Embed Size (px)
DESCRIPTION
Introduction Forensic Pathology
Citation preview
7/13/2008
1
AN INTRODUCTION TO FORENSIC PATHOLOGY
By Howard W. Oliver, D.O.
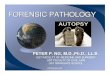
This is hemopericardium as demonstrated by the dark blood in the pericardial sac opened at autopsy. Penetrating trauma or massive blunt force trauma to the chest (often from the steering wheel) causes a rupture of the myocardium and/or coronary arteries with bleeding into the pericardial cavity. The extensive collection of blood in this closed space leads to cardiac tamponade.
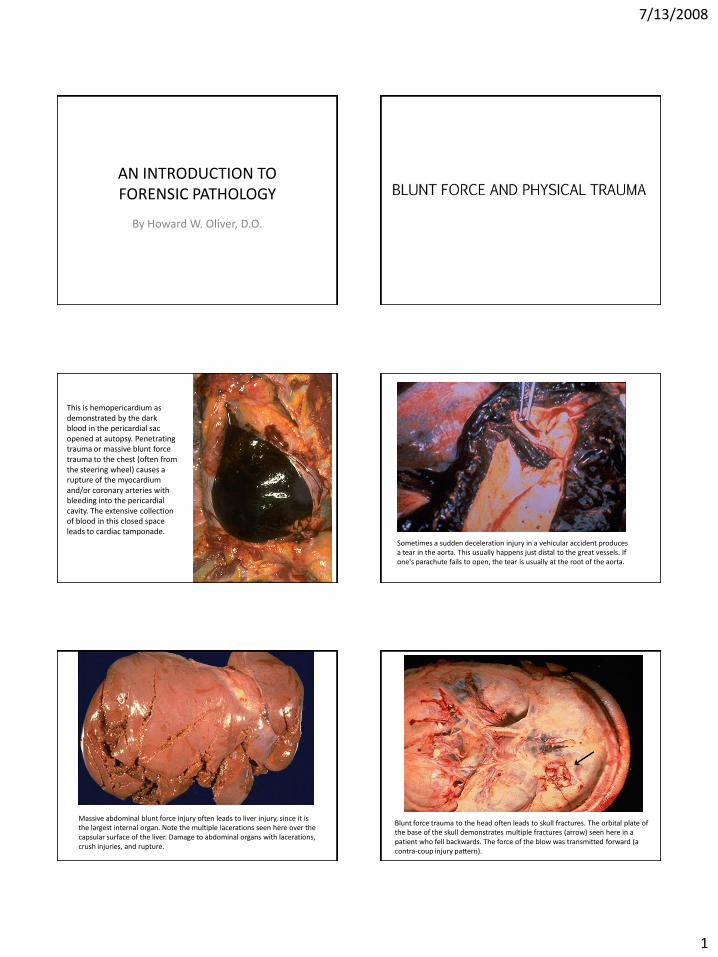
Sometimes a sudden deceleration injury in a vehicular accident produces a tear in the aorta. This usually happens just distal to the great vessels. If one's parachute fails to open, the tear is usually at the root of the aorta.
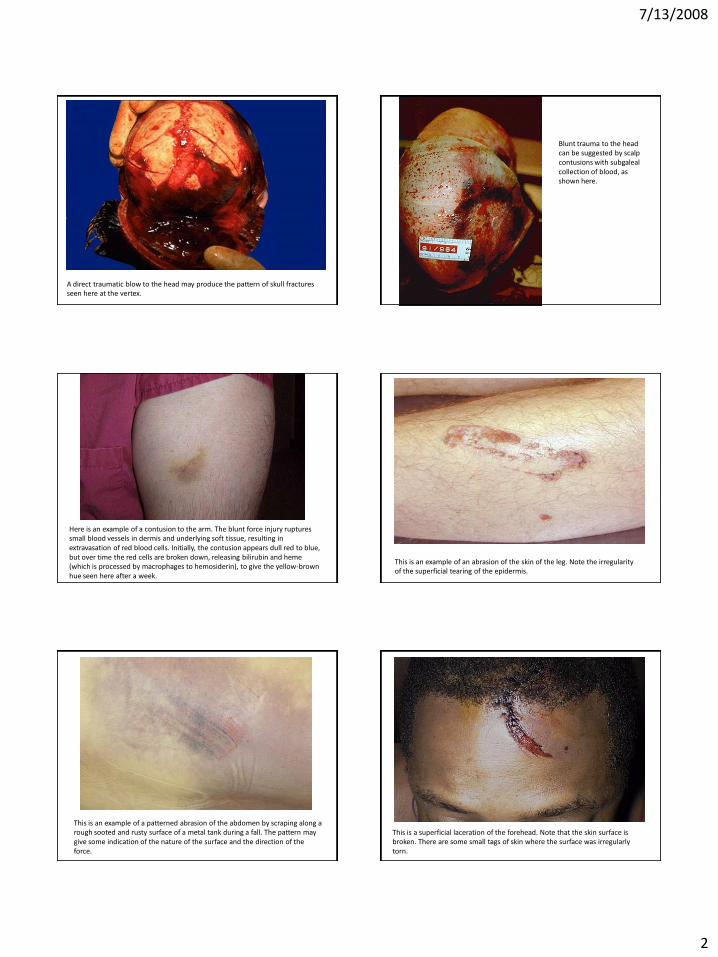
Massive abdominal blunt force injury often leads to liver injury, since it is the largest internal organ. Note the multiple lacerations seen here over the capsular surface of the liver. Damage to abdominal organs with lacerations, crush injuries, and rupture.
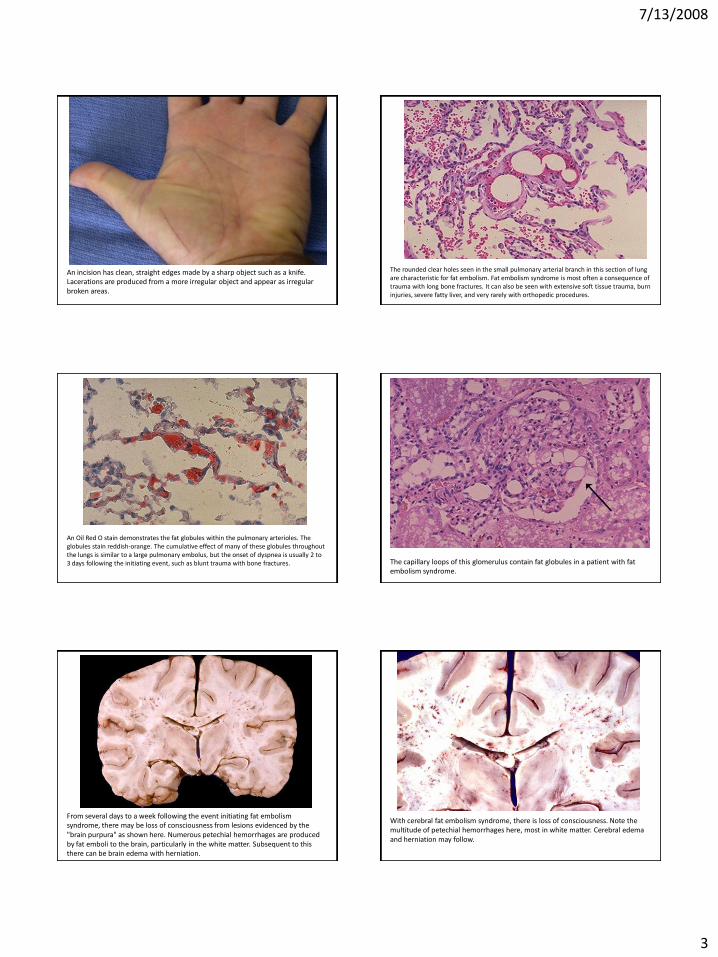
Blunt force trauma to the head often leads to skull fractures. The orbital plate of the base of the skull demonstrates multiple fractures (arrow) seen here in a patient who fell backwards. The force of the blow was transmitted forward (a contra-coup injury pattern).
7/13/2008
2
A direct traumatic blow to the head may produce the pattern of skull fractures seen here at the vertex.
Blunt trauma to the head can be suggested by scalp contusions with subgalealcollection of blood, as shown here.
Here is an example of a contusion to the arm. The blunt force injury ruptures small blood vessels in dermis and underlying soft tissue, resulting in extravasation of red blood cells. Initially, the contusion appears dull red to blue, but over time the red cells are broken down, releasing bilirubin and heme(which is processed by macrophages to hemosiderin), to give the yellow-brown hue seen here after a week.
This is an example of an abrasion of the skin of the leg. Note the irregularity of the superficial tearing of the epidermis.
This is an example of a patterned abrasion of the abdomen by scraping along a rough sooted and rusty surface of a metal tank during a fall. The pattern may give some indication of the nature of the surface and the direction of the force.
This is a superficial laceration of the forehead. Note that the skin surface is broken. There are some small tags of skin where the surface was irregularly torn.
7/13/2008
3
An incision has clean, straight edges made by a sharp object such as a knife. Lacerations are produced from a more irregular object and appear as irregular broken areas.
The rounded clear holes seen in the small pulmonary arterial branch in this section of lung are characteristic for fat embolism. Fat embolism syndrome is most often a consequence of trauma with long bone fractures. It can also be seen with extensive soft tissue trauma, burn injuries, severe fatty liver, and very rarely with orthopedic procedures.
An Oil Red O stain demonstrates the fat globules within the pulmonary arterioles. The globules stain reddish-orange. The cumulative effect of many of these globules throughout the lungs is similar to a large pulmonary embolus, but the onset of dyspnea is usually 2 to 3 days following the initiating event, such as blunt trauma with bone fractures. The capillary loops of this glomerulus contain fat globules in a patient with fat
embolism syndrome.
From several days to a week following the event initiating fat embolism syndrome, there may be loss of consciousness from lesions evidenced by the "brain purpura" as shown here. Numerous petechial hemorrhages are produced by fat emboli to the brain, particularly in the white matter. Subsequent to this there can be brain edema with herniation.
With cerebral fat embolism syndrome, there is loss of consciousness. Note the multitude of petechial hemorrhages here, most in white matter. Cerebral edema and herniation may follow.
7/13/2008
4
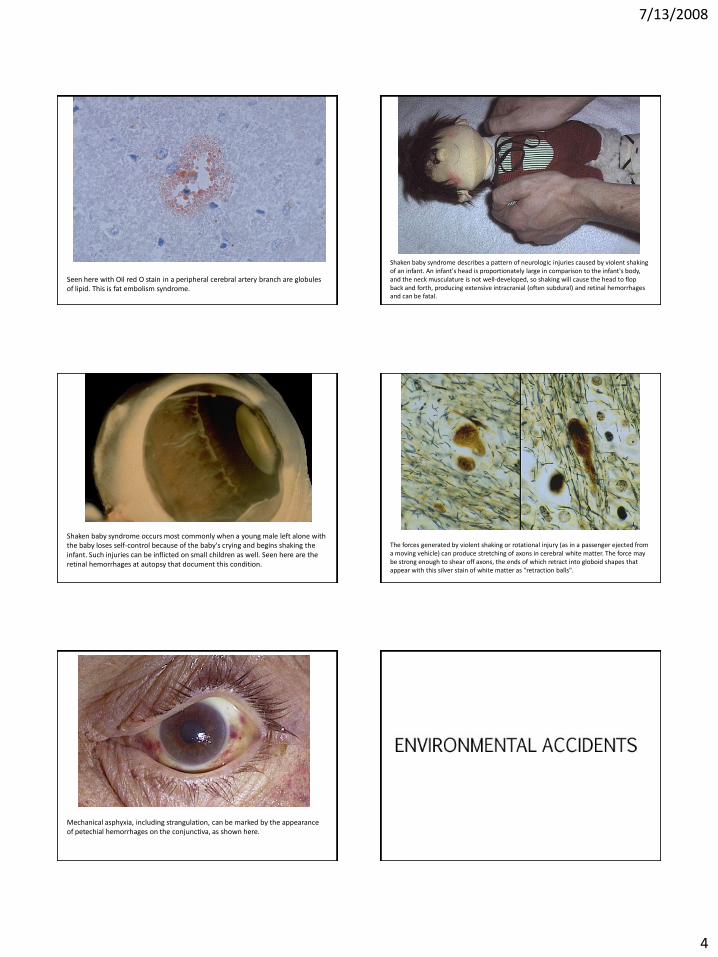
Seen here with Oil red O stain in a peripheral cerebral artery branch are globules of lipid. This is fat embolism syndrome.
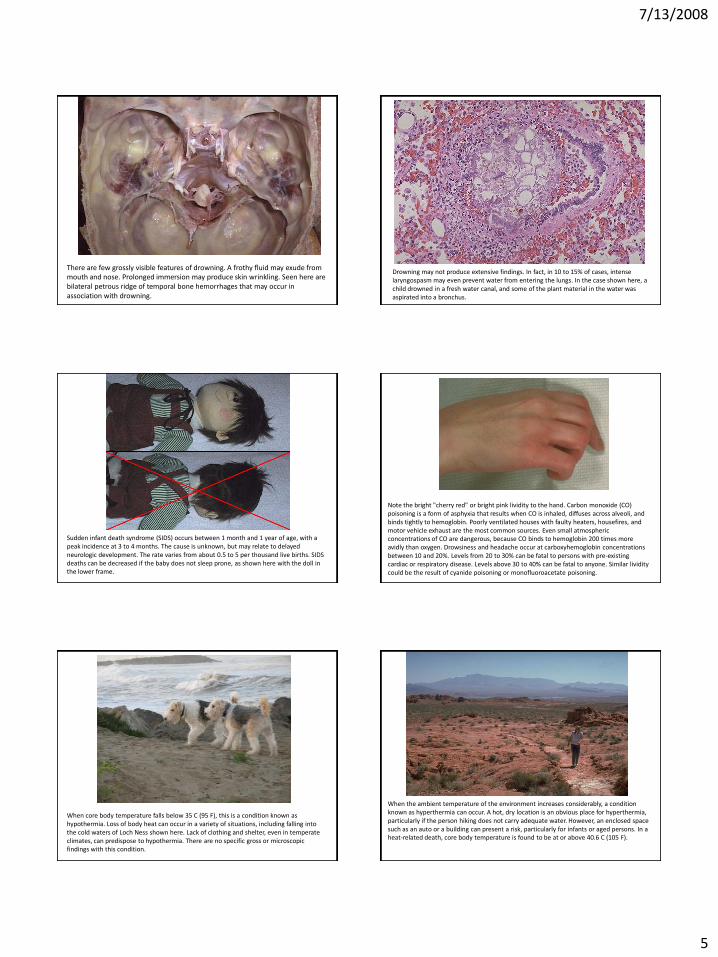
Shaken baby syndrome describes a pattern of neurologic injuries caused by violent shaking of an infant. An infant's head is proportionately large in comparison to the infant's body, and the neck musculature is not well-developed, so shaking will cause the head to flop back and forth, producing extensive intracranial (often subdural) and retinal hemorrhages and can be fatal.
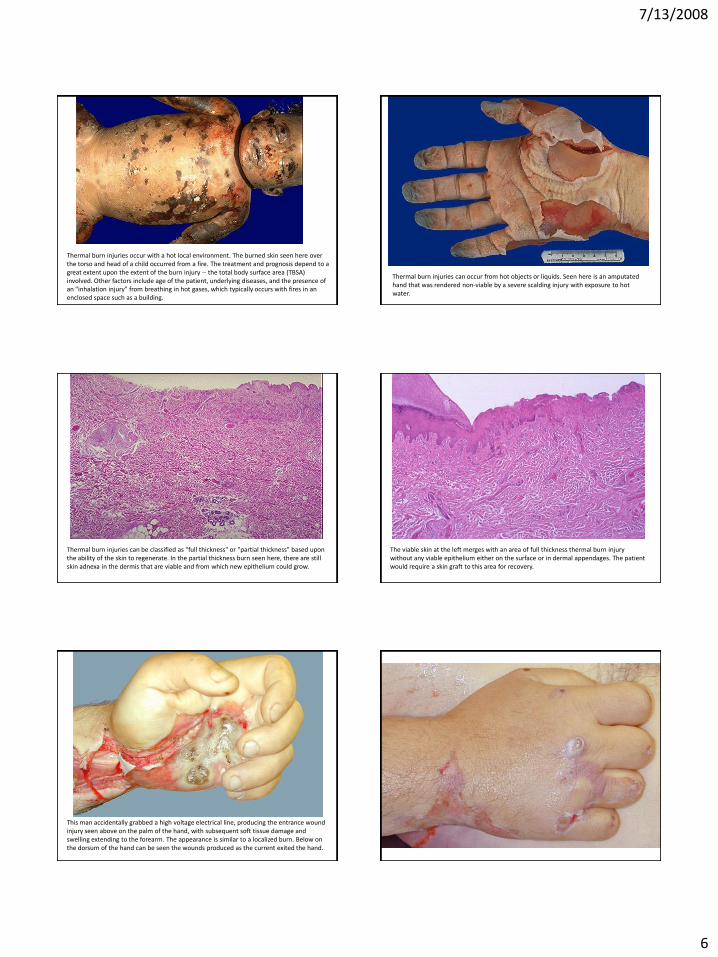
Shaken baby syndrome occurs most commonly when a young male left alone with the baby loses self-control because of the baby's crying and begins shaking the infant. Such injuries can be inflicted on small children as well. Seen here are the retinal hemorrhages at autopsy that document this condition.
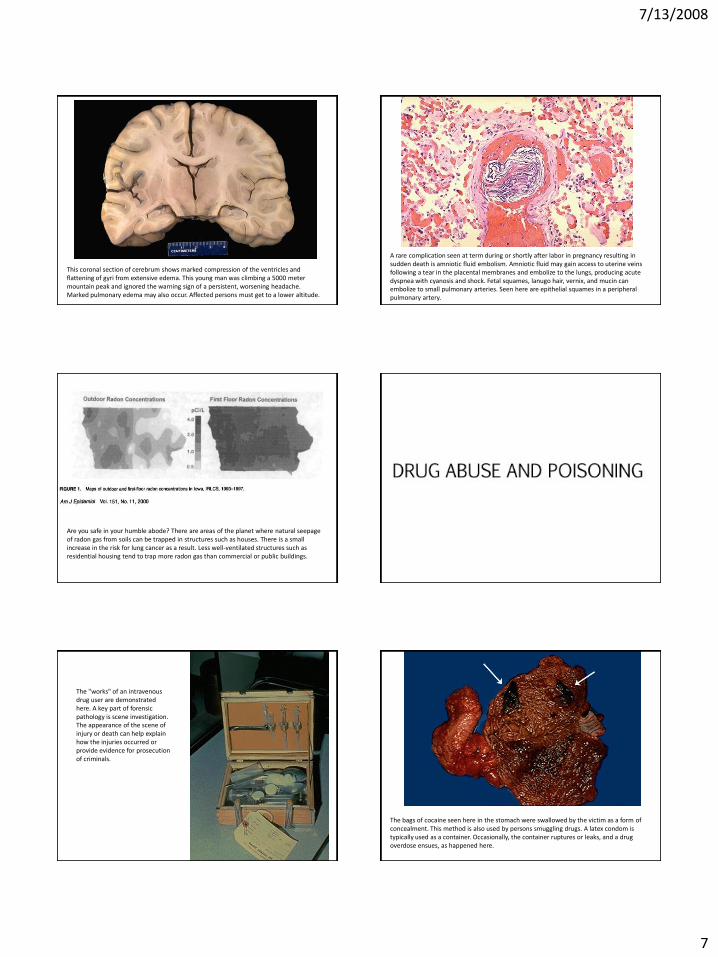
The forces generated by violent shaking or rotational injury (as in a passenger ejected from a moving vehicle) can produce stretching of axons in cerebral white matter. The force may be strong enough to shear off axons, the ends of which retract into globoid shapes that appear with this silver stain of white matter as "retraction balls".
Mechanical asphyxia, including strangulation, can be marked by the appearance of petechial hemorrhages on the conjunctiva, as shown here.
7/13/2008
5
There are few grossly visible features of drowning. A frothy fluid may exude from mouth and nose. Prolonged immersion may produce skin wrinkling. Seen here are bilateral petrous ridge of temporal bone hemorrhages that may occur in association with drowning.
Drowning may not produce extensive findings. In fact, in 10 to 15% of cases, intense laryngospasm may even prevent water from entering the lungs. In the case shown here, a child drowned in a fresh water canal, and some of the plant material in the water was aspirated into a bronchus.
Sudden infant death syndrome (SIDS) occurs between 1 month and 1 year of age, with a peak incidence at 3 to 4 months. The cause is unknown, but may relate to delayed neurologic development. The rate varies from about 0.5 to 5 per thousand live births. SIDS deaths can be decreased if the baby does not sleep prone, as shown here with the doll in the lower frame.
Note the bright "cherry red" or bright pink lividity to the hand. Carbon monoxide (CO) poisoning is a form of asphyxia that results when CO is inhaled, diffuses across alveoli, and binds tightly to hemoglobin. Poorly ventilated houses with faulty heaters, housefires, and motor vehicle exhaust are the most common sources. Even small atmospheric concentrations of CO are dangerous, because CO binds to hemoglobin 200 times more avidly than oxygen. Drowsiness and headache occur at carboxyhemoglobin concentrations between 10 and 20%. Levels from 20 to 30% can be fatal to persons with pre-existing cardiac or respiratory disease. Levels above 30 to 40% can be fatal to anyone. Similar lividity could be the result of cyanide poisoning or monofluoroacetate poisoning.
When core body temperature falls below 35 C (95 F), this is a condition known as hypothermia. Loss of body heat can occur in a variety of situations, including falling into the cold waters of Loch Ness shown here. Lack of clothing and shelter, even in temperate climates, can predispose to hypothermia. There are no specific gross or microscopic findings with this condition.
When the ambient temperature of the environment increases considerably, a condition known as hyperthermia can occur. A hot, dry location is an obvious place for hyperthermia, particularly if the person hiking does not carry adequate water. However, an enclosed space such as an auto or a building can present a risk, particularly for infants or aged persons. In a heat-related death, core body temperature is found to be at or above 40.6 C (105 F).
7/13/2008
6
Thermal burn injuries occur with a hot local environment. The burned skin seen here over the torso and head of a child occurred from a fire. The treatment and prognosis depend to a great extent upon the extent of the burn injury -- the total body surface area (TBSA) involved. Other factors include age of the patient, underlying diseases, and the presence of an "inhalation injury" from breathing in hot gases, which typically occurs with fires in an enclosed space such as a building.
Thermal burn injuries can occur from hot objects or liquids. Seen here is an amputated hand that was rendered non-viable by a severe scalding injury with exposure to hot water.
Thermal burn injuries can be classified as "full thickness" or "partial thickness" based upon the ability of the skin to regenerate. In the partial thickness burn seen here, there are still skin adnexa in the dermis that are viable and from which new epithelium could grow.
The viable skin at the left merges with an area of full thickness thermal burn injury without any viable epithelium either on the surface or in dermal appendages. The patient would require a skin graft to this area for recovery.
This man accidentally grabbed a high voltage electrical line, producing the entrance wound injury seen above on the palm of the hand, with subsequent soft tissue damage and swelling extending to the forearm. The appearance is similar to a localized burn. Below on the dorsum of the hand can be seen the wounds produced as the current exited the hand.
7/13/2008
7
This coronal section of cerebrum shows marked compression of the ventricles and flattening of gyri from extensive edema. This young man was climbing a 5000 meter mountain peak and ignored the warning sign of a persistent, worsening headache. Marked pulmonary edema may also occur. Affected persons must get to a lower altitude.
A rare complication seen at term during or shortly after labor in pregnancy resulting in sudden death is amniotic fluid embolism. Amniotic fluid may gain access to uterine veins following a tear in the placental membranes and embolize to the lungs, producing acute dyspnea with cyanosis and shock. Fetal squames, lanugo hair, vernix, and mucin can embolize to small pulmonary arteries. Seen here are epithelial squames in a peripheral pulmonary artery.
Are you safe in your humble abode? There are areas of the planet where natural seepage of radon gas from soils can be trapped in structures such as houses. There is a small increase in the risk for lung cancer as a result. Less well-ventilated structures such as residential housing tend to trap more radon gas than commercial or public buildings.
The "works" of an intravenous drug user are demonstrated here. A key part of forensic pathology is scene investigation. The appearance of the scene of injury or death can help explain how the injuries occurred or provide evidence for prosecution of criminals.
The bags of cocaine seen here in the stomach were swallowed by the victim as a form of concealment. This method is also used by persons smuggling drugs. A latex condom is typically used as a container. Occasionally, the container ruptures or leaks, and a drug overdose ensues, as happened here.
7/13/2008
8
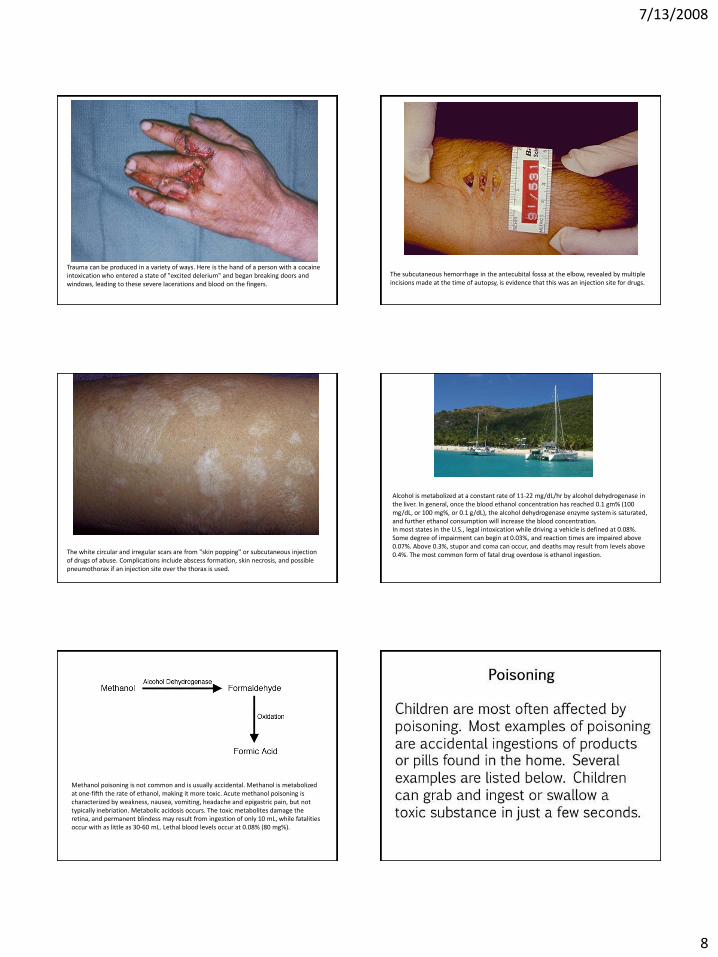
Trauma can be produced in a variety of ways. Here is the hand of a person with a cocaine intoxication who entered a state of "excited delerium" and began breaking doors and windows, leading to these severe lacerations and blood on the fingers.
The subcutaneous hemorrhage in the antecubital fossa at the elbow, revealed by multiple incisions made at the time of autopsy, is evidence that this was an injection site for drugs.
The white circular and irregular scars are from "skin popping" or subcutaneous injection of drugs of abuse. Complications include abscess formation, skin necrosis, and possible pneumothorax if an injection site over the thorax is used.
Alcohol is metabolized at a constant rate of 11-22 mg/dL/hr by alcohol dehydrogenase in the liver. In general, once the blood ethanol concentration has reached 0.1 gm% (100 mg/dL, or 100 mg%, or 0.1 g/dL), the alcohol dehydrogenase enzyme system is saturated, and further ethanol consumption will increase the blood concentration. In most states in the U.S., legal intoxication while driving a vehicle is defined at 0.08%. Some degree of impairment can begin at 0.03%, and reaction times are impaired above 0.07%. Above 0.3%, stupor and coma can occur, and deaths may result from levels above 0.4%. The most common form of fatal drug overdose is ethanol ingestion.
Methanol poisoning is not common and is usually accidental. Methanol is metabolized at one-fifth the rate of ethanol, making it more toxic. Acute methanol poisoning is characterized by weakness, nausea, vomiting, headache and epigastric pain, but not typically inebriation. Metabolic acidosis occurs. The toxic metabolites damage the retina, and permanent blindess may result from ingestion of only 10 mL, while fatalities occur with as little as 30-60 mL. Lethal blood levels occur at 0.08% (80 mg%).

7/13/2008
9
This scene illustrates the mechanism for "defense wounds". Such wounds result from an attempt to ward off the assailant. The victim holds up forearms and hands in front of the body.
7/13/2008
10
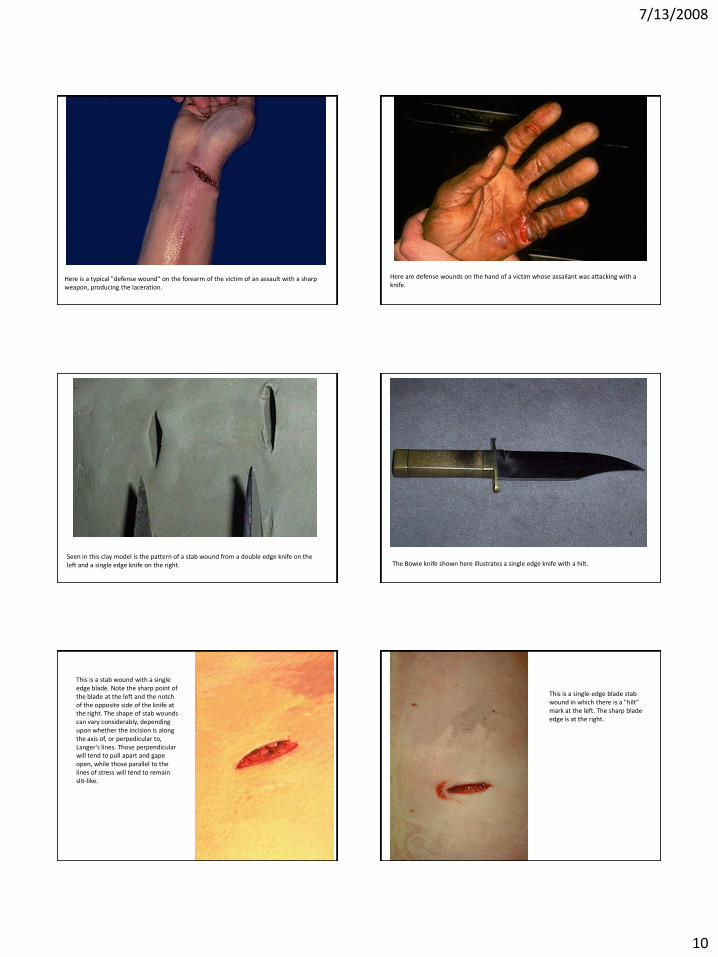
Here is a typical "defense wound" on the forearm of the victim of an assault with a sharp weapon, producing the laceration.
Here are defense wounds on the hand of a victim whose assailant was attacking with a knife.
Seen in this clay model is the pattern of a stab wound from a double edge knife on the left and a single edge knife on the right. The Bowie knife shown here illustrates a single edge knife with a hilt.
This is a stab wound with a single edge blade. Note the sharp point of the blade at the left and the notch of the opposite side of the knife at the right. The shape of stab wounds can vary considerably, depending upon whether the incision is along the axis of, or perpedicular to, Langer's lines. Those perpendicular will tend to pull apart and gape open, while those parallel to the lines of stress will tend to remain slit-like.
This is a single-edge blade stab wound in which there is a "hilt" mark at the left. The sharp blade edge is at the right.
7/13/2008
11
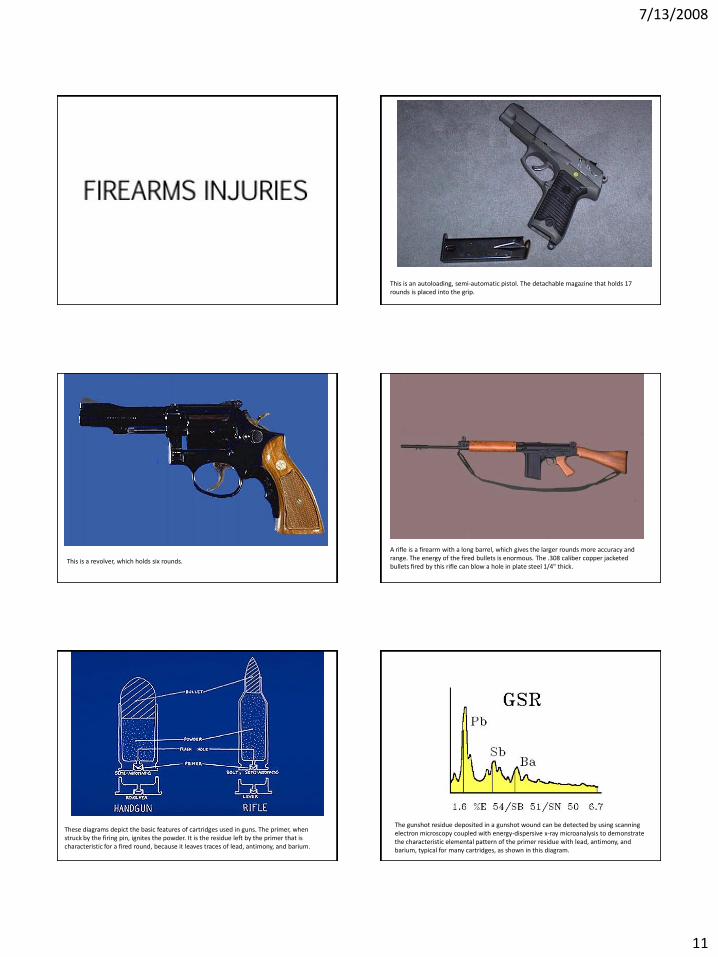
This is an autoloading, semi-automatic pistol. The detachable magazine that holds 17 rounds is placed into the grip.
This is a revolver, which holds six rounds.
A rifle is a firearm with a long barrel, which gives the larger rounds more accuracy and range. The energy of the fired bullets is enormous. The .308 caliber copper jacketed bullets fired by this rifle can blow a hole in plate steel 1/4" thick.
These diagrams depict the basic features of cartridges used in guns. The primer, when struck by the firing pin, ignites the powder. It is the residue left by the primer that is characteristic for a fired round, because it leaves traces of lead, antimony, and barium.
The gunshot residue deposited in a gunshot wound can be detected by using scanning electron microscopy coupled with energy-dispersive x-ray microanalysis to demonstrate the characteristic elemental pattern of the primer residue with lead, antimony, and barium, typical for many cartridges, as shown in this diagram.
7/13/2008
12
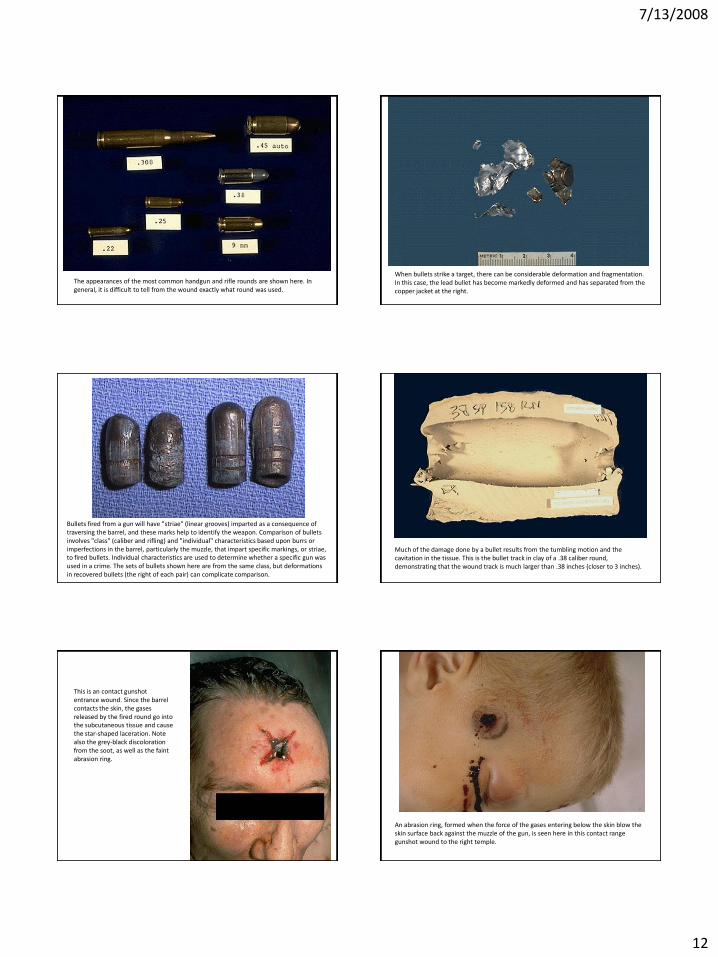
The appearances of the most common handgun and rifle rounds are shown here. In general, it is difficult to tell from the wound exactly what round was used.
When bullets strike a target, there can be considerable deformation and fragmentation. In this case, the lead bullet has become markedly deformed and has separated from the copper jacket at the right.
Bullets fired from a gun will have "striae" (linear grooves) imparted as a consequence of traversing the barrel, and these marks help to identify the weapon. Comparison of bullets involves "class" (caliber and rifling) and "individual" characteristics based upon burrs or imperfections in the barrel, particularly the muzzle, that impart specific markings, or striae, to fired bullets. Individual characteristics are used to determine whether a specific gun was used in a crime. The sets of bullets shown here are from the same class, but deformations in recovered bullets (the right of each pair) can complicate comparison.
Much of the damage done by a bullet results from the tumbling motion and the cavitation in the tissue. This is the bullet track in clay of a .38 caliber round, demonstrating that the wound track is much larger than .38 inches (closer to 3 inches).
This is an contact gunshot entrance wound. Since the barrel contacts the skin, the gases released by the fired round go into the subcutaneous tissue and cause the star-shaped laceration. Note also the grey-black discoloration from the soot, as well as the faint abrasion ring.
An abrasion ring, formed when the force of the gases entering below the skin blow the skin surface back against the muzzle of the gun, is seen here in this contact range gunshot wound to the right temple.
7/13/2008
13
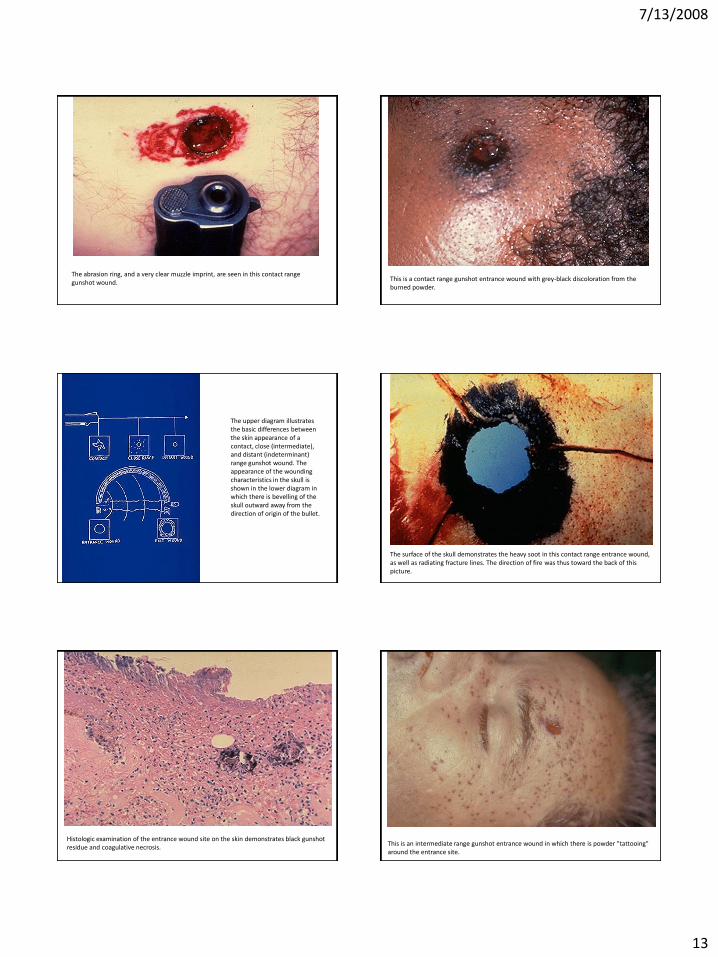
The abrasion ring, and a very clear muzzle imprint, are seen in this contact range gunshot wound.
This is a contact range gunshot entrance wound with grey-black discoloration from the burned powder.
The upper diagram illustrates the basic differences between the skin appearance of a contact, close (intermediate), and distant (indeterminant) range gunshot wound. The appearance of the wounding characteristics in the skull is shown in the lower diagram in which there is bevelling of the skull outward away from the direction of origin of the bullet.
The surface of the skull demonstrates the heavy soot in this contact range entrance wound, as well as radiating fracture lines. The direction of fire was thus toward the back of this picture.
Histologic examination of the entrance wound site on the skin demonstrates black gunshot residue and coagulative necrosis.
This is an intermediate range gunshot entrance wound in which there is powder "tattooing" around the entrance site.
7/13/2008
14
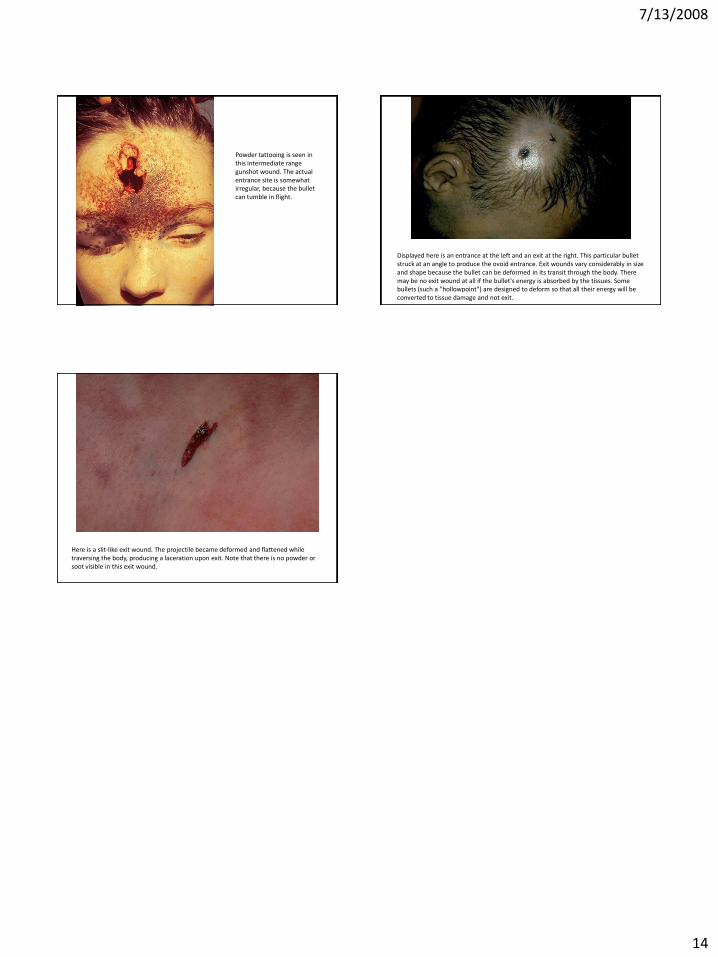
Powder tattooing is seen in this intermediate range gunshot wound. The actual entrance site is somewhat irregular, because the bullet can tumble in flight.
Displayed here is an entrance at the left and an exit at the right. This particular bullet struck at an angle to produce the ovoid entrance. Exit wounds vary considerably in size and shape because the bullet can be deformed in its transit through the body. There may be no exit wound at all if the bullet's energy is absorbed by the tissues. Some bullets (such a "hollowpoint") are designed to deform so that all their energy will be converted to tissue damage and not exit.
Here is a slit-like exit wound. The projectile became deformed and flattened while traversing the body, producing a laceration upon exit. Note that there is no powder or soot visible in this exit wound.