Embed Size (px)
Citation preview
LETTERS TO THE EDITOR
ISOLATED MUSCULOCUTANEOUS NERVEPALSY DURING SLEEP
The musculocutaneous nerve originates from the upperand middle trunks of the brachial plexus (C5, C6, andsometimes C7) and runs in the lateral cord. Its motorbranches supply the coracobrachialis, biceps brachii, andbrachialis muscles, and the sensory branch innervates thelateral aspect of the forearm as the lateral antebrachialcutaneous nerve (LACN). There are several reports ofnontraumatic isolated musculocutaneous nerve pal-sy,1,2,5,9–11 usually associated with heavy exercise involvingthe arm. We report a case of unilateral isolated musculo-cutaneous nerve palsy developing during sleep and result-ing from complete conduction block between the axillaand Erb’s point.
A 35-year-old man with no previous medical historyexperienced weakness in right elbow flexion and paresthe-sias in the lateral aspect of his right forearm when heawakened after 8 h of sleep. On the previous evening, hehad drunk a large quantity of alcohol and slept in anunusual prone position with his head resting on his fullyabducted right arm. Neurological examination revealedweakness in the right biceps brachii muscle (grade 2 onthe Medical Research Council scale). Power in the othermuscles of the right arm was normal. The right bicepstendon reflex was absent. Hypalgesia was noted in thelateral aspect of the right forearm, in the cutaneous terri-tory of the LACN.
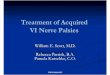
Electrophysiological studies were performed 2 days af-ter the onset of the palsy. Compound muscle action po-tentials (CMAPs) were recorded from the biceps brachiimuscle using surface electrodes in a belly–tendon arrange-ment.12 Supramaximal electrical stimuli of the musculocu-taneous nerve were applied at the axilla and Erb’s point bya standard surface stimulator. For Erb’s point stimulation,collision stimulation6 of the radial nerve at the axilla wasperformed to eliminate contamination by volume-conductedpotentials from the triceps brachii muscle. An almost com-plete conduction block was observed in the right musculo-cutaneous nerve between the axilla and Erb’s point (Fig. 1a).The LACN was stimulated at the elbow just lateral to thetendon of the biceps brachii muscle, and sensory nerve ac-
tion potentials (SNAPs) were recorded from the lateral fore-arm 15 cm more distally (antidromic recordings) and fromErb’s point (orthodromic recordings) using surface elec-trodes. Antidromic sensory conduction velocity (SCV) andSNAP amplitude of both LACNs were normal (61.2 m/s and20.9 �V, respectively, on the right, and 60.6 m/s and 21.9 �Von the left). The orthodromic SCV and SNAP amplitude atErb’s point were 65.3 m/s and 2.5 �V, respectively, on the leftLACN, but could not be evoked on the right. Motor andsensory conduction studies of the right median, ulnar, andradial nerves were also performed by standard methods andwere normal. Needle electromyography of the right bicepsbrachii muscle showed no abnormal spontaneous activitiesand a reduced interference pattern at maximal force withnormal motor unit potentials.
The paresthesias and hypalgesia in the lateral forearmdisappeared in 1 month, and the weakness of the bicepsbrachii muscle gradually improved over a period of 5months. No muscle atrophy in the biceps brachii musclewas observed. The motor conduction studies performed 1and 5 months after onset of the palsy showed an improve-ment in the conduction block without a reduction of the
FIGURE 1. Motor conduction studies of the musculocutaneousnerve 2 days after the onset (a), 1 month later (b), and 5 monthslater (c). Motor conduction velocity (MCV) between Erb’s pointand axilla is indicated. The compound muscle action potentials(CMAPs) at Erb’s point were obtained after collision and subtrac-tion of the CMAPs by radial nerve stimulation at the axilla. Analmost complete conduction block was observed between theaxilla and Erb’s point in the right musculocutaneous nerve, whichresolved completely at 5 months.
Letters to the Editor MUSCLE & NERVE December 2003 773

CMAP at the axilla (Fig. 1b,c). The orthodromic SNAP ofthe right LACN could be elicited after 5 months (61.1 m/sand 1.3 �V).
In this case of unilateral isolated musculocutaneousnerve palsy, musculocutaneous motor conduction studiesrevealed an almost complete conduction block betweenthe axilla and Erb’s point that improved completely after 5months. Although brachial plexopathy should be consid-ered in the differential diagnosis, the typical clinical signsand the results of conduction studies strongly suggested anisolated musculocutaneous nerve palsy. Additional needleexamination of other muscles around the shoulder andarm would have been helpful in excluding the possibilityof brachial plexopathy.
Musculocutaneous nerve palsy has been reported aftershoulder dislocation,8 fracture of the clavicle,12 or support-ing a heavy object above the head,7 often accompanied byinvolvement of other nerves. Nontraumatic isolated mus-culocutaneous nerve palsy may occur with heavy exerciseinvolving the arm, such as weight lifting,1,2,11 throwingobjects,5,9 rowing a boat,9 using a sledge-hammer,9 orcarrying a heavy load on the shoulder.10 In such cases,entrapment of the nerve where it penetrates the coraco-brachialis muscle was suspected. Postoperative musculocu-taneous nerve palsy has also been reported3,4 when thearm was abducted and externally rotated during an oper-ation, and attributed to compression or stretch of thenerve by the humeral head. In our case, the palsy wasthought to be induced by his sleep position on the eveningbefore the palsy. With the arm fully abducted and thepatient’s head resting on the arm, the musculocutaneousnerve might have been compressed by the humeral heador the patient’s head.
In nerve conduction studies, selective nerve stimula-tion is important for evaluation of conduction block; how-ever, co-activation of other nerves is unavoidable withErb’s point stimulation. Therefore, we used the collisiontechnique6 for eliminating volume-conducted potentials,and were able to show the conduction block between theaxilla and Erb’s point. Appropriate use of the collisiontechnique is important for the precise evaluation of con-duction block, especially with Erb’s point stimulation.
Akira Inaba, MD, PhDTakanori Yokota, MD, PhD
Department of Neurology, Tokyo Medical and Dental University,Tokyo, Japan
1. Bird SJ, Brown MJ. Acute focal neuropathy in male weightlifters. Muscle Nerve 1996;19:897–899.
2. Braddom RL, Wolfe C. Musculocutaneous nerve injury afterheavy exercise. Arch Phys Med Rehabil 1978;59:290–293.
3. Dundore DE, DeLisa JA. Musculocutaneous nerve palsy: anisolated complication of surgery. Arch Phys Med Rehabil1979;60:130–133.
4. Ewing MR. Postoperative paralysis in the upper extremity.Report of five cases. Lancet 1950;1:99–103.
5. Kim SM, Goodrich JA. Isolated proximal musculocutaneousnerve palsy: case report. Arch Phys Med Rehabil 1984;65:735–736.
6. Kimura J. Collision technique: physiologic block of nerveimpulses in studies of motor nerve conduction velocity. Neu-rology 1976;26:680–682.
7. Kuhlman KA, Batley RJ. Bilateral musculocutaneous nervepalsy: a case report. Am J Phys Med Rehabil 1996;75:227–231.
8. Liveson J. Nerve lesions associated with shoulder dislocation;an electrodiagnostic study of 11 cases. J Neurol NeurosurgPsychiatry 1984;47:742–744.
9. Mastaglia FL. Musculocutaneous neuropathy after strenuousphysical activity. Med J Aust 1986;145:153–154.
10. Sander HW, Quinto CM, Elinzano H, Chokroverty S. Carpetcarrier’s palsy: musculocutaneous neuropathy. Neurology1997;48:1731–1732.
11. Swain R. Musculocutaneous nerve entrapment: a case report.Clin J Sport Med 1995;5:196–198.
12. Trojaborg W. Motor and sensory conduction in the musculo-cutaneous nerve. J Neurol Neurosurg Psychiatry 1976;39:890–899.
© 2003 Wiley Periodicals, Inc.
– – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – –
ABSENCE OF MUTATIONS IN THEHYPOXIA RESPONSE ELEMENT OF VEGFIN ALS
Vascular endothelial cell growth factor (VEGF), firstdiscovered as a tumor-secreted protein that promotesvascular permeability, is an important angiogenesis fac-tor.1 VEGF is expressed in many tissues and is rapidlyupregulated during hypoxia, which occurs duringacute or chronic vascular disease, pulmonary disease,or cancer. The precise mechanisms governing this up-regulation remain unknown, but oxygen deprivation isa key regulator of VEGF gene expression with cellsrapidly accumulating hypoxia-inducible transcriptionfactors (HIFs) in response to decreased oxygen ten-sion.2 In the absence of oxygen, HIF-1 binds to a spe-cific consensus sequence (5�-TACGTGGG-3�) calledhypoxia response elements (HRE) in the promoter oftargeted genes, thereby activating the expression ofnumerous hypoxia-response genes such as VEGF.4 Re-cently, Oosthuyse and colleagues described a mousemodel where deletion of the hypoxia-response elementin the VEGF promoter leads to muscle weakness, atro-phy, and death due to degeneration of lower motorneurons.3 Therefore, loss of HRE in the VEGF pro-moter may play a role in the pathogenesis of amyotro-phic lateral sclerosis (ALS). The mechanism underly-ing the phenotype in these mice is not clear; bothchronic neuronal ischemia and loss of a direct trophiceffect of VEGF on motor neurons have been proposed.
We have searched for mutations or potentialfunctional polymorphisms in the promoter region ofthe VEGF gene to determine whether sequence vari-ants may have a direct role in the development ofALS. PCR primer pairs (forward primer, TGCTG-GCGGGTAGGTTTGAATCAT; reverse primer, TG-GCCTGCAGACATCAAAGTGAGC) were designedto amplify a 312-bp fragment surrounding the HREin the VEGF promoter for 96 different DNA samplesfrom non-CuZn superoxide dismutase (SOD1) and
774 Letters to the Editor MUSCLE & NERVE December 2003

non-ALS2 familial ALS (FALS) individuals and 188matched non-ALS controls. Both autosomal domi-nant and recessive cases were included in our 96FALS cohort. PCR reactions were performed in mi-crotiter plates and analyzed for DNA sequence vari-ations using denaturing high-performance liquidchromatography (DHPLC). Representative samplescontaining potential sequence variations were thensequenced on both strands.
Only one sequence variation within the VEGFpromoter was found among the cases. This polymor-phism, present in two different unrelated FALS in-dividuals, was a G insertion 78-bp upstream of HRE.This insertion is unlikely to be associated with ALS asit was also detected in one of the 188 non-ALSnormal control individuals.
The results of Oosthuyse et al.3 suggest a possiblelink between VEGF and ALS, where failure of anappropriate response to hypoxia is predicted to con-tribute to motoneuron degeneration in ALS pa-tients. This report is a starting point to study therelevance of VEGF to the pathogenesis of humanALS. Although our study failed to detect functionalDNA variations in the VEGF promoter of FALS cases,further analysis is needed to better understand thepossible link between VEGF and ALS.
Francois Gros-Louis, MSc1
Sandra Laurent1
Ana Amelia Simoes Lopes, MD1
Jawad Khoris, MD2
Vincent Meininger, MD3
William Camu, MD, PhD2
Guy A. Rouleau, MD, PhD1
1McGill University Health Centre Research Institute and Centre forResearch in Neuroscience, Montreal, Quebec, Canada2UNCD Molecular Unit, INSERM V336, Institute of Biology,Montpellier, France, and Department of Neurology, Hopital Gui deChauliac, Montpellier, France3Service de Neurologie, Division Mazarin, Hopital Pitie-Salpetriere,Paris, France
1. Carmeliet P. Mechanisms of angiogenesis and arteriogenesis.Nat Med 2000;6:389–395.
2. Liu Y, Cox SR, Morita T, Kourembanas S. Hypoxia regulatesvascular endothelial growth factor gene expression in endothe-lial cells. Identification of a 5� enhancer. Circ Res 1995;77:638–643.
3. Oosthuyse B, Moons L, Storkebaum E, Beck H, Nuyens D,Brusselmans K, Van Dorpe J, Hellings P, Gorselink M, Hey-mans S, Theilmeier G, Dewerchin M, Laudenbach V, VermylenP, Raat H, Acker T, Vleminckx V, Van Den Bosch L, CashmanN, Fujisawa H, Drost MR, Sciot R, Bruyninckx F, Hicklin DJ,Ince C, Gressens P, Lupu F, Plate KH, Robberecht W, HerbertJM, Collen D, Carmeliet P. Deletion of the hypoxia-responseelement in the vascular endothelial growth factor promotercauses motor neuron degeneration. Nat Genet 2001;28:131–138.
4. Semenza GL. Expression of hypoxia-inducible factor 1: mech-anisms and consequences. Biochem Pharmacol 2000;59:47–53.
© 2003 Wiley Periodicals, Inc.
Letters to the Editor MUSCLE & NERVE December 2003 775