilo-Parra A, Guevara-Gutierrez E, Guiterrez-Murillo F et al, Pimecrolimus 1% cream for thetreatment of discoid lupus erythematosus.Rheumatology (Oxford) 2005; 44(12):1564-8
29. Kreuter A, Gambicher T, Breuckmann F et al.Pimecrolimus 1% cream for cutaneous lupuserythematosus. J Am Acad Dermatol 2004; 51(3): 407-10
30. TangSP, Lingesh S, Mathan RN et al. Clinical featuresof Juvenile Dermatomyositis at diagnosis. Unpublishedstudy - personal communication
31. Smith RL, Sundberg J, Shamiyah E, et al. Skininvolvement in juvenile dermatomyositis is associatedwith loss of end row nailfold capillary loops. JRheumatol 2004; 31(8) : 1644-9
32. Seshadri R, Feldman BM, Ilowite N et al. The role ofaggressive corticosteroid therapy in patients withjuvenile dermatomyositis: a propensity score analysis.Arthritis Rheum 2008; 59(7): 989-95
33. Hollar CB, Jorizzo JL. Topical tacrolimus 0.1% forrefractory skin disease in dermatomyositisL a pilotstudy. J Dermatolog Treat 2004;15:35-39
34. Garcia-Doval I, Cruces M. Topical tacrolimus incutaneous lesions of dermatomyositis: lack of effect inside-by-side comparison in five patients. Dermatology2004; 209: 247-248

6 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
35. Hassan J, van der Net JJ, van Royen-Kerkhof A.Treatment of refractory juvenile dermatomyositis withtacrolimus. Clin Rheumatol 2008; 27(11):1467-71
36. Martin Nalda A, Modesto Caballero C, Arnal GuimeralC et al. Efficacy of tacrolimus in the treatment ofrecalcitrant juvenile dermatomyositis. Med Cin (Barc)2006; 127 (18): 697-701
37. Sansome A, Dubowitz V. Intravenous immunoglobulinin juvenile dermatomyositis : four year review of ninecases. Arch Dis Child 1995; 75: 25-28
38. Al-Mayouf SM, Laxer RM, Schneider R, et al.Intravenous immunoglobulin therapy for juveniledermatomyositis: efficacy and safety. J Rheumatol2000; 27: 2498-2503
39. Lang B, Murphy G. Treatment of dermatomyositiswith intravenous globulin. Am J Med 1991;91:169-72
40. Wtter DA, Davis MD, Yiannias JA, et al. Effectivenessof intravenous immunoglobulin therapy in skin diseaseother than toxic epidermal necrolysis: a retrospectivereview of Mayo clinic experience. Mayo Clin Proc2005; 80 (1): 41-7
41. Riley P, Maillard SM, Wedderburn R et al. Intravenouscycophosphamide pulse therapy in juveniledermatomyositis: a review of efficacy and safety.Rheumatology (Oxford) 2004; 43: 491-496
42. Riley P, McCann LJ, Malillard SM et al. Effectivenessof infliximab in the treatment of refractory juveniledermatomyositis with calcinosis. Rheumatology(Oxford) 2008; 47(6): 877-80
43. Cooper MA, Willingham DL, Brown DE et al.Ritximab for the treatment of juveniledermatomyositis: a report of four paediatric patients.Arthritis Rheum 2007; 56(9) : 3107-11
7MJD 2009 June Vol 22
Malaysian Journal of Dermatology
DERMATO-ONCOLOGY - Original Article
Pattern of cutaneous malignancies in a tertiary hospital
in Sarawak
Yap FBB, MRCP, Pubalan M, MRCP
Abstract
Background Most Asian studies have determined that basal cell carcinoma (BCC) is the commonestskin cancer followed by squamous cell carcinoma (SCC), malignant melanoma (MM) and others.The pattern of cutaneous malignancies has never been determined in Sarawak. Thus, thisretrospective study was performed to determine the pattern among patients attending the skin clinicin Sarawak General Hospital.
Materials and Methods The clinic notes of 87 patients diagnosed to have skin cancerhistopathologically between 2000 and 2008 were retrieved and subjected to descriptive analysis.Analysis for the pattern of disease and demographics was performed.
Results BCC constituted the main skin cancer with 49.4% (n=43) followed by SCC with 26.4%(n=23), cutaneous lymphomas (CL) with 9.2% (n=8), MM with 4.6% (n=4) and other cutaneousmalignancies with 10.3% (n=9). The number of cases detected steadily increased over the 8 yearperiod, with most BCC and SCC diagnosed after 2003. The mean age of presentation was highest inpatients suffering from SCC at 62.7 years followed by BCC 60.9 years, MM 59 years, CL 54.3 yearsand other malignancies 40.6 years. Female predominance was noted in all the malignancies exceptsquamous cell carcinoma. Chinese constituted the majority of cases (50.6%) followed by Malays(29.9%), Bidayuhs (9.2%), Ibans (8.0%) and other indigenous people of Sarawak (2.3%). Thispattern of distribution corresponds with the racial distribution of the clinic attendance.
Conclusion Cutaneous malignancies in Sarawak differ from regional pattern in that CL is ranked asthe third commonest skin cancer and that female predominance was seen in BCC, CL, MM and otherskin cancers.
Keywords skin cancer, pattern of disease, demographics
CorrespondenceDr Yap Felix Boon Bin, MRCPDepartment of Dermatology, Sarawak General HospitalJalan Hospital, 93586 Kuching, Sarawak, MalaysiaEmail : [email protected] of interest : Nil
IntroductionCutaneous malignancy is estimated to occur in 20%to 30% of all malignancies in Caucasians, 2% to 4%of all neoplasm in Orientals, and 1% to 2% of allcancers in Africans and Indians1. It has beenrecognized as the most common malignancy amongCaucasian population2,3. In neighbouring Singapore,skin cancer is ranked seventh in their cancerregistry4.
Basal cell carcinoma (BCC) is the most commonskin malignancy in Orientals, Caucasians,Hispanics1,4,5. However, among Indians andAfricans, squamous cell carcinoma (SCC) isrecognized as the most common skin cancer6,7.
Malignant melanoma (MM) is seen as the thirdmost common cutaneous malignancy amongAsians, Caucasians, Hispanics and Africans4,7,8. InJapan, cutaneous T cell lymphoma is seen as thefourth commonest skin malignancy, representingapproximately 5% of the skin cancer9. Kaposi’ssarcoma is seen as a common cancer in Africans,representing around 10% of their cancer load10. Thepattern of skin cancer in Sarawak has never beenreported. Sarawak is unique as it is inhabited by thenative tribes. In Kuching where the SarawakGeneral
8 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
General Hospital is situated, Bidayuhs and Ibans arethe major ethnic tribes served. Skin clinic inSarawak General Hospital is the only skin referralcentre for the whole state of Sarawak. This tertiarycentre caters mainly for the Chinese, Malays,Bidayuhs and Ibans. A retrospective study isundertaken to determine the pattern of skinmalignancy seen in the Sarawak General Hospitalbetween 2000 and 2008.
Materials and methodsAll the clinic cards of patients attending skin clinic,Sarawak General Hospital between 2000 and 2008were searched. Of these, 87 patients were diagnosedto have cutaneous malignancy histopathologically.Demographic data and type of malignancy wererecorded. The data collected was subjected todescriptive analysis. The analysis was done for thepattern of the skin cancer seen and presented as thepercentage of each type of cancer. Among eachtype, demographic data regarding age, sex, race andoccupation were described. The occupationdescribed in this study is divided into those who arefrequently sun exposed e.g. farmers andconstruction workers or those who are not sunexposed e.g. clerk, administrators and housewives.This is to determine whether the cancer recordedhas any relevance to sun exposure.
ResultsBetween 2000 and 2008, 87 patients werediagnosed to have cutaneous malignancies. Ofthese, 49.4% (n=43) had BCC, 26.4% (n=23) hadSCC, 9.2% (n=8) had cutaneous lymphomas (CL),
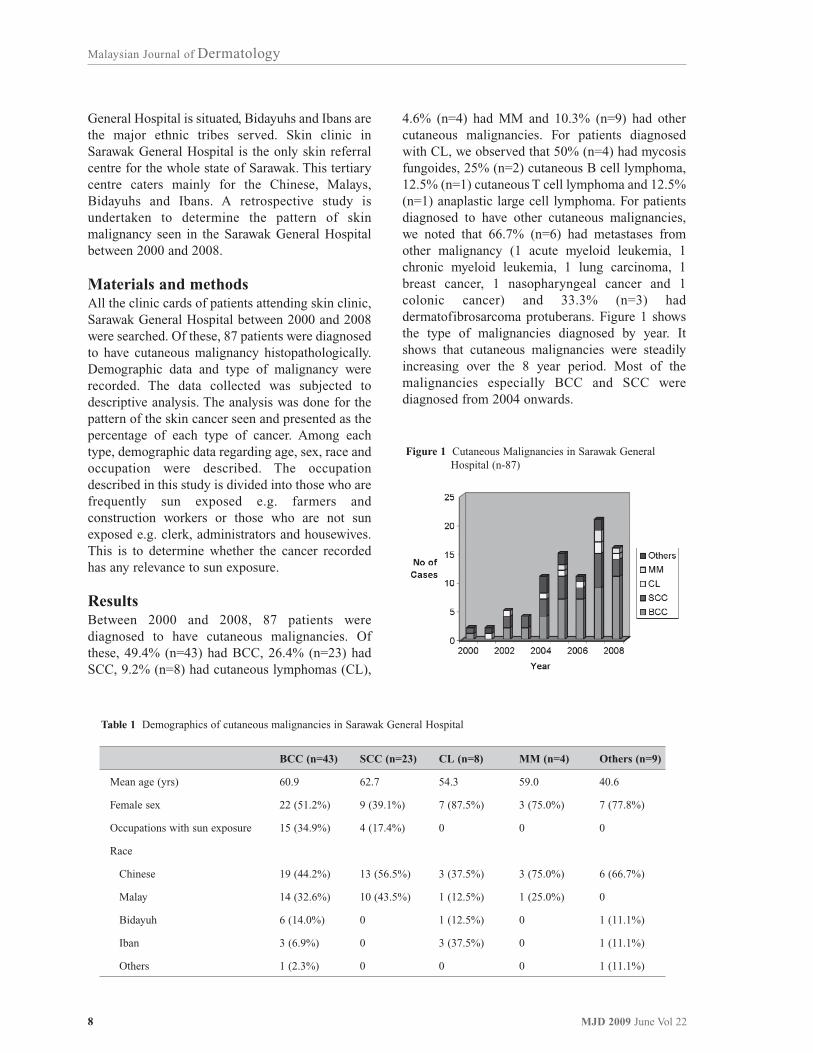
4.6% (n=4) had MM and 10.3% (n=9) had othercutaneous malignancies. For patients diagnosedwith CL, we observed that 50% (n=4) had mycosisfungoides, 25% (n=2) cutaneous B cell lymphoma,12.5% (n=1) cutaneous T cell lymphoma and 12.5%(n=1) anaplastic large cell lymphoma. For patientsdiagnosed to have other cutaneous malignancies,we noted that 66.7% (n=6) had metastases fromother malignancy (1 acute myeloid leukemia, 1chronic myeloid leukemia, 1 lung carcinoma, 1breast cancer, 1 nasopharyngeal cancer and 1colonic cancer) and 33.3% (n=3) haddermatofibrosarcoma protuberans. Figure 1 showsthe type of malignancies diagnosed by year. Itshows that cutaneous malignancies were steadilyincreasing over the 8 year period. Most of themalignancies especially BCC and SCC werediagnosed from 2004 onwards.
Table 1 Demographics of cutaneous malignancies in Sarawak General Hospital
BCC (n=43)
60.9
22 (51.2%)
15 (34.9%)
19 (44.2%)
14 (32.6%)
6 (14.0%)
3 (6.9%)
1 (2.3%)
SCC (n=23)
62.7
9 (39.1%)
4 (17.4%)
13 (56.5%)
10 (43.5%)
0
0
0
CL (n=8)
54.3
7 (87.5%)
0
3 (37.5%)
1 (12.5%)
1 (12.5%)
3 (37.5%)
0
MM (n=4)
59.0
3 (75.0%)
0
3 (75.0%)
1 (25.0%)
0
0
0
Others (n=9)
40.6
7 (77.8%)
0
6 (66.7%)
0
1 (11.1%)
1 (11.1%)
1 (11.1%)
Mean age (yrs)
Female sex
Occupations with sun exposure
Race
Chinese
Malay
Bidayuh
Iban
Others
Figure 1 Cutaneous Malignancies in Sarawak General Hospital (n-87)

9MJD 2009 June Vol 22
Malaysian Journal of Dermatology
Table 1 shows the demographic data of patientswith various cutaneous malignancies. We observeda female predominance in all the malignanciesexcept squamous cell carcinoma. Among patientsdiagnosed with MM, CL and other malignancies,more than 75% were female. The mean age ofpresentation was highest in patients suffering fromSCC with 62.7 years (range, 33 to 85 years)followed by BCC with 60.9 years (range, 35 to 83years); MM with 59 years (range, 40 to 75 years);CL with 54.3 years (range, 28 to 89 years) and othermalignancies with 40.6 years (range, 18 to 58years). Occupation related to constant sun exposurewas observed in 34.9% with BCC and 17.4% withSCC. None of the patients with CL, MM and othercancers had occupation related to constant sunexposure.
DiscussionIn Sarawak General Hospital, we noted that BCC isthe commonest skin cancer followed by SCC, CLand MM. In Singapore, Koh et al also noted thatBCC was the commonest skin cancer in their studyfollowed by SCC. However, they noted that MMwas ranked third4. The differences might beattributed to the ethnicity of the population. Seventyseven percent of Singaporeans are Chinese withFitzpatrick skin types III and IV, 14% Malays withskin type V and 8% Indians with having skin typeVI4. In Sarawak, Ibans with skin type V make up30% of the total population, Chinese 26%, Malays21% and Bidayuhs with skin type VI and V 10%11.Fairer skin Chinese are more prone to have MMthan darker skin Indians4. Moreover, Caucasianswith skin type I and II are 3 to 7 times more proneto develop MM than Hispanics with skin type II andIV. In turn, Hispanics are 1 to 4 times more pronethan blacks with skin type VI and Asians8,12.
Thus, by having a darker skin complexion,population of Sarawak are more protected fromdeveloping MM. Another possibility is that MM isunder diagnosed in Sarawak as the acral lentiginoustype commonly seen here might be misdiagnosed asother diseases e.g. fungal infection, mole andtrauma and never referred to the skin clinic forproper assessment.
The finding of CL as the third commonest skinmalignancy in Sarawak is very interesting. Thereason for the high incidence of CL of 9.2% andespecially in Ibans is unknown. Similarly, the high
incidence of mycosis fungoides of 12.1% amongblacks is also unknown7. Generally mycosesfungoides is seen twice as common in blackscompared to whites13. A possible postulate is thatthe darker skin type that protects against MMallows the expression of CL.
The pattern of primary CL seen in Sarawakcorresponds to the pattern seen in the United States.Zackheim et al noted that mycosis fungoidesconstituted 82.3% of total primary CL casesfollowed by lymphomatoid papulosis with 9.4%, Bcell lymphoma 4.5%, primary T cell lymphoma2.9% and anaplastic large cell lymphoma 0.9%14. Inour study, we found that mycosis fungoides was thecommonest primary CL seen followed by primaryB cell CL, primary T cell CL and anaplastic largecell lymphoma. However, the proportion of patientsdiagnosed with mycosis fungoides was lower, atonly 50%.
In Taiwan, 1.02% of the 12146 patients withinternal malignancies had metastasized to the skin15.The highest rates of skin metastases were found tooccur from carcinoma of the breast, followed by thelung, oral mucosa, colon and rectum, stomach, andesophagus. We also found skin metastases frombreast and colon. Interestingly, we also found apatient with skin metastases from nasopharyngealcancer, one of the commonest cancers in Sarawak.
BCC is commonly seen in males with a male tofemale ratio of 2: 116. In Australia, the incidence ofBCC in those aged under 40 is higher in womenthan men, after which rates in men exceed women17.However, our study showed the ratio of both sexeswas almost equal. In Singapore, Koh et al alsonoted an almost equal incidence of BCC among thepredominant Chinese and Malay population4. InSCC, the male to female ratio was between 1.5 and1.9 among the Singaporean Chinese4. Here, wenoted that the ratio was 1.6. CL is more common inmales with a ratio of 2:118. MM has almost equalsex distribution among Japanese but more commonin males among Singaporean Chinese4,9. InSarawak, we noted that both these conditions weremore common in females. Nevertheless, thenumber of patients in this study is small and mightnot be representative of the population in the wholestate.

10 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
Cutaneous malignancies are increased inindividuals with total, occupational, andrecreational sun exposure. Those with total andoccupational sun exposure are at increase risk ofhaving SCC while those with recreational exposurehave higher risk of MM and BCC19. The nature ofultraviolet (UV) radiation exposure responsible forBCC is unclear16. However, it is noted that the riskof BCC is associated with ease of sun burningespecially during childhood16. High cumulative UVexposure is only related to SCC. It is expected thatmost of the patients with SCC will be working andspending most of their time under the sun. However,we only noted that 17.4% of our patients with SCChad occupation related to constant sun exposure.
This might indicate that living in the tropics,without working constantly under the sun, increasesthe individual risk to skin cancer. This study islimited by its retrospective nature and the smallnumber of patients. Analysis of CL, MM and otherskin cancers were affected mainly by the smallnumber of patients with these malignancies.
In conclusion, cutaneous malignancies in Sarawakdiffer from regional pattern in that CL is ranked asthe third commonest skin cancer. In addition,female predominance was seen in BCC, CL, MMand other skin cancers in Sarawak.
References
1. Gloster Jr HM, Neal K. Skin cancer in skin of color. JAm Acad Dermatol 2006; 55: 741-60
2. Diepgen TL, Mahler V. The epidemiology of skincancer. Br J Dermatol 2002; 146: 1-6
3. LeBlanc WG, Vidal L, Kirsner RS, et al. Reported skincancer screening of US adult workers. J Am AcadDermatol 2008;59: 55-63
4. Koh D, Wang H, Lee J, et al. Basal cell carcinoma,squamous cell carcinoma and melanoma of the skin:analysis of the Singapore Cancer Registry Data 1968-1997. Br J Dermatol 2003; 148: 1161-1166
5. Kikuchi A, Shimizu H, Nishikawa T. Clinical andhistopathological characteristics of basal cellcarcinoma in Japanese patients. Arch Dermatol 1996;132: 320-4
6. Budhraja SN, Pillai VC, Periyanayagam WJ, et al.Malignant neoplasms of the skin in Pondicherry (astudy of 102 cases). Indian J Cancer 1972; 9: 284-95
7. Halder RM, Bang KM. Skin cancer in blacks in theUnited States. Dermatol Clin 1988; 6: 397-405
8. Cress RD, Holly EA. Incidence of cutaneous melanomaamong non-Hispanic whites, Hispanics, Asians, andblacks: an analysis of California Cancer Registry data,1988-1993. Cancer Causes Control 1997; 8: 246-52
9. Ishihara K, Saida T, Yamamato A. Updated statisticaldata for malignant melanoma in Japan. Int J Clin Oncol2001; 6: 109-16
10. Isaacson C. Cancer of the skin in urban blacks of SouthAfrica. Br J Dermatol 1979; 100: 347-50
11. www.sarawak.gov.my12. Bergfelt L, Newell GR, Sider JG, et al. Incidence and
anatomic distribution of cutaneous melanoma amongUnited States Hispanics. J Surg Oncol 1989; 40:222-6
13. Weinstock MA, Horm JW. Mycosis fungoides in theUnited States. JAMA 1988; 260: 42-6
14. Zackheim HS, Vonderheid EC, Ramsay DL, et al.Relative frequency of various forms of primarycutaneous lymphoma. J Am Acad Dermatol 2000; 43:793-6
15. Hu SC, Chen GS, Wu CS, et al. Rates of cutaneousmetastases from different internal malignancies:experience from a Taiwanese medical center. J AmAcad Dermatol 2009; 60: 379-87
16. Tran H, Chen K, Shumack S. Epidemiology andaetiology of basal cell carcinoma. Br J Dermatol 2003;149: 50-52
17. Staples M, Marks R, Giles G. Trends in the incidenceof nonmelanocytic skin cancer (NMSC) treated inAustralia 1985-95: Are primary prevention programsstarting to have an effect? Int J Cancer 1998; 78:144-8
18. Panda S. Mycosis Fungoides: Current trend indiagnosis and management. Indian J Dermatol 2007;52: 5-20
19. Ridky TW. Nonmelanoma skin cancer. J Am AcadDermatol 2007; 57: 484-501

11MJD 2009 June Vol 22
Malaysian Journal of Dermatology
AUTOIMMUNE DISORDERS - Original Article
Henoch - Schönlein Purpura: Relationship between
cutaneous clinical manifestations with severity
outcomes: A 5-year retrospective study
Tarita T, M Med, Lee CE, MBBS, Rohna R, MRCP
Abstract
Background Henöch - Schonlein Purpura (HSP) is an Immunoglobulin A-mediated systemic smallvessel vasculitis of childhood and adults. HSP usually presents with a classical tetrad of rash,polyarthralgia, abdominal pain, and renal disease. Complications may arise from vasculitis ofsystemic organs.
Objectives The purpose of the study was to determine the clinical patterns of HSP and whether thecutaneous clinical manifestations of HSP can prognosticate the severity outcome of the disease.
Methodology We conducted a retrospective study of all patients diagnosed with HSP bydermatologists in Selayang Hospital between January 2003 and December 2007. The data wereobtained from the case records and analyzed with regard to age, sex, race, associated triggeringfactors, cutaneous clinical symptoms and signs, associated systemic clinical features and systemiccomplications.
Results There was a total of 50 patients during this period. HSP was diagnosed more in adults thanchildren. Fifty-four percent of patients were of Malay origin. The mean age at presentation forchildren was 6.6 years and 31 years for the adult group. There was an overall female preponderancein adults HSP. Majority (48%) of patients presented within 1 week of the onset of symptoms. Thepurpuric rashes were distributed on the trunk in 20% of cases, and on the upper limbs in 56% ofcases. Vasculitic ulcer was part of the clinical features in 4% of cases while vasculitic blisters in 12%.There was a significant association (Fisher Exact Test, p =0.02) and correlation (Pearson, p = 0.03)between the extent of skin involvement with gastrointestinal haemorrhage in the former and renalinvolvement in the latter. There was no significance association between vasculitic blisters or ulcerwith the disease severity outcomes. There was no significant difference of cutaneous presentationwith regards to the triggering factors of the disease.
Conclusion The results of our retrospective study demonstrated that the cutaneous clinicalpresentation is one of the predictive factors of renal and gastrointestinal outcomes in HSP. There wasa female preponderance among HSP in adults patients with a low occurrence of articular syndromes
Keywords Henoch Schönlein Purpura, Leucocytoclastic Vasculitis
CorrespondenceDr Tarita Taib, M MedDepartment of Dermatology, Selayang HospitalLebuhraya Selayang-Kepong, 68100 Batu Caves, SelangorEmail : [email protected] of interest : Nil
IntroductionHenoch - Schonlein Purpura (HSP) is anImmunoglobulin A- mediated systemic vasculitis of
childhood and adults. Complications arise fromvasculitis of systemic organs. The long-termmorbidity of HSP is predominantly attributed torenal involvement, while the short term morbidity ismainly attributed to gastrointestinal complication.
The rash, which occurs in all patients, ischaracterized clinically as palpable purpura. Thelesions are typically nonblanching, as theyrepresent extravasation of blood into the skin, andthey

12 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
they often occur in groups that can persist for 3 to10 days1. They can occur anywhere on the skin butare often concentrated on the lower legs and arms.These vasculitic rashes may manifest with ulcer andvesico-bullous lesions. In children, localangioedema may precede the development of thepurpura. Other cutaneous manifestations includeskin oedema, urticaria and erythema multiforme.
The clinical manifestations of HSP are aconsequence of widespread leukocytoclastic
vasculitis (LCV) with IgA deposition in vesselwalls. IgA deposition in the renal mesangiumcauses nephritis in some patients. HSP is associatedwith abnormalities involving IgA1 alone, but notIgA2. Pathogenesis may due to abnormalies inglycosylation of IgA1 and IgA1-receptorinteractions2. The histopathology revealssubepidermal hemorrhages, necrotizing vasculitisof the small vessels of the dermis with IgA & C3deposition.
Figure 1 Flow-chart of the study work-process

13MJD 2009 June Vol 22
Malaysian Journal of Dermatology
Adult HSP is infrequently reported in adults overthe age of 20, is characterized by a lower frequencyof abdominal pain and fever, and a higher frequencyof joint symptoms, and renal involvement whichtend be severe3,4,5,6. It has been reported that thespread of purpura to the trunk apart from otherclinical factors; a recent infectious history, pyrexia,the spread and biologic markers of inflammation,are predictive factors for renal involvement7. Weaim to study the clinical patterns of HSP referred tothe Dermatology Department, Selayang Hospital,Malaysia and to determine whether the cutaneousclinical signs could prognosticate the severityoutcomes of the disease.
Materials and methodsThis study was conducted in a retrospective - cohortmanner after research and ethical approval.
It included all patients with HSP who werediagnosed by dermatologists in Selayang Hospitalover a 5-year period, from January 2003 tillDecember 2007. The diagnosis was establishedclinically in the presence of cutaneous syndromewith symmetrical declivitous region non-thrombocytopenic purpura. The study group wasselected by universal sampling, from thedepartment records which concluded the in-patientand out-patients census. Further data was abstractedfrom the Cerner system incorporated in SelayangHospital medical-services computers. Aretrospective review of records had eliminated afew patients diagnosed with vasculitis syndromeswhich mimicked HSP at initial presentations(Figure 1).
Details of information which was collectedincluded the demographic data, associatedtriggering factors, cutaneous clinical symptoms andsigns, associated systemic clinical features, relatedlaboratory investigations and systemiccomplications. The non - parametric variablesgathered included the following; age, duration atpresentation, haematuria, protenuria, 24 Hour-urinary protein, hemoglobin and anti-Streptolysin OTitre. Under categorical data were sex, race, stooloccult blood, skin morphology, skin distributionand HSP trigger factors.
The data findings were analyzed using SPSS(version 14.0) statistical analysis software. TheFisher's exact test was used for univariate analysis,
and multiple logistic regression for multivariateanalysis. Bivariate linear correlations are used withnumerical data. The null hypothesis postulated wereas following; 1) there is no relation betweencutaneous manifestation of HSP and the severity ofthe disease, 2) there is no relation between thedisease cutaneous manifestation and the variousHSP triggering factors.
Abbreviations• FBC full blood count• RP renal rofile • LFT liver function test • ESR erythrocyte sedimentation rate• ASOT anti-streptolysin O titre,• C3 complement factor 3,• C4 complement factor 4,• ANA antinuclear antibody,• UFEME urine full examination and
microscopic examination,• GIT gastrointestinal• UFEME urine full examination and
microscopic examination,• GIT gastrointestinal
ResultsOver the 5-year period, a total 50 patients werediagnosed with HSP of whom 27 (54%) werefemale and 23 (46%) male. The age at presentationranged between 4 to 65 yrs old (overall mean 31 +17). Among the children who comprised 10% of thestudy patients, the mean age at presentation was 6.2years, whereas in adults it was 31 years old.
Overall, 90% of patients were adults. There wasmale preponderance in the children group with amale to female ratio of 1.5:1 and a femalepreponderance in the adult group with a female tomale ration of 1.25: 1. Majority of patients (26%)seen were within the age category of 21 to 30 yrsold. The racial distribution for all cases of HSP wasas follows: 54 % Malay, 28% Chinese, 12% Indianand 6% others (table 1).
Digestive hemorrhage was found in 8 patients andrenal involvement of variable severity was found in38 patients. The age of patients who had digestivehaemorrhage is as following; 1 patient aged 6yrsold, 4 patients aged between 20 to 24 yrs-old, 2aged between 50 to 59 yrs old and 1 aged 64 yrs old.A 32 yr old Malay lady and a 20 yrs old Chineseman had urgent gastrointestinal endoscopy donewhich

14 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
which demonstrated gut vasculitis. None of thepatients reported gastrointestinal angiogramabnormality. 3 children (60% of total children) anda similar percentage of adult patients had renalinvolvement. Chronic kidney desease secondary toIg A nehropathy was documented as early as 2months after disease onset in a 25 year old Indianlady and as late as 4 years in a 33 year old Malaylady. Thirty two percent of patients weredocumented as HSP post-Sreptococcus infection.HSP was associated with a Gullain BarreSyndrome, infective endocarditis in a case, varicellazoster infection, hepatocellular carcinoma in a caseand metastatic mitotic lesions (died of myocardialinfarction) (Table 2). Several factors other thanstreptococcal infection have been known to beassociated as triggers of HSP such as Helicobacterpylori, various viral agents, foods, drugs, insectbites, vaccinations, exposure to cold and neoplasticdisorders.
Quantitative data analysis revealed that there was asignificant association (Fisher’s Exact Test, p =0.02) between vasculitic rashes distribution on thetrunk and gastrointestinal haemorrhage. Correlationanalysis showed significant correlation (Pearson p =
0.03) between distribution of vasculitic rash onhands with renal involvement and also significantcorrelation (Pearson, p = 0.03) between extent ofvasculitic rash on the trunk and upper limbs withrenal involvement. Further analysis showed nosignificant association between cutaneous clinicalmorphology and the severity outcomes of HSP.There was also no significant difference betweenthe cutaneous clinical presentation of post-Streptococcus HSP and non post-StreptococcusHSP.
The result of fischer exact test is as follows:
Chi-Square Test
a. 1 cell (25.0%) have expected count less than 5. The minimum expected count is 1.60.
b. Computed only for a 2x2 table
Pearson Chi-Square
Continuity Correctionb
Likelihood Ratio
Fisher's Exact Test
Number of Valid Cases
Value
5.357a
3.358
4.500
50
df
1
1
1
Asymp. Sig.(2-sided)
.021
.067
.034
Table 1 Baseline demographic characteristics of study patients
Characteristics
Age (mean) years
Age (years)1 - 1011 - 2021 - 3031 - 4041 - 5051 - 6061 - 70
SexMaleFemaleM: F ratio
RaceMalayChineseIndianOthers
Adult (N = 45)
31 (12 - 65)
-10 (20%)13 (26%)9 (18%)3 (6%)7 (18%)3 (6%)
20250.8: 1
241263
Children < 12yrs old (N = 5)
6.2 (4 - 9) years
5 (10%)
321.5: 1
3200

15MJD 2009 June Vol 22
Malaysian Journal of Dermatology
Table 2 Clinical manifestations of Henöch Schonlein Purpura
Clinical Presentation
Duration at presentation: Less than 1 week>/= 1 week to < 2 weeks>/= 2 weeks to < 1 month>/= 1 month
Cutaneous morphology:Palpable purpuraVesico-bullous vasculitisVasculitic ulcer
Distribution:Upper limbs
HandsForearms and arms
TrunkLower LimbsGluteal region
Articular Syndrome
Digestive Syndrome
Digestive haemorrhage
Renal involvement
HSP post Streptococcus infection
Associated systemic IllnessHepatocellular CaMetastatic mitotic lesions of unknown primaryGullain Barre SyndromeInfective endocarditisVaricella Zoster Infection
No of patients
2477
12
5062
287
25
105021
25
30
8
38
16
11111
Percentage (%)
48
100124
561450
2010042
50
60
16
76
32
Parametric correlation is used as both are categorical data
* Correlation is significant at the 0.05 level (2-tailed)
hand finger Pearson CorrelationSig. (2-tailed)N
haem + prot Pearson CorrelationSig. (2-tailed)N
handfinger
1.000
50.000
.298*
.03650
haem +prot
.298*
.03650
1.000
50.000
Correlation

16 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
DiscussionHenoch Schonlein Purpura was one of thecommonest causes of leucocytoclastic vasculitis(LCV) in our centre. Other common causes of LCVinclude drug induced, infection and connectivetissue disease. There were 50 reported HSP cases inSelayang Hospital between 2003 and 2007.
The racial predilection of HSP among the ethnicMalays probably reflects the pattern of racialattendance in the clinic. However, we believe thatthis number was underestimated as smaller Malaycommunities still reside in rural areas anduncomplicated HSP especially among childrenwere under diagnosed. The palpable purpuric rashwas not the initial presenting sign in one-quarter ofpediatric case and in infants; they tend to be amilder disease. Although the majority of cases wereseen by dermatologist within 1 week of symptom,there were still cases seen after months of symptomonset. This could be explained by the lack ofurgency by primary care doctors in referringpatients with suspected with HSP to the tertiaryhospital centre.
Although previous studies had showed malepredominance (1.5:1)8,9, our study showed adultHSP had an overall female predominance (1.2:1).The reason of this remains unclear. The childrengroup however, showed male predominance.
HSP is infrequent in adults over the age of 20. Astudy by Gedalia A et al10, showed that 75% ofpatients were between 2 to 11 years of age. BlancoR et al3 and Gedalia A et al found that 50% of theirstudy population were aged l5 years or less. AdultHSP may manifest with blisters and necrosisalthough this is rare in children. None of thechildren in our study manifested with a vasuliticulcer. This is in contrast to a study by Blancho et al3
where there was a significantly higher proportion ofcutaneous ulcers in the adult population. Vesico-bullous vasculitis was found in 20% of the childrengroup and 11% in adult group. It is worthmentioning that the cutaneous morphology of HSPin pediatric case has a tendency to become as severeas adult patient.
Overall, our study also showed a lower incidence ofarticular syndromes. Symptoms of polyarthralgiaswere reported to present in more than 80% ofpatients1. They most commonly affect the knees andankles and are often associated with edema.
Gastrointestinal manifestations are also commonsymptoms in patients with HSP; includingabdominal pain in 50%-75% of subjects, melena orguaiac-positive stools in 50%, haematemesis in30%, massive haemorrhage in 2%, andintussusception in 2%11,12,13. Our study showed 60%had gastrointestinal involvement and 16%gastrointestinal haemorrhage as evidence by apositive of stool occult blood and decrease inhaemoglobin. None of our patients presented withmassive haemorrhage. Higher percentage (20%)occurrence of digestive haemorrhage was foundamong children compared to 16% in the adultgroup. Adult HSP is characterized by a lowerfrequency of abdominal pain and fever, and a higherfrequency of joint symptoms and renalinvolvement3,4. These findings were challenged by astudy by Blancho et al who found that adults had asignificantly higher proportion of melena.However, the gastrointestinal manifestations werenoted to be more severe in the adult patients. Renalinvolvement was high in our study which reflectedthe dominant adult patients in our study. Severity ofhaematuria and protenuria had significantpredictive factors for chronic kidney disease. Thehigh number of adult HSP in our centre raised aconcern of long term sequelae of renalcomplications. Proper long term medical follow-upis required.
A few studies have looked at the outcome andprognostic factors and also predictive factors ofHSP associated with glomerulonephritis in adultpatients5,6,7. However, as the researchers were mainlynephrologists, none observed the cutaneousmanifestation in detail. There was a significantassociation and correlation between extent of rashdistribution and severity of disease outcomes. Thiswas consistent with a study by Tancrede-Bohin E etal7 who showed that the spread of purpura to thetrunk was one of the predictive factors of renalinvolvement. Our study found that there was nosignificant association between the severity ofcutaneous morphology and severity diseaseoutcomes. As the occurrence of these presentationsis rare, a higher number of cases is probablyrequired to contribute to statistical analysisconclusion. Lastly, the cutaneous clinicalpresentations didn’t signify HSP trigger factoralthough isolated cases of HSP associated withmalignancy did demonstrate the severity in extentand morphology of cutaneous presentation.

17MJD 2009 June Vol 22
Malaysian Journal of Dermatology
An epidemio-clinical study focusing on cutaneouspresentation of HSP as one of the predictive factorsof renal and gastrointestinal outcome in both adultsand pediatric population is lacking in Malaysia.Hence, identification of this prognostic factor maypermit the design of future prospective studies.
ConclusionThe result of our retrospective study demonstratedthat the cutaneous clinical presentation is one of thepredictive factors of renal and gastrointestinaloutcomes in HSP. However, for more definitiveconclusions, a prospective study would help inconfirming the results of our study.
References
1. Paul F.; Waller T A.; Brinker T M.; Riffe I Z et al.Henoch-Schönlein Purpura: A Review Article.Southern Medical Journal 2007; 100(8) : 821-824
2. Saulsbury FT. Clinical update: Henoch-Schönleinpurpura. Lancet 2007; 369(9566): 976-8
3. Blanco R, Martinez-Taboada VM, Rodriguez-ValverdeV. Henoch- Schönlein purpura in adulthood andchildhood: two different expressions of the samesyndrome. Arthritis Rheum 1997; 40: 859-864
4. Roth R, Wilz DR, Theil GB. Schönlein-Henochsyndrome in adults. Q J Med 1985; 55: 145-159
5. Fogazzi G, Pasquali S, Moriggi M. Long-termoutcome of Schönlein-Henoch nephritis in the adult.Clin Nephrol 1989; 31(2): 60-66
6. Pillebout E, Thervet E, Hill G. Henoch-Schönleinpurpura in adults: outcome and prognostic factors. JAm Soc Nephrol 2002;13:1271-1278
7. Tancrede - Bohin E. HSP in adult patients. Predictorsfor IgA glomerulonephritis in a retrospective study of57 cases. Arch Dermatol 1997;133: 438-442
8. Jennette JC, Falk RJ. Medical progress: small-vesselvasculitis. N Engl J Med 1997; 337: 1512-1523
9. Piette WW. What is HSP and why should we care? ArchDermatol.1997; 133: 515-518
10. Gedalia A. Henoch-Schönlein purpura. CurrRheumatol Rep 2004;6:195-202
11. Abdel-Al YK, Hejazi Z, Majeed HA. Henoch-Schonlein Purpura in Arab children. Analysis of 52cases. Trop Geogr Med 1990; 42:52-57
12. Hyams, Jeffrey S. Corticosteroids in the treatment ofgastrointestinal disease. Curr Opin Paediatr 2000;12(5): 451-455
13. Al-Sheyyab M, El-Shanti H, Ajlouni S. Henoch-Schonlein Purpura: Clinical experience andcontemplations on a streptococcal association. J TropPaediatr 1996; 42:200-203
14. Henoch-Schönlein purpura. Saulsbury, Frank T. MD.Current opinion in Rheumatol 2002; 13(1): 35-40
15. Micki N, Thomas S B. Henoch-Schonlein Purpura inan Adult. SKINmed 2003; 2(4):262-264
16. Wananukul S, Pongprasit P, Korkij W. Henoch-Schonlein purpura presenting as hemorrhagic vesiclesand bullae: case report and literature review. PediatrDermatol 1995; 12(4): 314-7
17. Crosby DL, Feldman SD. A pruritic vesicular eruption.Henoch-Schonlein purpura. Arch Dermatol 1990;126(11):1497-8, 1500
18. Robson WL, Leung AK. Henoch-Schönlein purpura.Adv Pediatr 1994; 41:163-194
19. Mills JA, Michael BA et al. The ARA 1990 criteria forclassification of HSP. Athritis Rheum 1990; 33(8)1114-1121

18 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
ANNOUNCEMENT - Continuous Professional Development
34th Annual General Meeting& Malaysian Dermatology
Congress
OrganizersDermatological Society of Malaysia
ThemeCutting Edge Dermatology
VenueHotel Andaman, Langkawi
Date10 - 13 December 2009
Programwebsite: www.dermatology.org.my
19th Regional Congress
of Dermatology(Asian - Australasian)
OrganizersDermatological Society of Malaysia
ThemeDermatology without Borders
VenueSutera Harbour Resort Hotel, Kota Kinabalu, Sabah (tentative)
Date28th - 31st October 2010
ProgramIncorporation of the 2nd Meeting of the AADV

19MJD 2009 June Vol 22
Malaysian Journal of Dermatology
Keywords acute cardiac failure, atopic, Churg-Strauss
IntroductionChurg-Strauss syndrome is a granulomatous small-vessel vasculitis in which multiple organ systemscan be involved. It is often diagnosed late andphysicians need to be vigilant and keep thisuncommon diagnosis in mind. The appearance ofvisible cutaneous features is often the key todiagnosis and skin biopsy is confirmatory. Earlyrecognition and aggressive therapy is required toprevent end-organ complications and mortality.
Case reportA 21 year old Chinese female event organiserpresented with a one-month history of intermittentfever with myalgia, lethargy and loose stools. Herdiarrhoea had been persistent and she was admittedfor intravenous rehydration for a period of two daysearlier in the month. Over a period of three days,she developed bilateral lower limb swelling, a non-productive cough with shortness of breath, andscattered non-painful hemorrhagic vesicles on thelower limbs and elbows.
She was a lifelong non-smoker and had a pasthistory of asthma since childhood for which she hashad multiple admissions for exacerbations. Shewas on inhaled beta-agonists and inhaledcorticosteroids. She had occasional short courses oforal corticosteroids during flares, but had nevertaken oral leukotriene antagonists before. She alsohad allergic rhinitis and chronic sinusitis, for whichshe underwent a frontal ethmoidectomy and
AUTOIMMUNE DISORDERS - Case Report
Acute cardiac failure in a young atopic patient
Pan JY1, MRCP, Yong WH2, FAMS, Audrey TWH1, FAMS
fibreoptic endoscopic sinus surgery in November2007.
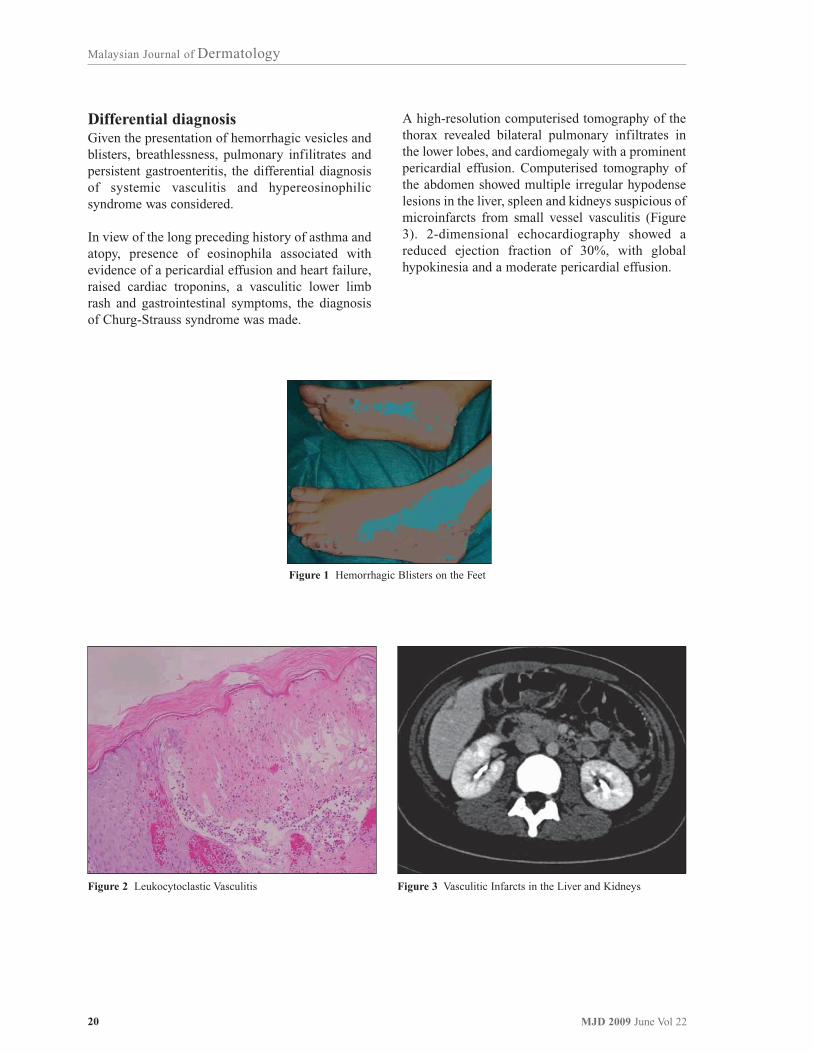
On examination, she was afebrile but tachypnoeic atrest. She had an elevated jugular venous pressure,basal crepitations on auscultation of the lungs andbilateral pitting oedema of the lower limbs to thelevel of the knees. Her blood pressure and heartsounds were normal and she did not have anymurmurs on auscultation. Abdominal examinationrevealed mild hepatomegaly but no splenomegalyand the kidneys were not ballotable. Multiplehemorrhagic vesicles and papules were noted onher feet, shins, ankles, knees and elbows (Figure 1).There was no evidence of joint swelling orsynovitis.
InvestigationInvestigations showed a haemoglobin valueof 12.4 g/dL, a white blood cell count of 24.8 x109/L (with 15.8% eosinophils) and a plateletcount of 360 x 109/L. Urea, creatinine andelectrolytes were normal. Liver functiontests revealed a raised alkaline phosphatase(139U/L) and gamma-glutamyltransferase (94U/L),with hypoalbuminaemia (32g/L). Erythrocytesedimentation rate (34 mg/L) and C-reactive protein(35.6mg/L) were both raised. Brain natriureticpeptide was raised (960 pg/mL). Creatinine kinasewas normal but Troponin I was mildly elevated(0.84 ug/L). Urine microscopy showed mildhaematuria and pyuria.
The chest X-ray showed bilateral basal pulmonaryinfiltrates and widening of the cardiac silhouette.Electrocardiography revealed small voltagescompatible with a pericardial effusion. A skinbiopsy of the hemorrhagic blisters showedleucocytoclastic vasculitis with eosinophils in thedermis (Figure 2), and direct immunofluorescencerevealed deposits of IgM and C3 on the basementmembrane. The patient was negative for anti-nuclear antibodies and anti-neutrophil cytoplasmicantibodies. She had a rheumatoid factor titre of>200 RU/ml, and hepatitis B and C serologies werenegative.
CorrespondenceDr Pan Jiun Yit1, MRCP (UK)1National Skin Centre, SingaporeE-mail : [email protected]
2Department of RheumatologyAllergy and ImmunologyTan Tock Seng Hospital, Singapore
20 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
Differential diagnosisGiven the presentation of hemorrhagic vesicles andblisters, breathlessness, pulmonary infilitrates andpersistent gastroenteritis, the differential diagnosisof systemic vasculitis and hypereosinophilicsyndrome was considered.
In view of the long preceding history of asthma andatopy, presence of eosinophila associated withevidence of a pericardial effusion and heart failure,raised cardiac troponins, a vasculitic lower limbrash and gastrointestinal symptoms, the diagnosisof Churg-Strauss syndrome was made.
A high-resolution computerised tomography of thethorax revealed bilateral pulmonary infiltrates inthe lower lobes, and cardiomegaly with a prominentpericardial effusion. Computerised tomography ofthe abdomen showed multiple irregular hypodenselesions in the liver, spleen and kidneys suspicious ofmicroinfarcts from small vessel vasculitis (Figure3). 2-dimensional echocardiography showed areduced ejection fraction of 30%, with globalhypokinesia and a moderate pericardial effusion.
Figure 1 Hemorrhagic Blisters on the Feet
Figure 2 Leukocytoclastic Vasculitis Figure 3 Vasculitic Infarcts in the Liver and Kidneys

21MJD 2009 June Vol 22
Malaysian Journal of Dermatology
Management and clinical courseThe patient was initially treated with intravenoushydrocortisone at 100 mg 6 hourly for 2 days,followed by pulsed methylprednisolone at 500mgdaily for 3 days. She was also given an intravenousinfusion of cyclophosphamide at 700mg daily for 4days.
With this treatment, the patient’s symptomsrecovered significantly, with improvement of lowerlimb swelling and resolution of the breathlessnessand diarrhoea. The vasculitic lesions on her lowerlimbs and elbows also started to resolve. She wasdischarged on oral prednisolone 45 mg daily andenalapril 2.5mg twice a day. On follow-up, thecutaneous lesions were mostly healed with noscarring.
DiscussionAllergic rhinitis, asthma, and prominent bloodeosinophilia are key features of Churg-Strausssyndrome1. It is believed to be an autoimmuneprocess due to prominent allergic features, alteredT-cell and humoral immunity, and vasculitis withcirculating IgE-containing immune complexes2.The skin, lungs, gastrointestinal, kidneys,cardiovascular and nervous systems are ofteninvolved.
Accurate diagnosis of Churg-Strauss syndrome isdifficult as individual features of the syndrome canoccur in isolation, and there may be a largetemporal gap before additional features appear. Forexample, in our patient, she had chronic relapsingasthma since childhood, together with chronicsinusitis which required surgery. As theseconditions are common in our general population,the attending physician may not be alerted to thisunderlying condition until other symptoms occur.
In 1990, the American College of Rheumatology(ACR) developed the following criteria3 tocharacterize Churg-Strauss syndrome: (1) asthma,(2) blood eosinophilia > 10% (differential leukocytecount), (3) mononeuropathy / polyneuropathy, (4)migratory lung infiltrates, (5) paranasal sinusabnormalities, and (6) histology showing a bloodvessel with extravascular granulomas. The findingof 4 of the 6 criteria has a sensitivity of 85% and aspecificity of 99.7% in the diagnosis of Churg-Strauss syndrome.
The clinical course occurs in 3 phases. Theprodromal phase usually occurs when the patient isin his twenties or thirties, presenting with late-onsetrespiratory atopy: (allergic rhinitis and asthma)which is often severe. However, our patient hadasthma from a very young age (3 years old)requiring multiple admissions, together withallergic rhinitis and sinusitis.
Asthma severity and the number of exacerbationsmay increase as the prodromal phase progresses.However, prolonged treatment of asthma maypartially suppress the signs of untreated Churg-Strauss syndrome, and the disease may not beobvious until glucocorticoids are stopped, orsubstituted for a leukotriene receptor antagonist4.Leukotriene type I receptor antagonists likemontelukast block production of LTC4, LTD4, and
LTE4 without affecting LTB4 receptors5. This results
in unopposed LTB4 activity and chemoattraction for
eosinophils and neutrophils6. This mechanism hasbeen postulated to be important in the pathogenesisof Churg-Strauss syndrome. Our patient did nothave any history of leukotriene antagonist usage,but received about three short courses of oralprednisolone every year for the treatment of asthmaexacerbations.
The second or eosinophilic phase is characterizedby prominent blood eosinophilia. Multiple organsincluding the lung and gastrointestinal tract may beinfiltrated by eosinophils. The eosinophilia that wasdetected on the full blood count examination of ourpatient during her previous admissions wasattributed to her history of atopy and asthma, withcorticosteroid-induced reductions in eosinophilcounts.
The third phase or vasculitic phase usually occurs inthe mid-thirties to forties. Systemic vasculitis of thesmall and medium vessels may occur, leading tocutaneous, coronary and mesenteric vasculitis, lunginfiltrates, pericarditis, peripheral neuropathy, andeosinophilic gastroenteritis. Our patient probablyentered the vasculitic phase over a month’s period,where she developed fever, breathlessness andpersistent diarrhea due to eosinophilicgastroenteritis, culminating in the symptoms ofcardiac failure and hemorrhagic papules andblisters on the legs over the duration of three days.The cutaneous manifestations were instrumental inalerting the attending physician to the possibility ofChurg

22 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
Churg-Strauss Syndrome and the histologicalfindings of leucocytoclastic vasculitis weresupportive of this diagnosis.
The cutaneous manifestations of Churg-Strausssyndrome are protean, ranging from erythemamultiforme-like lesions, to petechiae, purpura andecchymosis, urticarial wheals, and tendersubcutaneous nodules7. Two-thirds of patients in thevasculitic phase of disease have cutaneous lesions.The classic histologic findings are eosinophilicgranulomas surrounded by macrophages and giantcells. These granulomas are the reason for theclassical description of Churg-Strauss syndrome -`allergic granulomatous angiitis’8. A small vesselnecrotizing vasculitis may be also be commonlyfound Cardiovascular disease is a frequent cause ofmortality in Churg-Strauss syndrome9. Our patienthad evidence of pericarditis, pericardial effusion,myocardial injury with elevated cardiac troponinsand heart failure with a reduced ejection fraction.Early corticosteroid and azathioprine therapy hasbeen shown to halt worsening of biventricularfunction, leading to resolution of pericardialeffusions10. Our patient responded well to themethylprednisolone and cyclophosphamide regimedescribed above.
Allergic rhinitis is extremely common8. Otherforms of nasal and sinus involvement includerecurrent sinusitis and nasal polyposis.Exophthalmos, deafmess, chronic otitis, andeosinophilic granulomatous infiltration of the skullbase are rare late complications. Necrotizinglesions of the nasopharynx and upper airway areuncommon compared to Wegener Granulomatosis11.
Peripheral neuropathy or mononeuritis multiplexmay occur in up to 75% of patients12, which mayworsen to involve multiple nerves if untreated13.Cerebral hemorrhage and infarction are importantcauses of death. Joint and muscle involvement arerare.
About 27% of patients have kidney involvement14.Disease severity ranges from proteinuria andmicroscopic hematuria to renal insufficiency.However, renal failure is uncommon and occurs inless than 10% of patients, unlike Wegener’sgranulomatosis15. Renal infarction may result insecondary hypertension. Our patient had mildhematuria on urine microscopy, but blood pressurewas normal.
An eosinophilic gastroenteritis may occur,presenting with abdominal pain, diarrhoea, orgastrointestinal bleeding. This may precede thevasculitic phase of Churg-Strauss syndrome. Ourpatient had diarrhoea of a month’s durationpreceding the onset of the vasculitic rash and wasinitially thought to have an infective gastroenteritis.
Systemic corticosteroids are the cornerstone oftherapy, usually at high doses of 0.5-1.5 mg/kg/dayfor 6-12 weeks. Higher doses are needed forpatients with neuropathy, cardiac or renalimpairment. Eosinophil count and erythrocytesedimentation rate can be used to monitor responseto treatment and to detect relapses. Late relapsesafter a successful response to treatment are rare.
Cyclophosphamide, azathioprine and high doseintravenous immune globulin are useful in severedisease, including fulminant glomerulonephritis notresponding to corticosteroids16. Glucocorticoidscombined with interferon-alpha have been reportedto be beneficial17. Plasma exchange has not beendemonstrated to be useful18. Anti-IgE (omalizumab)was reported to improve lung function and decreaseabsolute eosinophil counts in a single patient19, butmore studies are required.
Most deaths occur in the vasculitic phase of thedisease, and are most often due to heart failure ormyocardial infarction, cerebral bleeding, kidneyfailure, gastrointestinal bleeding or statusasthmaticus. The presence of significant cardiac orgastrointestinal disease is the strongest indicator ofpoor prognosis20, and both are present in our patient.
ConclusionChurg-Strauss syndrome is a multisystem disorderin which the diagnosis is easily missed in the earlystages. Dermatologists should consider thisdiagnosis in atopic patients with unexplainedpersistent eosinophilia who develop features ofcutaneous vasculitis and other systemic symptoms.Cutaneous manifestations of Churg-Strausssyndrome, in combination with other symptoms ofthe disease, were crucial in alerting the attendingphysician to this important diagnosis. Our patienthas some indicators of poor prognosis and shouldbe followed up closely to monitor for relapses.

23MJD 2009 June Vol 22
Malaysian Journal of Dermatology
References
1. Churg J, Strauss L. Allergic granulomatosis, allergicangiitis, and periarteritis nodosa. Am J Pathol 1951;27:277-301
2. Hellmich, B, Ehlers, S, Csernok, E, Gross, WL. Updateon the pathogenesis of Churg-Strauss syndrome. ClinExp Rheumatol 2003; 21:S69
3. Masi AT, Hunder GG, Lie JT, Michel BA, Bloch DA,Arend WP, et al. The American College ofRheumatology 1990 criteria for the classification ofChurg-Strauss syndrome (allergic granulomatosis andangiitis). Arthritis Rheum. Aug 1990; 33(8):1094-100
4. Wechsler, ME, Garpestad, E, Flier, SF, et al. Pulmonaryinfiltrates, eosinophilia, and cardiomyopathy followingcorticosteroid withdrawal in patients with asthmareceiving zafirlukast. JAMA 1998;279:455
5. Drazen JM, Israel E, O’Byrne PM. Treatment ofasthma with drugs modifying the leukotriene pathway.N Engl J Med. 1999;340:197-203
6. Crooks SW, Stockley RA. Leukotriene B4. Int JBiochem Cell Biol. 1998;30:173-178
7. Schwartz, RA, Churg, J. Churg-Strauss syndrome. Br JDermatol 1992;127:199
8. Chumbley LC, Harrison EG Jr, DeRemee RA: Allergicgranulomatosis and angiitis (Churg-Strauss syndrome):Report and analysis of 30 cases. Mayo Clin Proc52:477-484, 1977
9. Hasley, PB, Follansbee, WP, Coulehan, JL. Cardiacmanifestations of Churg-Strauss syndrome: Report of acase and review of the literature. Am Heart J 1990;120:996
10. Uren NG, Hammond PJ. Myopericarditis in Churg-Strauss syndrome. Texas Heart Institute Journal1991;18:127-31
11. Specks, U. Pulmonary vasculitis. In: Interstitial LungDisease, 4th ed, King, TE Jr, Schwarz, MI (Eds), BCDecker, Hamilton, ON 2003. p. 615
12. Guillevin, L, Cohen, P, Gayraud, M, et al. Churg-Strauss syndrome. Clinical study and long-term follow-up of 96 patients. Medicine (Baltimore) 1999;78:26
13. Hattori, N, Ichimura, M, Nagamatsu, M, et al.Clinicopathological features of Churg-Strausssyndrome-associated neuropathy. Brain 1999; 122(Pt 3):427
14. Sinico RA, Di Toma L, Maggiore U, et al. Renalinvolvement in Churg-Strauss syndrome. Am J KidneyDis 2006; 47:770-779
15. Clutterbuck, EJ, Evans, DJ, Pusey, CD. Renalinvolvement in Churg-Strauss syndrome. Nephrol DialTransplant 1990; 5:161
16. Hellmich, B, Gross, WL. Recent progress in thepharmacotherapy of Churg-Strauss syndrome. ExpertOpin Pharmacother 2004;5:25
17. Tatsis, E, Schnabel, A, Gross, WL. Interferon-alphatreatment of four patients with the Churg-Strausssyndrome. Ann Intern Med 1998;129:370
18. Guillevin, L, Cevallos, R, Durand-Gasselin, B, et al.Treatment of glomerulonephritis in microscopicpolyangiitis and Churg-Strauss syndrome. Indicationsof plasma exchanges, meta-analysis of 2 randomizedstudies on 140 patients, 32 with glomerulonephritis.Ann Med Interne (Paris) 1997;148:198
19. Giavina-Bianchi, P, Giavina-Bianchi, M, Agondi, R,Kalil, J. Three months' administration of anti-IgE to apatient with Churg-Strauss syndrome. J Allergy ClinImmunol 2007;119:1279
20. Guillevin, L, Cohen, P, Gayraud, M, et al. Churg-Strauss syndrome. Clinical study and long-term follow-up of 96 patients. Medicine (Baltimore) 1999;78:26
24 MJD 2009 June Vol 22
Malaysian Journal of Dermatology
ANNOUNCEMENT - Administrative Update
Pain as a 5th vital sign
Mary SC, MMed (anaes)
Ministry of Health Malaysia has introducedpain as a 5th vital sign this year. It isparticularly relevant in Toxic EpidermalNecrolysis where uncontrolled pain may havesevere systemic consequences and increasesmorbidity and mortality.
Regular analgesia may be required for severepain, given 1/2 hr prior to dressing. DF118,Tramadol morphine may be considered.
Self-administered analgesia i.e. PCA (patientcontrolled analgesia) with morphine may beindicated if patient is in severe pain.
After administering analgesia, we need to re-assess the patient. Increasing the dose ofanalgesia or changing to other analgesic maybe required if the patient continues to havesevere pain. Assess pain score on admissionto assess the severity of pain (baseline score),1/2 an hour after analgesics given to assessanalgesic action and every time vital signstaken (4 hourly) as the 5th vital sign.
CorrespondenceDr Mary Suma Cardosa Department of AnaesthesiaSelayang Hospital, Selangor, Malaysia Email : [email protected]