Embed Size (px)
Citation preview

Initial Management of Complex
Pelvic Fractures
Jeffrey Anderson, MDSaint Mary’s Trauma Center
05 May 2011

Course Objectives
• Identify high risk pelvic fractures
• Attain basic knowledge of biomechanics involved
with pelvic fractures
• Understand initial management strategy for
complex pelvic fractures
• Awareness of potential pitfalls in management
• Understand which patients require angiographic
studies versus exploratory laparotomy

Overview of Problem
• Common: 5-10% of all high-speed MVC
occupants will sustain pelvic fractures
• High incidence of serious associated
injuries
• Highly lethal: some studies show a mortality
approaching 50%
• Good outcomes require a rapid and
multidisciniplary team approach

Bony Pelvic Anatomy
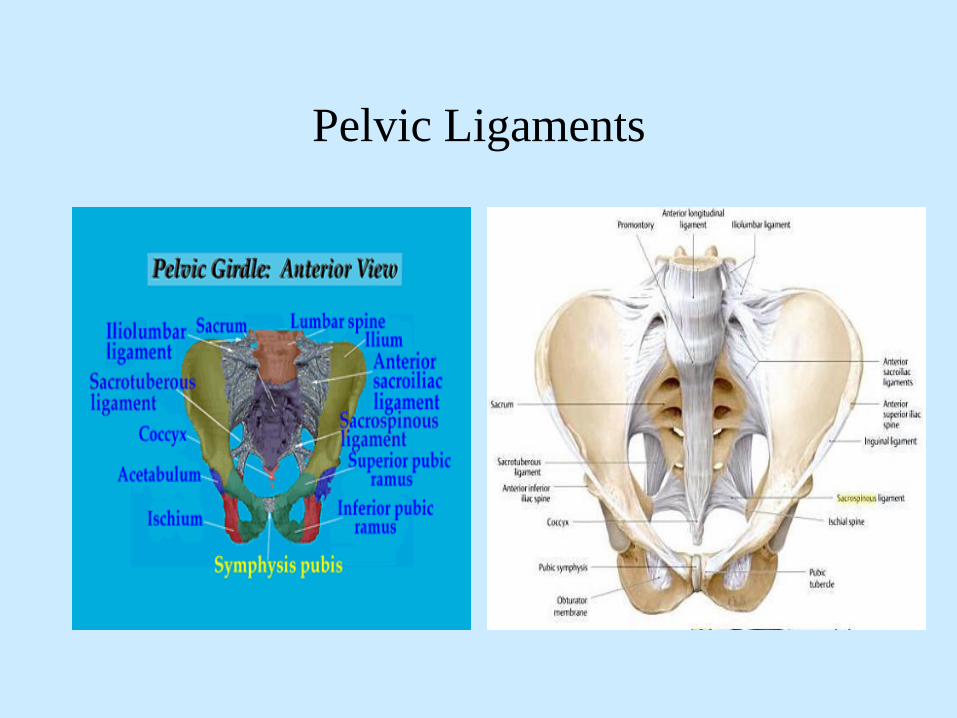
Pelvic Ligaments

Pelvic Ligaments
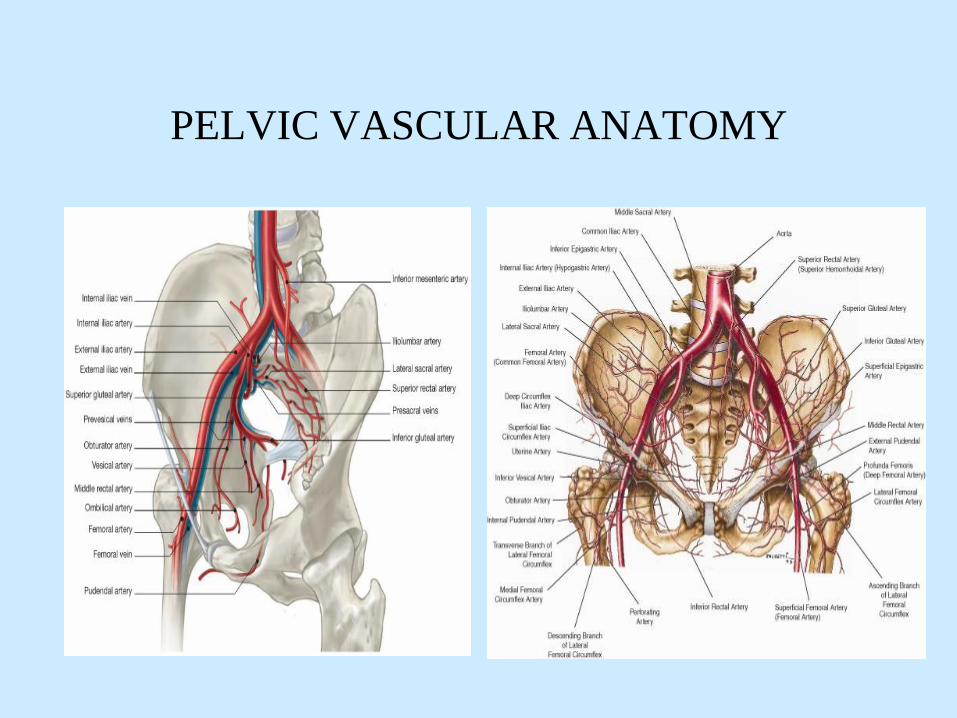
PELVIC VASCULAR ANATOMY

PELVIC VASCULAR ANAOTMY
With high impact pelvic
fractures approximately
15-20% of bleeding is
arterial; from branches of
internal iliac arteries
PELVIC STABILITY
• Bony pelvis has no inherent stability
– pelvic stability highly dependent on ligaments
• Symphysis and sacral-iliac ligaments
• Fractures of the pelvis imply high energy forces
• MVC, MCC
• pedestrian vs auto
• fall from height
• pelvis is a bony ring and hence fractures typically occur at
two or more sites

PELVIC STABILITY
• Anterior stability
– Pubic symphysis and pubic bones act as a strut
• sectioning of the symphysis creates a diastasis of less than 2.0
cm
• Posterior stability
– stability depends on integrity of sacroiliac complex
• sectioning of the symphysis and the anterior sacroiliac
ligaments allows symphysis to separate > 2.5 cm
• sectioning of the symphysis and both anterior and posterior
sacroiliac ligaments allows for vertical instability

Pelvic Ligaments
• Major contributor to
pelvic stability• Pubic symphysis
• Anterior and posterior
sacroiliac ligaments

Young and Burgess Classification
of Pelvic Fractures
• Useful in the clinical setting
• Addresses injury mechanism and
• Seeks to quantify forces involved
– anterior posterior compression
– lateral compression
– vertical shear
– combination

• Young and Burgess Classification Pelvic Fractures
– AP compression (APC) - direct anterior force
• Type 1: disruption of pubic symphysis < 2.0 cm
– low energy forces (sports)
– stable
• Type 2: symphysis > 2.0 cm and disruption of
anterior SI ligaments
– high energy, “open book”; MVC, ped vs auto
– unstable
– high risk hemorrhage
• Type 3: symphysis > 2.0 cm and disruption of
anterior and posterior SI ligaments
– very unstable
– highest incidence of major hemorrhage

Anterior-Posterior Compression (APC)
• APC 1
– anterior force of mild-
moderate force (sports)
– symphysis separation
< 2cm
– stretching of anterior
sacroiliac ligaments
– stable fracture

Anterior-Posterior Injury
• Grade I
• Symphysis < 2cm
• SI joints intact
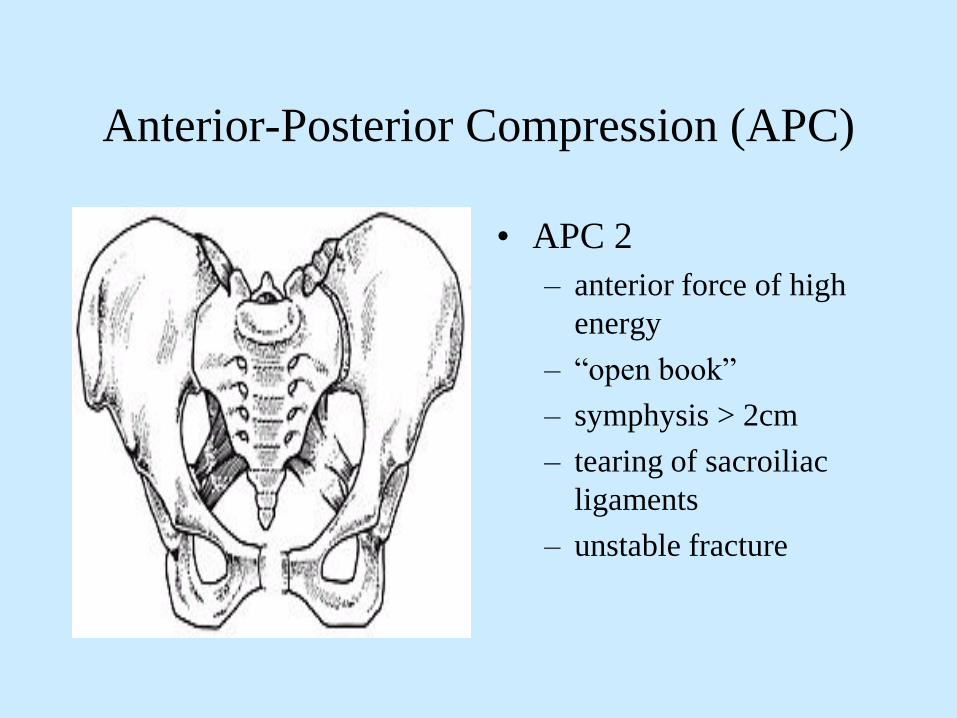
Anterior-Posterior Compression (APC)
• APC 2
– anterior force of high
energy
– “open book”
– symphysis > 2cm
– tearing of sacroiliac
ligaments
– unstable fracture

Anterior-Posterior Compression (APC)
• APC 3
– high energy force
– hemipelvis rotates
externally
– symphysis >2cm
– rupture of anterior &
posterior sacroiliac
ligaments
– highest incidence of
major hemorrhage
– unstable fracture
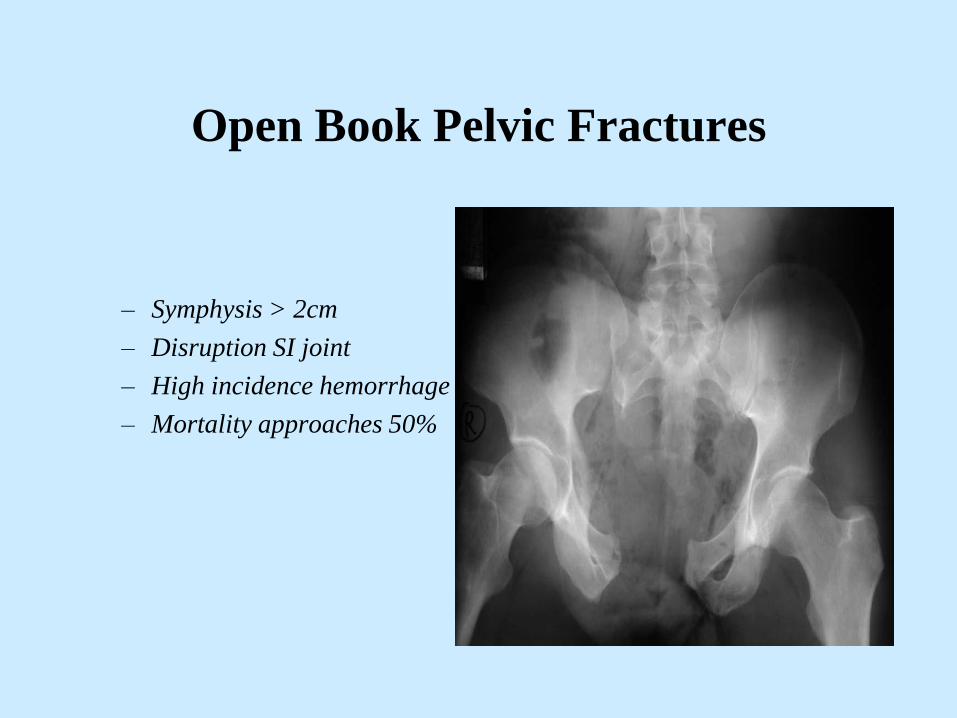
Open Book Pelvic Fractures
– Symphysis > 2cm
– Disruption SI joint
– High incidence hemorrhage
– Mortality approaches 50%

• Young and Burgess
– lateral compression (LC)
• Type 1: unilateral rami fracture and ipsilateral
sacroiliac compression - stable
• Type 2: unilateral rami fracture and ipsilateral
posterior sacroiliac fracture
– unstable fracture
– high risk for hemorrhage
• Type 3: type 2 plus injury to contralateral
hemipelvis
– unstable fracture
– high risk for hemorrhage

Lateral Compression Fractures
• Type I:
• Pubic rami fracture
• Sacral compression
• stable
• Type 2:
• Pubic rami fracture
• Iliac fracture
• Unstable
• Higher incidence
hemorrhage

Lateral compression fractures
• Bilateral pubic rami fractures
• Sacral deformity / fracture
• Lateral compression type fractures are usually stable and rarely hemodynamically unstable
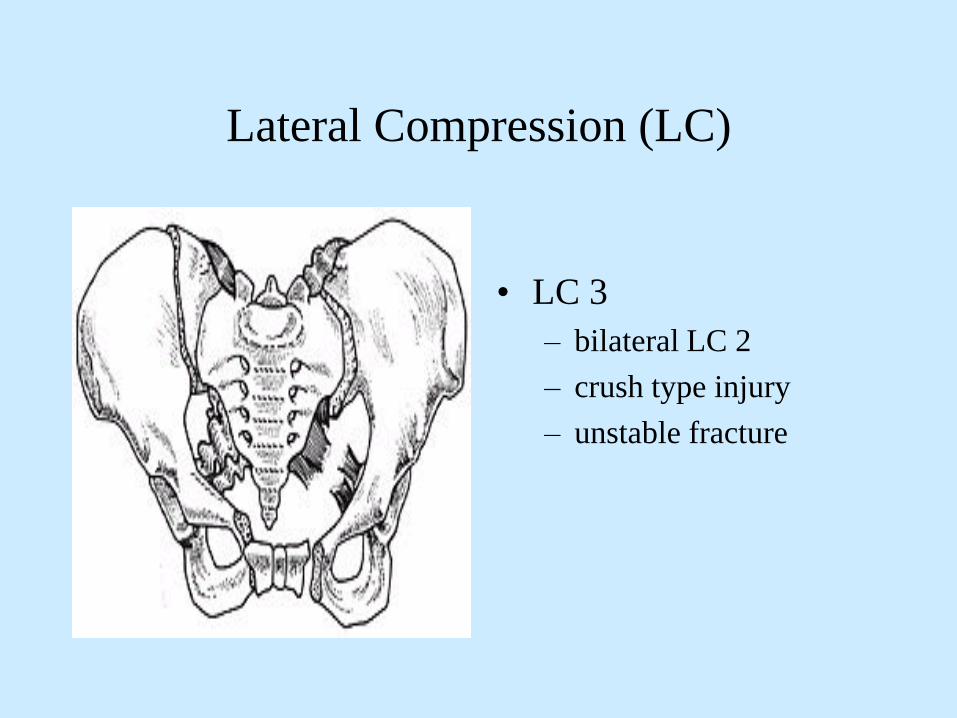
Lateral Compression (LC)
• LC 3
– bilateral LC 2
– crush type injury
– unstable fracture

Classification Pelvic Fractures
• Young and Burgess
– vertical shear (VS): fall
from a height
• Vertical displacement
of hemipelvis
• unstable
• high incidence of
hemorrhage

VERTICAL SHEAR
• Complete disruption of
hemipelvis
• anterior and posterior
vertical displacement
• fall from a height
• high incidence of pelvic
hemorrhage
• unstable pelvis

UNSTABLE PELVIS
• APC2, APC3, LC2, LC3,
VS, and combination
injuries are all unstable pelvic
fractures and are associated with a
higher incidence of vascular
disruption and hemodynamic
compromise
• this does not imply that bony
instability equates to hemodynamic
instability

Pelvic Fractures
• High energy
– MVC, falls from
height, crush injury
– 75% associated injuries
– 15-25% intra-
abdominal injuries
– often hemodynamically
unstable
– mortality up to 55%
• Low energy
– falls from standing
• Lateral compression
– elderly / osteopenic
– associated injuries
uncommon
– hemodynamically
stable
– mortality < 1%

AP Pelvis Radiograph
• Indicators of potential
vasculature injury:• diastasis symphysis >
2.0 cm
• fractures all 4 rami
• widening SI joint >0.5
cm
• vertical displacement at
the SI joint

High Energy Pelvic Fractures
• MVC, auto-pedestrian, motorcycle accidents
• 5-10% of high speed MVCs will sustain pelvic fractures
• mortality correlates highly to hemodynamic stability
• stable < 4%
• unstable > 50%
• mortality:
• 50% acute hemorrhage
• 25% associated injuries
• 25% sepsis / MODS
• associated injuries: TBI, thoracic, intra-abdominal
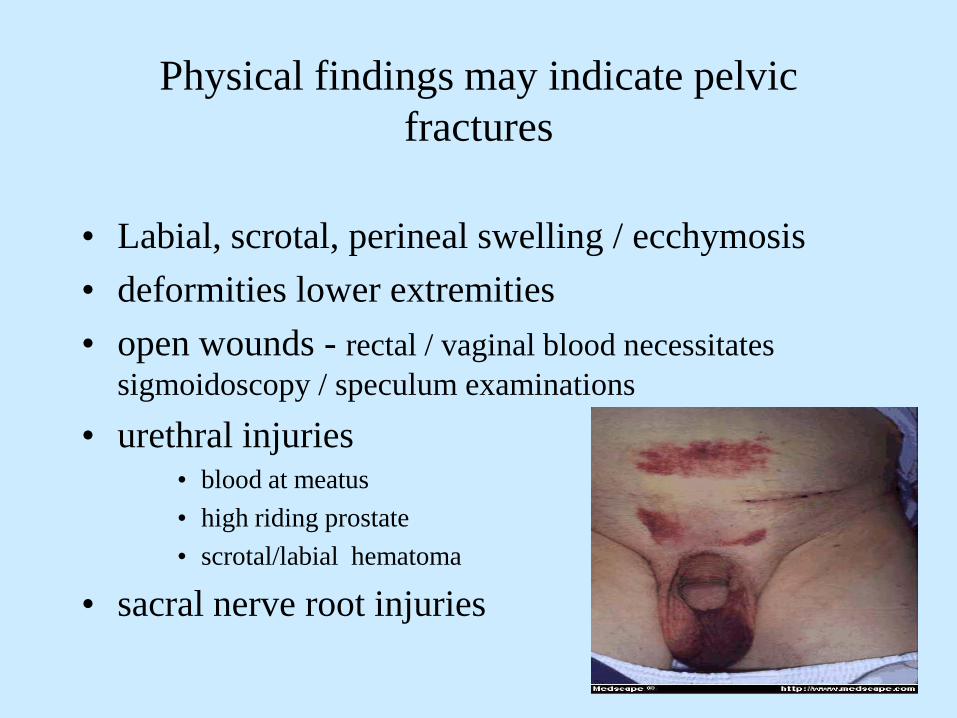
Physical findings may indicate pelvic
fractures
• Labial, scrotal, perineal swelling / ecchymosis
• deformities lower extremities
• open wounds - rectal / vaginal blood necessitates
sigmoidoscopy / speculum examinations
• urethral injuries• blood at meatus
• high riding prostate
• scrotal/labial hematoma
• sacral nerve root injuries

• Physical maneuvers to establish pelvic
stability are of questionable benefit
• pelvic rock, springing, compression, distraction are
crude and insensitive
• exacerbate hemorrhage and soft tissue injury
• painful and unnecessary maneuvers
– initial pelvic radiographs better indicator of stability

Routine Pelvic X-rays
• Examination of the pelvis is extremely unreliable;
especially in the obtunded, intoxicated, or obese patients
• Routine A-P pelvic and chest x-ray is still indicated in the
multiply or obtunded injured patient

• Hemorrhage in pelvic fractures:
– Venous bleeding (85%)
• fracture surfaces of cancellous bone
• venous plexuses
– Arterial bleeding (15%) - from branches of the superior
gluteal artery ( fracture through sciatic notch) or other branches of
internal iliac artery
• Most common source of significant hemorrhage in
pelvic fractures is NOT the pelvis

Pelvic Stabilization
• Purpose:• controls non-arterial hemorrhage
• aids in clot formation
• decreases fracture site movement and clot
dislodgement
• decreases volume of pelvis and promotes tamponade
• exact mechanism in which stabilization decreases
hemorrhage has not been elucidated

Pelvic Stabilization
• Three basic methods:• non-invasive techniques
• external fixation
• open reduction / internal fixation

Pelvic Stabilization
• 1. Non-invasive techniques:– Sheet wrap
– Proprietary devices / binders
• Most appropriate in the trauma bay for unstable
pelvic fractures
• temporary measures
• Controls hemorrhage as effectively as external
fixation
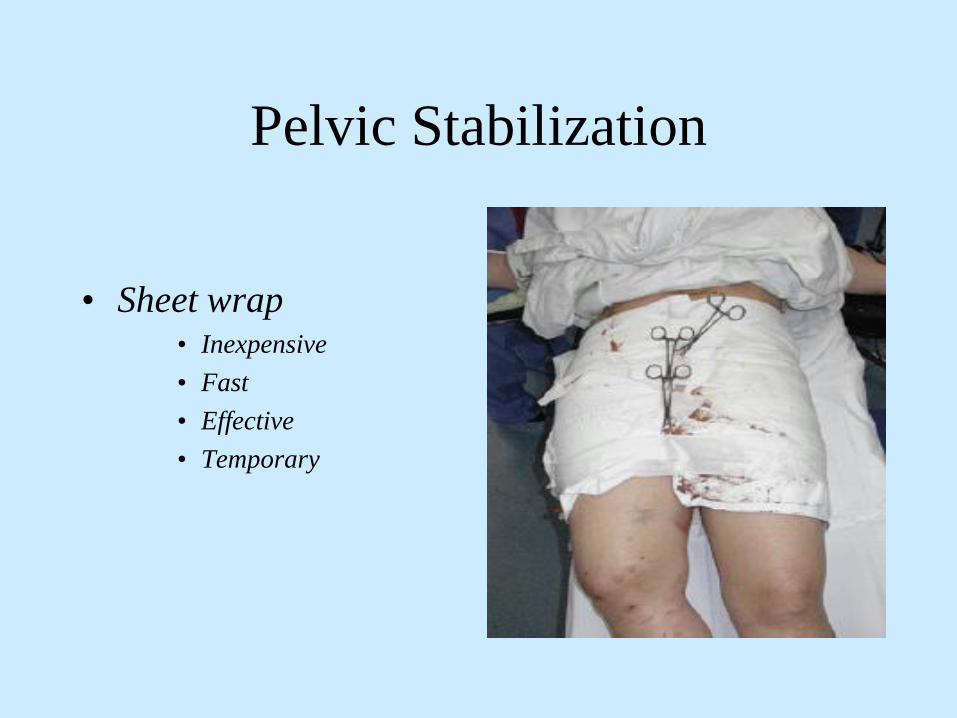
Pelvic Stabilization
• Sheet wrap• Inexpensive
• Fast
• Effective
• Temporary

Pelvic Binders
• T POD
– Cost: $125.00
– Fast
– Efficient
– Temporary

T-Pod: Non-invasive Pelvic Stabilization

Pelvic Stabilization
• External fixation devices:• anterior fixation device - ideally suited for “open-book”
deformities
• C-clamp device - ideally suited for posterior disruptions
– unstable pelvic fractures associated with hypotension
– can be placed in the trauma bay, OR, ICU
– should be placed prior to skin incision in patients
needing a laparotomy
– complications / drawbacks:
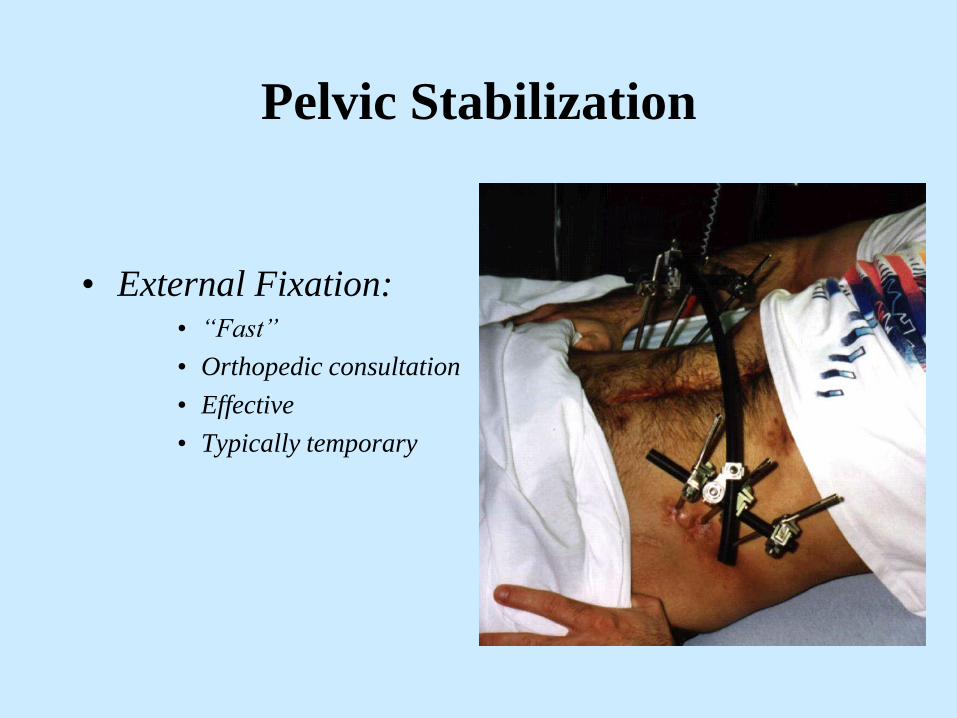
Pelvic Stabilization
• External Fixation:• “Fast”
• Orthopedic consultation
• Effective
• Typically temporary
External Fixation
• Should be applied as soon as possible with unstable pelvis
• May be applied in trauma bay, OR, or TICU
• Anterior bridging bars placed low over pelvis so as not to interfere with laparotomy incision
• Ideally placed prior to laparotomy

External Fixation

Pelvic Stabilization
• Internal stabilization:• limited value in the
acute setting
– occasionally used in
“open-book”
deformities after
laparotomy in the
stable patient
• reserved for patients
who are
hemodynamically stable
• definitive treatment

• No convincing data to support one method of pelvic stabilization over another in the acute setting:
• all methods equally effective
• T-POD HAS GAINED WIDE EXCETANCE
• But studies do support some form of bony stabilization
• decreases hemorrhage
• decreases transfusion requirements
PRINCIPLES OF ANGIOGRAPHY AND
EMBOLIZATION
• Used to control bleeding that cannot be corrected with
surgery
• Purpose is to slow bleeding rather than create large areas
of ischemia and necrosis
• Limit areas of ischemia and necrosis to smallest extent
possible
• Must be done expeditiously prior to onset of “lethal triade”

Angiography
• HEMORRHAGIC SHOCK:
• Surgically correctable injuries directly to operating room
• Non-surgically correctable injuries to angiographic department
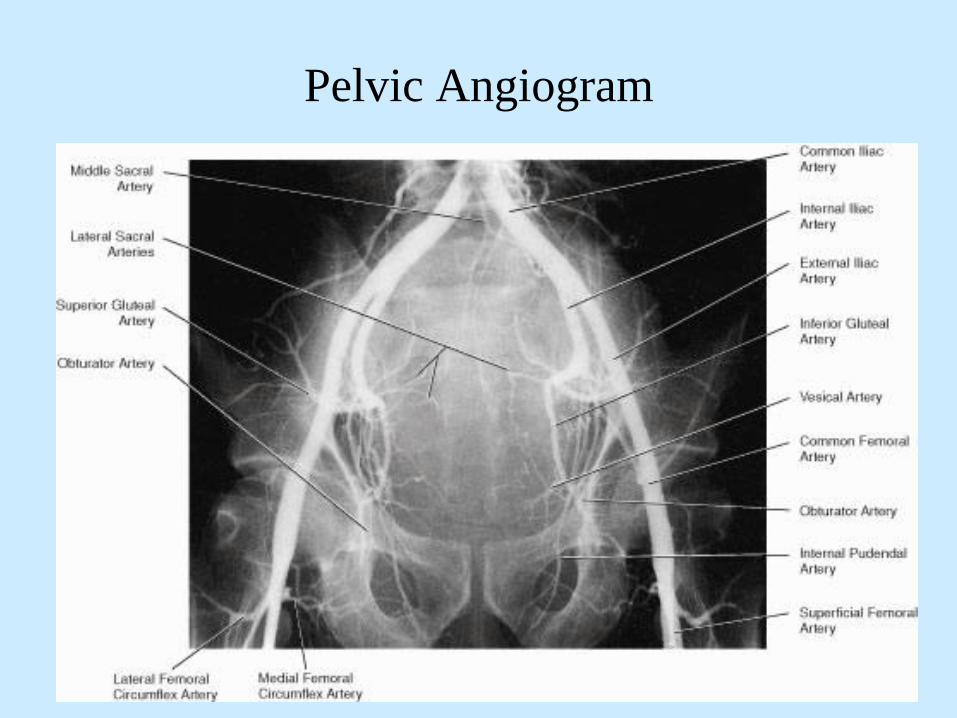
Pelvic Angiogram

Angiography
• Approximately 7-11% of pelvic fractures will require
embolization to control arterial bleeding.
• lateral compression fractures: 2%
• anteroposterior compression: 20%
• vertical shear injury: 20%
• combination: 20%
• Approximately 25-40% of cases will require embolization of more
than one artery
• Segina, D., Agnew,S., OTA Annual Meeting 2000

Angiographic Embolization
• Embolization is only
effective for arterial
source of hemorrhage
-90% effective

When To Transfer to Angiography ?
• IMMEDIATELY:• Patients who are
hemodynamically
unstable as the result of
their pelvic fractures
AND if laparotomy is
not indicated

Hypotension and Associated High
Energy Pelvic Fracture
• Etiology of hypotension will be secondary
to non-pelvic sources at least 50% of time• thorax
• abdomen
• long bone fractures
• externally / at the scene

5 Major Sites of Blood Loss
• Chest
• Abdomen
• Retroperitoneum
• Muscle compartment of thigh
• Injury scene

Problem!
• Where is the source of hemorrhage / hypotension?
– If solely related to the pelvic fracture(s) - then
angiography and embolization is the best and initial
therapeutic option
– If hemorrhage secondary to an abdominal injury then
laparotomy is the best and initial therapeutic option
– If hemorrhage secondary to a thoracic injury then tube
thoracostomy and possibly thoracotomy is indicated
• How to determine source of bleeding?

Diagnosing intra-abdominal hemorrhage
• FAST
• Diagnostic peritoneal lavage (DPL)
• Diagnostic peritoneal tap: supra-umbilical
approach appears to be the most reliable test for intra-
abdominal hemorrhage, which requires laparotomy
• CT scan
• E.A.S.T., Practice Management Guidelines, 2001

Focused Abdominal Sonography for Trauma
• FAST
• Ultrasound examination to
determine presence of free
fluid in the pericardial or
peritoneal cavities
• High sensitivity /
specificity

Diagnostic Peritoneal Lavage
Diagnostic Peritoneal Tap
• Catheter introduced
through a supraumbilical
incision
• 5-10cc gross blood is
positive tap and an
indication for immediate
laparotomy
• 1 liter crystalloid solution
infused

Critical Questions ?
• Which patients warrant early pelvic
stabilization?
• Which patients warrant pelvic angiography
and possible embolization?
• Which patients warrant emergent
laparotomy?
Early Pelvic Stabilization
• Patients with unstable pelvic fractures
associated with hypovolemia
• All patients with “unstable pelvis”
diastasis of symphysis > 2.0
cm
fractures all 4 rami
widening SI joint >0.5 cm
vertical displacement at the
SI joint

Early Angiography
• Pelvic fractures with signs of ongoing hemorrhage after non-pelvic sources of blood loss have been ruled-out
• Patients with pelvic fractures with ongoing hemorrhage that cannot be controlled at laparotomy
• Arterial extravasation noted in pelvis on CT scan
Emergent Laparotomy
• Patients with hypotension and gross blood
in the abdomen or evidence intestinal
perforation
• FAST / DPL are most reliable diagnostic
tests

Initial Management
• initial assessment: “ABCDE’s”
• radiographic assessment: CXR, A-P pelvis, FAST
• hemodynamically unstable patients:
– 50% of patients with severe pelvic fractures are
bleeding from sources other than the pelvis
– associated injuries very common
– determine source of hemorrhage!!

• “patients in hemorrhagic shock with a
surgically correctable lesion should be
transported to the OR”
• “patient in hemorrhagic shock with an
unknown source of bleeding, as well as,
lesions best treated by embolization should
be transported to the angiography suite”
• Bassam, D., Am. Surg., 1998, 862-867

When to perform laparotomy
• Indications for laparotomy in the face of
hypotension and pelvic fractures remain the same
• intra-abdominal hemorrhage
• intestinal perforation
• peritoneal signs

Intraoperative Management
• If laparotomy is required for ongoing bleeding:
• control non-pelvic sources of hemorrhage
• if pelvic bleeding identified; enlarging hematoma
– do not open retroperitoneum
– pack pelvis
– exercise damage control
– escort patient to angiography suite: embolization is the
best method to control pelvic arterial bleeding; effective in
90% of cases
Open Pelvic Fractures
• Fracture site communicates through the skin, rectum,
vagina
• High incidence of associated injuries, mortality approaches
80%
• Vital to make diagnosis early - blood in rectum / vagina
necessitates further evaluation
• basic tenants apply to all open fractures - thorough irrigation
and debridement, prophylactic antibiotics, fracture stabilization

Open Pelvic Fractures
• Treatment same
• Early prophylactic
antibiotics• ancef / gentamycin

CONCLUSION
• Do not delay treatment
• Priorities remain the same: ABCDE’s
• Pelvic stabilization mandatory
• Rule –out other sources of bleeding
• Exploratory laparotomy: indications remain the same
• Angiography / embolization: must be considered
early to mobilize appropriate personnel
• early transfer to a trauma center may be life
saving