Embed Size (px)
Citation preview

INTEGRATED CASE BASED DISCUSSION
Chairperson : Dr.P.Ramalingam, Professor of General Surgery
Panel Members : Dr.U.L Lakshmi Narasamma, Professor of General Surgery.
Dr.V.Vijaya Sree, Associate Professor of Pathology.
Dr.Ashish U Kamdi, Assistant Professor of Anatomy.
1/19/2016

CASE DETAILS
1/19/2016

A 40 year old obese female Presented with pain abdomen radiating to right
shoulder & back with fever & chills since 2 days. Yellowish discoloration of eyes since 2 days. Past h/o recurrent colicky abdominal pain in last 6
months. O/E Temp.38 degrees, Icterus +. P/A Right upper quadrant tenderness +. Murphy’s sign positive.
CASE DETAILS

What is the Clinical Diagnosis ?
1/19/2016

What are the possible Differential Diagnosis ?
1/19/2016

What is the anatomical basis for Murphy’s sign ?

Fundus of gall bladder lies deep to the tip of ninth costal cartilage.
Hence , when patient takes a breath , the inflamed gall bladder descends, comes out of the thoracic cage & strikes the finger,leading to the sudden severe pain, which makes the patient wince.

Why there is referred pain felt at right shoulder tip in acute cholecystitis ?

Irritation of parietal diaphragmatic peritoneum supplied by right phrenic nerve is responsible for this pain.
Phrenic nerve ( C3,C4,C5 ) & supraclavicular nerve ( C3,C4 ) .

WHAT ARE THE SIGNS OF BILIARY OBSTRUCTION ?
1/19/2016

Answer
Jaundice Dark orange, foamy urine Steatorrhea Clay-coloured stools pruritis

Who is at risk?

High fat diet Obesity Genetic predisposition > 60years Type I DM( high triglycerides) Low calorie, liquid protein diet Rapid wt.loss ( increased cholesterol)

WHAT ARE THE INVESTIGATIONS YOU WILL DO ?
1/19/2016

Complete Blood PictureHb : 10 g/dl ( 13 – 17 g/dl )WBC : 11300/ cumm ( 4000 – 10000/cumm)Neutrophils : 70 % ( 40-80 % )Lymphocytes :25 % ( 20-40 %)Eosinophils : 03% ( 1-6 %)Monocytes : 02% (2-10%)Basophils :0% (0-2 %)Platelet count : 2.74 lakhs/cu mm (1.4 – 4 L/cumm)Peripheral Smear : Normocytic Normochromic
1/19/2016

Bleeding time : 02min 00 seconds (2-7 mins ) Clotting time : 04min 00 seconds (1-9 mins) Blood grouping : “A” Rh positive RBS : 131mg/dl Blood Urea : 15mg/dl (10-50 mg/dl) Serum Creatinine : 0.6 mg/dl (0.5 -1.3 mg/dl) Serum Sodium : 140 mmol/l(135-155 mmol/l) Serum Potassium : 3.9 mmol/l (3.5-5.5 mmol/l) Serum Chloride : 100 mmol/l (98-109 mmol/l)
1/19/2016

LIVER FUNCTION TESTS
• Total Bilirubin : 3.5 mg/dl (0.2 – 1.0 mg/dl )• S. Albumin : 3 g/dl (3.8 -5.4 g/dl )• Prothrombin time : 13.8 seconds. (upto 14 secs.)• Alkaline phosphatase : 340 U/L( upto 280 U/L )• Alanine aminotransferase:240 U/L ( upto 40 U/L)• Gamma glutamyl transferase:381 U/L (upto 40 U/L)
1/19/2016

• POSITIVE FINDINGS
• Increased WBC count
• Increased total bilirubin-direct&indirect (indicates bile duct obstruction)
• Increased amylase & lipase (due to pancreatic involvement)
• Increased AST,LDH,Alk.phosphatase
• Increased sr.cholesterol

RADIOLOGICAL INVESTIGATIONS ?
1/19/2016

X ray erect abdomen showing gall stones in gall bladder.Usually gall stones are radiolucent.( only 15% are radio opaque)
1/19/2016

USG ABDOMEN SHOWING TWO STONES IN GALL BLADDER.95 % Sensitivity & Specificity.
1/19/2016

ERCP
1/19/2016

MRCP
1/19/2016

Why stone formation is common in gall bladder ?

Gall bladder receives bile from liver consisting of cholesterol ,bilirubin , calcium.
Bile is not only stored in gall bladder but also concentrated upto 10 times.
Hence tendency to form stones.

What are components of sphincter of oddi ?


What is the Pathology of Acute Cholecystitis ?
1/19/2016

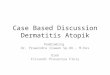
IDENTIFY THESE SLIDES ?
C
A
B
?

1/19/2016
A. Acute cholecystitis superimposed on a chronically inflamed gallbladder. The mucosa has a characteristic "angry,red" color.Note the marked edema of the wall and the serosal hyperemia.
B. Acute cholecystitis showing extensive ulceration, hemorrhage, and edema but only scanty inflammation.
C. Reactive epithelial atypia associated with
acute cholecystitis.This changes should not be over diagnosed as dysplasia or carcinoma in situ.

List out the conditions which are associated with follicular cholecystitis?

Answer
Typhoid fever
Primary sclerosing cholangitis,
Gram negative bacterial infection of bile.

What is Cholesterosis of gallbladder ?

Collections of lipid-filled foamy cells are present in the tips of the villi , in the stroma separating the
glands.

What are the possible causes of Jaundice in this patient?

DEFECTIVE DRAINAGE OF BILEEntry of bile pigments into the circulation through damaged gall bladder mucosa.Choledochal spincter spasm.
OBSTRUCTION TO FLOW OF BILE DUE TO STONE DISEASEConcomitant choledocholithiasis.Compression of CBD due to enlarged Cystic node of lund.

WHAT ARE THE COMPLICATIONS OF ACUTE CHOLECYSTITIS ?
1/19/2016

MUCOCELE OF GALL BLADDER. EMPYEMA OF GALL BLADDER. EMPHYSEMATOUS CHOLECYSTITIS. GANGRENE OF GALL BLADDER. PERFORATION OF GALL BLADDER. PERICHOLECYSTIC ABSCESS. CHOLECYSTO ENTERIC FISTULA. GALL STONE ILEUS.
1/19/2016

What are the Causes of Obstructive Jaundice ( Surgical Jaundice) ?

Biliary Atresia/Stricture. Cancer of Gall bladder or Pancreas. Cholangitis. Cholelithiasis & choledocholithiasis. Congenital Structural Defects. Cysts of the bile duct.(Choledochal cysts) Lymph node enlargement. Pancreatitis. Parasitic infections. Trauma including Surgical Complications.

WHAT IS THE TREATMENT IN THIS CASE ?
1/19/2016

PRE OPERATIVE
GI rest - NBM NG tube if vomiting IV Fluids Analgesics (not morphine) Antibiotics for cholecystitis (against GN & enterococcus) inj. Vit.K (if Prothrombin time is prolonged.)

OPERATIVE TREATMENT
1/19/2016

EMERGENCY CHOLECYSTECTOMY + CBD EXPLORATION. LAPROSCOPIC
OPEN.
1/19/2016

WHAT ARE THE OTHER MODES OF TREATMENT FOR ACUTE CHOLECYSTITIS?
1/19/2016

ACUTE CALCULUS CHOLECYSTITIS?
1/19/2016

ACUTE CALCULUS CHOLECYSTITIS WITH CBD STONE AND JAUNDICE IN A MORIBUND PATIENT
TREATMENT ?
1/19/2016

ACUTE CALCULUS CHOLECYSTITIS WITH GANGRENE OF GALL BLADDER ?
1/19/2016

Indications of Cholecystectomy ?
1/19/2016

1/19/2016
Indications for Cholecystectomy
Urgent[*]
Acute cholecystitis Emphysematous cholecystitis Empyema of the gallbladder Perforation of the gallbladder Previous choledocholithiasis with endoscopic duct clearance
Elective
Biliary dyskinesia Chronic cholecystitis Symptomatic cholelithiasis

DIFFERENT PROCEDURES OF CHOLECYSTECTOMY ?
1/19/2016

1/19/2016

What are the parts of the Extra hepatic biliary apparatus ?

Right and left hepatic ducts The common hepatic duct The gall bladder The cystic duct The bile duct

WHAT IS CALOT’S TRIANGLE ?
1/19/2016


WHAT IS THE LENGTH AND DIAMETER OF COMMON BILE DUCT ?
1/19/2016

LENGTH :6-8 CM
DIAMETER : 6 mm
1/19/2016

What are the conditions which cause gall bladder wall thickening ?
1/19/2016

Answer
A. Acute cholecystitis
B. Polyp
C. GB-malignancy
D. Chronic cholicystitis
E. Adenomyomatosis
F. Emphysematous cholecystitis
G. Gangrenous cholecystitis

What are the indications for CBD exploration after cholecystectomy ?
1/19/2016

INDICATIONS FOR CHOLECYSTOSTOMY ?
1/19/2016

CHOLECYSTOSTOMY
INDICATIONS :
HYDROPIC GALL BLADDER.
PURULENT CHOLECYSTITIS
MORIBUND PATIENT WITH ACUTE CHOLECYSTITIS
GANGRENOUS CHOLECYSTITIS.
DECOMPRESS GALL BLADDER & PROVIDE DRAINAGE.
1/19/2016

Complications of Laparoscopic Cholecystectomy?
1/19/2016

Complications of Lap. Cholecystectomy
Haemorrhage. Bile duct injury. Bile leak. Retained stone. Pancreatitis. Wound Infection Pneumoperitoneum related.
1/19/2016

WHAT ARE THE CAUSES OF POST OPERATIVE BILE LEAK ?
1/19/2016

ACCESSORY HEPATIC DUCTS. DUCT OF LUSHKA . CYSTIC DUCT STUMP LEAK.
1/19/2016

What are the sites of opening of accessory hepatic ducts ?


WHAT IS MEANT BY NASO BILIARY DRAINAGE ?
1/19/2016

NASO BILIARY DRAINAGE
It is a mode of biliary decompression in:
Obstructive jaundice and cholangitis
Malignancy
Bile leak after primary surgery
Urgent drainage in suppurative cholangitis sclerosing cholangitis
Pre operative.1/19/2016

WHAT IS SUMP SYNDROME ?
1/19/2016

1/19/2016
The syndrome occurs when there is malfunction of the sphincter of Oddi and the distal common bile duct acts as a 'sump' or stagnant reservoir for stones and other debris. This can lead to recurrent abdominal pain, cholangitis, pancreatitis or biliary obstruction.

1/19/2016
THANK YOU