Embed Size (px)
Citation preview

Session 2: Localized prostate cancer
Role of radiotherapy
Jeffrey Tuan, FRCR
Radiation Oncology
National Cancer Centre Singapore15 Dec 2016

Structure
• Modern treatment technique
• Dose escalation – Hypo fractionation; SBRT;
HDR
• Permanent seed implantation; LDR
• Combination with hormonal treatment (intermediate and high-risk)
• Side effects
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 2

Mechanism of Action of RT
• Radiotherapy causes DNA Damage
• Ionizing the atoms making up DNA to cause double-stranded breaks
• Direct: Direct Ionizing damage to DNA
• Indirect: Indirectly ionizing via formation of free radicals (majority)
• Fate of irradiated cells:
• No effect
• Apoptosis (early)
• Cell senescence
• Mitotic catastrophe (late)
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 3

4 field technique of prostate and pelvic lymph nodesMoss and Cox, textbook of Radiation Oncology 1990
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 4

EBRT
• Cornerstone of curative management of localized
prostate cancer
– 25% for patients <65 years
– 50% patients >65 years
• 1990s: dose escalation 64-60>70-74>76-80Gy
– 5 year FFBF (L,I,H): >90%, 60-85%, 50-70%
– 10 year FFBF (L,I,H): 45-90%, 40-60%, 20-50%
– 5 year OS/DM/CSM: 82-97%/1-14%/0-8%
– RTOG late G3 <5% (depends on 3DCRT vs. IMRT)
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 5

Dose escalation
RCT show dose escalation >70Gy associated with improved bDFS
• If dose >75Gy use of IMRT with daily image guidance essential
– Low risk: 75.6-79.2Gy
– Intermediate to High risk: 75.6 -81.0Gy
• PTV whole prostate with 1cm margin all around except posterior 0.5-1cm
• Pelvic LN should be treated in all high risk patients or PLN risk >15% to dose of 45-48.6Gy
• Dose to Enlarged PLN 54-79.2Gy
Rectal bleeding (Laser-surgery, Transfusion) 3D-CRT
Peeters et al IJROBP 61:1019, 2005
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 6

Evolution of RT techniques
• 3DCRT to IMRT
– IGRT: portal imaging, kv
kv, fiducials, MVCT, CBCT,
intra-fraction, tracking
– VMAT
• Enable Dose escalation
• Decreased toxicities
(GI); GU similar
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 7

Intensity-modulated Radiation therapy, proton therapy, or conformal radiation
therapy and morbidity and disease control in localized prostate cancerSheets et al., JAMA 307, 2012
• IMRT lowers probability of new tumor treatment
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 8

Image guided RT (IGRT): in room 3D tools
Trans-perineal ultrasound systemUsed for image registration, set up and monitoring of intra-fractional movement
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 9

Improved outcome with IGRT
• N=376, TD 86.4Gy IMRT
• 186 with daily IGRT
• 190 without daily IGRT
• Med FU: 2.8 years
Zelefsky et al. , Int J Radiat Oncol. Biol. Phys. 2012
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 10

Dose escalationDearnaley at al, Lancet Oncol 15, 2014
• RT01 Dose escalation trial
• 843 patients– N=421: 64Gy -32Fx
– N=422: 74Gy -37Fx
– T1-T3a N0 M0
– PSA <50ng/ml
• Neo adjuvant ADT 6-9 mo
• Med FU 10 years
• OS no difference
• bNED:20% benefit
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 11

Biochemical failure at 10 yearsHou et al , J Cancer Res Clin Oncol, 2014
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 12

Overall survivalHou et al , J Cancer Res Clin Oncol, 2014
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 13

RT fractionation Arcangeli and Greco Nat Rev Urol 2016 Jul; 13(7):400-8
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 14

Dose and fractionation
• RT is delivered in fractions over several treatment sessions.
– Protects non-malignant tissues: • Repair of sub lethal damage
• Repopulation of cells in between fractions.
– Increases tumor damage: • Re oxygenation of hypoxic cells
during treatment, causing them to be more radiosensitive
• Redistribution of tumor cells into more radiosensitive phases of the cell cycle
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 15

Hypo fraction: what is α/β?
• α/β ratio: Suggests response of different tissues to ionizing radiation.– Dose where linear and quadratic
component cause the same amount of cell killing.
• Large ratio: Suggests early-responding tissues– More sensitive to radiation
– Less affected by fraction size
• Small α/β ratio: Suggests late-responding tissues– Less sensitive to radiation
– More affected by fraction size
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 16

Hypo fraction: what is α/β?
• Radiobiological description (for radiation sensitivity)
• Estimated on the basis of experimental and clinical data
• Normal: is high (>8) for tumor
• For PCA: reported to be 1.5 +/-0.3 (Fowler at al, Acta Oncologica 44(3):265-276, 2001)
• Lower than rectum and bladder (~5)
• Suggest significant fractionation sensitivity
• Higher single doses (>2Gy) better
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 17

Hypo-fractionated radiotherapy for organ-confined
prostate cancer: is less more? Arcangeli and Greco Nat Rev Urol 2016 Jul; 13(7):400-8
• Conventional fractionated vs. hypo fractionated similar outcomes
• 50-66Gy in 2.1-3.5Gy/#
– 5 year FFBF (L,I,H risk): >90%, 60-85%, 50-70%
– 10 year FFBF: 45-90%, 40-60% 20-50
– Late GU and GI similar
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 18

Conventional versus hypo fractionated high dose radiotherapy for prostate cancer: 5-
year outcomes of the randomized, non-inferiority, phase 3 CHHiP trialDearnaley et al 17: 1047-60 Lancet Oncol 2016
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 19

Conventional versus hypo fractionated high dose radiotherapy for prostate cancer: 5-
year outcomes of the randomized, non-inferiority, phase 3 CHHiP trialDearnaley et al 17: 1047-60 Lancet Oncol 2016
• Biochemical failure-free rates: hypo
fractionation 60Gy/20# non-inferior
to conventional fractionation (HR
0.84, 90% CI 0.68-1.03, p=0.0018)
• Overall survival: no significant
difference between all groups
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 20

Clinical recommendation
• Can be recommended as an alternative to conventional fractionation for carefully selected patients
• Efficacy and toxicity are similar to conventional fractionated IMRT in most trials – at least at early time point (5yr follow up)
• Shorter fractions beneficial in improving health-related quality of life
– Shorter duration of treatment
– Fewer days off work
• Data mostly for primary treatment – insufficient data for hypo fractionation in adjuvant setting
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 21

SBRT
• Extreme hypo fractionation
• Taking advantage of low
α/β• Short follow up (~5years)
• 36.25Gy/5#
• 5 year FFBF: >85% for low
risk patients
• Seems to result in greater GI
toxicity
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 22

How is SBRT delivered?
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 23

EvidenceArcangeli and Greco Nat Rev Urol 2016 Jul; 13(7):400-8
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 24
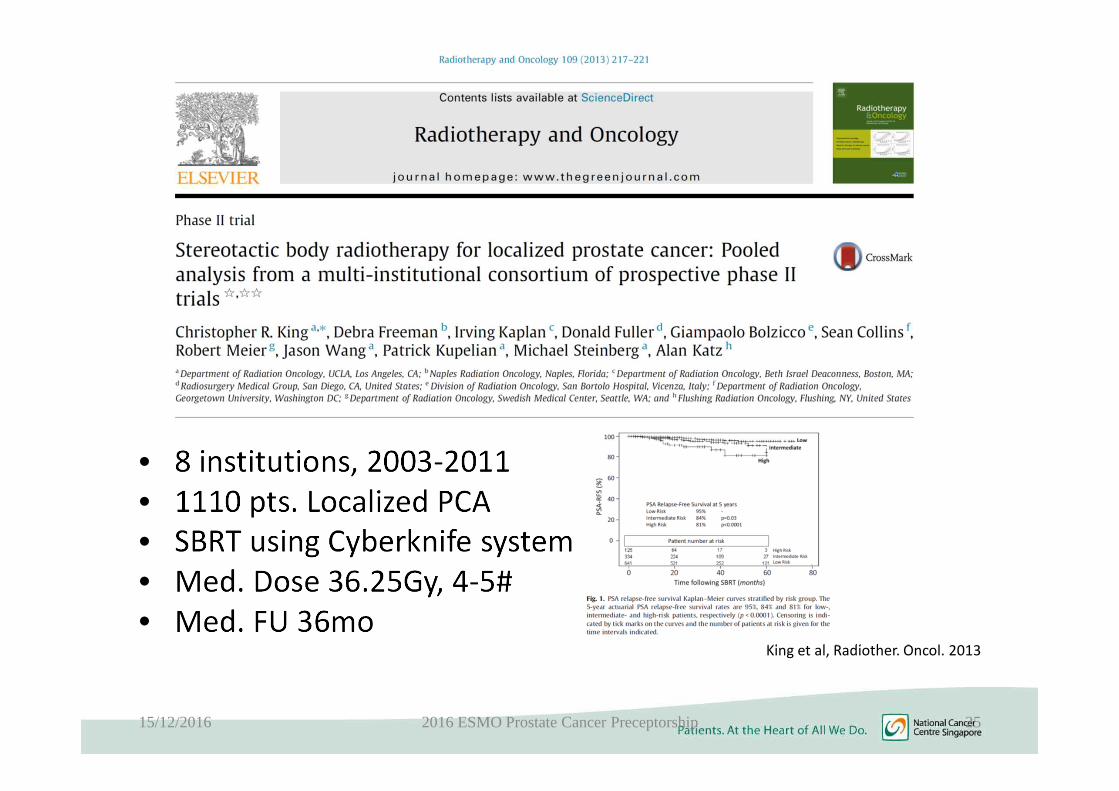
• 8 institutions, 2003-2011
• 1110 pts. Localized PCA
• SBRT using Cyberknife system
• Med. Dose 36.25Gy, 4-5#
• Med. FU 36moKing et al, Radiother. Oncol. 2013
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 25

Katz et al Front Oncol. 2014 Oct 28;4:301
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 26
ASTRO SBRT model policy
• Consider cautiously as an alternative to conventional fractionated regimens.
• The evidence is not strong enough to justify widespread use
• Requires longer follow-up data (>10 years)
• Larger scale studies (multi-institution)
• But the current interim data suggest that it is at least as good as other types of RT for patients with equivalent risk levels.
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 27

HDR
• HDR after loader, planning
systems
– a/b of prostate cancer (~1.5)
• Iridium source
• Low risk: Monotherapy (short
follow up) 31.5-38Gy in 3-4#
• High risk: Boost (19-21gy 2#;
15gy/1#) with EBRT 45Gy
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 28

LDR: permanent implants
Permanent implants; 145Gy/125Gy
Iodine125 /palladium 103 (monotherapy for
low, low intermediate risk)
PSA<15, GS6-7, T1-2c
5 year FFBF: >85%, 69-97%, 63-80%
As boost: 5 year FFBF 85%
Similar OS DM CSM as EBRT
Contraindications: no rectum, large gland size,
pubic arch interference, large TURP, low peak
flow, fit for anesthesia
Toxicity: urinary stenosis
Advantages: less radiation exposure to bladder and
rectum, low risk of RT toxicity due to short range of
radiation, low rates of impotence
Disadvantages: anesthesia, radiation protection
issues, higher irritative and voiding problems
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 29

Multi-institutional analysis stage T1-2 with LDRZelefsky et al., Int. J. Radiat. Oncol. Biol. Phys. 67,2007
• I-125 dose >130Gy D90: 8 years bNED 93% vs. 76% (p<0.001)
• Quality of implantation important
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 30

Comparative analysis of prostate-specific antigen free survival outcomes for patients
with low, intermediate and high risk prostate cancer treatment by radical therapy
Results from the Prostate Cancer Results Study Group Grimm P et al BJU Int. 2012 Feb;109 Suppl 1:22-9
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 31

Neo-adjuvant HT + RT
• Reduction of prostate mass (20-30%)
• Reduce clonogenic tumor cells
• Reduce proportion of bladder/rectum: high dose level
• Reduce D95 bladder: 40-50%
• Reduce D95 rectum: 15-20%
• Conclusion:
– Dec. rate of late side effects
– Inc. tumor control rate
Zelefsky at al., Urology 1997
Pollack and Zagars, Sem. Radiat Oncol 1998
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 32

Neo-adjuvant HT + RTD’Amico et al., JAMA 299,2008
• Prospective Ph3 RCT
• 206 pts.
• 70Gy vs 70Gy + 2+2+2
mo HT
• Randomization: 1995-
2001• Med. FU: 7.6yrs
• 5 year OS88% vs 78% (p<0.05)
• 7 yrs HR 1.8 (p=0.01)
• Low co-morbidity rate: HR 4.2
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 33

Increased mortality with ADTNguyuen at al., JAMA 306, 2011
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 34

Adjuvant RT
• High risk features: + margins, ECE, SV
involvement, persistent PSA elevation
• 3 RCT shows upfront adjuvant therapy
improves local control, risk of metastasis, OS
vs. observation
– Within 4 mo and PSA<1.5
– Adjuvant 64-66Gy; salvage 66-70.2-79.2Gy
– Early salvage vs. adjuvant not clear
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 35

Protons
• Excellent disease control
rates and a low side effect
profile in prospective series
• Good quality-of-life and
high patient satisfaction
rates
• Reduced risks of 2nd
radiation-associated
malignancies than other
external beam techniques
• More expensive
• Limited evidence
• Toxicity may not be
better
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 36

Randomized trial comparing conventional-dose with high dose conformal radiation
therapy in early-stage adenocarcinoma of the prostate: Long-term results from
Proton Radiation Oncology Group/American College of Radiology 95-09Zietman et al JCO 2010 Mar 128 (7) 1106-11
• At 10 years the phoenix BF rates were 30%
vs 17.4% for conventional vs. high dose
grps
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 37

• Results
• PSA-FFS– Low risk 99%, intermediate risk 99%
– High risk 76%• Late G3 GU ~5%
• Late G3 GI ~1%
• Patient reported QOL outcomes bowel and urinary scores relatively stable
• Some decline in sexual scores
Int J Radiation Oncol Biol Phys 88;2014
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 38

• A proton therapy plan and a 6-MV IMRT plan were constructed
• The risk of an SMN was estimated by use of risk models from the Committee on the Biological Effects of Ionizing Radiation.
Results:
• Proton therapy reduced the risk of an SMN by 26% to 39% compared with IMRT.
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 39

Toxicities
• GU: urine frequency, dysuria, hematuria
• GI: rectal bleeding, cramping, diarrhea
• Sexual: RT vs age related vs. ADT
• 2nd cancers
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 40

IMRT Results MSKCCZelefsky et al., J. Urol 176, 2006; Alikus et al., Cancer 2011
• MSKCC New York
• 1996-2000:561 pts
• 81Gy
• N=170
• Med. FU:99 mo
5 years 10 years
Erectile dysfunction (%) 51
GU-late side effects G2/3 (%) 9/3 11/5
GI-late side effects G2/3 (%) 2/0.1 2/1
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 41

Erectile dysfunction after RT
• 5 years after RT:30-60%
• 2 randomized trials
• Double blind, placebo-controlled
• 60 pts• Sildenafil and Tadalafil (20mg)
• 50-60% significant improvement
Oheshalom et al., J. Urol. 174, 2005
Incrocci et al., Int J. Radiat. Oncol. Biol. Phys. 66, 2006
Budaeus et al. Eur. Urol. 2012
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 42

Secondary cancers – Re-analysis of the SEER data
• What is the risk?
• Conclusion: patients choosing EBRT might be at a greater absolute risk of developing a second malignancy – not just from the RT per se, but possibly related to other factors such as longer follow up or older age, or more risk factors – an additional 207 cases of 100,000 patients or 0.2% can be expected. However the incidence of second cancers that could be possibly RT-induced (RTSPC) was shown to be 162 of 100,000 or 0.16% in the present study – although it might be actually be significantly lower …
Abdel-Wahab et al., Int. J. Radiat. Oncol. Biol. Phys. 72, 2008
Secondary tumors: 0.2% (207/100 000)
Real RT-induced tumors: 0.16% (162/100 00)
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 43

Conclusions
• RT, RP, LDR, and AS comparable for low risk PCA
• IMRT with IGRT standard, total doses 74-80Gy
• Intermediate risk: 4-6mo ADT, RT alone dose 76-78Gy
• High risk: selected cases 6 mo ADT, usually 2-3 years, RT 76-78Gy
• Severe side effects: GI>2%, GU more common,
erectile dysfunction
15/12/2016 2016 ESMO Prostate Cancer Preceptorship 44

Thank you
New NCCS
4 gantry PTC + 17 RT
bunkers
Integrated labs
2021
4515/12/2016 2016 ESMO Prostate Cancer Preceptorship





























