Embed Size (px)
Citation preview
Neurosurgery Publish Ahead of PrintDOI: 10.1227/NEU.0b013e3182093355
ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.
Page 1
Short Segment Internal Maxillary Artery to Middle Cerebral Artery Bypass: A Novel Technique for Extracranial-to-Intracranial Bypass Saleem I. Abdulrauf, M.D., Justin M. Sweeney, M.D., Yedathore S. Mohan, M.D., M.S., Sheri K. Palejwala, B.S.
Saint Louis University Center for Cerebrovascular and Skullbase Surgery Saint Louis University School of Medicine Saint Louis, MO Saleem I. Abdulrauf [email protected] (314) 268-7888 Professor, Neurological Surgery Director, Saint Louis University Center for Cerebrovascular and Skull Base Surgery Saint Louis University School of Medicine St. Louis, Missouri, USA

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.
Page 2
Objective and Importance: Traditional high flow extracranial-to-intracranial (EC-IC) bypass procedures require a cervical incision and long (20-25cm) radial artery or saphenous vein graft. This technical note describes a novel EC-IC bypass technique using a short-segment (8-10cm) of the radial artery to anastomose the internal maxillary artery (IMAX) to the middle cerebral artery (MCA). The purpose of introducing this technique is to make the standard high flow EC-IC bypass, a relatively extensive neurosurgical procedure, less invasive.
Clinical Presentation: Anatomic dissections were performed on 6 cadaveric specimens to assess the location of the IMAX artery using an extradural middle fossa approach. Subsequently, the procedure was implemented in a patient with a giant fusiform internal carotid artery aneurysm.
Technique: A straight line was drawn anteriorly from the V2/V3 apex along the inferior edge of V2. The IMAX was found 8.6mm on average, anteriorly from the lateral edge of the foramen rotundum. We drilled to a depth of 4.2mm on average to find the medial extent of the artery and then lateral and deep drilling exposed an average of 7.8mm of graft. The IMAX was consistently found running just anterior and parallel to a line between the foramens rotundum and ovale. In the clinical case presented, both intraoperative ICG and postoperative conventional angiography revealed a patent graft. The patient did well clinically without any new deficits.
Conclusion: The advantages of this new technique include the avoidance of a long cervical incision and potentially higher patency rates secondary to shorter graft length than currently practiced.
Short Title: IMAX to MCA bypass Keywords: extracranial-to-intracranial bypass, giant aneurysm, internal maxillary artery,
minimally invasive
Yaşargil performed the first extracranial-to-intracranial procedure using a superficial temporal artery (STA) to middle cerebral artery (MCA) shunt on October 30, 1967, while Lougheed and colleagues reported the first successful high flow common carotid to intracranial carotid bypass using a saphenous vein graft in 1971.1,2 Sekhar et al. then detailed the use of radial artery grafts for high flow bypasses from the external carotid artery (ECA) to the MCA, for the treatment of large intracranial aneurysms.3 EC-IC bypasses have since been performed for a wide array of pathologies including skull-base neoplasms, atherosclerotic carotid disease, and cerebrovascular lesions.4-12 The cerebral revascularization procedure currently requires graft vessel harvesting, cervical incision for the proximal anastomosis, craniotomy for distal anastomosis, and parent vessel occlusion. In this report, we illustrate a technique that avoids a long cervical incision and allows for purely intracranial extradural access to the internal maxillary artery (IMAX) to perform a short segment high flow anastomosis from it to the middle cerebral artery (MCA), using a radial artery graft.
For the standard superficial temporal artery (STA)-MCA bypass procedure, as described by Yaşargil, which required a conventional craniotomy, we introduced the concept of performing the procedure through a burr-hole sized craniectomy to make it more minimally invasive.13 Similarly, for high flow bypass, the introduction of this new technique is an attempt to transform what is considered an extensive neurosurgical procedure, slightly less invasive.

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.
Page 3
Methods Prior to clinical application of our bypass, we performed a series of 6 adult cadaveric
dissections. The IMAX was dissected via a middle fossa extradural approach in the cadaveric specimens in order to elucidate the middle fossa surface landmarks, location, and depth of the artery (Figures 1 and 2). This methodology was subsequently implemented in a clinical case as outlined below.
Results We drew a straight line extending anteriorly from the V2/V3 apex along the inferior edge of V2. The distance from the V2/V3 apex to the lateral rotundum was 7.8mm ± 3.033mm. The distance from the lateral edge of the foramen rotundum to the medial extent of the IMAX was 8.6mm ± 2.074mm anteriorly. We drilled to a depth of 4.2mm ± 1.304mm into the greater wing of the sphenoid bone, ultimately exposing an average of 7.8mm ± 1.643mm of the maxillary artery (Table 1). The IMAX was consistently found running just anterior and parallel to a line between the foramen rotundum and the foramen ovale. Clinical Presentation and Technique
A 55-year-old female originally presented with new-onset visual blurring in her right-eye, and a work-up revealed bilateral transitional (cavernous and clinoidal) internal carotid artery (ICA) aneurysms larger on the right side (Figure 3A-3B). She underwent a formal balloon test occlusion with associated SPECT analysis showing significant asymmetry. She was felt to be a good candidate for EC-IC bypass with trapping of the aneurismal segment.
The patient was taken to the operating room and underwent an extradural middle fossa approach. The anterolateral triangle between V2 and V3 was identified. Using the above-mentioned measurements taken in the laboratory, the anterior loop of the IMAX was found, just anterior and parallel to a line running between the foramens rotundum and ovale. The greater wing of the sphenoid bone was drilled at this location and the anterior loop of the internal maxillary artery was identified.
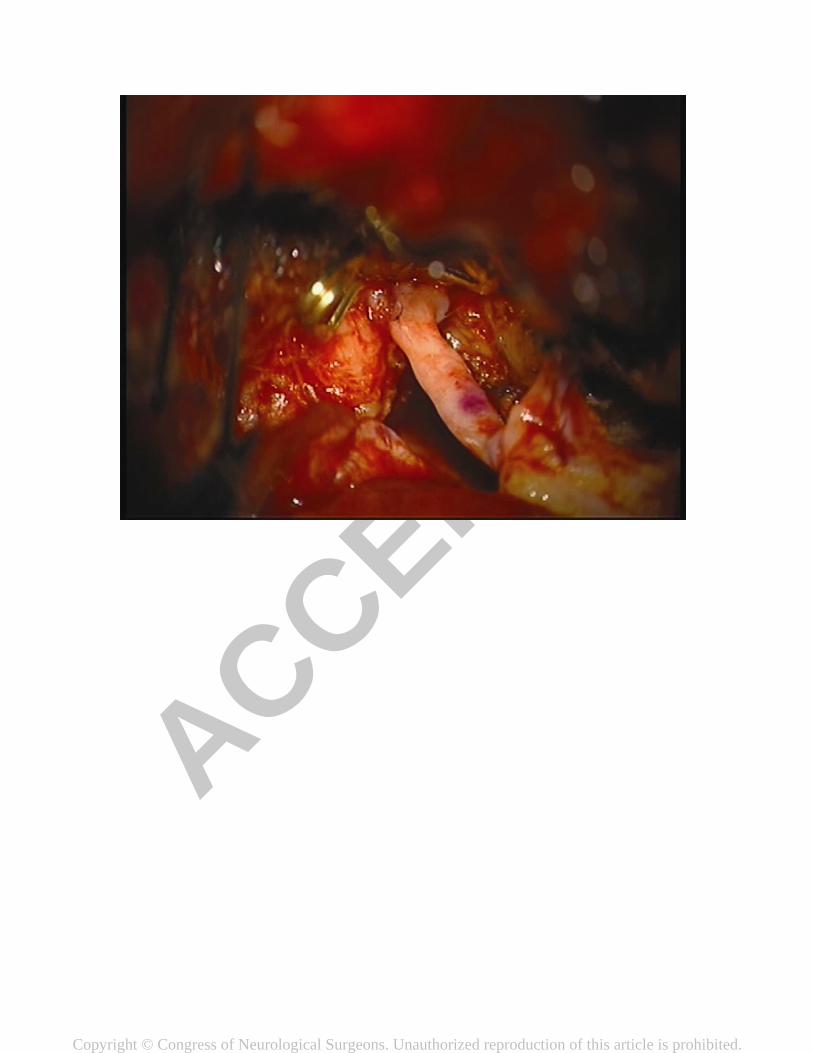
Simultaneous radial artery harvest was undertaken. An end-to-side anastomosis of the radial artery graft to the IMAX was performed, followed by an end-to-side anastomosis to the recipient M3 branch within the Sylvian fissure (Figures 4 and 5). Intraoperative ICG angiography showed graft patency (Figure 6). The ICA was occluded proximally (due to presence of an infundibulum in the supraclinoidal protion of the ICA just distal to the giant aneurysm, we decided not to occlude the ICA distally). The proximal clipping of the ICA, in this specific case, required a very small high cervical incision (2cm) to avoid clipping the ICA within the cavernous segment. Postoperatively, the patient did well, without any new neurological deficits, and underwent formal angiography showing a patent graft (Figures 7A-7B). The patient was discharged home on post-operative day 5, at the 3-week follow-up visit she had resumed normal activity without any restrictions. Discussion
Giant aneurysms represent 3-5% of all intracranial aneurysms and typically present with mass effect, cranial nerve palsies, seizures, hemiparesis, visual deficits, or subarachnoid hemorrhage, secondary to rupture, in up to 35% of patients. Giant aneurysms managed conservatively have 68% and 80% mortality at 2 and 5 years, respectively.14 Current practices

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.
Page 4
for high flow EC-IC bypass involve harvesting a long segment of the radial artery or saphenous vein to perform a bypass from the ECA, involving a lengthy cervical incision, to the MCA.
Radial artery and Saphenous vein (SVG) grafts have been used to achieve bypasses requiring higher flow rates, 50-150 ml/min and 100-200 ml/min, respectively.14 Radial artery grafts are more difficult to harvest but have decreased size discrepancy at the distal anastomotic site decreasing flow turbulence. SVGs are also subject to arterialization and accelerated atherosclerosis, where radial artery grafts are not associated with these long-term problems, implying greater long-term patency.3,14 Radial artery grafts are, however, associated with vasospasm, which does not occur with SVG grafts. Taking all these factors into account, we, in our practice, chose to harvest the radial artery.
Standard EC-IC bypasses involve anastomosis of the M2 or M3 segment of the MCA with the external carotid artery (ECA) with subsequent occlusion of the ICA or trapping of the aneurysm. The procedure requires a transverse cervical incision with exposure of the common, external, and internal carotid arteries. This increases the operative morbidity of the patient, as well as both operative and recovery time.
We present a novel technique that avoids the need for a long cervical incision, exposure of the ECA, ICA, and CCA, by anastomosing the MCA to the IMAX via an interpositioned radial artery graft. Here the revascularization can be performed using a single craniotomy with a middle fossa, extradural approach as described above. Obstruction of the parent vessel can also be performed through the single cranial incision in cases where the aneurysm is distally located rather than the more proximal variant we encountered with this patient, which required a small high cervical incision for proximal occlusion of the ICA. Alternatively, the proximal ICA occlusion can be performed using endovascular techniques.
In the specific case presented we performed an end-to-side anastomosis to the IMAX; we did not occlude the distal IMAX. It is possible to perform end-to-end anastomosis, with the advantage of providing increased IMAX length. However, we prefer end-to-side anastomoses over end-to-end anastomoses in order to better match the size of donor and recipient vessels.
We believe that it is preferable to ligate the ICA at the level of the bifurcation with the external carotid artery. Leaving a stump of the ICA can propagate thrombus formation and serve as a potential source of emboli. It is also reasonable to consider performing an additional zygomatic osteotomy, which we did not do in this specific case, to increase the space available for performing the proximal anastomosis.
Clearly to us the main potential advantage of this procedure is better long-term patency due to the relatively short length of the graft when compared to the standard high-flow EC-IC bypass, from the cervical carotid artery to the MCA. This will, however, require extended review of this technique compared to the standard technique in order to assess the long-term benefits.
Maxillary artery to middle cerebral artery or supraclinoid internal carotid artery bypass using a radial artery graft has been described in cadaveric dissections.15-21 These procedures described end-to-end proximal anastomosis between the maxillary artery and arterial graft, following transection of the maxillary artery at the infraorbital artery. We avoided IMAX transection by instead performing an arteriotomy and end-to-side anastomosis. Conclusions
To the best of our knowledge, based on a review of current literature, this is the first report of a high flow IMAX-MCA EC-IC bypass applied clinically. We feel that use of a short segment of

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.
Page 5
the radial artery will potentially improve long-term graft patency in addition to postoperative overall morbidity. References 1. Yaşargil MG, Krayenbuhl HA, Jacobson JH, 2nd. Microneurosurgical arterial reconstruction.
Surgery. Jan 1970;67(1):221-233. 2. Lougheed WM, Marshall BM, Hunter M, Michel ER, Sandwith-Smyth H. Common carotid
to intracranial internal carotid bypass venous graft. Technical note. J Neurosurg. Jan 1971;34(1):114-118.
3. Sekhar LN, Duff JM, Kalavakonda C, Olding M. Cerebral revascularization using radial artery grafts for the treatment of complex intracranial aneurysms: techniques and outcomes for 17 patients. Neurosurgery. Sep 2001;49(3):646-658; discussion 658-649.
4. Lawton MT, Hamilton MG, Morcos JJ, Spetzler RF. Revascularization and aneurysm surgery: current techniques, indications, and outcome. Neurosurgery. Jan 1996;38(1):83-92; discussion 92-84.
5. O'Shaughnessy BA, Salehi SA, Mindea SA, Batjer HH. Selective cerebral revascularization as an adjunct in the treatment of giant anterior circulation aneurysms. Neurosurg Focus. Mar 15 2003;14(3):e4.
6. Sundt TM, Jr., Piepgras DG, Marsh WR, Fode NC. Saphenous vein bypass grafts for giant aneurysms and intracranial occlusive disease. J Neurosurg. Oct 1986;65(4):439-450.
7. Tulleken CA, Verdaasdonk RM, Berendsen W, Mali WP. Use of the excimer laser in high-flow bypass surgery of the brain. J Neurosurg. Mar 1993;78(3):477-480.
8. Abdulrauf SI. Extracranial-to-intracranial bypass using radial artery grafting for complex skull base tumors: technical note. Skull Base. Aug 2005;15(3):207-213.
9. Amin-Hanjani S, Butler WE, Ogilvy CS, Carter BS, Barker FG, 2nd. Extracranial-intracranial bypass in the treatment of occlusive cerebrovascular disease and intracranial aneurysms in the United States between 1992 and 2001: a population-based study. J Neurosurg. Nov 2005;103(5):794-804.
10. Hauck EF, Samson D. A1-A2 interposition grafting for surgical treatment of a giant "unclippable" A1 segment aneurysm. Surg Neurol. May 2009;71(5):600-603.
11. Haque R, Kellner C, Solomon RA. Spontaneous thrombosis of a giant fusiform aneurysm following extracranial-intracranial bypass surgery. J Neurosurg. Mar 2009;110(3):469-474.
12. Zhang YJ, Barrow DL, Cawley CM, Dion JE. Neurosurgical management of intracranial aneurysms previously treated with endovascular therapy. Neurosurgery. Feb 2003;52(2):283-293; discussion 293-285.
13. Coppens JR, Cantando JD, Abdulrauf SI. Minimally invasive superficial temporal artery to middle cerebral artery bypass through an enlarged bur hole: the use of computed tomography angiography neuronavigation in surgical planning. J Neurosurg. Sep 2008;109(3):553-558.
14. Drake CG. Giant intracranial aneurysms: experience with surgical treatment in 174 patients. Clin Neurosurg. 1979;26:12-95.
15. Ustun ME, Buyukmumcu M, Ulku CH, Cicekcibasi AE, Arbag H. Radial artery graft for bypass of the maxillary to proximal middle cerebral artery: an anatomic and technical study. Neurosurgery. Mar 2004;54(3):667-670; discussion 670-661.
16. Arbag H, Ustun ME, Buyukmumcu M, Cicekcibasi AE, Ulku CH. A modified technique to bypass the maxillary artery to supraclinoid internal carotid artery by using radial artery graft: an anatomical study. J Laryngol Otol. Jul 2005;119(7):519-523.

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.
Page 6
17. Buyukmumcu M, Ustun ME, Seker M, Karabulut AK, Uysal YY. Maxillary-to-petrous internal carotid artery bypass: an anatomical feasibility study. Surg Radiol Anat. Nov-Dec 2003;25(5-6):368-371.
18. Arbag H, Cicekcibasi AE, Uysal, II, Ustun ME, Buyukmumcu M. Superficial temporal artery graft for bypass of the maxillary to proximal middle cerebral artery using a transantral approach: an anatomical and technical study. Acta Otolaryngol. Sep 2005;125(9):999-1003.
19. Ulku CH, Ustun ME, Buyukmumcu M, Cicekcibasi AE, Ziylan T. Radial artery graft for bypass of the maxillary to proximal posterior cerebral artery: an anatomical and technical study. Acta Otolaryngol. Sep 2004;124(7):858-862.
20. Vrionis FD, Cano WG, Heilman CB. Microsurgical anatomy of the infratemporal fossa as viewed laterally and superiorly. Neurosurgery. Oct 1996;39(4):777-785; discussion 785-776.
21. Karabulut AK, Ustun ME, Uysal, II, Salbacak A. Saphenous vein graft for bypass of the maxillary to supraclinoid internal carotid artery: an anatomical short study. Ann Vasc Surg. Sep 2001;15(5):548-552.
Figures Figure 1: Cadaveric dissection showing the relationship between IMAX and V2 Figure 2: Cadaveric IMAX dissection from an extradural middle fossa approach Figure 3A: Pre-operative lateral right internal carotid artery DSA showing a fusiform aneurysm Figure 3B: Pre-operative AP 3-dimensional reconstruction of the right ICA DSA showing a
fusiform aneurysm Figure 4: Proximal radial artery graft to internal maxillary artery anastomosis Figure 5: Radial artery graft connecting the IMAX (top) to the M3 segment of the MCA (bottom) Figure 6: Intraoperative ICG angiogram showing patency of the radial artery graft Figure 7A: Post-operative AP right CCA DSA showing the radial artery graft extending from the
IMAX to the MCA Figure 7B: Post-operative 3-dimensional CTA showing the radial artery graft projecting through
the middle fossa floor

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.
Table 1: Cadaveric Dissection Measurements
Cadaver V2/V3 Apex to
Lateral Rotundum (mm)
Lateral Rotundum to Localization
Point (mm)
Depth to Drill (mm)
Length of IMAX Exposed (mm)
1 - - 4 10 2 10 10 - - 3 5 6 3 9 4 4 7 6 6 5 10 9 5 7 6 10 11 3 7
Mean 7.8 8.6 4.2 7.8 Standard deviation
3.033 2.074 1.304 1.643

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.
ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

ACCEPTED
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.