Embed Size (px)
Citation preview

From the Society for Vascular Surgery
Ischemic complications after endovascularabdominal aortic aneurysm repairThomas S. Maldonado, MD, Caron B. Rockman, MD, Eric Riles, BA, Diah Douglas, MD,Mark A. Adelman, MD, Glenn R. Jacobowitz, MD, Paul J. Gagne, MD, Matthew N. Nalbandian, MD,Neal S. Cayne, MD, Patrick J. Lamparello, MD, Stephanie S. Salzberg, MD, and Thomas S. Riles, MD,New York, NY
Objectives: Limb and pelvic ischemia are known complications after endovascular abdominal aortic aneurysm repair(EVAR). The objective of this paper is to present our experience with the incidence, presentation, and management ofsuch complications.Methods: Over 9 years 311 patients with aortic aneurysms underwent EVAR. A retrospective review identified 28 patients(9.0%) with ischemic complications.Results: Among 28 patients with ischemic complications, 21 had lower extremity ischemia and 7 had pelvic ischemia:colon (n � 4), buttock (n � 2), and spinal cord (n � 2). Of the 21 patients with lower extremity ischemia, 15 had limbocclusions (71.4%), 3 due to embolization (14.7%) and 3 the result of common femoral artery thromboses (14.7%). Limbocclusions were manifested as severe acute arterial ischemia (n � 6), rest pain (n � 3), intermittent claudication (n � 5),and decreased femoral pulse (n � 1). Limb occlusions were managed with thrombectomy and stent placement (n � 4),femorofemoral bypass (n � 7), eventual explantation because of persistent endoleak (n � 1), and expectant management(n � 3). The 3 patients with occlusions managed expectantly all had intermittent claudication, which has subsequentlyimproved. In the 6 patients with lower extremity ischemia due to embolization or common femoral artery injurypresentation was acute, and embolectomy was performed, followed by femoral artery endarterectomy and patchangioplasty or placement of an interposition graft. One patient who had a prolonged postoperative course includingcardiac arrest subsequently required distal bypass and ultimately above- knee amputation. Among the 7 patients withpelvic ischemia, 2 patients had unilateral hypogastric artery embolization before the original surgery. Among the patientswith colonic ischemia, 3 were seen immediately postoperatively, and required colectomy and colostomy. Two patientswho required urgent colectomy subsequently had multiple organ failure, and died in the perioperative period. Onepatient had abdominal pain 1 week after surgery, which was managed with bowel rest, with subsequent improvement. In2 patients spinal cord ischemia developed immediately after surgery, w hich resulted in persistent paraplegia. Buttockischemia developed in 2 patients, 1 of whom required fasciotomy because of gluteal compartment syndrome, and hadtransient renal failure.Conclusions: Ischemic complications are not uncommon after EVAR, and may exceed the incidence with open surgical repair.Limb ischemia is most often a result of limb occlusion, and can be successfully managed with standard interventions. Pelvicischemia often results from atheroembolization despite preservation of hypogastric arterial circulation. Colonic and spinalischemia are associated with the highest morbidity and mortality. ( J Vasc Surg 2004;40:703-10.)
Pelvic ischemic complications after open infrarenal aor-tic reconstruction occur in 1% to 2% of patients, with anassociated mortality rate greater than 40%.1-3 Likewise,lower extremity ischemia after aortic reconstructions, oftenreferred to as “trash foot” is a well-recognized result ofatheroemboli, and occurs in 1% to 5% of patients.4-7
The advent of endovascular abdominal aortic aneurysmrepair (EVAR) has led to a decrease in postoperative mor-bidity, shorter hospital stay, and quicker recovery time.Nevertheless, EVAR continues to be burdened with thesame ischemic complications seen with open aortic surgery.
From the Division of Vascular Surgery, Department of Surgery, New YorkUniversity School of Medicine.
Competition of interest: none.Presented at the Fifty-seventh Annual Meeting of the Society for Vascular
Surgery, Anaheim, Calif, Jun 3, 2004.Reprint requests: Thomas S. Maldonado, MD, NYU Medical Center, 530
First Ave, Ste 6F, New York, NY 10016 (e-mail: [email protected]).
0741-5214/$30.00Copyright © 2004 by The Society for Vascular Surgery.doi:10.1016/j.jvs.2004.07.032
Indeed, ischemic complications after EVAR occur in 3% to10% of patients.8-17 Mechanisms purported to contributeto pelvic ischemia include interruption of hypogastric arte-rial circulation and atheroembolization, whereas lower ex-tremity ischemia after EVAR appears to be more commonlyassociated with limb occlusion.9,12,13 The purpose of thisstudy was to examine the incidence, management, andoutcome of pelvic and lower extremity ischemia afterEVAR.
METHODS
A retrospective review was performed of a prospectivelycompiled database of all EVAR procedures performed atNew York University Medical Center. From 1994 through2003, 311 EVAR procedures were attempted. The first 46procedures (14.8%) were performed during approved clin-ical trials, including the Endovascular Technologies trialand the Excluder trial (W. L. Gore & Associates). Theremaining 265 procedures (85.2%) were performed afterapproval of the devices by the US Food and Drug Admin-
703

y.
JOURNAL OF VASCULAR SURGERYOctober 2004704 Maldonado et al
istration (FDA) in 1999. Devices used after FDA approvalincluded the Ancure (Guidant), AneuRx (Medtronic), Ex-cluder (W. L. Gore & Associates), and Zenith (Cook)grafts. In all cases endovascular grafts were deployed belowthe renal arteries, with suprarenal or infrarenal fixation,depending on the device, and distally in either the commoniliac artery or external iliac artery, depending on the extentof aneurysmal disease. In cases in which hypogastric arterieswere coiled, embolization was routinely staged to precedeEVAR by 1 or 2 days. Two patients underwent bilateralhypogastric coil embolization, with an interval of 2 to 3weeks between embolizations. Coils were placed in theinternal iliac artery through either the ipsilateral or con-tralateral approach with a variety of catheters. Care wastaken to not place coils past the proximal internal iliac arteryso as to preserve pelvic collateral circulation. EVAR wasperformed only in patients with asymptomatic disease, withthe exception of 1 patient in whom embolism was known tobe occurring preoperatively.
Significant pelvic ischemia was defined as buttocknecrosis, as well as colonic or spinal ischemia. Buttockclaudication was not considered. Lower extremity isch-emia was stratified as limb occlusion, common femoralartery injury, or atheroembolism. There were no bilaterallimb occlusions. In 311 EVAR procedures, 28 patientshad pelvic or lower extremity ischemic complications.This group formed the focus of our study. The follow-upperiod ranged from 2 to 72 months (mean, 22.5months). Twenty-four of 311 patients (7.7%) were lostto follow-up. An office visit, including history and phys-ical examination, and computed tomography was madeat 1, 6, and 12 months, and yearly thereafter.
Statistical analysis was performed with the SPSS statis-tical software package. Proportional data were analyzedwith the �2 test, the Fisher exact test was used where
Table I. Lower extremity ischemic complications
Limb occlusion
Leg ischemia 15Onset
Early (�30 days postoperative) 9Late (�30 days postoperative) 6
PresentationLoss of pulse 1Claudication 5Rest pain 4Cool “threatened” limb 5
TreatmentStent/PTA 4Femorofemoral bypass 7Femoral endarterectomy 0Thrombectomy 0Interposition graft 0Expectant management 3Explantation 1
OutcomeAmputation 0Limb salvage 15
CFA, Common femoral artery; PTA, percutaneous transluminal angioplast
appropriate, continuous variables were analyzed with the2-tailed Student t test. P � .05 was considered statisticallysignificant.
RESULTS
Endovascular repair was attempted in 311 patients, 44women (14.1%) and 267 men (85.9%), with a mean age of72.2 years (range, 58-93 years). In 6 patients (all withEVT/Ancure) conversion to open repair was required be-cause of device malfunction or difficulty during deploy-ment (98.1% success rate). Mean aortic aneurysm diameterwas 5.8 cm (range, 4.7-8 cm). Ancure grafts were placed in238 patients (76.5%), Excluder grafts in 30 patients (9.6%),AneuRx grafts in 28 patients (9.0%), and Zenith grafts in 15patients (4.8%). Fourteen endografts (4.5%) were tubeconfigured, and 297 (96.1%) were bifurcated devices.Among 28 patients with ischemic complications, 21 hadlower extremity ischemia and 7 had pelvic ischemia: colon(n � 4), buttock (n � 2), and spinal cord (n � 2). Four of28 ischemic complications occurred in women (14.3%).Nine of 28 patients (32.1%) had aneurysmal common iliacarteries. Ischemic complications occurred in patients withthe following endografts: Zenith (n � 1, 3.6%)), Excluder(n � 1, 3.6%), AneuRx (n � 2, 7.1%), and Ancure (n � 24,85.7%). The only perioperative deaths occurred in 2 of 7patients with pelvic ischemia (28.6%; P � .0001). Nopatients with limb ischemia died as a result of a complica-tion.
Lower extremity ischemic complications. A sum-mary of lower extremity ischemic complications is pre-sented in Table I. Of 21 patients with lower extremityischemia, this complication was the result of limb occlusionin 15 patients (71%), atheroembolization in 3 patients(14.7%), and common femoral artery thrombosis in 3 pa-tients (14.7%).
CFA injury Embolus Total
3 3 21
3 3 150 0 6
2 1 40 0 50 0 31 2 8
0 0 40 0 72 0 23 3 31 0 10 0 30 0 1
1* 0 12 3 20

JOURNAL OF VASCULAR SURGERYVolume 40, Number 4 Maldonado et al 705
Limb occlusions manifested with pain and parasthesia(n � 5), rest pain alone (n � 4), intermittent claudication(n � 5), and decreased femoral pulse as the sole finding(n � 1). No patient had motor deficits. Limb occlusionswere managed according to surgeon preference, as follows:4 patients underwent thrombectomy and stent placement,7 patients underwent femorofemoral bypass, 1 graft waseventually explanted because of persistent type I endoleak,and 3 patients were managed expectantly. The 3 patientsmanaged expectantly all had intermittent claudication,which has subsequently improved. In 14 of 15 patients withlimb occlusions unsupported endografts (Ancure) wereimplanted. Five limb occlusions in patients with Ancuredevices in place had been stented a priori, because of kinkedor stenosed limbs noted at the initial EVAR. One patientwith a supported endograft (AneuRx) had limb occlusion at6 months post-EVAR. In 4 of 15 occluded limbs (26.7%)devices were deployed in the external iliac artery (P �.206). Average limb diameter of the 15 occluded limbs was13.2 mm.
In all 3 patients with atheroembolization resulting inlower extremity ischemia the diagnosis was made early aftersurgery and was treated with embolectomy. One patienthad an absent pedal pulse 6 hours postoperatively. Twopatients’ limbs were noted to be markedly ischemic atsurgery, and a diagnosis was made of emboli to the super-ficial femoral artery and tibioperoneal trunk. In 1 patientthe underlying superficial femoral artery lesion was treatedwith a stent after embolectomy.
Three patients had lower extremity ischemia, diagnosed inthe immediate postoperative period, as a result of commonfemoral artery injury and thrombosis. One required a bypassinterposition graft, because of severe dissection in the com-mon femoral artery. Two patients underwent common fem-oral endarterectomy and patch angioplasty. One of thesepatients had cardiac arrest on the first postoperative day, atwhich time both lower extremities were thrombosed. Afterunsuccessful thrombectomy a distal bypass was performed,which subsequently also became thrombosed. This patientwas presumed to have an underlying hypercoagulable condi-
Table II. Pelvic ischemia after endovascular abdominal ao
Colon
Pelvic ischemia 4Presentation
Acute (�30 days postoperative) 4Late (�30 days postoperative) 0
ManagementColon resection 3Colostomy 3Fasciotomy 0Expectant 1
OutcomeDeath 2Paralysis 0Recovery 2
*One patient with spinal ischemia had concomitant buttock ischemia.
tion, and subsequently required above-knee amputation ofthe limb.
Pelvic ischemic complications. A summary of pelvicischemic complications is presented in Table II. The singlepatient to undergo EVAR for treatment of an embolizinganeurysm had extensive atheroembolic ischemia to thecolon and soft tissues, which required colectomy, andmassive debridement and reconstruction of the anteriorabdominal wall.
Anatomic characteristics of patients in whom pelvicischemia developed after EVAR are presented in Table III.Among the 7 patients with pelvic ischemia, 2 had unilateralhypogastric artery embolization before the original surgery(colon ischemia, n � 1; buttock ischemia, n � 1). Fourpatients had a patent inferior mesenteric artery beforeEVAR; colon ischemia developed in all 4 patients. Threepatients had small distal necks, and 2 patients had thrombusin the proximal neck.
Among 4 patients with colonic ischemia, 3 presentedimmediately postoperatively, and required colectomy andcolostomy. In 2 patients who required urgent colectomymultiple organ system failure developed, and they died inthe perioperative period. Another patient had abdominalpain 1 week after surgery. Ischemic colitis was confirmed atcolonoscopy, was managed with bowel rest, and improved.
Hypogastric artery embolization was performed in 1patient with colon ischemia. EVAR in this patient wascomplicated by a detached limb, which necessitated con-version to an aortouniiliac device and coiling of the rightcommon and internal iliac arteries in addition to a fem-oral-femoral bypass. The left internal iliac artery waspatent and perfused retrograde after femorofemoral by-pass. In addition to colonic necrosis requiring urgentcolectomy, Fournier gangrene developed in this patient,which could also be attributed to atheroemboli. Subse-quently multiple organ system failure developed, and thepatient died in-hospital.
In 2 patients spinal cord ischemia developed immedi-ately after surgery, resulting in persistent paraparesis inboth patients.15 One of these patients underwent conver-
neurysm repair
Spinal Buttock Total
2* 2 7
2 2 70 0
0 0 30 0 30 1 12 1 3
1 0 31 1 20 1 3
rtic a

enteric
JOURNAL OF VASCULAR SURGERYOctober 2004706 Maldonado et al
sion to open repair when the Ancure graft failed to com-pletely unsheath. Postoperatively this patient had transientelevation in creatine phosphokinase (CPK) concentration,and patchy areas of left buttock skin necrosis, which re-solved. The other patient underwent successful EVAR, butsevere paraparesis and bladder dysfunction developed. Bothpatients underwent magnetic resonance imaging imagingof the spine, which confirmed atheroembolization to theconus medullaris.
In an additional patient severe global buttock ischemiadeveloped, and required fasciotomy to treat gluteal com-partment syndrome. This patient was morbidly obese(weight, 350 lb) and had transient renal failure as a result ofbuttock ischemia. The anatomy was suboptimal in thatthere was a short angulated neck; however, other comorbidconditions precluded open repair. EVAR required preop-erative hypogastric artery embolization and limb deploy-ment in the external iliac artery, because of a 40-mmcommon iliac artery aneurysm. Pathologic analysis failed toshow evidence of thrombosis or embolization to the glu-teus muscle, making the ischemic complication more likelya result of interruption of the internal iliac artery.17
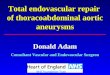
Effect of internal iliac artery embolization on isch-emic complications (Fig). One or both hypogastric arter-ies were either coiled (n � 41) or inadvertently covered(n � 2) in 43 patients undergoing EVAR (13.8%). In 2patients bilateral hypogastric arteries were coiled beforeEVAR; pelvic ischemia did not develop in either patient.Ischemic complications developed in 16.3% of patientswith any sacrificed hypogastric artery, compared with 8.0%of patients in whom both hypogastric arteries were pre-served (P � .091). Pelvic ischemia occurred in 4.7% ofpatients with hypogastric embolization, compared with1.9% of those without hypogastric embolization (P � .26).In 42 of the 43 patients in whom a hypogastric artery wasoccluded limbs were deployed in the external iliac artery.Limb ischemia occurred in 11.6% of patients with hypogas-tric coil embolization, compared with 6.1% of patientswithout embolization (P � .19).
DISCUSSION
As endovascular aortic aneurysm repair has gained ac-ceptance by the medical community and the public alike,
Table III. Anatomic characteristics of patients with pelvic
PatientIschemic
complicationPreviouscolectomy
Iliacaneurysm
Ithro
1 Spine, buttock No No Y2 Spine No Yes Y3 Colon, abdominal
wallNo No N
4 Colon, Fourniergangrene
No No N
5 Colon Yes No N6 Colon No No Y7 Buttock No Yes Y
EVAR, Endovascular abdominal aortic aneurysm repair; IMA, inferior mes
most AAAs are now treated with this minimally invasiveprocedure. The resultant decreased postoperative cardio-pulmonary morbidity and hospital cost is of clear benefit.However, this is tempered by the ischemic complicationsthat persist in a subset of patients.
Our finding of 2.25% pelvic ischemic complications isconsistent with similar reports in the literature,13,18 andappears to equal that described for open repair, approxi-mately 1% to 2%.1-3 Dadian et al13 reported a 2.9% inci-dence of colon ischemia in 8 of 278 patients after EVAR.Half of these patients (n � 4) required colectomy, andsubsequently 3 of these patients died. In our series, 7 of 28ischemic complications resulted in pelvic ischemia. Three of4 patients who had colonic ischemia required urgent colec-tomy, and 2 died. The diagnosis of colon ischemia in ourstudy was based entirely on clinical presentation. Thus,while our results confirm that clinically apparent colonicischemia after EVAR or open repair is often lethal, we mayhave underestimated its true incidence. Ernst et al19 pro-spectively evaluated all patients after open aortic recon-structions with routine colonoscopy, and found that theincidence of ischemia increases to 6% from the well-established incidence of 1% to 2%. The spectrum of isch-emia in the colon when evaluated at endoscopy ranges frommild edema to pseudomembranes. In our study the 1patient with colon ischemia seen 10 days post-EVAR withabdominal pain was fortunate to have only patchy ery-thema, which was successfully managed with bowel restalone.
All but one of the EVAR procedures in our study wasperformed in patients with asymptomatic disease. One pa-tient who had “trash feet” and elevated creatinine concen-tration as a result of atheroemboli from an AAA underwentEVAR. Widespread atheroembolism to the pelvis and ab-dominal wall subsequently developed, and the patient diedpostoperatively. Treatment of embolizing abdominal aneu-rysms with endovascular stents is often considered exceed-ingly high risk, because of the well-founded concern thatthe unstable plaque or thrombus will dislodge as a result ofcatheter and wire manipulations before deployment. This islikely the mechanism that resulted in such widespreadatheroemboli and pelvic ischemia in our patient. Neverthe-less, Shames et al20 have reported promising results in their
emia after EVAR
Neckthrombus
Sacthrombus
Hypogastricembolus
IMApatent Death
No Yes No No NoYes Yes No No NoNo Yes No Yes Yes
Yes Yes Yes Yes Yes
No Yes No Yes NoNo Yes No Yes NoNo Yes Yes Yes No
artery.
isch
liacmbus
eseso
o
oeses

JOURNAL OF VASCULAR SURGERYVolume 40, Number 4 Maldonado et al 707
treatment of embolizing arterial lesions with stent grafts.None of the 8 patients treated with covered stents in theirseries had atheroembolic complications as a result of theprocedure. Likewise, Dougherty et al21 successfully im-planted covered stents in 2 patients with embolizing ather-oma in the infrarenal aorta without causing further embo-lization.
The 2 patients in our study with spinal ischemia afterEVAR have been previously presented as case reports, andhad permanent paraplegia as a result of atheroemboli to theconus medullaris diagnosed at magnetic resonance imag-ing.15 They accounted for 2 of 28 patients (7.1%) withischemic complications, for an overall incidence of 0.64%.Others have reported a similarly low incidence of spinalischemia after EVAR.11,18 A review of the European Col-laborators on Stent Graft Techniques for Abdominal AorticAneurysm Repair (EUROSTAR) registry identified 6 of2862 patients (0.21%) with spinal cord ischemia.11 Therewas a significant correlation between coil embolization ofthe hypogastric or lumbar arteries (P � .029) and spinalcord ischemia in that study.
This significance of hypogastric artery occlusion fordevelopment of pelvic ischemia has been a subject of somecontroversy. The most common sequela after interruptionof hypogastric arteries as an adjunct to EVAR appears to bedevelopment of buttock claudication. The incidence ofbuttock claudication ranges from 11% to 50% after coilembolization of one or both internal iliac arteries.15,18,22-25
Colonic ischemia, however, appears to be much less com-mon after interruption of the hypogastric circulation.Mehta et al23 reviewed a series of 154 patients in whomhypogastric arteries were interrupted as part of either open(n � 47) or endovascular (n � 107) repair, and found nopatients with ischemic colitis that required laparotomy orbuttock necrosis. Those authors staged embolization andEVAR in some, but not all, patients, and conclude thathypogastric embolization as part of EVAR can be donesafely without significant risk for severe pelvic ischemia.
Internal iliac artery interruption and ischemic complications afterendovascular abdominal aortic aneurysm repair. Note: 16.3% of allpatients treated with coil embolization had an ischemic event,compared with 8.0% of patients who underwent internal iliac arteryembolization (P � .091).
In our study we staged coil embolization and EVAR by1 or 2 days. There is no consensus regarding the appropri-ate staging interval between embolization of a single hypo-gastric artery and EVAR. Indeed, some authors have pro-posed that simply covering the hypogastric artery duringEVAR does not increase the risk for endoleak or ischemiaand averts the need for a preoperative embolization proce-dure.26 Nevertheless, most authors agree that when bilat-eral hypogastric artery embolization is planned, EVARshould be delayed by 2 to 4 weeks.13,18,23
Interruption of bilateral internal iliac arteries has alsobeen reported to be free from colon ischemia. Englke etal27 reviewed 16 patients with bilateral embolization beforeEVAR, and found buttock claudication and sexual dysfunc-tion to be the only adverse events. Others are more wary ofinterrupting important pelvic collateral vessels in the settingof EVAR.14,18,22,28-30 Leyden et al18 report 1 of 21 pa-tients (4.3%) with colonic ischemia after hypogastric arteryembolization. Likewise, Karp et al31 reviewed 24 patientswith either coiled or unintentional covering of a hypogas-tric artery during EVAR, and found 3 patients (12%) inwhom colon ischemia developed, requiring resection in 1patient. Our study found 2 of 43 patients (4.3%) withhypogastric arteries either covered or coiled in whom pelvicischemia developed. This was in contrast to 5 of 268patients (1.9%) with intact iliac arteries (P � .26). Theseresults suggest that coil embolization of hypogastric arter-ies before EVAR does not predispose to pelvic ischemia.Rather, the cause of pelvic ischemia would appear to bemore consistent with atheroemboli. All 7 patients withpelvic ischemia had copious thrombus in the aneurysm sac.All but 2 patients had thrombus in the neck or accessvessels, and in 1 of the 2 embolization was occurringpreoperatively. In 3 of 7 patients with pelvic ischemia in ourstudy widespread pelvic ischemia developed, to the colonand abdominal wall, the colon and perineum, and the spineand buttock, respectively. Dadian et al13 documented athe-roemboli in pathologic specimens from 4 of 8 patients withcolon ischemia after EVAR. They also report that wide-spread atheroemboli is associated with a poorer prognosisthan isolated colon ischemia.13 Indeed, in our series ofpatients with pelvic ischemia the 2 patients who died hadwidespread atheroembolism after EVAR.
Other predisposing factors to pelvic ischemia mightinclude inadequate mesenteric collateral vessels, either as aresult of intrinsic disease or iatrogenic (ie, after colectomy).We did not assess the status of the inferior mesenteric arteryin most patients, nor were we able to evaluate the arch ofRiolan or marginal artery collateral vessels, but found that 5of 7 patients with pelvic ischemia had patent inferior mes-enteric arteries before EVAR. Likewise, in only 1 patientwith previous colectomy did mild self-limited colonic isch-emia develop.
Lower extremity ischemia after EVAR is most fre-quently a result of limb occlusion, although atheroemboli-zation has also been reported. A case series of early vascularcomplications after EVAR by Aljabri et al 9 demonstrated a9.6% incidence of lower extremity ischemia (4 limb occlu-

JOURNAL OF VASCULAR SURGERYOctober 2004708 Maldonado et al
sions, 1 embolization). A review of the literature by thesame authors found a mean incidence of lower extremityischemia of 5.1% (range, 0.6%-9.9%) at short-term follow-up.9 The EUROSTAR prospective registry identified 18%of patients requiring secondary intervention for treatmentof limb occlusions at more than 12 months after EVAR.32
In our study we identified 21 patients (6.75%) withlower extremity ischemia after EVAR: 15 limb occlusions(4.5%), 3 embolizations (0.9%), and 3 common femoralinjuries (0.9%). Complex aortoiliac anatomy, including tor-tuous, narrow, and calcified access vessels, as well as narrowdistal necks, have all been proposed as harbingers of limbocclusion. Carroccio et al12 examined anatomic and device-related causes of limb occlusion in a series of 351 patients(702 graft limbs at risk). Thrombosis occurred in 26 of the702 limbs at risk (3.7%), and was associated with smallerlimb diameter (�14 mm; P � .3) and extension into theexternal iliac artery (P � .01). These authors did not find asignificant association between limb thrombosis and devicetype. This may be explained by the relatively low number ofAncure devices (n � 8) in their series. Others have shownthat limb occlusion is indeed device-related. Ouriel et al33
examined device-specific complications after EVAR, andfound that limb occlusions occurred most often with theunsupported Ancure device (11.6% � 4.6% at 12 months;P � .009). Another review by Parent et al16 of 67 patientswith Ancure devices in place demonstrated a 13.4% rate oflimb occlusion or stenosis. Subgroup analysis in that studydemonstrated that when limbs were primarily stented atEVAR they were free from subsequent limb dysfunction. Inour series the Ancure device was used most often (n � 238,76.5%). 14 of 15 patients with limb occlusions had Ancureunsupported endografts in place. Our seemingly lowerincidence of limb thrombosis (4.5%), compared with theexperience of Ouriel et al33 and Parent et al,16 may beattributed to the fact that surgeons at our institution havea low threshold for preemptively stenting iliac limbs atEVAR. Nonetheless, 5 of the limb occlusions in patientswith Ancure devices in place had been stented a priori,because of kinked or stenosed limbs noted at the initialEVAR. Nevertheless, the more cumbersome and bulkierdesign of the Ancure endograft may contribute to higherrisk for atheroembolization. In particular, the extra manip-ulations required for contralateral limb deployment maypredispose this device to higher ischemic complications.The disproportionate number of Ancure devices in ourstudy prevent us from drawing any device-specific conclu-sions. Of note, in 2 of 7 patients with pelvic ischemiadevices other than Ancure were implanted (Gore, 1;AneuRx, 1). Thus atheroembolization is clearly a risk asso-ciated with any EVAR procedure, and will likely persistdespite diminishing profiles and less fastidious deploymenttechniques.
Most patients with limb occlusions (80.0%) in our studyrequired intervention to reestablish flow to the ischemic ex-tremity. Management of limb occlusions consisted of throm-bectomy and stent placement in 4 patients. This was doneunder fluoroscopic guidance, because of fear of dislodging the
endograft, and always identified an underlying kink or steno-sis. Seven patients underwent femorofemoral bypass, and 3patients were managed expectantly. Carroccio et al12 reportedsimilar management of limb occlusion in their series, althoughthey used thrombolysis rather than thrombectomy. Eighteenof 26 patients (69.2%) in that study required interventions,and the remaining 8 patients (31.8%) were managed expect-antly.
Thromboembolism to the lower extremity during EVARmay be more common than previously appreciated, albeitsubclinical. Using an ultrasound-based method to detectlower extremity embolization, Thompson et al34 detectedsignificantly greater microemboli in endovascular comparedwith conventional open repair of AAA. In addition, in 3 of 20patients (15%) who underwent EVAR and had high particu-late counts at ultrasound scanning transient petechiae to thefeet developed. The incidence of clinically apparent macroem-boli to the lower extremities is approximately 2%.35 Our studyidentified 3 patients (0.09%) with atheroemboli that causedlower extremity ischemia. These were all successfully treated,with thrombectomy and stent placement in 1 patient fortreatment of an underlying superficial femoral artery stenosis.
In summary, ischemic complications after EVAR oc-curred in 9% of patients in our series. Pelvic ischemia oftenresults from atheroembolization, despite preservation ofhypogastric arterial circulation. The overall ischemic com-plications after interruption of hypogastric arteries beforeEVAR was 16.3%, compared with 8% in intact hypogastricarteries (P � .091). This approaches statistical significance,and is likely due to limb deployment in the external iliacartery in those patients with coiled hypogastric arteries.Colonic and spinal ischemia are associated with the highestmorbidity and mortality. Limb ischemia is most often aresult of limb occlusion, and can be successfully managedwith standard interventions.
REFERENCES
1. Brewster DC, Franklin DP, Cambria RP, Darling RC, Moncure AC,LaMuraglia GM, et al. Intestinal ischemia complicating abdominalaortic surgery. Surgery 1991;109:447-54.
2. Diehl JT, Cali RF, Hertzer NR, Beven EG. Complications of abdominalaortic reconstruction. An analysis of perioperative risk factors in 557patients. Ann Surg 1983;197:49-56.
3. Jarvinen O, Laurikka J, Salenius JP, Lepantalo M. Mesenteric infarctionafter aortoiliac surgery on the basis of 1752 operations from the Na-tional Vascular Registry. World J Surg 1999;23:243-7.
4. Noirhomme P, Buche M, Louagie Y, Verhelst R, Matta A, SchoevaerdtsJC. Ischemic complications of abdominal aortic surgery. J CardiovascSurg (Torino) 1991;32:451-5.
5. Imparato AM. Abdominal aortic surgery: prevention of lower limbischemia. Surgery 1983;93(1 Pt 1):112-6.
6. Strom JA, Bernhard VM, Towne JB. Acute limb ischemia followingaortic reconstruction. A preventable cause of increased mortality. ArchSurg 1984;119:470-3.
7. Sayers RD, Thompson MM, Nasim A, Healey P, Taub N, Bell PR.Surgical management of 671 abdominal aortic aneurysms: a 13 yearreview from a single centre. Eur J Vasc Endovasc Surg 1997;13:322-7.
8. Alric P, Hinchliffe RJ, MacSweeney ST, Wenham PW, Whitaker SC,Hopkinson BR. The Zenith aortic stent-graft: a 5-year single-centerexperience. J Endovasc Ther 2002;9:719-28.

JOURNAL OF VASCULAR SURGERYVolume 40, Number 4 Maldonado et al 709
9. Aljabri B, Obrand DI, Montreuil B, MacKenzie KS, Steinmetz OK.Early vascular complications after endovascular repair of aortoiliac an-eurysms. Ann Vasc Surg 2001;15:608-14.
10. Becquemin JP, Kelley L, Zubilewicz T, Desgranges P, Lopeyre M,Kobeiter H. Outcomes of secondary interventions after abdominalaortic aneurysm endovascular repair. J Vasc Surg 2004;39:298-305.
11. Berg P, Kaufmann D, van Marrewijk CJ, Buth J. Spinal cord ischaemiaafter stent-graft treatment for infra-renal abdominal aortic aneurysms.Analysis of the EUROSTAR database. Eur J Vasc Endovasc Surg2001;22:342-7.
12. Carroccio A, Faries PL, Morrissey NJ, Teodorescu V, Burks JA, Grav-ereaux EC, et al. Predicting iliac limb occlusions after bifurcated aorticstent grafting: anatomic and device-related causes. J Vasc Surg 2002;36:679-84.
13. Dadian N, Ohki T, Veith FJ, Edelman M, Mehta M, Lipsitz EC, et al.Overt colon ischemia after endovascular aneurysm repair: the impor-tance of microembolization as an etiology. J Vasc Surg 2001;34:986-96.
14. Lin PH, Bush RL, Chaikof EL, Chen C, Conklin B, Terramani TT, etal. A prospective evaluation of hypogastric artery embolization in endo-vascular aortoiliac aneurysm repair. J Vasc Surg 2002;36:500-6.
15. Rockman CB, Riles TS, Landis R. Lower extremity paraparesis orparaplegia subsequent to endovascular management of abdominal aor-tic aneurysms. J Vasc Surg 2001;33:178-80.
16. Parent FN III, Godziachvili V, Meier GH III, Parker FM, Carter K,Gayle RG, et al. Endograft limb occlusion and stenosis after Ancureendovascular abdominal aneurysm repair. J Vasc Surg 2002;35:686-90.
17. Su WT, Stone DH, Lamparello PJ, Rockman CB. Gluteal compartmentsyndrome following elective unilateral internal iliac artery embolizationbefore endovascular abdominal aortic aneurysm repair. J Vasc Surg2004;39:672-5.
18. Lyden SP, Sternbach Y, Waldman DL, Green RM. Clinical implicationsof internal iliac artery embolization in endovascular repair of aortoiliacaneurysms. Ann Vasc Surg 2001;15:539-43.
19. Ernst CB, Hagihara PF, Daughtery ME, Sachatello CR, Griffen WO Jr.Ischemic colitis incidence following abdominal aortic reconstruction: aprospective study. Surgery 1976;80:417-21.
20. Shames ML, Rubin BG, Sanchez LA, Thompson RW, Sicard GA.Treatment of embolizing arterial lesions with endoluminally placedstent grafts. Ann Vasc Surg 2002;16:608-12.
21. Dougherty MJ, Calligaro KD. Endovascular treatment of embolizationof aortic plaque with covered stents. J Vasc Surg 2002;36:727-31.
22. Kritpracha B, Pigott JP, Price CI, Russell TE, Corbey MJ, Beebe HG.Distal internal iliac artery embolization: a procedure to avoid. J VascSurg 2003;37:943-8.
23. Mehta M, Veith FJ, Ohki T, Cynamon J, Goldstein K, Suggs WD, et al.Unilateral and bilateral hypogastric artery interruption during aortoiliacaneurysm repair in 154 patients: a relatively innocuous procedure. JVasc Surg 2001;33(2 Suppl):S27-32.
24. Welborn MB III, Seeger JM. Prevention and management of sigmoidand pelvic ischemia associated with aortic surgery. Semin Vasc Surg2001;14:255-65.
25. Cynamon J, Lerer D, Veith FJ, Taragin BH, Wahl SI, Lautin JL, et al.Hypogastric artery coil embolization prior to endoluminal repair ofaneurysms and fistulas: buttock claudication, a recognized but possiblypreventable complication. J Vasc Interv Radiol 2000;11:573-7.
26. Tefera G, Turnipseed W, Carr S, Pulfer K, Hoch J, Acher C. Is coilembolization of hypogastric artery necessary during endovascular treat-ment of aortoiliac aneurysms? Ann Vasc Surg 2004;18:143-6.
27. Engelke C, Elford J, Morgan RA, Belli AM. Internal iliac artery embo-lization with bilateral occlusion before endovascular aortoiliac aneu-rysm repair: clinical outcome of simultaneous and sequential interven-tion. J Vasc Interv Radiol 2002;13:667-76.
28. Lin PH, Bush RL, Lumsden AB. Sloughing of the scrotal skin andimpotence subsequent to bilateral hypogastric artery embolization forendovascular aortoiliac aneurysm repair. J Vasc Surg 2001;34:748-50.
29. Marty B, Perruchoud C, Wicky S, Guillou L, Von Segesser LK. Athe-roembolization: a harmful complication of therapeutic internal iliacartery occlusion. J Vasc Surg 2002;36:1062-5.
30. Kalliafas S, Albertini JN, Macierewicz J, Yusuf SW, Whitaker SC,Macsweeney ST, et al. Incidence and treatment of intraoperative tech-nical problems during endovascular repair of complex abdominal aorticaneurysms. J Vasc Surg 2000;31:1185-92.
31. Karch LA, Hodgson KJ, Mattos MA, Bohannon WT, Ramsey DE,McLafferty RB, et al. Adverse consequences of internal iliac arteryocclusion during endovascular repair of abdominal aortic aneurysms. JVasc Surg 2000;32:676-83.
32. Laheij RJ, Buth J, Harris PL, Moll FL, Stelter WJ, Verhoeven EL. Need forsecondary interventions after endovascular repair of abdominal aortic an-eurysms: intermediate-term follow-up results of a European collaborativeregistry (EUROSTAR). Br J Surg 2000;87:1666-73.
33. Ouriel K, Clair DG, Greenberg RK, Lyden SP, O’Hara PJ, Sarac TP, etal. Endovascular repair of abdominal aortic aneurysms: device-specificoutcome. J Vasc Surg 2003;37:991-8.
34. Thompson MM, Smith JL, Bell PR. Thromboembolic complicationsduring endovascular aneurysm repair. Semin Vasc Surg 1999;12:215-9.
35. Woodburn KR, May J, White GH. Endoluminal abdominal aorticaneurysm surgery. Br J Surg 1998;85:435-43.
Submitted May 27, 2004; accepted Jul 20, 2004.
DISCUSSION
Dr Michael L. Marin (New York, NY). Embolization andhypoperfusion have always plagued conventional vascular surgery,and it’s not surprising that any newcomer to this field will suffersimilar consequences. Ischemic complications after EVAR havebeen recognized and described since Parodi first told us about thisprocedure in 1990.
Dr. Maldonado and colleagues report today their findings in28 patients in whom postoperative ischemia developed after EVARfrom a 9-year experience treating 311 patients. I’d like to ask theauthors several questions to enhance our understanding of thiscomplex problem.
Ischemic complications following all vascular surgery proce-dures, EVAR not excluded, surely are not limited to the colon,spine, pelvis, and lower extremities; rather, renal artery occlusionsand embolizations, and proximal embolization from aneurysmalthrombus into the suprarenal components of the aorta resulting inarm ischemia, stroke, and even MI have been reported. Could theauthors tell us a little about these other ischemic events that mayhave occurred in their 311 patients so we’d have a broader pictureof the problem of ischemia after EVAR.
Several years ago Dr Timothy Chuter alerted us to the problem ofcomplex aortic aneurysm thrombus and the possibility of increasedrisk for embolization from EVAR. Specifically, he described multiplechannels in the aneurysm clot that may be predisposed to emboliza-tion with the passage of endoluminal devices. Did the authors en-counter this sort of pathologic finding in any of their patients witheither mild or massive forms of ischemia?
In our experience with EVAR at Mount Sinai, which nowincludes over a thousand patients, common femoral arterydisease is common, and perhaps more common than is oftendescribed. In fact, at the end of most procedures reconstructionof the common femoral artery by one means or another is goingto invariably be required. Did the authors use the highly fash-ionable percutaneous EVAR technique in any of their patients,which would preclude the ability to recognize the types of vesselinjury commonly seen after EVAR and thereby prevent theischemic sequelae?
Your description of severe and devastating colon and spinalcord ischemia in association with gluteal gangrene is a sadly familiarcomplication, which anybody who has been involved in this field

JOURNAL OF VASCULAR SURGERYOctober 2004710 Maldonado et al
for a number of years has seen. We have not seen this problem sincethe early portions of our experience, and we’ve attributed this togreater personal experience and more facile devices that are lessbulky. Are the massive forms of ischemia of the pelvis that youdescribed to us today a product of your earliest experience, or is itsomething you believe is a continuing problem in the treatment ofpatients with EVAR?
Finally, could you briefly clarify your recommendations, basedon your experiences, for management of coexisting iliac arteryaneurysms in EVAR. More specifically, how do you time yourselective internal embolizations? Do you stage bilateral emboliza-tions to perhaps reduce the risk for pelvic ischemia? And do you dopreemptive flexible sigmoidoscopy to actually find the problembefore it can become a more significant clinical issue?
Dr Thomas S. Maldonado.This study did not address the incidence of renal or suprarenal
ischemic complications. However, I will tell you that we had noinstances of stroke, upper extremity ischemia, or massive MI that wecan attribute to an atheroembolic cause. Insofar as the renal ischemia,in the event that a renal artery is inadvertently covered we have alwaysbeen successful in stenting the renal artery open. Atheroembolizationto the renal artery, however, may well occur. No instances of acuterenal failure or infarct occurred in our series; however, it would beinteresting to review postoperative CT and or renal function tests toidentify any subclinical sequelae of embolization.
We did not see any CT characteristics, such as flow channelswithin the thrombus, that might help predict embolization. The
MRA I showed you for the patient with embolization preopera-tively may have had some of that, but is more difficult to interpret.
We do not have any experience with the percutaneous en-dograft technique. However, I agree that repair of the commonfemoral artery is occasionally required in our experience, as well.
Our experience is indeed mostly with the Ancure device, abulkier device, and surely that may have had some role inpredisposing these patients to ischemic complications. How-ever, there were 2 patients among the 7 with pelvic ischemiawho had other devices implanted. So I believe that this is aproblem that will persist despite the Ancure device being nolonger available. Endovascular manipulation of catheters, wires,and devices within a thrombin-laden sac will always pose acertain risk for embolization, regardless of lower profile and lesscumbersome devices.
Insofar as our treatment of common iliac artery aneurysms andour staging of coil embolizations, we tend to stage the emboliza-tion at least 2 days before EVAR. In patients with bilateral coilembolizations we usually wait approximately 2 weeks between coilembolizations. In addition, in patients at increased risk for isch-emia (eg, previous colectomies or bilateral hypogastric emboliza-tions) I think it advisable to interrogate the mesenteric collateralcirculation at angiography. Finally, given the 2.25% incidence ofpelvic ischemia after EVAR, we do not use routine preemptivesigmoidoscopy. However, in theory this may surely help in earlierdiagnosis and intervention.