Embed Size (px)
Citation preview

0
0.2
0.4
0.6
0.8
1
2.5 5 10 15
Ne
gati
ve P
red
icti
ve V
alu
e
% of Fusion Positive Sample in 200ng Input Material
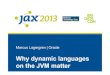
Limit of Detection Determination
y = -36484x + 1E+06
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
450,000
500,000
202122232425262728293031
# o
f U
niq
ue
Re
ads
Cycle Threshold (Ct) Value
Evaluation of the Archer FusionPlex Solid Tumor Panel in the JAX Cancer Treatment ProfileTM
Samantha Helm1, Talia Mitchell1, Aleksandra Ras1, Vanessa Spotlow1, Kevin Kelly1, Susan Mockus1, Cara Statz1, Guruprasad Ananda1, Joan Malcolm1, Gregory J. Tsongalis1, 2
1The Jackson Laboratory for Genomic Medicine, Farmington, CT. 2Dartmouth Hitchcock Medical Center and The Audrey and Theodor Geisel School of Medicine at Dartmouth, Lebanon, NH.
Different tumor types are often associated with reoccurring mutations. Performing detailed genetic profiling to identify the milieu of actionable gene variants characteristic of specific tumors may guide targeted approaches to treatment, as well as uncover new therapeutic targets. To this end, we used the JAX Cancer Treatment ProfileTM (JAX-CTPTM), a next-generation sequencing (NGS)-based molecular diagnostic assay, to identify characteristic actionable variants across various solid tumors. A comprehensive somatic tumor profile with associated treatment selection options requires the detection of gene fusions. Therefore, the JAX Cancer Treatment Profile™ (JAX-CTP) assay was modified and optimized to incorporate the detection of fusions. The Archer FusionPlex Solid Tumor Panel (AFPSTP) best met the needs of a clinical assay, in terms of workflow, specimen type, nucleic acid input material, streamlined analytics and turnaround time. Once verified, the JAX® Genomic Medicine (JAX® GM) in-house Clinical Knowledgebase (CKB) will then be utilized to generate a clinical report informing the selection of targeted therapeutics for cancer treatment.
Materials and Methods
Among the 6 JAX PDX lung cases, 2 samples were found to contain EML4-ALK variant 3b, both of which corresponded to tumor strains originating from the same patient. The EML4-ALK fusion found in 2 of the PDX samples had been previously identified by an independent technology, which further validates this finding. Among the cell lines included in the validation, 9 showed fusion events that have been previously identified by independent technologies. The remaining samples were determined to be wild-type. The turn around time for this assay was approximately 4 days.
Results
This analysis demonstrates analytical validation for the incorporation of Archer FusionPlex Solid Tumor Panel into the JAX-CTP™ test system. The limit of detection at 5% corresponds to a minimum of 15 supporting reads and 5 unique start sites. Intra- and inter-assay reproducibility studies demonstrated 100% concordance between samples. The Archer fusion detection assay enables novel and known fusion detection with ease and an acceptable turn around time for a clinical laboratory. RT-PCR will be used as an inexpensive and efficient way of confirming novel fusions.
After the successful evaluation process a full validation of the AFPSTP assay was conducted. AFPSTP was validated using 25 samples consisting of 6 JAX Patient Derived Xenograft (PDX) lung cases (RNA purification performed with a Trizol-based method), 4 known positive control samples acquired from HorizonDX (total nucleic acid purified utilizing Qiagen RNeasy FFPE kit), 12 cell lines, 2 DHMC samples, and a normal human RNA sample from Amsbio. Library preparation was performed according to Archer’s Universal RNA Reagent kit v2 protocol for Illumina. This protocol utilizes a PCR-based enrichment method with primers for 53 genes specific to fusions in solid tumors. A Pre-Seq qPCR QC assay was performed to determine the quality of the input material. Final libraries were quantified by qPCR and sequenced on an Illumina MiSeq using a FASTQ Generation workflow. Analysis was performed using Archer Analysis v3.3. The validation consisted of a sensitivity study as well as an inter and intra-assay reproducibility study.
JAX Clinical Genomics Booth #1804 JAX® Genomic Medicine | 860-837-2320 | www.jax.org/clinical-genomics | [email protected]
Background
Conclusions
MBC Adapter Structure
Utility of the Pre-Seq Quality Assessment
Before proceeding to library preparation, an RT-PCR quality assessment is performed on the newly synthesized cDNA. This generates a Ct value for each sample, which negatively correlates to the number of unique sequencing fragments. Any sample with a pre-Seq Ct value over 30 is not processed through the remaining portions of the assay due to insufficient quality of the input material.
CTP™ Workflow with AFPSTP Assay Incorporation
Observed False Positives
Wild-Type Read Through Fusion Events
Homologous Gene Mispriming Fusion events
ADCK4-NUMBL TEX40-ESRRA ETV4-ETV1 & ETV4-ETV1 PRCKG-PRCKB
Samples Known Fusions HorizonDx ROS+ Control SLC34A2-ROS1 HorizonDx RET+ Control CCDC6-RET
HorizonDx EML4/ALK+ Control EML4-ALK variant 1
HorizonDx ALK, RET, ROS + Control
EML4-ALK Variant 1 SLC34A2-ROS1
CCDC6-RET JAX PDX Specimen 1&2 EML4-ALK variant 3b
ASPS-1 cell line ASPSCR1-TFE3 A673 cell line EWSR1-FLI1 VCaP cell line TMPRSS2-ERG
KM-12 cell line TPM3-NTRK1 RPMI-2650 cell line BRD4-NUTM1 NCI-H716 cell line FGFR2-COL14A1 OCI-AML2 cell line MBNL1-RAF1
REH cell line ETV6-RUNX1 MDA-MB-175-VII cell line TENM4 -NRG1
Specimen Arrival
Day 1: All prep
Extraction
RNA Through AFPSTP Assay
Day 2 • Random Priming • cDNA Synthesis • Pre-Seq QC • End Repair/dATail • Adapter Ligation • First PCR
DNA Through Target Enrichment
• Fragmentation • End Repair/dATail • Adapter Ligation • Pre-capture PCR • Hybridization
• Second PCR • Quantification • 2nM Dilutions • Pooling • MiSeq
Sequencing
• Hyb Wash • Capture PCR • Quantification • 2nM Dilutions • Pooling • NextSeq
Sequencing
Day 3
Day 4
Sequencing Sequencing
Submission to Archer Analysis Virtual Machine
Day 5
Upon completion of analysis, both sets of data are sent simultaneously to curation to generate one cohesive patient report
Fastq Generation and Submission
to Analysis Pipeline




















![Loading [MathJax]/jax/output/CommonHTML/jax](https://img.dokumen.tips/doc/110x75/625335b291158e3f663c6c05/loading-mathjaxjaxoutputcommonhtmljax.jpg)






