Embed Size (px)
Citation preview

_Journal ofNeurology, Neurosurgery, and Psychiatry 1996;60:667-670
Intra-arterial thrombolysis in acute ischaemicstroke: experience with a superselective catheterembedded in the clot
Luciano Casto, Lionello Caverni, Massimo Camerlingo, Bruno Censori, Luca Moschini,Maria Cristina Servalli, Tania Partziguian, Giorgio Belloni, Angelo Mamoli
2nd NeurologicalDepartmentL CastoM CamerlingoB CensoriM C ServalliT PartziguianA MamoliNeuroradiologicalUnit, Ospedali Riuniti,24100 Bergamo, ItalyL CavemiL MoschiniG BelloniCorrespondence to:Dr Luciano Casto, Divisionedi Neurologia 2, OspedaliRiuniti di Bergamo, LargoBarozzi 1, I 24100, Italy.Received 1 1 August 1995and in revised form23 January 1996Accepted 23 February 1996
AbstractObjectives-To report experience ofintra-arterial thrombolysis for acutestroke, performed with a microcatheternavigated into the intracranial circulationto impale the clot.Methods-Patients were selected on thefollowing criteria: (1) clinical examina-tion suggesting a large vessel occlusion instroke patients between 18 and 75 years;(2) no radiographic signs of large actualischaemia on CT at admission; (3) angio-graphically documented occlusion of themiddle cerebral artery (MCA) stem or ofthe basilar artery (BA), without occlusionof the ipsilateral extracranial internalcarotid artery or of both the vertebralarteries; (4) end of the entire procedurewithin six hours of stroke. 12 patients withacute stroke were recruited, eight ofwhom had occlusion of the MCA stemand four ofthe BA. Urokinase was used as
the thrombolytic agent.Results-Complete recanalisation in sixMCA stem and in two BA occurred, andpartial recanalisation in two MCA stemand one BA. There was no recanalisationin one BA. A clinically silent haemor-rhage occurred in two patients, and a
parenchymal haematoma in one patient,all in MCA occlusions. At four monthsfive patients achieved self sufficiency(four with MCA and one with BA occlu-sion). Six patients were dependent (threetotally), and one died.Conclusions-The strict criteria of eligi-bility allowing the enrolment of very fewpatients and the procedure itself, requir-ing particular neuroradiological exper-
tise, make this procedure not routine.Nevertheless, the approach can be consid-ered a possible option for patients withacute ischaemic stroke.
(7 Neurol Neurosurg Psychiatry 1996;60:667-670)
Keywords: acute ischaemic stroke; cerebral arterialocclusion; intra-arterial thrombolysis
To use thrombolysis effectively in acuteischaemic stroke is a major current challenge.Cumulative experiences with intravenous or
intra-arterial treatment have shown its feasibil-ity in humans, and suggest an associationbetween recanalisation and clinical improve-ment.' Unfortunately, some clinical trialswith intravenous drugs had to be interrupted
because of an excess of cerebral haemorrhages,and the conclusions from the EuropeanCooperative Acute Stroke Study (ECASS)4clearly indicate that intravenous thrombolysisis not a treatment for all patients with acutestroke. The intra-arterial approach hasrecently been improved by the introduction ofcatheters that can be navigated into theintracranial circulation and are able to disruptthe thrombus with the tip before deliveringdrugs. We report 12 patients treated with thisapproach.
Patients and methodsFrom January 1991 to February 1995, afterprevious experience with a local intra-arterialapproach,5 we have considered patients pre-senting within four hours of a severe acuteischaemic stroke for mechanical disruption ofthe thrombus and intra-arterial delivery of thethrombolytic agent. Exclusion criteria were:(1) inability to end the entire procedure withinsix hours of the onset of stroke; (2) occlusionof the extracranial arteries ipsilateral to strokein patients with hemispheric stroke or of bothvertebral arteries in cases of brainstem stroke;(3) direct or indirect signs of large actualongoing infarction or of any disease other thanstroke on CT at admission; (4) age < 18 or> 75 years; (5) regression of signs before start-ing the procedure; (6) any contraindication forthrombolytic agents; (7) severe systolic hyper-tension (> 180 mm Hg) despite appropriatetreatment; (8) severe concurrent diseasesinterfering with natural life expectancy; (9)absence of informed consent from patients orrelatives. Indirect signs of pronouncedischaemia of middle cerebral artery territorieswere effacement of most sulci, diffuseswelling, early parenchymal hypodensity, andloss of putaminal hyperdensity. The protocolwas approved by our ethics committee.Patients who were selected were submitted toarteriography with the Seldinger method, util-ising a digital subtraction device (TG 200,CER, Paris, France). Topographic localisationof the occluded segments of the middle cere-bral artery was adapted from Boazzao et a16(Ml = the mainstem of the middle cerebralartery before the lenticular arteries, M2 = themainstem after the lenticular arteries, and M3= the bifurcation of the mainstem). Onceappropriate occlusion of the middle cerebralartery stem or of the basilar artery was demon-strated, a microcatheter (Tracker 18, TargetTherapeutics, San Jose, CA) was mounted onthe guidewire, and pushed onwards to impale,
667
on March 1, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.60.6.667 on 1 June 1996. D
ownloaded from

Casto, Caverni, Camerlingo, Censori, Moschini, Servalli, et al
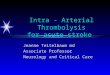
Figure 1 Patient 2: (A)pretreatment Ml occlusion.(B) The tip of the catheteris beyond the thrombus withopacification of the distalvessels. (C) Post-treatmentrecanalisation with possibleembolisation in some distalpanietal branches.
I
and pass through, the clot. After showing thepatency of the circulation beyond the clot,urokinase was delivered. We used urokinase,because it was the thrombolytic agent allowedfor intra-arterial delivery in our hospital. Weused a bolus of 100 000 units, followed by a
pump infused dose of 500 000 units over one
hour. In cases of persistent arterial occlusionurokinase was added to a total of 1 000 000units. Recanalisation was defined as absent,
Clinical characteristics: time to treatment, dose of urokinase,four months
partial, or complete. Patients were then closelymonitored in our stroke unit, for bleeding andother complications. Subcutaneous calciumheparin (12 500 units twice a day), was started30 minutes after the end of the procedure andcontinued until oral anticoagulation or
antiplatelet treatment was initiated. Brain CTwas carried out on admission, within seven
days of treatment, and whenever clinicallyrequired. Neurological examination was car-
ried out on admission, immediately after thetreatment, daily for seven days, and at one andfour months after treatment and scored withthe National Institute for Health Scale.7Outcome was assessed with a modified Rankinscore scale at four months.8 A score 1-2 was
deemed self sufficiency, 3 partial dependency, 4and 5 total dependency, and 6 death.
ResultsA total of 1342 stroke patients were admittedin our ward over the study period. The eligibil-ity criteria immediately ruled out 603 patientsas outside the age limits. Of the others, 162were seen within four hours and 18 of themunderwent angiography. Three already hadpatent intracranial circulation and three hadan extended occlusion of the extracranialinternal carotid artery and siphon. Twelvepatients were eventually treated (five women
recanalisation, haemorrhagic transformations, and outcome at
Occlusion TimeAgelsex Signs Risk factors site (min) UK (MU) Rec Haem Rankin
1 27/F LH Pill M2 120 0-6 T HT 12 31/F LH VAF M1 120 0-6 T - 23 33/F LH MVD M1 130 0 7 T - 24 35/M TP/S Hyp BA 180 0-8 T - 25 44/M TP/S None BA 120 1.0 No - 56 50/M TP/S None BA 120 0 7 T - 37 53/M RH/A Sm M3 120 0-8 P - 38 58/M LH MVD M1 300 0-8 T - 49 68/F LH AF M3 180 0-8 T - 2
10 68/F LH AF/Sm/Hyp M1 120 0-7 T PHE 411 69/M TP/S Hyp BA 120 1.0 P 612 72/M RH/A AF M3 300 0-8 P HT 3
LH = Left hemiplegia; RH = right haemiplegia; A = aphasia; TP/S = tetraparesis and stupor; MVD = mitral valve disease; VAF =valvar atrial fibrillation; Sm = smoking, AF = atrial fibrillation; hyp = hypertension; Ml; 2; 3, see text; BA = basilar artery occlusion;Time = time from stroke to treatment; UK = urokinase; MU = MegaUnits; Rec = recanalisation; T = total; P = partial; Haem =brain haemorrhage; HT = haemorrhagic transformation; PHE = parenchymal haematoma.
668
_ _
....... _
on March 1, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.60.6.667 on 1 June 1996. D
ownloaded from

Intra-arterial thrombolysis in acute ischaemic stroke: experience with a superselective catheter embedded in the clot
Figure 2 Patient 4: (A)pretreatment occlusion ofthe distal basilar artery.(B) The microcatheter tip(arrows) is beyond thethrombus, which is clearlyvisible (arrowhead). (C)Post-treatment thrombusdissolution withembolisation in the leftposterior cerebral artery. I I
n3.A
and seven men, aged 27 to 72 years). Six ofthem had potential cardiac sources ofemobolism, and two were free from risk fac-tors for stroke. The clinical picture of strokewas: a left hemiplegia plus hemianopia andhemineglect in six patients, a right hemiplegiaplus aphasia and hemianopia in two, tetrapare-sis and stupor in four. Arteriography showedarterial occlusion at the Ml segment in fourpatients, at M2 in one, at M3 in three, and inthe basilar trunk in four. Recanalisation wasachieved in 11 patients. It was complete ineight and partial in three. Haemorrhage wasseen in three patients: in two it was clinicallysilent, in one it was accompanied by clinicaldeterioration with CT features of parenchymalhaematoma. It always occurred in the stroketerritories. None of the patients had systemichaemorrhages. After four months five patients(four with middle cerebral artery and one withbasilar artery occlusion) regained self suffi-ciency, three were partially dependent, andthree were totally dependent. One patient died14 days after stroke because of reocclusion of a
partially reopened basilar artery, after dra-matic temporary improvement. The tablegives the results.
DiscussionOur experience suggests that intra-arterialthrombolysis with a microcatheter brought upto impale the clot can be beneficial for patientswith acute stroke from middle cerebral arterystem or basilar artery occlusion, but it cannotbe considered as a routine approach. Thistechnique is associated with a higher rate ofarterial recanalisation than the intravenousapproach.' Recanalisation, which is a require-ment of efficacy,9-'9 seems related to locationand nature of the occlusion; the extracranialportions of the internal carotid artery were lessamenable to recanalisation than the distalones.20-22 The rationale of this technique issupported by the concept that the mechanicaldisruption of the clot would increase the areaof contact with the drug, mimimising the risksof local and systemic bleeding. Eight patientsimproved and five patients regained total self-sufficiency. Our results are in agreement withthe report of a recent revision of publishedexperiences with intra-arterial thrombolysis asfar as recanalisation and outcome are con-cerned.23 Bollaert et al, using the same proce-dure, reported more deaths and pooreroutcomes than we did.'4 In that series, how-ever, there were more patients with occlusionat the carotid siphon. Patient 8 of our series,despite recanalisation, had a poor outcome. Inthis case the time elapsed from stroke to treat-ment was 300 minutes, and this might havebeen crucial together with the pulmonaryoedema from cardiac failure that occurred thenext day. Intraparenchymal cerebral haema-toma was seen in one patient. In two otherpatients with a haemorrhage it was clinicallysilent and not necessarily related to treatmentas haemorrage as well as parenchymalhaematoma can be part of the natural historyof ischaemic stroke.'5 Two patients with basi-lar stroke had the worst outcomes (death andlocked in syndrome). These were associatedwith persistent occlusion in one and reocclu-sion of the partially recanalised trunk in theother. Both were probably of atherothrom-botic origin, as was the case with middle cere-bral artery occlusion described by Jungreis etal26 and treated in the same way. Two patients
669
.Wl
0 $g-.-
0 '.. "::
0
on March 1, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.60.6.667 on 1 June 1996. D
ownloaded from

Casto, Caverni, Camerlingo, Censori, Moschini, Servalli, et al
with persistent recanalisation after basilarartery occlusion became independent, and ithas to be considered an excellent outcome inthis vascular syndrome, in which the prognosisis poor.27 Our experience has to be consideredanecdotal, due to the few patients and theabsence of a randomised control group, whichprecluded statistical analysis. We are contem-poraneously involved in a joint clinical trialwith an intravenous approach for patients withcarotid artery stroke, with broader age limitsand without requirement for angiography.Less than 20 of the patients included in thosetrials could be treated with an intra-arterialapproach according to our criteria. If thesewere included the numbers would still be verysmall. A large trial would certainly be advis-able, but would be costly, with requirement ofa great number of centres selecting amongthousands of patients.28 Objections might thenbe raised after an angiography not followed byany treatment after showing the appropriateocclusion.
With these limitations, we think that thisapproach can be a therapeutic option in thetreatment of acute ischaemic stroke, possiblyintegrated in the future with new diagnostictools able to give further information in thevery early stages.29 30 It has to be rememberedthat conventional CT is still a reliable tool inthe hyperacute setting of a stroke.3' Theimportance of a quick referral of the selectedpatient, evaluation by trained neurologists,and rapid access to neuroradiological facilitiesstaffed by a skilled interventional team mustbe stressed.
AddendumBy the time this paper was completed, theresults of the trial with intravenous tissue plas-minogen activator in acute ischaemic strokehad been published.32 The conclusions arethat treatment within three hours of the onsetof acute ischaemic stroke improves clinicaloutcome at three months. The selection made,with inclusion of patients with a broad rangeof neurological deficits and stroke subtypesnot angiographically proved, while giving amore optimistic view on intravenous throm-bolysis, does not lessen in our opinion thevalidity of the intra-arterial approach in partic-ularly defined cases.
1 del Zoppo JG. Thrombolytic therapy in acute stroke, recentexperience. Cerebrovasc Dis 1993;3:256-63.
2 Wardlaw JM, Warlaw CP. Thrombolysis in acute ischemicstroke: does it work? Stroke 1992;23:1826-39.
3 Brott T, Broderick J, Kothari R. Thrombolytic therapy forstroke. Current opinion in Neurology 1994;7:25-35.
4 Hacke W, Kaste M, FieschiC, et al. Intravenous thrombol-ysis with recombinant tissue plasminogen activator foracute hemispheric stroke: the European CooperativeAcute Stroke Study (ECASS). JAMA 1995;274:1017-25.
5 Casto L, Moschini L, Camerlingo M, et al. Local intraarte-rial thrombolysis for acute ischemic stroke in the carotidartery territory. Acta Neurol Scand 1992;86:308-1 1.
6 Bozzao L, Bastianello S, Fantozzi CM, Angeloni V,Argentino C, Fieschi C. Correlation of angiographic andsequential CT findings in patients with evolving cerebralinfarction. AJ7NRAm J Neuroradiol 1989;10:1215-22.
7 Brott T, Adams HP Jr, Olinger CP. Measurement of acutecerebral infarction: a clinical examination scale. Stroke1989;20:864-70.
8 Bamford JM, Sandercock PAG, Warlow CP, Slattery J.Interobserver agreement for the assessment of handicapin stroke patients. Stroke 1989;20:828.
9 del Zoppo JG, Poek K, Pessin MS and the Acute strokeStudy group. Recombinant tissue plasminogen activatorin acute thrombotic and embolic stroke. Ann Neurol1992;32:78-86.
10 Mori E, Yoneda Y, Tabuchi M, et al. Intravenous recombi-nant tissue plasminogen activator in acute carotid arteryterritory stroke. Neurology 1992,42:976-82.
11 Von Kummer R. Intravenous tissue plasminogen activatorin acute stroke. In: Hacke W, del Zoppo JG, HirchbergM, eds. Thrombolytic therapy in acute ischemic stroke.Heidelberg: Springer, 1991;161-7.
12 Yamaguchi T. Intravenous rtPA in acute embolic stroke.In: Hacke W, del Zoppo JG, Hirshberg M, eds.Thrombolytic therapy in acute ischemic stroke. Heidelberg:Springer, 1991:168-74.
13 del Zoppo JG, Ferbert A, Otis S, et al. Local intraarterialfibrinolythic therapy in acute carotid territory stroke: apilot study. Stroke 1988;19:307-13.
14 Mori E, Tabuchi M, Yoshida T, Yamadori A. Intracarotidurokinase with thromboembolic occlusion of the middlecerebral artery. Stroke 1988;19:802-12.
15 Zeumer H, Freitag HG, Grzyka U, Neunzig HP. Localintra arterial fibrinolysis in acute vertebrobasilar occlu-sion: technical developments and recent results.Neuroradiology 1989;31:336-40.
16 Theron J, Courtheoux P. Casasco A, et al. Local intra-arterial fibrinolysis in the carotid territory AJNR Am JNeuroradiol 1989;10:753-65.
17 Matsumoto K, Satoh K. Topical intraarterial urokinaseinfusion for acute stroke. In: Hacke W, del Zoppo JG,Hirschberg M, eds. Thrombolytic therapy in acute ischemicstroke. Heidelberg: Springer, 1991:207-12.
18 del Zoppo JG, Zeumer H, Harker LA. Thrombolytic therapyin acute stroke: possibilities and hazards. Stroke 1986;17:595-607.
19 Mori E. Fibrinolytic recanalization therapy in acute cere-brovascular thromboembolism. In: Hacke W, del ZoppoJG, Hirschberg M, eds. Thrombolytic therapy in acuteischemic stroke. Berlin: Springer Verlag, 1990:137-46.
20 Caplan LR. Brain embolism revisited. Neurology 1993;43:1281-7.
21 Ito Z, Suzuki A, Menura K. Prognostic factors in sponta-neous recanalization of middle cerebral artery occlusion.In: Ito Z, Kutzuzawa T, Yasui N, eds. Cerebral ischemia-an update. Amsterdam: Excerpta Medica, 1983:159-66.
22 del Zoppo GJ, Pessin MS, Mori E, Hacke W.Thrombolytic therapy in acute thrombotic and embolicstroke. Semin Neurol 199111:368-84.
23 Von Kummer R. Intraarterial fibrinolysis in intracranialartery occlusion. In: Bozzao L, ed. NeuroradiologiaUdine: Ed del Centauro, 1995:179-82.
24 Bollaert PE, Bracard S, Boulanger T, et al. Early localintraarterial thrombolysis for severe middle cerebralartery stroke. Cerebrovasc Dis 1995;5:292-6.
25 Homig CR, Dorndorf W, Agnoli A. Hemorrhagic cerebralinfarction-a prospective study. Stroke 1986;17: 179-85.
26 Jungreis CA, Wechsler RR, Horton J. Intraarterial throm-bolysis with a catheter embedded in the clot. Stroke 1989;20:1578-80.
27 Hacke W, Zeumer H, Ferbert A, Brukmann H, del ZoppoJG. Intraarterial thrombolysis improves outcome inpatients with acute vertebrobasilar occlusive disease.Stroke 1988;19:1216-22.
28 Ferguson RDG, Ferguson JG. Cerebrebral intraarterial fib-rinolysis at the crossroads: is a phase III trial advisable atthis time? A3tNRAmJ Neuroradiol 1994;15:1201-16.
29 Warach S,Chien D, Li W,Ronthal M, Edelmann RR. Fastmagnetic resonance diffusion weighted imaging of acutehuman stroke. Neurology 1992;42: 1717-23.
30 Rother J, Guckel F, Neff W, Kuhnen J, Hennerici M,Schwartz A. Assessment of cerebral blood volume inacute stroke using dynamic contrast enhanced magneticresonance imaging. Neurology 1994;44 (suppl 2) :182A.
31 Mohr J, Biller J, Hilal SK, Yiu WTC, Tatemichi TK.Magnetic resonance versus computed tomographic imag-ing in acute stroke. Stroke 1995;26:807-12.
32 The National Institute Of Neurological Disorders andStroke rt-PA Stroke Study Group. Tissue plasminogenactivator for acute ischemic stroke. N Engl J Med 1995;333:1581-7.
670
on March 1, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.60.6.667 on 1 June 1996. D
ownloaded from