Embed Size (px)
Citation preview

Br Heart J 1991;65:41-5
Interatrial shunt flow profiles in newborn infants:
a colour flow and pulsed Dopplerechocardiographic study
Satoshi Hiraishi, Youtaro Agata, Koichi Saito, Kohki Oguchi, Hitoshi Misawa,Nobuyuki Fujino, Yasunori Horiguchi, Kimio Yashiro
Department ofPaediatrics, KitasatoUniversity School ofMedicine,Sagamihara,Kanagawa, JapanS HiraishiY AgataK SaitoK OguchiH MisawaN FujinoY HoriguchiK YashiroCorrespondence toDr Satoshi Hiraishi,Department of Paediatrics,Kitasato University Schoolof Medicine, 1-15-1Kitasato, Sagamihara,Kanagawa 228, Japan.Accepted for publication10 July 1990
AbstractInteratrial shunt flow profiles in 36 nor-mal term infants were examined seriallyby colour flow and pulsed Dopplerechocardiographic techniques fromwithin an hour of birth to four or fivedays after birth. Shunt flow across theforamen ovale was detected in 33 normalinfants (92%) within an hour of birth(mean 40 minutes). The occurrence ofinteratrial shunting decreased with age,but a shunt signal was still detected in 17infants (47%) on the fourth or fifth dayof life, by then the ductus arteriosus hadalready closed in all the normal infants.The direction of interatrial shunt flowwas predominantly left-to-right, but in64% there was a coexistent small right-to-left shunt in diastole within an hour ofbirth; by four to five days it was found in19%. In the six patients with persistentfetal circulation the direction of theinteratrial shunt flow was predomin-antly right-to-left with biphasic peaks indiastole and systole at the early stage ofthe disease, and the period of right-to-left shunt flow during each cardiac cyclewas significantly longer than that in nor-mal infants examined within 1 hour ofbirth. In all patients the ductus closedbefore the foramen ovale. At the time ofductal closure in all patients with persis-tent fetal circulation right-to-left shuntflow was seen during diastole and itsperiod was still prolonged.These findings suggest that interatrial
shunting, predominantly left-to-right, iscommon in normal newborn infants.Evaluation of the characteristics of theinteratrial shunt by Doppler echo-cardiography may be useful for predict-ing the progress of or improvement inneonates with persistent fetal circula-tion.
Dramatic changes occur in the circulation ofthe newborn infant. In most normal newborninfants the foramen ovale functionally closeswithin an hour of birth as a result of theincrease in pulmonary venous return, decreasein blood flow in the inferior vena cava, andincrease in systemic arterial resistance afterdelivery.'2 However, a recent Doppler echo-cardiographic study suggested that in normalneonates, right-to-left shunting occurred dur-ing most of diastole, with coexistent left-to-right shunting for some time.3 In addition,
little is known about the prevalence and serialchanges in interatrial shunt flow in normalinfants because previous studies did notdirectly analyse interatrial blood flow."' Alsointeratrial haemodynamic function in patientswith persistent fetal circulation syndrome ispoorly understood.
Therefore, we analysed interatrial shuntflow profiles using colour flow and pulsedDoppler echocardiography to establish (a) thefrequency of a patent foramen ovale duringnormal postnatal life, (b) flow dynamics acrossthe foramen ovale in normal infants and inpatients with persistent fetal circulation, and(c) the relation between ductal shunting orclosure and interatrial shunt flow profiles.
Subjects and methodsSUBJECTSWe studied 36 term infants with a gestationalage of > 38 weeks. Each was the product of anormal pregnancy, labour, and delivery.Infants were of average size for gestationalage, and birth weight ranged from 2600 to3700 g (mean 3100 g). None had received anymedication or supplementary oxygen beforethe study. All infants had normal findings onphysical examination and echocardiographicexamination showed that they were free ofcardiovascular disease. The initial study wasperformed within an hour of birth (mean 40minutes) in all infants and serial studies wereperformed during the first five days after birthat 3 (0 5) (mean (SD)), 24 (1), and 109 (8)hours (4 to 5 days). These examinations wereundertaken when the infants were in a quietstate.We also studied six term infants with
typical persistent fetal circulation and whopresented with early cyanosis within 12 hoursof birth, with low arterial oxygen tension(under 45 mm Hg when inhaling kQ0%oxygen) after structural heart disease had beenexcluded by cross sectional and Dopplerechocardiography.6 Birth weights ranged from2400 to 3400 g (mean 2900 g). There was norecognisable pulmonary, haematological, orcentral nervous system disease in five patientsbut one had mild pulmonary parenchymaldisease caused by meconium aspiration.Initial examinations were performed within24 hours of birth in all patients and serialstudies were performed one or two times a dayuntil all clinical findings disappeared.
COLOUR FLOW AND DOPPLERECHOCARDIOGRAPHIC EXAMINATIONSAll infants were studied with a commercially
41
on June 14, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.65.1.41 on 1 January 1991. D
ownloaded from

Hiraishi, Agata, Saito, Oguchi, Misawa, Fujino, Horiguchi, Yashiro
available system (Hewlett-Packard, Model77020 AC) with a 5 MHz shallow focus or 3 5MHz transducer. For analysis we used theimage that best demonstrated the colour flowimaging of transatrial flow. This was mostoften obtained from the subxiphoid approachas described previously.4 The lower para-sternal approach was also attempted in someinfants. In addition, the entire length of theductus arteriosus was visualised from the highparasternal approach.7 For Doppler colourflow imaging, flow directed toward the trans-ducer was conventionally coded as redwhereas flow directed away from the trans-ducer was blue. Variations in velocity wererepresented by the brightness and intensity ofthe colour. For colour flow imaging the gainwas initially reduced and then progressivelyincreased until an acceptable colour image wasobtained. Interatrial left-to-right shuntingwas judged to be present when red, yellow, ormosaic signals crossed the atrial septum andextended into the right atrium. Right-to-leftshunting was considered to be present if blueor mosaic signals crossed the atrial septumand extended into the left atrium. Ductal left-to-right shunting was considered to be presentif red, yellow, or mosaic signals were seenacross the ductus from the descending aorta tothe main pulmonary artery. Right-to-left duc-tal shunting was judged to be present if blueor mosaic signals crossed the ductus from themain pulmonary artery to the descendingaorta.When colour mapping showed interatrial or
ductal shunting the findings were confirmed bypulsed Doppler analysis, which indicated thedirection of the flow across these orifices. Thesample volume was placed on the colourDoppler echocardiographic shunt flow signal.Doppler profiles and simultaneous electro-cardiograms were recorded at 50-100 mm/sand were stored on video tape for later playbackand analysis in stop frame mode. When therewas a bi-directional pattern at the site of theinteratrial communication the time intervalswere measured as described elsewhere.8 In
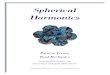
brief, the turning point from the right-to-left tothe left-to-right shunt was designated as T, andthe turning point from the left-to-right to theright-to-left shunt as T2 (fig 1). The ratio of theTI-T2 interval to the RR interval of theelectrocardiogram (T - T2/RR) was calculatedand a mean taken from the recordings of 10consecutive beats.
STATISTICAL ANALYSISWe used non-parametric techniques to analyseserial changes in the frequency of interatrialshunting and Student's t test for differences inmean values between the two groups. Aprobability value of <0 05 was regarded assignificant.
ResultsNORMAL NEWBORN INFANTSWithin an hour of birth left-to-right shunt flowwas detected in 10 infants (28%) and bi-direc-tional shunt flow in 23 (64%) (table, fig 2). Theproportion in whom the foramen ovale wasfunctionally closed did not change within threehours of birth but increased significantly fromthree to 24 hours (p < 0 01). There had been afurther increase in the functional closure by thefourth and fifth days of life, but 10 (28%)infants still had a left-to-right shunt signal andseven (19%) a bi-directional one. The ductusarteriosus was patent three hours after birth inall infants and it closed functionally in 52% at24 hours of life. By the fourth to the fifth day oflife, there had been spontaneous functionalclosure of the ductus in all infants.
ANALYSIS OF INTERATRIAL SHUNT FLOWDYNAMICS IN HEALTHY NEWBORN INFANTSA left-to-right shunt signal was recorded insystole and early diastole (fig 2). A slight right-to-left shunt signal was noted in diastole,mostly in atrial systole; during three examina-tions in two infants a right-to-left shunt signalwas noted in both diastole and systole. In 23infants with a bi-directional shunt flow withinan hour of birth the mean TI - T2/RR ratioranged from 0 68 to 0 95 (mean 0 85) (fig 3).
+88.1
ECG
CM
EC
-67.3
Figure 1 Interatrial shunt flow profile determined by Doppler echocardiography. The sample volume was placed at the site of theforamen ovale. Doppler spectral display above the zero line represents left-to-rightflow and that below the zero line right-to-left. Theduration of left-to-right interatrialflow (T, - T2) was measured and expressed as the ratio to the RR interval of the electrocardiogram(T, - T2/RR). ECG, electrocardiogram; LA, left atrium; RA, right atrium.
42 on June 14, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.65.1.41 on 1 January 1991. Dow
nloaded from

Interatrial shunting in the newborn infant
Figure 2 Colourflow andpulsed Doppler echocardiogramsfrom a normal infant 30 minutes after delivery. (A) Subxiphoid view showingtransatrial red signal (arrow) during systole, which is indicative of left-to-right shuntflow. (B) Note the blue signal (arrow) crossingfrom rightatrium to left atrium in diastole. (C) Doppler signal showing that the direction of shuntflow is predominantly left-to-right (L-R), which isrepresented as Doppler signal toward the transducer. There was a small amount of right-to-left (R-L) shunt flow (Doppler signal awayfromtransducer) of short duration in atrial systole. RA, right atrium; LA, left atrium; ant-inf, anterior-inferior; post-sup, posterior-superior; rt, right;It, left.
Occurrence and direction of interatrial shuntflow
Age after birth
Direction of shuntflow 20-60 (min) (n(%)) 2-4 (h) (n(%)) 23-26 (h) (n(%)) 4-5 (days) (n(%))
No shunt 3 (8) 4 (11) 13 (36) 19 (53)Left-to-right shunt 10 (28) 13 (36) 12 (33) 10 (28)Bi-directional shunt 23 (64) 19 (53) 11 (31) 7 (19)
PATIENTS WITH PERSISTENT FETAL CIRCULATION
At the initial examination the direction ofinteratrial shunt flow was predominantly right-to-left. The right-to-left shunt signal was
1@0-
i -
|0.51
CD
0
Normal 1 2
neonates Persistent fetalcirculation
Figure 3 T, - T2/RR ratio in 23 normal infants with abi-directional shuntflow and six patients with persistentfetal circulation (PFC) associated with considerablehypoxaemia (PFC-1) and ductdl closure (PFC-2). Theratio of T, - T2/RR was smaller in PFC-1 than innormal infants (p < 0 01) and the value in the PFC-2lay between values in the other two groups. The bars showmean (ISD).
recorded in both diastole and systole (fig 4). Intwo patients, small left-to-right shunt flow wasdetected in late systole. During the sameperiod, the direction of the shunt flow withinthe ductus was predominantly right-to-leftduring systole and a small left-to-right shuntflow was detected during diastole in fivepatients. In all infants the ductus closed spon-taneously between 24 hours and 120 hours afterbirth. At the time of ductal closure, interatrialshunt flow pattern was bi-directional and right-to-left shunt flow was detected in diastole in allsix patients. Inspired oxygen was needed tomaintain arterial oxygen tension between 50and 60 mm Hg and the fraction of inspiredoxygen ranged from 0 4 to 0-8 in each patient.Figure 3 shows that the T1 - T2/RR ratio wassignificantly lower in the early phase of persis-tent fetal circulation than at the time of theductal closure (p < 0.01) and both values werealso significantly lower than those seen withinan hour of birth in normal infants (p < 0-01).These bi-directional shunt patterns changed toleft-to-right flow between the sixth and 20thday of life, and functional closure of theforamen ovale was noted in four patients by onemonth.
DiscussionThe data presented in this study showed that aninteratrial shunt, predominantly left-to-right,was common in normal newborn infants.Colour flow mapping clearly distinguished be-tween interatrial left-to-right shunting andflow in the superior vena cava. The results ofcolour flow mapping were confirmed by pulsedDoppler spectral analysis. The frequency ofinteratrial shunting did not change within thefirst three hours of birth, but it was significantlydecreased from three to 24 hours after birth.
43 on June 14, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.65.1.41 on 1 January 1991. Dow
nloaded from

Hiraishi, Agata, Saito, Oguchi, Misawa, Fujino, Horiguchi, Yashiro
Figure 4 Colour Dopplerechocardiogramsfrom apatient with persistentfetal circulation. Thetransatrial blue signal,which is indicative ofright-to-left shuntflow,was recorded in diastole.Note the mosaic signal(arrow) crossing to theforamen ovale in systole,indicating aliaising.Combined pulsed Dopplerflow mapping andcontinuous Dopplertechnique showed that theblue signal originatedfrom'tricuspid regurgitantjetwith high velocity of 3-5 i-m/s. TV, tricuspid valve;MV, mitral valve; RA,right atrium; LA, leftatrium.
Drayton and Skidmore reported that ductalleft-to-right shunt flow of 62 ml/kg/minute interm infants (95% confidence interval 43 to 82)shortly after birth decreased rapidly over thefirst 12 hours.9 This result was consistent withthe time course of changes in the morphologyand flow patterns in the ductus arteriosus.'`I'From these observations, it seems that theductal left-to-right shunting in early postnatallife increases the frequency and magnitude ofthe left-to-right shunting through the foramenovale. However, this mechanism does notexplain the finding that interatrial shunt flowwas detected in 47% of our subjects in thefourth to fifth day of life when the ductus hadalready closed in all infants. An earlier study4and our study found that the patent foramenovale was either a redundant flap valve of theseptum primum or a septal drop out at thesuperior rim of the septum primum. Othersalso found that patent foramina ovale were ofnormal size with unduly short or lax valves orwere oversized with a normal sized valve.'2Incompetence ofthe foramen ovale could occurif the development of various portions of theatrial septum was unbalanced, even in theabsence of left atrial enlargement,"3 left sidedlesions, and left ventricular failure.'4We assessed the phase and the duration of
interatrial left-to-right or right-to-left shunt-ing during each cardiac cycle from simul-taneous recordings of the Doppler determinedflow velocity pattern and the electrocardio-gram. In most normal infants left-to-rightshunting was dominant and slight right-to-leftshunt flow was frequently noted in diastole;however, right-to-left shunt was seen in bothdiastole and systole in two infants with moder-ate tricuspid regurgitation. On the other hand,in all six patients with persistent fetal circula-tion, right-to-left shunting was dominant withbiphasic peaks in diastole and in systole; but intwo infants there was a small left-to-right shuntflow in later systole. We did not monitorrespiration, and respiration especially mechan-ical ventilation, might have an effect on theinteratrial shunt flow pattern. All six infantswith persistent fetal circulation, however,
showed conversion from dominant right-to-left shunting to bi-directional shunting duringintubation and ventilation, and two had pureleft-to-right shunting immediately before theextubation. These manoeuvres seemed to havelittle effect upon changes in the flow patterns inour patients.The interatrial pressure gradient, which can
determine the direction and the phase of shuntflow5'5 may be affected by (a) the difference indistensibility of the right and left ventricles,(b) the capacitance ofthe systemic and pulmon-ary venous systems, (c) tricuspid regurgitation,and/or (d) persistence of a right-to-left or left-to-right shunt at the level of the ductus arter-iosus. Analysis of the filling patterns of theright and left ventricles in normal neonates316suggested that the right ventricle becomes lessdistensible in the neonatal period and that thismay cause diastolic interatrial shunting. If thisig an effect of raised pulmonary resistance, thenthe pulmonary artery hypertension associated'with persistent fetal circulation should predis-pose to an increase in diastolic right-to-leftinteratrial shunt flow as seen in our study. Onthe other hand, in an earlier cineangiographicstudy of ventricular volume in 10 patients withpersistent fetal circulation we found that adecrease in pulmonary blood flow reduced thepreload of the left ventricle.'7 We also foundthat a regurgitant tricuspid jet crossed theforamen ovale and entered the left atrium intwo normal infants and four with persistentfetal circulation. These observations raise thepossibility that systolic right-to-left shuntingresults from a smaller capacity of the pulmon-ary venous system than that of systemic venoussystem, from tricuspid regurgitation, or fromboth.
All six patients with persistent fetal circula-tion responded to conventional treatmentssuch as infusion of tolazoline hydrochlorideand hyperventilation. The ductus arteriosusclosed before the foramen ovale in all sixpatients. At the time of the ductal closure theinteratrial shunt flow pattern was bi-directionaland the duration of diastolic right-to-left shuntflow was still longer than in normal infants. At
44
on June 14, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.65.1.41 on 1 January 1991. D
ownloaded from

Interatrial shunting in the newborn infant
this stage these patients had mild to moderatehypoxaemia. Our data indicate that relativelyreduced distensibility ofthe right ventricle maypersist after ductal closure, resulting in inter-atrial right-to-left shunting in diastole. Thereduced distensibility ofthe right ventricle maybe related to the persistence of relatively highpulmonary arterial pressure seen even afterductal closure in infants with persistant fetalcirculation."'
Evaluation of interatrial shunting byDoppler echocardiography depends on thisknowledge of the characteristics of interatrialshunting in normal newborn infants. TheDoppler technique can be useful in assessingthe severity and course of persistent fetalcirculation.
This work was supported by a grant from the KitasatoUniversity Foundation and a Grant-in-Aid for GeneralScientific Research from the Ministry ofEducation, Science andCulture in Japan.We thank all members ofthe neonatal intensive care unit, Miss
Harumi Kawai, and Mr Masahiro Ohe.
1 Gessner I, Krovetz LJ, Benson RW, Prystowsky H, StengerV, Eitzman DV. Hemodynamic adaptations in the new-born infant. Pediatrics 1965;36:752-62.
2 Arcilla RA, Oh W, Wallgren G, Hanson JS, Gessner IH,Lind J. Quantitative studies of the human neonatalcirculation II. Hemodynamic findings in early and laterclamping of the umbilical cord. Acta Paediatr Scandi'Suppl! 1967;179:23-42.
3 Steinfeld L, Almeida OD, Rothfeld EL. Asynchronousatrioventricular valve opening as it relates to right to leftinteratrial shunting in the normal newborn. J Am CollCardiol 1988;12:712-8.
4 Bierman FZ, Williams RG. Subxiphoid two-dimensionalimaging of the interatrial septum in infants and neonateswith congenital heart disease. Circulation 1979;60:80-90.
5 Kupferschmid C, Lang D. The valve of the foramen ovale ininteratrial right-to-left shunt: echocardiographic cine-
angiocardiographic and hemodynamic observations. AmJ Cardiol 1983;51:1489-94.
6 Gersony WM. Neonatal pulmonary hypertension: clinicalreview. In: Doyle EF, Engle MA, Gersony WM,Rashkind WJ, Talner NS, eds. Pediatric cardiology. NewYork, Berlin, Heidelberg, Tokyo: Springer-Verlag, 1986:876-9.
7 Hiraishi S, Horiguchi Y, Misawa H, et al. NoninvasiveDoppler echocardiographic evaluation of shunt flowdynamics of the ductus arteriosus. Circulation 1987;75:1146-53.
8 Satomi G, Nakazawa M, Takao A, et al. Blood flow patternof the intraatrial communication in patients with completetransposition of the great arteries: a pulsed Dopplerechocardiographic study. Circulation 1986;73:95-9.
9 Drayton MR, Skidmore R. Ductus arteriosus blood flowduring first 48 hours of life. Arch Dis Child 1987;62:1030-4.
10 Hiraishi S, Misawa H, Oguchi K, et al. Two-dimensionalDoppler echocardiographic assessment of closure of theductus arteriosus in normal newbom infants. J Pediatr1987;111:755-60.
11 Hiraishi S, Misawa H, Saito K, et al. The relationshipbetween the morphology and flow patterns in the ductusarteriosus of newborn infants under physiologic condi-tions and with increased oxygen inspiration. J Jpn PediatrSoc 1988;92:1259-63 [in Japanese].
12 Edwards JE. Malformations of the atrial septal complex. In:Gould SE, ed. Pathology of the heart and blood vessels, 3rded. Springfield Illinois: Charles C Thomas, 1968:262-79.
13 Rudolph AM, Mayer FE, Nadas AS, Grosse RE. Patentductus arteriosus: a clinical and hemodynamic study of23 patients in the first year of life. Pediatrics 1958;22:892-904.
14 Pagtakhan RD, Hartmann AF Jr, Goldring D, Kissane J.The valve-incompetent foramen ovale: a report on seveninfants with left-to-right atrial shunt. J Pediatr 1967;71:848-54.
15 Minagoe S, Tei C, Kisanuki A, et al. Noninvasive pulsedDoppler echocardiographic detection of the direction ofshunt flow in patients with atrial septal defect: usefulnessof the right parasternal approach. Circulation 1985;71:745-53.
16 Riggs TW, Rodriguez R, Snider R, et al. Doppler echo-cardiographic evaluation of right and left ventriculardiastolic function in normal neonates. J Am Coll Cardiol1989;13:700-5.
17 Hiraishi S. Ventricular volume variables in patients withpersistent fetal circulation syndrome. In: Doyle EF, EngleMA, Gersony WM, Rashkind WJ, Talner NS, eds.Pediatric cardiology. New York, Berlin, Heidelberg,Tokyo: Springer-Verlag, 1986:885-8.
18 Musewe NN, Poppe D, Smallhorn JF, et al. Dopplerechocardiographic measurement of pulmonary arterypressure from ductal Doppler velocities in the newborn.J Am Coll Cardiol 1990;15:446-56.
45
on June 14, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.65.1.41 on 1 January 1991. D
ownloaded from