Embed Size (px)
Citation preview

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 20111
International Health Regulations Coordination Department
Review of activities 2011Core Capacity Development• Monitoring• National Legislation• NFP Communications and Coordination• Surveillance and Response• Preparedness• Risk Communication• Human Resources• Laboratory• Points of Entry
WHO Global IHR CommitmentsFuture DirectionsAnnexes • IHR Publications and Reference Tools• Collaborating Institutions• Financial Summary
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 20112 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 20113
International Health Regulations Coordination Department
Activity Report 2◊11Table of contents
P 4 Acronyms P 5 Foreword P 7 Introduction
Review of activities 2011
P 11 Core Capacity Development P 13 •Monitoring P 17 •NationalLegislation P 19 •NFPCommunications andCoordination P 21 •SurveillanceandResponse P 25 •Preparedness P 29 •RiskCommunication P 33 •HumanResources P 37 •Laboratory P 41 •PointsofEntry
P 45 WHO Global IHR Commitments
P 51 Future Directions P 55 Annexes P 57 •IHRPublications andReferenceTools P 61 •CollaboratingInstitutions P 64 •FinancialSummary
The designations employed and the presentation of the materi-al in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization con-cerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommend-ed by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
WHO/HSE/GCR/LYO/2012.3
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publi-cation. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
© World Health Organization 2012All rights reserved.
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 20112

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 20114 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 20115
ForewordAcronyms
Doingourworkbettercouldwellbedescribedasthedriving forcebehindWHOover thepastyear.ThereformoftheOrganization,whichhasinvolvedanex-tensive and sometimes painful analysis of its func-tioning, led to a substantive restructuring designedtomakeWHObetterabletorespondtopublichealthneedsinallcountriesaroundtheworld.
FortheHealthSecurityandEnvironmentcluster(HSE),andinparticularasregardsthe revisedInter-national Health Regulations (2005), the process ofevaluationbeganinApril2010withtheexternalreviewof the functioning of the IHR in the context of pan-demicH1N12009.TheworkoftheReviewCommitteeconcludedinMay2011withthereportofitsfindingsandrecommendationspresentedtotheWorldHealthAssemblybyitsChair,ProfessorHarveyFineberg.
ThemainfindingsoftheCommitteewerethattheIHRhelpedbetterpreparetheworldtocopewithpublichealthemergencies,thatWHOperformedwellinmanyways during the pandemic, confronted systemic dif-ficulties and demonstrated some shortcomings, andthattheworldiscurrentlyill-preparedtorespondtoaseverepandemicoranyotherpublichealthemergencyonasimilarlyglobalandthreateningscale.TheCom-mitteealsopresentedWHOwithasetofrecommenda-tions,describedonpage48,whichservetoguidetheOrganization in furtherstrengthening the IHR frame-worksothatitmaybetterprotecttheworldagainstthepublichealtheventswemayfaceinthe21stcentury.
Well-functioning national public health systemsarethecoreoftheinternationalsystemforcoordinat-edresponse toevents thatmightconstituteapublichealthemergencyofinternationalconcern.TheIHRre-quirethatcountrieshavethecorecapacitiesinplaceby 15June 2012. Amain focus of thework over thepastyearhasthereforebeentomeetthecorecapacity
requirements,identifygapsandassistcountrieswiththe development of national action plans to achievethe minimum capacity requirements. The Depart-ment hasworked diligently with the regional officesthroughouttheyeartogetherwithcountriestomobi-lizeresourcesneededtobuildmissingcapacities.
In2011wewitnessedthedevastationcausedbytheearthquakeandnuclearaccidentsinJapan.Theseevents were a disturbing wake-up call to the globalcommunity,atragicreminderofhowcloselylinkedweare,fromonecountrytoanother,fromregiontoregion.
The IHR provide not only the legal framework
but also a unique opportunity for the internationalcommunitytoworkcloselytogethertobebetterpre-paredtorespondcollectivelytopotentialpublichealtheventsthatthreatenourglobalhealthsecurity.Thereismuchwork to be done, andWHO is committed tocontinuing itswork incollaborationwiththeregionaloffices to support countries to strengthen their corecapacitiesforpreparednessandresponsetoallpublichealthevents.
ACI AirportsCouncilInternational
AFRO WHORegionalOfficeforAfrica
AMP AgencedeMédecinePréventive
AMRO/PAHO WHORegionalOfficefortheAmericas
APSED AsiaPacificStrategy
forEmergingDiseases
CAPSCA CooperativeAgreementforPreventing
theSpreadofCommunicableDiseases
throughAirTravel
CDC UnitedStatesCentersforDiseaseControl
andPrevention
EID EmergingandReemergingInfectiousDiseases
EIS EventInformationSite
EMRO WHORegionalOffice
fortheEasternMediterranean
EQA ExternalQualityAssessment
EU EuropeanUnion
EURO WHORegionalOfficeforEurope
FAO FoodandAgricultureOrganization
oftheUnitedNations
FETP FieldEpidemiologyTrainingProgramme
FOS FoodSafetyandZoonoses
GCR GlobalCapacities,AlertandResponse
GLaD GlobalLaboratoryDirectory
HSE HealthSecurityandEnvironment
IAEA InternationalAtomicEnergyAgency
IATA InternationalAirTransportAssociation
ICAO InternationalCivilAviationOrganization
IDSR IntegratedDiseaseSurveillance
andResponse
IHR InternationalHealthRegulations
ILO InternationalLabourOrganization
IMO InternationalMaritimeOrganization
ITH InternationalTravelandHealth
NFP NationalIHRFocalPoint
OIE InternationalOfficeofEpizootics
PAG Ports,AirportsandGroundCrossings
PAGNet PublicHealthandPorts,Airports
andGroundCrossingsNetwork
PHEIC PublicHealthEmergency
ofInternationalConcern
PoE PointsofEntry
REACT ReactiontoEmergencyAlertsUsingVoice
andClusteringTechnologies
SEARO WHORegionalOfficeforSouth-EastAsia
SSC ShipSanitationCertificates
TEPHINET TrainingProgrammesinEpidemiology
andPublicHealthInterventionNetwork
UNWTO UnitedNationsWorldTourismOrganization
USAID UnitedStatesAgency
forInternationalDevelopment
WER WeeklyEpidemiologicalRecord
WHO WorldHealthOrganization
WMO WorldMeteorologicalOrganization
WPRO WHORegionalOfficefortheWesternPacific

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 20116 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 20117
Introduction
Health Security and Environment (HSE) restructuring
The HSE cluster underwent a refining andstreamlining process in 2011 to improve coordina-tionbetweenthedifferenttechnicalteamsandbetterfulfil itsmandate of ensuring global health security.On1DecemberthenewHSEstructurewasmadeof-ficial. Formerly comprised of five departments, HSEnowhousesfourdepartments.TheGlobalCapacitiesAlert and Response Department (formerly IHR Coor-dination),whichnowincludestheAlertandResponseOperationsUnit, thus expanding themandate of thedepartment and uniting country capacity buildingand global alert and response activities under onegroup.ThePandemicandEpidemicDiseasesDepart-ment,alsonew,isresponsibleforinfluenza,hepatitis,meningitis and other epidemic-prone diseases andincludes a special unit on antimicrobial resistance.ThePublicHealthandEnvironmentandFoodSafetyDepartments remain unchanged. All four HSE de-partments contribute to the workings of the revisedIHR framework,whichcoversnotonly infectiousandfoodbornediseasesbutalsorisksthatcanarisefromchemical,nuclearandradiologicalevents.Allthefourdepartmentswork inclosecollaborationwith thesixWHOregionaloffices.
Priority activities in 2011
Strong national public health systems and ca-pacities are the core of the international system forcoordinatedresponsetoeventsthatmightconstituteapublichealthemergencyofinternationalconcern.AllStates Parties are required to have or developmini-mumcorepublichealthcapacities to implement theIHR(2005)effectively.
The IHRrequire thatcountrieshave inplacethecorecapacitiesby15June2012.Thefocusoftheworkoverthepastyearwasthereforetomeetthecoreca-pacity requirements and where necessary, identifygapsandassistcountrieswiththedevelopmentofna-tionalactionplans toachieve theminimumcapacityrequirements.InviewoftheJunedeadline,butalsoinlinewiththerecommendationoftheReviewCommit-teethatWHOassistcountriestoacceleratetheacqui-sitionofthecapacitiesneededtobebetterprepared,theDepartmentandregionalofficesworkeddiligentlywithcountriestoassesstheirexistingcapacitiesanddevelop national action plans to address gaps andmobilizetheresourcesneededtobuildthemissingca-pacities.Thisprocessofreviewingcapacities,identify-ingprioritiesanddevelopingnationalroadmapstoac-celerate implementationwas launched inZimbabwe fortheAfricanRegionandtheprocesshassincebeenduplicatedintheWHOEuropeanRegionandwillcon-tinue (this activity is described in greater detail onpage15).
Forcountriesthatareunabletoachievethecorenational health capacities by June 2012, extensionsarepossibleandWHOisfacilitatingthisprocess.
Partners in IHR implementation
WHO’s vision for international public health se-curity isamoresecureworldthat isonthealertandreadytorespondcollectivelytothethreatofepidemicsandotherpublichealthemergenciesthatrepresentanacutethreattopublichealthsecurity,anunbrokenlineofdefenceusinghighlytrainedpersonnelandmakingeffectiveuseofup-to-date-technologies.
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 20118 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 20119
WHO office in Lyon and its local and regional partners
Since its creation in2001, theWHOLyonOfficehasbenefited fromthecommittedsupportoftheGovernmentofFrance,theInstitutPasteur,theInstitutdeVeilleSanitaire,theRhône-AlpesRegion,theRhôneDepart-ment,theGrandLyonandtheFondationMérieux,whowasinstrumentalin establishing the Office. The financial and technical support of thesepartnersiscriticaltothesuccessfulimplementationofthedepartment’swide-reaching activities to help counties strengthen their public healthsystems.EachyeartheWHOLyonOfficecollaborateswiththelocalLyonandgreaterRhône-AlpesRegioninoutreachactivitiestoraiseawarenessofprioritypublichealthissuesandactivitiestofacethesechallenges.
Highlights in 2011 included :
BioVision roundtable, co-organizedwith the FondationMérieux and theInstitutPasteur:Securing Global Health in the 21st Century: epidemic in-telligence, identification of risks and opportunities for control. SpeakersincludedNobelPrizewinnerProfessorFrançoiseBarré-Sinoussi,DoctorGuénaëlRodier,DirectoroftheDivisionofCommunicableDiseases,WHORegional Office for Europe, and Doctor Robert Breiman, Country Direc-tor,CDC-KenyaandHead,GlobalDiseaseDetectionDivision,CDC-Kenya.Theroundtableincluded160expertsfromthescientificcommunityoftheGrand Lyon, the greater Rhône-AlpesRegion, and national and interna-tionalinstitutions.
Global partnership
Inacloselyinterdependentworld,globalpartner-shipsareessentialtothesuccessfulimplementationof the Regulations. Partnership is required betweenall countries to share technical skills and resources,tosupportcapacitystrengtheningatalllevels,tosup-porteachother intimesofcrisisandpromotetrans-parency. Partnership between different sectors (e.g.health, agriculture, travel, trade, education, defence)isalsoessentialtobuildcoherentalertandresponse
systemswhichcoverallpublichealththreats,and,atthetimeofevents,areabletorapidlymobilizethere-quiredresourcesinaflexibleandresponsiveway.
IHRactivitiesarecarriedout inpartnershipwiththe WHO regional offices in all WHO regions and inmany countries thanks to the commitment and sup-portofitstechnicalandmainfundingpartners.
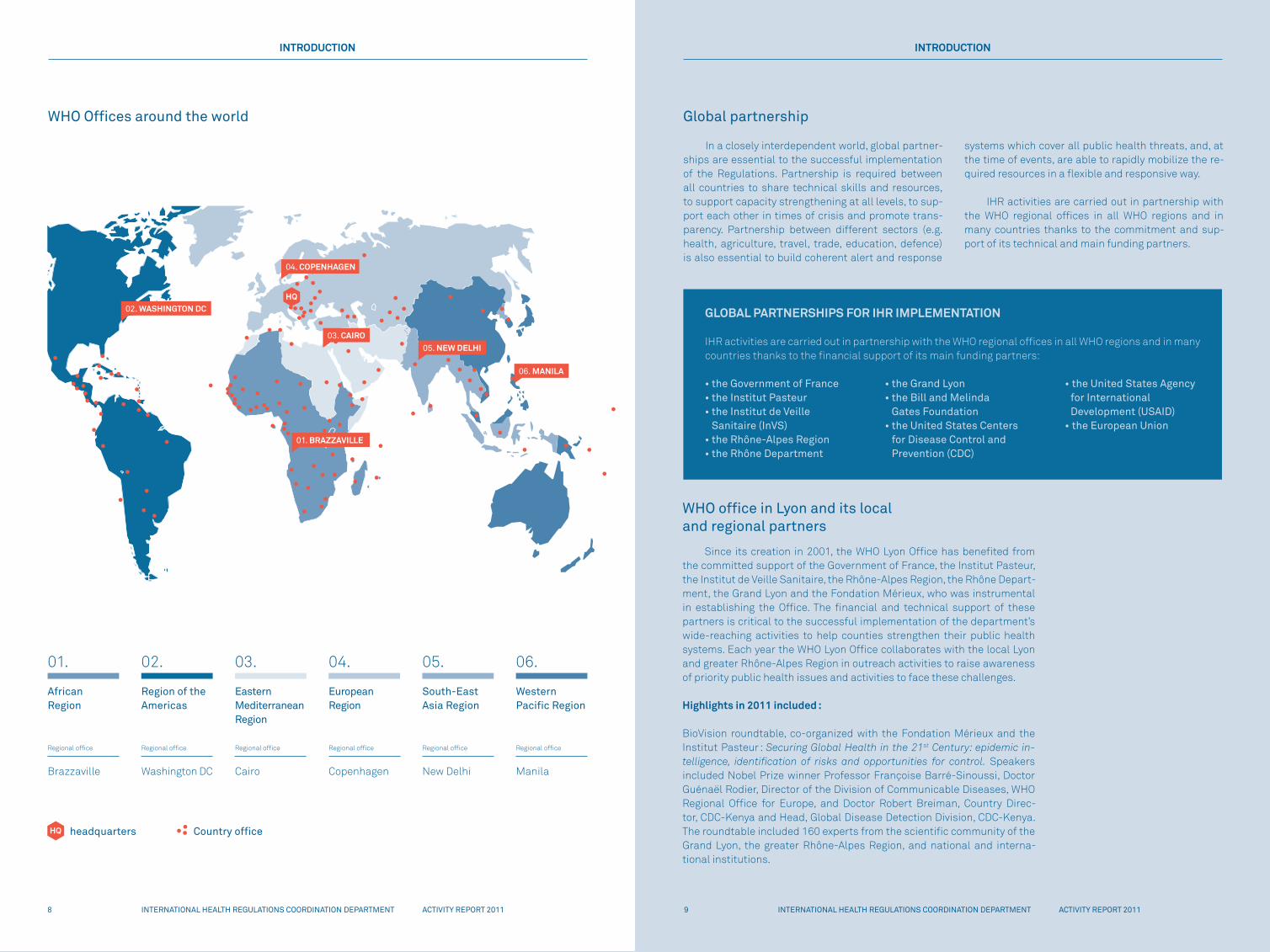
WHO Offices around the world
INTRODUCTION INTRODUCTION
GLOBAL PARTNERSHIPS FOR IHR IMPLEMENTATION
IHRactivitiesarecarriedoutinpartnershipwiththeWHOregionalofficesinallWHOregionsandinmanycountriesthankstothefinancialsupportofitsmainfundingpartners:
•theGovernmentofFrance•theInstitutPasteur•theInstitutdeVeille Sanitaire (InVS)•theRhône-AlpesRegion•theRhôneDepartment
•theGrandLyon•theBillandMelinda Gates Foundation•theUnitedStatesCenters for Disease Control and Prevention (CDC)
•theUnitedStatesAgency for International Development (USAID)•theEuropeanUnion
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 20118
02. WASHINGTON DC
04. COPENHAGEN
01. BRAZZAVILLE
05. NEW DELHI
06. MANILA
03. CAIRO
01.
African Region
02.
Region of the Americas
03.
Eastern Mediterranean Region
04.
EuropeanRegion
05.
South-East Asia Region
06.
Western Pacific Region
Regionaloffice
Brazzaville
Regionaloffice
WashingtonDC
Regionaloffice
Cairo
Regionaloffice
Copenhagen
Regionaloffice
NewDelhi
Regionaloffice
Manila
headquarters Country office

ACTIVITY REPORT 2011 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201111INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201110 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 2011
Review of activities 2011
Core Capacity Development
The IHR i-course :oneofthemostwide-reachingawarenessraisingvehicles,eachyearthecoursetrainsupto40publichealthprofessionalsfromaround theworldon IHR implementation.These IHRprofessionalsthentransfertheir IHRexpertisetostaff intheirnationalhealth institu-tions,thusbroadeningandstrengtheningthenetworkofIHRpartners(de-scribedinmoredetailonpage35).Sincethecoursewaslaunchedin2009,theFondationMérieuxhasprovidedmuchneededsupport to thiswide-reachingandambitiousprogramme,makingitpossibleforparticipantstobehostedatitsconferencecentreLesPensièresatVeyrier-du-Lacduringtheface-to-facesessionsofthecourse.
Europeanheritagedays:eachyeartheMuséeDr.Mérieuxwelcomes250-300participants,includingscientists,universitystudentsandschoolgroups,duringthiseventfocusingonchallengestopublichealthandad-vancesinthescientificcommunitytomeetthesechallenges.Duringthisevent, theWHOoffice inLyonhostsan informationstand, invitingques-tionsandexchangeswithvisitorstotheevent.Inaddition,eachyearWHOexpertsparticipateinthemuseum’stemporaryexhibitions.Thisyearfea-turedexhibitionsonCalmette-Guérinand theirdiscoveryof theTB/BCGvaccine,andthecommemorationofGlobalRabiesDay.
Structure of this report
PreviousIHRCoordinationDepartmentactivityreportsdescribedtheactivities during the preceding year according to the responsibilities ofeachtechnicalteam.Thisyear'sreportlaysoutactivitiesnotbytechnicalteam,butbycorecapacity,therebyhighlightingthesupporttocountriestostrengthentheirnationalpublichealthcapacities.Thisnewstructurealsoechoesthemoreharmonizedapproachbetweentechnicalteams,acrossdepartmentsand theentireWHO tomeet its commitment to theglobalcommunityforasaferworld.
The report focuses on the core capacities 1-9, which fall under itsmandate. Preparedness, core capacity 5, however, is an activity that iscarried out in all technical units throughoutWHO.Therefore, under this sectionthereporthighlightsaselectionofactivitieswiththeprovisionthatallactivities in theDepartmentandacross theHSEcluster includepre-parednesscomponentsintheirwork.Additionalworkonwholeofsociety preparedness has just started in theHSE cluster. Activities to face thechallengesofallhazards(corecapacities10-13)areledbytheFoodSafe-tyandPublicHealthandEnvironmentDepartmentsinclosecollaborationwiththeIHR(nowGCR)Department.
Finally, theworkof assessingexisting core capacitiesand identify-inggapsincountriesmustbeginwithasituationanalysis;therefore,thenextsectionofthisreportbeginswiththeactivitiestomonitorIHRimple-mentationincountriesandtoaccelerateimplementationinthecountrieswherethisisneeded.
11
01. National legislation
02. National Focal Point communications and coordination
03. Surveillance
04. Response
05. Preparedness
06. Risk communications
07. Human resources
08. Laboratory
09. Points of entry
10. Food safety events
11. Chemical events
12. Nuclear events
13. Radiological events
IHR core capacities

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201112 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201113INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 2011
Strong national public health systems and capacities are the core of the interna-tional system for coordinated response to events that might constitute a public health emergency of international concern. All States Parties are required to have or develop minimum core public health capacities to implement the IHR (2005) effectively.
Monitoring
Assessment of IHR core capacities
Withregardstoassessmentandmonitoringtools,WHO has developed a number of generic and core-capacity specific guidance for IHR.These include in-depth assessment protocols, specific assessmenttools(pointsofentry,laboratory,riskcommunications,legislation,etc.),monitoringchecklists,StatesPartiesquestionnaires,andotherguidance.WHOregionalof-fices also have ongoing regional strategies such asthetheIntegratedDiseaseSurveillanceandResponse(IDSR),theEmergingInfectiousDiseases(EID)andtheAsiaPacificStrategy forEmergingDiseases (APSED)onwhichcountriesneedtobuildwhendevelopingtheIHRcorecapacities.
In2011, following theReviewCommittee recom-mendationtoaccelerateIHRimplementationincoun-tries,adeskreviewplanningandadvocacyguidewasdeveloped to support States Parties in fulfilling thecorecapacityrequirements.Thisguideisaninterme-diarytoolwhichidentifiesgapsandstrengths,permitsthedevelopmentofrobustplans,whilevalidatingthequality of the States Parties reports, within a shorttimeframe.
WHO HQ and regional offices have assisted anumberofcountriestoassesstheir IHRcorecapaci-
tiesusingtheassessmenttoolorthedeskreviewandplanning guide, to develop or update plans of actionbased on gaps or weaknesses identified, and to de-velopspecificcorecapacities.
Monitoring of IHR core capacity development
Amonitoringframeworkandcorrespondingtoolshave beenmade available to allowStates Parties tomonitorthestatusoftheirnationalcorecapacities,inaccordancewiththerequirementssetoutinAnnex1of theRegulations,andto identifyareas that requireaction.Thisframeworktakes intoaccounttheStatesParties'obligationtoreportontheimplementationofthe IHR to theWorldHealthAssembly.The status ofIHRcorecapacitydevelopmenthasbeenmonitoredbyWHOthroughtheannualStatesPartiesquestionnaire,which is self-reported data. The IHR monitoringprocessassessesthestatusofdevelopmentofeightcore capacities, as well as capacities developmentatpointsofentryfor IHR-relatedhazards (biological,i.e. zoonotic and food safety; chemical, radiologicaland nuclear) through a checklist of twenty globalindicators.
CORE CAPACITY DEVELOPMENT
12

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201114 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201115
Tabletop exercises
In order to support States Parties in their abil-itytoensurethattheircorecapacitiesarefunctionalattherequiredlevel,tovalidateplans,andtocontri- bute to thebuildingof relationshipsandoperationalconfidenceacrossrelevantstakeholders,anexercisedesign handbook and accompanying five-day work-shop platform has been developed. Working withinthecontextofthecorecapacities,participantsintheworkshopusetheexercisedesignhandbookasabasetextandthroughaseriesofinteractivesessionslearntoapplyastandardprocesstodevelopatabletopex-ercisearoundachosentopic.
In 2011 two workshops were held, the first in Ankara, Turkey and the second in Nairobi, Kenya. Participants fromeach of theseworkshopswill con-ductexercisesin2012.TheAnkaraworkshopincludedparticipants from Bosnia and Herzegovina, Georgia,theIslamicRepublicofIran,Jordan,Kosovo,Lebanon,Morocco, Oman, Pakistan, the Republic of Albania,the Republic of Armenia, the Republic of Macedo-nia, the Republic ofMoldova, Serbia, Syria, and Tur-key. The Kenyaworkshop included participants fromCameroon, Congo, Eritrea, Ethiopia, Gabon, Gambia,Ghana,Mauritius,Mozambique,Namibia, Swaziland,TanzaniaandUganda.Afghanistan,Iraq,LebanonandUgandahaveallexpressedadesiretoconductanIHR-relatedexercisein2012.
Web-based tools
Inordertofacilitatethedatacollectionandfeed-backprocess,aweb-basedtoolhasbeendeveloped,allowing States Parties to submit and update theirdata online, and generate reports charts and tablesafterdatasubmission.ItalsoallowsStatesPartiestoupdatetheir informationthroughouttheyearonpro-gressmade inthe implementationof IHR.Thismoni-toringtoolhasundergoneseveralrevisions,includinga"talkingpresentation"during2011,andwillforeseesupportforallsixofficial languagesin2012.TheIHRPortal, introducedin late2010,originallydesignedtogive IHRNationalFocalPointsa "onestopshop" foraccessing the applications and data they need, hasbeen revised and is now available to subjectmatterexperts,IHRregionalcontactpoints,IHRNFPsaswellasWHOstaff.Virtualmeeting softwarewill facilitatethecontactwithIHRregionalcontactpointsandsub-jectmatterexpertsasthe2012deadlineapproaches.
CORE CAPACITY DEVELOPMENT
MONITORING
CORE CAPACITY DEVELOPMENT
MONITORING
AFRO:IHRexpertsbriefingandlaunchofdeskreviewforacceleratedIHRimplementationintheAfricanRegion
The IHR desk review consultant briefing meeting, organized by HQ and AFRO in October was part of the plan to support Member States to accelerate the de-velopment of national IHR core capacities. The Hara-re briefing brought together 25 IHR experts from WHO country offices, key staff in the ministry of health and from other relevant institutions in the African Region
to prepare for the IHR desk review, to take place in Benin,Côted’Ivoire,EquatorialGuinea,Eritrea,Gui- nea, Liberia, Mauritania, Nigeria, Sao Tome & Princi-pe, Senegal, Togo, Zambia and Zimbabwe. Zimbabwe led the process with its desk review. Desk reviews have since been carried out in all of the countries listed above.
Status
TherevisedStatesPartiesquestionnairewassenttoMemberStatesin2010and2011,andsolicited128and150completedresponsesrespec-tively.Thedata for2011showedStatesPartiesmaking fairprogress foranumberofcorecapacities,notablythoseforsurveillance(withaglobalaveragescoreof75%),response(withaglobalaverageof73%),laboratory (withaglobalaverageof71%),andzoonotic events(withaglobalaverageof77%).Ontheotherhand,mostregionsreportedrelativelylowcapacitiesinhuman resources(withaglobalaverageof46%),atpoints of entry(withaglobalaverageof59%)andforChemical events detection and response (withaglobalaverageof45%).
In comparing1 core capacity status for countries reporting in bothyears (asshown in thegraphbelow), there isoverallprogressacrossallcorecapacities,withtheincreaserangingfrom3%to12%.Themostno-ticeableprogressisinsurveillance(from67%to79%)andpreparedness (from49%to60%),whilethereisrelativelyslowerprogressincoordina-tion(from69%to73%)andrisk communication(from65%to68%).
•Radiological
•Chemical
•FoodSafety
•Zoonosis
•PoE
•Laboratory
•Hum
anResources
•RiskCom
munication
•Prepardness
•Response
•Surveillance
•Coordination
•Legislation
54
48 47
43
70
67
78
73
61
54
72
68
49
41
68
65
60
49
74
70
79
67
73
69
65
58
2010
2011
1.Inordertomakevalidcomparisonbetween2010and2011,dataof109countriesthatreported inbothyearswereused.Thisiswhythescoresintheparagraphandgraphoncomparisonmight differfromthoseintheparagraphwhichshowsscoresof156countriesthatreportedin2011.

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201116 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201117
Legally-oriented aspects of IHR implementation cover a range of activities support-ed by WHO, including implementation of the IHR in national legislation and other areas of legal advice on IHR implementation. With the many new or expanded rights and obliga-tions for States Parties under the IHR (2005), States Parties have been strongly advised since adoption of the IHR to assess their existing legal frameworks in all relevant areas to ensure full implementation - including any legal instruments necessary to support the additional technical capacities being developed in connection with Annex 1 of the IHR. In some States Parties, implementation of the IHR may require that they adopt implement-ing or enabling legislation for some or all of these obligations and rights. Even where new or revised legislation may not be specifically required it can facilitate implementation in a more efficient or effective manner, can serve to institutionalize and strengthen the role of IHR (2005), and facilitate coordination among the different national entities involved in implementation.
National Legislation
CORE CAPACITY DEVELOPMENT
Country requirements
AllStatesPartieshavebeenlegallyboundtoim-plement the IHR since their entry into force in 2007(excepting those who became WHO Member StatesafterIHRadoption).Tofulfillthisobligation,sufficientnationallegislationneedstohavebeenandcontinuein place for fulfillment of all IHR State Party obliga-tionsandallimportantStatePartyrights.
WHO commitments
WHOissupportingStatesPartiesintheirassess-mentsandfollow-upactions,asnecessary,forfulland
efficientimplementationoftheIHR(2005)innationallegislation, and provides additional advice and gui-danceconcerningIHRapplicationnationally.
General status in countries
TheIHRmonitoringdatashowsthat,in2011,71%ofreportingcountriesindicatedhavingcarriedoutle- gislativeassessmentsand51%ofrespondingStatesParties reported having implemented recommenda-tionsafterconductingsuchassessments.
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201118 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201119
HIGHLIGHTS
Inthecontextofnationallegislation,WHOhassupportedStatesPar-tiesin2011through:individualmissionsinvolvingnationallegislation(e.g.IranandSaudiArabia);a teleconferenceconcerningnational legislationissues(Sudan),preparationofpresentationonlegislativeassessmentandrevisionfor lawmakers(tobepresentedbycolleaguesinUzbekistan) le-gislationfacilitationofexpertconsultantadvice(EastTimor),preparationoflegislativeandthecontinuedavailabilityoftheextensiveIHRnationallegislationguidancematerials.WHOalsopresentedandspokeonnationallegislationandotherlegalissuestothestudentsattheWHOi-courseonimplementingtheIHR(2005),andsubstantiallyrevisedandcontributedtotherelatedwrittenmaterialspreparedbyGeorgetownUniversity.
WHOheldtwointeractiveworkshopsonassessmentandrevisionofnationallegislationforIHRimplementationon24-26and28-30NovemberinHarare,Zimbabwe,withthecombinedparticipationof17StatesPartiesof theAfricanRegion.For thefirst time,both legal/legislativeand tech-nical/IHR officialswere invited from each country so that the guidancewouldfocusonthesetwokeysectorsforlegislativeassessmentandrevi-sionforIHRimplementationtopreparethemforcompletingtheseactions,andtofacilitateestablishmentofanetworkoflegalandIHRofficialsintheAfricanRegionfamiliarwiththeprocessandmethodologiesforlegislativeassessmentandreviewtosharetheirknowledgewithofficialsinotherna-tionalgovernmentsaswellastheirown.
CORE CAPACITY DEVELOPMENT
NATIONAL LEGISLATION
CORE CAPACITY DEVELOPMENT
The effective implementation of the IHR at both global and national levels is dependant upon multisectoral and multidisciplinary collaboration to achieve alert and response systems that function across a broad range of public health risks. The National IHR Focal Point (NFP) plays a critical role in such coordination within a State Party, as well as being the national centre for IHR communications with WHO. The designation of National IHR Focal Points by virtually all States Parties was recognized as an important achievement by the IHR Review Committee that reported to the World Health Assembly in May 2011. The NFP is established under the IHR as a centre rather than an individual and must be accessible at any time to communicate with the WHO IHR contact points and with the relevant government sectors and other stakeholders in the country.
NFP Communications and Coordination
Country requirements
Countriesarerequiredtoestablishamechanismforthecoordinationofrelevantsectors intheimple-mentation of IHR. These coordination functions arefrequently the responsibility of the State's NFP andthe WHO guide to the NFP role makes reference tosomeaspectsofthiscoordination.NationalstandardoperatingproceduresorequivalentareencouragedtofacilitatethecoordinationbetweenIHRNationalFocalPointsandrelevantsectors.
The NFPs have a critical communications func-tion with WHO in both urgent situations relating topublic health events and risks, and regular adminis-trative communications relevant to IHR implementa-tion(e.g.submissionofmonitoringdata,requestsforextensions to the capacity deadline or lists of portsproviding ship sanitary certification). It is important
that the contact details of NFPs are updated andmaintainedtoensureeffectivecommunicationduringapublichealthemergency.To facilitateupdating theSecretariat providesNFPswith an internet interfacelinkeachmonth,usingwhichNFPscaneasilyconfirmorupdatetheircontactdetailsincludingtheir24/7ac-cessinformation.
WHO commitments
TheWHO IHR Contact Points in the six regionalofficesprovidetheclosestsupportto,andcommuni-cationwiththeNFPfunctionsinStates;workingwiththeNFPsinthemanagementofpublichealtheventsandorganizingregularmeetingstoupdateNFPsandfacilitatelearningfromregionalexperiences.GCRsup-portssuchmeetingswithmaterials, informationandpresentationsfromaglobalperspective.

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201120 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201121
CORE CAPACITY DEVELOPMENT
NFP COMMUNICATIONS AND COORDINATION
The IHR Review Committee recommended thatcountries ensure that NFPs "have the authority, re-sources,procedures,knowledgeandtrainingtocom-municate with all levels of their governments andonbehalfof theirgovernments".WHOwillupdate itsguideontheNFProletosupporttheimplementationofthisrecommendation.
General status in countries
Analysis of the IHRmonitoring data shows thataroundhalfofthe150StatesPartiesprovidingdatabyJanuary2012scorebetween75and100inthecapac-ityareaofcoordination,withtheaveragescoreinthiscapacityareabeing69.Thesefiguresareverysimilarto those from the 2010 data when only 125 Statesreportedon thisaspectof implementation. Inearlierreports in2008and2009countrieshadindicatedin-creasing levelsofcollaborationbetweenNFPsandabroadeningspectrumofnationalsectorsandpartners.
InaquantitativestudyoftheuseofAnnex2oftheIHRinnotificationofeventstoWHO,among133NFPs,88% reportedhavingexcellentor goodknowledgeofthecontentsofAnnex2,77%reportedalwaysorusually using Annex 2 for assessing public health emergen-cies,and76%indicatedtheircountryhadsomelegal,regulatoryoradministrativeprovisionsrelatingtotheuseofAnnex2.
HIGHLIGHTS
Event information site
WHOisobligedtoprovidetoStatesPartiestimelyinformationonre-levantpublichealthrisksofinterna-tionalimportancewhilerespectingthesensitivityandpotential confidentiality of such information. To thateffect,WHOhasdevelopedapassword-protectedwebsiteforsecurecommunicationswithnational IHRfo-calpoints.TheEventInformationSite(EIS)ismanagedcentrally.GCRensuresaccesstositebyasmallnum-berof individualsdesignatedbyeachNFP,aswellas
stafffromtheSecretariatandbyalimitednumberofotherinternationalorganizations.Whenthereisanewacutepublichealtheventorasignificantupdateonaneventpostedonthesecurewebsite,WHOsendsane-mailalertmessagetotheusers.
An online user satisfaction survey of the eventinformation site has been carried outwith a view toimproving theserviceprovided toStatesParties.Theresultsofthesurveyhavebeenpublishedonthesite.SurveyresponsessupportedthreeongoingactionsforWHO:firstly, theredesignofthesitetoenhanceuseraccessandutilityoftheinformationshared;secondly,to augment value-added information provided suchas public health risk assessments or event relevantguidelines or best practices; and thirdly, a cohort ofEIS-registered users comprising NFP staff and stafffrom all levels of the Organization self-identified aswillingtoparticipateinimprovementstopublichealthevent-based information sharing through the Eventinformationsite.
Early notifications by NFPs
TheNFPsdoprovideWHOwithearlynotificationsofevents thatmightbecomepublichealtheventsofinternationalconcern(PHEIC).Duringthe2009/10in-fluenzapandemictheNFPsprovidedtheOrganizationwithearlynotificationsofcasesaswellascontinuingaggregated information thatallowedtheevolutionoftheglobalemergencytobemonitored.AlthoughithasbeennotedbytheReviewCommitteethat"NFPsarenotyetatimelysourceofinitial,earlyinformationonevents that might constitute a potential PHEIC" theNFPsarealreadyprovidingimportantverificationandadditional information on events identified throughWHO'ssurveillanceactivities.It is important to note that this work was carried
out by the Alert and Response Operations Unit (ARO), which was not part of the IHR department in 2011. As of 1 December 2011, ARO and IHR are merged in the new GCR department. For more about this see page 7.
The IHR require the rapid detection of public health risks, as well as the prompt risk assessment, notification, and response. To this end, a sensitive and flexible surveillance system is needed with an early warning function. The structure of the system and the roles and responsibilities of those involved in implementing the system need to be clear and preferably should be defined through public health policy and legislation. Chains of responsibility need to be clearly identified to ensure effective communications within the country, with WHO and with other countries as needed.
Command, communications and control mechanisms are required to facilitate the coordination and management of response operations to outbreaks and other public health events. Multidisciplinary/multisectoral Rapid Response Teams should be esta-blished and be available 24 hours a day, 7 days a week. They should be able to rapidly respond to events that may constitute a public health emergency of national or interna-tional concern. Appropriate case management, infection control, and decontamination are all critical components of this capacity.
Surveillance and Response
CORE CAPACITY DEVELOPMENT
Country requirements — surveillance
Indicator-based surveillance includes an earlywarning function for the early detection of a publichealthevent.Countrieshavecommittedtokeepingalist of priority diseases, conditions and case defini-tionsforsurveillanceavailableaswellasdesignatingaspecificunit forsurveillanceofpublichealth risks.Surveillancedataonepidemic-proneandprioritydis-easesshouldbeanalysedatleastweeklyatnationalandsub-nationallevels.Countriesmustalsoestablishevent-basedsurveillancebyidentifyingaresponsibleunit as well as operating guidelines. Country experi-encesandfindingsonimplementationofevent-based
surveillance,andtheintegrationwithindicator-basedsurveillance,shouldbedocumentedandsharedwiththeglobalcommunity.Countriesshouldalsouse thedecision instrument in Annex 2 of the IHR (2005) tonotify potential public health events of internationalconcern toWHO.The IHRnational focalpointshouldrespond to 100% of verification requests fromWHOwithin24hours.
Country requirements — response
Countries should establish public health emer-gency responsemechanisms such as casemanage-
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201122 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201123
CORE CAPACITY DEVELOPMENT
SURVEILLANCE AND RESPONSE
CORE CAPACITY DEVELOPMENT
SURVEILLANCE AND RESPONSE
mentguidelines forpriority conditionsaswell as rapid response teamstorespondtoeventsthatmayconstituteapublichealthemergencyavai-lable24hoursaday,7daysaweek.Casemanagementguidelinesmustbeavailableforpriorityepidemic-pronediseases.Efficientoutbreakinvesti-gationmustbeensuredthroughtrainedpersonnelusingspecificguide-linesandcollaboratingeffectivelywithlaboratories.Appropriateandrapidmeasuresfordisinfection,decontaminationandvectorcontrolshouldbetaken.Infectioncontrolandbiosafetymustbereinforcedathospitalsandotherhealthfacilities.
WHO commitments
WHO shall assist States Parties, upon request, to develop, streng-thenandmaintainthesecapacities.WHOshallcollectinformationregard-ingeventsthroughitssurveillanceactivitiesandassesstheirpotentialtocauseinternationaldiseasespreadandpossibleinterferencewithinter-national traffic.WHOmay take intoaccount reports fromsourcesotherthanStateParties'notificationsorconsultationsandshallassessthesereports according to established epidemiological principles and thencommunicate information on the event to theStateParty inwhose ter-ritorytheeventisallegedlyoccurring.Beforetakinganyactionbasedonsuchreports,WHOshallconsultwiththeStatePartyandattempttoobtainverificationinaccordancewiththeproceduresetforthinArticle10.Tothisend,WHOshallmaketheinformationreceivedavailabletotheStatesPar-tiesandonlywhereitisdulyjustifiedmayWHOmaintaintheconfidential-ityofthesource.
General status in countries
Aselfassessmentofcorecapacityfulfillmentin2011showsaglobalaverage score of 75%of reaching the requirements of surveillance.ThescorebyWHOregionshowsforAfrica:63%,theAmericas:76%,theEast-ern Mediterranean: 80%, Europe: 81%, South-East Asia: 69% and theWesternPacific:83%.
Forresponsecapacity,theglobalaveragescoreis73%,andtheave-ragebyregionisthefollowing:Africa:54%,theAmericas:77%,theEasternMediterranean:73%,Europe:78%,South-EastAsia:74%andtheWesternPacific:89%.
HIGHLIGHTS
Central Africa Surveillance (SURVAC) Project
FundedbytheBillandMelindaGatesFoundation,theprojectstartedin2009and is jointly coordinatedby theWHO IHRDepartmentand theWHORegionalOfficeforAfrica,theWHOIntercountrySupportTeambasedinLibreville,theWHOCountryOfficeineachofthethreecountries,aswellastheUSCentersforDiseaseControlandPrevention.TheSURVACprojectcomprises Cameroon, the Central African Republic and the Democratic
RepublicofCongo,countriesthatsharesimilarepidemiologicalprofiles,simi-largaps inthecapacitytodetectandcontrolhealththreats,andtheFrenchlanguage.Epidemic-proneandvaccine-preventablediseasesareprioritized,inlinewithnationalprioritiesinthethreecountries.
EPISOUTH Plus Project
Basedon theexperiencegainedduring itsfirst years,EpiSouthentereda second phase called “Episouth Plus” in October 2010. EpiSouth Plus is a33-monthprojectfundedbytheEuropeanUnion(EU),whichaimstoincreasehealth security in theMediterranean area and south-easternEurope by en-hancingpreparednesstohealth threatsandbio-security risksatnationalorregionallevelsintheframeworkofIHRimplementation.Theprojectinvolves27countriesfromtheEuropean,theEasternMediterraneanandtheAfricanWHORegions.ActivitiesareorganizedinsevenWorkPackages(WP),jointlyledbyEUandnon-EUcountries.WorkPackage7 isco-ledbyWHOandthe ItalianNa-tionalInstituteofHealth.In2011theWP7steeringteamwasconsolidatedandthespecificobjectiveoftheWPwasidentified:coordinationofsurveillanceandresponsebetweenpointsofentryandnationalsystems,andacross-cuttingtopictobeapproachedbyallworkpackages:surveillance, identificationandmanagementofhealtheventscausedbyvector-bornediseases.
Surveillancebymobilephone:Developingamodelsystemforefficientelectronicdatatransmissionandmanagementinroutinenationalepidemiologicalsurveillance
Part of the SURVAC programme, this project is developing a model system of data transmission that uses mobile and wireless technologies. The back-ground is rapid advance in mobile technology and a continued growth in coverage of mobile phone net-works, which now extend far beyond the reach of electricity grids, especially in developing countries.
A first field pilot test was carried out in the Central African Republic, where surveillance data generated at remote locations was sent via SMS using mobile phones. The surveillance data is collected at peripheral health facilities and transmitted to a district office, which is responsible for the basic surveillance actions and transmission of data to an intermediate or regional surveillance office, which in turn forwards to the central level. Common problems in the current surveillance systems are incomplete
data, poor validity and timeliness, and undertrained staff with too heavy a workload. At district level, data was verified and imported in a data analysis application, and finally, aggregated district data was transmitted to the central level. The only technology required in the peripheral health facility is a mobile phone, sometimes with a small solar panel for power. In the upper levels, a computer manages data received by SMS, launching automated checks and generating responses to the senders. A surveillance operator checks and validates the data, and imports it into the surveillance database with user-friendly procedures. All the processes are automated, but users can keep control at every step. In this way, multiple benefits are foreseen, time is saved between the occurrence of health events and the availability of information for analysis and action.

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201124 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201125
CORE CAPACITY DEVELOPMENT
SURVEILLANCE AND RESPONSE
CORE CAPACITY DEVELOPMENT
Training in field epidemiology: biostatistics
AnewversionofaselflearningCD-ROMonbiostatisticswaslaunchedin2011 incollaborationwith theAgencedeMédecinePréventive (AMP).Themainlearningobjectiveofthisprogrammeistounderstandthepur-poseofbiostatisticsthroughrealisticcasesandtoacquirebasicbiostatis-ticsskills.Thetargetaudiencesofthistrainingaremedicalandbiomedi-calstudents,laboratoryspecialistsandotherprofessionalswhoneedtouseorunderstandbasicbiostatistics.However, itmayalsobeahelpfulremindertoepidemiologists.IthasbeendesignedanddevelopedinsuchawaythattraineescanworkindependentlyusingonlytheCD-ROMwhennobookortutorisavailable.Sinceitslaunchthistoolhasbeeninhighde-mand,anditstranslationintoFrenchisplannedfor2012.
Accreditation of Field Epidemiology Training Program (FETP)
TEPHINETisanon-profit,professionalallianceofallfieldepidemio-logyandlaboratorytrainingprogrammeswiththeaimofstrengtheningin-ternationalpublichealthcapacitythroughthesupportandnetworkingoffield-basedtrainingprogrammes.TEPHINETFieldEpidemiologyTrainingProgram(FETP)directorshaveagreedtoimplementanFETPaccreditationprocess.TheprimarypurposeofaccreditationistoimprovethequalityofFETPs,theireffectivenessinincreasingglobalfieldepidemiologycapacity,andthereforeintheacquisitionofsurveillanceandresponsecapacityasrequiredbyIHR.In2011“AccreditationReferenceDocumentforFieldEpi-demiologyTrainingPrograms”waslaunched.
Morocco:Assessmentoftrainingneedsforhealthstaffcontributingtotheepidemiologicalsurveillancesystem
This project is part of a process in which WHO supports countries in the region to build nation-al strategies for training the human resources to strengthen epidemiological surveillance.
The Moroccan assessment has been done through a survey by questionnaire to all staff involved in the surveillance system in the countries 16 regions, followed by a visit to five regions as well as to key health ministry structures at central level. The fol-lowing method was used to describe the situation by
region and by type of surveillance structure: the type of training received by the staff, their perception on the training gaps and their opinion on the most ap-propriate modalities for training in their particular context. The study revealed a number of factors, di-rectly or indirectly linked to training, which affect the motivation of staff to stay and to excel in their per-formance. In Morocco, this course of action is set to continue in 2012 within the consensus of the health authorities and collaborating agencies.
Preparedness includes the development of national, intermediate and community/primary response level public health emergency response plans for relevant biological, chemical, radiological and nuclear hazards. Other components of preparedness include mapping of potential hazards and hazard sites, the identification of available resources, the development of appropriate national stockpiles of resources and the capacity to support operations at the intermediate and community/primary response levels during a public health emergency.
Preparedness
Country requirements
Countries have committed to develop a multi-hazard national public health emergency prepared-ness and response plan which should be tested inactual emergency or simulation exercises and up-datedasneeded.Countryexperiencesandfindingsonemergencyresponseandinmobilizingsurgecapacity,should be documented and shared with the globalcommunity. Countries have also committed to mappriorityhealthriskandresourcesanddevelopadirec-toryofexpertsinhealthandothersectorstosupportaresponsetotheIHR-relatedhazards.
General status in countries
AselfassessmentdonebyStatePartiesin2011,showsaglobalaveragescoreof58%ofreachingtherequirementsofpreparedness.IfwebreakthescoresdowntoaveragebyWHOregion,wefindthefollowingresults:Africa:35%,theAmericas:57%,EasternMed-iterranean:61%,Europe:70%,South-EastAsia:58%andtheWesternPacific:73%.
HIGHLIGHTS
The work within the area of preparedness hasduring 2011 been carried out bymany departmentsandcoversawiderangeoftechnicalareas.
Towards the end of 2011 the responsibility wasconsolidated intoone teamunder the supervisionoftheAssistantDirector-GeneralfortheHealthSecurityandEnvironmentcluster.SomeexamplesoftheworkcarriedoutbytheIHRDepartmentduring2011arede-scribedbelow.
WHOBioriskManagementAdvancedTrainer Programme
In 2011, three further sessions of the trainingcourse for trainerswereorganized to strengthen thebiorisk management capacities and capabilities oftrainersofthepolionetwork;CzechRepublic,Switzer-landforcountriesoftheeasternEuropeanRegion,andinMaliforFrench-speakingAfricancountries.Shorterbioriskmanagement courses for userswere also or-ganized:withintheAfricanTBnetworkinTanzania,for
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201126 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201127
CORE CAPACITY DEVELOPMENT
PREPAREDNESS
CORE CAPACITY DEVELOPMENT
PREPAREDNESS
the Caribbean sub-Region in Trinidad andTobago, for English-speakingAfricancountriesinGhanaandfortheinfluenzanetworkintheMaldives.
International Travel and Health - book and web site
Almost900million international journeyswereundertaken in2009.Globaltravelonthisscaleexposesmanypeopletoarangeofhealthrisks,manyofwhichcanbeminimizedbyprecautions.TheyearlyeditionsoftheITHbookandwebsiteexplainshowtravellerscanstayhealthyandprovidesWHOguidanceonvaccinations,malariachemoprophylaxisandtreatment,personalprotectionagainstinsectsandotherdiseasevectors,andsafetyin different environmental settings. It covers all the principal risks totravellers’health,bothduring their journeysandat theirdestinations. Itdescribesallrelevantinfectiousdiseases,includingtheircausativeagents,modesoftransmission,clinicalfeaturesandgeographicaldistribution,andprovidesdetailsofprophylacticandpreventivemeasures.Thisinformationis intended for themedical andpublic health professionalswho advisetravelers,butitisalsoastandardreferencefortravelagents,airlinesandshippingcompanies–andfortravelersthemselves.ThebookiscurrentlytranslatedintoFrench,Spanish,GreekandItalian.≥ www.who.int/ith
Yellow fever vaccination - revised recommendations
The IHR require WHO to publish regularly a list of countries andareaswherethere isariskofyellowfevervirustransmission.This list isupdatedeveryyearinAnnex1oftheWHOpublicationInternationalTravelandHealth.Toaddressthechangingepidemiologyofyellowfeverandthecurrentconcernsregardingseriousadverseeventsassociatedwithyellowfevervaccine,asystematicreviewwasundertakenforeachcountrywherethereisariskofyellowfevervirustransmission.TheDepartmentconvenedconsultationsonyellow feverand international travel in2008and2010andselectedaworkinggrouptosystematicallyassesstheriskforyellowfevervirustransmission inAfricaandSouthAmericaandtoensurethatmapsand vaccination recommendationswereharmonizedon thebasisofconsistentcriteria.UpdatedinformationhavebeenpublishedinWHOWeekly Epidemiological Record (WER), onWHO International travel andhealthwebsiteandtheLancet.
Database for electronic archiving of reports on yellow fever epidemiology.
Theworkinggroupofexpertsoncountry-specificmappingofyellowfever risk is continuing its work by means of a review of criteria andmethodologiestocategorizecountries’yellowfeverriskstatus.Inordertopermityellowfeverriskmappingtoberefined,thisgrouphasdevelopedadatabaseforelectronicarchivingofnon-publishedreportsonyellowfeverepidemiology.
Preparation for mass gatherings : Health conditions for travellers to Saudi Arabia for the pilgrimage to Mecca (Hajj)
The Department prepared with the Ministry ofHealthofSaudiArabia the requirementsandrecom-mendationsforentryvisasfortheHajjandUmrasea-sonsin2011.
These are published in the WHOWeekly Epide-miologicalRecordtoinformvisitorsofthefullrequire-mentsforentryintoSaudiArabiaduringthepilgrimage.
FieldexerciseinSpain:Publichealthemergencyresponseinairtravel
This public health emergency simulation exercise was undertaken by WHO in close collaboration with the Spanish Ministry of Health, joined by observers from the Interna-tional Civil Aviation Organization (ICAO) EU-ROPE and public health experts from all WHO regions. The objective of the exercise was to acquire experience, to share lessons learnt, to underpin the emergency planning at points of entry and to contribute to improve technical guidance tools in this matter. The simulation was part of Spain's national efforts to update and develop capacities for responding to pub-lic health emergency involving points of entry and international travel and transport, in a multisectoral approach, in line with the IHR requirements and other international agree-ments, such as the International Civil Avia-tion Convention.Madrid Barajas airportwaschosen to host the field activities of the ex-ercise taking into account that it is the main international airport in Spain, and that it had undergone assessment and development of IHR core capacities and has previous experi-ence (Pandemic (H1N1) 2009)) in developing and implementing protocols for responding to public health events integrated at the airport emergency plan. As a result from this experi-ence, other airport public health emergency exercise is being planned in Spain for 2012 and lessons learned shared nationally and at international fora during 2011.
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201128 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201129
CORE CAPACITY DEVELOPMENT
Risk communication is an integral part of managing public health emergencies. Ex-periences at the community, national and international level in responding to disease outbreaks, natural disasters and other acute events have demonstrated the negative impact when communication has not been integrated, strategically planned, and well executed.
Effective management of public health emergencies relies on the coordinated ac-tions of individuals, groups and organizations to rapidly identify the source, provide ap-propriate care and treatment to those affected and to prevent further exposure and loss of life through promoting appropriate risk reduction and health protective behaviours to those affected and/or at risk. Often, these actions and the decisions which produce them, are taken when information is scarce, and uncertainty and anxiety are high. These condi-tions have reinforced the value and necessity of making sure that risk communication procedures, protocols, mechanisms and human resources are in place and functional well ahead of an event, especially against the backdrop of a changing media landscape with the explosion of social media and alternative sources of "authoritative" knowledge.
Subsequently, there has been a recognition that capacity building in risk communi-cation must be broader in scope and address a range of communication functions and roles; consider the socio-cultural, economic and political contexts of health emergen-cies; take into account the realities, needs and priorities of developing countries and build on what already exists; be able to offer practical tools and methodologies; and be linked to existing body of science, knowledge and good practice from health communi-cation and relevant disciplines such as anthropology, psychology and sociology.
The activities highlighted in this report reflect these findings and mark the continued progress that is being made to integrate risk communication within routine public health preparedness.
Risk Communication
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201130 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201131
CORE CAPACITY DEVELOPMENT
RISK COMMUNICATION
CORE CAPACITY DEVELOPMENT
RISK COMMUNICATION
Country requirements
The States Parties have committed to establishpolicy andprocedures for public communicationsaswellasmechanismsforeffectiveriskcommunicationduring a public health emergency. This includesidentifying risk communication stakeholders andpartners,aswellasaunitresponsibleforcoordinationof public communications during a public healthevent. States Parties should also develop riskcommunicationpoliciesandplansandexercisethese.Riskcommunicationcarriedoutduringapublichealtheventshouldbeevaluated.
WHO commitments
Under the IHR, WHO is committed to supportMember States in the acquisition and maintenanceof core risk communication capacity for respondingto public health emergencies. Capacity-buildingfor risk communication has been delivered over thepast several years through a number of constantlyevolvingandresponsivemechanisms:globalmeetingsto develop and refine core capacities and abilities;regional training workshops to test methodologiesfor enhancing skills and competencies in risk com-municationatcountrylevels;andthedevelopmentofasetofcorematerialsforuseonlineaswellasface-to-face.
General status in countries
A self assessment done by State Parties by theendof2011showsaglobalaveragescoreof64%ofreachingtherequirementsofriskcommunications.IfwebreakthescoresdowntoaveragebyWHOregion,wefindthefollowingresults:Africa:43%,theAmericas:70%, theEasternMediterranean:67%,Europe:68%,South-EastAsia:68%,andtheWesternPacific:84%.
HIGHLIGHTS
AFRO Workshop on strengthening Risk Communication Responses
This workshop was held in December 2011 inHarare, Zimbabwe and focused on strengtheningrisk communication responses to support epidemic
preparedness and response in the African Region.It was an internal WHO strategic thinking andplanning workshop to establish consensus on riskcommunicationinpublichealthemergenciesrelevantfor theAfricanRegion.Thisworkingmeetingbroughttogetherstaff fromthethree levelsofWHOtobettersupportandrespondtotheneedsandprioritiesofWHOcountry offices.The outcome is a product documentthatoutlinesaframeworkforriskcommunicationandstrategicactionsatthethreelevelsofWHO.
AMRO/PAHO
In the Americas, the risk communication group focused on strengthening capacity at the national levels with workshops designed for health ministrycommunicators, epidemiologists and hospital direc-tors. The training centered on case studies and theneed to createNationalRiskCommunicationStrate-giesweightedheavilyonplanningandpreparation.
Atthesametime,AMROintroducedasix-monthcertifiedon-lineriskcommunicationcourseinSpanish.The programme, hosted on PAHO’s Virtual Campus,enabled20healthprofessionalsfromthroughouttheRegion to work on actual projects related to publichealtheventsintheircountries.Theparticipantsalsolearnedskillstosharetheirtrainingatthelocallevels.
Giventheneedtosustainthetrainingandmovefrom theory to action, PAHO formed a Regional riskcommunicationtaskforcetoproduceafieldguideinEnglishandSpanish.
EMRO
Risk communication was recognized as a keyarea that requires support and capacity building.EMRO through the IHR Department conducted anassessmentoftheIHRcorecapacitiesandorganizeda regional workshop in order to assess the needsfor capacity building. During the workshop severalrecommendationsweresuggestedtostrengthenriskcommunicationincludingbuildingcapacityofnationalfocalpointsofIHRandbeableto:
• conductcomprehensiveIHRawarenessand advocacy activities at all levels (risk detection and communication, joint response and emergency planning and preparedness)
• develop/strengthennationalriskcommunication strategies
• establishcoordinationwithothersectors.
Internal discussion is being held to collaborateandagreeonaframeworktofurtherexpandtrainingopportunityintheareaofriskcommunication
EURO Central Asia: sub regional training workshop
This workshop held in Ashkabad, Turkmenistanfrom29Novemberto2December2011,wasaplannedfollow-up to the outcomes of the Central Asia subregional IHRcorecapacitymeetingheld inTashkent,Uzbekistan spring 2011. Both the workshop andthe meeting were jointly organized by WHO EUROandWHOHQ. Thiswas the first risk communicationworkshop held in the sub region, and for the fiveparticipating countries Kazakhstan, Kyrgyzstan,Tajikistan,Turkmenistan andUzbekistan.The overallpurpose of the training workshop was to supportthe IHR implementation process and core capacitydevelopmentintheparticipatingcountriesaswellasprovide inputs for strengthening risk communicationstructures,communicationchannelsandcoordinationmechanismstorespondtopublichealthemergencies.It also acted as a platform for exchange of bestpracticesandlessonslearnedinriskcommunicationamongtheparticipatingcountries.About30personsparticipatedrepresentingalltheparticipatingMemberStates,UNagenciesaswellasregionalpublichealthinstitutions.
SEAROandWPROWorkshoponriskcommunicationsforpublichealthemergencies
This workshop was organized by SEARO and WPRO and held in Manila, Philippines in November 2011. Risk communication fo-cal points from 19 countries participated to: share and reflect on national experiences from past health emergencies; distill lessons learnt and best practice; and develop work plans for national and regional capacity de-velopment in line with the Asia Pacific Strat-egy for Emerging Diseases (APSED 2010).
The participants concluded that health emergency communications is a fundamen-tal component in managing public health emergencies and in ensuring a sense of trust during times of uncertainty and needs to be institutionalized. As part of the International Health Regulations core capacity require-ments, participants agreed that developing sustainable health emergency communica-tions capacity is essential within the Ministry of Health. Suggestions and recommendations from the workshop are to be incorporated into the APSED work plan on risk communications.

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201132 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201133
CORE CAPACITY DEVELOPMENT
Strengthening the skills and competencies of public health personnel is critical to the sustainment of public health surveillance and response at all levels of the health system and the effective implementation of the IHR.
Human Resources
Country requirements
Throughtherevised IHR, it is requestedthatallMemberStateshavethecapacitytodetectandreportevents thatmay constitute a potential public healthemergencyofinternationalconcern.Sufficienthumanresourcesarekeytoachievethisgoal.
StatesPartiesarerequiredtohavethesufficienthumanresourcesavailabletoimplementIHRcoreca-pacity requirements. This includes the identificationof a unit responsible for the development of humanresourcecapacityincludingfortheIHR.Countriesareadvised to conduct a needs assessment to identifygapsinhumanresourcesandtrainingtomeetIHRre-quirementsanddevelopaworkforceor trainingplanthat includes human resource requirements for IHR.Countriesshouldalsodevelopastrategyorplantoac-cessfieldepidemiologytrainingforoneyearormorein-country,regionallyor internationally.CountriesarealsoencouragedtoallocateaspecificprogrammeandbudgettotrainworkforceforIHR-relevanthazards.
WHO commitments
Strengthening the public health personnelthroughdevelopmentofappropriateknowledge,skillsand competencies is critical for effective implemen-tation of the IHR. Development of human resources
should enable sustainable practice of public healthsurveillance and response at all levels of the healthsystem. Although being cross-cutting by nature, hu-manresourceshavethereforebeendefinedasoneoftheeightessentialcapacitiesthatStatesPartiesneedtostrengthentoachievecompliancewithIHRrequire-ments.
General status in countries
For 2011, 150 Member States have done a selfassessment, which shows a global average score of46%of reaching the requirements of human resour-ces. Ifwebreak thescoresdown toaveragebyWHOregion,wefindthefollowingresults:Africa:33%,the Americas: 58%, the Eastern Mediterranean: 55%, Europe:35%,South-EastAsia:56%andtheWestern Pacific:61%.Whereas58.3%oftherespondentMem-berStatesdeclare tohaveastrategy toaccessfieldepidemiology training (one year or more) in-country,regionally or internationally, only 40.9% confirm tohavingaworkforcedevelopmentortrainingplanthatincludeshumanresourcerequirementsforIHR.

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201134 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201135
CORE CAPACITY DEVELOPMENT
HUMAN RESOURCES
CORE CAPACITY DEVELOPMENT
HUMAN RESOURCES
HIGHLIGHTS
Thedevelopmentof toolsandstrategies tosup-port the reinforcement of human resources is a responsibility of every technical team in the Depart-ment. One team in the department however, has aspecificexpertiseinHRdevelopmentandtrainingandprovides support as required to the technical teamsbygivingguidance,developingtoolsaswellasdesign-ing and implementing courses (i.e. highlighted IHR i-course).
TheworkoftheDepartmentregardingHRdevel-opmentandtrainingcanbeseenalongfouraxes:
01. Development of generic curricula and/or training materials
Genericcurriculaareoftenreferredtoastrainingtoolkitorpackagesandconsistofacollectionoffilestobuilda trainingmoduleorcourse.Allcomponentscanbemodifiedtofitasmuchaspossibletheneedsandthecontextof thetrainingcourse (i.e. language).Training materials can be designed for face-to-facetrainingore-learning.
Examplesofprojects:
• Laboratory Quality Management Systems: development of a training toolkit ≥www.who.int/ihr/training/laboratory_quality/en/•SURVAC- project: design of generic course on surveillance for professionals at intermediary and peripheral levels(seep.22)•Ship Sanitation Certificates: design of a training toolkit (seep.42)• Infectious substances shipping training: design of a course for shippers(seep.39)•BiostatisticCD-ROMforselflearning(seep.24)
02. Organization of specific courses
Theseactivitiestargetaspecificgroupoftraineesat a specific time and place. The courses are oftenorganized in collaboration with external institutionsand sometimes operated through them. Some ofthesecourseslaterleadtothedevelopmentofgenericcurricula.
Examplesofprojects:
• IHR implementation course(seep.35)
• Leadership and management for laboratory directors(seep.38)•Bioriskmanagement(seep.25)• Table top simulation exercises(seep.15)
03. Partnerships and networks
The activities aim at pooling resources and ef-forts from different institutions for the developmentand implementationofHRdevelopmentand trainingstrategiesandtools.
Examplesofprojects:
• Participation in the Third Influenza Training Network meeting: lessons learned on capacity building during pandemic influenza (4-8April2011)•Support to TEPHINET(seep.24)
04. Guidance and support for strategy development
ProvidingguidanceandsupportfordevelopingHRstrengtheningandtrainingstrategiesinrelevantare-asofwork;i.e.definitionofkeyfunctionsandrelatedprofessional categories; development/promotion ofcompetency frameworks for those categories; inven-tory of existing resources and planning for neededworkforce; assessment of pre-service and in-servicetrainingneeds;identificationofeducationandtrainingresources;etc.
Examplesofprojects:
• Epidemiological surveillance: evaluation of training needs in Morocco (seep.24)•Ship inspection: development of a competency framework for ship inspection and delivery of ship sanitation certificates (seep.42)•Risk Communication: development of competency framework
IHRimplementationcourseThe IHR implementation course aims to strengthen critical human
resources engaged to set-up and manage systems for securing global public health under the IHR implementation framework, as well as to develop communication capacities for efficient international collabora-tion. This on-the-job training targets public health professionals, mainly belonging to National IHR Focal Points, but also professionals from other related sectors from national or international organizations, in the public and private sectors.
The third global IHR implementation course, which started in 2011 enrolled 37 participants from all the WHO regions. The course is operated by the HR development and training team, in collaboration with the Uni-versity of Pretoria, South Africa, Georgetown University Law Center, USA, theUniversityofGeneva,Switzerlandand InstitutBioforceDéveloppe-ment, France. During all three IHR i-courses 89 public health profession-als have been trained, coming from 59 different Member States from all the six WHO regions.
A post-training evaluation of the first and second IHR i-courses was conducted during 2011 showing that the course is valuable to the stu-dents. The participants report that in relation to their day-to-day work, the course content was relevant to their work and has given them a global understanding of IHR, allowing them to be more confident when dealing with the topic. Most competencies learned have been put into practiceintheirdailyworkandmaterialfromthecoursere-used.Beingable to exchange with peers during and after the course is underlined as especially valuable.
The IHR i-course is now being adapted for use both at national and regional levels. The first regional adaptation will be for Russian speak-ing countries, and planning has started in collaboration with EURO. The needs analysis will be carried out in Spring 2012 after the end of the 3rd global course, together with the identification of collaborating institu-tions for design and delivery.
Basedonthemodeloftheglobal"IHRImplementationCourse",thecourse is currently being adapted to the national level in Indonesia, target-ing specifically port health staff and surveillance staff at regional level. Other Member States have expressed interest in adapting the course to their needs, and discussions are ongoing.

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201136 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201137
CORE CAPACITY DEVELOPMENT
Laboratory services are part of every phase of alert and response, including de-tection, investigation and response, with laboratory analysis of samples performed either domestically or through Collaborating Centres. States Parties need to establish mechanisms that assure the reliable and timely laboratory identification of infectious agents and other hazards likely to cause public health emergencies of national and in-ternational concern, including shipment of specimens to the appropriate laboratories if necessary. Laboratory quality systems ensure the generation of accurate and reliable results and are the keystone of confidence in laboratory results. During disease out-breaks, laboratories are at the very heart of the public health investigation.
Laboratory
Country requirements
Through the revised IHR,WHO requests that allMemberStateshavethecapacitytodetectandreportevents thatmay constitute a potential public healthemergency of international concern (PHEIC). Thisimplies accurate and sufficiently detailed laboratoryresults, produced either domestically or throughCollaborating Centres. States Parties are advisedto have established policies and strategic plans toimprove the national laboratory system and ensureessential public health functions of laboratories.Laboratorydiagnosticandconfirmatorycapacitymustbe established, and laboratory services available totestforpriorityhealththreats.Qualityofthelaboratorytesting should be ensured by the compliance withnationalorinternationallyrecognizedstandards.Theremust be a system in place for collection, packagingand transportation of clinical specimens across thenationallaboratorynetworkandbeyond.Goodbioriskmanagementpracticesmustbeinplacetoguaranteelaboratorybiosafetyandbiosecurity.
WHO commitments
Under the IHR, WHO is committed to supportMember States in the acquisition and maintenanceof core laboratory capacity for responding to publichealthemergencies,includingmanagementofbioriskinlaboratoryandtransportenvironments.
General status in countries
Aselfassessmentdonebyendof2011showsaglobalaveragescoreof71%of reaching the require-ments of laboratory. If we break the scores down toaveragebyWHOregion,wefindthefollowingresults:Africa:65%,theAmericas:74%,theEasternMediter-ranean:71%,Europe:73%,South-EastAsia:67%andtheWesternPacific:75%.Itisimportanttonotice,thatthesedataareselfreported,andmightbeinaccurate.ThisunderlinestheimportanceforWHOtokeepwork-ingwith thecountries inorder to refineand improvetheaccuracyoftheinformationreported.
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201138 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201139
CORE CAPACITY DEVELOPMENT
LABORATORY
CORE CAPACITY DEVELOPMENT
LABORATORY
HIGHLIGHTS
AFRO and EMRO: Microbiology External Quality Assessment Programmes
InAfrica,aswellasintheEasternMediterraneanRegioncommunicablediseasesconstituteaconsider-ablepublichealthproblem,andoutbreaksposeprom-inenthealthsecuritythreats.Theeconomicandsocialimpactofthesediseases isenormous.Nationalpub-lichealth laboratoriesshouldgeneratedata toguidediseaseprevention,controlandsurveillanceactivities.However in many countries, reliable confirmation ofsuspectedinfectiousdiseasesishamperedbylackofstandardizedmethodsamongotherfactors.
The African External Quality Assessment pro-grammewas launched in 2002 byWHO and theNa-tionalInstituteforCommunicableDiseases,basedonproficiency testing of African national public healthmicrobiology laboratories that routinely investigateepidemic-prone and other communicable diseases.Participation in this programme increased from 30to 46 countries in the African Region between 2002and 2011 and the number of enrolled laboratoriesgrew from39 to93.Theexternalqualityassessmentprogramme inAfricaassessesnationalpublichealthlaboratories'proficienciesarounddetectionofprioritydiseasesofpublichealthimportance:malaria,tuber-culosis, plague, enteric andmeningitis bacterial dis-eases.
The WHO Microbiology EQA programme in theEasternMediterraneanRegionwassimilarlylaunchedin 2005. The programme covers bacteriology: entericandmeningealpathogensandantibioticsusceptibilitytesting, parasitology: stool parasites, leishmaniasis,mycologyandviralserology.ThetechnicalorganizationoftheprogrammeisdonebytwoEasternMediterrane-anRegioncountry reference laboratories: theHealthReference Laboratory of Iran and the Oman CentralPublic Health Laboratory. Four referee laboratoriesfromtheAfrican,EuropeanandtheEasternMediter-raneanRegionsprovideguidanceandexternalqualitycontrolofmaterialssenttoparticipatinglaboratories.The number of participating laboratories is now ex-tendedto23in19EasternMediterraneancountries.
Regional approaches to strengthening national laboratory systems
Under the IHR, countries are obliged to rapidlydetectandreporttotheinternationalcommunityanyeventoroutbreakofinternationalconcern,andaqual-itylaboratorysystemisakeyfactortoensuretimelydi-agnosticofepidemic-pronediseases.Manycountriesstill lackanationalframeworktorunandstrengthentheirnational laboratorysystem.Toavoidfragmenta-tionandstrengthennational laboratoryservices, theWHOofficeinLyonhascooperatedactivelywithWHOregions to initiate and reinforce work in this area.TheLaboratoryQualityManagementSystemTrainingToolkit is intended toprovide comprehensivemateri-alsthatwillallowfordesigningandorganizingtrain-ingworkshopsforallstakeholdersinhealthlaboratoryprocesses, from management, to administration, tobench-worklaboratorians.During2011thehandbookofthistoolkitwasfinalized,andisnowavailablebothelectronically on the IHRweb site aswell as in hardcopy.AFrenchversionofthetrainingtoolkitwasalsomadeavailableduring2011andahandbookisunderway.ARussianversionofthetoolkitwillbemadeavail-ablein2012.
Global Laboratory Directory - GLaD
ThescopeofdevelopingaGlobalLaboratoryNet-worksDirectory (GLaD)was initially tomapandcon-nectlaboratorynetworksthatcanbemobilizedtosup-portepidemic-pronediseasesalertandresponse.Theinitialprojecthadthreemainparts:GLaDMap listingandmappingnetworks,GLaDResourceoffering toolsand documents to manage networks and GLaDSup-port linkingnetworksandsharing information.An in-ternational consultation between the stakeholderswasorganizedinDecember2011torevisittheproject,identifypriorityareasofworkandsuggestalternativeapproaches.
The Leadership and Management Training Course for Laboratory Directors
The WHO office in Lyon organized a meeting inMay2011withpotentialpartnerinstitutionsandtech-nical experts to discuss the concept of a leadershipandmanagementtrainingcourseforlaboratorydirec-torsandotherseniorstaff.Theobjectivesweretoraiseawarenessoftheprojectandtoenablecollectivedis-cussionoftheexpectedcompetenciesoflaboratorydi-rectorsintermsofleadershipandmanagementskills;
andtoexplorewaysofdevelopingandimplementinganappropriatetrain-ingcoursetoaddresstheseneedsbasedonadrafttermsofreference.Theoutcomesofthemeetingincludeddefiningtheleadershipandmanagementskill competencies for laboratorydirectors tobeachievedby the trainingcourse;recommendationsonhowthesecompetencieswouldbeachievedintermsoftypeoftrainingprogramme(s)andcontentoftheprogramme(s);andinputonadraftTermsofReferenceforthetrainingprogramme.
The PulseNet Middle East Network
PulseNet International Network is an early warning system for out-breaks of foodborne disease which includes a network of national andregional laboratory networks dedicated to tracking foodborne infectionsand information sharing worldwide. As a member of PulseNet Interna-tional, PulseNet Middle East is a regional network of public health andfoodregulatoryagencylaboratoriesthatusemoleculartypingmethodsforrapidanalysisandcomparisonofDNA"fingerprints"ofbacteriaforbetter detection and investigation of outbreaks of foodborne illnesses. During2011thefifthstrategicplanningconsultationonPulseNetMiddleEastwasorganizedinMuscat,Oman.MicrobiologistsandepidemiologistsfromtenEasternMediterraneancountriesparticipatedintheconsultationtodiscussprogress, challengesandbarriers encountered in implementingactivitiesandtodevelopcountries’actionplansfor2012.AllmemberlaboratoriesarenowcertifiedbytheUSNavalMedicalResearchUnit3(NAMRU-3)inCairo,EgyptforBioNumericssoftwareanalysisandseverallaboratorieshaveal-readyobtainedcertificationforPFGEofSalmonellaandShigellapathogens.
The WHO Laboratory Twinning Initiative
The InternationalLaboratoryTwinning Initiativeaimstocontribute tothe strengthening of public health laboratories which often have limitedresources.Theprojecttwinslaboratorieswithscarceresourceswithmoredevelopedlaboratories,workingonspecificcollaborativeprojects,basedonanassessmentofneedsandmutuallyagreedpriorities.Throughlaboratorytwinning,referencelaboratoriesfromspecializedinstitutionshelpresource-limited laboratories strengthen their diagnostic capability and scientificexpertisesotheycanbuild theirowncapacitiesat thenational level.Thefundinggrantedforlaboratorytwinningislimited,andoftenusedasseedmoneytogettheprojectstarted.Anumberofthetwinnedlaboratorieshavein addition been able to attract additional funding from other donors toprolongandexpandtheproject.Around50laboratorieshaveparticipatedinthelaboratorytwinninginitiativesinceitstartedin2006,andonehasbeenabletoobtainISO15189accreditation.
WHO transport of infectious substances training and certification (ISST)
The number of competent shippers of infectious substances keepsgrowing.In2011,atotalof164shippersofinfectioussubstanceshasbeencertified.Face-to-faceinfectioussubstancesshippingtrainingcourseswereorganized inmany places: Benin, Brazil, Ghana, theMaldives,Mauritius,
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201140 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201141
CORE CAPACITY DEVELOPMENT
LABORATORY
CORE CAPACITY DEVELOPMENT
Tanzania,andTrinidadandTobago.Thecourseswereheld in several languages, including English, French,Spanish and Portuguese. The electronic refreshercourseisapproachingcompletion.
EUprojectonBioriskManagement
Attheendof2011,theJointActionentitledSup-port of WHO activities in the area of biosafety andbiosecurity in the framework of the EuropeanUnionStrategyagainsttheproliferationofWeaponsofMassDestructionwas completed.With the support of theEU,theseriesofregionalandnationaloutreachwork-shopsonbioriskmanagementforvariousregionsinavarietyofvenuescouldbecontinued.Workshopswereorganized inBrazil, Ghana and theMaldives. BioriskmanagementneedsassessmentvisitswereorganizedinBolivia,IndonesiaandSriLanka.
WHOBioriskManagementAdvancedTrainer Programme
Furthersessionsofthistrainingcoursefortrain-erswasarrangedin2011.Readmoreonpage25.
Support to other WHO programmes and external partners
Collaborations with the Stop TuberculosisProgramme for the development of guidance onbiosafetyrelatedtotuberculosislaboratorydiagnosticproceduresisongoing.Forthecontainmentofvariolavirus, the new protocol for the regular biosafetyassessmentvisitsofthetwoWHOrepositoriesintheRussianFederationandtheUnitedStatesofAmericais being reviewed, in preparation for the next visitsplannedin2012.
Human-animalinterface:Strengtheninglaboratorycapacities
The IDENTIFY project, which is part of the USAID-funded Emerging Pandemic Threats programme is being jointly implemented by the Food and Agriculture Organization of the United Nations, the World Organisation for Animal Health, and WHO. The project aims to strengthen laboratory capacity to detect known pathogens responsible for disease in humans and animals in three geographic re-gions determined by USAID to be at higher risk of emergence of novel pathogens: the CongoBasininCentralAfrica,SoutheastAsiaand selected countries in South Asia. Most of the activities supported by WHO are be-ing implemented by the relevant regional and country offices. As the regional offices have already established their own platforms for capacity-building, and since the objectives of those platforms in terms of laboratory capa-city are fully consistent with IDENTIFY, it has been decided that IDENTIFY will contribute to, and be implemented as, part of these ex-isting platforms. This secures WHO present-ing a single message on capacity building to Member States. IDENTIFY commenced activi-ties in Africa in 2010 and in 2011, the project was introduced to stakeholders in Southeast Asia at a number of meetings. A joint meet-ing of public health and animal health coun-terparts was held in Kuala Lumpur in October 2011. The project is seen as providing a strong impetus for closer cooperation between the public health and animal health sectors in the Region.
The objective of implementing the IHR requirements at points of entry, is to prevent and contain international spread of diseases, and provide response to events commen-surate to public health risks related to international travel and transport. The IHR core capacities at points of entry aims to ensure that conveyances travelling internationally and facilities used by travellers at points of entry are maintained in a sanitary condition and kept free of sources of infection or contamination and if public health events occurs, they are detected early and contained in a timely and adequate manner. This is done by maintaining routine health control measures and developing public health response capacity at designated airports, ports and ground crossings and for travel and transport operations. This includes possible coordinated multisectoral interventions at points of entry facilities and with travellers, conveyances, cargo, goods and postal parcels, as well as specific control measures for vectors and reservoirs.
Points of Entry
Country requirements
Through the revised IHR,allStatesPartiesshalldesignate the international airports and ports, andwhere justified forpublichealth reasons,maydesig-nategroundcrossings,whichwilldevelopspecificca-pacitiesforapplicationofthepublichealthmeasuresrequiredtomanageavarietyofpublichealthrisksandrelatedevents.Also StatePartiesshall identifycom-petentauthoritiesforitsapplicationateachdesignat-edpointofentry.Countrieswithinternationalshippingtraffic,shouldalsoidentifyportsauthorizedtoinspectshipsandissueshipsanitationcertificates,accordingto IHRmodeland requirementsand this informationshouldbesent toWHO forworldwidedissemination,especially among shipping industry and port healthauthorities.Relevantnationallegislation,regulations,administrativeacts,protocols,operationalprocedures
andothergovernmentinstrumentsshouldbeupdatedasneeded.StatePartiesshallalsobecapabletofur-nish to WHO, as far as practicable, when requestedin response to specific potential public health risk,relevant data concerning sources of infection andcontamination, includingvectorand reservoirs,at itspointsofentry,whichcouldresultininternationaldis-easespread.
WHO commitments
The implementationof IHRatpointsofentryre-quiresamultisectoralapproachandWHOleadershipaswellasadvocacy,networkingandcoordinationwithinternationalorganizationsandotherstakeholdersin-volved inpublichealth, travelandtransport. Itseeksglobal harmonization of IHR requirements andWHO

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201142 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201143
guidance tools with other international instrumentsandoperationalproceduresforconveyanceoperatorsandpointsofentrymanagement.WHO iscommittedtopromote international cooperationwithothersec-tors,aswelltosupportcountriesintheirworktocom-plywiththecorecapacitiesofpointsofentry.Inclosecooperation with the regional offices WHO providestechnical advice, training tools and support for theplanning,assessment,developmentandmaintenanceof core capacities for routine preventive and controlmeasures and public health emergency contingencyplandevelopmentatdesignatedpointsofentry.Thisinvolvestheimplementationofshipinspectionandis-suanceof thenewshipsanitationcertificates, intro-ducedbytheIHR2005,aswellasthedisseminationoftechnicalguidanceandIHRrelatedinformation,suchasupdatingthelistofauthorizedports,toissueshipsanitationcertificates,andpromotingandsupportingthe specialized network on public health and ports,airportsandgroundcrossings,forinstancePAGNet.
General status in countries
AselfassessmentperformedbyMemberStatesattheendofDecember2011showsaglobalaveragescoreof59%ofreachingtheoverallnationalrequire-mentsofpointsofentry (communicationandcoordi-nation,routinecapacitiesandcapacitiestorespondtopublichealthevents). IfwebreakthescoresdowntoaveragebyWHOregion,wefindthefollowingresults:Africa:48%,TheAmericas:55%,theEasternMediter-ranean:58%,Europe:67%,South-EastAsia:67%andtheWesternPacific:58%.
HIGHLIGHTS
Core Capacity assessment
During 2011, WHO regional and country officessupportedseveralcorecapacityassessmentsincoun-tries, and the IHR Department participated in ninemissions;toBarbados,Bhutan,China,Egypt,Equato-rialGuinea,Lebanon,SaudiArabia,SouthAfrica,andTurkey. In addition two regional meetings were heldinManilaand forGulfCooperationCouncilcountriesin Riyadh, Saudi Arabia to support work at regional offices. Workshops were also held in Spain and Uzbekistan.
Coordination and cooperation among Public Health and International Civil Aviation Sector
The cooperation with the aviation sector is in-creasingandmainpartnersaretheUNAgencyInter-nationalCivilAviationOrganization(ICAO)andindustryassociations, such as the International AirTransportAssociation (IATA) and the Airports Council Interna-tional(ACI).WHOandICAOhavebeenworkingtogetherin theharmonizationof IHR requirementswith inter-nationalstandardsandrecommendationsandtechni-calguidanceandproceduresrelatedtopublichealthand air travel, such as for the development and im-plementationofpreparednessplansforpublichealthemergenciesinvolvingairtransport.
CAPSCA Project
— Cooperative Agreement for Preventing theSpreadofCommunicablediseases throughAir travel—underthe leadershipof the ICAOand incoordina-tionwithWHOandotherpartnersisaglobalcoopera-tionwiththecivilaviationsector.Thisprojectaimstohelpreducetheriskofseriousspreadofcommunica-blediseasesthroughair travelbymeansofcoopera-tivearrangementsbetweenparticipatingstates.Thisinvolvesseminars,workshopsandassistancevisitsbyaviationandpublichealthexpertsforthedevelopmentandimplementationofcontingencyplansatairports.WHO supports CAPSCAwhile assisting states to im-plementpublichealthemergencyresponseplans forairtransportaspartoftheIHRcorecapacityrequire-mentsforpointsofentry.ThisProjectwasfirstimple-mentedinAsia-Pacific(2006)andAfrica(2007),whiletheRegionoftheAmericaswasincludedin2010.ThefirstmeetingsfortheEuropeanandEasternMediter-raneanRegionswereheldin2011.
Public health emergency response in air travel: field exercise in Spain
This emergency simulation exercise was under-takenbyWHOinclosecollaborationwiththeMinistryofHealth,Spain,joinedbyobserversfromICAOEuropeandpublichealthexpertsfromallWHOregions.Readmoreaboutthisonpage27.
Ship Sanitation
EU SHIPSAN
WHO collaborated closelywith the EUSHIPSANproject,whichwascompleted inOctober2011. Itde-veloped an integrated programme on sanitation andcontrolofcommunicablediseasesonpassengershipsincluding a training programme and a communica-tionnetwork.The lastphaseof this initiative, theEUSHIPSANTRAINETdevelopedaEuropeanmanual forhygiene standards and communicable diseases sur-veillance on passenger ships. Training material wasdeveloped and training given to port health officersinEUandEUROMEDcountries,aswellasmanagersandcrewmembersofpassengershipping lines.Dur-ing 2011, pilot hygiene inspections were conductedonpassengershipssailinginEUwatersbasedontheEuropeanmanualforhygienestandardsandcommu-nicablediseases surveillance onpassenger ships. Inparallel, the project developed and operated a com-munication network for sharing information relatedtopublichealtheventsamongEUcompetentauthori-ties,usedduringrealpublichealtheventsaswellaslargescalepilotexercises.An informationsystemforrecording Ship Sanitation Control Exemption Certifi-cates/ShipSanitationControlCertificateswasdevel-opedbased on theWHOHandbook for inspection ofshipsandissuanceofshipsanitationcertificatesandtherehasbeenanincreasinggrowinginterestbymanyport health authorities, both within and outside theEU,inusingthisdatabase.EUisbuildingontheresultsandexperiencesfromthisprojectintheirprioritiesfor2012undertheEUPublicHealthProgramme.
Contact tracing after exposure to infectious diseases in public ground transport
EU REACT Project
This project supports assessment and devel-opment of core capacities and tools in response toemerging infectious disease and addresses someissues related to IHR implementation and specifi-cally thepackage6,aimedtoproducea riskassess-ment profile for contact tracing related to exposedground transport passengers. An initial proposal foradisease-specificriskassessmenttoolhasbeende-velopedtosupportdecisionmakingwhetherornottoinitiate contact tracing after exposure to infectiousdiseasesinpublicgroundtransport,withparticipationofWHOexperts.Thistoolstillcallsforfurtherdevelop-mentandvalidationforreachingconsensusinitsuse.
Public health emergency response to radionuclear event
Radionuclear accident - earthquake Japan
WHOcontinuestostrengthenitscooperationwithother international and intergovernmental organi-zations. This was particularly important during theFukushimanuclearemergencyinJapan,duringwhichthe Organization collaborated extensively with inter-nationalpartners,andwiththetransportsector (seepage49).
Specialized network on public health and ports, airports and ground crossing - PAGNet
PAGNet is a network that brings together aca-demic institutions and national authorities on thematter of public health, travel and transport relatedissues, responsible for implementing public healthrelatedactivitiesatports,airportsandgroundcross-ings.Thisincludeshelpingpreparednessforresponseto health emergencies affecting international travelandtransport.PAGNetaimstocontributetoprotectingthehealth of populationsand theprevention, detec-tionandcontrolofinternationalspreadofdiseaseanditsagentsthroughinternationaltravelandtransport.PAGNetkickedoffitspilotphaseinJuly,2010,bring-ingtogether127membersfrom43countriestillnow.Itprovidesaglobalplatformforinformationsharing,ex-perienceand lessons learnedexchanging,advancingknowledgeofinternationaltravelandtransportrelat-edpublichealthissue,particularduringpublichealthemergency,whichinturnaddsvaluestostrengtheningIHRimplementationatpointsofentry,The3rdPAGNetmeetingwasarrangedin2011,attendedby57partici-pantsfromWHOregionaloffices,internationalorgani-zationsrelatedtointernationaltravelandtransportaswellasfromnationalinstitutions.PAGNetpilotphasewebsite:≥ www.pagnet.info
List of authorized ports
AllStatesPartiestotheIHRarerequiredtosendtotheWorldHealthOrganizationalistofallportsau-thorizedbytheStatePartyincludingauthorizedportsin all of its applicable administrative areas and ter-ritories to issuethe followingShipSanitationCertifi-
CORE CAPACITY DEVELOPMENT
POINTS OF ENTRY
CORE CAPACITY DEVELOPMENT
POINTS OF ENTRY

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201144 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201145
CORE CAPACITY DEVELOPMENT
POINTS OF ENTRY
cates: ship sanitation control exemption certificates,shipsanitationcontrolcertificates,and,extensionstotheshipsanitationcertificates.Thislistofauthorizedportswasupdatedonaweeklybasisduring2011andthenumberofportsisincreasingyearbyyear.Attheendof2011,thelistincludedaround1600portsin78countries.Workisongoingtolaunchasearchableda-tabaseforallpointsofentryin2012.
Handbook for inspection of ships and issuance of ship sanitation certificates
Thishandbook,publishedin2011, is intendedtobeusedasreferencematerialforporthealthofficers,regulators, ship operators and other competent au-thorities inchargeof implementingthe IHR(2005)atportsandonships.ThehandbookisbasedontheIHR(2005)provisionsregardingshipinspectionandissueofshipsanitationcertificates.
Guide to ship sanitation - third edition
This guide is the global reference on health re-quirements for ship construction and operation. Theprimaryaimoftherevisedguideistopresentthepub-lichealthsignificanceofshipsintermsofdiseaseandto highlight the importance of applying appropriatecontrolmeasures.Theguideisintendedtobeusedasa basis for the development of national approachesto controlling the hazards thatmay be encounteredonships,aswellasprovidingaframeworkforpolicy-making and local decision-making. The guide mayalsobeusedasreferencematerialforregulators,shipoperatorsandshipbuilders,aswellasachecklistforunderstandingandassessingthepotentialhealthim-pactsofprojectsinvolvingthedesignofships.
Review of activities 2011
WHO Global IHR Commitments
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201145

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201146 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201147
WHO GLOBAL IHR COMMITMENTS
As required by IHR (2005), WHO is required to develop and maintain a global frame-work to detect, assess and provide a coordinated response to events that may constitute a public health emergency of international concern. The framework is based on strong national public health systems and capacities and an effective international system for coordinated response. This international system must be able to continuously assess the global context of public health risks (global risk assessment) and be prepared to respond rapidly to unexpected, internationally-spreading events and to contain specific public health threats.
WHO Global IHR Commitments
HIGHLIGHTS
Decision instrument: Annex 2
Whenassessingpublichealtheventsfornotifica-tiontoWHO,StatesPartiesarerequiredtousethede-cisioninstrumentcontainedinAnnex2oftheRegula-tions.ThepurposeoftheWHOguidanceonAnnex2istohelpnationalauthoritiestousethedecisioninstru-ment.TheguidancedocumentistargetedtoNationalIHRFocalPointsandothersresponsibleforassessingtheneedtonotifyWHOofpublichealtheventsundertheRegulations.
A summary of the studies on the evaluation ofthefunctioningofAnnex2oftheIHRwasprovidedtothefirstIHRReviewCommitteeforconsideration.Theaggregated results helped the Review Committee informulating recommendations to guide WHO in pro-vidingsupport toStatesParties in implementing theIHReventassessmentandnotificationprocess.Theserecommendations are reflected in the Review Com-mittee's report to the64thWorldHealthAssembly. Inaddition, results about the reliability and validity of
the notification assessment process utilizing Annex2havebeenpublishedintheWHOBulletin.Moreover,information about the level of awareness and know-ledgeamongNFPsofAnnex2,thepracticaluseofthetool,theiractivitiestakentoimplementit,anditsper-ceivedusefulnessanduser-friendlinessissoontobepublished in the peer-reviewed journalGlobalizationandHealth.
IHR Roster of experts
TheIHRRosterofExperts,requiredbytheIHRtoprovide a pool of expertise to serve on IHR commit-tees,was first established in 2007 and in 2011 newproceduresweredevelopedandimplementedfortherenewal or discontinuation of those roster expertswhoseinitialfouryeartermhadexpired. Infollow-upoftherecommendationsoftheIHRReviewCommittee,theareasofexpertiserepresentedintherosterarebe-ingreviewedandexpandedsothattherostercanofferthebestpossibleselectionswhensettingupanEmer-gencyorReviewCommittee.Similarlytheprocedurestoscreenforpotentialconflictsofinterestshavebeen
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201146

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201148 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201149
WHO GLOBAL IHR COMMITMENTSWHO GLOBAL IHR COMMITMENTS
revisedtoassisttheearlieridentificationofsuchpo-tentialconflictsduring theestablishmentofany IHRcommittee.
IHR Emergency Committee
TheInternationalHealthRegulationsobligeWHOtoestablishanemergencycommittee thatshallpro-videitsviewsonwhetheraneventconstitutesapublichealthemergencyofinternationalconcern;thetermi-nation of a public health emergency of internationalconcern; and the proposed issuance, modification,extension or termination of temporary recommenda-tions.TheEmergencyCommittee shall be composedof experts selected from the IHR expert roster and,whenappropriate,otherexpertadvisorypanelsoftheOrganization.Noemergencycommitteewasconvenedduring2011.
IHR Review Committee
TheInternationalHealthRegulationshaveaprovi-sionthatcallsforareviewoftheirfunctioningnolaterthanfiveyearsaftertheirentryintoforce.In2008,theWorldHealthAssemblydecidedthat thisfirst reviewshouldbeundertakenbytheSixty-thirdWorldHealthAssemblyinMay2010.Thisprovisionandthisdecisionwereinplacepriortotheonsetofthe2009H1N1influ-enzapandemic,and,duringtheJanuary2010sessionoftheExecutiveBoard,itwasdecidedthatthesched-uledIHRreviewshouldalsobeusedtoassessthein-ternationalresponsetotheinfluenzapandemic.
The2010 IHRActivityReportdescribed thecon-vening and work of this IHR Review Committee es-tablished to provide an external evaluation of thefunctioning of the IHR and global responses to the Influenza pandemic of 2009¹. The fourth and finalmeeting of the IHR Review Committee took place inGenevawithaplenarysessionon28March²followedbydeliberativemeetingsof theCommitteemembersto finalize their report. This final report³ was trans-mittedtotheWorldHealthAssemblybytheWHODi-rector- General whereMember States endorsed theCommittee's work including its findings and recom-mendations.Keyfindingsof the IHRReviewCommit-teewere: i) the IHR helped better prepare theworldto cope with public health emergencies; ii) WHO
performed well in many ways during the pandemic,confronted systemic difficulties and demonstratedsome shortcomings; iii) the world is currently ill-prepared to respond to a severepandemic or to any other public health emergency on a similarly globaland threatening scale. The recommendations werepresented to the Assembly by the Chairman of the Review Committee, Professor Harvey Fineberg andare summarized in thebox.These recommendations provideanimportantfocusforWHOactivitiesin2011andplanningforthenewbiennium2012-2013.
Summary of IHR Review Committee Recommendations:
a. For the IHR
• Accelerateimplementationofcorecapacities requiredbytheIHR• EnhancetheWHOEventInformationSite• Reinforceevidence-baseddecisionsontraffic andtrade• Ensurenecessaryauthorityandresourcesforall NationalIHRFocalPoints
b. For WHO pandemic preparedness
• StrengthenWHO'sinternalcapacityfor sustainedresponse• Improvepracticesforappointmentofan emergencycommittee• Revisepandemicpreparednessguidance• Developandapplymeasurestoassessseverity• Streamlinemanagementofguidancedocuments• Developandimplementastrategic,organization widecommunicationspolicy• Encourageadvanceagreementsforvaccine distributionanddelivery
c. For the global response
• Establishamoreextensiveglobal,publichealth reserveworkforce• Createacontingencyfundforpublichealth emergencies• Reachagreementonthesharingofvirusesand accesstovaccinesandotherbenefits• Pursueacomprehensiveinfluenzaresearchand evaluationprogramme
Global partnerships
WHOcontinuestostrengthenitscooperationwithother international and intergovernmental organiza-tions.ThiswasparticularlyimportantduringtheFuku-shimanuclearemergency inJapan,duringwhichtheOrganizationcollaborateddirectlywiththeIAEA,whilealso participating as a member of the Inter-AgencyCommitteeonRadiologicalandNuclearEmergencies,a coordinatingbody for the existing international ar-rangementsforpreparednessandresponsetoradio-logical and nuclear emergencies. The nuclear eventalso stimulated extensive collaboration with inter-nationalpartners in the transport sector (seearticlebelow).ProgressisalsobeingmadeonWHO’scollabo-rationwithotherorganizationsandpartnerstotacklehealth risks at the human–animal–environmentalinterface.Theseeffortsincludethetripartitearrange-mentswithTheUNFoodandAgricultureOrganization(FAO) and TheWorld Organisation for Animal Health(OIE).
Publichealthemergencyresponsetoradionuclearevent
As part of the response efforts to the earthquake and nuclear accidents in Japan in March 2011, several technical areas at WHO HQ, in coordination with WHO West Pacific Regional Office and its global network of ex-perts worked in close collaboration with the Japanese authorities and other International Agencies and stakeholders, at the highest level of the organizations, to gather and dis-seminate updated information and best risk assessment results. The work of WHO is sup-ported by a global network comprising more than 40 specialized institutions in radiation emergency medicine. A specific transporta-tion working group supported by WHO was organized with different agencies and chaired by the International Civil Aviation Organiza-tion (ICAO) arranging weekly conference calls involving ICAO, IAEA, WHO, IMO, WMO, UNWTO, ILO, IATA, ACI. The group exchanged updated information from different sources and pro-duced harmonized notes for public informa-tion to websites and press. That collaborative response and ‘one voice’ public information message with concerned United Nations agencies and travel and transport industry proved successful in reassuring the travel-ling public and were very important during the event, since the risk perception from different sectors and countries were fear factor and key for overreaction. The existing networks PAGNet and CAPSCA (see more information on pages 42-43) helped in informing and re-ceiving good information from national au-thorities. Two countries, Canada and Germany issued specific technical advice for dealing with ships and decontamination procedures.
1.2010IHRActivityReportpages5-72.www.who.int/ihr/4th_meeting/en/index.html3.http://apps.who.int/gb/ebwha/pdf_files/WHA64/A64_10-en.pdf

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201150 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201151
Future Directions
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201151

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201152 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201153
Future DirectionsThe uniting of the IHR Coordination and Global Alert and Response Departments will
ensure better coordination between building the necessary public health core capaci-ties at national level, and global response to public health events that may constitute a public health emergency of international concern.
In the year ahead, GCR will continue to work with the regional offices to assist coun-tries — particularly those who are most vulnerable — to acquire and strengthen the IHR core public health capacities, which are the cornerstone of a strong national pub-lic health system. This work is informed by the analysis and recommendations of the External Review Committee, which serves to guide WHO in further strengthening the IHR framework so that it may better protect the world against health events we may face in the 21st century.
However, WHO cannot fulfill this ambition alone ; the Organization will continue to work with its international, multi-sectoral network of partners and will strive to engage more partners in its mission to achieve global health security.
FUTURE DIRECTIONS
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201152
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201154 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201155
Annexes
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201155

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201156 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201157
IHR Publications and Reference Tools
ANNEXES
01. General IHR guidance and monitoring tools
Checklist and indicators for monitoring progress in the development of IHR core capacities in States Parties
The revised versionof the IHRmonitoring frameworkhasbeen releasedand isavailableonline.This referencedocumentproposesa frameworkandprocesses forStatesPartiestomonitorthedevelopmentoftheircorecapacitiesatthenational,in-termediateandlocalcommunity/primaryresponse.≥www.who.int/ihr/IHR_Monitoring_Framework_Checklist_and_Indicators.pdf
IHR key publications 2007-2011
A new leaflet gives an overview of key IHR publications and reference tools developedfrom2007–2011bytheIHRCoordinationDepartmentandotherWHOpro-grammes that support IHR implementation in countries. Many of these tools were developedinpartnershipwithcollaboratingorganizations.Theleafletgivesoverviewofallthelanguageversionsofthedocuments.≥www.who.int/ihr/publications/ihr_key_publications/en/index.html
IHR core capacities: an introduction in 13 flashcards
This interactiveCD-ROMwasdesignedtogiveanoverviewofthe13corecapa- cityrequirementslaidoutintheIHR.Structuredasaquiz,theflashcardsprovidebasicinformationabout thecapacitiesaswellas linksto toolsandtechnicalguidancetosupportIHRimplementation.Toobtainacopycontact≥[email protected]
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201156

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201158 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201159
ANNEXES
IHRPUBLICATIONSANDREFERENCETOOLS
ANNEXES
IHRPUBLICATIONSANDREFERENCETOOLS
02. Laboratory, biosafety and biosecurity
Laboratory quality management system handbook
This Laboratory quality management systemhandbookisintendedtoprovideacomprehensiveref-erenceonlaboratoryqualitymanagementsystemforall stakeholders in health laboratoryprocesses frommanagementtoadministrationtobench-worklabora-torians. It covers topics thatareessential forqualitymanagementofapublichealthorclinical laboratory.TheyarebasedonbothISO15189andCLSIGP26-A3 documents. The handbook is linked to the trainingtoolkiton laboratoryqualitymana-gementsystem. Itisavailablebothinprintandelectronicversions.≥www.who.int/ihr/publications/lqms/en/index.html
Laboratory quality management system training toolkit: French version
Originally released in English in 2010, a Frenchversionofthistoolkitisnowavailable.Itaimstotrainlaboratory managers, senior biologists, and tech-nologists in quality management systems as a steptowards obtaining international recognition, a stepthatall countriesshould take.This training toolkit isintendedtoprovidecomprehensivematerialsthatwillallowfordesigningandorganizingtrainingworkshopsfor all stakeholders in health laboratory processes,frommanagement, to administration, to bench-worklaboratorians.Thetoolkitwasdevelopedthroughcol-laborationbetweenWHO,theUSCentersforDiseaseControlandPrevention(CDC)andtheClinicalandLab-oratoryStandardsInstitute(CLSI).≥www.who.int/ihr/training/laboratory_quality/fr/index.html
Infectious substances shipping training - a course for shippers: Revised edition
A revised edition of the Infectious substanc-es shipping training - a course for shippers is nowavailable on the IHR web site. The training is avail-able in English, French, Spanish, as well as Portu-guese.WHOcontributestothedevelopmentofUnited Nations Model Regulations for the transport of in-fectious substances. These Model Regulations arethe basis for international and national regulationsaddressing transportbyair, road, rail, sea.Toensurethat this information is available to shippers of in-
oftheIHR(2005).Printcopiescanbeorderedbysendingane-mailtoWHOPressat: ≥[email protected]
04. Travel and health
International travel and health - 2011 edition
The yearly publication, International travel and health, is a WHO bestseller. Itcoversallthemainhealthriskstotravelersandincludesdescriptionsoftherelevantinfectiousdiseases, includingcausativeagents,modesof transmission,clinical fea-tures,geographicaldistributionandprophylacticandpreventivemeasures.
The2011editionincludesaglobalrevisionofyellowfeverriskaswellasupdatesonmalariariskandprevention.Italsoprovidesinformationoninfectiousdiseasesandonallvaccinepreventablediseasesaswellasonvaccines.Theinformationfortravel-lerswithHIV/AIDS,hasalsobeenrevisedforthenewedition.
Thewebpagesof International travelandhealth,updated throughout theyear,nowfeaturesinteractivediseasedistributionmaps,andregularupdatesfortravellers.International travel and healthisavailableinprintandonline.≥www.who.int/ith
Revised recommendations for yellow fever vaccination for international travellers
Continuedreportsofrarebutseriousadverseeventsassociatedwithyellowfevervaccineand thechangingepidemiologyof thediseasehavehighlighted theneed torevisitcriteriaforthedesignationofareaswherethere isariskofyellowfevervirus activity,andtorevisethevaccinerecommendationsforinternationaltravel.Therecom-mendationsofaworkinggroupofinternationalexpertsconvenedbyWHOhavebeenpublished in the Weekly Epidemiological Record. These recommendations include criteriaforthedesignationofyellowfeverrisk,specificchangestotheclassificationofareaswithriskforyellowfevervirustransmission,andrevisedvaccinationmapsforinternationaltravel.
•Weekly Epidemiological Record: www.who.int/wer/2011/wer8637.pdf• WER: www.who.int/wer/2011/wer8637.pdf • The Lancet: www.lancet.com/journals/laninf/article/PIIS1473-3099%2811%2970147-5/fulltext • WHO International travel and Health, 2011 edition • Country list: www.who.int/ith/chapters/ith2011countrylist.pdf • Annex 1: www.who.int/ith/chapters/ith2011annexs.pdf • Yellow fever map Africa: gamapserver.who.int/mapLibrary/Files/Maps/ITH_YF_vaccination_africa.png• Yellow fever map Americas: gamapserver.who.int/mapLibrary/Files/Maps/ITH_YF_vaccination_americas.png
Saudi Arabia - Hajj pilgrimage
RequirementsandrecommendationsforentryvisasfortheHajjseasonsin2011havebeenpublishedintheWeeklyEpidemiologicalRecord(WER).
fectious substances, WHO has developed a trainingcourse. The course is generally given in a classroomsetting,andparticipantshaveanopportunitytoprac-tice package assembly and completion of shippingdocumentation. The course is divided into modules addressing the classification, documentation, mark-ing,labelling,packagingofinfectioussubstances,andthepreparationofshipmentsrequiringtheuseofdryice.Thematerialisavailabletotrainerswishingtopro-vide training courses for shippers of infectious sub-stances.≥www.who.int/ihr/i_s_shipping_training/en/
Guidance on regulations for the transport of infectious substances: Spanish version
The Guidance on regulations for the transportof infectious substances 2011-2012 (Applicable asfrom 1 January 2011) already available in Englishand French, is now available in Spanish. The docu-ment provides information for identifying, classify-ing, marking, labeling, packaging, documenting andrefrigerating infectious substances for transporta-tionandensuring their safedelivery. It alsoprovidespractical guidance to facilitate compliance with ap-plicableinternationalregulationsforthetransportof infectioussubstancesbyallmodesoftransport,bothnationallyandinternationally,andincludethechangesthatapplyfrom1January2011andreplacesthedocu-ment issuedbytheWorldHealthOrganization(WHO)in2008(documentWHO/CDS/EPR/2008.10).Thispub-lication,however,doesnotreplacenationalandinter-nationaltransportregulations.≥www.who.int/ihr/publications/who_hse_ihr_20100801/es/index.html
03. Ports, airports and groundcrossings
Handbook for inspection of ships and issuance of ship sanitation certificates
The print version of this handbook was relea-sed in 2011. The handbook serves as a referencetool for port health officers, regulators, ship opera-tors and other competent authorities in charge ofimplementing the IHR (2005) at ports and on ships.Thehandbook is based on the IHR (2005) provisionsregarding ship inspection and issue of SSCs. Theyprovide guidance for preparing and performing theinspection, completing the certificates and apply-ing public health measures within the framework

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201160 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201161
05. Other training and self-learing tools
WHO training evaluation guide
TrainingisconductedthroughoutWHO,targetingbothWHOstaffmembersandexter-nalhealthprofessionalsaroundtheworld.Yetthefollow-uptothistrainingremainsa challenge. Evaluating the impact of training often seems second priority, even if donors,partners,participants,aswellastheglobalcommunity increasinglyneedtoknow if the traininghasbeeneffectiveandmadeadifference.TheWHOevaluationtrainingguideisadocumentdesignedtoencouragetrainingdesignersandmanagerstoplanandconductevaluation.TheguidewasdevelopedbyWHOprofessionalsbasedontheirexperiencesinconductingandfollowinguptrainingoutcomes.Itisaworkinprogressandwillberevisedbasedonthefeedbackfromtheusersofthisguide.
Biostatistics: New CD-ROM for self-learning
Anew version of a self-learningCD-ROMonbiostatistics is nowavailable.Themainobjectiveof theself learningprogramme is tounderstand thepurposeofbio-statisticsthroughrealisticcasesandtoacquirebasicbiostatisticsskillsthatcanbeappliedtowork.Thetargetaudiencesaremedicalandbiomedicalstudents, labora-tory specialists and other professionals who need to use or understand basic bio-statistics.However,itmayalsobeahelpfulremindertoepidemiologists.Thissecond versionoftheself-learningprogrammehasbeenco-producedbyWHOandtheAgencedeMédecinePréventive(AMP).IthasbeendesignedanddevelopedinsuchawaythattraineescanworkindependentlyusingonlytheCD-ROMwhennobookortutorisavail-able.TraineescansolvethesixproblemswiththeresourcesprovidedintheCD-ROMthrough142knowledgesheets. ForfurtherinformationaboutIHRguidanceandreferencetoolscontact:≥[email protected]
ANNEXES
IHRPUBLICATIONSANDREFERENCETOOLS
ANNEXES
Collaborating institutionsInstitution Acronym City Country
• AcademicCentreforTravelMedicine&Vaccines,RoyalFree
&UniversityCollegeMedicalSchool,UniversityCollege RFUCMS London theUnitedKingdom
• AfricanBiologicalSafetyAssociation AfBSA Nairobi Kenya
• AfricanCentreforIntegratedLaboratoryTraining ACILT Johannesburg SouthAfrica
• AfricanFieldEpidemiologyNetwork AFENET Kampala Uganda
• AgenceFrançaisedeDéveloppement AFD Paris France
• AgencyofPreventiveMedecine AMP Paris France
• AirportsCouncilInternational ACI Geneva Switzerland
• AmericanBiologicalSafetyAssociation* ABSA Mundelein theUSA
• AmericanSocietyforMicrobiology ASM Washington,DC theUSA
• AsianPacificBiosafetyAssociation A-PBA Singapore Singapore
• Associationfrançaisedenormalisation AFNOR Paris France
• AssociationofPublicHealthLaboratories APHL Washington,DC theUSA
• AssociationofUKPortHealthAuthorities APHA London theUnitedKingdom
• Bill&MelindaGatesFoundation B&MGF Seattle theUSA
• Bioforce Lyon France
• BiologicalandToxinsWeaponsConvention BTWC Geneva Switzerland
• CanadianFieldEpidemiologyProgram CFEP/PHAC Ottawa Canada
PublicHealthAgencyofCanada
• CarribeanEpidemiologyCentre CAREC Port-of-Spain TrinidadandTobago
• CenterforDiseaseControl Tehran theIslamicRepublicofIran
• CentersforDiseaseControlandPrevention,USA CDC Atlanta theUSA
• CentersforDiseaseControlandPreventionFoundation,USA CDCF Atlanta theUSA
• CentralPublicHealthLaboratory CPHL Muscat Oman
• CentrePasteurduCameroun Yaoundé Cameroon
• CityUniversity London theUnitedKingdom
• ClinicalandLaboratoryStandardsInstitute CLSI Wayne theUSA
• ConnectingHealthOrganizations
forRegionalDiseaseSurveillance CHORDS Washington theUSA
• CounciloftheEuropeanUnion Brussels Belgium
• CruiseLineInternationalAssociation,Inc. CLIA FortLauderdale theUSA
• DepartmentofHealthandHumanServices DHSS Washington,DC theUSA
• DetNorskeVeritasFoundation DNV Singapore Singapore
• EmoryUniversitySchoolofMedicine Atlanta theUSA

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201162 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201163
ANNEXES
COLLABORATINGINSTITUTIONS
ANNEXES
COLLABORATINGINSTITUTIONS
Institution Acronym City Country
• Epicentre Paris France
• EuropeanBiosafetyAssociation* EBSA Frankfurt Germany
• EuropeanCentreforDiseasePreventionandControl ECDC Stockholm Sweden
• EuropeanCommission EC Brussels Belgium
• FondationMérieux Lyon France
• FoodandAgricultureOrganizationoftheUnitedNations FAO Rome Italy
• FrenchFoodSafetyAgency AFSSA Maisons-Alfort France
• GeneralAdministrationofQualitySupervision,
InspectionandQuarantineofthePeople'sRepublicofChina AQSIQ Beijing China
• GenevaUniversityHospitals,
DepartmentofInternalMedicine,
Serviceforthepreventionandcontrolofinfections HUG Geneva Switzerland
• GenevaUniversity,MedicalSchool,
InstituteofSocialandPreventiveMedicine UNIGE/IMSP Geneva Switzerland
• GeorgetownUniversityLawCentre,
O'NeillInstituteforNationalandGlobalHealthLaw Washington,DC theUSA
• GlobalHealthSecurityActionGroupLaboratoryNetwork GHSAG Ottawa Canada
• GlobalHealthSecurityInitiative GHSI Washington,DC theUSA
• HamburgPortHealthCenter Hamburg Germany
• HealthProtectionAgency HPA London theUnitedKingdom
• HealthReferenceLaboratory Tehran theIslamicRepublicofIran
• Hôpitald'InstructiondesArmées,Laveran HIA Marseille France
• HospicesCivilsdeLyon,HôpitaldelaCroix-Rousse,
CentredeBiologieNord Lyon France
• HospitalforTropicalDiseases,
DepartmentofClinicalParasitology HTD London theUnitedKingdom
• IngénieurssansFrontières ISF Brussels Belgium
• InstitutdeMédecineTropicale
duServicedeSantédesArmées IMTSSA Marseille France
• InstituteforPublicHealthSurveillance InVS Saint-Maurice France
• InstituteofPublicHealthResearch IPHR Tehran theIslamicRepublicofIran
• InstituteofVirologyandImmunoprophylaxis IVI Mittelhäusern Switzerland
• InstitutPasteurdeBangui Bangui CentralAfricanRepublic
• InternationalAirTransportAssociation IATA Geneva Switzerland
• InternationalAssociationofIndependentTankerOwners INTERTANKO London theUnitedKingdom
• InternationalAssociationofNational
PublicHealthInstitutes IANPHI Atlanta theUSA
• InternationalCentreforDiarroealDiseaseResearch ICDDR Dhaka Bangladesh
• InternationalCivilAviationOrganization ICAO Montreal Canada
• InternationalCouncilfortheLifeSciences ICLS Washington,DC theUSA
• InternationalLabourOrganisation ILO Geneva Switzerland
• InternationalMaritimeOrganization IMO London theUnitedKingdom
• InternationalShippingFederation ISF London theUnitedKingdom
• InternationalSocietyofTravelMedicine ISTM Geneva Switzerland
• InternationalUnionofRailwayMedicalServices UIMC Bern Switzerland
• InternationalUnionofRailways UIC Paris France
• IstitutoSuperiorediSanità ISS Rome Italy
• JointUnitedNationsFoodandAgricultureOrganization
InternationalAtomicEnergyAgencyProgramme FAO/IAEA Vienna Austria
• LausanneUniversity,InstituteofHealthEconomics
andManagement IEMS Lausanne Switzerland
*locationfollowingtotherotationofthepresidency
Institution Acronym City Country
• NationalBiosafetyAssociationofBrazil ANBio RiodeJaneiro Brazil
• NationalHealthInstituteDrRicardoJorge NHI Lisbon Portugal
• NationalHealthSurveillanceAgency ANVISA Brasília Brazil
• NationalInstituteforCholeraandEntericDiseases NICED Calcutta India
• NationalInstituteforCommunicableDiseases
NationalHealthLaboratoryService NICD/NHLS Johannesburg SouthAfrica
• NationalInstitutesofHealth NIH Bethesda theUSA
• NationalMicrobiologyLaboratory NML Winnipeg Canada
• NationalSchoolofPublicHealth Athens Greece
• NationalTravelHealthNetworkandCentre NaTHNaC London theUnitedKingdom
• NationalUniversityHealthSystem,DivisionofInfectiousDiseases Singapore Singapore
• NoguchiMemorialInstituteforMedicalResearch NMIMR Accra Ghana
• PanAmericanFoot-and-MouthDiseaseCenter PANAFTOSA RiodeJaneiro Brazil
• PanafricanInstituteforDevelopment PAID Ouagadougou/ BurkinaFaso/
Douala Cameroon
• PasteurInstitute IP Paris France
• PathWestLaboratoryMedicine WA Perth Australia
• PublicHealthAgencyofCanada Winnipeg Canada
• ResearchInstituteforTropicalMedicine,
MolecularParasitologyLaboratory RITM Muntinlupa thePhilippines
• RobertKochInstitute RKI Berlin Germany
• RoyalTropicalInstitute Amsterdam Netherlands
• SandiaNationalLaboratories Sandia Albuquerque theUSA
• SecretariatoftheBaselConvention Geneva Switzerland
• SpiezLaboratory Spiez Switzerland
• StateResearchCenterofVirologyandBiotechnology VECTOR Novosibirsk Russian
• SwedishInstituteforInfectiousDiseaseControl SMI Solna Sweden
• SwissFederalOfficeofPublicHealth FOPH Bern Switzerland
• TehranUniversityofMedicalSciences Tehran theIslamicRepublicofIran
• TemasecLifeSciencesLaboratory TLL Singapore Singapore
• TheEasternMediterraneanPublicHealthNetwork Emphnet Amman Jordan
• TheInternationalCriminalPoliceOrganization INTERPOL Lyon France
• TheUnitedKingdomNationalExternalQuality
AssessmentServiceformicrobiology UKNEQAS London theUnitedKingdom
• TrainingProgramsinEpidemiologyandPublicHealth
InterventionsNetwork,Inc. TEPHINET Atlanta theUSA
• UnitedNationsCommitteeofExpertsfortheTransport
ofDangerousGoods UNCETDG Geneva Switzerland
• UnitedStatesAgencyforInternationalDevelopement USAID Washington,DC theUSA
• UnitedStatesFoodandDrugAdministration FDA Washington,DC theUSA
• UnitedStatesNavalMedicalResearchUnit3 NAMRU-3 Cairo Egypt
• UnitedStatesStateDepartment Washington,DC theUSA
• UniversalPostalUnion UPU Bern Switzerland
• UniversityofMassachusetts Massachusetts theUSA
• UniversityofOttawa uOttawa Ottawa Canada
• UniversityofPretoria,SchoolofHealthSystemsandPublicHealth SHSPH Pretoria SouthAfrica
• UniversityofSydney Sydney Australia
• UniversityofThessaly Athens Greece
• UniversityofZurich UZH Zurich Switzerland
• WorldOrganizationforAnimalHealth OIE Paris France
• WorldTourismOrganization WTO Madrid Spain

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201164 INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201165
Financial summary
ANNEXES
INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201165
Expenditure by project area 2010 - 2011
Total contributions for 2010 - 2011 by source of funding USD 36 156 259
ManagementandAdministration
Communications
LaboratoryAlliancesandBiosafety
NationalCapacityMonitoring
Regulations,ProceduresandInformation
LaboratoryQualityandManagementStrengthening
NationalSurveillanceandResponseStrengthening
Ports,AirportsandGroundCrossings
FrenchGovernment
GrandLyon
Rhônedépartment
Rhône-AlpesRegion
InstitutPasteur
GTZ
EuropeanCommission
GatesFoundation
UsCDC
USA
Canada
Japan
WHO
Others(China,UK,NL,IHRCourse,Pulsenet)
20%
4%
16%
8%19%
13%
14%
6%
26%
3%
2%
2%
2%
18%
14%
3%
13%
3%
2%1%
4%
7%

INTERNATIONAL HEALTH REGULATIONS COORDINATION DEPARTMENT ACTIVITY REPORT 201166
International Health Regulations Coordination Department
WHO Lyon Office
58 avenue DebourgF-69007 Lyon - France
tel : +33 4 72 71 64 70fax : +33 4 72 71 64 71
www.who.int/ihr/lyon
WHO Geneva
Avenue Appia 20CH-1211 Geneva 27 Switzerland
tel : +41 22 791 21 11fax : +41 22 791 31 33
www.who.int/ihr
WHO - IHR Training Site
http://extranet.who.int/ihr/training





























