Embed Size (px)
Citation preview

647
Comparison of Finger and Intra-arterialBlood Pressure Monitoring at Rest and
During Laboratory TestingGianfranco Parati, Roberto Casadei, Antonella Groppelli,
Marco Di Rienzo, and Giuseppe Mancia
The accuracy of blood pressure values obtained by continuous noninvasive finger blood pressurerecording via the FINAPRES device was evaluated by comparison with simultaneous intra-arterial monitoring both at rest and during performance of tests known to induce fast and oftenmarked changes in blood pressure. The comparison was performed in 24 normotensive oressential hypertensive subjects. The average discrepancy between finger and intra-arterial bloodpressure recorded over a 30-minute rest period was 6.5±2.6 mm Hg and 5.4±2.9 mm Hg forsystolic and diastoiic blood pressure, respectively; a close between-method correspondence wasalso demonstrated by linear regression analysis. The beat-to-beat changes in finger systolic anddiastoiic blood pressure were on average similar to those measured intra-arterially during teststhat induced a pressor or depressor response (hand-grip, cold pressor test, diving test, Valsalvamaneuver, intravenous injections of phenylephrine and trinitroglycerine) as well as during teststhat caused vasomotor changes without major variations in blood pressure (application of lowerbody negative pressure, passive leg raising). The average between-method discrepancy in theevaluation of blood pressure changes was never greater than 4.3 and 2.0 mm Hg for systolic anddiastoiic blood pressure, respectively; the corresponding standard deviations ranged between4.6 and 1.6 mm Hg. Beat-to-beat computer analysis of blood pressure variability over the30-minute rest period provided standard deviations almost identical when calculated byseparate consideration of intra-arterial and finger blood pressure tracings (3.7 and 3.8 mm Hg,respectively). The two methods of blood pressure recording also allowed similar assessments ofthe sensitivity of baroreceptor control of heart rate (vasoactive drug injections) and bloodpressure (neck chamber technique) to be obtained. Thus, beat-to-beat blood pressure recordingvia FINAPRES provides an accurate estimate of means and variability of radial blood pressurein groups of subjects and represents in most cases an acceptable alternative to invasive bloodpressure monitoring during laboratory studies. (Hypertension 1989; 13:647-655)
In the early 1970s a Czech physiologist, IanPenaz, described a new approach to continu-ous noninvasive recording of blood pressure at
the finger level,1 based on a volume-clamp method.This device was improved in its technical aspects(finger plethysmograph of reduced dimension, feed-back system for finger volume control, and auto-matic calibration) by Wesseling and coworkers,2
resulting in an instrument called "FINAPRES"(from FINger Arterial PRESsure). In preliminary
From the Cattedra di Scmciotica Medica e Istituto di ClinicaMedica Generate e Terapia Medica, Universita di Milano; Cen-tro di Fisiologia Clinica e Ipertensione, Ospedale Maggiore;Centro Auxologico Italiano; Centro di Bioingegneria, Fondazi-one Pro Juventute e Politecnico di Milano (M.DR.), Milan, Italy.
Address for correspondence: Prof. Giuseppe Mancia, Centro diFisiologia e Ipertensione, via F. Sforza 35, 20122 Milano, Italy.
Received September 28, 1988; accepted January 19, 1989.
studies performed in patients undergoing surgery,FINAPRES was shown to provide blood pressurevalues close to those simultaneously recordedintra-arterially.3-3
Our study was undertaken to evaluate the accu-racy of FINAPRES in reproducing intra-arterial bloodpressure values in a large number of subjects. Becausethe potential importance of this method resides in itsability to provide noninvasively a beat-to-beat esti-mate of rapid blood pressure changes, we comparedFINAPRES and intra-arterial blood pressures notonly in resting conditions but also during a numberof laboratory maneuvers that caused rapid andpronounced blood pressure rises and falls. Thecomparison included the standard deviation of rel-atively prolonged blood pressure tracings to assessthe ability of FINAPRES to measure an importantfeature of blood pressure, variability.
by guest on June 9, 2018http://hyper.ahajournals.org/
Dow
nloaded from

648 Hypertension Vol 13, No 6, Part 1, June 1989
Subjects and MethodsSubjects
The study was performed 1 week after admissionto hospital in 17 subjects with uncomplicated essen-tial hypertension and in eight normotensive subjectsaffected by noncardiovascular diseases. In eachsubject blood pressure was recorded with theFINAPRES device, and the data were comparedwith those simultaneously recorded from the radialartery of the same or the contralateral side. How-ever, because the quality of the finger pressurerecording was unsatisfactory in one hypertensivepatient, only data collected in 24 subjects (19 men,five women; mean age 48.2 years, range 25-64years) were processed. The subjects were given nocardiovascular drugs at the time of the study, andhypertensive patients had discontinued their ther-apy at least 15 days before the study period. Theprotocol of the study was approved by the ethicalcommittee of our institute, and each subject enteredthe study only after giving informed consent.
Hemodynamic RecordingsThe intra-arterial blood pressure signal was ob-
tained by a catheter (11 cm length, 1.3 mm i.d.) thatwas introduced percutaneously into a radial arteryafter local anesthesia with 2% lidocaine. The cathe-ter was connected by a rigid polyethylene tube to aStatham transducer (P23ID, Oxnard, California), andsignal was recorded on a Grass polygraph (GrassEquipment, Quincy, Massachusetts) to allow calcu-lation of beat-to-beat systolic blood pressure, dia-stolic blood pressure, and mean blood pressure (whichwas obtained by electronic damping of the pulsatiletracing). The intra-arterial signal was also sent to aRacal recorder (Racal Recorders Limited, Hythe,Southampton, UK) and stored on magnetic tape.
The finger pressure recording was obtained bythe Model n.5 prototype of the FINAPRES device(TNO, Academic Medical Centre, Amsterdam, TheNetherlands), a version of which is commerciallyavailable as Ohmeda 2300 FINAPRES blood pres-sure monitor (Ohmeda Monitoring Systems, Engle-wood, Colorado).
The FINAPRES method has been described indetail elsewhere.3-6 Briefly, the instrument operatesthrough a small finger cuff equipped with an infraredphotoplethysmograph to measure the arterial bloodvolume under the inflatable cuff. The cuff is con-nected with a front-end box wrapped to the patient'shand. The box contains a fast proportional pneu-matic valve, connected with a source of com-pressed air, an electropneumatic transducer, andthe electronics for the plethysmograph. The fingerarterial blood volume, as assessed by the plethys-mograph, is clamped at a set point value correspond-ing to two thirds of the maximum arterial volume7
by adjustment of the cuff pressure in parallel withintra-arterial pressure through a fast-reacting elec-tropneumatic servo system, with a bandwidth of at
least 40 Hz.2 The volume-clamp set point is peri-odically adjusted to keep the finger arteries fullyunloaded at zero transmural pressure46 and to allowthe cuff pressure to continuously reflect intra-arterial pressure. In 19 subjects the cuff was wrappedaround the middle or ring finger of the hand ipsUat-eral to that from which the intra-arterial signal wasderived. In the remaining five subjects it waswrapped on the hand opposite to that instrumentedwith the intra-arterial catheter because ipsilateralmeasurements were technically unfeasable. In thesesubjects the between-arm difference in sphygmo-manometric blood pressure, as assessed three timesby two observers who switched both arms andcuffs, was always less than 5 mm Hg.
Throughout the study, the finger equipped withthe FINAPRES cuff was kept at the same level asthe transducer to which the intra-arterial bloodpressure signal was directed.
ProtocolThe study started 15 minutes after insertion of the
radial artery catheter and proper positioning of thefinger cuff. First, during a 30-minute period whenthe subjects were lying quietly, blood pressure wasmeasured by the two methods (resting conditions);then it was measured before and during perfor-mance of tests that raised blood pressure either bydirectly induced vasoconstriction (intravenous bolusof 100 fig phenylephrine) or by an increase insympathetic drive induced by 1) stimulation ofskeletal muscle receptors by a hand-grip exerciseperformed at 40% of subject's maximal strength for90 seconds with the hand contralateral to the oneinstrumented with the blood pressure monitoringdevices, 2) stimulation of skin receptors by immer-sion of the noninstrumented hand in ice water for 60seconds, and 3) trigeminal and chemoreceptor stim-ulation by immersion of subject's face into ice waterfor 15-20 seconds. The blood pressure signalobtained by the two methods was further assessedduring 1) the mechanical and reflex changes inblood pressure that accompanied a Valsalva maneu-ver that was performed by blowing into a plastictube connected to a mercury manometer to raise themercury column by 40 mm Hg for 20 seconds, 2)the fall in blood pressure accompanying the vasodi-latation induced by an intravenous bolus of 100 fignitroglycerine, and 3) the rise and fall in bloodpressure induced by deactivating or stimulatingcarotid baroreceptors through 2-minute applica-tions of three positive and three negative pressuresin a neck chamber within the range of ±40 mm Hg.These tests were complemented by the assessmentperformed before and during a 20-minute deactiva-tion of cardiopulmonary receptors (application of-40 mm Hg pressure to the lower body) and a20-minute stimulation of cardiopulmonary recep-tors (passive elevation of the legs to 60°) that causedperipheral vasoconstriction and vasodilatation,
by guest on June 9, 2018http://hyper.ahajournals.org/
Dow
nloaded from

Parati et al Finger Blood Pressure Monitoring 649
RESTING VALUES ( n = 2 4 )
220
| 200
UJ 180cc
« 1 6 0ua.°- 140DCUJ
O 120zLL.
1OO
120-
110-
100
SO
8 0
70
60
50
D B P
•V
/
r -093• = 5.43b- 0 969
100 120 140 160 180 200 220INTRA- ARTERIAL
SO 60PRESSURE
70 80ImmHg)
90 100 110 120
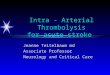
FIGURE 1. Plots of systolic blood pres-sure (SBP) and diastolic blood pressure(DBP) values obtained by simultaneousintra-arterial and finger blood pressurerecording over a 30-minute resting period.Data are shown as individual averages of24 subjects. Diagonal lines represent linesof identity between pairs of values pro-vided by two recording systems. Numberson right of each panel refer to the corre-lation coefficient (r), the regression coef-ficient (b), and the intercept (a) of thelinear regressions between the two sets ofdata.
respectively, in the absence of marked blood pres-sure changes.
All tests were applied randomly; each was per-formed twice and spaced from the preceding one byat least 15 minutes. Except for diving, all tests weregiven to at least 9-10 subjects to have a sufficientlylarge data base for comparison.
Data AnalysisResting conditions. The intra-arterial blood pres-
sure tracing obtained in the resting condition wasanalyzed by manual calculation of the average sys-tolic and diastolic values of 20-second periods,which were regularly taken at 3-minute intervals toobtain mean values for the 30-minute recording.Furthermore, the blood pressure tracing stored onmagnetic tape was digitized on 12 bits by a com-puter (Digital PDP 11/23), which sampled the signalat 165 Hz. The digitized signal was stored on amagnetic disk and edited by means of an interactiveprogram to eliminate possible morphological arti-facts (e.g., arrhythmias or reduced amplitude of the
intra-arterial tracing). Average mean blood pressurevalues of each minute recording were calculated,and the corresponding standard deviations werefurther averaged to obtain a measure of the ten-dency of blood pressure to vary within very shorttime intervals.89 The finger blood pressure signalwas edited and analyzed in an identical fashion.
Responses to laboratory tests. The changes inintra-arterial blood pressure induced by the varioustests were calculated by averaging systolic anddiastolic blood pressure values during a 20-secondperiod taken 1 minute before the test and comparingthem with the average blood pressure values mea-sured in the final 10 seconds of the test (hand-grip,cold pressor test, diving) or at regular 3-minuteintervals during the test (lower body negative pres-sure and passive leg raising). Likewise, the intra-arterial blood pressure changes induced by theValsalva maneuver were calculated by comparisonof the baseline 20-second values with the peakincrease, decrease, and increase in blood pressureobserved after the beginning, before the end, and in
+ 20
+20 1.+ 10H
°I _
SBP
120 140 160 180 200
DBP
-V-i-
30 50 70 90 110INTRA-ARTERIAL PRESSURE (mmHf)
130
220
I-BSD
— 2SD
150
FIGURE 2. Average discrepancies (A)between finger and intra-arterial systolic(SBP) and diastolic blood pressure (DBP).Data refer to averages of a 30-minuteresting period and are shown as individualdifferences between finger pressure andintra-arterial pressure. The latter is taken asthe zero reference value. Dashed lines in-dicate the average discrepancies in the groupas a whole (n=24) and the + or - 2 SD.
by guest on June 9, 2018http://hyper.ahajournals.org/
Dow
nloaded from

650 Hypertension Vol 13, No 6, Part 1, June 1989
INTRA - ARTERIAL
MAP"
HG
ABP
FIN A- PRES
MAP-
ABP
HR
. i L i , i I I I r I I ) | | I I I I I I I : i I I
• I •
200
mmHg
0
200
mm
Hg
2 0 0
•V"
FIGURE 3. Original tracings ofintra-arterial (upper panels) andfinger blood pressure (lower pan-els) from one subject during per-formance of cold pressor test(CPT) and hand-grip exercise(HG). MAP, mean arterial pres-sure; ABP, pulsatile arterial pres-sure; HR, heart rate.
io«ec
the rebound phase, respectively, after the termina-tion of the Valsalva maneuver (phase 1, 2, and 3).Finally, the changes in intra-arterial blood pressureinduced by intravenous injections of phenylephrineand nitroglycerine were calculated by comparisonof the average systolic and diastolic blood pressureof the five beats before injection and the peak bloodpressure change induced by the injection. The finger
blood pressure signal was analyzed in an identicalfashion. Data obtained during two performances ofeach test were averaged.
The intra-arterial blood pressure increases andreductions induced by phenylephrine and nitroglyc-erine were also used to stimulate and deactivatearterial baroreceptors and to evoke reflex bradycar-dia and tachycardia, respectively. Heart rate was
BPmfflHg
200-i
180
160-
140
MO
100
80
C HO
n-13
C CPT
n:14
I—I
C LBNP
S—-5
• — . INTRA-ARTERIAL
o- -o FINGER
FIGURE 4. Systolic (S) and diastolic (D)blood pressure values in control condi-tions (C) and during hand-grip (HG) exer-cise, cold pressor test (CPT), applicationof lower body negative pressure (LBNP),passive leg raising (LR), intravenous injec-tion of phenylephrine (PHE), and intrave-nous injection of trinitroglycerine (TNG).Mean±SEM from individual intra-arterialand finger blood pressure values areshown, n, number of subjects in which agiven test was performed.
by guest on June 9, 2018http://hyper.ahajournals.org/
Dow
nloaded from

Parati et al Finger Blood Pressure Monitoring
TABLE 1. Average Discrepancies Between Finger and Intra-arterial Blood Pressure Responses to Laboratory Tests
651
Laboratory tests
Hand grip(/i =13)
Cold pressor(n=14)
Lower body negative pressure(-40mmHg, i = l l )
Leg raising(n=12)
Phenylephrine(100/igi.v.,/!=14)
Trinitroglycerine(100/igi.v.,i=14)
A (nunRegardless
SBP
3.5±3.6
4.6±4.1
4.1±3.7
4.1±3.0
3.4±2.0
3.8±1.1
Hg)the sign
DBP
1.3+1.5
2.1±1.2
3.5±3.2
2.4±1.8
2.3+2.1
2.5±1.8
A (mm Hg)Considering the
SBP
+ 2.5±4.4
+4.3+4.51
-3.1±4.6*
+ 3.8±3.4t
+0.9±3.9
+ 1.4±3.8
sign
DBP
+ 1.2±1.6*
+0.1±2.5
+ 1.7±4.5
+0.5±3.0
+ 1.9±2.5*
+ 1.4+2.8
Values are mean±SD. A, discrepancies in responses; SBP, systolic blood pressure; DBP, diastolic bloodpressure.
*p<0.05; tp<0.01 between finger and intra-arterial blood pressure changes induced by various laboratorymaneuvers.
measured by an electrocardiogram (ECG), and thebaroreceptor reflex sensitivity was estimated as theslope of the linear regression relating changes in RRinterval with rises and falls in systolic bloodpressure.l01 • Another measure of baroreceptor reflexsensitivity was obtained by the ratio between thechanges in tissue pressure outside the carotid sinuses,induced by neck chamber pressure changes, and theresulting alterations in mean arterial pressure. Datafrom the three positive or the three negative neckpressures were averaged.12-14 The same analysis wasperformed for the finger blood pressure tracing.
Comparison Between Finger and Intra-arterialBlood Pressure Data
Means and variabilities obtained in the restingcondition by intra-arterial and finger blood pressurerecording were compared with use of linear regres-sion analysis between the two sets of data; a perfectcorrespondence was indicated by an intercept equalto zero and a regression coefficient equal to one.15
In addition, the average discrepancies (mean±SD)between finger and intra-arterial values were calcu-lated for individual subjects and for the group as awhole.
Linear regression analysis was also used to com-pare baroreceptor reflex sensitivities, whereas aver-age discrepancies (±SD) were employed to evalu-ate the correspondence between the responses tothe laboratory tests obtained intra-arterially andthose obtained by the finger pressure method. Thestatistical significance of the differences was esti-mated by Student's paired t test.16
Throughout the study a p<0.05 was taken as theminima] level of statistical significance.
ResultsResting Condition
As shown in Figure 1, the average systolic anddiastolic blood pressure obtained at rest by the
FINAPRES device and the intra-arterial cathetershowed a relatively narrow scattering around theidentity line; the linear regression analysis betweenthe two sets of data showed correlation and regres-sion coefficients close to optimal values. The indi-vidual average paired differences between fingerand intra-arterial blood pressures ranged from —13.4to +6.7 mm Hg for systolic and from -14.6 to +8.7mm Hg for diastolic blood pressure; the mean groupdiscrepancies (±SD) were + 1.2±5.4 mm Hg and+2.9±5.0 mm Hg, respectively (Figure 2).
Responses to Laboratory TestsAs exemplified in Figure 3, the marked beat-
to-beat changes in intra-arterial blood pressureinduced by laboratory tests were reproduced by theFINAPRES device in a qualitatively similar fash-ion. The systolic and diastolic blood pressuresmeasured intra-arterially before and during eachtest were on average similar to those measurednoninvasively by finger pressure recording for thetests that induced a pressor or a depressor responseas well as for those that caused vasomotor changeswithout major variations in blood pressure (Figure4). The average between-method discrepancy in theevaluation of the blood pressure changes was nevergreater than 4.3 mm Hg or 1.9 mm Hg for systolicand diastolic pressure, respectively. The correspond-ing standard deviations were always less than ±4.6mm Hg and ±4.5 mm Hg (Table 1) indicating thatthe discrepancies were also small in individualsubjects. The differences were only slightly higherwhen individual data were averaged regardless thesign to avoid negative errors to compensate for" thepositive ones (Table 1).
The fast and marked intra-arterial blood pressurerises that characterized the diving test were alsoclosely reproduced by the FINAPRES method,both with regard to their time course (Figure 5) andto their absolute changes. The average difference
by guest on June 9, 2018http://hyper.ahajournals.org/
Dow
nloaded from

652 Hypertension Vol 13, No 6, Part 1, June 1989
DIVING REFLEXFIN • A • PRES
TABLE 2. Blood Pressure Response to Diving Test
MAP
ABP
INTRA - ARTERIAL
MAP
ABP
r200-mm
-Hg
-50
r 250
mmHg
L50
L60
—t—I—i—1—i—1—1—1—
10sec
FIGURE 5. Original tracing of intra-arterial (lower panel)and finger blood pressure (upper panel) from one subjectduring performance of diving test. MAP, mean arterialpressure; ABP, pulsatile arterial pressure; HR, heart rate.
(computed with or without the sign) was nevergreater than 5.4 mm Hg with a standard deviationnever greater than ±2.7 mm Hg (Table 2). This wasusually the case also for the fast and marked bloodpressure increases and decreases that occurred dur-ing the Valsalva maneuver (Figure 6).
Blood Pressure Variability and BaroreceptorReflex Sensitivity
The standard deviation of mean arterial pressureobtained by the beat-to-beat analysis of the 30-minute resting period was almost identical when
Change inuitra-arterial
pressure(mm Hg)
Change infinger
pressure(mm Hg)
A (mm Hg)Regardless
the sign
A (mm Hg)Considering
the sign
SBP +56.9±9.1DBP +27.3+4.9MAP +33.0±6.7
+57.5±11.0+ 25.3±4.6+ 36.5±7.9
5.4±1.33.3+0.94.7+1.7
+0.6±2.7-2.0±1.5+3.5±2.2
Values are mean±SEM. A, mean difference between fingerand intra-arterial blood pressure changes induced by diving test;SBP, systolic blood pressure; DBP, diastolic blood pressure;MAP, mean arterial blood pressure. «=6 subjects.
measured intra-arterially and by the FINAPRESmethod (3.7 mm Hg and 3.8 mm Hg). Even whenaveraged regardless of the sign, the differencebetween the two methods amounted to only 0.29mm Hg, and the corresponding standard deviationwas only 0.28 mm Hg. This close correspondencewas confirmed by the high correlation and regres-sion coefficients between the two sets of values(Figure 7).
As shown in Figure 8, the sensitivity of thebaroreceptor-heart rate reflex, as assessed by nitro-glycerine injection, was very similar when the hypo-tension induced by the drug was estimated byintra-arterial or by finger pressure recording. Thetwo methods also provided good estimates of thesensitivity of the baroreceptor reflex, as assessedby phenylephrine injection and positive neck cham-ber pressure application, although in both instancesthe between-method differences were greater thanthose observed for nitroglycerine injection. On theother hand, when the baroreceptor reflex sensitivitywas measured by negative neck chamber pressureapplication, the estimate provided by finger pres-sure recording was less accurate.
DiscussionOur study confirms that measurements of finger
blood pressure by the FINAPRES method provideresting systolic and diastolic blood pressures similarto those existing in the radial artery. It also demon-strates, in a large number of subjects, that thissimilarity extends to the measurements of the fastand marked blood pressure increases and decreasesthat can be induced by laboratory maneuvers.
The similarity of the blood pressure valuesobtained by finger pressure and by intra-arterialrecording in resting condition is documented by thestrict linear relation between the systolic and dia-stolic blood pressures that were measured by thetwo methods. It is also documented by the fact that,in the group as a whole, finger and intra-arterialblood pressures differed by no more than 2 or 3mm Hg and the standard deviations of the averagedifferences were approximately 5 mm Hg. Thesefigures are largely within the requirements for newblood pressure-measuring devices of the Associa-tion for the Advancement of Medical Instrumenta-tion,17 which consider the difference between non-
by guest on June 9, 2018http://hyper.ahajournals.org/
Dow
nloaded from

mmHg
200
1 8 0
160
140
120
| i oo - |_ JCD
80
60
40-Control 1»' 2 n d
• • Intra-Arterlal
o - -o Finger
Parati et al Finger Blood Pressure Monitoring 653
VALSALVA MANOEUVRE (n=17)
CONSIDERING THE SIGN
FIGURE 6. Intra-arterial andfinger systolic (SBP) and diastolic(DBP) blood pressure valuesrecorded in control condition andduring phase 1,2, and 3 of Val-salva maneuver (see Methods).Data are shown as mean±SEMfrom 17 subjects. Left panel, abso-lute values and right panel, aver-age discrepancies computed con-sidering or not considering thesign.
3 r d Phase
invasive and intra-arterial measurements to beacceptable when less than or equal to 5±8 mm Hg(mean±SD). However, the most important result ofour study is that, in agreement with recent obser-vations made during the Valsalva maneuver,18 thecorrespondence between finger and intra-arterialblood pressure recording is good not only in theresting condition but also when blood pressureundergoes fast, marked, and variable changes. Thiscorrespondence makes this approach superior tomanual or automatic sphygmomanometric measure-ments, which lose accuracy when not performed at
mmHg
MAP VARIABILITY(SD,n=14)
0 2 4 6 mmHg
INTRA-ARTERIAL PRESSURE
FIGURE 7. Plot of mean arterial pressure (MAP) stan-dard deviation (SD) as assessed by separate beat-to-beatanalysis of finger and intra-arterial blood pressure trac-ings over a 30-minute resting period. Data from 14subjects, n, number of subjects; r is correlation coeffi-cient of regression.
0 5 10 15 20 25-PI/-SBP [miic/mmHg)
0 02 04-MAP -NTP Ir
OS 0 8 1.0imHg mmHgl
0 0 2 0 4 0.6 0.8 1.0• MAP'+NTP ImmHg/mmHg)
INTRA-ARTERIAL PRESSURE
FIGURE 8. Baroreceptor reflex sensitivity as estimatedby considering finger pressure and intra-arterial bloodpressure. Sensitivity of arterial baroreceptor control ofheart rate was assessed by slope of regression linebetween changes in systolic blood pressure induced byinjection of phenylephrine (PHE) or trinitroglycerine(TNG) and corresponding lengthening or shortening inpulse interval (PI). Sensitivity of carotid baroreceptorcontrol of blood pressure was assessed by ratio betweenchanges in neck tissue pressure (NTP) and resultingchanges in mean arterial pressure (MAP). Thin linesrepresent identity lines between paired values obtainedby two methods. Thick lines represent regression linesbetween same values, n, number of subjects included ineach analysis; r is correlation coefficient of variousregressions.
by guest on June 9, 2018http://hyper.ahajournals.org/
Dow
nloaded from

654 Hypertension Vol 13, No 6, Part 1, June 1989
rest.19-21 This superiority is further emphasized bythe fact that finger pressure recording can alsofollow, on a beat-to-beat basis, fast blood pressurechanges, thereby providing a description of the timecourse of these changes; this is the case for bloodpressure rises and systemic vasoconstrictions andfor blood pressure falls and systemic vasodilata-tions, which indicates that alterations in blood pres-sure gradient and peripheral artery tone do notimpair the ability of this peripheral instrument tosense intra-arterial blood pressure.
Although similar, the blood pressures obtainedby finger pressure and intra-arterial recording werenot superimposable. For example, the resting bloodpressure values were often slightly greater whenmeasured by finger pressure recording than by theintra-arterial catheter at the radial artery level.Furthermore, the overall small discrepanciesbetween the two sets of values showed an appre-ciable between-subject variability. Finally, in rareinstances, an acceptable finger blood pressure record-ing could not be obtained (see Subjects and Meth-ods). These problems probably originate from thefact that both intra-arterial blood pressure measure-ments and the measurements provided by theFINAPRES device may not necessarily be 100%accurate in all subjects.341722-24 It is possible,however, that the somewhat variable discrepancybetween the data provided by the two methods alsodepended on the different site of their blood pres-sure detection (i.e., on the fact that noninvasiveblood pressure was sensed at a more distal site thaninvasive blood pressure). This means that the lossof energy occurring in the arterial tree and the pulsewave reflection phenomenon may have affected thetwo pressures to a different degree, their influencevarying as a function of the arterial structural andfunctional status.22323-27 This raises the possibilitythat blood pressures provided by the FINAPRESmethod may be even more accurate than theyappear in this study. Two other results of our studydeserve to be mentioned. First, in virtue of itsability to accurately measure beat-to-beat restingblood pressure, finger pressure recording can pro-vide a precise measure of the standard deviation ofall blood pressure values occurring over a pro-longed monitoring period, thereby offering a reli-able index of blood pressure variability, particularlywhen changes in mean arterial pressure are consid-ered. This is important for basic and clinical studiesbecause blood pressure variability may reflect car-diovascular regulation in daily life.8928-33 It mayalso be a factor contributing to the adverse conse-quences of hypertension on its target organs.34-33
Second, the ability of the finger pressure deviceto accurately measure blood pressure changesinduced by vasoactive drug injection and the neckchamber device allows proper evaluation of thesensitivity of the baroreceptor control of the heartand peripheral circulation. This makes baroreceptorreflex functions testable in subjects in whom intra-
arterial blood pressure measurements cannot beeasily carried out (children, pregnant women, orseverely ill patients), greatly enhancing the possi-bility to obtain information on reflex modulation ofthe cardiovascular system in health and disease.
In conclusion, our data demonstrate that fingerblood pressure recording by the FINAPRES methodprovides an accurate estimate of the average radialblood pressure of a population and that it alsoallows a reasonably good estimate of intra-arterialblood pressure in individual subjects. The timecourse and the magnitude of the blood pressurechanges brought about by a variety of stimuli, thetendency of blood pressure to vary within a pro-longed time interval, and the relation between bloodpressure and baroreceptor control of circulation arealso reliably assessed by noninvasive finger pres-sure recording.
This reliability makes the finger blood pressurerecording approach valuable for laboratory studies,which can then collect the extensive informationprovided by continuous blood pressure monitoringwithout the risks and the inconveniences of intra-arterial catheters.36
AcknowledgmentsWe thank Dr. Karel Wesseling (T.N.O., Acade-
misch Medisch Centrum, Amsterdam, The Nether-lands) for having lent the FINAPRES device to usand the Commission of the European Communities(CEC), Concerted Action on Quantification ofParameters for the Study of Breakdown in HumanAdaptation, for providing travel funds. We alsothank Carla Zanchetti and Stefano Omboni for draw-ing the illustrations, Emanuela Mutti for typing themanuscript, and Riccardo Sarri for photography.
References1. Pefiaz J: Photoelectric measurement of blood pressure,
volume and flow in the finger. Digest of the InternationalConference on Medicine and Biological Engineering. Dres-den, Conference Committee of the 10th International Con-ference on Medicine and Biological Engineering, 104, 1973
2. Wesseling KH, De Wit B, Settels JJ, Klaver WH: On theindirect registration of finger blood pressure after Pefiaz.Funkt Biol Med 1982;l:245-250
3. Kurki T, Smith NT, Head N, Dec-Silver H, Quinn A:Noninvasive continuous blood pressure measurement fromthe finger: Optimal measurement conditions and factorsaffecting reliability. J Clin Monit 19873:6-13
4. Smith NT, Wesseling KW, De Wit B: Evaluation of twoprototype devices producing noninvasive pulsatile calibratedblood pressure from a finger. J Clin Monit 1985; 1:17-29
5. Wesseling KH, Settels JJ, Van Der Hoeven GMA, NrjboerJA, Butijn MWT, Dorlas JC: Effects of peripheral vasocon-striction on the measurement of blood pressure in a finger.Cardiovasc Res 1985;19:139-145
6. Wesseling KH, Settels JJ, De Wit B: The measurement ofcontinuous finger arterial pressure noninvasively in station-ary subjects, in Schmidt TH, Dembroski TM, Bluemchen G(eds): Biological and Psychological Factors in Cardiovascu-lar Disease. Berlin, Springer-Verlag, 1986, pp 355-375
7. Langewouters GJ, Zwart A, Busse R, Wesseling KH: Pres-sure-diameter relationship of segments of human fingerarteries. Clin Phys Physiol Meas 1986;7:43-55
by guest on June 9, 2018http://hyper.ahajournals.org/
Dow
nloaded from

Parati et al Finger Blood Pressure Monitoring 655
8. Mancia G, Ferrari A, Gregorini L, Parati G, Pomidossi G,Bertinieri G, Grassi G, Di Rienzo M, Pedotti A, Zanchetti A:Blood pressure and heart rate variabilities in normotensiveand hypertensive human beings. Circ Res 1983^3:96-104
9. Mancia G, Zanchetti A: Blood pressure variability, inZanchetti A, Tarazi RC (eds): Handbook of Hypertension.Pathophysiology of Hypertension: Cardiovascular Aspects.Amsterdam, Elsevier, vol 7, 1986, pp 125-152
10. Mancia G, Mark AL: Arterial baroreflexes in humans, inShepherd JT, Abboud FM (eds): Handbook of Physiology,Section 2. The Cardiovascular System IV. Bethesda, Md,American Physiological Society, 1983, pp 755-793
11. Smyth HS, Sleight P, Pickering GW: Reflex regulation ofarterial pressure during sleep in man. A quantitative methodof assessing baroreflex sensitivity. Circ Res 1969^4:109-121
12. Ludbrook J, Mancia G, Ferrari A, Zanchetti A: The variable-pressure neck chamber method for studying the carotidbaroreflex in man. Clin Sci Mol Med 1977,53:165-172
13. Mancia G, Ferrari A, Gregorini L, Valentini R, Ludbrook J,Zanchetti A: Circulatory reflexes from carotid and extra-carotid baroreceptor areas in man. CircRes 1977 ;41:309-316
14. Mancia G, Ferrari A, Gregorini L, Parati G, Ferrari MC,Pomidossi G, Zanchetti A: Control of blood pressure bycarotid sinus baroreceptors in human beings. Am J Cardiol1979;44:895-902
15. Draper N, Smith H: Applied Regression Analysis, ed 2. NewYork, John Wiley and Sons, Inc, 1981
16. SnedecorGW, Cochran WG: Statistical Methods. Ames, la,The Iowa State University Press, 1982
17. A.A.M.I: Standard for electronic or automated sphygmoma-nometers, in A.A.M.I. Standards. Arlington, VA, Associa-tion for the Advancement of Medical Instrumentation, 1980,PP2<M2
18. Imholz BPM, Van Montfrans GA, Settels JJ, Van DerHoeven GMA, Karemaker JM, Wieling W: Continuousnon-invasive blood pressure monitoring: Reliability ofFinapres device during the Valsalva manoevre. CardiovascRes 1988;22:390-397
19. Casadei R, Parati G, Pomidossi G, Groppelli A, Trazzi S,Mancia G: 24-hour blood pressure monitoring: Evaluation ofSpacelabs 5300 Monitor by comparison with intra-arterialblood pressure recording in ambulant subjects. J Hypertens1988;6:797-803
20. Gould BA, Homung MB, Cashman PMM, Altman D, RafteryEB: An evaluation of the Avionics Pressurometer HI 1978 athome and in hospital. Clin Cardiol 1986;9:335-343
21. Mancia G: Methods for assessing blood pressure values inhumans. Hypertension 1983;5(suppl 3):S5-S13
22. Gardner RM: Direct blood pressure measurement. Dynamicresponse requirements. Anesthesiol 1981:54:227-236
23. Molhoek GP, Wcsseling KH, Settels JJ, Van VollenhovenE, Weeda HWH, De Wit B, Arntzenius AC: Evaluation ofthe Penaz servo-plethysmomanometer for the continuous,non-invasive measurement of finger blood pressure. BasicRes Cardiol 1984;79:598-609
24. Stott FD: Sources of error in direct and indirect bloodpressure measurement, in Marches! C (ed): AmbulatoryMonitoring. Cardiovascular System and Allied Application.The Hague, Martinus Nyhoff, 1984, pp 17-25
25. Kroeker EJ, Wood EH: Comparison of simultaneouslyrecorded central and peripheral arterial pressure pulsesduring rest, exercise and tilted position in man. Circ Res1955;3:623-632
26. O'Rourke MF, Blazek JW, Morreels CL, Krovets LJ: Pres-sure wave transmission along the human aorta. Changeswith age and in arterial degenerative disease. Circ Res 1968;23:567-579
27. Rushmer RF: Structure and Function of the CardiovascularSystem, ed 2. Philadelphia, WB Saunders Co, 1976
28. Akselrod S, Gordon D, Mawded JB, Snidman DC, ShannonDC, Cohen RJ: Hemodynamic regulation: Investigation byspectral analysis. Am J Physiol 1985;249(//eart Circ Physiol18):H867-H875
29. De Boer RW, Karemaker JM, Strakee J: Hemodynamicfluctuations and baroreflex sensitivity in humans: A beat-to-beat model. Am J Physiol 1987;253(//<?arf Circ Physiol22):680-689
30. Parati G, Pomidossi G, Mancia G: Neural mechanisms inhuman cardiovascular regulation, in Schmidt TH, Dem-broski TM, BlOmchen G (eds): Biological and PsychologicalFactors in Cardiovascular Disease. Berlin/Heidelberg,Springer Verlag, 1986, pp 379-389
31. Mancia G, Parati G, Pomidossi G, Casadei R, Di Rienzo M,Zanchetti A: Arterial baroreflexes and blood pressure andheart rate variabilities in humans. Hypertension 1986;8:147-153
32. Pagani M, Lombardi F, Guzzetti S, Rimoldi O, Furlan R,Pizzinelli P, Sandrone G, Malfatto G, DcH'Orto S, PiccalugaE, Turiel M, BaseUi G, Cerutti S, Malliani A: Power spectralanalysis of heart rate and arterial pressure variabilities as amarker of sympatho-vagal interaction in man and consciousdog. Circ Res 1986^9:178-193
33. Parati G, Di Rienzo M, Bertinieri G, Pomidossi G, CasadeiR, Groppelli A, Zanchetti A, Mancia G: Evaluation of thebaroreceptor-heart rate reflex by 24-hour intra-arterial bloodpressure monitoring in humans. Hypertension 1988;12:214-222
34. Parati G, Pomidossi G, Albini F, Malaspina D, Mancia G:Relationship of 24-hour blood pressure mean and variabilityto severity of target-organ damage in hypertension. / Hyper-tens 1987^:93-98
35. Pessina AC, Palatini P, Sperti G, Cardone L, Libardoni M,Mos L, Mormino P, Di Marco A, Dal Palu' C: Evaluation ofhypertension and related target organ damage by averageday-time blood pressure. Clin Exp Hypertens A 1985;7:267-271
36. Murray IP: Complications of invasive monitoring. MedInstrument 1981;15:85-89
KEY WORDS • finger blood pressure recording • bloodpressure • baroreceptors • intra-arterial blood pressurerecording
by guest on June 9, 2018http://hyper.ahajournals.org/
Dow
nloaded from

In Support ofOfficial Journals of the American Heart Association
CirculationJohn Ross Jr., M.D., EditorISSN: 0009-7322Devoted to clinical research and advances inthe cardiovascular field. Original articles of cardio-vascular clinical and laboratory investigations.Clinical Progress Series, Research AdvancesSeries, Editorials, Editorial Comments, Letters tothe Editor, AHA News. Monthly.
Circulation ResearchHarry A. Fbzzard, M.D., EditorISSN: 0009-7330Concerned with basic cardiovascular research.Original articles and editorials for clinicians in-terested in basic science and for research workersin anatomy, biology, biochemistry, biophysics, mi-crobiology, physiology, pharmacology, and path-ology, as well as experimental medicine. BriefReviews, Brief Communications, Letters to theEditor, AHA News. Monthly.
HypertensionAllyn L. Mark, M.D., EditorISSN: 0194-911XPublishes reports of clinical and laboratory inves-tigations in hypertension. Designed for clinicians,clinical investigators, laboratory scientists. OriginalInvestigations, Brief Reviews, Symposia, CaseReports, AHA News. Monthly.
StrokeA Journal of Cerebral Circulation
Oscar M. Reinmuth, M.D., EditorISSN: 0039-2499Of interest to the practicing physician — especiallythe internist, cardiologist and neurologist — aswell as teacher, clinical investigator, laboratoryscientist, and student. Articles deal with preven-tion, diagnosis, treatment and rehabilitation.Progress Reviews, Original Contributions, ShortCommunications, Abstracts of Literature, Com-ments, Opinions, and Reviews, Letters to the Edi-tor, AHA News. Monthly.
ArteriosclerosisA Journal of Vascular Biology and Thrombosis
Edwin L. Bierman, M.D., EditorISSN: 0276-5047Includes original research papers and state-of-the-art reviews from a variety of disciplines bearingon the biology, prevention, and impact of vasculardiseases relating to arteriosclerosis. Designed forphysicians and investigators. Original Contributions,Editorials, Reviews, Meeting Summaries, SpecialReports, AHA News, Bimonthly.
Recurring Bibliography of HypertensionISSN: 0090-1326Published by the AHA in cooperation with the Na-tional Library of Medicine. Provides a rapid surveyof current published developments in the field ofhypertension. Bimonthly.
American Heart AssociationNational CenterScientific Publications7320 Greenville AvenueDallas, Texas 75231
For rate and order information:
Japan, contact:
Nankodo Co., Ltd.42-6 Hongo 3-chomeBunkyo-ku, Tokyo 113
JAPAN
Europe, contact:
Harcourt-Brace-JovanovichFoots Cray High StreetSidcupKent DA14 5HR ENGLAND
by guest on June 9, 2018http://hyper.ahajournals.org/
Dow
nloaded from

G Parati, R Casadei, A Groppelli, M Di Rienzo and G Mancialaboratory testing.
Comparison of finger and intra-arterial blood pressure monitoring at rest and during
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 1989 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/01.HYP.13.6.647
1989;13:647-655Hypertension.
http://hyper.ahajournals.org/content/13/6_Pt_1/647World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOffice. Once the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertension Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 9, 2018http://hyper.ahajournals.org/
Dow
nloaded from