Embed Size (px)
Citation preview

Inpatient Management of Diabetic Foot Complications
Eric Lew, DPM, FACFASDiplomate, ABFAS and ABPMUniversity of New MexicoCenter for Healing in the Lower Extremity (CHILE)

Introduction and Objectives
Discuss the epidemiology of diabetic foot ulcers in New Mexico and its impact on patients
Explain why functional limb salvage and wound care is important for these patients
Understand a practical and basic method of inpatient management of diabetic foot disorders
Recognize 3 main factors that threaten a limb for amputation and which entity takes priority in initial management
Review admission criteria and diagnostic modalities

Diabetes is a problem in New Mexico
• Approximately 184,000 New Mexicans (11.6% percent) have diabetes Additional 53,000 are undiagnosed
Estimated 587,000 (36.1%) have prediabetes
Hispanic (13%) and Native American(17.7%) populations are at much greater risk
Deadly: one of the 10 leading causes of death in New Mexico
Financial Burden: Estimated $2 billion per yearhttp://main.diabetes.org/dorg/PDFs/Advocacy/burden-of-diabetes/new-mexico.pdfhttp://hsc.unm.edu/about/features/archives/diabetes.shtmlhttp://apma.files.cms-plus.com/FileDownloads/DiabetesbytheNumbers_New%20Mexico.pdf

Complications of diabetes have significant impact on the lower extremity
Neuropathy (loss of protective sensation)
Diabetic Peripheral Angiopathy
Structural Deformities

Diabetic foot ulcers impact patients health
• Meta-analysis: 81,116 patient
• 8 studies
Browning et al. The association of ulceration of the foot with cardiovascular and all-cause mortality in patients with diabetes: a
meta-analysis. Diabetologica (2012)
Linked with higher risk of death, heart attack and stroke:
• 1.89-fold greater risk of death
• 2.22-fold risk of cardiac-related death
• 1.41-fold greater risk of fatal stroke

Patients with ulcerations are at more risk for more devastating complications
Up to 30 percent with peripheral neuropathy
Up to 25 percent will experience an ulcer
Ulcerations Infection Amputation
More than 50 percent of all foot ulcers will become infected requiring hospitalization
20% of infections result in amputation

These are reasons why limb preservation is pursued
• After a major amputation, 30-50% of people will have their other limb amputated within 2 years.- Goldner. Diabetes 1960- Armstrong, et al, J Amer Podiatr Med Assn, 1997
• The relative 5-year mortality rate after diabetic limb amputation is ~50%.
Multiple large-scale studies of patient self-reported quality of life have shown that limb loss has a larger negative impact on quality of life than any other complication of diabetes, including end-stage renal disease or blindness
Clarke P, Gray A, Holman R. Estimating utility values for health states of type 2 diabetic patients using the EQ-5D (UKPDS 62). Med Decis Making 2002; 22: 3409.
Laiteerapong N, Karter AJ, Liu JY, Moffet HH, Sudore R,Schillinger D, et al. Correlates of quality of life in older adults with diabetes: the diabetes & aging study. Diabetes Care 2011;34: 174953.

What do patients with diabetes fear most?
Dane Wukich, MD, Katherine Raspovic DPM, Natalie Suder, MPH. Patients With Diabetic Foot Disease Fear Major Lower-Extremity Amputation More Than Death, Foot and Ankle Specialist; Feb 1, 2017

Successful limb preservation depends on a multidisciplinary effort
Barches, et al, The system of care for the diabetic foot: objectives, outcomes, and opportunities, 2013
Vascular and Podiatric Surgery

“A team approach to management is optimal in patients with diabetic foot infections to increase the likelihood of limb salvage.”
- Dane Wukich, MD
Georgetown/Medstar Center for Wound Healing Baylor STEP (Save The Extremity Program) USC and University of Arizona SALSA (Southwestern Academic Limb Salvage
Alliance) UT Southwestern Medical Center UCSF Limb Preservation Center Temple Limb Salvage Center University of Michigan Scholl College of Podiatric Medicine’s CLEAR (Center for Lower Extremity
Ambulatory Research) UNM CHILE (Center for Healing in the Lower Extremity)
Wukich, Armstrong, Attinger, Boulton, Frykberg, Lipsky, Pinzur, et al. Inpatient Management of Diabetic Foot Disorders: A Clinical Guide. Diabetes Care 2013

Inpatient Clinical Pathway
Emergency Department
- Initial Assessment- Labs- Imaging- Non-invasive arterial studies- Consult EGS/Ortho- Consult Podiatry and/or Vascular
Admission
- Surgical Planning- Ancillary Studies - Advanced Imaging- Medical /Metabolic
- Hyperglycemia- Renal
- Culture-Directed Antibiotic Therapy?- Avoid Swab - Prefer Deep tissue or Bone
Post Op Care
- Activity (Non-weight bearing)- Consult Infectious Disease
- f/u Culture and Biopsies- Physical Therapy Wound Care- Diabetes Education- Management of Co-Morbidities
Limb Preserving Surgery
Source Control- Incision and Drainage- AmputationVascular Intervention- Endovascular- BypassSecondary Procedures- Debridement, Lavage- Secondary reconstruction
and closure
Discharge Planning
- Case Management- Patient and Family education- Provide Clear Discharge
Instructions
- Follow-up Appointments set up PRIOR to discharge:
- Primary Care- Podiatry- Vascular- ID/OPAT- Wound Care
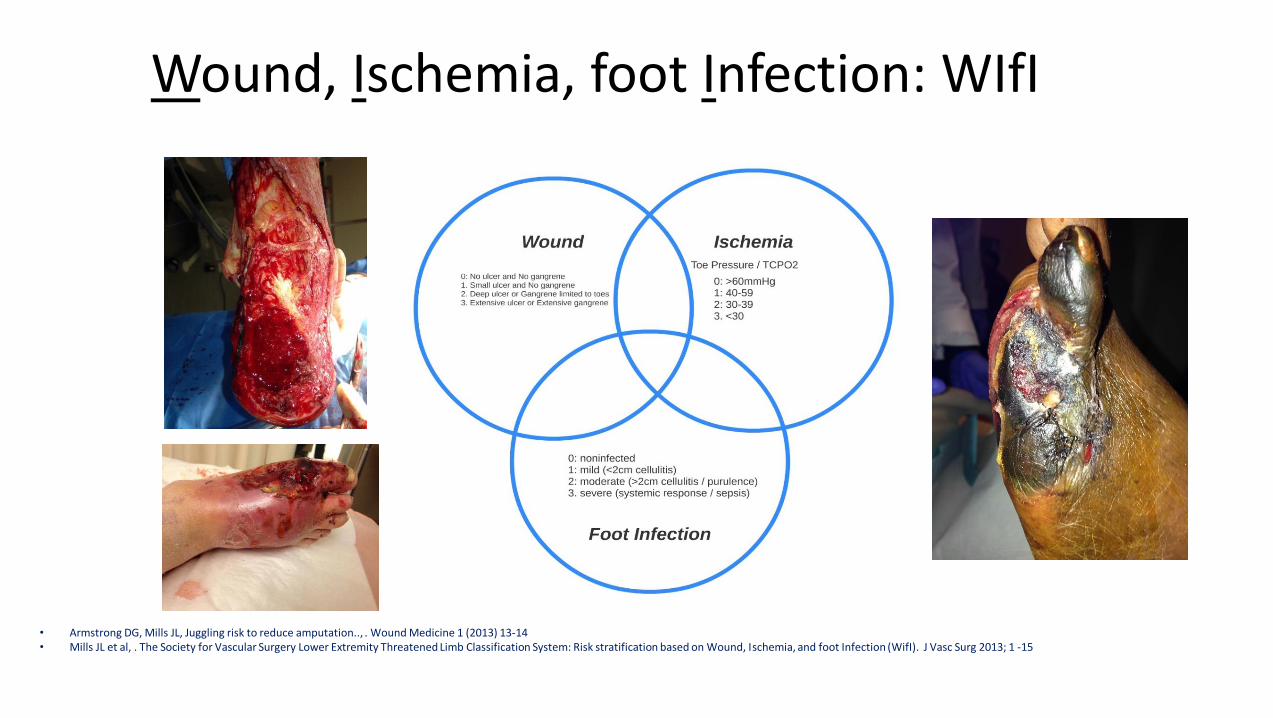
Wound, Ischemia, foot Infection: WIfI
• Armstrong DG, Mills JL, Juggling risk to reduce amputation.., . Wound Medicine 1 (2013) 13-14• Mills JL et al, . The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: Risk stratification based on Wound, Ischemia, and foot Infection (WifI). J Vasc Surg 2013; 1 -15

Case 1
56-year-old female with DM, HTN presents with an infected foot as shown after stubbing her pinky toe 2 weeks ago.

Case 1- Physical Exam
• Vitals: T 37.7, HR 99, R: 18, BP 169/78• General: Alert and oriented x 3 in NAD• Vascular: (+) palpable pulses
– Cap refil < 3 sec
• Neuro: absent protective sensation• MSK: acute edema, and pain to palpation• Derm: wet gangrenous 5th digit with
expanding tissue necrosis, fluctuanceerythema, edema along midfoot and plantar arch (+) purulence, malodor

IDSA Diabetic Foot Infection Classification - 2012
Uninfected: no purulence or signs of infection (erythema, edema, callor, purulence, sometimes pain)
Mild: Infection limited to superficial tissue, < 2 cm of periulcerative signs of infection; no systemic signs
Moderate: Infection involves deeper tissue, localized abscess, gangrene with > 2 cm signs of infection; systemically and metabolically stable
Severe: Foot infection AND systemic toxicity and/or metabolic instability Fever, Chills, Tachycardia, Hypotension, Hyperglycemia and Confusion
Patients with moderate and severe symptoms meet admission criteria

Case 1 – Initial ED work-up and Plan
Pertinent Labs: WBC 19.4, Hg A1c 14.9, Glucose 476, ESR 110, CRP 28.6, BUN 26, Cr 1.35, Lactate 1.3
X-rays: inconclusive for osteomyelitis, soft tissue edema
Non-Invasive Vascular Studies:
– Right ABI 1.13, Right Great toe pressure 63 and TBI 0.44
– Triphasic waveforms: popliteal, PT, DP
WIfI: Wound 2, Ischemia: 0, foot Infection: 3

Deep cultures obtained post debridement and lavage is considered a best practice
Ideally cultures should be obtained prior to starting antibiotics (except for IDSA Severe)
Deep tissue cultures, post debridement and irrigation are better than swab cultures
Use the laceration repair kit with a disposable #15 or #10 blade
Scrub the foot/extremity with betadine or chlorhexidine
Sharp Debridement
Irrigate thoroughly
Obtain tissue from depth of debridement with sterile instrumentation
Send to Microbiology (PowerChart order: CWDANA)

What does Osteomyelitis look like?
Radiographs:
• Osteomyelitis
• Osteitis
• Periostitis
• Osteonecrosis
Multiple Impressions:
Infectious Disease, Radiology, Ortho, Wound Care, Vascular Surgery

Definitive Diagnostic Criteria (>90%)
Bone sample with positive culture AND positive histology
Purulence in bone found in surgery
Pathologic fracturing found in surgery
Intraosseous abscess found on MRI
Ertugrul BM, Lipsky BA, Savk O. Osteomyelitis or Charcot neuro-osteoarthropathy? Differentiating these disorders in diabetic patients with a foot problem. Diabet Foot Ankle. 2013;4:10.3402/dfa.v4i0.21855. Published 2013 Nov 5. doi:10.3402/dfa.v4i0.21855

Probable Diagnostic Criteria (51-90%)
• Visible cancellous bone in an ulcer
• MRI showing bone marrow edema and effacement
• Bone sample with positive culture, but negative histology
• Bone sample with positive histology but negative culture

Possible Diagnostic Criteria (10-50%)
• Plain radiographs reveal cortical erosion
• MRI reveals bone marrow edema and effacement
• Non-healing wound despite adequate offloading and perfusion >6 weeks
• Positive probe to bone (with visible cortical bone)
• Ulcer of > 2 weeks duration with clinical evidence of infection

Unlikely Diagnostic Criteria (<10%)
• No signs or symptoms of inflammation
• Normal radiographic findings
• Normal MRI or Bone Scan
• Superficial ulceration < 2 weeks duration

What does osteomyelitis actually look like?

What does osteomyelitis look like?

Bone Biopsy
Histopathology Microbiology

Is a bone biopsy really the gold standard as a diagnostic test for osteomyelitis?
Statistical Reliability of Bone Biopsy for the Diagnosis of Diabetic Foot Osteomyelitis
• Andrew J. Meyer, et al, JFAS, 2011
• Retrospective analysis of 39 specimens
• 4 pathologists
– Told that it was a specimen of bone taken from a patient with diabetes to evaluate for osteomyelitis

Statistical Reliability of Bone Biopsy for Dx of Diabetic Foot Osteomyelitis
• Arrive at 1 of 3 potential diagnoses:
1. No evidence of osteomyelitis
2. No definitive findings of osteomyelitis, but cannot rule it out, OR
3. Findings consistent with osteomyelitis

Statistical Reliability of Bone Biopsy for Dx of Diabetic Foot Osteomyelitis
• Results:– 33% (13/39):
• Complete agreement between pathologists
– 41% (16/39):• Clinically significant disagreement between pathologists
– Kappa Coefficient of 0.31 (Fair agreement)
• Findings observed more frequently when diagnosis of “findings consistent with osteomyelitis”– Acute Inflammation
• Supports other studies: Lymphocytes, plasma cells, and PMN

Pitfalls of a microbiologic assessment of a bone culture
• Contiguous extension leading to contamination
• Culture swabs misrepresent the number and type of pathogens
• Antibiotics

Percutaneous Bone Biopsy or Obtaining cultures after thorough debridement and lavage are best
practices

Intravenous vs Oral Therapy for Osteomyelitis
• Systemic Review; 1,158 publications:
– No significant differences in outcome
– After excluding those who need urgent surgery for life or limb threatening infections, there is no clear evidence that surgical debridement of infected bone is routinely necessary
– No data to support the superiority of any particular route of delivery
Berendt, A.R., Peters, E.J.G., Bakker, K., Embil, J.M., Eneroth, M., Hinchliffe, R.J., Jeffcoate, W.J., Lipsky, B.A., Senneville, E., Teh, J. and Valk, G.D. (2008), Diabetic foot osteomyelitis: a progress report on diagnosis and a systematic review of treatment. Diabetes Metab. Res. Rev., 24: S145-S161. doi:10.1002/dmrr.836


Is parenteral antibiotic therapy always necessary?
Oral versus Intravenous Antibiotics for Bone and Joint Infection (OVIVA)Study Design: • Multicenter (26 UK Hospitals) • Open-label, randomized, controlled, noninferiority trial • Patients with acute or chronic bone & joint infections
– Randomization within 7 days after surgery (or start of antibiotics if medical management only) to: o 6 weeks IV therapy o 6 weeks PO therapy o Antibiotic agents determined by clinician
• Primary outcome: definite treatment failure within 1 year of randomization Defined by clinical, microbiologic or histologic criterion
HK Li, et al N Engl J Med. 2019;380:425-36

OVIVA Results (Osteomyelitis)
• 1,054 (51%) randomized– Osteomyeltis of the foot (20%)
– PAD (6%)
• Conclusion: Oral therapy was noninferior to intravenous therapy when used for the 1st 6 weeks of treatment in well-selected patients.
• Oral antibiotic therapy was associated with a shorter length of hospital stay and with fewer complications than intravenous therapy.

How long should I give antibiotics?
Site of Infection, by Severity or Extent
Route of Administration Setting Duration of Therapy
Soft Tissue Only
Mild Topical or Oral Outpatient 1-2 wk; may extend up to 4 wek, if slow to resolve
Moderate Oral (or initial parenteral) Outpatient/inpateint 1-3 wk
Severe InitialParenteral,switch to oral when possible
Inpatient; then outpatient 2-4 wk
Bone or Joint
No Residual infected tissue (eg. Postapmutation)
Parenteral or oral 1-5d
Residual infected soft tissue (but not bone)
Parenteral or oral 1-3 wk
Residual infected (but viable) bone InitialParenteral, then consideroral switch
4-6 wk
No surgery, or residual dead bone postoperatively
InitialParenteral, ten consider oral switch
> 3 mo

My approach and comments on diabetic foot osteomyelitis
• Osteomyelitis is first and foremost a clinical and pathological/microbiological diagnosis
• Labs and Imaging support your clinical suspicion of osteomyelitis– Plain radiographs are confirmatory– MRI is useful for surgical planning
• Bone biopsy (microbiologic and histopathology) remains our best diagnostic tool, but has pitfalls
• Treatment is based on clinical presentation• We are likely over utilizing IV in DFO in well-selected patients with
adequate surgical management


Case 1 – Surgical and Post-op Course
• OR – right 5th ray, partial resection, incision and drainage, excisional debridement
• Micro: Group B Strep, klebpneumo, enterobacter
• Pathology: – Proximal phalanx (+) OM at
metatarsal resection, – (+) Necrotizing Fasciitis
• ID Consulted – Ertapenem 1 g IV q 24 x 4 weeks

Case 1: Negative Pressure Wound Therapy is the ideal modality for managing deep diabetic foot ulcers post debridement:

Case 1 – Final Surgical and Post-op Course
• NPWT• Immobilization in Posterior Splint• Weekly Follow –ups• Repeat X-Rays, CRP, ESR - Stable• STSG at 8 weeks post-op• Prescriptive Footgear• Gradual Return to activity,
informal physical therapy• Close follow-up with Podiatry
and PCP• Wound free x 4 years

Case 2: Landscaper
HPI: 50-year-old-male with DM presented with a necrotic right 3rd
to with a sub metatarsal head ulcer draining purulence, forefoot redness, and swelling after stepping on a nail 1 month ago while landscaping. He admits to fevers and chills for 2 days.

Case 2- Physical Exam
• Vitals: T: 38 R: 20, HR 108, BP 88/58 R: 18
• General: Alert and oriented x 3 in NAD
• Vascular: (+) palpable pulses
– Cap refill < 3 sec
• Neuro: absent protective sensation
• MSK: edema, clawtoe deformities
• Derm: full thickness ulceration plantar foot, dusky 3rd digit with fluctuance, purulence, edema, callor, crepitation from the toe to the ankle,(+)pain

Case 2 – Initial ED work-up and Plan
Pertinent Labs: WBC 23.3, Hg 13.9, Hct 4, Glucose 635, ESR 82, CRP 22.7, BUN 65, Cr 4.42, Hg A1c 7.6, Lactate 1.5
X-rays: 3rd distal phalangeal erosion, osteolysis and soft tissue emphysema
Non-invasive Vascular Studies– Rt ABI 1.16, TBI 0.82, Toe
pressure 100 mmHg– Biphasic waveforms: popliteal,
PT, DPWIfI: Wound 2, Ischemia: 0 foot Infection 3

Gas gangrene on a diabetic foot is considered a surgical emergency
Often associated with mixed aerobic and anaerobic
Gradual progression with better prognosis if diagnosed early
More common than clostridial gas gangrene
Brucata et al, Diagnosis of Gas Gangrene: does a discrepancy exist between published data and practice. JFAS, 2014 March-April

Case 2 – Clinical Presentation
Post-op day 1 (s/p I and D, open 3rd toe amputation by surgery)
Foot is swollen, fluctuant with crepitus, and purulence

Case 2 – Surgical and Post-op Course
• Return to OR – Right 3rd ray partial resection, incision and drainage, excisional debridement
• Micro: Strep Viridans, Strep Milleri, mixed anaerobes
• Pathology: Skin and subcutis (+) Necrotizing Fascitis, clean margin at metatarsal
• ID Consulted –– Unasyn initially– Ceftriaxone 2 g IV q 24 hours and flagyl 500
mg PO q8h x 4 weeks– PO Augmentin 875 PO BID, Cipro 750 mg PO
BID

Case 2 – Surgical and Post-op Course
• NPWT• Immobilization in Posterior
Splint• Weekly Follow –ups• Repeat X-Rays, WBC,CRP, ESR -
Stable• Prescriptive Footgear• Gradual Return to activity• Close follow-up with Podiatry
and PCP

Case 3 – Store Owner/Manager
HPI: 79 y/o male with h/o DM, CKD. C/o right foot swelling x 2 weeks. PCP Rx’d PO abx.
- Admitted x 1 week, parenteral therapy. 2nd and 3rd digits, progressively becoming dusky.
- c/o mild pain at rest
ROS: (+) right foot worsening wound with increased discoloration and drainageFamily Hx:
– Brother with CAD s/p CABG, DM with pedal ulcers

Case 3 - Physical Exam
Vitals: T: 36, BP: 157/69, HR: 73, R: 20 SpO2 99Right Lower Extremity• Vascular:
– DP barely palpable, PT nonpalpable– Audible monophasic signals to DP, PT and perforating
peroneal
• Neurological: absent protective sensation with 5.07 SW monofilament
• Dermatological:– Impending tissue loss and necrosis of the 2nd and
3rd digits with apparent fluctuant abscess along the dorsum.
– Localized erythema, edema– Cold, dusky 2nd and 3rd dgits– Absent pedal hair growth
• Msk: – Mild pain on palpation– (+) equinus

Labs/Radiographs
Pertinent Labs WBC 10.5 Hg 9.4 Hct 29 ESR 115 CRP 17.4 BUN 71 Cr: 6.21 Albumin 2.1 HgA1c: 7.7
X-rays: no obvious osteomyelitis Clearly see metatarsal artery calcification

Initial Plan
- Operative 2nd and 3rd toe amputations, Incision and drainage of the abscess and excision of necrotic tissue
- Micro: none, but (+) swab, Staph Epi
- Pathology: (+) gangrenous necrosis and osteomyelitis of the digits
- ID recs: Aztreonam 500 mg IV q 12 H
- Wound Care: Packing, wet to dryWIfI: wound 2, Ischemia: 2 Foot Infection: 0 (2)

Diabetes and PAD
PAD in patients with diabetes Primarily involves below knee vessels
Higher prevalence of long occlusions in the tibial arteries
Medial artery disease = fibrosis of the medial wall
Big Artery Disease (BAD) = atherosclerotic arterial disease Hypercholesterolemia and tobacco use
Small Artery Disease (SAD) = diabetic macroangiopathy, Diabetes and Renal Disease
Michael Edmunds et al. Diabetic Peripheral Arteriopathy: A tale of Two diseases, 2017Roberto Ferraresi et al. BAD transmission and SAD distribution: a new scenario for critical limb ischemia, 2018

Diabetic Peripheral Angiopathy is an Indicator of Poor Health
– More commonly found in CKD and diabetics• Older male patients
– Indicator of the severity and duration of diabetes– Association with
• Neuropathic foot ulcerations• PAD• Amputations• CV morbidity• Mortality
– Correlates with non-compressible arteries and elevated ankle brachial indices

Lower Extremity Amputation Risk Factors Associated with Elevated Ankle Brachial
Indices and Radiographic Artery CalcificationsEric Lew, DPM, FACFAS, Nicole Nicolosi, DPM AACFAS, Georganne Botek, DPM,
FACFAS
Journal of Foot and Ankle Surgery, 2015. Volume 54, Issue 3, Pages 473–477
Purpose
• Does an elevated ABI or poorly compressible arteries and radiographic artery calcification have prognostic value?
• What are the implications of such vasculopathy in patients with diabetes?

BAD SAD

Conclusions
• 1. Elevated ABIs, poorly compressible arteries, and radiographic artery calcifications:
– Prognostic risk factors for amputation and delayed wound healing
• 2. U-shaped relationship between low and high ABIs:
– High ABI or PCA are equally prognostic as having a low ABI
• 3. Radiographic calcific vasculopathy in patients with DM or CKD is significant
– Considered an individual risk factor for LE amputation

TCPO2 is useful to determine healing potential

Case 3: Transferred to UNMH for Non-Invasive Vascular Exams
- Right ABI 0.77
- Right TBI 0.37
- Rt Great Toe pressure 36 mmHg
- Waveforms:- Triphasic common femoral
and popliteal
- Monophasic DP and PT

Case 3: Second Surgical Encounter
• Consulted Vascular Surgery • Right LE angiogram
– 3rd order cannulation of peroneal and anterior tibial– peroneal angioplasty, entire length with 3.5-3 mm tapered angioplasty balloons– Intra-op findings:
• Patent common femoral, proximal profunda and SFA• SFA- significant calcifications, mild stenosis in distal segment• Popliteal – patent but calcified• Tibioperoneal trunk – patent• Posterior tibial - stenosis• Run-off:
– anterior tibial with moderate stenosis at ankle and microvascular disease at the dorsalis pedis– Peroneal artery – high grade stenosis entire length to the bifurcation with collateralization
• Main inline vessel to the foot is the perforating peroneal artery.

Post-intervention; not responding to NPWT…What Next?

Which level of amputation will he heal?
A. Transmetatarsal
B. Chopart’s
C. Symes
D. Transtibial

Case 3: Third Surgery
TMA
• Micro: negative growth
• Pathology: (+) OM but (-) at resection margin
• ID Consult:
– D/C’d Aztreonam (completed 4 weeks)
– Transitioned to PO Doxycycline 100 mg BID x 2 weeks post TMA

Case 3: Follow-up
5 days post-op
Day of Surgery
8 weeks post-op

Long-term Follow-up
• Close surveillance
• Gradual Return to activity
• Prescriptive AFO, shoes/inserts
• AV Fistula and HD

Case 4 – Construction Painter
• HPI: 60 y/o male• Relates 2 week h/o of “bad callous”• Left 5th toe is turning dusky, malodorous
swollen and mildly painful foot
• PMH: DM, HTN, Tobacco use• Surg Hx: None• All: NKDA• Fam Hx: unknown• SocHx:
– Painter, Life long ETOH, Tobacco, no current illicit drug use
• ROS: (+) fever, chills, nausea and vomiting

Case 4- Physical Exam
• Vitals: T 38.1, HR 100, R: 18, BP 144/82• General: Alert and oriented x 3 in NAD• Vascular: (+) non palpable DP or PT
– No cap refill to 5th digit, delayed all– Monophasic signals
• Neuro: diminished protective sensation• MSK: acute edema, and pain to palpation• Derm: full thickness tissue loss with bone
exposure, expanding tissue necrosis, fluctance erythema, edema along midfoot and plantar arch along the peroneal longus tendon (+) purulence, malodor

Case 4 – Initial ED work-up and Plan
Pertinent Labs: WBC 17.1, Hg 14.4, Hct 41, Hg A1c 8.1, Glucose 476, ESR 96, CRP 16.0, BUN 16, Cr 0.75, Lactate 1.6
X-rays: left 5th digit possible osteomyelitis, tissue loss and edemaMRI: (+) abscess periarticular 5th MPJ and to the dorsal plantar and lateral aspect. (+)osteomyelitis of the fifth metatarsal head and base proximal phalanx. (+) myonecrosis abductor digiti minimi, tenosynovitis extensor longus, and peroneals

Case 4– Initial ED work-up and Plan
• Non-Invasive Vascular Studies
– Left ABI 0.57, TBI 0.23, toe pressure 37 mmHg
– Monophasic waveforms: popliteal, PT, DP
– Diminished waveform: left great toe WIfI: Wound 2, Ischemia: 3, foot Infection: 3

Case 4 – Surgical Course
• Podiatry – Left 5th ray, partial resection,
incision and drainage, excisional debridement
• Vascular– Left endarterectomy of common
and deep femoral arteries
– External Iliac stenting
– Common femoral to popliteal artery bypass with great saphenous

Case 4 – Surgical and Post-op Course
• Return to OR for further incision and drainage and excisional debridement
• Micro: MSSA, Mixed Anaerobic Flora
• Pathology: gangrenous necrosis extending to fascia– Osteomyelitis negative at
metatarsal resection
• ID Consulted – Cefazolin 1 g IV q8h x 4 weeks (tenosynovitis)

Case 4 – Post-hospital Course
• NPWT, Regular debridement, Advanced Biologics
• Immobilization in Posterior Splint• Weekly Follow –ups• Repeat X-Rays, CRP, ESR - Stable• Prescriptive Footgear• Gradual Return to activity• Close follow-up with Podiatry,
Vascular and PCP

Conclusion
”Patients don’t care how much you know until they know how much you care.”
~ David Armstrong, DPM, MD, PhD

Special thanks and appreciation to:
UNM Internal Medicine and Family Medicine
Infectious Disease/OPAT
Ortho and Gen Surgery
First Choice Community Healthcare
IHS
UNMH Rehabilitation – Wound Care

CHILE Team

CHILE Consults and Appointments FAQ:
• 1. How do I get a hold of CHILE for consultations?– Check Amion (M-F)
– My Cell: 515-783-6791 or through Tiger Text
– CHILE APP – Leslie Dunlap
2. How do I schedule an appointment for a patient in CHILE?
– Non-urgent patients: CHILE Adhoc
– Urgent patients: CHILE Adoc plus a Chart Message to Eric Lew, Nancy Barrientos (CHILE Clinic Supervisor), and/or Valeria Quintana (CHILE Orthotech/MA)

Questions: [email protected]

References
David G. Armstrong, Lawrence A. Lavery, Sharone Stern, Lawrence B. Harkless, Is Prophylactic Diabetic Foot Surgery Dangerous? Journal of Foot and Ankle Surgery 35(6):585-589, 1996)Robert G. Frykberg, Nicholas J. Bevilacqua, Geoffrey Habershaw, Surgical off-loading of the diabetic foot. J Vasc Surg 2010;52:44S-58S.David Armstrong, Lawrence A. Lavery, Jefferery R. Vasquez, Brian Shorth, Heather R. Kimbriel, Brent P Nixon, Andrew JM Boulton. Clinical Efficacy of the First Metatarsophalangeal Joint Arthroplasty as a Curative Procedure for Hallux Interphalangeal Joint Wounds in Patients with Diabetes. DIABETES CARE, VOLUME 26, NUMBER 12, DECEMBER 2003Lawrence A Lavery, Effectiveness and safety of elective surgical procedures to improve wound healing and reduce re-ulceration in diabetic patients with foot ulcers. Diabetes Metab Res Rev 2012; 28(Suppl 1): 60–63.Oleg Petrov, Mark Pfeifer, Michael Flood, William Chagares, Christopher Daniele, Recurrent Plantar Ulceration Following Pan Metatarsal Head Resection. The Journal of Foot and Ankle Surgery 35(6):573-577, 1996D. G. Armstrong and R. G. Frykberg, Classifying diabetic foot surgery: towardA rational definition. Diabetic Medicine 20, 329–331Tyler P. Kearney, Nathan A. Hunt, Lawrence A. Lavery. Safety and effectiveness of flexor tenotomies to heal toe ulcers in persons with diabetes. Diabetes Research and Clinical Practice 89 (2010) 224 – 226Michael J Mueller, David R Sinacore, Mary Kent Hastings, Michael J aSTrube, Jeffrey Johnson, Effect of Achilles Tendon Lengthening on Neuropathic Plantar Ulcers. A Randomized Clinical Trial. The Journal of Bone and Joint Surgery, Vol 85-A. No. 8, 2003Gareth David Griffiths, FRCS, Thomas Jeffery Wieman, MD. Metatarsal Head Resection for Diabetic Foot Ulcers. Arch Surg. 1990;125:832-835Giurini JM; Basile P; Chrzan JS; Habershaw GM; Rosenblum BL, Panmetatarsal head resection .A viable alternative. JAPMA, Vol 83; 2 1993, 101-107A. Piaggesi, E. Schipani, F. Campi, M. Romanelli, F. Baccetti, C. Arvia, R. Navalesi. Conservative Surgical Approach Versus Non-surgical Management for DiabetiNeuropathic Foot Ulcers: a Randomized Trial. Diabet. Med. 15: 412–417 (1998)Armstrong, David G;Stacpoole-Shea, Susan;Nguyen, Hienvu;Harkless, Lawrence B, Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the Foot. Journal of Bone and Joint Surgery; Apr 1999; 81, 4Per Holstein, Michael Lohmann, Mikael Bitsch, Bo Jørgensen, Achilles tendon lengthening, the panacea for plantar forefoot ulceration? Diabetes Metab Res Rev 2004; 20(Suppl 1): S37–S40.





























